2/17/2009 1 Pharmacology: Pharmacology: Therapeutics of Calcium Metabolism Therapeutics of Calcium Metabolism John P. Bilezikian, M.D. John P. Bilezikian, M.D. Professor of Medicine and Pharmacology Professor of Medicine and Pharmacology Chief, Division of Endocrinology Chief, Division of Endocrinology February 18 2009 February 18 2009 February 18, 2009 February 18, 2009 Outline of Lecture • Hypercalcemia Hypercalcemia • Hypocalcemia Hypocalcemia • Osteoporosis Osteoporosis

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
2/17/2009
1
Pharmacology: Pharmacology: Therapeutics of Calcium MetabolismTherapeutics of Calcium Metabolism
John P. Bilezikian, M.D.John P. Bilezikian, M.D.Professor of Medicine and PharmacologyProfessor of Medicine and Pharmacology
Chief, Division of EndocrinologyChief, Division of EndocrinologyFebruary 18 2009February 18 2009February 18, 2009February 18, 2009
Outline of Lecture
•• HypercalcemiaHypercalcemia•• HypocalcemiaHypocalcemia•• OsteoporosisOsteoporosis
2/17/2009
2
CAUSES OF HYPERCALCEMIACAUSES OF HYPERCALCEMIA
•• Primary Primary HyperparathyroidismHyperparathyroidism
•• Vitamin DVitamin DToxicityToxicity
•• MalignancyMalignancy•• Other endocrinopathyOther endocrinopathy
HyperthyroidismHyperthyroidismPheochromocytomaPheochromocytomaVIPomaVIPomaAdrenal insufficiencyAdrenal insufficiency
•• MedicationsMedicationslithiumlithium
yyGranulomatous diseaseGranulomatous disease
–– TuberculosisTuberculosis–– SarcoidosisSarcoidosis–– Any otherAny other
•• LymphomaLymphoma•• FHHFHH•• ImmobilizationImmobilization
thiazide diureticsthiazide diureticsthyroid hormone thyroid hormone Vitamin AVitamin AVitamin DVitamin D
•• Acute or chronic renal Acute or chronic renal diseasedisease
Clinical Features of HypercalcemiaClinical Features of Hypercalcemia
•• ConstitutionalConstitutional
•• Central nervous systemCentral nervous system
•• Gastrointestinal tractGastrointestinal tract
•• RenalRenal
•• CardiovascularCardiovascular
2/17/2009
3
Factors That Influence SymptomatologyFactors That Influence Symptomatologyin Hypercalcemiain Hypercalcemia
S l i t tiS l i t ti•• Serum calcium concentrationSerum calcium concentration•• Rate of riseRate of rise•• DurationDuration•• Individual variabilityIndividual variability
Pathophysiologic Features of Pathophysiologic Features of Acute HypercalcemiaAcute Hypercalcemia
I. New or Existing Stimulus to HypercalcemiaI. New or Existing Stimulus to Hypercalcemia•• Osteoclast activation virtually always presentOsteoclast activation virtually always presentOsteoclast activation virtually always presentOsteoclast activation virtually always present•• Renal tubular conservation of calcium (PTH, PTHRP)Renal tubular conservation of calcium (PTH, PTHRP)•• GI hyperabsorption of calcium (less important)GI hyperabsorption of calcium (less important)•• Reduced mobilityReduced mobilityII. Hypercalcemia Becomes SymptomaticII. Hypercalcemia Becomes Symptomatic
P l iP l i•• PolyuriaPolyuria•• PolydypsiaPolydypsia•• AnorexiaAnorexia

2/17/2009
4
Pathophysiologic Features of Pathophysiologic Features of Acute HypercalcemiaAcute Hypercalcemia
III. Worsening HypercalcemiaIII. Worsening Hypercalcemia•• Reduced fluid intakeReduced fluid intake•• Continued polyuriaContinued polyuria•• DehydrationDehydrationIV. Reduced Plasma VolumeIV. Reduced Plasma Volume•• Impaired renal functionImpaired renal functionImpaired renal functionImpaired renal function•• Reduced renal calcium clearanceReduced renal calcium clearance•• Rapidly worsening hypercalcemiaRapidly worsening hypercalcemia
At What Level Should HypercalcemiaAt What Level Should HypercalcemiaBe Treated Emergently?*Be Treated Emergently?*
•• < 12 mg/dL ?< 12 mg/dL ?
•• 1212--14 mg/dL ?14 mg/dL ?
•• >14 mg/dL ?>14 mg/dL ?
*Typical nl range 8.4-10.2 mg/dl

2/17/2009
5
General Management of HypercalcemiaGeneral Management of Hypercalcemia
•• Intravenous rehydrationIntravenous rehydration•• Saline administrationSaline administration•• Diuresis with furosemideDiuresis with furosemide•• Dialysis (if necessary)Dialysis (if necessary)•• MobilizationMobilization•• MobilizationMobilization
2/17/2009
6
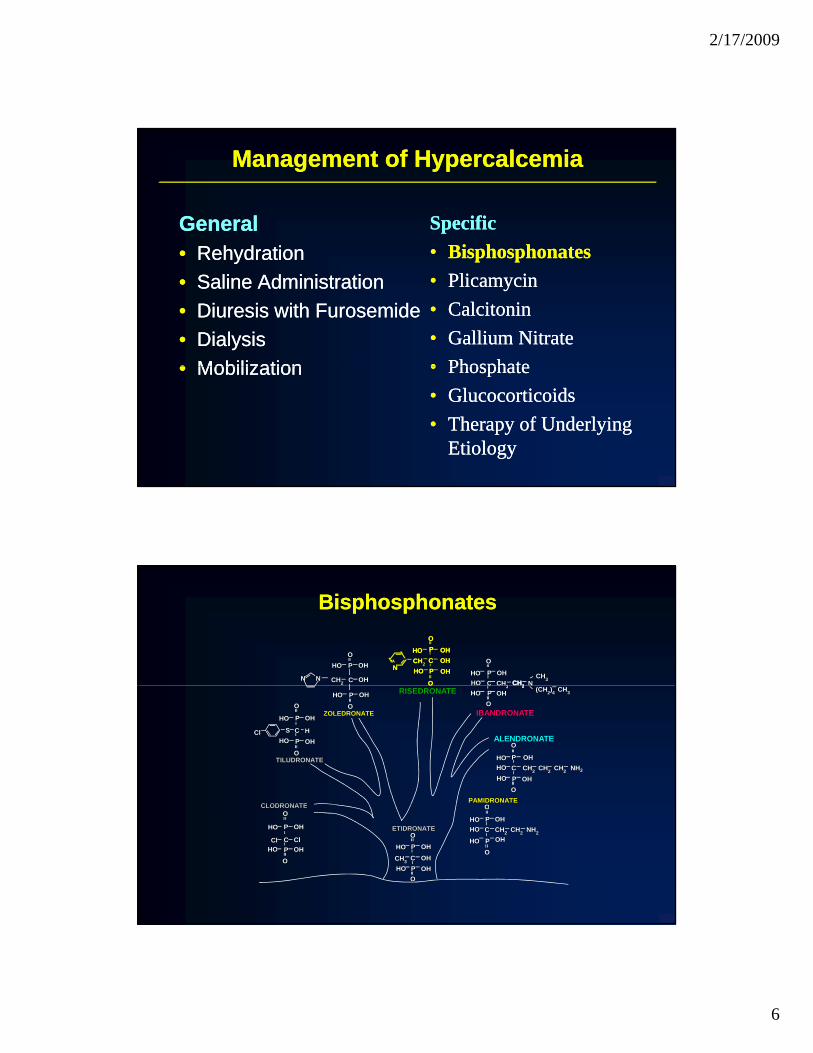
Management of HypercalcemiaManagement of Hypercalcemia
GeneralGeneralR h d tiR h d ti
SpecificSpecificBi h h tBi h h t•• RehydrationRehydration
•• Saline AdministrationSaline Administration•• Diuresis with FurosemideDiuresis with Furosemide•• DialysisDialysis•• MobilizationMobilization
•• BisphosphonatesBisphosphonates•• PlicamycinPlicamycin•• CalcitoninCalcitonin•• Gallium NitrateGallium Nitrate•• PhosphatePhosphate•• MobilizationMobilization •• PhosphatePhosphate•• GlucocorticoidsGlucocorticoids•• Therapy of Underlying Therapy of Underlying
EtiologyEtiology
PPCC
OO
HOHO OHOHCHCH22HOHO CHCH22 NN
CHCH33
PPP
CCCPPP
OOO
OOO
HOHOHO OHOHOH
OHOHOHHOHOHOOHOHOHCHCHCH22NNN
NN NN CHCH32 CC
PPHOHO OHOHOO
OHOH
BisphosphonatesBisphosphonates
OO
PPCCPP
OO
OO
HOHO OHOH
OHOHHOHOCHCH22HOHO CHCH22 CHCH22 NHNH22
CCPPOO
OHOHHOHOCHCH22HOHO CHC 22 NN
(CH(CH22))44 CHCH33
PP
CCPP
OO
OO
HOHO OHOH
OHOHHOHOHHSSClCl
PAMIDRONATEPAMIDRONATE
ALENDRONATEALENDRONATE
IBANDRONATEIBANDRONATE
RISEDRONATERISEDRONATE
TILUDRONATETILUDRONATE
CLODRONATECLODRONATE
OOO
ZOLEDRONATEZOLEDRONATE
PPHOHO OHOH
OO
CHCH33
PP
CCPP
OO
OO
HOHO OHOH
OHOHHOHOClClClCl
PPCC
PP
OO
OO
HOHO OHOH
OHOHHOHOCHCH22HOHO CHCH22 NHNH22
ETIDRONATEETIDRONATE
CLODRONATECLODRONATE
PP
CCPP
OO
HOHO OHOH
OHOHHOHOOHOH
OO

