Osteoporosis in Lung Transplantation Candidates with End-Stage Pulmonary Disease Elizabeth Shane, MD, Shonni J. Silverberg, MD, Daniel Donovan, MD, Anastasio Papadopoulos, MD, Ronald B. Staron, MD, Vicki Addesso, Birgit Jorgesen, RN, Carlton McGregor, MD, Larry Schulman, MD, New York, New York PURPOSE: Fractures, a common complication of cardiac and liver transplantation, have not been reported in association with lung transplantation. However, many patients with end-stage pulmonary disease have multiple risk factors for osteoporosis, and several studies have suggested that osteoporosis before transplantation may increase the risk of fracture after transplantation. Therefore, we evaluated a group of patients with end-stage pulmonary disease who were awaiting lung transplantation to determine the prevalence of osteoporosis. METHODS: Seventy patients (aged 18-70 years) were evaluated consecutively with bone densitometry by dual-energy x-ray absorptiometry. The patients were predominantly Caucasian (96%). Bone mass was expressed as bone mineral density (BMD; g/cm*), as the number of standard deviations (SD) below peak bone mass (T score), and as bone mineral apparent density (BMAD; g/cm3), a measurement that minimizes the effects of bone size on BMD. Spine radiographs were obtained in a subset of 50 consecutive patients to detect vertebral compression fractures. Vitamin D status was assessed with serum concentrations of 25-hydroxyvitamin D. The patients were sorted into groups by pulmonary diagnosis: chronic obstructive pulmonary disease (COPD; n = 28); cystic fibrosis (n = 11); idiopathic pulmonary fibrosis; and other lung diseases (Other; n = 31). RESULTS: In the group as a whole, osteoporosis (T score below -2.5) was present in 30% of the patients at the lumbar spine and 49% at I I From the Departments of Medicine and Radiology (RBS), Columbia- Presbyterran Medrcal Center and College of Physrcians & Surgeons, Co- lumbia Unrversrty, New York, New York. Reorint reauests should be addressed to Elizabeth Shane. MD. Depart men; of Medicine, College of Physicians and Surgeons, Columbia Univer- sitv, 630 West 168th Street, New York, New York 10032. Supported in part by grants 006645 and RO-1 AR51391 from the Na- tional lnshtutes of Health. Manuscript submitted January 19, 1996 and accepted in revised form May 15, 1996. the femoral neck. Osteopenia (T score between -1 and -2.5) was present in an additional 35% at the lumbar spine and 31% at the femoral neck. The average femoral neck T score of patients with COPD and cystic fibrosis fell into the osteoporotic range (-2.7 + 0.3 and -2.6 -c 0.3, respectively), significantly (P ~0.01) below that of the patients in the Other category (- 1.5 t 0.3). The average lumbar spine T score fell into the osteopenic range in all three groups. Low BMAD in patients with cystic fibrosis confirmed that their low BMD was not due to their smaller body size. The prevalence rate of vertebral fractures was 29% in patients with COPD and 25% in those with cystic fibrosis. Vitamin D deficiency (25- hydroxyvitamin D levels 110 rig/ml) was present in 36% of patients with cystic fibrosis and 20% with COPD and Other lung diseases. Lumbar spine BMD tended to be lower in cystic fibrosis patients with vitamin D deficiency. Patients with exposure to glucocorticoids (n = 46) had significantly more vertebral fractures (P ~0.05) and duration of exposure correlated negatively with lumbar spine BMD (r =: -0.398; P = 0.008). COPD and Other patients not on glucocorticoids had mild lumbar spine osteopenia (0.972 2 0.06 g/cm*; T = -1.2 i- 0.6). Very few of the patients on glucocorticoids were on any regimen to prevent osteoporosis. CONCLUSIONS: Osteoporosis and vitamin D deficiency are extremely common in patients with end-stage pulmonary disease. Only 34% of patients had normal lumbar spine BMD and only 22% had normal BMD at the hip. Patients with cystic fibrosis and glucocorticoid-treated patients with COPD were most severely affected. Therapies to prevent bone loss and treat established osteoporosis are uncommonly utilized in glucocorticoid-treated patients with end-stage pulmonary disease. Candidates for lung transplantation should be evaluated for osteoporosis and vitamin D deficiency at the time of acceptance to the transplant waiting list. Am J Med. 1996; 101:262-269. 262 01996 by Excerpta Medica, Inc. OOOZ-9343/96/$15.00 All rights reserved. PII SOOO2-9343(96)00155-6

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Osteoporosis in Lung Transplantation Candidates with End-Stage Pulmonary Disease Elizabeth Shane, MD, Shonni J. Silverberg, MD, Daniel Donovan, MD, Anastasio Papadopoulos, MD, Ronald B. Staron, MD, Vicki Addesso, Birgit Jorgesen, RN, Carlton McGregor, MD, Larry Schulman, MD, New York, New York
PURPOSE: Fractures, a common complication of cardiac and liver transplantation, have not been reported in association with lung transplantation. However, many patients with end-stage pulmonary disease have multiple risk factors for osteoporosis, and several studies have suggested that osteoporosis before transplantation may increase the risk of fracture after transplantation. Therefore, we evaluated a group of patients with end-stage pulmonary disease who were awaiting lung transplantation to determine the prevalence of osteoporosis.
METHODS: Seventy patients (aged 18-70 years) were evaluated consecutively with bone densitometry by dual-energy x-ray absorptiometry. The patients were predominantly Caucasian (96%). Bone mass was expressed as bone mineral density (BMD; g/cm*), as the number of standard deviations (SD) below peak bone mass (T score), and as bone mineral apparent density (BMAD; g/cm3), a measurement that minimizes the effects of bone size on BMD. Spine radiographs were obtained in a subset of 50 consecutive patients to detect vertebral compression fractures. Vitamin D status was assessed with serum concentrations of 25-hydroxyvitamin D. The patients were sorted into groups by pulmonary diagnosis: chronic obstructive pulmonary disease (COPD; n = 28); cystic fibrosis (n = 11); idiopathic pulmonary fibrosis; and other lung diseases (Other; n = 31).
RESULTS: In the group as a whole, osteoporosis (T score below -2.5) was present in 30% of the patients at the lumbar spine and 49% at
I I
From the Departments of Medicine and Radiology (RBS), Columbia- Presbyterran Medrcal Center and College of Physrcians & Surgeons, Co- lumbia Unrversrty, New York, New York.
