Osteoporosis Osteoporosis UBC Internal Medicine Program Dr. Mark Fok Dr. Maria Ashley

Osteoporosis UBC Internal Medicine Program Dr. Mark Fok Dr. Maria Ashley.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

OsteoporosisOsteoporosis
UBC Internal Medicine Program
Dr. Mark FokDr. Maria Ashley

DefinitionDefinitionOsteoporosis and osteopenia are skeletal
disorders characterized by low bone mass and microarchitectural fragility.
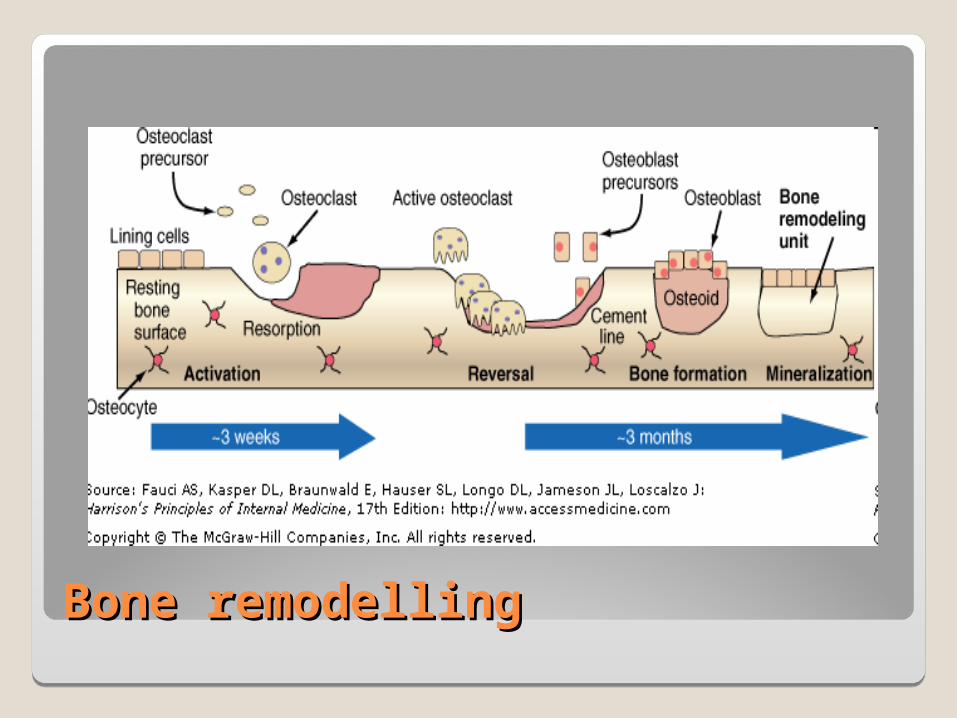
Bone remodellingBone remodelling
IncidenceIncidence
1.4 million Canadians affected1 in 4 women over age 50 and 1 in 8 men
over age 50Estimated cost of $1.9 billion to treat
osteoporosis and fractures in Canada70% of hip fractures are osteoporosis
related www.osteoporosis.ca

What else do you want to know?What else do you want to know?
Major Risk Factors for OsteoporosisAge >65Vertebral compression #Family hx of osteoporotic #>5 months glucocorticoid txMalabsorbtion syndrome1 hyperparathyroidismOsteopenia on XRHypogonadismEarly menopause (before 45)

Minor Risk Factors
◦Rheumatoid arthritis◦Hyperthyroidism◦Prolonged anticonvulsants◦Prolonged heparin use◦Body weight <57kg◦Low calcium intake◦Excess caffeine (>4 cups/day)◦Excess alcohol (>2 drinks/day)◦Smoker

Risk for FractureRisk for FractureLow Bone Mineral DensityPrior fragility fractureLong term (>3 months) glucocorticoidsIncreasing ageFamily history of osteoporotic fracture

Signs and Symptoms of OsteoporosisSigns and Symptoms of Osteoporosis
Self reported height loss >3cmWeight <51kgKyphosis - Self reported hump backGrip strength <40lbTooth count <20

