Original article Osteomyelitis: clinical update for practical guidelines Ercole Concia a , Napoleone Prandini b , Leo Massari c , Franco Ghisellini d , Vincenzo Consoli e,* , Francesco Menichetti f and Elena Lazzeri g Bone infections represent a diagnostic or therapeutic challenge for the infectivologist, orthopaedic surgeon, radiologist and nuclear medicine physician. Staphylococcus aureus is the major bacterium responsible for bone infections although Mycobacterium tuberculosis is emerging as an infectious agent in Italy because of immigration from Africa and Asia. Osteomyelitis requires long and expensive antibiotic treatment, including rifampicin administered parenterally for several weeks and the use of antimicrobial-impregnated cement in prosthesis substitution. Sometimes it is necessary to carry out surgical debridement of a necrotic bone or the consolidation of compromised bones and joint prosthesis implants. Radiographs and bone cultures are mainstays for the diagnosis of bone infections but are often useless in the lengthy management of these patients. Diagnosis of skeletal infections still includes conventional radiography but magnetic resonance imaging is essential in haematogenous and spinal infections. Bone scans are still useful in acute osteomyelitis whereas scintigraphy using labelled white blood cells is preferred in infections of peripheral bone segments or joint prosthesis. In the axial skeleton a combination of an agent for detecting inflammation ( 67 Ga citrate) and a metabolic agent ( 99m Tc-methylene diphosphonate) enables an infection and an area of increased metabolic activity to be distinguished. [ 18 F]Fluorodeoxyglucose positron emission tomography, where available, has a significant impact in the study of infections using radionuclides: high-resolution tomographic images represent an effective alternative to gallium in the assessment of inflammation of spine lesions but a comparison with morphological examinations (computed tomography or magnetic resonance imaging) is essential. Nucl Med Commun 27:645–660 c 2006 Lippincott Williams & Wilkins. Nuclear Medicine Communications 2006, 27:645–660 Keywords: osteomyelitis, spondylodiskitis, prosthesis-related infections, radionuclide imaging, antibiotics, antitubercular, arthroplasty, replacement a Istituto di Malattie Infettive e Tropicali, Universita ` di Verona, Italy, b Struttura Complessa di Medicina Nucleare, Azienda Ospedaliero-Universitaria, Ferrara, Italy, c Clinica Ortopedica e Traumatologica, Universita ` di Ferrara, Italy, d Divisione Ortopedica Ospedale Maggiore, Novara, Italy, e Clinica Ortopedica 3, Azienda Ospedaliero-Universitaria, Pisa, Italy, f Malattie Infettive and g Istituto di Medicina Nucleare, Universita ` degli Studi di Pisa, Italy. Correspondence to Dr Napoleone Prandini, Struttura Complessa di Medicina Nucleare, Azienda Ospedaliero Universitaria, Corso Giovecca 203, 44100 Ferrara, Italy. Tel: + 39 0532 236387; fax: + 39 0532 237553; e-mail: [email protected] Received 22 June 2005 Accepted 5 May 2006 Introduction Bone is normally highly resistant to infection, which can occur after large inoculums, trauma or in the presence of metal hardware or in the case of immunocompromised hosts. Infection associated with prosthetic joints is typically caused by microorganisms growing in bio film into organized communities. Bio film protects bacteria from antimicrobial agents and host immune responses. Staphylococcus aureus is the major cause of bone infections: microorganisms adhere to bone and to devices surgically implanted by expressing bone matrix receptors and a phenotypic resistance to antimicrobial treatment [1]. Mycobacterium tuberculosis is an emerging agent of vertebral column infections in Italy as a consequence of immigra- tion from Africa and Asia. Early and specific treatment of osteomyelitis, before extensive bone destruction or necrosis, produces the best results. The identification of the causative microorganisms is essential for specific antibiotic treatment but evidence from swabs of ulcers or fistulae is often misleading. Infections of joint prostheses, where bio film microorgan- isms are involved, should be treated with a combination of antibiotics, which must include rifampicin. Surgery is usually unnecessary in acute haematogenous osteomyelitis and in diskitis but a combined antimicrobial and surgical approach should be common after injury with an open fracture or in infections associated with joint prostheses. Surgical treatments include debridement with retention of the prosthesis, or two-stage exchange with re-implantation of the new prosthesis delayed for a variable period of time. The use of antimicrobial- impregnated cement is suggested to correct length and allows partial joint mobility. The diagnosis of skeletal infections includes a variety of imaging methods, but conventional radiography is still * In memory of Professor Vincenzo Consoli–March 2006. 0143-3636 c 2006 Lippincott Williams & Wilkins Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Osteomyelitis Clinical Practice Guidelines
Mar 22, 2016
Concia E, Prandini N, Massari L, et al. Osteomyelitis: clinical update for practical guidelines. Nuclear Medicine Communications. 2006;27(8):645.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Original article
Osteomyelitis: clinical update for practical guidelinesErcole Conciaa, Napoleone Prandinib, Leo Massaric, Franco Ghisellinid,Vincenzo Consolie,*, Francesco Menichettif and Elena Lazzerig
Bone infections represent a diagnostic or therapeuticchallenge for the infectivologist, orthopaedicsurgeon, radiologist and nuclear medicine physician.Staphylococcus aureus is the major bacterium responsiblefor bone infections although Mycobacterium tuberculosis isemerging as an infectious agent in Italy because ofimmigration from Africa and Asia. Osteomyelitis requireslong and expensive antibiotic treatment, includingrifampicin administered parenterally for several weeks andthe use of antimicrobial-impregnated cement in prosthesissubstitution. Sometimes it is necessary to carry outsurgical debridement of a necrotic bone or theconsolidation of compromised bones and joint prosthesisimplants. Radiographs and bone cultures are mainstays forthe diagnosis of bone infections but are often useless inthe lengthy management of these patients. Diagnosis ofskeletal infections still includes conventional radiographybut magnetic resonance imaging is essential inhaematogenous and spinal infections. Bone scans are stilluseful in acute osteomyelitis whereas scintigraphy usinglabelled white blood cells is preferred in infections ofperipheral bone segments or joint prosthesis. In theaxial skeleton a combination of an agent for detectinginflammation (67Ga citrate) and a metabolic agent(99mTc-methylene diphosphonate) enables an infection andan area of increased metabolic activity to be distinguished.
[18F]Fluorodeoxyglucose positron emission tomography,where available, has a significant impact in the studyof infections using radionuclides: high-resolutiontomographic images represent an effective alternative togallium in the assessment of inflammation of spine lesionsbut a comparison with morphological examinations(computed tomography or magnetic resonance imaging) isessential. Nucl Med Commun 27:645–660 !c 2006Lippincott Williams & Wilkins.
Nuclear Medicine Communications 2006, 27:645–660
Keywords: osteomyelitis, spondylodiskitis, prosthesis-related infections,radionuclide imaging, antibiotics, antitubercular, arthroplasty, replacement
aIstituto di Malattie Infettive e Tropicali, Universita di Verona, Italy, bStrutturaComplessa di Medicina Nucleare, Azienda Ospedaliero-Universitaria, Ferrara,Italy, cClinica Ortopedica e Traumatologica, Universita di Ferrara, Italy, dDivisioneOrtopedica Ospedale Maggiore, Novara, Italy, eClinica Ortopedica 3, AziendaOspedaliero-Universitaria, Pisa, Italy, fMalattie Infettive and gIstituto di MedicinaNucleare, Universita degli Studi di Pisa, Italy.
Correspondence to Dr Napoleone Prandini, Struttura Complessa di MedicinaNucleare, Azienda Ospedaliero Universitaria, Corso Giovecca 203, 44100Ferrara, Italy.Tel: + 39 0532 236387; fax: + 39 0532 237553;e-mail: [email protected]
Received 22 June 2005 Accepted 5 May 2006
IntroductionBone is normally highly resistant to infection, which canoccur after large inoculums, trauma or in the presence ofmetal hardware or in the case of immunocompromisedhosts. Infection associated with prosthetic joints istypically caused by microorganisms growing in bio filminto organized communities. Bio film protects bacteriafrom antimicrobial agents and host immune responses.Staphylococcus aureus is the major cause of bone infections:microorganisms adhere to bone and to devices surgicallyimplanted by expressing bone matrix receptors and aphenotypic resistance to antimicrobial treatment [1].Mycobacterium tuberculosis is an emerging agent of vertebralcolumn infections in Italy as a consequence of immigra-tion from Africa and Asia.
Early and specific treatment of osteomyelitis, beforeextensive bone destruction or necrosis, produces the best
results. The identification of the causative microorganismsis essential for specific antibiotic treatment but evidencefrom swabs of ulcers or fistulae is often misleading.Infections of joint prostheses, where bio film microorgan-isms are involved, should be treated with a combination ofantibiotics, which must include rifampicin.
Surgery is usually unnecessary in acute haematogenousosteomyelitis and in diskitis but a combined antimicrobialand surgical approach should be common after injury withan open fracture or in infections associated with jointprostheses. Surgical treatments include debridementwith retention of the prosthesis, or two-stage exchangewith re-implantation of the new prosthesis delayed for avariable period of time. The use of antimicrobial-impregnated cement is suggested to correct length andallows partial joint mobility.
The diagnosis of skeletal infections includes a variety ofimaging methods, but conventional radiography is still*In memory of Professor Vincenzo Consoli–March 2006.
0143-3636 !c 2006 Lippincott Williams & Wilkins
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

necessary at presentation of acute osteomyelitis. It is ofless importance during follow-up or in secondary andchronic infections. Ultrasonography and computed tomo-graphy (CT) are very useful for guiding needle biopsies inclosed infections of either soft tissues or bones. CT andmagnetic resonance imaging (MRI) have excellentresolution and can reveal oedema and any periostealreaction or soft-tissue involvement: MRI is the preferreddiagnostic imaging method for spinal osteomyelitis, but isnot suitable for all patients and has certain limitations inthe presence of metallic implants [2].
Nuclear medicine imaging procedures to evaluate osteo-myelitis include three-phase bone scans, the use ofleukocytes (white blood cells, WBCs) labelled with either99mTc-hexamethylpropylene amine oxime (99mTc-HMPAO) or 111In-oxime, and the use of 2-[18F]fluoro-2-deoxy-D-glucose (18F-FDG) positron emission tomo-graphy (PET) and 67Ga citrate [3–5]. The three-phasebone scan is the test of choice in evaluating acuteosteomyelitis and doubtful diskitis but the specificity ofthis method falls in secondary osteomyelitis. The findingof increased metabolic activity in osteomyelitis isindistinguishable from post-traumatic injury or followingsurgery or cancer.