Reorint reauests should be addressed to Elizabeth Shane. MD. Depart men; of Medicine, College of Physicians and Surgeons, Columbia Univer-
sitv, 630 West 168th Street, New York, New York 10032. Supported in part by grants 006645 and RO-1 AR51391 from the Na-
tional lnshtutes of Health. Manuscript submitted January 19, 1996 and accepted in revised form
May 15, 1996.
the femoral neck. Osteopenia (T score between -1 and -2.5) was present in an additional 35% at the lumbar spine and 31% at the femoral neck. The average femoral neck T score of patients with COPD and cystic fibrosis fell into the osteoporotic range (-2.7 + 0.3 and -2.6 -c 0.3, respectively), significantly (P ~0.01) below that of the patients in the Other category (- 1.5 t 0.3). The average lumbar spine T score fell into the osteopenic range in all three groups. Low BMAD in patients with cystic fibrosis confirmed that their low BMD was not due to their smaller body size. The prevalence rate of vertebral fractures was 29% in patients with COPD and 25% in those with cystic fibrosis. Vitamin D deficiency (25- hydroxyvitamin D levels 110 rig/ml) was present in 36% of patients with cystic fibrosis and 20% with COPD and Other lung diseases. Lumbar spine BMD tended to be lower in cystic fibrosis patients with vitamin D deficiency. Patients with exposure to glucocorticoids (n = 46) had significantly more vertebral fractures (P ~0.05) and duration of exposure correlated negatively with lumbar spine BMD (r =: -0.398; P = 0.008). COPD and Other patients not on glucocorticoids had mild lumbar spine osteopenia (0.972 2 0.06 g/cm*; T = -1.2 i- 0.6). Very few of the patients on glucocorticoids were on any regimen to prevent osteoporosis.
CONCLUSIONS: Osteoporosis and vitamin D deficiency are extremely common in patients with end-stage pulmonary disease. Only 34% of patients had normal lumbar spine BMD and only 22% had normal BMD at the hip. Patients with cystic fibrosis and glucocorticoid-treated patients with COPD were most severely affected. Therapies to prevent bone loss and treat established osteoporosis are uncommonly utilized in glucocorticoid-treated patients with end-stage pulmonary disease. Candidates for lung transplantation should be evaluated for osteoporosis and vitamin D deficiency at the time of acceptance to the transplant waiting list. Am J Med. 1996; 101:262-269.
262 01996 by Excerpta Medica, Inc. OOOZ-9343/96/$15.00 All rights reserved. PII SOOO2-9343(96)00155-6

OSTEOPOROSIS AND END-STAGE PULMONARY DISEASE/SHANE ET AL
R ecent advances in immunosuppressive therapy have improved survival rates after heart and
lung transplantation.’ However, the decline in peri- operative mortality has been associated with the de- velopment of painful fractures that adversely affect the quality of life of many transplant patients.“-” In a recent prospective longitudinal study, we observed that the incidence of fractures during the initial year after cardiac transplantation was 36%.‘” In that study, women who fractured had significantly lower bone density prior to transplantation, while men who fractured lost bone more rapidly after transplanta- tion.
16% of the entire group. Patients with all remaining diagnoses were included in a single category desig- nated “Other” (44%). We have observed that pa- tients with alpha-1 antitrypsin deficiency have low bone mass even when there is no history of exposure to glucocorticoids (unpublished observations), per- haps because of a potential influence of alpha-l an- titrypsin deficiency on osteoclast function.‘7 Since the 4 patients with this alpha-l antitrypsin deficiency may not be typical of other patients with COPD with respect to bone turnover, they were included in the “Other” category.
Many patients with end-stage pulmonary disease being considered for lung transplantation have sig- nificant risk factors for osteoporosis, such as Cau- casian race, older age, postmenopausal status, phys- ical inactivity, excessive use of tobacco, and previous or current therapy with glucocorticoids. All of these factors could contribute to a state of low bone mass prior to transplantation. In addition, both children and adults with cystic fibrosis may have low bone density compared with normative popula- tions.‘.‘-” At our institution, we have observed that osteoporotic fractures of various types also occur frequently after lung transplantation. Since patients with low bone mass before transplantation may be at increased risk to sustain fractures after transplan- tation, I3 we evaluated 70 patients with end-stage pul- monary disease who were awaiting lung transplan- tation to determine the prevalence of osteoporosis in this population.
Study Design Historical information was obtained from all pa-
tients on current and past exposure to glucocorti- coids, tobacco exposure, pharmacologic regimen, and generally accepted risk factors for osteoporosis such as menopausal status and family history of this disorder. These data were confirmed by review of the medical record.
METHODS Study Population
Between January 1, 1993 and May 31, 1995, 70 adult men and women with end-stage pulmonary dis- ease were consecutively evaluated following their acceptance to the lung transplantation waiting list. The patients were predominantly Caucasian (96%). Individuals with the following disorders known to affect bone and mineral metabolism were excluded: primary hyperparathyroidism, multiple myeloma, thyrotoxicosis or therapy with thyroid hormone that resulted in suppressed sensitive TSH, and renal in- sufficiency (serum creatinine >2.5 mg/dL). The study population included 28 patients with chronic obstructive pulmonary disease (COPD) ; 4 with al- pha-l antitrypsin deficiency; 11 with cystic fibrosis; 11 with idiopathic pulmonary fibrosis; 4 with primary pulmonary hypertension; 3 with Eisenmenger’s syn- drome; 3 with lymphangioleiomyomatosis; and 2 each with cystic bronchiectasis, tuberous sclerosis, and sarcoidosis. Patients were grouped into catego- ries by diagnosis. The patients with COPD accounted for 40%, while those with cystic fibrosis comprised
Each patient was evaluated with bone mineral densitometry (BMD) of the lumbar spine, hip, and nondominant forearm as measured by dual energy x- ray absorptiometry (DXA) using a QDR- 1000 bone densitometer (Hologic, Inc., Waltham, Massachu- setts). Measurement of lumbar spine BMD repre- sented the average of three vertebrae, usually the second, third, and fourth (L2-4). If one of these ver- tebrae was fractured, Ll was analyzed instead. In our laboratory, the reproducibility of the QDR-1000 den- sitometer using an anthropomorphic spine is 0.51%. The short-term in vivo coefficient of variation is 0.68% for the lumbar spine phantom (L-4) and 1.36% for the proximal femur. BMD was expressed in conventional terms as g/cm’; standardized T score analyses were also used to compare individual bone density determinations with those of a young normal control population of the same gender. The T score is a statistical transformation of data that represents a measure of the number of standard de- viations from mean peak bone mass of normal indi- viduals of the same gender.
