Intracranial Complications of Otitis Media Department of ENT Presenter-Surendra Poudel (2010/58)

Otitis media intracranial complications
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Intracranial Complications of Otitis Media
Department of ENT
Presenter-Surendra Poudel
(2010/58)

Intracranial Complications of OtitisMedia
Meningitis
Otogenic brain abscess
Lateral sinus thrombophlebitis
Epidural abscess
Subdural abscess
Otitic hydrocephalus
1. Meningitis
Inflammation of leptomeninges(piamater and arachnoid mater) .
Most common and serious intracranial complication.
Follows Acute otitis media (AOM) in children and infants (blood borne spread);
And Chronic suppurative otitis media(CSOM) in adults. (bone erosion or retrograde thrombophlebitis).

Clinical features
Rise in temperature(102-104∙F)often with chills and rigor
Headache
Neck rigidity
Photophobia and mental irritability
Nausea and vomiting(sometimes projectile)
Drowsiness which may progress to delirium or coma
Cranial nerve palsies and hemiplegia
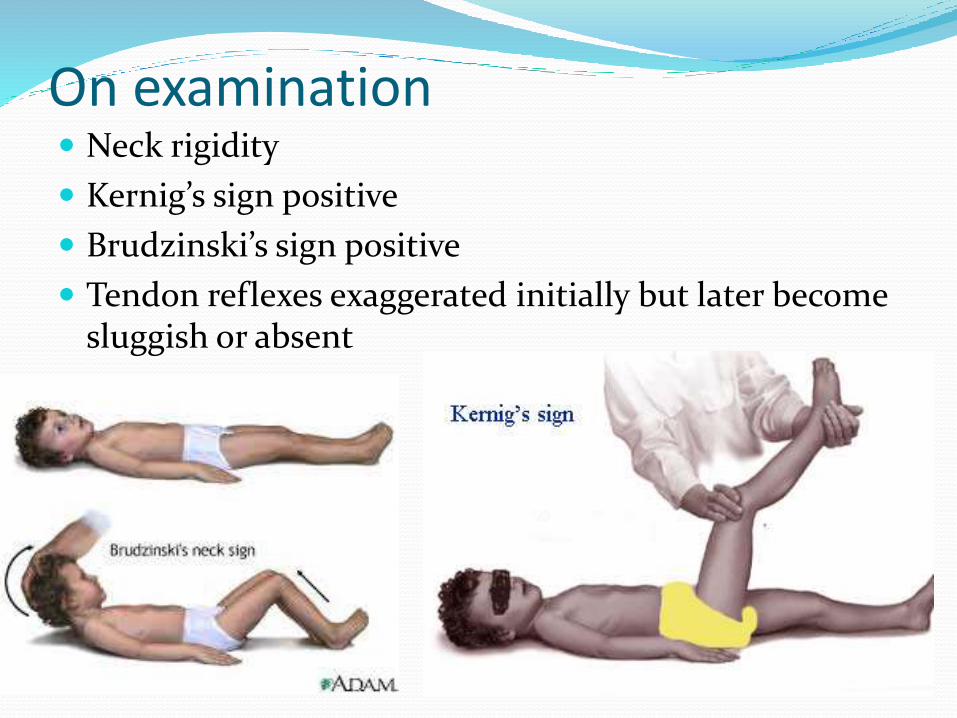
On examination Neck rigidity
Kernig’s sign positive
Brudzinski’s sign positive
Tendon reflexes exaggerated initially but later become sluggish or absent

Diagnosis History and clinical presentation
Investigation;
lumbar puncture: cell count , protein, sugar
CT scan , MRI
Treatment Antimicrobials with Dexamethasone
Surgical controversial) only in cases of antimicrobials failing to respond in 48 hrs

2. Otogenic Brain Abscess
Develops in the temporal lobe or the cerebellum of the affected side .
Temporal lobe abscess is twice as common as cerebellar abscess.
In children, 25% of brain abscesses are otogenic;
50% in case of adults
Brain abscess develops through 4 stages
1. Stage of invasion (initial encephalitis)
-usually asymptomatic
2. Stage of localisation(latent abscess)
3. Stage of enlargement(manifest abscess) -aggravation of symptoms
4. Stage of termination(rupture of abscess) - fatal meningitis
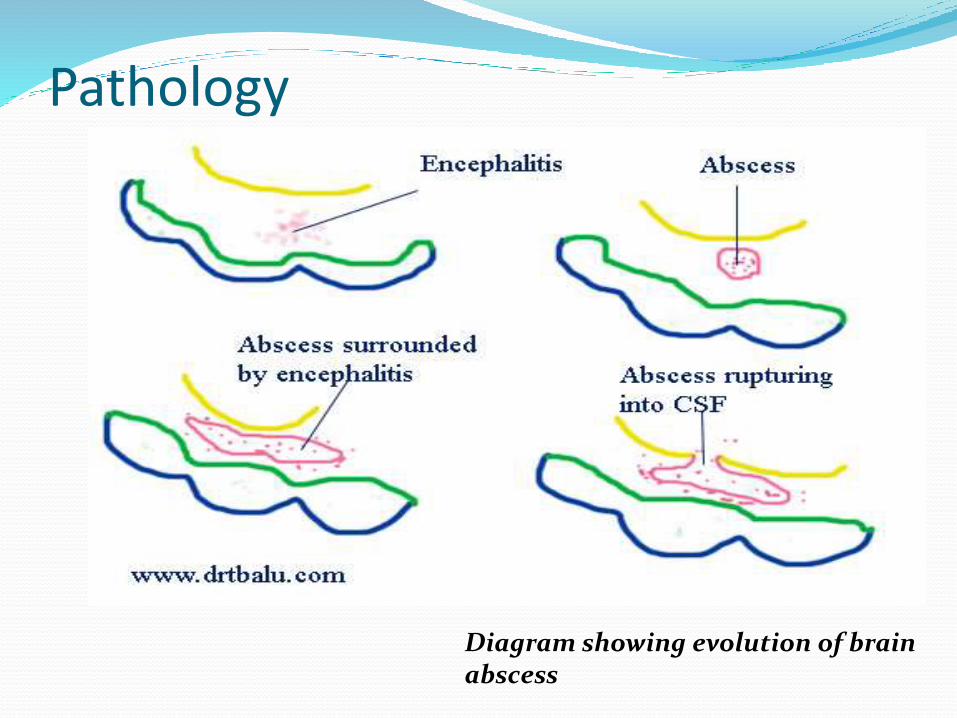
Pathology
Diagram showing evolution of brain abscess

