ORIGINAL RESEARCH E18 April 2014 • InterventionalOncology360.com Outcomes Following CT-Guided Percutaneous Radiofrequency Ablation of Primary Renal Tumors Nancy Lee, MS 1 ; John H. Rundback, MD 2 ; Kevin Chaim Herman, MD 2 ; John Kerns, MD 2 ; Ravit Barkama, MD 2 From the 1 George Washington University School of Medicine and Health Sciences, Washington, DC, and the 2 Interventional Institute, Holy Name Medical Center, Teaneck, New Jersey. Abstract: Purpose: The purpose of this study was to analyze outcomes in a single-center cohort of patients undergoing CT-guided percutaneous renal radiofrequency ablation (rRFA) to determine if lesion size was a dif- ferentiator of outcomes, and to describe the temporal changes in lesion size following rRFA. Materials and Methods: Forty lesions in 37 patients (27 males, 10 females; mean age 70±13 years) were treated with rRFA from 2006 to 2013. Patient, tumor, and treatment characteristics were analyzed. Statistical analysis included the entire treated cohort with particular attention paid to subgroupings based on (a) whether patients had a renal mass <3 cm or ≥3 cm, and (b) whether the lesion was biopsy-proven renal-cell carcinoma (RCC). To evaluate lesion changes after ablation, a mixed-effects ANOVA model was fit to lesion size values over time. Results: Kaplan-Meier survival curves showed trends toward worse primary recurrence and overall survival in lesions ≥3 cm, but these were not statistically significant (P=.13 and P=.27 respectively). Secondary recurrences were the same in both groups. The rate of change over time in lesion size following rRFA did not differ significantly either by initial lesion size (P=.65), or between biopsy-proven and non-biopsy-proven RCC (P=.46). Conclusion: rRFA is safe and effective in treating kidney tumors. Overall success of tumor ablation was unrelated to initial size. Serial changes in tumor size after ablation are similar regardless of original size and whether the lesion had been proven RCC by biopsy. Key words: carcinoma, renal cell carcinoma, radiofrequency ablation. R enal cell carcinoma (RCC) constitutes the majority of kidney malignancies. 1 The number of RCC cases is increasing with approximately 65,000 new cases diagnosed each year in the United States. 1,2 Almost twice as many men as women are diagnosed with RCC, and the age at di- agnosis peaks between ages 50 and 80 years. 2,3 Ciga- rette smoking and obesity have consistently been es- tablished as risk factors. 1 Guidelines indicate active surveillance, surgical in- tervention, and minimally invasive therapy as manage- ment methods for RCC. 4 Renal radiofrequency abla- tion (rRFA) is a favorable alternative in patients who are poor surgical candidates because it spares kidney tissue and retains renal function. Renal radiofrequency ablation has no negative effects on glomerular filtra- tion rate in the short or intermediate term, 5 and it also poses less risk for developing chronic kidney disease (CKD) when compared to radical nephrectomy. 6,7 Many studies have shown high clinical success rates Rundback_v.indd 18 4/16/14 4:25 PM Copyright HMP Communications

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ORIGINAL RESEARCH
E18April 2014 • InterventionalOncology360.com
Outcomes Following CT-Guided Percutaneous Radiofrequency Ablation of Primary Renal TumorsNancy Lee, MS1; John H. Rundback, MD2; Kevin Chaim Herman, MD2; John Kerns, MD2; Ravit Barkama, MD2
From the 1George Washington University School of Medicine and Health Sciences, Washington, DC,
and the 2Interventional Institute, Holy Name Medical Center, Teaneck, New Jersey.
Abstract: Purpose: The purpose of this study was to analyze outcomes in a single-center cohort of patients undergoing CT-guided percutaneous renal radiofrequency ablation (rRFA) to determine if lesion size was a dif-ferentiator of outcomes, and to describe the temporal changes in lesion size following rRFA. Materials and Methods: Forty lesions in 37 patients (27 males, 10 females; mean age 70±13 years) were treated with rRFA from 2006 to 2013. Patient, tumor, and treatment characteristics were analyzed. Statistical analysis included the entire treated cohort with particular attention paid to subgroupings based on (a) whether patients had a renal mass <3 cm or ≥3 cm, and (b) whether the lesion was biopsy-proven renal-cell carcinoma (RCC). To evaluate lesion changes after ablation, a mixed-effects ANOVA model was fit to lesion size values over time. Results: Kaplan-Meier survival curves showed trends toward worse primary recurrence and overall survival in lesions ≥3 cm, but these were not statistically significant (P=.13 and P=.27 respectively). Secondary recurrences were the same in both groups. The rate of change over time in lesion size following rRFA did not differ significantly either by initial lesion size (P=.65), or between biopsy-proven and non-biopsy-proven RCC (P=.46). Conclusion: rRFA is safe and effective in treating kidney tumors. Overall success of tumor ablation was unrelated to initial size. Serial changes in tumor size after ablation are similar regardless of original size and whether the lesion had been proven RCC by biopsy.
Key words: carcinoma, renal cell carcinoma, radiofrequency ablation.