WBCs accumulate at sites of infection and in bonemarrow. The combination of the 111In-oxime WBC scanwith a 99mTc-sulfur colloid bone marrow scan is con-sidered the ‘gold standard’ method for the study ofinfections of hip prostheses but can be also helpful in thestudy of peripheral bone segments. Three-phase 99mTc-HMPAO WBC scintigraphy is widely used in Italy as ahelpful alternative to the combined method of WBC/sulfur colloid: a WBC scan is less sensitive for imagingthose bones where red marrow is present (i.e., the axialskeleton and spine). In these cases, by combining 67Gacitrate and bone scintigraphy it is possible to distinguishthe activity of secondary vertebral osteomyelitis fromother causes of increased bone metabolism. 18F-FDGPET, where available, has a significant impact in theradionuclide study of infections: the high-resolutiontomographic images represent an effective alternative togallium in the assessment of inflammation of spinallesions but a comparison with morphological examina-tions (CT or MRI) is essential.
The pathophysiology of osteomyelitisOsteomyelitis is an inflammatory suppurative process ofthe bone marrow in which both the endosteum andperiosteum participate actively whereas the trabeculaeand Haversian system participate passively with necrosisand osteolysis. Bone is a tissue that is resistant tobacterial colonization and, in effect, to cause a boneinfection, other negative events must occur such astraumas, the presence of foreign bodies, prostheses or an
inoculation of aggressive bacteria or other bacteria thatgenerally have characteristics that inherently favourimplants; characteristics of adherence, for example [6].
Classification of osteomyelitisThe classification by Waldvogel et al. [7] is rather old, butstill topical, and is based on the genesis of osteomyelitis(haematogenous or secondary) and on the modality ofonset. Acute haematogenous osteomyelitis symptoms lastno more than 10 days. The chronic form is by far the morefrequent and includes all the remaining cases (Table 1).The classification by Cierny et al. [8] is more recent andrelevant as it proposes the anatomical and histologicalsubdivision of osteomyelitis (medullary, superficial, lo-cated or diffused) and introduces the important conceptof host immunocompetence, which is highly relevantregarding the onset and diffusion of infections (Table 2).
Haematogenous osteomyelitisHaematogenous osteomyelitis affects children in 85% ofall cases and it often originates from unknown primaryfoci (nasopharynx) via direct inoculation but can also becontiguous. The most affected group varies from 2 to5 years of age and the elective location is the lower limbs(femur 27%, tibia 22%). The incidence of osteomyelitis isbetween 1:1000 and 1:20 000 and mortality reached 50%in the pre-antibiotic era. Nowadays, mortality throughosteomyelitis is almost zero. The primary focus is not
Table 1 Classification of osteomyelitis according to Waldvogel etal. [7] (modified)
K Haematogenous osteomyelitisK Secondary
Infection next to focal pointWith vascular impairmentWithout vascular impairment
K AcuteSuppuration and oedema, vasal congestion and small vessel thrombosisVascularization is compromised if nearby soft tissue becomes involvedIf haematic and periosteal flow rates are reduced, large areas of dead orisolated tissue form
K ChronicA knot of necrotic bone tissue or scar tissue surrounded by ischaemic softtissue
Table 2 Classification of osteomyelitis according to Cierny et al.[8]
Anatomical typeI Medullary osteomyelitisII Superficial osteomyelitisIII Localized osteomyelitisIV Diffuse osteomyelitis
Physiological classA–Host Good immune system and deliveryB–Host Compromised locally (BL) or systemically (BS)C–Host Requires suppressive or no treatment; minimal dis-
ability; treatment worse than disease; not a surgicalcandidate
Clinical stageType+ class =Clinical stageExample Stage IV BS osteomyelitis = a diffuse lesion in a
systemically compromised host
BL: local host compromised; BS: sistemic host compromised.
646 Nuclear Medicine Communications 2006, Vol 27 No 8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

found in 70% of cases and even when present, may be farfrom clear. It can be from a simple boil, an infected ulcer,a urinary tract infection or other soft-tissue focalinfection. In adults, the infection locations are often inthe vertebrae. S. aureus is the most frequent microorgan-ism but in the 2–3 year age group, streptococci such asHaemophilus influenzae can predominate. In haematogenousosteomyelitis, Gram-negative microorganisms (Escherichiacoli, Klebsiella, Salmonella and Proteus) are found, and insome immunocompromised patients (e.g., drug addicts)Pseudomonas aeruginosa and, occasionally, Candida aspergillus[9,10].
Secondary osteomyelitisSecondary osteomyelitis includes post-traumatic osteo-myelitis after compound fractures involving a mass ofbacteria, the nature of which depends on the environ-ment in which contamination occurred. Post-operativeosteomyelitis partly includes the above for open-fracturereduction but also other operations on bones such as thecranium, vertebral column and sternum, and for prosthe-sis implants and ozone therapy.
Contiguous osteomyelitisContiguous osteomyelitis includes, besides the classicaldiabetic foot, osteomyelitis of the heel following un-recognized traumas (puncture and scratch injuries) andosteomyelitis of the jaw following radiotherapy forneoplasms of the head and the neck.
S. aureus is the most frequent microorganism of post-surgical osteomyelitis and it is multi-resistant to anti-biotics: in Italy, the global incidence of methicillin-resistant staphylococci exceeds the 50% of the isolatedbacteria. Nevertheless, the surgical prophylaxis guide-lines still foresee the use of cephazolin, which is noteffective over two of these infections. It should thereforebe necessary for each hospital to assess its own incidenceof methicillin-resistant infections, using glycopeptides insurgical prophylaxis only when the incidence of thesemicroorganisms exceeds 50%. Hence, the indiscriminateuse of teicoplanin and vancomycin can be avoided.
Periprosthetic osteomyelitisPeriprosthetic osteomyelitis is the new osteomyelitis.Nowadays, the elderly insist on more mobility and anever-increasing number of prostheses are being fitted; atpresent there are more than 600 000 in the USA (Table3). Post-operative infections of prosthetic joints havedecreased from 5.9% (± 1.8) in the 1970s to 1.2 (± 0.5)since 2000 [11]. In Italy, between 45 000 and 50 000prosthetic hip joints and between 9000 and 10 000 kneesare fitted each year. Although the incidence of hipprosthesis infections in 1999 was approximately 1.5% peryear for new implants, this incidence tripled in re-implantation cases even if the re-implant was not
required for a previous infection of the prosthesis. Wecan therefore estimate that 10–15 significant infectionswill develop in each 100 prosthetic operations over a 10-year period, which is the average life span of a prosthesis.The orthopaedic surgeon’s worst enemy is still S. aureus,even if other clinically significant bacteria such as P.aeruginosa and S. epidermidis appear [12,13].
The early forms of periprosthetic osteomyelitis developin the first month, while the delayed form arises in thefirst year following surgery and the late form can arisemany months or years after the initial event. Thesymptoms are pain, fever, oedema and fistula.
Table 4 gives a classification of prosthesis infections. Inprecocious prosthetic hip infections, infection tends toset in within a month of surgery and stems from bacterialactivity during surgery, or in the immediate post-operative period, around the operation site, then developsin the periprosthetic soft tissues with little involvementof the bone–prosthesis interface. This means that theinfection is located within the surgical access area and toidentify it we can use a method that thoroughly studiessoft tissues. If diagnosed early, these infections have agood prognosis and save the use of another implant.
In delayed or late infections that have occurred from 2 to15months after an operation, the rejection of, or reactionto, a foreign body (the prosthesis) can offer an excellentpoint of attack for bacteria that lodge in the body. Duringthe course of 1 day, there can be episodes of bacteraemiain the blood which are easily overcome by healthysubjects. In patients with prosthesis, however, if thebacteraemia is severe, perhaps because the patient has a
Table 3 Incidence of device-associated infections in the UnitedStates
Device Usage/year Infection risk (%)
Joint prostheses 600 000 1–3Fracture fixators 2 million 5–10Dental implants 1 million 5–10
Table 4 Classification of prosthesis infections
Onset of infection Infecting organism
Precocious ( < 1month) Staphylococcus aureusStaphylococcus coagulase-negativeAerobic Gram-negative bacteria
Delayed (2–12months) Staphylococcus coagulase-negativeSkin bacteria (S. epidermidis)
Late ( >12months) Staphylococcus aureus (methicillin-resistant)Staphylococcus coagulase-negative
Skin bacteria (S. epidermidis)Anaerobes
Streptococcus speciesEscherichia coli
Osteomyelitis: clinical update for practical guidelines Concia et al. 647
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

dental abscess or a chronic urinary tract infection,osteomyelitis develops on the prosthesis. This is alsodue to the presence of a reactive phenomenon to the useof polyethylene in prostheses. This results in a subse-quent reaction with the appearance of periprostheticosteolysis or of less vascularized centres and the possibleoccurrence of circulating bacterial colonies. In thisinfection, the seat is typically the prosthesis/bone inter-face, with the soft tissue involved secondarily. In thiscase, the diagnostic approach must be to use a methodthat allows this to be carefully studied. Prognosis in thesecases is rather poor and the nuclear physician andradiologist must therefore be fully aware of the patient’sclinical background and have all the relevant laboratorydata [14–16].
Infections of the vertebral columnInfections of the vertebral column are haematogenousinfections but primarily strike adults over 50 years of age.Drug addicts are an exception and are particularlyexposed to infections of the vertebral column just likediabetics and dialysis patients. The infections present asspondylitis or vertebral osteomyelitis, diskitis and sec-ondary diskitis where the infection shows an effect eitherby itself or in association with adjacent vertebrae andintervertebral disks. Diskitis is a specific or non-specificbacterial infectious process (very occasionally mycotic) oftwo or more adjoining vertebrae and of the respectiveintervertebral disk. The infection sometimes spreads tothe surrounding soft tissue. Backwards extension of theinfection can result in an epidural or subdural abscess orin meningitis, whereas forward and/or lateral extensioncan result in para vertebral, retropharyngeal, mediastinalor retroperitoneal abscesses [6,17,18].
Infections of the vertebral column can be divided intospontaneous and iatrogenic forms, these last due toinvasive manoeuvres or to surgical interventions. Thespontaneous forms, which are supported by an arterialhaematogenous dissemination in almost all cases, areunspecific bacterial or mycotic and they represent the 2–4% of all vertebral osteomyelitis. The source of infectioncan be presented both from venous inoculation and fromdifferent kinds of sources (e.g., genitourinary apparatus,cutaneous or subcutaneous, respiratory, dental) or fromvascular devices. In 24–37% of cases, the source ofinfection remains unknown. The most susceptiblevertebrae are the lumbar (45%), followed by the dorsal,above all the inferior, (35%) and the cervical (20%). Agreater incidence of the cervical forms has been noticedamong the drug addicts. S. aureus is the most frequentlyisolated agent (55–85% of cases), followed by coagulase-negative staphylococci, enterobacterias (Salmonella spp,E. coli, Klebsiella spp, Serratia spp), P. aeruginosa (frequentamong drug addicts) and Candida (among drug addictsand in infections of vascular devices) [19,20].
