
Osteomyelitis Reşat ÖZARAS, MD, Prof. Infection Dept. [email protected] [email protected].
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
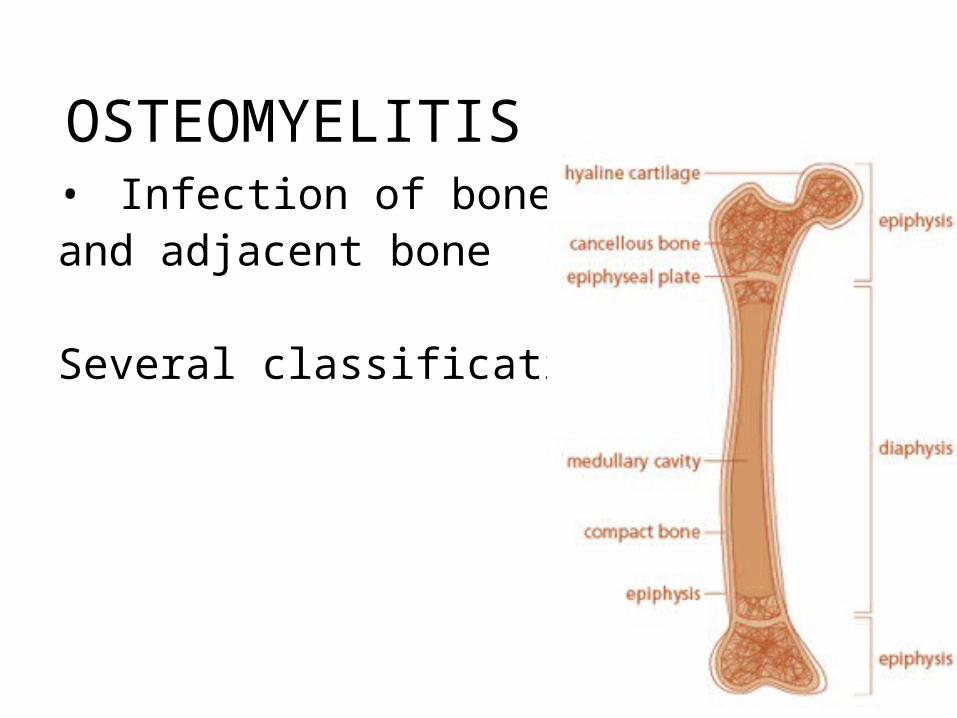
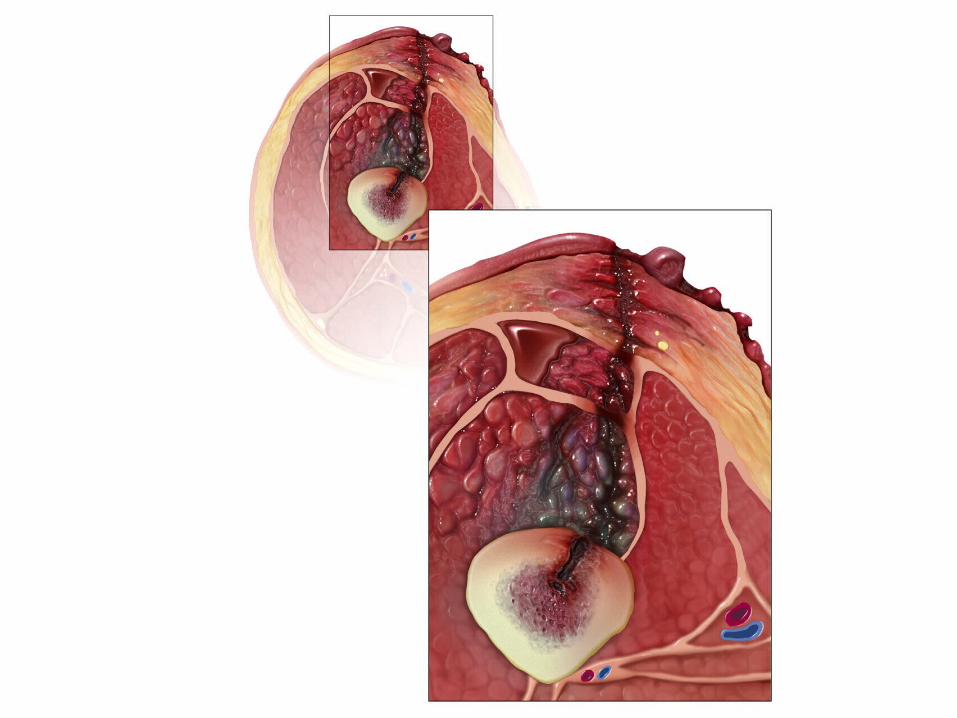
OSTEOMYELITIS• Infection of bone marrow and and adjacent bone Several classifications
The duration of the disease
• Acute osteomyelitis• Subacute osteomyelitis• Chronic osteomyelitis
The way of occurence
1 - Hematogenous osteomyelitis2 – Osteomyelitis secondary to direct transmission
- Any vascular disease may/not associate 3 - Chronic osteomyelitis (necrotic bone)
Anatomical classification
• Stage 1: medullary osteomyelitis• Stage 2: superficial osteomyelitis• Stage 3: localized osteomyelitis• Stage 4: diffuse osteomyelitis
SYSTEMIC AND LOCAL FACTORS Systemic Local
Malnutrition Chronic lymphedema Renal, hepatic failure Venous failure Diabetes mellitus Vascular insufficiency Chronic hipoxia Arteritis Alcohol and/or tobacco use Tissue scar Malignant disorders Radiation fibrosis Advanced age Neuropathy Immune suppression HIV/AIDS

ETIOLOGY
• Babies (<1 year)• Group B streptococci • S. aureus• E. coli
• Children (1 - 16 years)• S. aureus• S. pyogenes• H. influenzae
• Adult(> 16 years)• S. epidermidis• S. aureus• P. aeruginosa
EPIDEMIOLOGY
• Acute hematogenous osteomyelitis: a disorder of childhood period
• A trend to increase: traffic accidents, increasing rates of orthopedic interventions.
• Adults– Vertebtal osteomyelitis (Spondylodiscitis)

CLINICAL FEATURESAcute Hematogenous Osteomyelitis - Systemic disorder - No structural bone changes - A history of less than 10 days - No previous episodes
Subacute Hemotogenous Osteomyelitis -Systemic disorder (not as severe as the acute form) -Bone changes -A history of more than 10 days - No previous episodes
Chronic osteomyelitis -Systemic disorder may/not associate -Bone changes - There is/are previous episode(s).
Clinical Features• Depends on the way of development (hematogenous,
direct, from adjacent tissues), patient's characteristics and the period of the disorder
• Hematogenous osteomyelitis – fever, fatigue, restlessness – Tenderness, pain, and edema on the affected site – Decreased mobility of the affected extremity – Muscle spasms
• From adjacent tissue; pain, redness, swellings, a draining sinus from the site of trauma, wound, or operation
• Dorsal/back pain in vertebral osteomyelitis .