Renal cell carcinoma (RCC) constitutes
the majority of kidney malignancies.1 The
number of RCC cases is increasing with
approximately 65,000 new cases diagnosed each year
in the United States.1,2 Almost twice as many men as
women are diagnosed with RCC, and the age at di-
agnosis peaks between ages 50 and 80 years.2,3 Ciga-
rette smoking and obesity have consistently been es-
tablished as risk factors.1
Guidelines indicate active surveillance, surgical in-
tervention, and minimally invasive therapy as manage-
ment methods for RCC.4 Renal radiofrequency abla-
tion (rRFA) is a favorable alternative in patients who
are poor surgical candidates because it spares kidney
tissue and retains renal function. Renal radiofrequency
ablation has no negative effects on glomerular filtra-
tion rate in the short or intermediate term,5 and it also
poses less risk for developing chronic kidney disease
(CKD) when compared to radical nephrectomy.6,7
Many studies have shown high clinical success rates
Rundback_v.indd 18 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
April 2014 • InterventionalOncology360.com E19
for rRFA, especially in cases where the lesions are
exophytic and <3 cm8-11 or <4 cm.12-15 The purpose of
this study was to analyze outcomes in a single-center
cohort of patients undergoing CT-guided rRFA, to
determine if lesion size was noted to be a differentia-
tor of outcomes, and to describe temporal changes in
lesion size following rRFA in patients with smaller vs
larger tumors.
MATERIALS AND METHODSPatient and Tumor Characteristics
IRB approval was obtained for this study. A retro-
spective review was performed of our single institu-
tional experience performing CT-guided percuta-
neous RFA. From June 2006 to June 2013, 40 renal
masses in 37 patients (27 males, 10 females; mean age,
70±13 years; range, 40-89 years) were ablated. One
patient had bilateral tumors; another patient had 3 tu-
mors (1 on the right kidney, 2 on the left kidney).
Four patients had previous partial nephrectomy. Pa-
tient characteristics are summarized in Table 1.
Tumor size ranged from 1.2 cm to 6.3 cm (mean,
2.9±1.1 cm). Nineteen lesions (7 clear cell, 6 papillary,
2 chromophobe, 2 mixed, 3 unspecified) were con-
firmed to be RCC by image-guided biopsy. Similar
to our experience, routine biopsy prior to rRFA is of-
ten not performed.6,10,12-14 Two lesions were parapelvic
(central), and 38 lesions extended to the renal cortex
(exophytic). Additional tumor characteristics are listed
in Table 2.
Percutaneous rRFA Procedure
Prior to the procedure, informed consent was ob-
tained from all patients. With patients under general
endotracheal or laryngeal mask anesthesia and lying
prone on the CT table, scanning was performed to de-
termine the exact location of the lesions. The method
of anesthesia was at the discretion of the treating an-
esthesiologist. Appropriate skin sites for ablation were
prepped and draped in standard sterile fashion and lo-
cally anesthetized with 1% lidocaine. Under direct CT
guidance, electrodes (range, 2.5 cm to 5 cm active tip)
were inserted into the lesions (Figure 1). The elec-
trodes were multitined in 32 cases (LeVeen; Boston
Scientific) and Cool-Tip in 8 cases (Covidien). Ad-
justments were made to confirm precise positioning
of the needle within the mass. Aside from variations in
technique of each performing radiologist, manufac-
turer instructions were followed for power and abla-
tion time (mean, 21±10 minutes).
With LeVeen probes, ablations were performed un-
til roll-off was achieved using a 200-watt generator;
a second ablation was performed starting at 70% of
the initial maximal ablation energy according to treat-
ment guidelines until roll-off occurred. Tumors ≥3 cm
were treated with overlapping lesions, often deep and
centrally within the mass. After retracting and remov-
ing the needles, CT scanning was performed to evalu-
ate for any procedural complications. Streaking in the
perirenal fat and the presence of gas bubbles in the
ablated bed provided indication of ablation efficacy
on noncontrast study. Patients were extubated prior
to transfer to the recovery room. Treatment characters
are listed in Table 3.
Patient Follow-Up
Patients were scheduled for a pre- and post-con-
trast CT scans at 1, 3, and 6 months after the proce-
Rundback_v.indd 19 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E20April 2014 • InterventionalOncology360.com
dure followed by planned annual imaging for 5 years.
Variations existed depending upon patient availabil-
ity, scheduling conflict, and patient’s ability to receive
iodinated contrast. The mean duration of follow-up
for all patients was 19.3±17.5 months (median, 14.1
months). Twenty patients were followed up with dual-
phase CT,5 with noncontrast CT alone,8 with MRI,
and 1 with PET CT. Two patients were lost to follow-
up, while 1 patient had not yet reached the 1-month
follow-up point.
Analysis & Statistics
The analysis included the entire treated cohort, with
particular attention paid to subgroupings based on (a)
whether patients had a renal mass <3 cm (Group 1)
or ≥3 cm (Group 2) and (b) whether or not the lesion
was biopsy-proven RCC. Student t test, Fisher exact
test, and chi-square test were performed via MedCalc
to compare patient, lesion, and treatment character-
istics between Groups 1 and 2. Kaplan-Meier (KM)
survival curves were also created via MedCalc to ana-
lyze primary recurrence and overall survival.