To ascertain the effect upon bone mineral density of the smaller body size of the patients with cystic fibrosis, densitometric data were also reported as bone mineral apparent density (BMAD) in g/cm”, a calculation made by dividing the bone mineral con- tent (BMC) by a reference bone volume as described by Marcus and colleagues’“,” with modifications. This expression of bone mass reduces the influence of bone size on bone density measurements and per- mits a reasonable comparison of bone density among persons of differing heights. To calculate BMAD for the spine, the vertebral bodies are as- sumed to show geometric proportionality (width -
September 1996 The American Journal of Medicine” Volume 101 263
OSTEOPOROSIS AND END-STAGE PULMONARY DISEASE/SHANE ET AL
TABLE I Biochemistries in Patients with End-Stage Pulmonary Disease
Parameter COPD Cystic Fibrosis Other
Serum calcium (8.4-10.2 mg/dL) 9.1 ” 0.1 9.1 + 0.3 9.0 t 0.1 Parathyroid hormone (lo-65 pg/mL) 42 5 5 402 11 35 2 4 25 Hydroxyvitamin D (9-52 ng/mL) 20 + 2 1724 14 t 2 1,25 Dihydroxyvitamin D (15-60 pg/mL) 45 i- 5 43 2 6 31 + 4* The serum calcium levels reported in this table are corrected for the corresponding serum albumin level. * P ~0.05 compared with COPD.
,
height - thickness); the reference volume of L2-4 was estimated to be proportional to the projected area (A,) on the densitometry scan by the relation- ship: Volume,,, = Ap3”. Therefore, the BMAD of the spine was derived by the following: BMAD (La-4) = BMCIA,““. At the femoral neck and radius, the den- sitometry software imposes a fixed value of 1.5 and 2.0 em, respectively, on the length of bone that is scanned. Measurement of area at these sites, there- fore, changes only in proportion to bone width. The derived bone volume is therefore (A,,) (-4Jlength). Since the femoral neck length = 1.5 cm, Volume,,, = (4) (Api1.5). Thus BMAD of the femoral neck was estimated as: BMAD = BMC/(A,)(Ap/l.5). Since the radius length = 2 cm, Volume,,, = (A,)(A,/Z). Thus BMAD of the femoral neck was estimated as: BMAD = BMC/(A,) (A,/2).
A subset of 50 consecutive patients had a standard set of anteroposterior and lateral radiographs of the thoracic and lumbar spine to detect undiagnosed compression fractures. Radiographs were analyzed by one of us (RBS) and vertebral fractures (includ- ing wedge, biconcave, and compression deformities) were classified according to the method of Eastell et al.‘” Briefly, vertebrae T4-L5 are marked on lateral radiographs and measured to the nearest mm of an- terior (ha), middle (hm) , and posterior (hp) heights. Three t.ypes of vertebral deformity were considered to constitute a vertebral fracture: wedge deformity = (hp - ha)/hp X 100; biconcave defor- mity = (hp - hm)/hp X 100; compression deformity = (hp ’ - hp)/hp ’ x 100, where hp ’ is the posterior vertebral height of the adjacent upper or lower vert- bra1 body. Each vertebral area was compared with a normal range for that vertebra.l” A vertebral defor- mity was diagnosed if the degree of deformity was more than 3 SD from the norm.
Blood was obtained in the fasting stat.e for mea- surement of serum calcium, phosphorus, blood urea nitrogen (BUN), creatinine, parathyroid hormone (PTH) , metabolites of vitamin D, and osteocalcin, a protein synthesized by osteoblasts that is considered to be a marker of bone formation/turnover.‘o The samples were run together in batches. Serum cal- cium, phosphate, albumin, alkaline phosphatase ac-
tivity, creatinine, and BUN were measured by stan- dard auto-analyzer techniques (Technicon Instruments, Tarrytown, New York). Serum osteo- calcin was measured by radioimmunoassay.” Intact PTH was measured by radioimmunometric assay.” Serum levels of 25hydroxyvitamin D and 1,25 dihy- droxyvitamin D were measured as previously de- scribed.‘” The normal ranges for all biochemical measurements are given in Table I.
Statistical Methods All data are presented as the mean i: SEM. Asso-
ciations between various demographic, bone den- sity, and biochemical parameters were assessed us- ing Student’s unpaired t-test and analysis of variance.
This study was approved by the Institutional Re- view Board of Columbia-Presbyterian Medical Cen- ter, and written informed consent for participation was obtained from all subjects. The study was con- ducted in the Irving Center for Clinical Research and the Cardiopulmonary Transplant Unit of Columbia- Presbyterian Medical Center.
RESULTS The average age of the 70 patients was 47 years
(range, 18-70 years). Virtually all (96%) were Cau- casian. There were 25 men, 23 postmenopausal women, and 22 premenopausal women. Three of the premenopausal women were amenorrheic and 4 of the cyclic women were taking oral contraceptive medication. Four of the postmenopausal women were on estrogen replacement therapy.
The most common diagnosis was chronic obstruc- tive pulmonary disease (n = 28)) followed by cystic fibrosis (n = 11) and idiopathic pulmonary fibrosis (n = 11) . Thirty-six patients (51%) had a history of cigarette smoking. The average tobacco exposure was 56 pack-years (range, 10-130).
Bone Densitometry Low bone mass (expressed as T scores) was ex-
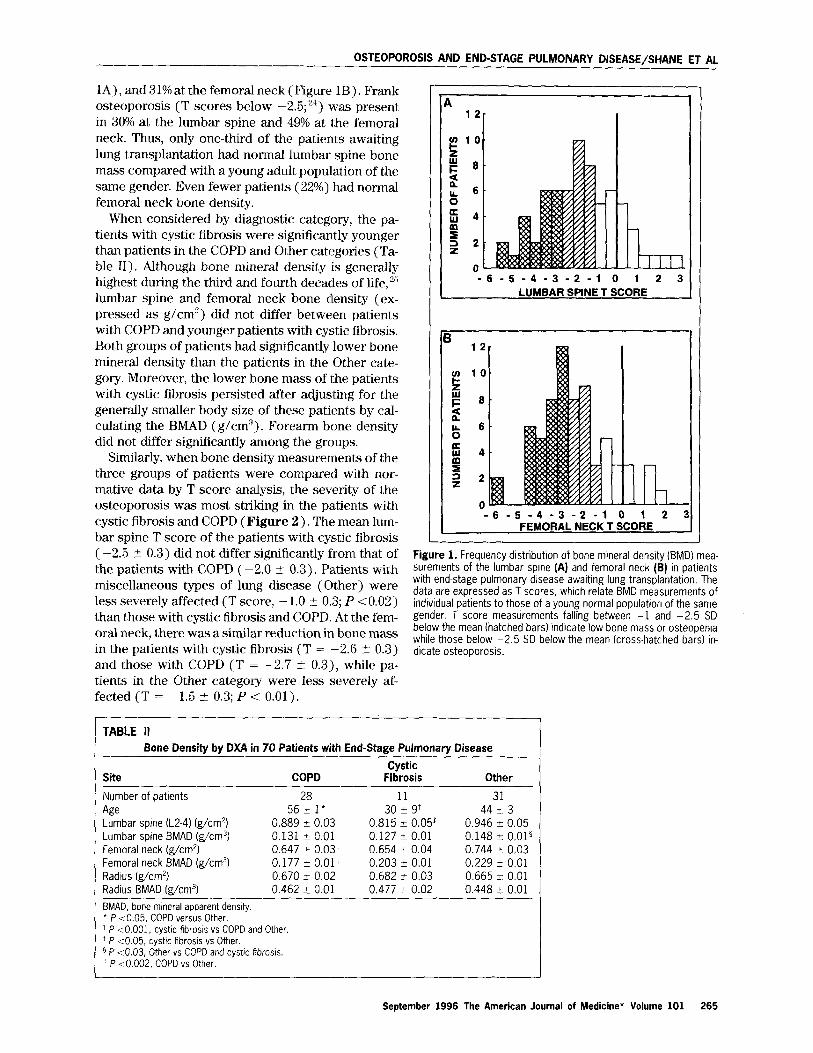
tremely common in the entire group of patients (Fig- ure 1). T scores between - 1.0 and -2.5, which rep- resent low bone mass or osteopenia,21 we:re present in 35% of the patients at the lumbar spin.e (Figure
264 September 1996 The American Journal of Medicines Volume 101
OSTEOPOROSIS AND END-STAGE PULMONARY DISEASE/SHANE ET AL
1A) , and 31% at the femoral neck (Figure 1B). Frank osteoporosis (T scores below -2.5;“) was present in 30% at the lumbar spine and 49% at the femoral neck. Thus, only one-third of the patients awaiting lung transplantation had normal lumbar spine bone mass compared with a young adult population of the same gender. Even fewer patients (22%) had normal femoral neck bone density.