2/17/2009
7
Bisphosphonates For Acute Hypercalcemia Bisphosphonates For Acute Hypercalcemia
•• Osteoclast inhibitorsOsteoclast inhibitors
•• Intravenous route necessaryIntravenous route necessary
•• Reduction in serum calcium begins Reduction in serum calcium begins 2424--36 hours after first dose36 hours after first dose
D ration of effect is ariableD ration of effect is ariable•• Duration of effect is variableDuration of effect is variable
PPCC
OO
HOHO OHOHCHCH22HOHO CHCH22 NN
CHCH33
PPP
CCCPPP
OOO
OOO
HOHOHO OHOHOH
OHOHOHHOHOHOOHOHOHCHCHCH22NNN
NN NN CHCH32 CC
PPHOHO OHOHOO
OHOH
Bisphosphonates for Bisphosphonates for hypercalcemia
OO
PPCCPP
OO
OO
HOHO OHOH
OHOHHOHOCHCH22HOHO CHCH22 CHCH22 NHNH22
CCPPOO
OHOHHOHOCHCH22HOHO CHC 22 NN
(CH(CH22))44 CHCH33
PP
CCPP
OO
OO
HOHO OHOH
OHOHHOHOHHSSClCl
PAMIDRONATEPAMIDRONATE
ALENDRONATEALENDRONATE
IBANDRONATEIBANDRONATE
RISEDRONATERISEDRONATE
TILUDRONATETILUDRONATE
CLODRONATECLODRONATE
OOO
ZOLEDRONATEZOLEDRONATE
PPHOHO OHOH
OO
CHCH33
PP
CCPP
OO
OO
HOHO OHOH
OHOHHOHOClClClCl
PPCC
PP
OO
OO
HOHO OHOH
OHOHHOHOCHCH22HOHO CHCH22 NHNH22
ETIDRONATEETIDRONATE
CLODRONATECLODRONATE
PP
CCPP
OO
HOHO OHOH
OHOHHOHOOHOH
OO

2/17/2009
8
Adverse Effects of ParenteralAdverse Effects of ParenteralEtidronate for HypercalcemaEtidronate for Hypercalcema
Hypocalcemia (“overshoot”)Hypocalcemia (“overshoot”)

2/17/2009
9
Pamidronate in the management of hypercalcemia
Zoledronate vs. Pamidronate For HypercalcemiaZoledronate vs. Pamidronate For Hypercalcemia
Mean Corrected Serum Calcium C at baseline and days 4, 7, and 10 after treatment of hypercalcemia with ( ) zoledronic acid 4mg, ( ) zoledronic acid 8mg, or ( ) pamidronate 90mg.
Major et al, J Clin Oncology, 2001Major et al, J Clin Oncology, 2001

2/17/2009
10
Management of HypercalcemiaManagement of HypercalcemiaZoledronate vs. PamidronateZoledronate vs. Pamidronate
ZoldronateZoledronate
Zoldronate4mg
Zoldronate8mg
Time to Relapse ofHypercalcemiaMedian Duration ofComplete Response
Zoledronate
Zoledronate
Zoledronate
0 10 20 30 40 50
Pamidronate90mg
DaysDaysMajor et al, J Clin Oncology, 2001Major et al, J Clin Oncology, 2001
Adverse Effects of Adverse Effects of Pamidronate and ZoledronatePamidronate and Zoledronate
•• Mild, transient fever (<2Mild, transient fever (<2°°C)C)
•• Transient leukopeniaTransient leukopenia
•• Small reduction in the serum Small reduction in the serum h h th h tphosphatephosphate
•• Hypocalcemia (“overshoot”)Hypocalcemia (“overshoot”)

2/17/2009
11
Management of HypercalcemiaManagement of Hypercalcemia
GeneralGeneralR h d tiR h d ti
SpecificSpecificBi h h tBi h h t•• RehydrationRehydration
•• Saline AdministrationSaline Administration•• Diuresis with FurosemideDiuresis with Furosemide•• DialysisDialysis•• MobilizationMobilization
•• BisphosphonatesBisphosphonates•• PlicamycinPlicamycin•• CalcitoninCalcitonin•• Gallium NitrateGallium Nitrate•• PhosphatePhosphate•• MobilizationMobilization •• PhosphatePhosphate•• GlucocorticoidsGlucocorticoids•• Therapy of Underlying Therapy of Underlying
EtiologyEtiology
PlicamycinPlicamycin
•• Potent osteoclast inhibitorPotent osteoclast inhibitor
•• Intravenous, daily for up to 5 daysIntravenous, daily for up to 5 days
•• Reduction in serum calcium Reduction in serum calcium begins 12begins 12--24 hours after first dose24 hours after first dose
•• Duration of effect is variableDuration of effect is variable

2/17/2009
12
Plicamycin
Adverse Effects of PlicamycinAdverse Effects of Plicamycin
•• Hypocalcemia (“overshoot”)Hypocalcemia (“overshoot”)
•• Hepatic toxicityHepatic toxicity
•• NephrotoxicityNephrotoxicity
•• Bone marrow toxicity (platelets)Bone marrow toxicity (platelets)
2/17/2009
13
Management of HypercalcemiaManagement of Hypercalcemia
GeneralGeneralR h d tiR h d ti
SpecificSpecificBi h h tBi h h t•• RehydrationRehydration
•• Saline AdministrationSaline Administration•• Diuresis with FurosemideDiuresis with Furosemide•• DialysisDialysis•• MobilizationMobilization
•• BisphosphonatesBisphosphonates•• PlicamycinPlicamycin•• CalcitoninCalcitonin•• Gallium NitrateGallium Nitrate•• PhosphatePhosphate•• MobilizationMobilization •• PhosphatePhosphate•• GlucocorticoidsGlucocorticoids•• Therapy of Underlying Therapy of Underlying
EtiologyEtiology
Calcitonin For HypercalcemiaCalcitonin For Hypercalcemia
•• Osteoclast inhibitorOsteoclast inhibitor•• CalciureticCalciuretic•• IV or SC, Q12 hoursIV or SC, Q12 hours•• Rapid reduction in calcium (within 12 Rapid reduction in calcium (within 12
hours)hours)hours)hours)•• Weak and shortWeak and short--lived effectlived effect

2/17/2009
14
Calcitonin in the management of hypercalcemia
The Most Rapidly Acting Agents The Most Rapidly Acting Agents For HypercalcemiaFor Hypercalcemia
Calcitonin>Plicamycin>BisphosphonatesCalcitonin>Plicamycin>Bisphosphonates