To evaluate lesion changes over time after rRFA, a
mixed-effects ANOVA model was fit to lesion size val-
ues over time. Fixed effects included a separate inter-
cept for each subgroup and a separate slope over time
for each subgroup. Random effects included the ran-
dom effect for patient nested within subgroup and a
random slope over time for each patient nested within
subgroup. An intercept for the overall population was
estimated as the equally weighted average of the inter-
cept over the subgroups, and similarly for slope over
time. The test of equality of slopes between subgroups
was conducted as a t test within this ANOVA model.
The ANOVA model was fitted to lesion sizes as
reported and also to log-transformed lesion sizes. As
neither model provided a clearly superior fit to the
data, results are reported from the model without
log transformation.
RESULTSOnly one patient had residual enhancing tumor after
the initial rRFA at 1-month follow-up; all other le-
sions showed no enhancement on the first post-treat-
ment scan. In this case, a repeat ablation was performed
approximately 3 months after the initial procedure.
Three lesions demonstrated recurrence (range, 9.7-
28.6 months post-ablation), 2 were treated by repeat
ablations, and 1 was treated by partial nephrectomy.
The initial sizes of these lesions were 6.3 cm, 3.5 cm,
and 3.3 cm (mean, 4.4 cm). As of last follow-up, there
was no secondary recurrence after reintervention.
Patients who had lesions ≥3 cm were significantly
older (mean age, 76±10 vs 65±13, P<.005). There
were no significant differences in glomerular filtra-
tion rate (P=.74), serum creatinine (P=.44), number
of prior interventions (P=.61), gender (P=.15), eth-
nicity (P=.49), or a history of diabetes, hypertension,
and other diseases (P=.97) between the two groups.
There was also no significant difference in lesion lo-
cation (P=.49), kidney side affected (P=.34), and
type of probe used during ablation (P=.58). Lesions
≥3 cm were treated with larger probes (chi-square
test, P<.005) and ablated for longer periods of time
(mean time, 25+10 vs 16+6 minutes, P<.005) than
lesions <3 cm. Although KM survival curves (Figure
1) showed trends toward worse primary recurrence
Rundback_v.indd 20 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E21April 2014 • InterventionalOncology360.com
(P=.13, Figure 2A) and overall survival (P=.27, Figure
2B) in larger lesions, these trends were not statistically
significant.
Serial changes in lesion size after ablation were mod-
eled as a function of time. The rate of change over time
in lesion size following rRFA did not differ significant-
ly either by initial lesion size (<3 cm vs ≥3 cm, P=.65;
Figure 3A), or between biopsy-proven and non-biop-
sy-proven RCC (P=0.46; Figure 3B). The regression
line for the <3 cm group was lesion size (cm)=2.2139
cm–0.02208 cm×(number of months). For the ≥3 cm
group, the regression line was lesion size (cm)=3.6034
cm–0.01683 cm×(number of months). These models
thus estimate a reduction in treated lesion size (maxi-
mal diameter) over the course of 3 months by 0.066
cm in the <3 cm group, and by 0.050 cm in the ≥3
cm group. Over 12 months, estimated reductions in
treated lesion size are 0.265 cm in the <3 cm group
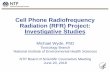
Figure1. Examples of successful and recurrent masses after rRFA. Successful RFA of a small renal tumor is shown in Figures 1A through 1C. Post contrast renal MRI shows a 2.5 cm solid interpolar left renal mass (A, arrow). RFA was performed with a 3 cm LeVeen electrode positioned centrally within the lesion (B, arrowhead). A follow-up CT performed 8 months later shows successful ablation with no residual tumor enhancement (C, asterisk). The le-sion is now smaller, measuring 2.0 cm in greatest dimension. Recurrence after RFA of a large renal tumor is shown in Figures 1D through 1G. A CT scan shows a 3.3 cm exophytic right renal mass (D, arrow). Ablation was performed with a 3.5 cm LeVeen electrode positioned deep (E, asterisk) and centrally (F, asterisk) within the mass. The patient initially did well, but a follow-up CT scan performed 29 months after the procedure (G) shows focal recurrence (ar-rowhead). The patient subsequently underwent partial nephrectomy.
Rundback_v.indd 21 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E22April 2014 • InterventionalOncology360.com
Figure 3. Rate of change in lesion size over time post renal radiofrequency ablation treatment. There was no significant difference in serial change in lesion size re-gardless of initial lesion size or biopsy status of lesion.
Figure 2. Kaplan-Meier survival curve of primary recurrence and overall survival. There was no significant difference in primary recurrence or overall survival between patients with lesions ≥3 cm and those with lesions <3 cm.
and 0.202 cm in the ≥3 cm group.
The pooled intercept and slope for the entire
population based on equal weighting over the 2
groups yielded the following regression line: lesion
size (cm)=2.9087 cm–0.01946 cm×(number of
months). This model thus estimates a reduction of
0.058 cm in treated lesion size over the course of 3
months and 0.233 cm over 12 months.
The regression line for the lesions that were not
biopsy-proven RCC was lesion size (cm)=3.236
cm–0.01547 cm×(number of months). For biop-
sy-proven RCC, the regression line was lesion size
(cm)=2.6276 cm–0.02376 cm×(number of months).