Diagnosis of OsteoporosisDiagnosis of Osteoporosis
Assessment bone microarchitecture – bone biopsy
Clinical – fracture in the right context
Gold standard…

Bone Mineral Density AssessmentBone Mineral Density Assessment
Dual-Energy Xray Absorptiometry (DXA)
◦Strong correlation between mechanical bone strength DXA measurement of BMD
◦Strong relationship between fracture risk and BMD measurement
Lotz JC et al. J Biomech Eng 1991Marshall D et al. BMJ 1996

DXADXA
Xray tube generates photon beams at two energy levels
Difference in attenuation BMD determination
For comparison, must use same machine

Interpreting a DXA Scan ?Interpreting a DXA Scan ?

Interpreting the DXAInterpreting the DXA
T-score: ◦Standard deviation between a pt’s BMD and
that of a young adult reference population
Z-score: ◦Standard deviation between a pt’s BMD and
that of an age matched population

Interpreting the DXA – WHO criteriaInterpreting the DXA – WHO criteria
Normal - 1 < T score
Low Bone Mass (osteopenia)
- 2. 5 < T score < - 1
Osteoporosis T score < - 2.5
Severe osteoporosis T score < - 2.5 + fragility fracture

DXA scan hip / L-spineDXA scan hip / L-spine

Treatment of OsteoporosisTreatment of Osteoporosis
Non-drug options
Drug options
Weight bearing exercisesWeight bearing exercises

Exercises that utilize your own body weight include activities like these, but also include simple activities like walking.

Calcium rich foods

Over the counter vitaminsOver the counter vitamins
1200-1500 mg elemental calcium per day
800 IU vitamin D per day

Drugs – “Bisphosphonates”Drugs – “Bisphosphonates”
Alendronate
Risedronate
Etidronate

DosingDosing
Once weekly dosing (70 mg q week) as effective as daily dosing of alendronate with similar side effect profile
Rizzoli et al. J Bone Miner Res 2002

Risedronate Risedronate
Similar efficacy
Comparable to Alendronate
Rosen et al. J Bone Miner. Res. 2005
““Selective Estrogen Selective Estrogen
Receptor Modulators”Receptor Modulators”
Raloxifene
Tamoxifen Bind with high affinity to Estrogen Receptor and
possess tissue selective agonist / antagonist properties bone specific “estrogen like” action

Bone Forming (Anabolic)Bone Forming (Anabolic) MedicationsMedications
Parathyroid Hormone –Teriparatide (brand name - Forteo®).
Teriparatide, a type of parathyroid hormone, is approved for the treatment of osteoporosis in postmenopausal women and in men who have very low BMD or are at high risk for a fracture.
Estrogen therapyEstrogen therapy
Fallen out of favor for treatment of osteoporosis since WHI study
Increased risk of CHD, VT, breast CA
Should not be used first line, except for in women using it for other indications


Quick quiz 1.Are you over 65? 2.Has either of your parents broken a bone after a minor bump or fall? 3.Have you broken a bone after a minor bump or fall? 4.Have you taken glucocorticoid pills (cortisone, prednisone, etc.) for more than three months? 5.Have you lost more than 4 cm (about 1 1/2 inches) in height since age 25 (or 6 cm if you are over 60)? 6.Do you have a tendency to fall? 7.Do you have primary hyperparathyroidism? 8.Do you have a medical condition (such as celiac disease or Crohn's disease) that inhibits absorption of nutrients? 9.Has a recent x-ray suggested you have low bone density (osteopenia)?
For Women:10.Did you undergo menopause before age 45? 11.Have your periods stopped for several months or more (other than for pregnancy or menopause)?
For Men:12.Have you ever suffered from impotence, lack of libido or other symptoms related to low levels of testosterone?
If you're over 50 and have answered yes to any of these questions, Osteoporosis Canada recommends that you talk to your doctor about having a bone mineral density (BMD) test.

Thank youThank you
Related Documents