RADIOLOGICAL FINDINGS
Plain X-ray;
• Diagnosis and the course of the disease • Increase in density of the surrounding soft
tissues (first 10 days)• Periostal reaction (after 10 days)• Bone loss in subacute period

Bone scan
• For early diagnosis
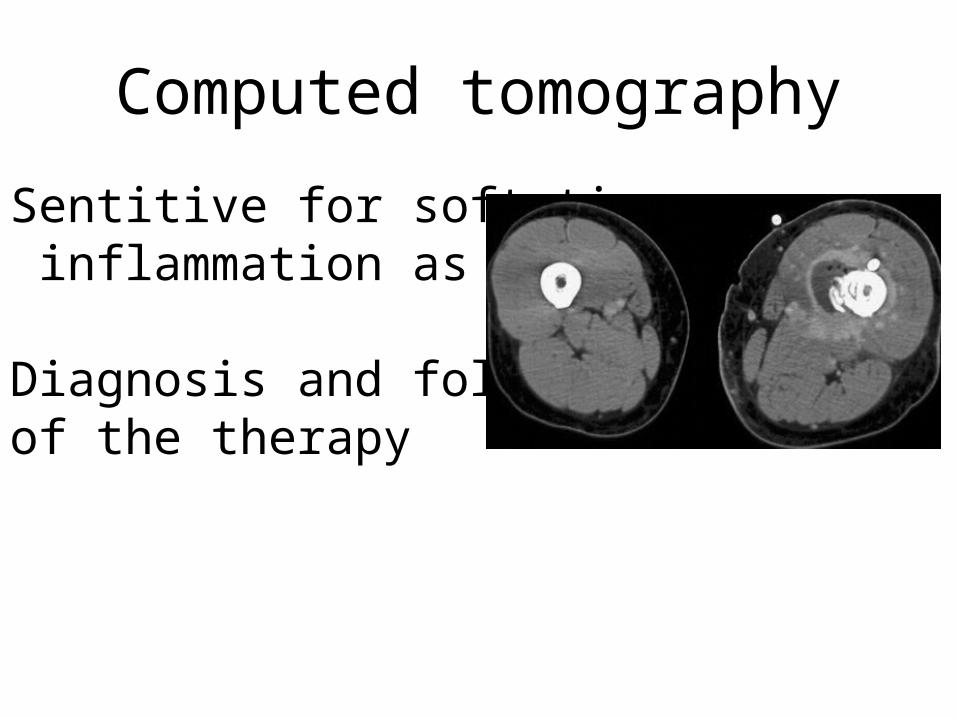
Computed tomography
Sentitive for soft tissue inflammation as well.
Diagnosis and follow-up of the therapy
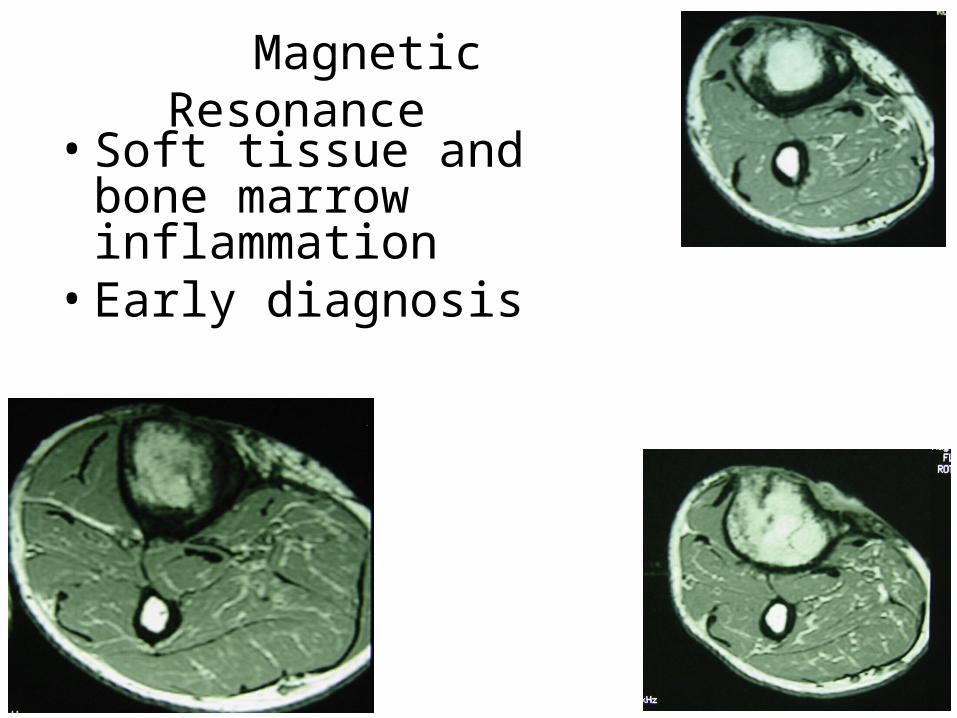
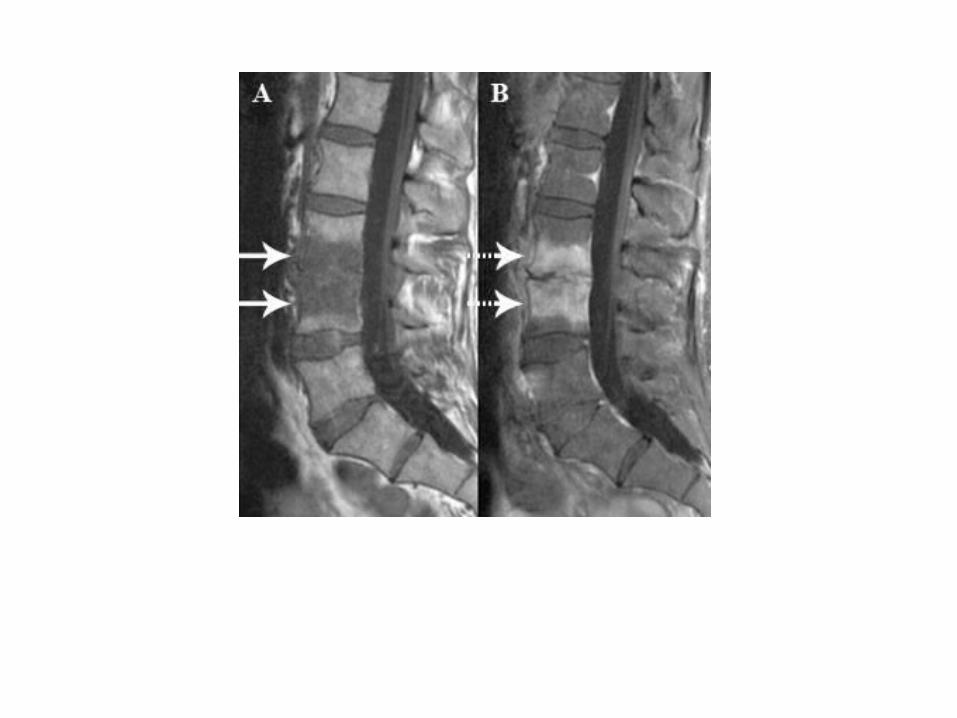
Magnetic Resonance • Soft tissue and bone marrow
inflammation• Early diagnosis