These models thus estimate a reduction in treated
lesion size (maximal diameter) over the course of
3 months by 0.046 cm in the non-biopsy-proven
group, and by 0.071 cm in the biopsy-proven group.
Over 12 months, estimated reductions in treated le-
sion size are 0.186 cm in the non-biopsy-proven
group and 0.285 cm in the biopsy-proven group.
0
1
2
3
4
5
6
7
8
9
0 10 20 30 40 50 60 70
Lesion
Size (cm)
Time (months)
Linear Regression -‐ Serial Change in Lesion Size
0
1
2
3
4
5
6
7
8
9
0 10 20 30 40 50 60 70
Lesion
Size (cm)
Time (months)
Linear Regression -‐ Serial Change in Lesion Size
A
B
Rundback_v.indd 22 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E23April 2014 • InterventionalOncology360.com
TABLE 1. PATIENT CHARACTERISTICS
All <3 cm ≥3 cm P value
n 37 20 19
Glomerular filtration rate*
≥60 21 (57) 12 (60) 9 (47) P=.7446
<60 17 (46) 8 (40) 9 (47) Fisher exact test
Serum creatinine**
≥1.5 8 (22) 3 (15) 5 (26) P=.4381
<1.5 30 (81) 17 (85) 13 (68) Fisher exact test
Prior interventions‡
Yes 4 (11) 3 (15) 1 (5) P=.6050
No 33 (89) 17 (85) 18 (95) Fisher exact test
Gender
Male 27 (73) 12 (60) 16 (84) P=.1552
Female 10 (27) 8 (40) 3 (16) Fisher exact test
Ethnicity
White 22 (59) 12 (60) 11 (58) P=.4900
Black 2 (5) 0 (0) 2 (11) Chi-squared test
Asian 4 (11) 2 (10) 2 (11)
Hispanic 9 (24) 6 (30) 4 (21)
Mean age (with SD) 70±13 65±13 76±10 P=.0039Student t-test
Diabetes 12 (32) 5 (25) 7
(37) P=.9732
Hypertension 25 (68) 12 (60) 15 (79) Chi-square test
Other history 17 (46) 7 (35) 10 (53)
*Missing glomerular filtration rate data for 1 patient in ≥3 cm group; 1 patient with 2 lesions <3 cm only ac-counted for one in <3 cm group.**Missing serum creatinine info for 1 patient in ≥3 cm group; 1 patient with 2 lesions <3 cm only accounted for one in <3 cm group.‡Type of intervention: partial nephrectomy of contralateral kidney.
Rundback_v.indd 23 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E24April 2014 • InterventionalOncology360.com
TABLE 2. LESION CHARACTERISTICS
All <3 cm ≥3 cm P value
n 40 21 19
Mean size (cm, with SD) 2.9±1.1 2.1±0.4 3.8±1.0 P<.0001
Image/biopsy-proven renal cell carcinoma #(%)
19 (48) 9 (43) 10 (53)
Clear cell 7 (37) 4 (44) 3 (30)
Papillary 6 (32) 3 (33) 3 (30)
Chromophobe 2 (11) 1 (11) 1 (10)
Mixed 2 (11) 0 (0) 1 (10)
Not specified 3 (16) 1 (11) 2 (20)
Location
Cortical or exophytic 38 (95) 19 (90) 19 (100) P=.4885
Parapelvic 2 (5) 2 (10) 0 (0) Fisher exact test
Side
Right 23 (58) 14 (67) 9 (47) P=.3375
Left 17 (43) 7 (33) 10 (53) Fisher exact test
TABLE 3. TREATMENT CHARACTERISTICS
All <3 cm ≥3 cm P value
Probe size (cm)
2.5 1 (3) 1 (5) 0 (0) P=.0026
3 17 (43) 14 (67) 3 (16) Chi-square test
3.5 14 (35) 6 (29) 8 (42)
4 7 (18) 0 (0) 7 (37)
5 1 (3) 0 (0) 1 (5)
Type of probe
LeVeen (Boston Scientific) 32 (80) 18 (86) 14 (74) P=.4420
Cool-Tip (Coviden) 8 (20) 3 (14) 5 (26) Fisher exact test
Mean # lesions treated (with SD) 1±0 1±0 1±0
Mean time of ablation (min) 21±10 16±6 25±10 P=.0020Student t-test
Rundback_v.indd 24 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E25April 2014 • InterventionalOncology360.com
TABLE 4: PUBLISHED RESULTS OF STUDIES COMPARING CRYOABLATION TO RADIOFREQUENCY ABLATION OF THE KIDNEY.
# Cases (# Patients)
Recurrence # (%)
Complication Success Conclusion
Atwell et al 2013
Cryoablation (CA): 189 (163)Radiofrequency ablation (RFA): 256 (222)
CA: 4 (2.1%) mean 0.9 years post treatmentRFA: 7 (2.7%) mean 2.8 years post treatment
CA: 4.5%RFA: 4.3%
CA: 97.3%, 90.6%, 90.6%RFA: 100%, 98.1%, 98.1%(1-, 3-, and 5-year local recurrence-free survival respec-tively)
CA and RFA can effectively treat renal masses <3 cm.