Spontaneous specific diskitisSpontaneous specific diskitis is represented by vertebraltuberculosis or Pott’s disease supported by a haemato-genous dissemination originating from the lung or fromother lymph nodes or from genitourinary infections, oftenwithin disseminated tuberculosis. Vertebral infections areincreasing, especially among immigrants from Romania,India, Sri Lanka and Africa, as well as in patients over80 years of age who have compromised immune systems.The tubercular infection begins from the anterior part ofthe vertebral body and usually involves the subcondralregion, spreading then to the cortical region and to theadjacent disk. It can result in vertebral abscessesinvolving the ileopsoas muscles. The classic symptoma-tology of spontaneous specific diskitis is represented by‘back pain’ with accentuation of the painful symptoma-tology in the passage from the clino to the orthostaticposition and from the seated to the erect position.Because of the insidious symptomatology, whose progresscan last weeks or months, the moment of the diagnosis itis often delayed (it may be between 3weeks and3months). The fever, usually around 37.51C, is presentin 50% of patients. Laboratory data show a modestleukocytosis in 50% of subjects while erythrocytesedimentation rate (ESR) and C-reactive protein (CRP)are usually increased [19,21].
Iatrogenic diskitisIatrogenic diskitis follows direct inoculation of micro-organisms after spinal anaesthesia, chemonucleolysis andlocal infiltrations with analgesic purpose. Above all, itfollows surgical interventions for slipped disk, spondylo-lysis and spondylolisthesis. Also, in such cases, staphylo-cocci play the principal aetiological role, with theprevalence of coagulase-negative strains. The painfulsymptomatology, similar to that in spontaneous diskitis,involves the site of the intervention and can sometimesbe associated with subcutaneous infections noticeableduring physical examination. The onset of the painfulsymptomatology can vary from a few days to 2–3monthsfrom the invasive or surgical manoeuvre. The fever is notconstant, while an increase of ESR and CRP is typical,with or without variations in granulocytes [22].
Assessment of the diseaseSymptoms of osteomyelitisThe symptoms of osteomyelitis are variable: in the typicalform, fever, pain, motor limitations and local inflamma-tion or septicaemia, are found, as is usual amonginfectious diseases. A bone infection leads to tissuedestruction, which can result in the functional loss of theinvolved bone and the surrounding soft tissues [23].Results of laboratory tests (CRP, ESR, neutrophilia) areused in the diagnosis of the infection, but a precisediagnosis and effective therapy cannot be formulatedunless the microorganism is isolated and the cultureexamined [6,7,17,18].
648 Nuclear Medicine Communications 2006, Vol 27 No 8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Onset of infection is variable: a thick inoculation ofvirulent bacteria generates an acute infection but a thickcontamination in a guest immunocompetent patientproduces a faint infection. In these cases, the appearanceis delayed, even after years: there are often fewer virulentbacteria but with adhesive abilities. A third possibility isthat there is a low intra-operating contamination, withlow virulence of the organism, and it can be easy tomaintain under controlled conditions. Possibly, it alsoexists in a haematogenous manner, it is not frequent andis a consequence of oral, endoscopic or urinary surgicalinterventions. The infection should be prevented byeffective antibiotic prophylaxis before the intervention.
Radiological investigationIn the initial phases of the haematogenous osteomyelitis,we find a medullar inflammation characterized by thehyperaemia, the oedema, the leukocytes infiltration andthe purulent transformation. In this phase the radiologicaldiagnosis is limited because there are no definite signs ofinfection in the first 2 weeks after onset. There are somespecific signs such as soft-tissue oedema and thedisappearance of the fascial levels, which are easily foundby nuclear medicine techniques and MRI [24,25]. Theabscess of Brodie is a unique focal infection, with chronicevolution, generally located at the proximal metaphysis ofthe tibia or femur. X-rays show an oval osteolytic area thatis better seen by MRI with spin-echo T2-weightedsequences and a heterogeneous signal hyperintensity.The stir sequences of the MRI provoke the suppressionof the fat, and they confirm the presence of oedema andthe involvement of the soft tissues [26,27].
The infection can spread to the cortical with lifting of theperiosteum and interruption of the vascular support.X-ray examination shows osteopenia and a worm-holeaspect of the bone with a meaningful re-absorption up tothe osteolysis. The consequence is bone death, which canlead to alterations such as swelling of the surroundingskeletal soft tissues, periosteitis, endosteitis and thedisappearance of the medullar canal up to the lamellarosteonecrosis and thickened bone. In the following phase,sequestration with clear demarcation of necrotic bonefrom healthy bone can be seen; this is due to thephenomenon of osteoclastic demolition. After thesequestrum, a chronic process is followed with theoverproduction of bone and therefore a demarcation fromthe surrounding bone. Conventional X-rays show osteo-lytic areas of infection delimited by a diffusely andheterogeneously thickened bone. The MRI spin-echoT1-weighted sequences demonstrate sequestration ofbone and the activity of the infection. If a patientreceives gadolinium, the MRI shows hyperaemia, definiteexpression of the process activity [28–30]. The CTshowsvery well the partly corpuscular swelling of the softtissues around bones and joints.
Radionuclide imagingRadionuclide imaging is usually employed after theradiological investigations, in the diagnosis of haemato-genous osteomyelitis and of soft-tissue infections. Thethree-phase bone scan with 99mTc-disphosphonatesshows an increase of bone perfusion and of thesurrounding soft tissues in the dynamic and blood poolimages. In delayed images bone uptake appears blurred inthe boundaries of healthy bone, and can easily bedistinguished from cellulites in which the involvementalso includes soft tissues. However, the efficacy of athree-phase bone scan decreases in follow-up or afterantibiotic or surgical treatment because the modificationsof bone metabolism, and the normalization of scinti-graphic images, are very slow. An increased uptake oflabelled diphosphonates can persist for months or yearsafter recovery of a bone fracture or after osteomyelitis. Inpaediatric patients the water content and perfusionsupply of bone are increased in comparison with adults.So, septic bone necrosis is not rare and can result in coldareas on methylene diphosphonate bone scintigraphy(Fig. 1). Haematogenous osteomyelitis can involve morebones, which is the reason why a whole-body bone scan isessential in these cases.
The diagnosis of bone infections becomes difficult incases of recently implanted prostheses, in delays ofconsolidation of exposed fractures and after repeatedsurgical or therapeutic interventions. The principalproblem in osteomyelitis remains the search for infectionsin a bone with altered structure caused by re-absorptionor new apposition processes where there is a loss ofspecificity of bone scintigraphy, CT and MRI. Radiologi-cal methods are also limited by the presence of synthesismaterials or by implants or prostheses that provokeimportant artefacts in both CT and MRI scans. In thesecontexts the most reliable investigation for verifying thepresence of bone infection remains scintigraphy withlabelled leucocytes. In this technique, either WBCs or
Fig. 1
Bone scan in a right foot osteomyelitis in a 6-year-old child. The coldarea corresponding to the navicular bone of the right foot is expressingseptic necrosis.
Osteomyelitis: clinical update for practical guidelines Concia et al. 649
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

pure granulocytes labelled with either 111In-oxime or99mTc-HMPAO can be used: the choice of cell orradiolabel is not critical. The most important factorinfluencing the accuracy of this examination is the timerequired to follow the diapedesis of the granulocytes,prolonging the examination to at least 24 h. In this way itis possible to observe labelled granulocytes migratingfrom the blood to the soft tissues and concentratingaround the prostheses, in the cavities, in fistulas, and,sometimes, in the regional lymph nodes [4,7,16–18].Moreover, the scintigraphic accuracy of labelled leuco-cytes is modified by the presence of the red marrow inbones involved in osteomyelitis. In haematogenousosteomyelitis of the axial skeleton or of the proximalappendicular skeleton 30–75% of cold areas are foundwith WBC scintigraphy. These are areas where there iszero or very low blood flow and are the equivalent ofsequestered bone on X-ray examinations. In thesecases scintigraphy with leucocytes (or even monoclonalantibodies) labelled in vitro, is useless in assessing theactivity of inflammation because cold areas can persistindefinitely, maintaining this situation for years. Inyoung patients the bone marrow is extended in all theskeleton segments up to the distal appendicular ones.Therefore, in paediatric age groups we have, more orless, the same limitations in the use of labelled WBCsthat we have in the axial skeleton of adults and labelledWBCs in vitro (or monoclonal antibodies) are oftenuseless.
Unspecific radiopharmaceuticals for detecting inflamma-tion, such as 67Ga or 18F-FDG, with an uptake propor-tional to the vascular permeability or to metabolicactivity, should be preferred in secondary bone infectionsof axial skeleton. In these cases the scintigraphy isordered only for assessing whether the infection is stillactive or not after therapeutic approaches (e.g., surgery,antibiotics).
Prosthetic jointsOrthopaedic surgeons and clinicians must identify theposition and extent of infection when dealing withprosthetic joints. Furthermore, they have to provideaccurate information on the prosthesis, taking intoaccount patient history, the clinical possibility of infec-tion, X-ray images, and laboratory data. Most importantly,they must identify the kind of prosthesis with which theyare working. Cemented prostheses are custom-madebecause the cement hardens within 20min and givesimmediate mechanical stability to the prosthesis. How-ever, as the cement hardens it produces an exothermicreaction, which may bring about an endosteal necrosisthat affects vascular flow in the bone–cement interface.The polyethylene waste product that builds up over timebecause of wear and tear of the cotyloid cavity may lead toosteolysis near the cement of the prosthesis showing a
characteristic accumulation of labelled diphosphonate.Non-cemented prostheses, on the other hand, inevitablybring about a reshaping of adjacent tissues that mayeither erode the bone or cause new bony deposits. Thisreshaping depends on the material used in the prosthesis,on its design, its primary anchoring, and on whether theprosthesis is coated with osteo-inductive materials.Chrome–cobalt–molybdenum alloys, once commonlyused, are very rigid, and produce significant reshapingof the bone, which induces a considerable necrosis inbone tissue due to the accumulation of deposits of bothbone and metal. For this reason, titanium alloys are nowbeing used, as they are less rigid and produce fewerdeposits and less bone necrosis [31].
Design and primary anchoring are equally important. Theso-called distal press-fit involves long prostheses whileproximal press-fit and distal filling have completelydifferent osteo-metabolic characteristics. Another keyfactor is the potential presence of an osteo-inductivecoating. The purity and porosity of this coating have animpact on the extent of reshaping that takes place aroundthe prosthesis, and consequently on the degree ofdiphosphonate uptake at bone scintigraphy.