2/17/2009
15
Combination Therapy For HypercalcemiaCombination Therapy For Hypercalcemia
•• Use of a rapidly acting agent (calcitonin)Use of a rapidly acting agent (calcitonin)
•• Simultaneous with a more potent, but more Simultaneous with a more potent, but more slowly acting agent (bisphosphonate)slowly acting agent (bisphosphonate)slowly acting agent (bisphosphonate)slowly acting agent (bisphosphonate)

2/17/2009
16
Management of HypercalcemiaManagement of Hypercalcemia
GeneralGeneralR h d tiR h d ti
SpecificSpecificBi h h tBi h h t•• RehydrationRehydration
•• Saline AdministrationSaline Administration•• Diuresis with FurosemideDiuresis with Furosemide•• DialysisDialysis•• MobilizationMobilization
•• BisphosphonatesBisphosphonates•• PlicamycinPlicamycin•• CalcitoninCalcitonin•• Gallium NitrateGallium Nitrate•• PhosphatePhosphate•• MobilizationMobilization •• PhosphatePhosphate•• GlucocorticoidsGlucocorticoids•• Therapy of Underlying Therapy of Underlying
EtiologyEtiology
Management of HypercalcemiaManagement of Hypercalcemia
GeneralGeneralR h d tiR h d ti
SpecificSpecificBi h h tBi h h t•• RehydrationRehydration
•• Saline AdministrationSaline Administration•• Diuresis with FurosemideDiuresis with Furosemide•• DialysisDialysis•• MobilizationMobilization
•• BisphosphonatesBisphosphonates•• PlicamycinPlicamycin•• CalcitoninCalcitonin•• Gallium NitrateGallium Nitrate•• PhosphatePhosphate•• MobilizationMobilization •• PhosphatePhosphate•• GlucocorticoidsGlucocorticoids•• Therapy of Therapy of
Underlying EtiologyUnderlying Etiology
2/17/2009
17
Outline of LectureOutline of Lecture
•• HypercalcemiaHypercalcemia• Hypocalcemia•• OsteoporosisOsteoporosis
Clinical Features of HypocalcemiaClinical Features of Hypocalcemia
•• Neuromuscular irritabilityNeuromuscular irritability•• Paresthesias (numbness and tingling)Paresthesias (numbness and tingling)Paresthesias (numbness and tingling)Paresthesias (numbness and tingling)•• Chvostek’s signChvostek’s sign•• Trousseau’s signTrousseau’s sign•• Prolonged QProlonged Q--T intervalT interval•• Carpal, pedal, broncho, or laryngeal spasmCarpal, pedal, broncho, or laryngeal spasm
S iS i•• SeizuresSeizures
2/17/2009
18
Clinical Features of HypocalcemiaClinical Features of Hypocalcemia
Determinants of signs and symptoms
•• Extent of hypocalcemiaExtent of hypocalcemia•• Rapidity of reductionRapidity of reduction•• Duration of hypocalcemiaDuration of hypocalcemia
SS
Management of HypocalcemiaManagement of Hypocalcemia
Indications for Acute Treatment
•• SymptomsSymptoms•• No symptoms but…No symptoms but…
–– Serum calcium Serum calcium (corrected for serum albumin) <7.5 mg/dL<7.5 mg/dL
–– History of seizuresHistory of seizuresHistory of seizuresHistory of seizures–– Previous compression fracturePrevious compression fracture
2/17/2009
19
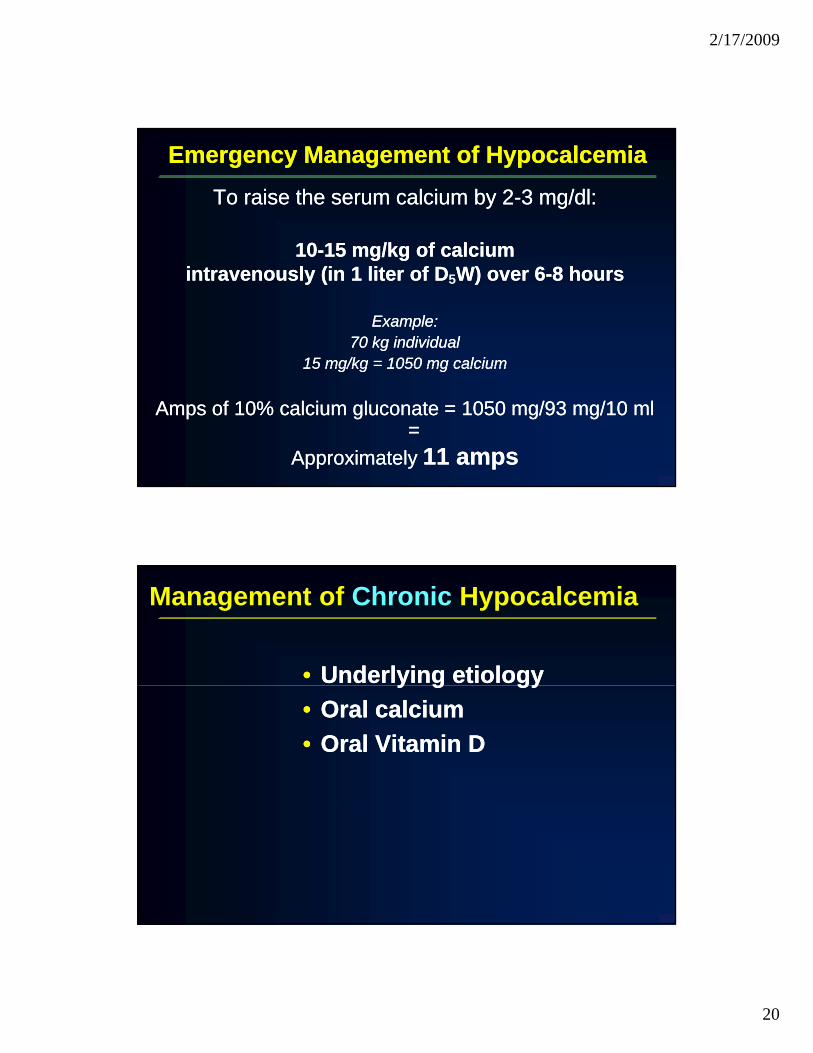
Emergency Management of HypocalcemiaEmergency Management of Hypocalcemia
Intravenous Preparation of Choice
Calcium gluconateCalcium gluconateCalcium chloride (do not use)Calcium chloride (do not use)
Emergency Management of HypocalcemiaEmergency Management of Hypocalcemia
FORFOR IMMEDIATEIMMEDIATE RELIEF OF SYMPTOMS:RELIEF OF SYMPTOMS:FOR FOR IMMEDIATE IMMEDIATE RELIEF OF SYMPTOMS:RELIEF OF SYMPTOMS:
11--2 amps of 10% calcium gluconate (93 mg of 2 amps of 10% calcium gluconate (93 mg of elemental calcium/amp) intravenously over elemental calcium/amp) intravenously over 1010 15 i t15 i t1010--15 minutes15 minutes
2/17/2009
20
Emergency Management of HypocalcemiaEmergency Management of Hypocalcemia
To raise the serum calcium by 2To raise the serum calcium by 2--3 mg/dl:3 mg/dl:
1010 15 mg/kg of calcium15 mg/kg of calcium1010--15 mg/kg of calcium15 mg/kg of calciumintravenously (in 1 liter of Dintravenously (in 1 liter of D5W) over 6W) over 6--8 hours8 hours
Example:Example:70 kg individual70 kg individual
15 mg/kg = 1050 mg calcium15 mg/kg = 1050 mg calcium15 mg/kg 1050 mg calcium15 mg/kg 1050 mg calcium
Amps of 10% calcium gluconate = 1050 mg/93 mg/10 ml Amps of 10% calcium gluconate = 1050 mg/93 mg/10 ml ==
Approximately Approximately 11 amps11 amps
•• Underlying etiologyUnderlying etiology
Management of Chronic Hypocalcemia
y g gyy g gy•• Oral calciumOral calcium•• Oral Vitamin DOral Vitamin D
2/17/2009
21
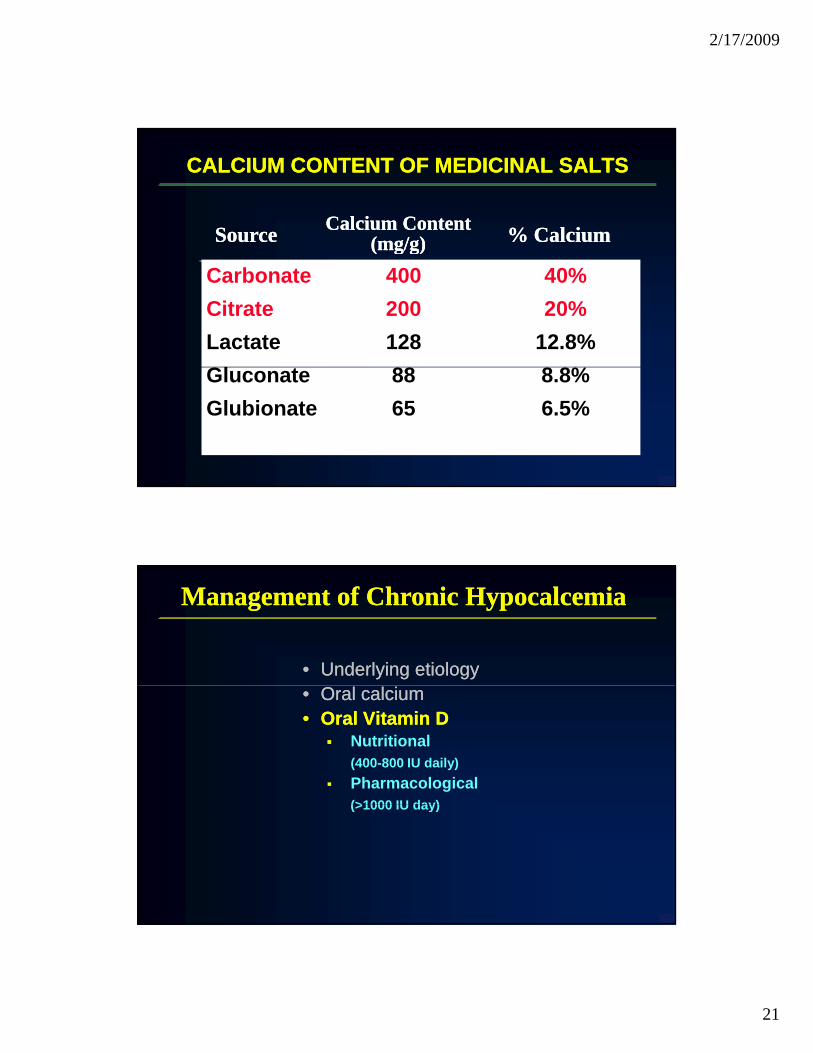
CALCIUM CONTENT OF MEDICINAL SALTSCALCIUM CONTENT OF MEDICINAL SALTS
SourceSource Calcium ContentCalcium Content(mg/g)(mg/g) % Calcium% Calcium
Carbonate 400 40%Citrate 200 20%Lactate 128 12.8%Gl t 88 8 8%
(mg/g)(mg/g)
Gluconate 88 8.8%Glubionate 65 6.5%
•• Underlying etiologyUnderlying etiology
Management of Chronic HypocalcemiaManagement of Chronic Hypocalcemia
•• Oral calciumOral calcium•• Oral Vitamin DOral Vitamin D
Nutritional (400-800 IU daily)Pharmacological (>1000 IU day)(>1000 IU day)