El Dib et al 2012CA: 500 (457)RFA: 507 (426)
N/ACA: 19.9%RFA: 19.0%
CA: 89%RFA: 90%(clinical efficacy)
CA and RFA can effectively treat renal tumors <4 cm.
Pirasteh et al 2011
CA: 70RFA: 41
CA: 7%RFA: 11%Both 10 months post treatment
CA: 1.4%RFA: 2.4%
N/ACA and RFA result in similar outcomes.
Rundback_v.indd 25 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E26April 2014 • InterventionalOncology360.com
TABLE 5. PUBLISHED RESULTS OF STUDIES COMPARING THERMAL ABLATIVE PROCEDURES (CRYOABLATION AND RADIOFREQUENCY ABLATION) TO SURGICAL PROCEDURES (PARTIAL NEPHRECTOMY AND RADICAL NEPHRECTOMY).
# Cases (# Patients)
Recurrence # (%) Complication Success Conclusion
Olweny et al 2012PN*: 37RFA: 37
PN: (5.4%)RFA: (8.3%) N/A
PN: 100%, 100%, 89.2%, 94.6%, 91.8%RFA: 97.2%, 97.2%, 89.2%, 91.7%, 97.2%(5-year OS, CSS, DFS, local RFS, MFS respectively)
RFA is an effective mini-mally invasive procedure in treating renal cell carcinoma.
Takaki et al 2010
PN: 10RN: 54RFA: 51
PN: 1 (10.0%)RN: 2 (3.7%)RFA: 1 (2.0%)[Distant Recur-rence]
PN: 10.0%RN: 7.4%RFA: 5.0%
PN: 100%RN: 100%RFA: 82.4% (Prima-ry), 100% (Second-ary)
Although RN and PN had higher OS than RFA, RCC-related survival and DFS were comparable between the 3 treatment methods.
Turna et al 2009
PN: 36 (36)CA: 36 (36)RFA: 29 (29)
PN: 2 (5.6%)‡CA: 6 (16.7%)RFA: 11 (37.9%)
PN: 26CA: 7RFA: 2
PN: 100%, 91%, 100%CA: 88.5%, 88.5%, 69.6%RFA: 83.9%, 83.9%, 33.2%(CSS, OS, DFS respectively)
Although PN provided the best oncological outcome, it had a higher complication rate and worse renal function results.
Lucas et al 2008
PN: 85RN: 71RFA: 86
PN: 2RN: 0RFA: 6
N/A N/ARFA provides similar on-cological outcomes while preserving renal function.
*CA: cryoablation, CSS: cancer-specific survival, DFS: disease-free survival, MFS: metastasis-free survival, OS: overall survival, PN: partial nephrectomy; RFA: radiofrequency ablation, RFS: recurrence-free survival, RN: radical nephrectomy.‡Positive surgical margins reported for partial nephrectomy.
Rundback_v.indd 26 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E27April 2014 • InterventionalOncology360.com
TABLE 6. PUBLISHED RESULTS OF RENAL RADIOFREQUENCY ABLATION STUDIES (2003-2013).
# Cases (Patients)
Follow-Up (Months)
Tumor Diam-eter (cm) Complication Technical
Success Conclusion
Atwell et al 2013 256 (222) — Mean: 1.9±0.5
Median: 1.8 4.3% 99.6%
5-year local RFS* rate for RFA: 93.2% (overall); based on location, 62.3% (central), 97.7% (exophytic), 92.8% (intraparenchymal).
Balageas et al 2013 71 (62) Mean: 38.8
Range: 18-78Median: 2.3(0.8-4.6) 5.9% (P) 95.2%
(S) 98.4%
5-year DFS: 61.9%OS: 90.1% (<3 cm) and 44.0% (>3 cm), P=.03Central location associated with increased risk of complications.
Nitta et al 2012 24 (22) Mean: 18
Range: 1-61Mean: 2.4 (1.0-4.5) 14% — OS: 79%, RFS: 85%
Zagoria et al 2011 48 (41) Median: 56 Median: 2.6 — —
Local RFS: 88%, DFS: 83%, 5-year OS: 66%Authors recommend RFA for RCCs less than 4 cm.
El Dib et al 2011 507 (426)
Mean: 18.1Range: 9.0-30.7
Mean: 2.7(2.0-4.3) 19% 90%
Numbers include laparoscopic renal RFA.CA and RFA are similar in terms of complication rates and technical success.
Ferakis et al 2010 39 (31) Mean: 61.2
Range: 36-84Mean: 3.1 (1.3-7.5) — (P) 90%
(S) 97%Larger tumors have a higher likeli-hood for recurrence.
Takaki et al 2010 51 (51) Mean:
34.0±23.2 Mean: 2.4±0.7 5% (P) 82.4%(S) 100%
5-year OS: 75%, 5-year DFS: 98%Complications were all minor; no major complications reported.