When considered by diagnostic category, the pa- tients with cystic fibrosis were significantly younger than patients in the COPD and Other categories (Ta- ble 11). Although bone mineral density is generally highest during the third and fourth decades of life, ” lumbar spine and femoral neck bone density (ex- pressed as g/cm’) did not differ between patients with COPD and younger patients with cystic fibrosis. Both groups of patients had significantly lower bone mineral density than the patients in the Other cate- gory. Moreover, the lower bone mass of the patients with cystic fibrosis persisted after adjusting for the generally smaller body size of these patients by cal- culating the BMAD (g/cm”). Forearm bone density did not differ significantly among the groups.
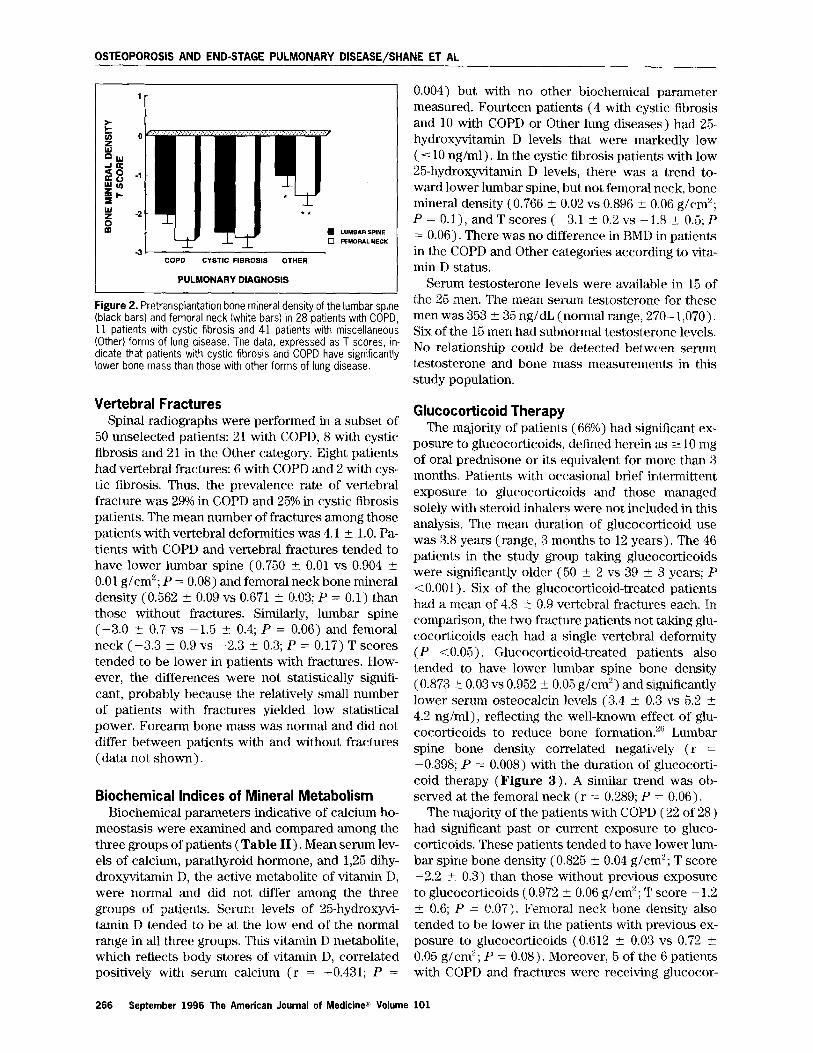
Similarly, when bone density measurements of the three groups of patients were compared with nor- mative data by T score analysis, the severity of the osteoporosis was most striking in the patients with cystic fibrosis and COPD (Figure 2). The mean lum- bar spine T score of the patients with cystic fibrosis (-2.5 2 0.3) did not differ significantly from that of the patients with COPD ( -2.0 2 0.3). Patients with miscellaneous types of lung disease (Ot.her) were less severely affected (T score, -1.0 t 0.3; P ~0.02) than those with cystic fibrosis and COPD. At the fem- oral neck, there was a similar reduction in bone mass in the patients with cystic fibrosis (T = -2.6 I- 0.3) and those with COPD (T = -2.7 ?I 0.3), while pa- tients in the Other category were less severely af- fected (T = -1.5 2 0.3; P < 0.01).
r 7
-6-S-4-3-2-1 ( LUMBAR SPINET SCORE
-8-5-4-3-2-l 0 1 2 : FEMORAL NECK T SCORE
L Figure 1. Frequency distribution of bone mineral density (BMD) mea- surements of the lumbar spine (A) and femoral neck (B) in patients with end-stage pulmonary disease awaiting lung transplantation. The data are expressed as T scores, which relate BMD measurements of individual patients to those of a young normal population of the same gender. T score measurements falling between -1 and -2.5 SD below the mean (hatched bars) indicate low bone mass or osteopenia while those below -2.5 SD below the mean (cross-hatched bars) in- dicate osteoporosis.