2/17/2009
22
Outline of Lecture
•• HypercalcemiaHypercalcemia•• HypocalcemiaHypocalcemia• Osteoporosis

2/17/2009
23
CALCIUM CONTENT OF MEDICINAL SALTSCALCIUM CONTENT OF MEDICINAL SALTS
Source Calcium Content(mg/g) % Calcium
Carbonate 400 40%Citrate 200 20%
( g g)
How much?H h t ti ?How much at a time?What form?Brand vs generic vs fancy?When?With food or without food?

2/17/2009
24
Nonpharmacological Approaches to the Management of Osteoporosis*
CalciumCalciumVitamin DVitamin DExerciseExerciseLifestyle Lifestyle (Smoking, Alcohol, etc)(Smoking, Alcohol, etc)
Fall PreventionFall Prevention
**Recommended for virtually everyone!Recommended for virtually everyone!

2/17/2009
25
Approved Pharmacologic Therapies in the Approved Pharmacologic Therapies in the United States for OsteoporosisUnited States for Osteoporosis
•• Hormone replacement therapy (HT)Hormone replacement therapy (HT)•• RaloxifeneRaloxifene•• BisphosphonatesBisphosphonates
AlendronateAlendronateRisedronateRisedronateIbandronateIbandronateZ l d tZ l d tZoledronateZoledronate
•• CalcitoninCalcitonin•• Teriparatide [humanPTH[1Teriparatide [humanPTH[1--34)]34)]
ESTROGEN REDUCES THE RISK OF ESTROGEN REDUCES THE RISK OF ALL CLINICAL FRACTURESALL CLINICAL FRACTURES
E+P: N=16,608 women ages 45E+P: N=16,608 women ages 45--7979Mean age: 63.2Mean age: 63.2Placebo or estrogen+progestin Placebo or estrogen+progestin RR 0.76 RR 0.76
95% CI (0 6995% CI (0 69--RR 0.70 RR 0.70
95% CI (0 6395% CI (0 63--CEE arm: N=10,739 ages 50CEE arm: N=10,739 ages 50--7979Mean age: 63.6Mean age: 63.6Placebo or CEE 0.625 mg dailyPlacebo or CEE 0.625 mg daily
Fractures: All clinical fractures Fractures: All clinical fractures (less than 10% were vertebral (less than 10% were vertebral fractures)fractures)
1.91%
1.47%
1.95%
1.39%
1%
2%
3%
ed fr
actu
re ra
te (%
)
95% CI (0.6995% CI (0.690.75)0.75)
95% CI (0.6395% CI (0.630.79)0.79)
Treatment intervals: E+P 5.2 years; Treatment intervals: E+P 5.2 years; CEE 6.8 yearsCEE 6.8 years
E+P: Rossouw JE,E+P: Rossouw JE, et al. JAMA. 2002;288:321-333.CEE: Anderson GL, et al. JAMA. 2004;291:1701-1712.
0%
1%
Ann
ualiz
e
E+P CEE
788/8102 503/5310650/8506 724/5429
CEE= conjugated equine estrogen.

2/17/2009
26
WHI HT Study: Combination ArmWHI HT Study: Combination ArmEffect of HT and Progestin on Hip Fracture Incidence Effect of HT and Progestin on Hip Fracture Incidence
0 70.80.9
ctur
e RH=0.66 (95% CI=0.45-0.98)• Preexisting fractures Elements Not Stated in Paper
00.10.20.30.40.50.60.7
of W
omen
With
Hip
Fra
cO
ver
5.2
Year
s
n=62 n=44
• Baseline BMD status• Calcium or vitamin D intake• Use of bisphosphonates and/or
calcitonin• Age distribution
of fractures
34%
Adapted from: Writing Group for the Women’s Health Initiative. JAMA. 2002;288:321-333.
Placebo(N=8102)
HRT(N=8506)
0% o 6
Risk Benefit
WHI HT StudyWHI HT StudyFindings at Early Interruption of CEE/MPA ArmFindings at Early Interruption of CEE/MPA Arm
Fracture ReductionColon Cancer
29% Increase29% Increase
Stroke
41% Increase41% IncreaseVenous Thrombolic
Events(VTE)
200% Increase200% Increase
Breast Cancer
26% Increase26% Increase
Coronary Artery Disease
Threshold LevelEarly STOP=Clear Harm
Threshold LevelEarly STOP=Clear Benefit
Adapted from: Writing Group for the WHI Investigators. JAMA. 2002;288:321-333.