Differential Diagnosis• Rheumatic fever• Cellulitis• Ewing’s sacroma • Septic arthritis• Osteosarcoma• Eosinophilic granuloma• Thrombophlebitis
Vertebral Osteomyelitis
• Frequent etiology: – S. aureus, – M. tuberculosis, – Brucella
• Gram-negative bacilli (Gastrointestinal or urinary system)• Postoperative • Pain and disability• May be indolent and fever may not be
seen
Tx
• Antibiotics • Surgery• Underlying disorder
Meticilin-sensitive Staph. → Cefazolin or Sulbactam/ampicillin
Meticilin-resistant Staph →Vancomycin or teicoplanin
Brucella → Rifampin+doxycycline
Tuberculosis → INH+RIF+PZA+EMB
Antibiotics

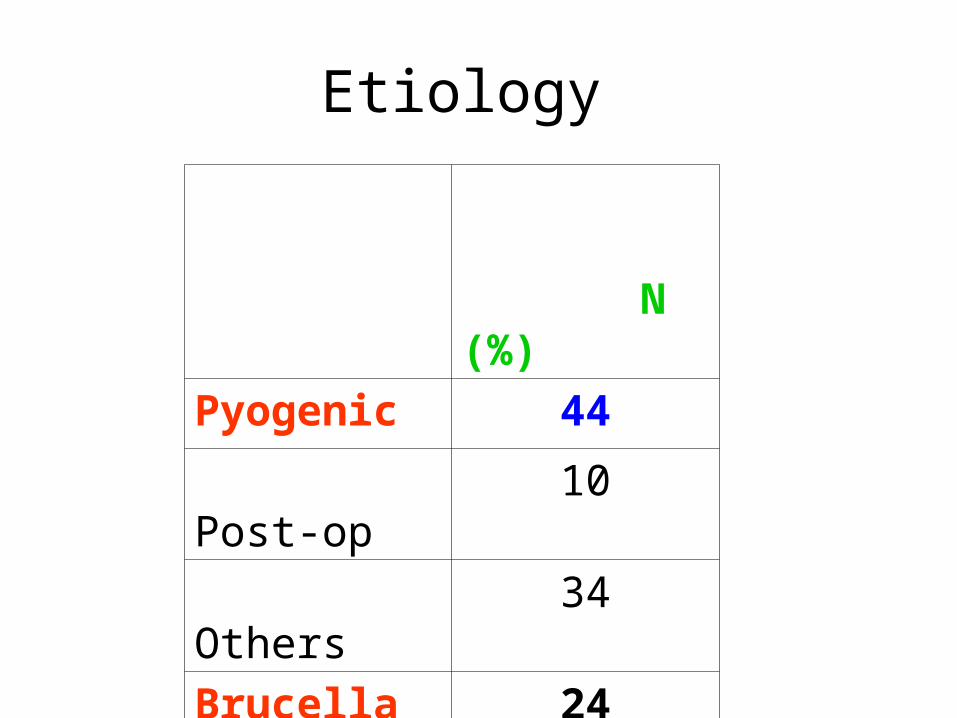
Etiology
N (%)
Pyogenic 44
Post-op 10
Others 34
Brucella 24
Tuberculosis 32
Total 100
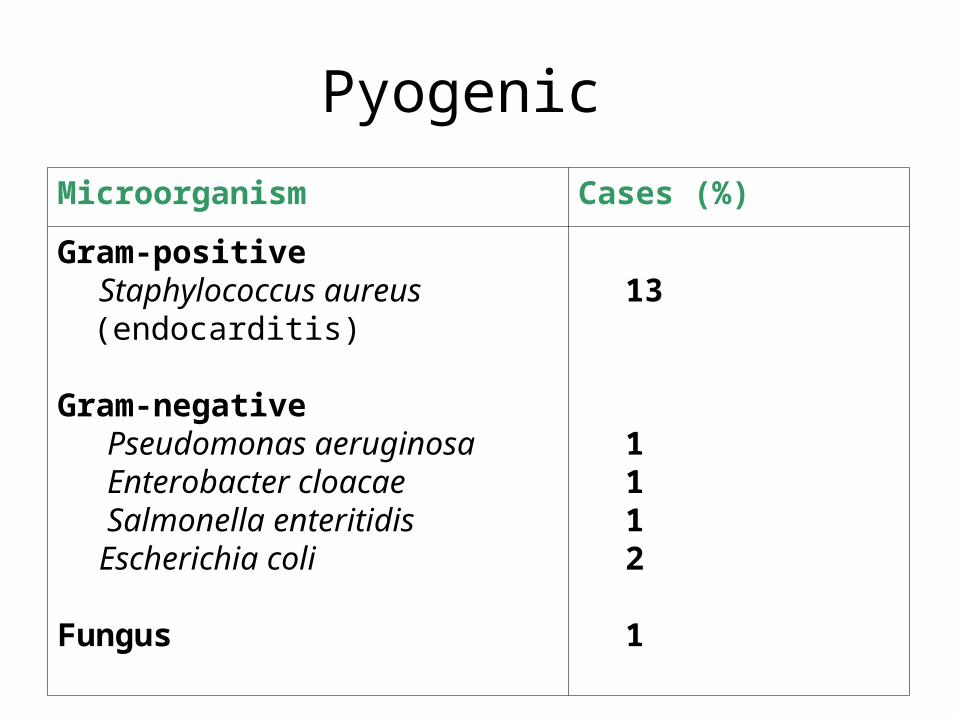
Pyogenic
Microorganism Cases (%)
Gram-positive Staphylococcus aureus
(endocarditis)
Gram-negative Pseudomonas aeruginosa Enterobacter cloacae Salmonella enteritidis Escherichia coli
Fungus
13
1112
1
Children: Acute hematogenousAdult: Chronic (hematogenous---from adjacent tissues…
Related Documents