TABLE II
Site
Bone Density by DXA in 70 Patients with End-Stage Pulmonary Disease
Cystic COPD Fibrosis Other
11 31 30 k 9+ 44 I3
0.815 _t 0.057 0.946 + 0.05 0.127 k 0.01 0.148 2 0.01" 0.654 + 0.04 0.744 +- 0.03 0.203 2 0.01 0.229 i: 0.01 0.682 t 0.03 0.665 z 0.01 0.477 ? 0.02 0.448 _t 0.01
Number of patients 28
Age 562 1’ Lumbar spine (L2-4) (g/cm21 0.889 t 0.03 Lumbar spine BMAD (g/cm31 0.131 k 0.01 Femoral neck &/cm*) 0.647 2 0.03' Femoral neck BMAD (g/cm31 0.177 5 0.01” Radius (g/cm21 0.670 i 0.02 Radius BMAD (g/cm31 0.462 t 0.01 BMAD, bone mineral apparent density. ’ P ~0.05, COPD versus Other. t P <O.OOl, cystic fibrosis vs COPD and Other. * P ~0.05, cystic fibrosis vs Other. B P 4.03, Other vs COPD and cystrc Rbrosls. ” P <O.OOZ, COPD vs Other. I
September 1996 The American Journal of Medicine” Volume 101 265
OSTEOPOROSIS AND END-STAGE PULMONARY DISEASE/SHANE ET AL
COPD CYSTIC FIBROSIS OTHER
PULMONARY DIAGNOSIS
Figure 2. Pretransplantation bone mineral density of the lumbar spine (black bars) and femoral neck (white bars) in 28 patients with COPD. 11 patients with cystic fibrosis and 41 patients’with miscellaneous (Other) forms of lung disease. The data, expressed as T scores, in- dicate that patients wrth cystic fibrosis and COPD have significantly lower bone mass than those with other forms of lung disease.
Vertebral Fractures Spinal radiographs were performed in a subset of
50 unselected patients: 21 with COPD, 8 with cystic fibrosis and 21 in the Other category. Eight patients had vertebral fractures: 6 with COPD and 2 with cys- tic fibrosis. Thus, the prevalence rate of vertebral fracture was 29% in COPD and 25% in cystic fibrosis patients. The mean number of fractures among those patients with vertebral deformities was 4.1 t 1.0. Pa- tients with COPD and vertebral fractures tended to have lower lumbar spine (0.750 + 0.01 vs 0.904 t 0.01 g/cm’; P = 0.08) and femoral neck bone mineral density (0.562 t 0.09 vs 0.671 t 0.03; P = 0.1) than those without fractures. Similarly, lumbar spine (-3.0 -C 0.7 vs -1.5 5 0.4; P = 0.06) and femoral neck (-3.3 -c 0.9 vs -2.3 I 0.3; P = 0.17) T scores tended to be lower in patients with fractures. How- ever, the differences were not statistically signifi- cant, probably because the relatively small number of patients with fractures yielded low statistical power. Forearm bone mass was normal and did not differ between patients with and without fractures (data not shown).
Biochemical Indices of Mineral Metabolism
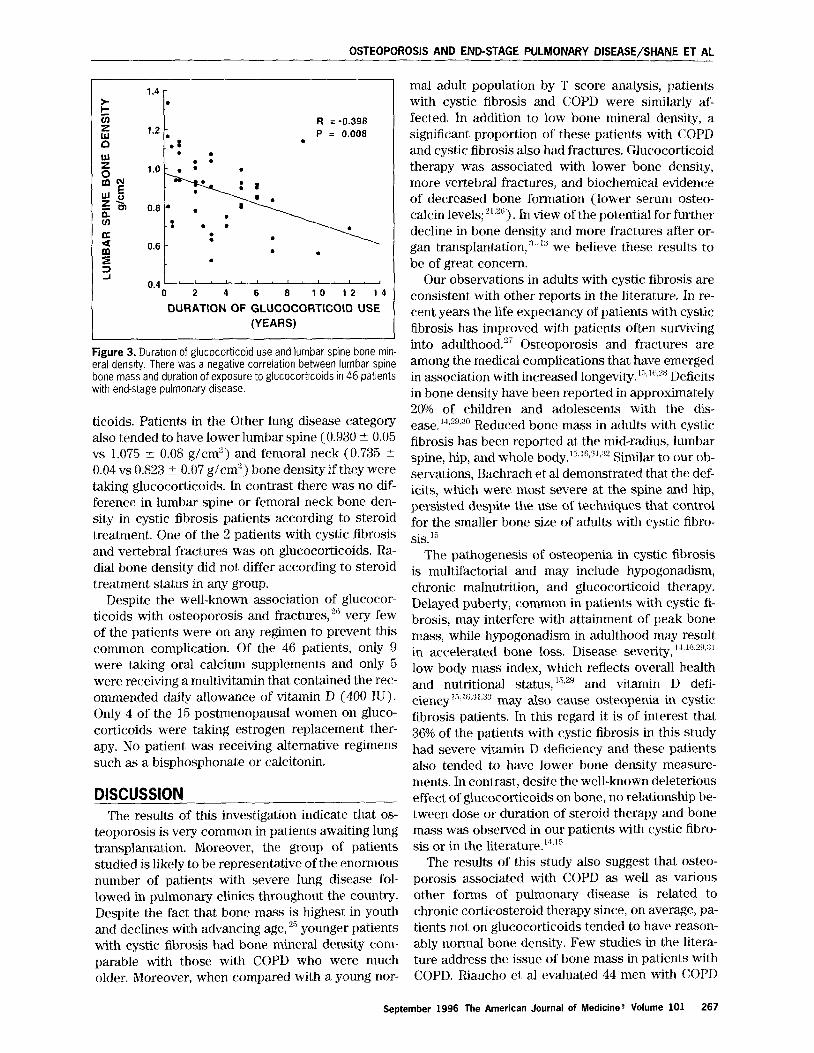
The majority of patients (66%) had significant ex- posure to glucocorticoids, defined herein as 2 10 mg of oral prednisone or its equivalent for more than 3 months. Patients with occasional brief intermittent exposure to glucocorticoids and those managed solely with steroid inhalers were not included in this analysis. The mean duration of glucocorticoid use was 3.8 years (range, 3 months to 12 years). The 46 patients in the study group taking glucocorticoids were significantly older (50 ? 2 vs 39 7t 3 years; P <O-001). Six of the glucocorticoid-treated patients had a mean of 4.8 i_ 0.9 vertebral fracturles each. In comparison, the two fracture patients not t.aking glu- cocorticoids each had a single vertebral deformity (P ~0.05). Glucocorticoid-treated patients also tended to have lower lumbar spine bone density (0.873 t 0.03 vs 0.952 f 0.05 g/cm’) and significantly lower serum osteocalcin levels (3.4 -C 0.3 vs 5.2 ? 4.2 rig/ml), reflecting the well-known effect of glu- cocorticoids to reduce bone formation.“” Lumbar spine bone density correlated negatively (r = -0.398; P = 0.008) with the duration of glucocorti- coid therapy (Figure 3). A similar trend was ob- served at the femoral neck (r = 0.289; P = 0.06).