2/17/2009
27
WHI: Conclusions regarding the skeleton*WHI: Conclusions regarding the skeleton*
•• Estrogen should not be used as a Estrogen should not be used as a primary therapy to prevent bone lossprimary therapy to prevent bone loss
•• Estrogen should not be used as a Estrogen should not be used as a primary approach to the treatment of primary approach to the treatment of osteoporosisosteoporosisosteoporosisosteoporosis
*This is a very controversial issue!
AgonistAgonist
The Concept of an Ideal SERMThe Concept of an Ideal SERM
AntagonistAntagonist
SkeletonSkeleton CardiovascularCardiovascular
Mitlak BH, et al. Drugs 1999;57:653-63.Lufkin EG, et al. Rheum Dis Clin North Am 2001;27:163-85.
BreastBreast UterusUterus

2/17/2009
28
Raloxifene:A Selective Estrogen Receptor Modulator
Basic Side ChainO
O Basic Side Chain
Estrogen Antagonist(uterus, breast)
OH
O
HO S
Ben othiophene moiet
Estrogen Agonist(bone, lipids)
• BMD (bone mineral density) increase• Decrease in total and LDL cholesterol
Benzothiophene moiety
2/17/2009
29
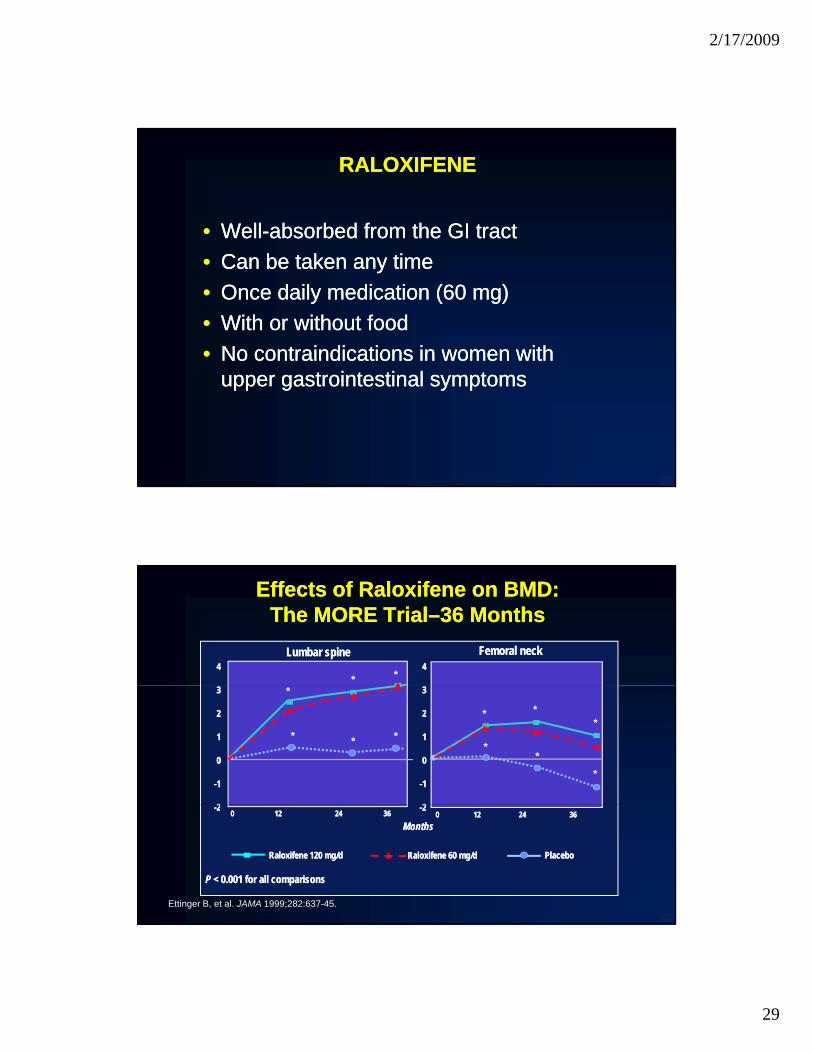
RALOXIFENERALOXIFENE
•• WellWell--absorbed from the GI tractabsorbed from the GI tract•• Can be taken any timeCan be taken any time•• Once daily medication (60 mg) Once daily medication (60 mg) •• With or without foodWith or without food•• No contraindications in women with No contraindications in women with
upper gastrointestinal symptomsupper gastrointestinal symptoms
Effects of RaloxifeneEffects of Raloxifene on BMD:on BMD:The MORE TrialThe MORE Trial––36 Months36 Months
44Femoral neckFemoral neckLumbar spineLumbar spine
44* *
33
22
11
00
--11
22
33
22
11
00
--11
22
*
* * *
* **
**
*
--2200 1212 2424 3636
MonthsMonths00 1212 2424 3636
--22
PlaceboPlacebo
Ettinger B, et al. JAMA 1999;282:637-45.
P P < 0.001 for all comparisons< 0.001 for all comparisons
Raloxifene 120 mg/dRaloxifene 120 mg/d Raloxifene 60 mg/dRaloxifene 60 mg/d