Traditional X-ray reveals specific details of the bone–prosthesis interface but it is of little help if the infectionis in soft tissue. Characteristic signs are small and unclear,and conventional X-rays often give negative results. Insoft-tissue infection, ultrasonography will provide highlydetailed information; for example, in identifying whetheran abscess is relative to vascular and nerve bundles. Thisis essential to plan access, intervention and debridement.If this infection is extensive, it can spread to theabdomen or the pelvis. The limits of the technique arethat, in the early phase, it fails to distinguish post-surgicalhaematoma from septic haematoma, which may affectsoft tissues [32].
CT and MRI are excellent techniques but, when dealingwith infections near prostheses, lose some of theireffectiveness because the quality of the resulting imagesis severely affected by the presence of the metalhardware. CT can provide information about the move-ment of the prosthesis, but fails to distinguish betweenmechanical and infectious loosening. However, CT canplay a role if used with WBC scintigraphy, which allows amorphological examination of their location and accumu-lation. Likewise, CT–PET can reveal the morphology of18F-FDG accumulation. By using CT, the surgeon canobtain important information on the extent to which aninfection has spread through muscular tissues, while CTfistulography is useful if abdominal tissue is involved. CTallows the biopsy to be guided to the location of infectionand an antibiogram, which is essential for curing theinfection with specific antibiotics, to be obtained.
650 Nuclear Medicine Communications 2006, Vol 27 No 8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
With infections in hip prostheses, a three-phase bone scanshows an increase in early perfusion and a delayedmetabolic accumulation of diphosphonate all around theprosthesis, marking out its contour. The specificity of bonescintigraphy in hip prostheses ranges from 50 to 70%according to case specific circumstances [33] because thebone scan signal requires months if not years beforereturning to normality even if the clinical problem has beenresolved. In the case of simple instability, on the otherhand, there is no early increase in perfusion while thedelayed accumulation of diphosphonate is typically con-centrated in the load-bearing points at the top of theacetabulum, in the minor and major trochanter and at thetop of the prosthesis stem. A three-phase bone scan has asensitivity of about 85% in hip prostheses infection [34]. Inknee prostheses, the role of three-phase bone scintigraphyis less definite and it is more difficult to differentiate a caseof movement from a case of infection [35].
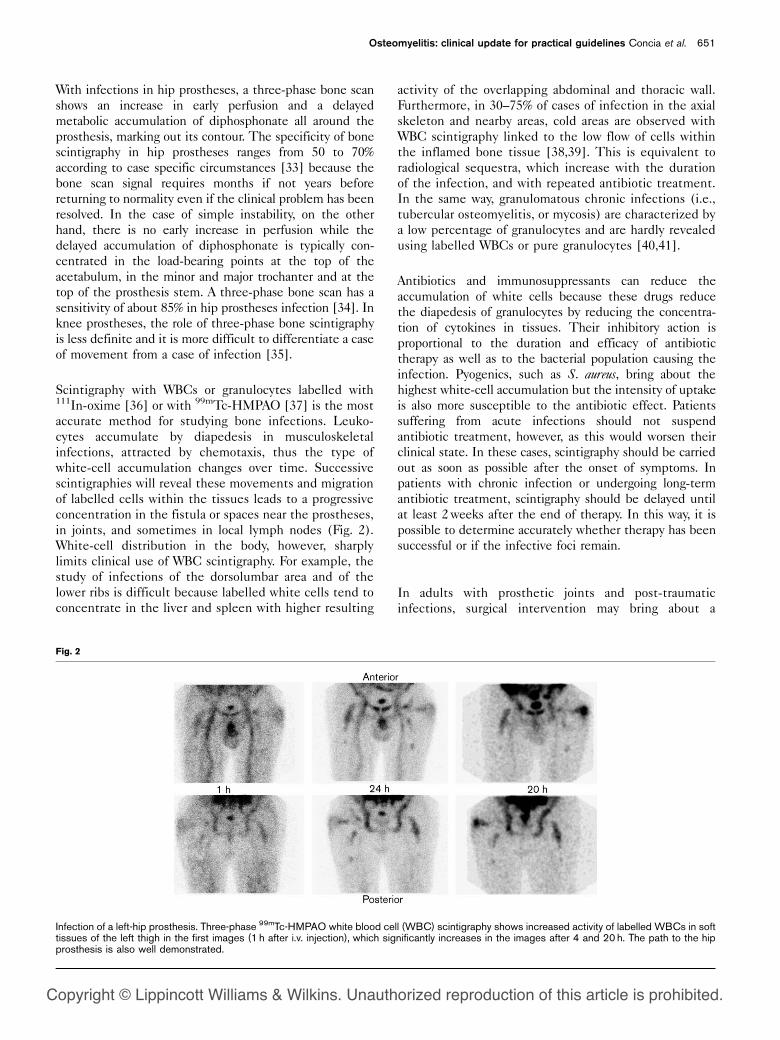
Scintigraphy with WBCs or granulocytes labelled with111In-oxime [36] or with 99mTc-HMPAO [37] is the mostaccurate method for studying bone infections. Leuko-cytes accumulate by diapedesis in musculoskeletalinfections, attracted by chemotaxis, thus the type ofwhite-cell accumulation changes over time. Successivescintigraphies will reveal these movements and migrationof labelled cells within the tissues leads to a progressiveconcentration in the fistula or spaces near the prostheses,in joints, and sometimes in local lymph nodes (Fig. 2).White-cell distribution in the body, however, sharplylimits clinical use of WBC scintigraphy. For example, thestudy of infections of the dorsolumbar area and of thelower ribs is difficult because labelled white cells tend toconcentrate in the liver and spleen with higher resulting
activity of the overlapping abdominal and thoracic wall.Furthermore, in 30–75% of cases of infection in the axialskeleton and nearby areas, cold areas are observed withWBC scintigraphy linked to the low flow of cells withinthe inflamed bone tissue [38,39]. This is equivalent toradiological sequestra, which increase with the durationof the infection, and with repeated antibiotic treatment.In the same way, granulomatous chronic infections (i.e.,tubercular osteomyelitis, or mycosis) are characterized bya low percentage of granulocytes and are hardly revealedusing labelled WBCs or pure granulocytes [40,41].
Antibiotics and immunosuppressants can reduce theaccumulation of white cells because these drugs reducethe diapedesis of granulocytes by reducing the concentra-tion of cytokines in tissues. Their inhibitory action isproportional to the duration and efficacy of antibiotictherapy as well as to the bacterial population causing theinfection. Pyogenics, such as S. aureus, bring about thehighest white-cell accumulation but the intensity of uptakeis also more susceptible to the antibiotic effect. Patientssuffering from acute infections should not suspendantibiotic treatment, however, as this would worsen theirclinical state. In these cases, scintigraphy should be carriedout as soon as possible after the onset of symptoms. Inpatients with chronic infection or undergoing long-termantibiotic treatment, scintigraphy should be delayed untilat least 2weeks after the end of therapy. In this way, it ispossible to determine accurately whether therapy has beensuccessful or if the infective foci remain.
In adults with prosthetic joints and post-traumaticinfections, surgical intervention may bring about a
Fig. 2
Infection of a left-hip prosthesis. Three-phase 99mTc-HMPAO white blood cell (WBC) scintigraphy shows increased activity of labelled WBCs in softtissues of the left thigh in the first images (1 h after i.v. injection), which significantly increases in the images after 4 and 20 h. The path to the hipprosthesis is also well demonstrated.
Osteomyelitis: clinical update for practical guidelines Concia et al. 651
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

peripheral displacement of the bone marrow towardssurrounding spaces, which may then be mistakenlyinterpreted as septic. To avoid this inconvenience,Palestro et al. [42] suggested comparing 111In-leukocytescintigraphy with a bone marrow scan (with 99mTc-sulfurcolloids). The discrepancy between the two scintigraphicimages (leukocytes greater than colloids) very accuratelyidentifies the presence of infection. As an alternative,repeating scintigraphic observations at 1, 4 and 20 h afterthe re-injection of cells makes it possible to distinguishthe invariant accumulation with time (that is, bonemarrow) from progressively rising accumulation in osteo-myelitis. Comparing the three images, it may be possibleto follow the path taken by the white-cell diapedesis fromthe location of the infection to the fistulas or otherperiprosthesis spaces [43]. The two methods haveequivalent sensitivity at around 95% for peripheralbone tissue with a specificity of 97% [44]. The samefigures are lower for axial skeleton and in chronicinfections [45].
Management of patients with osteomyelitisA multidisciplinary and structured approach to themanagement of bone infections is important. Antibiotictherapy must rest on the identification of the pathogen.This allows an accurate antibiogram, which will pinpointthe group of antibiotics to be used in the treatment.Among these, we are then able to choose the antibioticthat can best penetrate bone tissue and which has lowtoxicity. Staphylococcus is enemy number one. Rifampicin,macrolides and teicoplanin have excellent diffusionprofiles, thus whenever possible this group of antibioticsshould be favoured. On the other hand, we know thatteicoplanin has a good degree of coverage for methicillin-resistant S. aureus and of vancomycin-resistant Enteroccoc-cus, although vancomycin is associated with a higher riskof relapse when compared to teicoplanin. As forquinolones, the paired quinolone–rifampicin has anexcellent pharmacokinetic profile and therefore can bea useful combination in treating some forms of staphy-lococci [46,47].
Aetiological therapyAetiological therapy cannot do without rifampicin, whichhas an optimal intercellular concentration, a very goodsensitivity profile for methicillin-resistant staphylococciand when used with teicoplanin offers significant clinicaladvantages that have been demonstrated both in thelaboratory and in practice [48]. Among new drugs,linezolid inhibits bacterial protein synthesis and is veryeffective on methicillin-resistant staphylococci and onvancomycin-resistant Enteroccoccus. Linezolid is also easilyabsorbed which is a great advantage when associated with100% bioavailability and has excellent bone penetration.For the time being, however, there are no agreedprotocols for the use of this antibiotic in osteomyelitis
[49,50]. Quinupristin–dalfopristin is sometimes used.This antibiotic also blocks protein synthesis, spreadseasily amongst macrophages, and has a good tissuedistribution. However, its use in osteomyelitis is advisableonly in particularly selected cases [51,52].