Biochemical parameters indicative of calcium ho- The ma;jority of the patients with COPD (22 of 28) meostasis were examined and compared among the had significant past or current exposure to gluco- three groups of patients (Table II). Mean serum lev- corticoids. These patients tended to have lower lum- els of calcium, parathyroid hormone, and 1,25 dihy- bar spine bone density (0.825 +- 0.04 g/en?; T score droxyvitamin D, the active metabolite of vitamin D, -2.2 t- 0.3) than those without previous exposure were normal and did not differ among the three to glucocorticoids (0.972 & 0.06 g/cm”; T score - 1.2 groups of patients. Serum levels of 25-hydroxyvi- ? 0.6; P = 0.07). Femoral neck bone density also tamin D tended to be at the low end of the normal tended to be lower in the patients with previous ex- range in all three groups. This vitamin D metabolite, posure to glucocorticoids (0.612 -+ 0.03 vs 0.72 rt which reflects body stores of vitamin I>, correlated 0.05 g/cm”; P = 0.08). Moreover, 5 of the 6 patients positively with serum calcium (r = -i-0.431; P = with COPD and fractures were receiving glucocor-
0.004) but with no other biochemical parameter measured. Fourteen patients (4 with cysti.c fibrosis and 10 with COPD or Other lung diseases) had 25- hydroxyvitamin D levels that were markedly low ( 5 10 rig/ml) . In the cystic fibrosis patients with low 25-hydroxyvitamin D levels, there was a trend to- ward lower lumbar spine, but not femoral neck, bone mineral density (0.766 5 0.02 vs 0.896 t 0.06 g/cm’; P = O.l), and T scores (-3.1 ? 0.2 vs -1.8 + 0.5; P = 0.06). There was no difference in BMD in patients in the COPD and Other categories according to vita- min D status.
Serum testosterone levels were availab1.e in 15 of the 25 men. The mean serum testosterone for these men was 353 f 35 ng/dL (normal range, 270- 1,070). Six of the 15 men had subnormal testosterone levels. No relationship could be detected between serum testosterone and bone mass measurements in this study population.
Glucocorticoid Therapy
266 September 1996 The American Journal of Medicinea Volume 101
OSTEOPOROSIS AND END-STAGE PULMONARY DISEASE/SHANE ET AL
1.4 - z .
cl
B
R = -0.398 1.2 - :. P = 0.008 : .
P l . .
0 l.O- . :
.
“2 wo 21 5J 01 0.8 * .
-: . . s : .
0.6
-
m . . 9 . =? 2 0.4" " r t t I
0 2 4 6 8 10-4
DURATION OF GLUCOCORTlCOlD USE
(YEARS)
Figure 3. Duration of glucocotticoid use and lumbar spine bone min- eral density. There was a negative correlation between lumbar spine bone mass and duration of exposure to glucocorticoids in 46 patients with end-stage pulmonary disease.
ticoids. Pat,ients in the Other lung disease category also tended to have lower lumbar spine (0.930 2 0.05 vs 1.075 2 0.08 g/cm’) and femoral neck (0.735 & 0.04 vs 0.823 i 0.07 g/cm’) bone density if they were taking glucocorticoids. In contrast there was no dif- ference in lumbar spine or femoral neck bone den- sity in cystic fibrosis patients according to steroid treatment. One of the 2 patients with cystic fibrosis and vertebral fractures was on glucocorticoids. Ra- dial bone density did not differ according to steroid treatment status in any group.
Despite the well-known association of glucocor- ticoids with osteoporosis and fractures,‘” very few of the patients were on any regimen to prevent this common complication. Of the 46 patients, only 9 were taking oral calcium supplements and only 5 were receiving a multivitamin that contained the rec- ommended daily allowance of vitamin D (400 IU). Only 4 of the 15 postmenopausal women on gluco- corticoids were taking estrogen replacement ther- apy. No patient was receiving alternative regimens such as a bisphosphonate or calcitonin.
DISCUSSION The results of this investigation indicat.e that os-
teoporosis is very common in patients awaiting lung transplantation. Moreover, the group of patients studied is likely to be representative of the enormous number of patients with severe lung disease fol- lowed in pulmonary clinics throughout the country. Despite the fact that bone mass is highest in youth and declines with advancing age, ” younger patients with cystic fibrosis had bone mineral density com- parable with those with COPD who were much older. Moreover, when compared with a young nor-
mal adult population by T score analysis, patients with cystic fibrosis and COPD were similarly af- fected. In addition to low bone mineral density, a significant proportion of these patients with COPD and cystic fibrosis also had fractures. Glucocorticoid therapy was associated with lower bone density, more vertebral fractures, and biochemical evidence of decreased bone formation (lower serum osteo- calcin levels; “,“j). In view of the potential for further decline in bone density and more fractures after or- gan transplantation,“-~“’ we believe these results to be of great concern.
Our observations in adults with cystic fibrosis are consistent with other reports in the literature. In re- cent years the life expectancy of patients with cystic fibrosis has improved with patients often surviving into adulthood.“’ Osteoporosis and fractures are among t,he medical complications that have emerged in association with increased longevity.‘“,‘“,‘” Deficits in bone density have been reported in approximately 20% of children and adolescents with the dis- ease. “WJ” Reduced bone mass in adults with cystic fibrosis has been reported at the mid-radius, lumbar spine, hip, and whole body.‘“~“~‘J’~‘” Similar to our ob- servations, Bachrach et al demonstrated that the def- icits, which were most severe at the spine and hip, persisted despite the use of techniques that control for the smaller bone size of adults with cystic fibro- sis.‘”
The pathogenesis of osteopenia in cystic fibrosis is multifactorial and may include hypogonadism, chronic malnutrition, and glucocorticoid therapy. Delayed puberty, common in patients with cystic fi- brosis, may interfere with attainment of peak bone mass, while hypogonadism in adulthood may result in accelerated bone loss. Disease severity, l’~l(i~“u.“l low body mass index, which reflects overall health and nutritional status, W’ and vitamin D defi- ciency 15xsx3 may also c’duse osteopenia in cystic fibrosis patients. In this regard it is of interest that 36% of the patients with cystic fibrosis in this study had severe vitamin D deficiency and these patients also tended to have lower bone density measure- ments. In contrast, desite the well-known deleterious effect of glucocorticoids on bone, no relationship be- tween dose or duration of steroid therapy and bone mass was observed in our patients with cystic fibro- sis or in the literature.““‘”
The results of this study also suggest that osteo- porosis associated with COPD as well as various other forms of pulmonary disease is related to chronic corticosteroid therapy since, on average, pa- tients not on glucocorticoids tended to have reason- ably normal bone density. Few studies in the litera- ture address the issue of bone maSs in patients with COPD. Riaucho et al evaluated 44 men with COPD
September 1996 The American Journal of Medicine” Volume 101 267

OSTEOPOROSIS AND END-STAGE PULMONARY DISEASE/SHANE ET AL
268 September 1996 The American Journal of Medicine” Volume 101
who had never received glucocorticoids.“* They found no difference in vertebral fracture prevalence or bone density (measured by the metacarpal index) between the patients with COPD and a group of nor- mal men. Similarly, biochemical indices of mineral metabolism, including osteocalcin, parathyroid hor- mone, 1,25 dihydroxyvitamin D, and urinary hydrox- yproline excretion, were normal in patients and controls. However, similar to our results, 25hydro- xyvitamin D levels were low, indicating that the pa- tients were vitamin D deficient.