2/17/2009
30
Effects of Raloxifene on New Vertebral Effects of Raloxifene on New Vertebral Fractures: The MORE Trial Fractures: The MORE Trial –– 36 Months36 Months
20
25 Placebo60 mg/d of raloxifene
ract
ure RR, 0.7 (95% CI, 0.6-0.9)
RR, 0.5 (95% CI, 0.4-0.6)
120 mg/d of raloxifene*
5
10
15
20
RR, 0.6 (95% CI, 0.4-0.9)
ents
with
incid
ent v
erte
bral
fr
RR, 0.5 (95% CI, 0.3-0.7)
Ettinger B, et al. JAMA 1999;282:634-45.
*Not FDA-approved dose.
0
5
No pre-existing fractures
% o
f pat
ie
Pre-existing fractures
Raloxifene: Benefits and Risks
Benefits• Improved bone mass
DisadvantagesI d h t• Improved bone mass
• Reduced number ofvertebral fractures
• No breast tenderness• No uterine bleeding or
spotting• Reduced risk of breast
• Increased hot flashes
• Increased leg cramps
• Increased risk of DVT• Reduced risk of breast
cancer* • No increased
cardiovascular risk
DVTand pulmonaryembolism
*New indication, 2007
2/17/2009
31
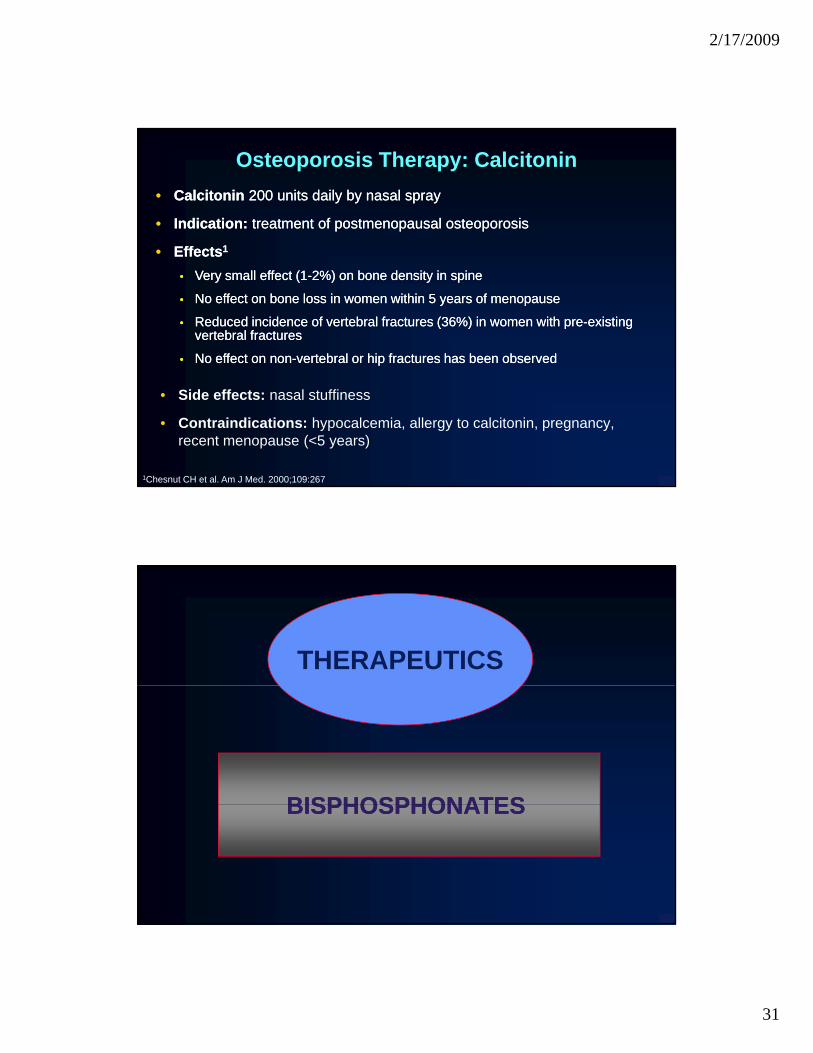
Osteoporosis Therapy: Calcitonin•• Calcitonin Calcitonin 200 units daily by nasal spray200 units daily by nasal spray
•• Indication: Indication: treatment of postmenopausal osteoporosistreatment of postmenopausal osteoporosis
Eff tEff t 11•• EffectsEffects11
•• Very small effect (1Very small effect (1--2%) on bone density in spine2%) on bone density in spine
•• No effect on bone loss in women within 5 years of menopause No effect on bone loss in women within 5 years of menopause
•• Reduced incidence of vertebral fractures (36%) in women with preReduced incidence of vertebral fractures (36%) in women with pre--existing existing vertebral fractures vertebral fractures
•• No effect on nonNo effect on non--vertebral or hip fractures has been observedvertebral or hip fractures has been observed
• Side effects: nasal stuffiness
• Contraindications: hypocalcemia, allergy to calcitonin, pregnancy, recent menopause (<5 years)
1Chesnut CH et al. Am J Med. 2000;109:267
THERAPEUTICS
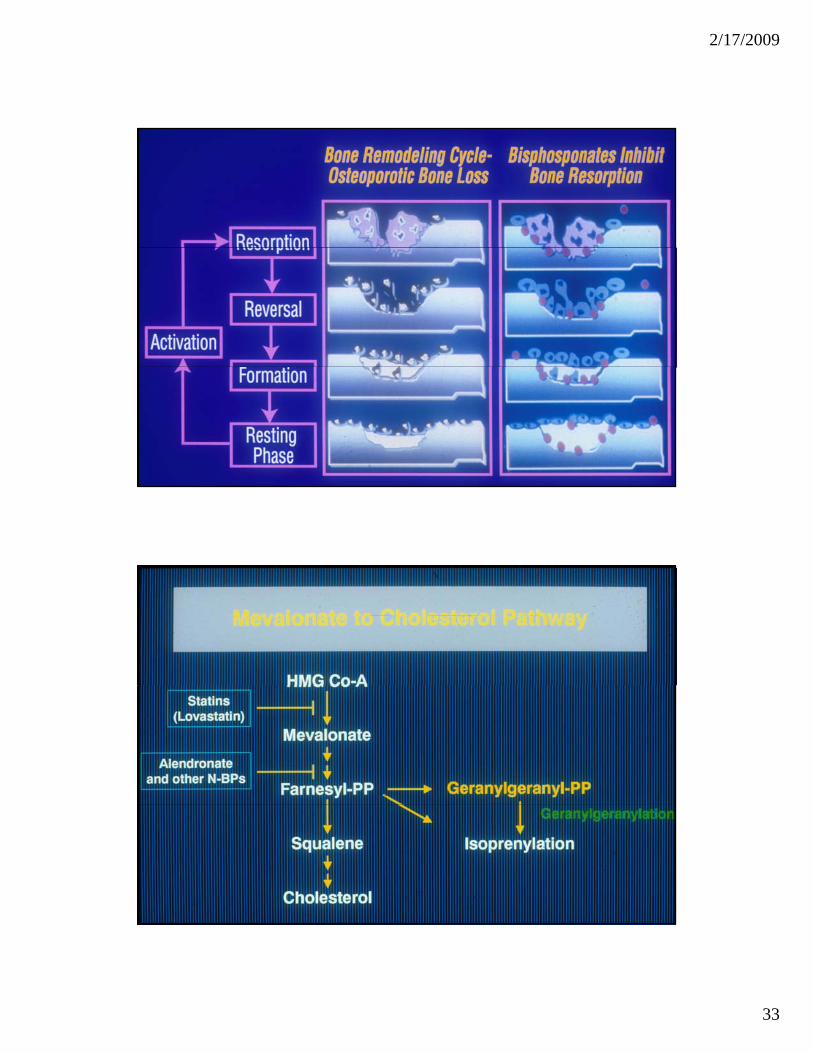
BISPHOSPHONATESBISPHOSPHONATESBISPHOSPHONATES BISPHOSPHONATES

2/17/2009
32
O
BISPHOSPHONATES APPROVED IN THE US FOR USE IN OSTEOPOROSIS
Alendronate
H2N
O
O
=
=P
P
OHOH
OHOHHO
Ibandronate
HO
CH 3N
O
O
=
=
P
P
OHOH
OHOH
O=
POH
O
=
POHOH
Risedronate
HON O
=
P
P
OH
OHOH
Zoledronate
HONN
O
=
P
P
OH
OHOH
Oral bisphosphonatesOral bisphosphonates•• Poorly absorbed (<1.0%)Poorly absorbed (<1.0%)•• Specific requirements for optimal oral absorptionSpecific requirements for optimal oral absorption
Fasting state with plain water onlyFasting state with plain water onlyFasting state with plain water onlyFasting state with plain water onlyMust be uprightMust be uprightNo food or drink for at least 30 minutes No food or drink for at least 30 minutes (for Ibandronate, 60 minutes)
•• Several halfSeveral half--liveslivesRapid uptake in bone and clearance by the Rapid uptake in bone and clearance by the kidneykidneykidneykidneyProlonged skeletal halfProlonged skeletal half--life (years)life (years)
•• GI intolerance has occurred with orally administered GI intolerance has occurred with orally administered aminoamino--substituted bisphosphonates (alendronate, substituted bisphosphonates (alendronate, risedronate, ibandronate)risedronate, ibandronate)
2/17/2009
33