Tracy et al 2010 243 (208) Mean: 27±23
Range: 1.5-90Mean: 2.4±0.8 (1.0-5.4) — 97% 5-year RFS: 93%, 5-year OS: 85%
Hiraoka et al 2009 77 (40) Median: 16
Range: 1-63Median: 2.4 (1.1-5.3) 3.9% 85%
Complications were all minor; no major complications reported.
Levinson et al 2008 34 (31)
Mean: 61.6Median: 62.4Range: 41-80
Mean: 2.1 (1.0-4.0) 20.6% 91.2%
Most reported complications were minor.DSS: 100%, MFS: 100%, RFS: 89.2%OS: 62.7% (all at 80 months)
Zagoria et al 2007 125 (104) Mean: 13.8 Mean: 2.7 (0.6-
8.8) 8% (P) 87.2%(S) 93%
Tumor-free survival: 100% (<3.6 cm), 47% (>3.7)Each cm 1 increase in diameter over 3.6 cm decreases tumor-free survival by a factor of 2.19.
Gervais et al 2003 42 (34) Mean: 13.2
Median: 9.9Mean: 3.2 (1.1-8.9) 7.4% 86%
Success based on size; small: 100%, large: 73%Centrally located renal masses up to a size of 5 cm can be successfully treated by RFA.
*P: primary, S: secondary, CA: cryoablation, CSS: cancer-specific survival, DFS: disease-free survival, MFS: metastasis-free survival, OS: overall survival, RFA: radiofrequency ablation, RFS: recurrence-free survival.
Rundback_v.indd 27 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E28April 2014 • InterventionalOncology360.com
Results for the pooled intercept and slope for the en-
tire population based on equally weighting over these
2 groups were very similar to the intercept and slope
pooled over the <3 cm group and the ≥3 cm group.
Two out of 3 recurrent lesions were biopsy-proven
papillary RCC. Whether or not a lesion was biopsy-
proven RCC was not a significant factor in determin-
ing primary recurrence (Fisher exact test, P=.33).
Complications
Eight out of 37 total patients experienced compli-
cations after rRFA. The severity of the complications
was determined using the Society of Interventional
Radiology (SIR) Clinical Practice Guidelines.16 In
our study, minor complications included hemorrhage
that did not require a blood transfusion (1), mild
perinephric hematoma (2), flank pain (3), postproce-
dure urinary tract infection (1), hydronephrosis (2),
gastroenteritis (1), and diarrhea (1). Major complica-
tions included thermal injury to an intercostal nerve
(1), chronic hematuria (1), renal insufficiency (1), and
colon injury (1). The patient with colon injury had a
posteriorly positioned splenic flexure that sustained
thermal injury during rRFA despite CT evidence of
a sufficient fat plane between the RFA probes and
the colon; this patient underwent colonic resection.
There were no other major unplanned procedures
following rRFA.
DISCUSSIONThermal ablation techniques including RFA and
cryoablation (CA) have demonstrated efficacy in
treating renal tumors. A recent review of published se-
ries studied 385 patients with 445 renal masses—all
measuring ≤3.0 cm—treated by either RFA (n=256
tumors in 222 patients) or CA (n=189 tumors in 163
patients).17 At a mean follow-up of 2.8 years, 7 cas-
es of recurrence and a 4.3% complication rate were
found for RFA. Following cryoablation, 4 cases of re-
currence (mean, 0.9 years after treatment) and 4.5%
complication rate were observed. There were no sig-
nificant differences between RFA and CA for techni-
cal success, complication rates, and recurrence rates.
The authors, however, recommended cryoablation for
large lesions due to the ability of cryophobes to create
large ice balls of up to 8 cm. They noted that cryo-
ablation may be preferential for centrally located le-
sions due to published results that described failures,
limitations, and incomplete ablations associated with
central lesions treated by RFA.18-20 The size of cryo-
ablated lesions may also decrease to a greater degree
and at a faster rate than those treated by RFA.21 In
another series comparing CA (n=600 cases) to RFA
(n=775 cases), RFA-treated lesions had significantly
higher rates of local tumor progression and a greater
tendency toward metastatic progression.22 Neverthe-
less, most studies indicate similar clinical outcomes for
RFA and CA (Table 4).17,21,23-24
A comparison of RFA and partial nephrectomy has
resulted in mixed findings (Table 5). In one study of
renal tumors in solitary kidneys, RFA had lower mor-
bidity and complication rates than laparoscopic partial
nephrectomy.25 Another study found no significant
difference between the two methods for 5-year dis-
ease-free survival probability, local recurrence-free sur-
vival probability, and metastasis-free survival probabil-
ity.26 Although patients with independent risk factors
Rundback_v.indd 28 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E29April 2014 • InterventionalOncology360.com
associated with increased recurrence were excluded
in this study, others argue that the outcomes of RFA
and partial nephrectomy cannot be directly compared
because of selection bias.6,27,28 For example, current
partial nephrectomy patients tend to be younger with
fewer comorbidities, contributing to increased overall
survival rates.6,28
Our report compares favorably to prior studies that
have demonstrated high technical success rates and
low complication rates for rRFA (Table 6). Similar to
prior results, we found a higher rate of primary recur-
rence for lesions ≥3 cm in maximal diameter. In fact,
there was no recurrence for smaller tumors. However,
the absolute rate of recurrence was still very low for
tumors ≥3 cm (3 out of 19 treated lesions [16%]). After
recurrent tumors were treated by repeat rRFA, there
was no difference in secondary recurrence or need for
additional therapy between the 2 groups. Notably, pa-
tients with larger lesions can still be successfully treat-
ed by RFA, although a second ablation may be nec-
essary in some patients. Many studies similarly show
high secondary success rates after repeat ablation.6,12,29
Thus, tumor size alone should not be considered a
contraindication to rRFA as long as close surveillance
is performed to allow repeat ablation if needed.