The prevalence of osteoporosis in these patients is of particular concern in that all of them had been accepted for lung transplantation. Osteoporosis and fractures are an unfortunate consequence of both liver and cardiac transplantation. The rate of fracture after liver transplantation ranges from 24% to 65%,‘-” particularly when there is preexisting osteoporosis such as is common in patients with primary biliary cirrhosis.” The prevalence rate of vertebral fracture after cardiac transplantation ranges from 18% to 50%.“-” We have recently reported that the inci- dence rate for fractures during the first year after cardiac transplantation was 54% for postmenopausal women and 29% for men.‘” In the same study we ob- served that older age and low pretransplant femoral neck bone mass were associated with an increased risk of fracture in postmenopausal women. In men, the rate of femoral neck bone loss aft.er transplan- tation rather than pretransplant bone density ap- peared to be related to fracture incidence. Since women comprised only 28% of the cardiac transplant recipients, but 66% of the patients on the lung trans- plant waiting list at our institution, our previous re- sults’“l raise the concern that the population of pa- tients awaiting lung transplantation are at particular risk for osteoporotic fractures.
The pathogenesis of fractures after organ trans- plantation is probably due, at least in part, to the immunosuppressive drugs used to prevent organ re- jection.” The majority of regimens include glucocor- ticoids, cyclosporine A, and azathioprine. Glucocor- ticoids, which are used in high doses early in the
posttransplant, course, cause bone loss and fractures by directly inhibiting bone formation and indirectly increasing bone resorption.‘” In addition, both cy- closporine A and tacrolimus (FK506) have been shown to cause severe bone loss in rodents.“‘,“” His- tologically, this bone loss is associated with mark- edly increased osteoclastic bone resorption and os- teoblastic bone formation. There are also data linking cyclosporine A to osteoporosis and high bone turnover in human subjects.“7 The combination of cyclosporine A, which increases bone resorption, and glucocorticoids, which inhibit bone formation, might be expected to have devastating consequences
on skeletal integrity. Given the strikingly high prev- alence of low bone mass and osteoporosis in the pa- tients in this study (65% at the lumbar spine, 78% at the femoral neck), it is likely that exposure to this particular drug regimen will result in marked pro- pensity for fracture after lung transplantation.
These results argue for routine skeletal evaluation of all patients with glucocorticoid-dependent pul- monary disease and all lung transplant candidates for osteoporosis and abnormal mineral metabolism. Such an evaluation should include bone densitome- try, spinal radiographs, and biochemical parameters of mineral metabolism, particularly 25-hydroxyvi- tamin D. Osteoporosis, when documented, should be treated aggressively so that the patients are in the best possible state when transplantation is accom- plished. General strategies should include rehabili- tation programs with weight-bearing exercise and supplementation with the recommended daily allow- ance of calcium (l,OOO-1,500 mg) and vitamin D (400 IU). Replacement of gonadal steroids in hypo- gonadal men and women is also reasonable. Estro- gen and progesterone have been shown tlo improve bone mass in postmenopausal women with estab- lished steroid-induced osteoporosis”” and should be considered if medically appropriate. Drugs that in- hibit bone resorption, such as calcitonin”“X4” or the bisphosphonates, “.” have been shown to prevent osteoporosis due to glucocorticoids and also to im- prove bone mass in patients with established steroid- induced osteoporosis.“” Given the long period of time between acceptance to the waiting list and transplantation, the status of these patient,s could be greatly improved by such interventions.
Finally, our results highlight the lack of att,ention given to the prevention of glucocorticoid-induced os- teoporosis by the medical community. Despite the well-known association of glucocorticoids and os- teoporosis, few patients were on any regimen to prevent this common complication of steroid ther- apy. In general, strategies to prevent ost.eoporosis are more successful than treatment of elstablished disease. Recent studies have established that gluco- corticoid-induced osteoporosis can be effectively prevented by calcitonin or cyclic etidronate therapy. The most opportune time to initiate such treatment is when glucocorticoid therapy is begun.
REFERENCES 1. Hosenpud JD. Nowck RJ, keen TJ, Keck B. Daily OP. The registry of the
international Society for Heart and Lung Transplantation: twelfth official report-
1995. J Heart Lung Transplant. 1995;14:805-815. 2. Shane E, Epstein S. lmmunosuppression and the skeleton. .rrends Endocri-
no/Metab. 1994;5:169-175. 3. Arnold JC, Hauser R, Ziegler R. et al. Bone dtsease after liverfransplantatlon.
Transplant Proc. 1994;24:2709-2710.

OSTEOPOROSIS AND END-STAGE PULMONARY DISEASE/SHANE ET AL
4. McDonald JA, Dunstan CR, Dilworth P, et al. Bone loss after liver transplan-
tabon. Hepatology. 1991;14:613-619. 5. Navasa M, Monegal A, Guanabens N, et al. Bone fractures in liver transplant
patrents. Br J Rheumatol. 1994;33:52-55. 6. Eastell R, Dickson ER, Hodgson SF, et al. Rates of bone loss before and
after liver transplantation in women with primary biliary cirrhosrs. Hepatology.
1991;14:296-300. 7. Porayko MK, Wlesner RH, Hay JE, et al. Bone drsease In liver transplant
recrplents: incrdence, trming and risk factors. Tramp/ant Pro<:. 1991;23:1462- 1465.
8. Meys E, Fontanges E, Fourcade N, Thomasson A, Pouyet M, Delmas PD.
Bone loss after orthotopic liver transplantation. Am J Med. 1994;97:445-450. 9. Rich GM, Mudge GH, Laffel GL, LeBoff MS. Cyclosporine A and prednlsone-
associated osteoporosis in heart transplant recipients. J Heart Lung Transplant.
1992;11:950-958.
10. Lee AH, Mull RL, Keenan GF, et al. Osteoporosis and bone morbidrty in
cardiac transplant recipients. Am J Med. 1995;96:35-41.