Clinical features
Due to raised ICP;
Headache
Nausea and vomiting
Level of consciousness
Papilloedema
Slow pulse and subnormal temperature

Localising features
Temporal lobe abscess Cerebellar abscess
Nominal aphasia Headache
Homonymous hemianopia Spontaneous nystagmus
Contralateral motor paralysis Ipsilateral hypotonia and weakness
Epileptic fits Ipsilateral ataxia
Pupillary changes andoculomotor palsy
Past pointing and intentiotremor
Dysdiadochokinesia
InvestigationsSkull X ray, CT scan , X ray mastoids or CT scan, lumbar pubcture
TreatmentMedical -
high dose intravenous broad spectrum antibiotics
ceftriaxone +metronidazole+gentamicin
Dexamethasone
Anti epileptics: phenytoin
Antibiotics ear drop andayral toilet
Surgical-
Multidisciplinary(Neurosurgeon +ENT surgeon)
- surgical drainage of the abscess, followed by mastoidectomy to clear the ear disorder.

3. Lateral sinus thrombophlebitis
Inflammation of inner wall of lateral venous sinus with formation of an intrasinus thrombus

PathophysiologyErosion of sigmoid sinus plate peri-sinus abscess inflammation of
outer wall endophlebitis mural thrombus infect, Propagateor size occlusion of sinus lumen intra-sinus abscess propagating infected thrombus

Clinical features Hectic Picket-fence type of fever with rigors
Headache
Progressive anaemia and emaciation
Griesinger’s sign(pathognomic)
Papilloedema
Tobey-Ayer test
Crowe-Beck test
Tenderness along jugular vein

Investigations
Blood smear, culture
CSF examination
X ray mastoids
Imaging
Culture and sensitivity of ear swab
Treatment
IV antibiotics
Mastoidectomy: Cortical (AOM), R/MRM (COM)
Expose the sinus Confirm by look, feel &
aspiration Evacuation

4. Epidural abscess
Collection of pus between the bone and duramater

Pathophysiology
The affected dura is covered with granulation and appear unhealthy and discolored
In AOM, bone over dura- destroyed by hyperemic decalcification.
In COM, destroyed by cholesteatoma.

Clinical features
Usu. Asymptomatic, and discovered accidentally during surgery(cortical or modified radial mastoidectomy)
However , presence is suspected when there is,
1. Persistent headache on the side of OM
2. Severe pain in the ear
3. General malaise with low grade fever
4. Pulsatile purulent ear discharge
5. Disappearance of headache with free flow of pus from the ear(spontaneous abscess drainage)

Diagnosis :
contrast enhanced CT or MRI
Treatment:
Antimicrobial therapy
surgical exploration

5. Subdural abscess
Collection of pus between dura and arachnoid mater

Pathology

Clinical featuresMeningeal irritation •Fever(102*F or more)
•Headache•Malaise, drowsiness•Neck rigidity•Kernig’s sign positive
Thrombophlebitis(cortical veins of cerebrum)
•aphasia•Hemianopia•Hemiplegia•Jacksonian type of epileptic fits
Raised ICP 3rd nerve involvement;papilloedema, ptosis,dilated pupil

Diagnosis by CT or MRI
Treatment
surgical emergency: managed by neurosurgeon
Treatment of choice:
High dose iv antibiotics
Once stabilised neurologically, then underlying ear disease managed
Surgery of ear
Antiepileptic medication

Otitic hydrocephalus
Characterised by raised intracranial pressure with normal CSF findings.
It is seen in children and adolescents with acute or chronic middle ear infections
Mechanism:lateral sinus thrombosis -> obstruction of venous return. If thrombosis extends to superior sagittalsinus,it will also impede the function of arachnoidvilli->Raised ICP

Cliniacal features
Headache
Drowsiness
Nausea & Vomiting
Blurring of vision
Diplopia
Papilloedema
6th CN nerve palsy
Eventually optic atrophy

Investigations
Lumbar Puncture
Elevated CSF pressures with normal biochemistry
Done with caution (herniation)
CT scan
MRI:
Imaging modality of choice
Allows for superior evaluation of venous sinuses

Management
Goal Eradication of ear disease and Lowering elevated intracranial pressure
Recommendations Decompression of sigmoid sinus CSF fluid drainage – shunts Optic Sheath decompression: To prevent optic
atrophy
Medical:MannitolDiuretics Corticosteroids Acetazolamide

Thank you
Related Documents