Overall complications were noted in 8 out of 37 pa-
tients (22%). Four patients (11%) experienced major
complications requiring either an unplanned hospital
admission or an unplanned increase in patient care.
Four patients (11%) experienced minor complications
that did not require extra patient care, hospital stay, or
intervention. One patient with a pre-existing history
of CKD started dialysis 39 months after treatment. No
other patients started dialysis after rRFA treatment,
confirming the safety of the procedure in preserving
viable renal mass.
Gervais et al18 noted that 6 months after ablation, 20
out of 23 tumors decreased in size only slightly by 1
cm or less; the remaining 3 tumors decreased by more
than 1 cm.30 To our knowledge, no prior work has de-
scribed serial changes to lesion size following RFA in-
tervention in detail. Therefore, we tracked lesion size
at each follow-up appointment after the initial pro-
cedure. A linear regression model illustrated that the
decline in lesion size after rRFA was similar despite
the baseline diameter of the treated lesion. Another
linear regression analysis showed post-rRFA reduc-
tion in size was preserved regardless of whether or not
the lesion was a biopsy-proven RCC. In our series,
recurrent tumors increased in size with new contrast
enhancement in follow-up images. Familiarity with
the anticipated temporal course in lesion size may be
important in early assessment of recurrence, particu-
larly in patients unable to receive iodinated contrast
for CT scans.
CONCLUSIONRenal radiofrequency ablation safely and effec-
tively treats kidney tumors, including RCC. Com-
plication and recurrence rates are more common
in lesions ≥3 cm, but major complications remain
low. A repeat ablation may be necessary in a small
percentage of patients with larger lesions. In this
group, a lack of subsequent recurrence suggests
that size alone should not be considered a con-
traindication to rRFA treatment. After ablation,
Rundback_v.indd 29 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E30April 2014 • InterventionalOncology360.com
serial changes in lesion size are similar regardless
of the original size and regardless of whether the
lesion had been biopsy-proven RCC.
ACKNOWLEDGEMENTSThe authors would like to thank Yitzchak David,
MPH, for providing the statistical analysis of the data,
and David Daniel for his assistance in researching ref-
erence materials.
REFERENCES1. Lipworth L, Tarone RE, and McLaughlin JK: The epi-
demiology of renal cell carcinoma. J Urol. 2006;176(6 Pt
1):2353-2358.
2. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013.
CA Cancer J Clin. 2013;63(1):11-30.
3. Tareen B, Harper W, Garg S, et al. FirstConsult: Renal cell
carcinoma. 2010. http://www.mdconsult.com.
4. Alberta Provincial Genitourinary Tumour Team. Re-
nal Cell Carcinoma. Edmonton, Alberta, Canada: Alberta
Health Services, Cancer Care; 2012.
5. Pettus JA, Werle DM, Saunders W, et al. Percutaneous ra-
diofrequency ablation does not affect glomerular filtration
rate. J Endourol. 2010;24(10):1687-1691.
6. Takaki H, Yamakado K, Soga N, et al. Midterm results of
radiofrequency ablation versus nephrectomy for T1a renal
cell carcinoma. Jpn J Radiol. 2010;28(6):460-468.
7. Lucas SM, Stern JM, Adibi M, Zeltser IS, Cadeddu JA,
Raj GV. Renal function outcomes in patients treated for
renal masses smaller than 4 cm by ablative and extirpative
techniques. J Urol. 2008;179(1):75-79.
8. Watanabe F, Kawasaki T, Hotaka Y, et al. Radiofrequency
ablation for the treatment of renal cell carcinoma: initial
experience. Radiat Med. 2008;26(1):1-5.
9. Hiraoka K, Kawauchi A, Nakamura T, Soh J, Mikami K,
Miki T. Radiofrequency ablation for renal tumors: Our
experience. Int J Urol. 2009;16(11):869-873.
10. Nitta Y, Tanaka T, Morimoto K, et al. Intermediate onco-
logical outcomes of percutaneous radiofrequency ablation
for small renal tumors: initial experience. Anticancer Res.
2012;32(2):615-618.
11. Varkarakis IM, Allaf ME, Inagaki T, et al. Percutaneous ra-
dio frequency ablation of renal masses: results at a 2-year
mean followup. J Urol. 2005;174(2):456-460.
12. Ferakis N, Bouropoulos C, Granitsas T, Mylona S, Poulias
I. Long-term results after computed-tomography-guided
percutaneous radiofrequency ablation for small renal tu-
mors. J Endourol. 2010;24(12):1909-1913.