Empirical therapyEmpirical therapy has to be resorted to when it isimpossible to isolate the root of the infection. In this caselocal epidemiological factors must be taken into account,together with determining whether the infection hasbeen contracted in hospital or elsewhere. Infectionscontracted outside hospitals are usually from methicillin-sensitive staphylococci, and are frequently polymicrobicinfections with the presence of Gram-negative bacteria.In these cases, the clinician should start with an aminopenicillin associated with a beta-lactamase inhibitor, onthe following antimicrobial associations: rifampicin +quinolone, oxacillin or teicoplanin or clyndamicin +ceftriaxon or cefepime or quinolone [53]. Hospital-contracted infections, on the other hand, have a highprobability of being derived from methicillin-resistantstaphylococci, which should be dealt with through aglycopeptide, particularly teicoplanin, together withrifampicin, possibly associated with antibiotics active onGram-negatives [14,54].
The antibiotics should preferably be administeredparenterally for several weeks. This raises the problemsof cost, patient cooperation, and morbidity. Most patientswill have to remain in hospital because it is not alwayspossible to identify an antibiotic that can be administeredparenterally at home, given that dosages are seldomintended for individual home use. Oral therapy has beenconsidered but we do not yet have enough data. For thetime being, oral therapy is indicated only in children.Furthermore, oral therapy can only be used with patientswhose compliance is certain. Treatment duration is notstandardized at present. In any event, it must be based onthe type of infection. For instance, haematogenousinfections must be dealt with by determining whetherbone sequestration is occurring and whether debridementis necessary. Depending on the specific case, therapy for4–6weeks may be enough or it may prove necessary toincrease it to 6weeks or longer [55,56].
Often osteomyelitis fails to improve because bacteriahave the ability to resist to antibiotics. S. epidermidis sticksto the prosthesis and is enclosed in the bio film: apolymeric matrix acts as a protective mantle to impedephagocytosis and the delivery of the antibiotic [57,58].The reduced growth of bio film bacteria is responsible fortheir resistance to many antibiotics that are only active inthis phase. Rifampicin acts on the bio film and musttherefore always be used with other antibiotics when aprosthesis infection is present. Failure to use rifampicin
652 Nuclear Medicine Communications 2006, Vol 27 No 8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

within a month or a few weeks of treatment will allowinfection to start again.
Treatment of prosthesis infectionsAntibiograms in prosthesis infections should be per-formed, mixing the materials that replicate the impact ofthe prosthesis itself. For example, ofloxacin affects theGram-positives of a fluid culture but adding somepolystyrene beads to the broth better simulates realconditions. In this case, antibiograms change completelyand bio film producing bacteria develop. It follows thatthe duration of the antibiotic treatment is not standar-dized. It has to be defined according to infection type: inhaematogenous infection, it is necessary to check forbone sequestration. If debridement is called for, therapyfor 4–6weeks can be enough or it may prove necessary toprolong therapy for 6weeks or more [19].
The causes of pain in hip prostheses can be mechanical or‘biological’. Mechanical causes are load bearing, excessiveperiprosthesis re-absorption, possible sinking followingthe original placement, fractures (macro or micro) in thefemur near or under the prosthesis. Biological causes arereactions to polyethylene deposits (in cases of antisepticmovements) and infection (in the case of septic move-ment). In cases of infection, a two-stage interventionmust be accompanied by medical therapy of up to6weeks, comprising collecting biotic samples and exam-ining cultures in the removal stage and resorting toantibiograms to fine-tune the antibiotic.
In the case of prosthesis infection, different surgicalinterventions are possible: from simple debridement, toone-stage or two-stage intervention, to outright removal.Different interventions will, of course, demand differenttherapies. In one-stage interventions, antibiotic therapymust be particularly long, at least 4 weeks before theintervention and up to 16weeks afterwards. Note that,especially in this type of intervention, resorting toempirical therapy will be simpler than the more rigorousaetiological approach. Therapies lasting less than 4weekshave been shown to carry a high risk of re-infection; thus,they should be continued for at least 6 weeks. While it isdifficult to be certain that the bone has healed,combining clinical, radiological and biochemical, informa-tion (such as carefully monitored CRP follow-up) candefinitely be of assistance. As for CRP data, it is well tokeep in mind that recurrent inflammation episodes mayover-ride all other considerations.
Use of antibiotic-loaded acrylic cementIn 1970, Buchholz and Engelbrecht [59] introducedantibiotic-loaded acrylic cement to the treatment ofprosthesis infections, a technique that has since beenused frequently. Simply put, its advantages are higherconcentrations of antibiotic in the soft tissues and in the
bone than would be possible by alternative deliverymethods, low serum concentration and, consequently,lower toxicity. In our opinion, the technique hasbenefited from the well-known suggestion, in 1988, byWilde and Ruth [60] of a space block and multiple stagetreatment. The space block has a double advantage:mechanical and biological. The first is in preventing jointhead fusion, while maintaining the correct length ofmuscular structures and reducing post-surgery bloodpooling. The second is in assisting the disinfection oflocalized septic points and maintaining high localconcentrations of antibiotic. In addition, the two-stagetechnique allows for a repeat of surgical cleaning and theuse of un-anchored prostheses.
The most important problem remains the choice ofdosage of the antibiotic associated with the cement.Bactericidal tests performed on various stocks of patho-genic agents have shown the absolute ineffectiveness ofsome antibiotics. Our conclusion is that for S. aureus andS. epidermidis and Pseudomonas, the most effectivebactericide was a combination of vancomycin andimipenem–cilastatin, most likely because their actionswere mutually reinforced to the greater porosity of thecement, which leads to a greater release of the antibiotic.Furthermore, two-stage procedures offer better control ofthe infection because they give the opportunity ofintroducing a prosthesis without cement, while the one-stage intervention forces the use of a cementedprosthesis [61,62]. This treatment requires cooperationbetween epidemiologists, microbiologists and nuclearphysicians. Its high cost may discourage hospital admin-istrations and private nursing homes, however [63].
Diagnosis of patients with suspectedosteomyelitisClinical examination of the patient always allows thedetection of functional impairment and laboratory testscan provide bone infection data. Conventional X-ray isthe first imaging procedure in the diagnostic flow chart ofosteomyelitis: if the results are positive, this is sufficientto begin the appropriate therapy.
Haematogenous osteomyelitisIn haematogenous osteomyelitis, a three-phase bone scancan provide a result within 24-48 h after the onset ofosteomyelitis symptoms and can be used very profitablyin radiologically negative cases or for whole-body studiesbecause haematogenous osteomyelitis is often multifocal.In children and adolescents, pain is the main symptom ofosteomyelitis, accompanied by other joint diseases suchas arthritis, aseptic necrosis or epiphysiolysis of the hip,which can be quickly identified and distinguished fromosteomyelitis by using bone scintigraphy. Finding coldareas on the scintigraphic image of a septic necrosisthat complicates haematogenous osteomyelitis is more
Osteomyelitis: clinical update for practical guidelines Concia et al. 653
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
common in children due to their higher bone watercontent [64].
The interpretation of conventional radiological resultsbecomes complicated where there are prosthetic jointsand secondary or post-traumatic osteomyelitis, or wherethere has been bone re-modelling, previous operationsand the presence of synthesis materials or metal supportdevices. Nevertheless, such tests are carried out to assessthe bone condition. If there are any doubts about the X-ray results, CT and MRI provide a more detailedmorphological study and offer the orthopaedic surgeon aguide regarding surgical drainage of abscesses or thedebridement of necrotic bone. The presence of synthesismaterials, however, hinders or limits the detection ofpersistent infection by CT or MRI imaging. In thesecases, where a surgical approach is difficult, it is necessaryto establish whether the secondary osteomyelitis is trulycured or whether it is merely present following con-solidation surgery. Scintigraphy with WBCs, in associationwith the appropriate suspension of antibiotic therapy, isthe most accurate way of determining the persistence ofan infection [65].
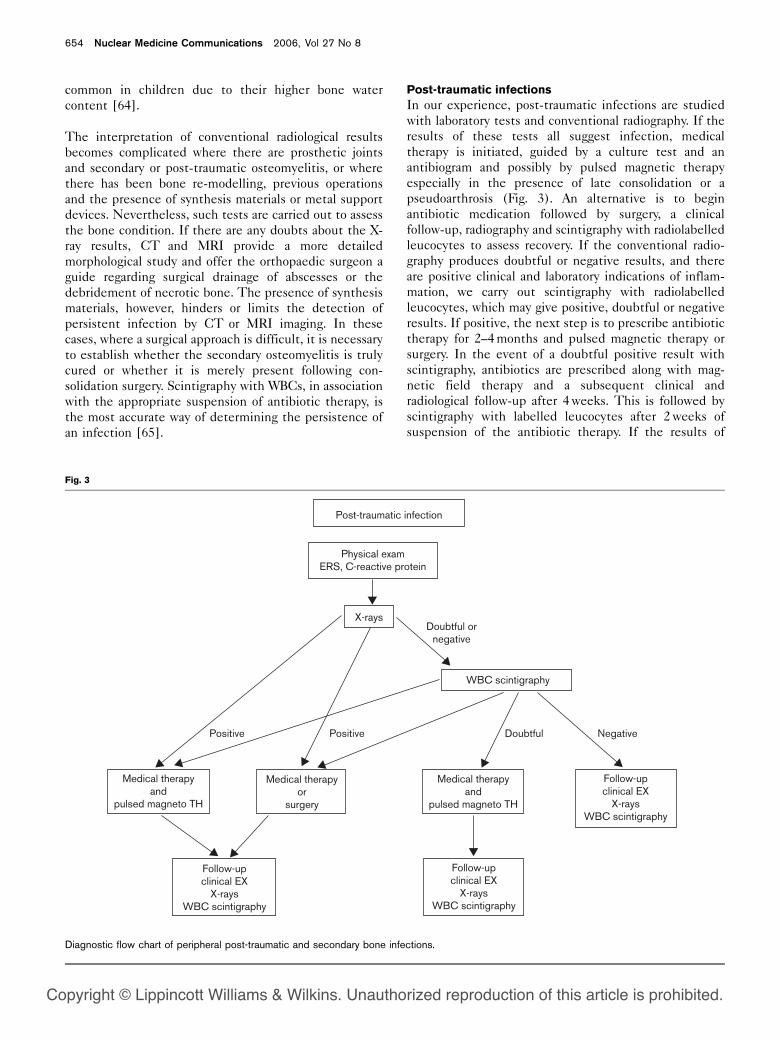
Post-traumatic infectionsIn our experience, post-traumatic infections are studiedwith laboratory tests and conventional radiography. If theresults of these tests all suggest infection, medicaltherapy is initiated, guided by a culture test and anantibiogram and possibly by pulsed magnetic therapyespecially in the presence of late consolidation or apseudoarthrosis (Fig. 3). An alternative is to beginantibiotic medication followed by surgery, a clinicalfollow-up, radiography and scintigraphy with radiolabelledleucocytes to assess recovery. If the conventional radio-graphy produces doubtful or negative results, and thereare positive clinical and laboratory indications of inflam-mation, we carry out scintigraphy with radiolabelledleucocytes, which may give positive, doubtful or negativeresults. If positive, the next step is to prescribe antibiotictherapy for 2–4months and pulsed magnetic therapy orsurgery. In the event of a doubtful positive result withscintigraphy, antibiotics are prescribed along with mag-netic field therapy and a subsequent clinical andradiological follow-up after 4weeks. This is followed byscintigraphy with labelled leucocytes after 2weeks ofsuspension of the antibiotic therapy. If the results of
Fig. 3
Post-traumatic infection
Physical examERS, C-reactive protein
X-raysDoubtful or
negative
Doubtful
WBC scintigraphy
NegativePositivePositive
Medical therapyand
pulsed magneto TH
Medical therapyand
pulsed magneto TH
Follow-upclinical EX
X-raysWBC scintigraphy
Follow-upclinical EX
X-raysWBC scintigraphy
Follow-upclinical EX
X-raysWBC scintigraphy
Medical therapyor
surgery
Diagnostic flow chart of peripheral post-traumatic and secondary bone infections.