1 I. Shane E, Rivas M del C, Silverberg SJ, Kim TS. Staron RB, Bilezikian JP.
Osteoporosis after cardiac transplantatton. Am J Med. 1993;94:257-264. 12. Sambrook PN, Kelly PJ, Keogh A, et al. Bone loss after cardiac transplan-
tation: A prospective study. J Heart Lung Transplant. 1994;1.3:116-121, 13. Shane E, Rivas M, Staron RB, et al. Fracture after cardiac transplantation:
A prospective longltudtnal study. J Clin Endocrinol Metab. 1996;81:1740- 1746. 14. Bhudhlkanok GS. Lrm J, Marcus R, Harkins A, Moss f<B, Bachrach LK.
Correlates of osteopenia in patients with cystic frbrosls. Pediatrics.
1996;97:103-111. 15. Bachrach LK, Loutit CW, Moss RB, Marcus R. Osteoporosis in adults with
cystrc fibrosis. Am J Med. 1994;96:27-34. 16. Grey AB, Ames RW, Matthews RD, Reid IR. Bone mineral density and body
composltion in adult patients with cystic fibrosis. Thorax. 1993;4:589-593. 17. Chambers TJ. Phagocytosis and trypsin-reslstent glass adhesion by oste-
oclasts in culture. J Pathol. 1979;127:55-60. 18. Katzman DK, Bachrach LK, Carter DR, Marcus R. Clinical and anthropo-
metric correlates of bone mineral acquisitron in healthy adolescent girls. J Clin
Endocrinol Metab. 1991;73:1332-1339. 19. Eastell R, Cede1 SL, Wahner HW, Rtggs BI, Melton LJ Ill. Classrficatron of
vertebral fractures. J Bone Miner Res. 1991;6:207-215. 20. Brown JP, Delmas PD, Malaval L, Edouard C, Chapuy MC, Meunler PJ.
Serum bone Gla-protein: a specific marker for bone formation in postmeno-
pausal osteoporosis. Lancet. 1984;11:1091-1093.
21. Gundberg CM, Wilson PS, Gallop PM, Parfitt AM. Determination of osteo-
calcin in human serum: results wrth two kits compared with those by a well.
characterized assay. Clrn Chem. 1985;31:1720-1723. 22. Nussbaum SR, Zahradnik RJ, Lavigne JR, et al. Htghly sensrtive twosIte
lmmunoradlometric assay of parathyrin, and its clinical utrlity in evaluating pa-
bents with hypercalcemia. Urn Chem. 1987;33:1364-1367. 23. Silverberg SJ, Shane E, de la Cruz L, et al. Skeletal disease in primary
hyperparathyroldism. J Bone Mrner Res. 1989;4:283-291.
24. Kanis JA, Melton LJ, Christransen C, Johnston CC, Khaltaev N. Perspective.
The diagnosis of osteoporosis. J Bone Miner Res. 1994;9:1137-1141.
25. Peel N, Eastell R. Measurement of bone mass and turnower. Baillieres C/in
Rheumatol. 1993;7:479-498.
26. Lukert BP, Raisz LG. Glucocorticoid-induced osteoporosrs: pathogenesis
and management. Ann Intern Med. 1990;112:352-364. 27. Corey M, McLaughkn FJ, Williams M, Levison H. A comparison of survival,
growth, and pulmonary function in patients wrth cystrc fibrosis in Boston and
Toronto. J Clan Epidemiol. 1988;41:583-591. 28. Henderson RC, Specter BB. Kyphosis and fractures in children and young
adults with cystic fibrosis. J Pedratr. 1994;125:208-212.
29. Gibbens DT, Grlsanz V, Boechat MI, Dufer 0, Carlson ME, Wang C-l. Osteo-
porosis in cystic fibrosis. J Pediatr. 1988;113:295-300. 30. Mischler EH, Chesney PJ, Chesney RW, Mazess RB. Demineralization rn
cystic fibrosrs. Am J Dis Chrld. 1979;133:632-635. 31. Stead RJ, Houlder S. Agnew J, et al. Vitamin D and parethyroid hormone
and bone mineralization in adults with cystic fibrosis. Thorax. 1988;43:190- 194. 32. Hanley JG, McKenna MJ, Qurgley C, Freaney R, Muldowney FP, Fitzgerald
MX. Hypovitaminosis D and response to supplementation rn older patients with
cystic fibrosis. Quart J Med. 1985;219:377-385. 33. Hahn TJ, Squires AE, Halstead LR, Strominger DB. Recuced serum 25.
hydroxyvitamln D concentration and disordered mineral metabolism rn patients
with cystic fibrosis. J Pediatr. 1979;94:38-42.
34. Riaucho JA, Gonzalez Macias J, Del Arco C, Amado JA, Freijanes J, Anton
MA. Vertebral compresslons fractures and mineral metabolism rn chronic ob-
structive lung disease. Thorax. 1987;42:962-966. 35. Schlosberg M, Movsowitz C, Epstern S, lsmail F, Fallon M, Thomas S. The
effect of cyclosporin A adminlstration and its withdrawal on bone mineral me-
taboksm in the rat. Endocrinology. 1989;124:2179-2184. 36. Cvetkovic M, Mann GN, Romero DF, et al. The deleterious effects of long-
term cyclosporine A, cyclosporine G and FK506 on bone mineral metaboksm
in vivo. Transplantation. 1994;57:1231-1237. 37. Wilmlnk JM, Bras J, Surachno S, Heyst JLAM, Horst JM. Bone repair in
cyclosporin treated renal transplant patients. Transplant Proc. 1989;21:1492- 1494. 38. Lukert 8, Johnson BE and Robinson RG. Estrogen and progesterone re-
placement reduces glucocortlcord-induced bone loss. J Bone Miner Res.
1992;7:1063-1069. 39. Montemurro L, Schlraldi G, Fraioli P, Tosi G, Riboldi A, Rlzzato G. Preventton
of corticosteroid-induced osteoporosis with salmon calcitonii In sarcoid pa-
tients. Calcified Tissue Int. 1991;49:71-76. 40. Nrshleka T, Kurayama M, Yasuda T, Udagawa J, Matsmura SC, Ntlmi H. Nasal
administration of salmon calcitonin for prevention of glucocorticoid-induced os-
teoporosis in children with nephrosis. J Pediatrics. 1991;118:703-707. 41. Mulder H, Struys A. intermrttent cyclical etrdronate in the prevention of
cortrcosteroid-induced bone loss. Br J Rheumatol. 1994;33:3r18-350. 42. Reid IR, King AR, Alexander CJ, lbbertson HK. Preventron of Steroid-Induced
osteoporosrs with (3.amino 1-hydroxypropylidine)-l,l-bisphosphonate (APD).
Lancet. 1988;i:143-146. 43. Diamond T, McGiugan L, Barbagalla S, Bryant C. Cyclical etldronate plus
ergocalclferol prevents glucocorticoid-induced bone loss in lpostmenopausal
women, Am J Med. 1995;98:459-463.
September 1996 The American Journal of Medicine” Volume 101 269
Related Documents