13. Tracy CR, Raman JD, Donnally C, Trimmer CK, Caded-
du JA. Durable oncologic outcomes after radiofrequency
ablation: experience from treating 243 small renal masses
over 7.5 years. Cancer. 2010;116(13):3135-3142.
14. Levinson AW, Su LM, Agarwal D, et al. Long-term on-
cological and overall outcomes of percutaneous radio
frequency ablation in high risk surgical patients with a
solitary small renal mass. J Urol. 2008;180(2):499-504.
Disclosure: The authors have completed and re-turned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no disclo-sures related to the content of this manuscript.Manuscript received February 16, 2014; provision-al acceptance given March 18, 2014; final version accepted March 25, 2014.
Address for correspondence: John H. Rundback, MD, 718 Teaneck Road, Teaneck, New Jersey 07666, United States. Email: [email protected] name.org
Suggested citation: Lee N, Rundback JH, Her-man KC, Kerns J, Barkama R. Outcomes follow-ing CT-guided percutaneous radiofrequency abla-tion of primary renal tumors. Intervent Oncol 360. 2014;2(4):E18-E31.
Rundback_v.indd 30 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions

ORIGINAL RESEARCH
E31April 2014 • InterventionalOncology360.com
15. Zagoria RJ, Traver MA, Werle DM, Perini M, Hayasaka S,
Clark PE. Oncologic efficacy of CT-guided percutaneous
radiofrequency ablation of renal cell carcinomas. AJR Am
J Roentgenol. 2007;189(2):429-436.
16. Sacks D, McClenny TE, Cardella JF, Lewis CA. Society
of Interventional Radiology clinical practice guidelines. J
Vasc Interv Radiol. 2003;14(9 Pt 2):S199-S202.
17. Atwell TD, Schmit GD, Boorjian SA, et al. Percutaneous
ablation of renal masses measuring 3.0 cm and smaller:
comparative local control and complications after radio-
frequency ablation and cryoablation. AJR Am J Roentgen-
ol. 2013;200(2):461-466.
18. Gervais DA, McGovern FJ, Arellano RS, McDougal WS,
Mueller PR. Radiofrequency ablation of renal cell carci-
noma: Part I. Indications, results, and role in patient man-
agement over a 6-year period and ablation of 100 tumors.
AJR Am J Roentgenol. 2005;185(1):64-71.
19. Gupta A, Raman JD, Leveillee RJ, et al. General anes-
thesia and contrast-enhanced computed tomography to
optimize renal percutaneous radiofrequency ablation:
multi-institutional intermediate-term results. J Endourol.
2009;23(7):1099-1105.
20. Frank I, Blute ML, Cheville JC, Lohse CM, Weaver AL,
Zincke H. Solid renal tumors: an analysis of pathologi-
cal features related to tumor size. J Urol. 2003;170(6 Pt
1):2217-2220.
21. Raman JD, Hall DW, Cadeddu JA. Renal ablative therapy:
radiofrequency ablation and cryoablation. J Surg Oncol.
2009;100(8):639-644.
22. Kunkle DA, Uzzo RG. Cryoablation or radiofrequency
ablation of the small renal mass: a meta-analysis. Cancer.
2008;113(10):2671-2680.
23. Pirasteh A, Snyder L, Boncher N, Passalacqua M,
Rosenblum D, Prologo JD. Cryoablation vs. Radiofre-
quency Ablation for Small Renal Masses. Acad Radiol.
2011;18(1):97-100.
24. El Dib R, Touma NJ, Kapoor A. Cryoablation vs radio-
frequency ablation for the treatment of renal cell car-
cinoma: a meta-analysis of case series studies. BJU Int.
2012;110(4):510-516.
25. Turna B, Kaouk JH, Frota R, et al. minimally invasive
nephron sparing management for renal tumors in solitary
kidneys. J Urol. 2009;185(2):2150-2157.
26. Olweny EO, Park SK, Tan YK, Best SL, Trimmer C, Ca-
deddu JA. Radiofrequency ablation versus partial ne-
phrectomy in patients with solitary clinical t1a renal cell
carcinoma: comparable oncologic outcomes at a mini-
mum of 5 years of follow-up. Eur Urol. 2012;61(6):1156-
1161.
27. Zagoria RJ, Pettus JA, Rogers M, Werle DM, Childs D,
Leyendecker JR. Long-term outcomes after percutaneous
radiofrequency ablation for renal cell carcinoma. Urology.
2011;77(6):1393-1397.
28. Faddegon S, Cadeddu JA. Does renal mass ablation pro-
vide adequate long-term oncologic control? Urol Clin
North Am. 2012;39(2):181-190.
29. Balageas P, Cornelis F, Le Bras Y, et al. Ten-year experi-
ence of percutaneous image-guided radiofrequency abla-
tion of malignant renal tumors in high-risk patients. Eur
Radiol. 2013;23(7):1925-1932.
30. Gervais DA, McGovern FJ, Arellano RS, McDougal WS,
Mueller PR. Renal cell carcinoma: clinical experience
and technical success with radio-frequency ablation of 42
tumors. Radiol. 2003;226(2):417-424.
Rundback_v.indd 31 4/16/14 4:25 PM
Copyri
ght H
MP Com
munica
tions
Related Documents