654 Nuclear Medicine Communications 2006, Vol 27 No 8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
WBC scintigraphy are negative, the antibiotics can be re-started to consolidate the results and the clinical andradiological follow-up can take place after 4weeksfollowed by labelled-leucocyte scintigraphy at 2months.
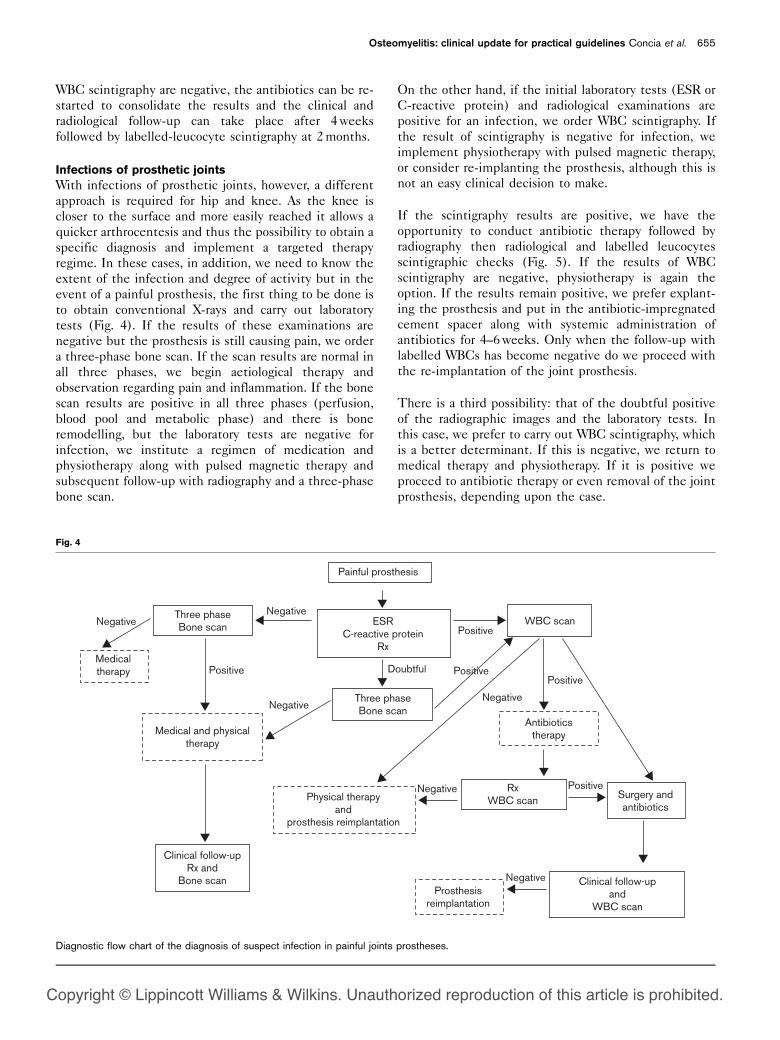
Infections of prosthetic jointsWith infections of prosthetic joints, however, a differentapproach is required for hip and knee. As the knee iscloser to the surface and more easily reached it allows aquicker arthrocentesis and thus the possibility to obtain aspecific diagnosis and implement a targeted therapyregime. In these cases, in addition, we need to know theextent of the infection and degree of activity but in theevent of a painful prosthesis, the first thing to be done isto obtain conventional X-rays and carry out laboratorytests (Fig. 4). If the results of these examinations arenegative but the prosthesis is still causing pain, we ordera three-phase bone scan. If the scan results are normal inall three phases, we begin aetiological therapy andobservation regarding pain and inflammation. If the bonescan results are positive in all three phases (perfusion,blood pool and metabolic phase) and there is boneremodelling, but the laboratory tests are negative forinfection, we institute a regimen of medication andphysiotherapy along with pulsed magnetic therapy andsubsequent follow-up with radiography and a three-phasebone scan.
On the other hand, if the initial laboratory tests (ESR orC-reactive protein) and radiological examinations arepositive for an infection, we order WBC scintigraphy. Ifthe result of scintigraphy is negative for infection, weimplement physiotherapy with pulsed magnetic therapy,or consider re-implanting the prosthesis, although this isnot an easy clinical decision to make.
If the scintigraphy results are positive, we have theopportunity to conduct antibiotic therapy followed byradiography then radiological and labelled leucocytesscintigraphic checks (Fig. 5). If the results of WBCscintigraphy are negative, physiotherapy is again theoption. If the results remain positive, we prefer explant-ing the prosthesis and put in the antibiotic-impregnatedcement spacer along with systemic administration ofantibiotics for 4–6weeks. Only when the follow-up withlabelled WBCs has become negative do we proceed withthe re-implantation of the joint prosthesis.
There is a third possibility: that of the doubtful positiveof the radiographic images and the laboratory tests. Inthis case, we prefer to carry out WBC scintigraphy, whichis a better determinant. If this is negative, we return tomedical therapy and physiotherapy. If it is positive weproceed to antibiotic therapy or even removal of the jointprosthesis, depending upon the case.
Fig. 4
Painful prosthesis
Negative
Negative
Negative
Negative
Negative
Negative
Positive PositiveDoubtful
Positive
Positive
Positive
WBC scan
Antibioticstherapy
Surgery andantibiotics
Clinical follow-upand
WBC scan
Clinical follow-upRx and
Bone scan
Three phaseBone scan
Three phaseBone scan
RxWBC scan
Prosthesisreimplantation
Physical therapyand
prosthesis reimplantation
Medical and physicaltherapy
Medical therapy
ESRC-reactive protein
Rx
Diagnostic flow chart of the diagnosis of suspect infection in painful joints prostheses.
Osteomyelitis: clinical update for practical guidelines Concia et al. 655
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Vertebral osteomyelitisIn diagnosing vertebral osteomyelitis, a series of haema-tochemical assessments must be carried out, includingindices of inflammation, culture tests on biologicalliquids and instrumental examinations, including biop-sies. Early diagnosis is the key to resolving septicspondylodiskitis as it can prevent the onset of permanentneurological deficits and the formation of vertebraldeformities. MRI is, without doubt, the most importantand most sensitive tool and allows the formulation of adifferential diagnosis with degenerative and metastaticprocesses as it supplies data on the anatomy and theextension of the infectious process in haematogenousspondylodiskitis.
In the study of post-operative spondylodiskitis, thesensitivity and specificity of radiological methods suffera substantial loss due to the presence of scar tissue and/orpost-operative reactions. From the diagnostic point ofview, biopsies are very important examinations inidentifying pathogenic agents and can be affected bythe transpedicular or disk routes or by open surgery. Thisprocedure can produce negative results in 30–50% ofcases, however, and is therefore not particularly useful indiagnosing spondylodiskitis, which in 90% of cases is post-operative, with bones that have been altered by non-specific re-modelling and is thus difficult to diagnoseusing radiological methods.