2/17/2009
34
The Vertebral FractureThe Vertebral Fracture
2/17/2009
35
0
10
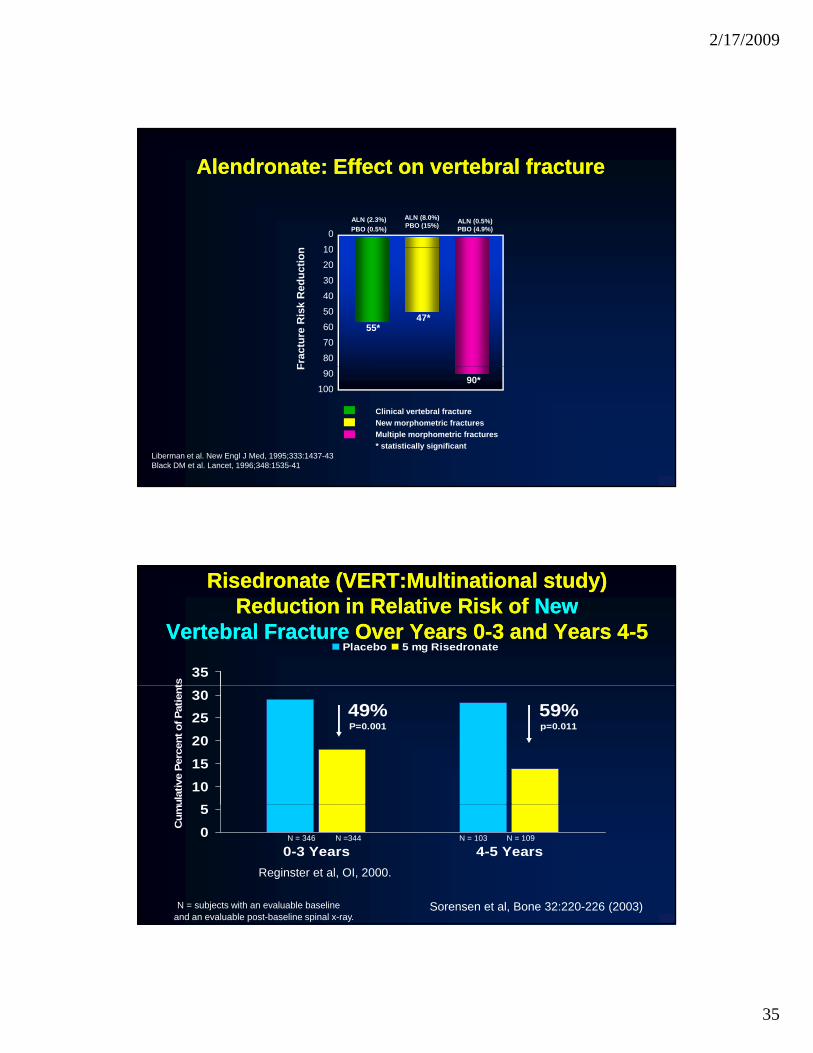
ALN (2.3%)PBO (0.5%)
ALN (8.0%)PBO (15%) ALN (0.5%)
PBO (4.9%)
Alendronate: Effect on vertebral fractureAlendronate: Effect on vertebral fracture
Frac
ture
Ris
k R
educ
tion 10
20
30
4050
6070
80
55*47*
Liberman et al. New Engl J Med, 1995;333:1437-43Black DM et al. Lancet, 1996;348:1535-41
Clinical vertebral fractureNew morphometric fracturesMultiple morphometric fractures* statistically significant
F
90
10090*
35
ts
Placebo 5 mg Risedronate
Risedronate (VERT:Multinational study)Risedronate (VERT:Multinational study)Reduction in Relative Risk of Reduction in Relative Risk of NewNew
Vertebral FractureVertebral Fracture Over Years 0Over Years 0--3 and Years 43 and Years 4--55
51015202530
ulat
ive
Perc
ent o
f Pat
ient
49%P=0.001
59%p=0.011
05
0-3 Years 4-5 Years
Cum
u
N = 346 N =344 N = 103 N = 109
Reginster et al, OI, 2000.
N = subjects with an evaluable baselineand an evaluable post-baseline spinal x-ray.
Sorensen et al, Bone 32:220-226 (2003)
2/17/2009
36
12
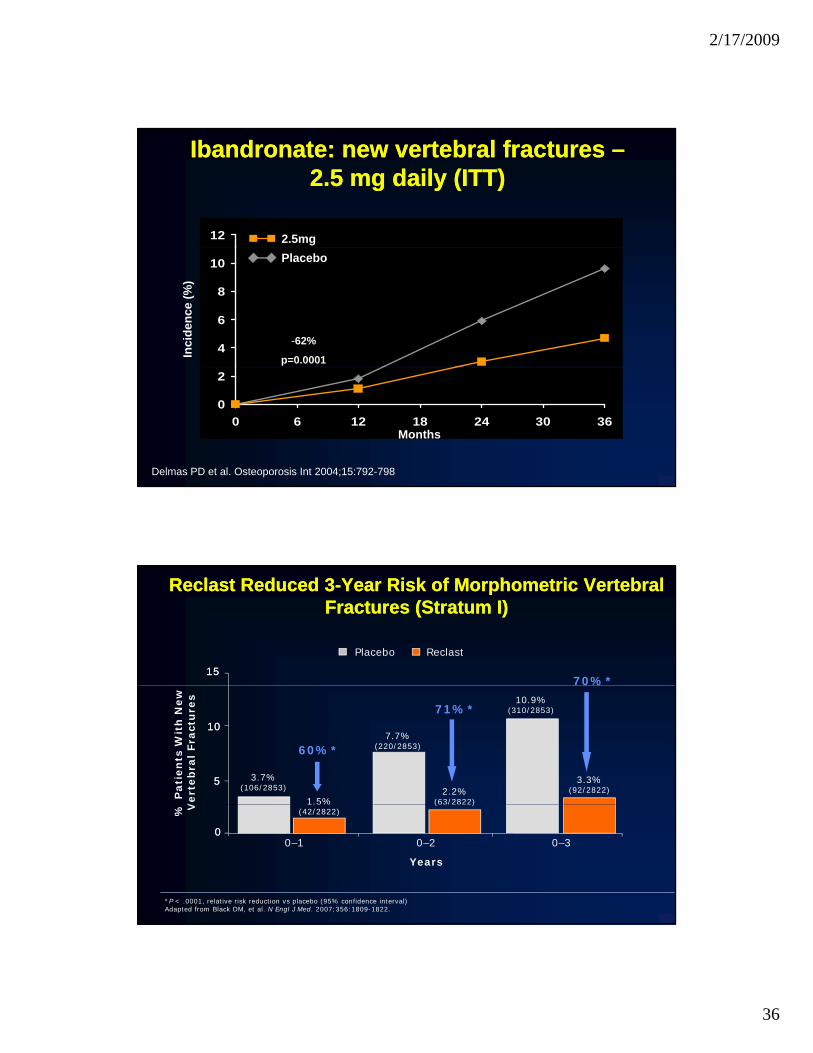
Ibandronate: new vertebral fractures Ibandronate: new vertebral fractures ––2.5 mg daily (ITT)2.5 mg daily (ITT)
2.5mg
4
6
8
10
Inci
denc
e (%
)
Placebo
-62%
p=0.0001
0
2
0 6 12 18 24 30 36Months
Delmas PD et al. Osteoporosis Int 2004;15:792-798
151570%*
Reclast Reduced 3Reclast Reduced 3--Year Risk of Morphometric Vertebral Year Risk of Morphometric Vertebral Fractures (Stratum I)Fractures (Stratum I)
Reclast Placebo
% P
ati
en
ts W
ith
New
V
ert
eb
ral
Fra
ctu
res
60%*
71%*1010
55
1.5%
3.7%(106/2853) 2.2%
(63/2822)
7.7%(220/2853)
3.3%(92/2822)
10.9%(310/2853)
0%
% V
000–1 0–2 0–3
Years
(42/2822)( / )
*P < .0001, relative risk reduction vs placebo (95% confidence interval) Adapted from Black DM, et al. N Engl J Med. 2007;356:1809-1822.

2/17/2009
37
NONNON--VERTBRAL FRACTURESVERTBRAL FRACTURES
20
NONVERTEBRAL AND HIP FRACTURESNONVERTEBRAL AND HIP FRACTURESALENDRONATE FRACTURE INTERVENTION TRIALALENDRONATE FRACTURE INTERVENTION TRIAL
5
10
15ControlAlendronate
RR=0.5 (0.2,1.0)
NS
0Nonvertebral Fractures Hip Fractures
After data from Black DM et al. Lancet 1996;348:1535-1541
33 total hip fracturesNVFX = all except pathological, traumatic, face/skull