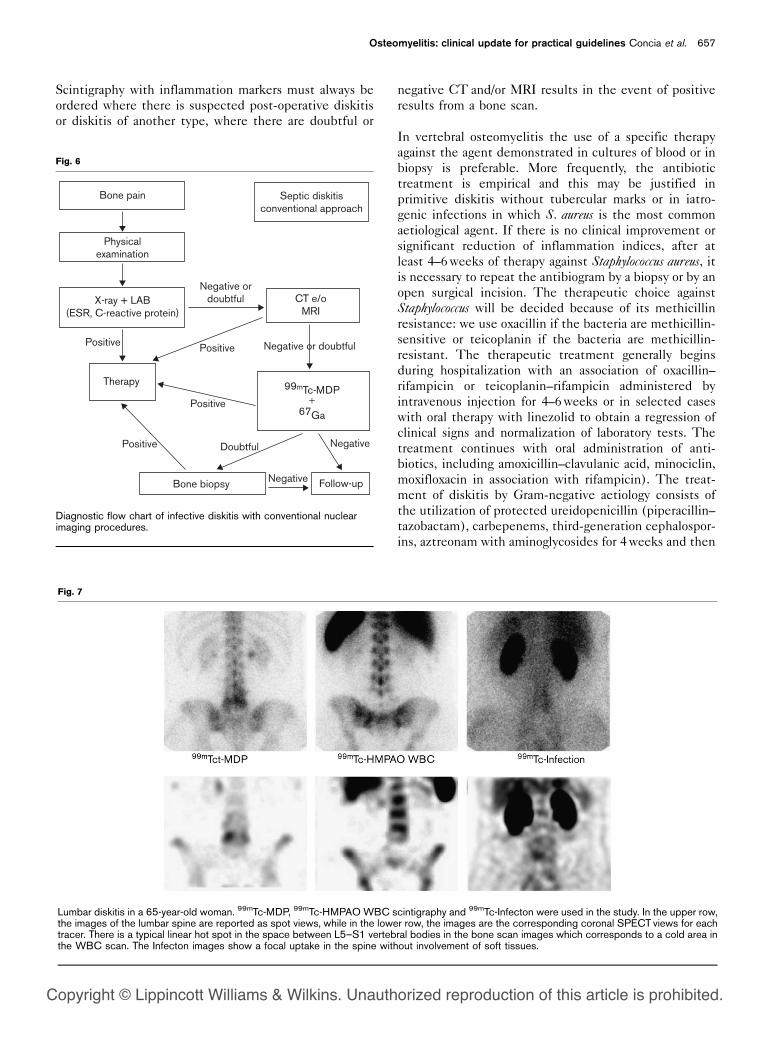
In traditional diagnostic algorithms (Fig. 6), scintigraphywith 99mTc-hydroxymethylene diphosphonate (99mTc-HDP) and 67Ga citrate are often mentioned. Both
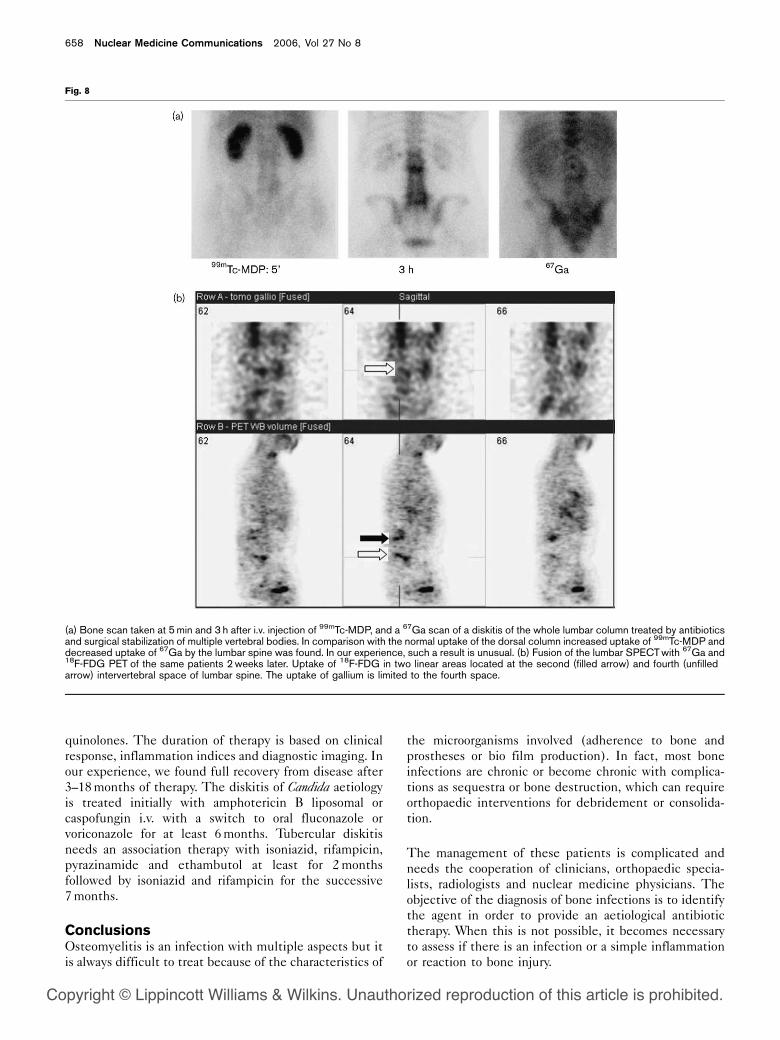
methods use tracers that accumulate in inflamed areasand are highly sensitive. Nowadays, even if this use hasnot been fully referred to in diagnostic algorithms,nuclear medicine makes great use of this technique indiagnosing post-operative spondylodiskitis. The radio-pharmaceuticals to be used in a case of suspectedspondylodiskitis are, amongst those available in all thecentres, 99mTc-HDP, 111In- and 99mTc-labelled WBCs,immunoscintigraphy with monoclonal antibodies and67Ga citrate. Others still in the experimental stageinclude 111In-biotin and 99mTc-ciprofloxacin (Fig. 7). Indescending order of accuracy of scintigraphic tracers, thedata from the study of spondylodiskitis is as follows: 18F-FDG (90%) (Fig. 8), 67Ga citrate (88.50%), anti-granulocyte antibodies (88.5%) and labelled WBCs(65.5–80%). The data regarding accuracy with experi-mental markers is 111In-biotin (95.2%) and 99mTc-ciprofloxacin (81.5%) [66–72].
This demonstrates therefore that the radiopharmaceuti-cals to be used in cases of suspected spondylodiskitis are99mTc-HDP and 67Ga citrate, which are available in all thecentres, 18F-FDG is available in selected centres and111In-biotin and 99mTc-ciprofloxacin where possible(Fig. 9).
Scintigraphy with inflammation tracers must be used as acomplementary examination to current radiological meth-ods (CT or MRI) where haematogenous diskitis issuspected. It may be chosen, however, as the primaryinvestigative tool in cases of suspected post-operativediskitis and its follow-up.
Fig. 5
Example of a woman with infection of a left-knee prosthesis. (a) Biphasic 99mTc-MDP scintigraphy on 3 September 2002. The 5 minutes imagesshow an increased perfusion in the tissues surrounding the knee prosthesis. The 3 hours images show that the uptake of MDP prevails in the tibialepiphysis and in patella. (b) Three-phase 99mTc-HMPAO WBC scintigraphy of the same patient on 18 September 2002 (i.e., 2weeks after theimages in panel a). There is significant increase of labelled WBCs both in femur and tibia periprosthetic bone, in surrounding soft tissues and in thearticular cavity. (c) Three-phase 99mTc-HMPAO WBC scintigraphy check-up on 5 December 2002, after removal of the infected knee prosthesis,with 6weeks of antibiotic therapy and the use of antimicrobial-impregnated cement in the articular cavity to allow partial joint mobility and length ofleg.
656 Nuclear Medicine Communications 2006, Vol 27 No 8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Scintigraphy with inflammation markers must always beordered where there is suspected post-operative diskitisor diskitis of another type, where there are doubtful or
negative CT and/or MRI results in the event of positiveresults from a bone scan.
In vertebral osteomyelitis the use of a specific therapyagainst the agent demonstrated in cultures of blood or inbiopsy is preferable. More frequently, the antibiotictreatment is empirical and this may be justified inprimitive diskitis without tubercular marks or in iatro-genic infections in which S. aureus is the most commonaetiological agent. If there is no clinical improvement orsignificant reduction of inflammation indices, after atleast 4–6weeks of therapy against Staphylococcus aureus, itis necessary to repeat the antibiogram by a biopsy or by anopen surgical incision. The therapeutic choice againstStaphylococcus will be decided because of its methicillinresistance: we use oxacillin if the bacteria are methicillin-sensitive or teicoplanin if the bacteria are methicillin-resistant. The therapeutic treatment generally beginsduring hospitalization with an association of oxacillin–rifampicin or teicoplanin–rifampicin administered byintravenous injection for 4–6weeks or in selected caseswith oral therapy with linezolid to obtain a regression ofclinical signs and normalization of laboratory tests. Thetreatment continues with oral administration of anti-biotics, including amoxicillin–clavulanic acid, minociclin,moxifloxacin in association with rifampicin). The treat-ment of diskitis by Gram-negative aetiology consists ofthe utilization of protected ureidopenicillin (piperacillin–tazobactam), carbepenems, third-generation cephalospor-ins, aztreonam with aminoglycosides for 4weeks and then
Fig. 6
Bone pain
Physicalexamination
X-ray + LAB(ESR, C-reactive protein)
Therapy
Bone biopsy Follow-up
Negative
Negative
Negative or doubtful
Negative ordoubtful
Positive
Positive Positive
Positive Doubtful
Septic diskitisconventional approach
CT e/oMRI
99mTc-MDP+
67Ga
Diagnostic flow chart of infective diskitis with conventional nuclearimaging procedures.
Fig. 7
Lumbar diskitis in a 65-year-old woman. 99mTc-MDP, 99mTc-HMPAOWBC scintigraphy and 99mTc-Infecton were used in the study. In the upper row,the images of the lumbar spine are reported as spot views, while in the lower row, the images are the corresponding coronal SPECT views for eachtracer. There is a typical linear hot spot in the space between L5–S1 vertebral bodies in the bone scan images which corresponds to a cold area inthe WBC scan. The Infecton images show a focal uptake in the spine without involvement of soft tissues.
Osteomyelitis: clinical update for practical guidelines Concia et al. 657
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
quinolones. The duration of therapy is based on clinicalresponse, inflammation indices and diagnostic imaging. Inour experience, we found full recovery from disease after3–18months of therapy. The diskitis of Candida aetiologyis treated initially with amphotericin B liposomal orcaspofungin i.v. with a switch to oral fluconazole orvoriconazole for at least 6months. Tubercular diskitisneeds an association therapy with isoniazid, rifampicin,pyrazinamide and ethambutol at least for 2monthsfollowed by isoniazid and rifampicin for the successive7months.
ConclusionsOsteomyelitis is an infection with multiple aspects but itis always difficult to treat because of the characteristics of
the microorganisms involved (adherence to bone andprostheses or bio film production). In fact, most boneinfections are chronic or become chronic with complica-tions as sequestra or bone destruction, which can requireorthopaedic interventions for debridement or consolida-tion.
The management of these patients is complicated andneeds the cooperation of clinicians, orthopaedic specia-lists, radiologists and nuclear medicine physicians. Theobjective of the diagnosis of bone infections is to identifythe agent in order to provide an aetiological antibiotictherapy. When this is not possible, it becomes necessaryto assess if there is an infection or a simple inflammationor reaction to bone injury.
Fig. 8
(a) Bone scan taken at 5min and 3 h after i.v. injection of 99mTc-MDP, and a 67Ga scan of a diskitis of the whole lumbar column treated by antibioticsand surgical stabilization of multiple vertebral bodies. In comparison with the normal uptake of the dorsal column increased uptake of 99mTc-MDP anddecreased uptake of 67Ga by the lumbar spine was found. In our experience, such a result is unusual. (b) Fusion of the lumbar SPECTwith 67Ga and18F-FDG PET of the same patients 2weeks later. Uptake of 18F-FDG in two linear areas located at the second (filled arrow) and fourth (unfilledarrow) intervertebral space of lumbar spine. The uptake of gallium is limited to the fourth space.