2/17/2009
38
20
NONVERTEBRAL AND HIP FRACTURESNONVERTEBRAL AND HIP FRACTURESRISEDRONATE VERTRISEDRONATE VERT--NANA
5
10
15Control
Risedronate
RR=0.6 (0.4,0.9)
NS
0Nonvertebral Fractures Hip Fractures
After data from Harris ST et al. JAMA 1999;282:1344-1352
27 total hip fractures (control + primary treatment group)NVFx = clavicle, humerus, forearm, pelvis, femur, lower leg; no consideration for trauma
20
NONVERTEBRAL AND HIP FRACTURESNONVERTEBRAL AND HIP FRACTURESIBANDRONATE BONE STUDYIBANDRONATE BONE STUDY
5
10
15Control
IBAN 2.5 mg daily
NS
NS
0Nonvertebral Fractures Hip Fractures
After data from Chesnut CH III et al. J Bone Miner Res 2004;19:1241-1249
10 total hip fractures (control + primary treatment group)NVFx = all except hands, feet, face, and skull
2/17/2009
39
20
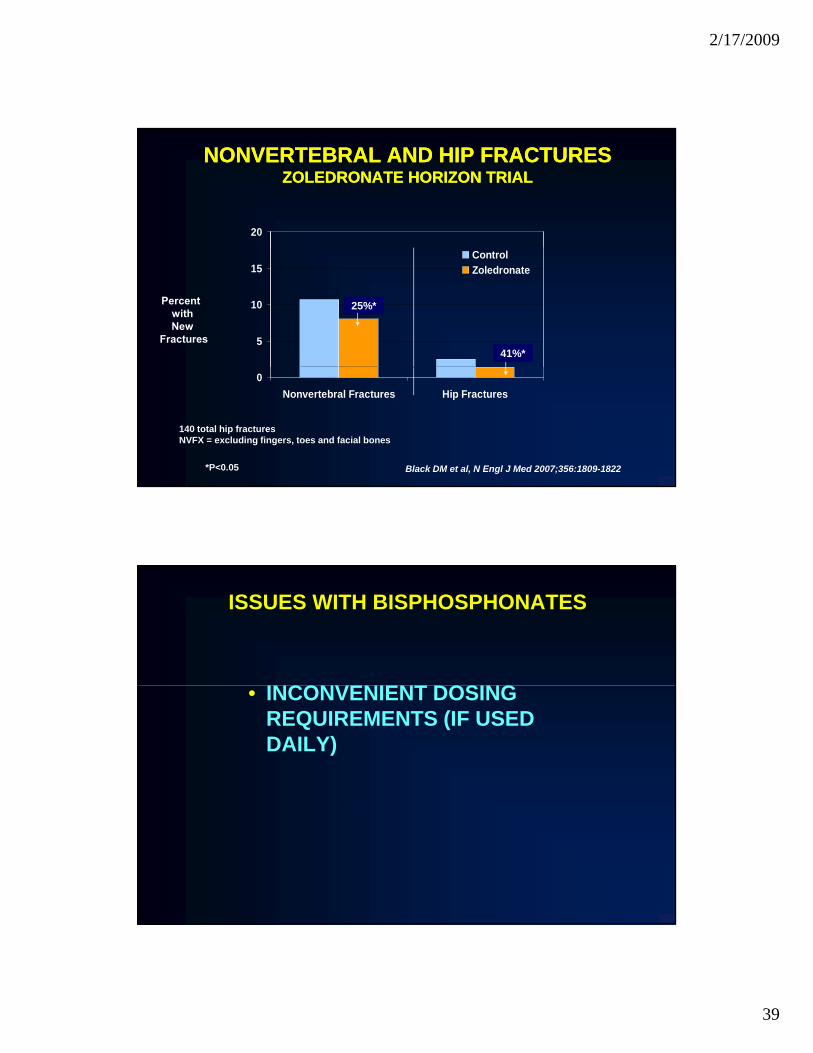
NONVERTEBRAL AND HIP FRACTURESNONVERTEBRAL AND HIP FRACTURESZOLEDRONATE HORIZON TRIALZOLEDRONATE HORIZON TRIAL
5
10
15ControlZoledronate
41%*
25%*
0Nonvertebral Fractures Hip Fractures
140 total hip fracturesNVFX = excluding fingers, toes and facial bones
*P<0.05 Black DM et al, N Engl J Med 2007;356:1809-1822
ISSUES WITH BISPHOSPHONATES
INCONVENIENT DOSING• INCONVENIENT DOSING REQUIREMENTS (IF USED DAILY)

2/17/2009
40
Bisphosphonates: Weekly DosingBisphosphonates: Weekly Dosing
• Effects of weekly vs daily dosing on BMD and turnover 6
Alendronate1 Risedronate2
nene nene 6dosing on BMD and turnover are the same
• Extrapolation of fracture protection from daily studies is reasonable
• Has improved acceptance, but ff t dh t 0
2
4
% c
hang
e fr
om b
asel
in%
cha
nge
from
bas
elin
% c
hang
e fr
om b
asel
in%
cha
nge
from
bas
elin
0
2
4
Spine BMD Spine BMD
effect on adherence not known
Not a direct comparisonNot a direct comparison
0Daily Weekly
%%Daily Weekly
%% 0
11Schnitzer T, et al. Aging Clin Exp ResSchnitzer T, et al. Aging Clin Exp Res. . 2000;12:12000;12:1--121222Brown JP, et al. Calcif Tissue IntBrown JP, et al. Calcif Tissue Int.. 2002;71:1032002;71:103--111111
BisphosphonatesBisphosphonatesOther administration regimensOther administration regimens
• Monthly dosing– Ibandronate– Risedronate
• Intravenous dosingIbandronate (every 3 months)Ibandronate (every 3 months)–– Ibandronate (every 3 months)Ibandronate (every 3 months)
–– Zoledronate (once yearly)Zoledronate (once yearly)
2/17/2009
41
Adverse events with bisphosphonates Adverse events with bisphosphonates for osteoporosisfor osteoporosis
•• Upper GI intoleranceUpper GI intolerance•• Acute Phase ReactionAcute Phase Reaction•• “Oversuppression of bone”“Oversuppression of bone”1
•• Osteonecrosis of the jawOsteonecrosis of the jaw2,3
1Odvina et al. J Clin Endocrinol Metab, 20052Bilezikian JP N Eng J Med, 2006 3Khosla et al, J Bone Mineral Res, 2007
♦ Hormone replacement therapy(HT)
All Antiresorptive Antiresorptive Therapies for OsteoporosisTherapies for Osteoporosis
( )♦ Raloxifene♦ Bisphosphonates
• Alendronate• Risedronate• Ibandronate• Ibandronate• Zoledronate
♦ Calcitonin
Inhibit Bone Resorption

2/17/2009
42
Actions of antiActions of anti--resorptive agentsresorptive agents
Stabilize orStabilize or increase BMD
Maintain trabecular architecture
Increase mineralization density of bone matrix
What the antiresorptivesdon’t do…

2/17/2009
43
Approved Therapies in theApproved Therapies in theUnited States for OsteoporosisUnited States for Osteoporosis
•• Hormone Hormone • Teriparatide therapy (HT)therapy (HT)
•• RaloxifeneRaloxifene
•• BisphosphonatesBisphosphonates–– AlendronateAlendronate–– RisedronateRisedronate
p[human parathyroid hormone (1-34)]
–– IbandronateIbandronate–– ZoledronateZoledronate
•• CalcitoninCalcitonin
HisGluSer
Human Parathyroid HormoneHuman Parathyroid Hormone
1 10Ser Val Ile Gln Leu Met Asn
LeuH2N
T i tidGly20
30
LysHisLeuAsnSerMetGluArgValGluTrpLeu
Arg Lys Lys Leu Gln Asp Val His Asn Phe
Gly Teriparatide
-COOH

2/17/2009
44
PTH as a Treatment for Osteoporosis:PTH as a Treatment for Osteoporosis:A Paradox
H PTH b t ti l th fH PTH b t ti l th f•• How can PTH be a potential therapy for How can PTH be a potential therapy for osteoporosis when the clinical disorder of osteoporosis when the clinical disorder of chronic PTH excess, primary chronic PTH excess, primary hyperparathyroidism,hyperparathyroidism,is associated with bone loss?is associated with bone loss?
PTH and Dose Determine Effect on BonePTH and Dose Determine Effect on Bone
Mode EffectMode Effect
Continuous(High Dose) Catabolic
Daily AnabolicDaily(Low Dose) Anabolic

2/17/2009
45
Teriparatide reduces the incidence of Vertebraland Non-Vertebral Fractures in
Postmenopausal Women with Osteoporosis
Non-vertebral fracturesNew vertebral fracture
6
8
10
12
14
16
18
20
ents
(%) w
ith fr
actu
re
P< 0.01
53%6
8
10
12
14
16
18
20
ient
s (%
) with
fra
ctur
e
P< 0.01
65%
Neer RM, et al. N Engl J Med. 2001;344:1434-41
0
2
4
6
Patie 53%
20 μg PTH0
2
4
6
Pat
20 μg PTH PlaceboPlacebo
What do the bones actually looklike after therapy with PTH?

2/17/2009
46
Improved Trabecular ConnectivityImproved Trabecular ConnectivityAfter hPTH (1After hPTH (1--34) Therapy34) Therapy
AfterCD: 4.6/mm3Before
CD: 2.9/mm3CD: 2.9/mm
Dempster DW, et al. J Bone Miner Res. 2001;16(10):1846-1853.

2/17/2009
47
OSTEOPOROSIS
PREVENTABLEPREVENTABLEAND AND
TREATABLETREATABLE
Related Documents