658 Nuclear Medicine Communications 2006, Vol 27 No 8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
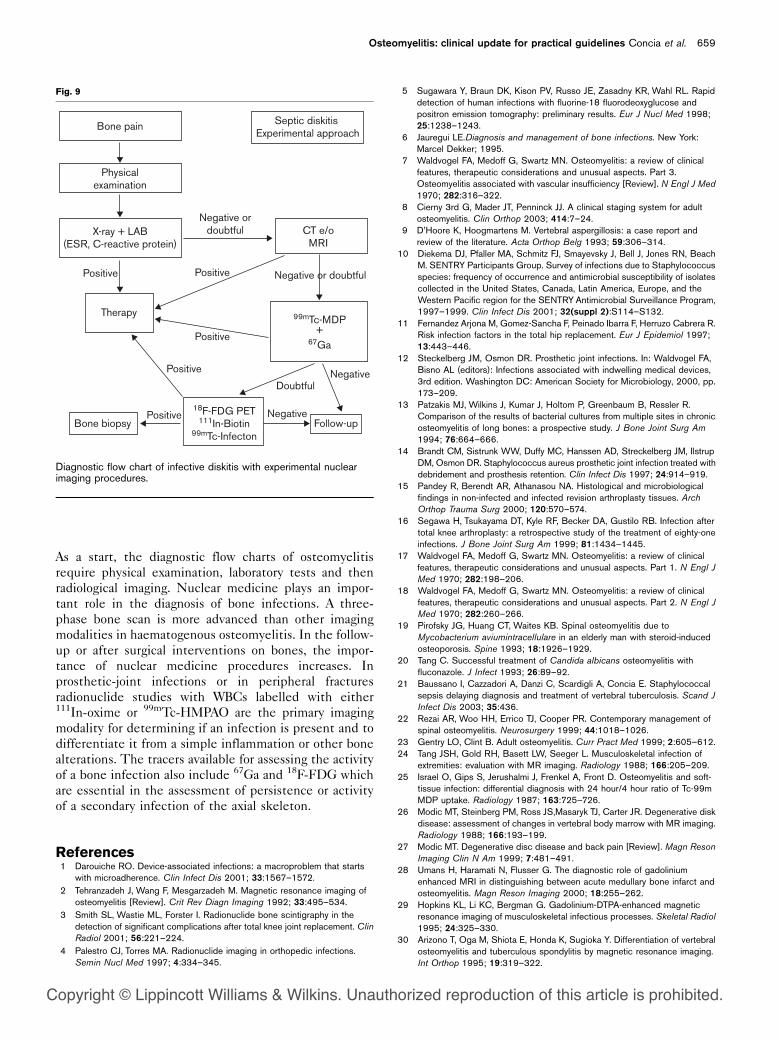
As a start, the diagnostic flow charts of osteomyelitisrequire physical examination, laboratory tests and thenradiological imaging. Nuclear medicine plays an impor-tant role in the diagnosis of bone infections. A three-phase bone scan is more advanced than other imagingmodalities in haematogenous osteomyelitis. In the follow-up or after surgical interventions on bones, the impor-tance of nuclear medicine procedures increases. Inprosthetic-joint infections or in peripheral fracturesradionuclide studies with WBCs labelled with either111In-oxime or 99mTc-HMPAO are the primary imagingmodality for determining if an infection is present and todifferentiate it from a simple inflammation or other bonealterations. The tracers available for assessing the activityof a bone infection also include 67Ga and 18F-FDG whichare essential in the assessment of persistence or activityof a secondary infection of the axial skeleton.
References1 Darouiche RO. Device-associated infections: a macroproblem that starts
with microadherence. Clin Infect Dis 2001; 33:1567–1572.2 Tehranzadeh J, Wang F, Mesgarzadeh M. Magnetic resonance imaging of
osteomyelitis [Review]. Crit Rev Diagn Imaging 1992; 33:495–534.3 Smith SL, Wastie ML, Forster I. Radionuclide bone scintigraphy in the
detection of significant complications after total knee joint replacement. ClinRadiol 2001; 56:221–224.
4 Palestro CJ, Torres MA. Radionuclide imaging in orthopedic infections.Semin Nucl Med 1997; 4:334–345.
5 Sugawara Y, Braun DK, Kison PV, Russo JE, Zasadny KR, Wahl RL. Rapiddetection of human infections with fluorine-18 fluorodeoxyglucose andpositron emission tomography: preliminary results. Eur J Nucl Med 1998;25:1238–1243.
6 Jauregui LE.Diagnosis and management of bone infections. New York:Marcel Dekker; 1995.
7 Waldvogel FA, Medoff G, Swartz MN. Osteomyelitis: a review of clinicalfeatures, therapeutic considerations and unusual aspects. Part 3.Osteomyelitis associated with vascular insufficiency [Review]. N Engl J Med1970; 282:316–322.
8 Cierny 3rd G, Mader JT, Penninck JJ. A clinical staging system for adultosteomyelitis. Clin Orthop 2003; 414:7–24.
9 D’Hoore K, Hoogmartens M. Vertebral aspergillosis: a case report andreview of the literature. Acta Orthop Belg 1993; 59:306–314.
10 Diekema DJ, Pfaller MA, Schmitz FJ, Smayevsky J, Bell J, Jones RN, BeachM. SENTRY Participants Group. Survey of infections due to Staphylococcusspecies: frequency of occurrence and antimicrobial susceptibility of isolatescollected in the United States, Canada, Latin America, Europe, and theWestern Pacific region for the SENTRYAntimicrobial Surveillance Program,1997–1999. Clin Infect Dis 2001; 32(suppl 2):S114–S132.
11 Fernandez Arjona M, Gomez-Sancha F, Peinado Ibarra F, Herruzo Cabrera R.Risk infection factors in the total hip replacement. Eur J Epidemiol 1997;13:443–446.
12 Steckelberg JM, Osmon DR. Prosthetic joint infections. In: Waldvogel FA,Bisno AL (editors): Infections associated with indwelling medical devices,3rd edition. Washington DC: American Society for Microbiology, 2000, pp.173–209.
13 Patzakis MJ, Wilkins J, Kumar J, Holtom P, Greenbaum B, Ressler R.Comparison of the results of bacterial cultures from multiple sites in chronicosteomyelitis of long bones: a prospective study. J Bone Joint Surg Am1994; 76:664–666.
14 Brandt CM, Sistrunk WW, Duffy MC, Hanssen AD, Streckelberg JM, IlstrupDM, Osmon DR. Staphylococcus aureus prosthetic joint infection treated withdebridement and prosthesis retention. Clin Infect Dis 1997; 24:914–919.
15 Pandey R, Berendt AR, Athanasou NA. Histological and microbiologicalfindings in non-infected and infected revision arthroplasty tissues. ArchOrthop Trauma Surg 2000; 120:570–574.
16 Segawa H, Tsukayama DT, Kyle RF, Becker DA, Gustilo RB. Infection aftertotal knee arthroplasty: a retrospective study of the treatment of eighty-oneinfections. J Bone Joint Surg Am 1999; 81:1434–1445.
17 Waldvogel FA, Medoff G, Swartz MN. Osteomyelitis: a review of clinicalfeatures, therapeutic considerations and unusual aspects. Part 1. N Engl JMed 1970; 282:198–206.
18 Waldvogel FA, Medoff G, Swartz MN. Osteomyelitis: a review of clinicalfeatures, therapeutic considerations and unusual aspects. Part 2. N Engl JMed 1970; 282:260–266.
19 Pirofsky JG, Huang CT, Waites KB. Spinal osteomyelitis due toMycobacterium aviumintracellulare in an elderly man with steroid-inducedosteoporosis. Spine 1993; 18:1926–1929.
20 Tang C. Successful treatment of Candida albicans osteomyelitis withfluconazole. J Infect 1993; 26:89–92.
21 Baussano I, Cazzadori A, Danzi C, Scardigli A, Concia E. Staphylococcalsepsis delaying diagnosis and treatment of vertebral tuberculosis. Scand JInfect Dis 2003; 35:436.
22 Rezai AR, Woo HH, Errico TJ, Cooper PR. Contemporary management ofspinal osteomyelitis. Neurosurgery 1999; 44:1018–1026.
23 Gentry LO, Clint B. Adult osteomyelitis. Curr Pract Med 1999; 2:605–612.24 Tang JSH, Gold RH, Basett LW, Seeger L. Musculoskeletal infection of
extremities: evaluation with MR imaging. Radiology 1988; 166:205–209.25 Israel O, Gips S, Jerushalmi J, Frenkel A, Front D. Osteomyelitis and soft-
tissue infection: differential diagnosis with 24 hour/4 hour ratio of Tc-99mMDP uptake. Radiology 1987; 163:725–726.
26 Modic MT, Steinberg PM, Ross JS,Masaryk TJ, Carter JR. Degenerative diskdisease: assessment of changes in vertebral body marrow with MR imaging.Radiology 1988; 166:193–199.
27 Modic MT. Degenerative disc disease and back pain [Review]. Magn ResonImaging Clin N Am 1999; 7:481–491.
28 Umans H, Haramati N, Flusser G. The diagnostic role of gadoliniumenhanced MRI in distinguishing between acute medullary bone infarct andosteomyelitis. Magn Reson Imaging 2000; 18:255–262.
29 Hopkins KL, Li KC, Bergman G. Gadolinium-DTPA-enhanced magneticresonance imaging of musculoskeletal infectious processes. Skeletal Radiol1995; 24:325–330.
30 Arizono T, Oga M, Shiota E, Honda K, Sugioka Y. Differentiation of vertebralosteomyelitis and tuberculous spondylitis by magnetic resonance imaging.Int Orthop 1995; 19:319–322.
Fig. 9
Bone pain
Physicalexamination
X-ray + LAB(ESR, C-reactive protein)
Therapy
Bone biopsy Follow-upNegative
Negative or doubtful
Negative ordoubtful
Positive
Positive
Positive
Positive
Positive
Doubtful
Septic diskitis Experimental approach
CT e/oMRI
99mTc-MDP+
67Ga
18F-FDG PET111In-Biotin
99mTc-Infecton
Negative
Diagnostic flow chart of infective diskitis with experimental nuclearimaging procedures.
Osteomyelitis: clinical update for practical guidelines Concia et al. 659
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
31 Zimmerli W, Waldvogel FA, Vaudaux P, Nydegger UE. Pathogenesis offoreign body infection: description and characteristics of an animal model. JInfect Dis 1982; 146:487–497.
32 Riebel TW, Nasir R, Nazarenko O. The value of sonography in the detectionof osteomyelitis. Pediatr Radiol 1996; 26:291–297.
33 Resnik D, Niwayama G. Osteomyelitis, septic arthritis and soft tissueinfection: the mechanism and situation. In: Resnick D, Niwayama G (editors):Diagnosis of bone and joint disorders, 2nd edition. Philadelphia: WBSaunders; 1981, pp. 2524–2618.
34 Love C, Palestro CJ. Radionuclide imaging of infection. J Nucl Med Technol2004; 32:47–57.
35 Duus BR, Boeckstyns M, Kjaer L, Stadeager C. Radionucleide scanningafter total knee replacement: correlation with pain and radiolucent lines.Aprospective study. Invest Radiol 1987; 22:891–894.
36 McAfee JC, Thakur ML. Survey of radioactive agents for the in vitro labelingof phagocytic leukocytes. I. Soluble agents. II. Particles. J Nucl Med 1976;17:480–492.
37 Peters AM, Danpure HJ, Hosman S, Hawker RJ, Henderson BL, HodgsonHJ, et al. Preliminary clinical experience with 99mTc-hexamethyl propylene-amineoxime for labelling leukocytes and imaging infection. Lancet 2 1986;8513:945–949.
38 Mello AM, Blake L, McDougall IR. ‘Cold’ lesions on indium-111 white bloodcell scintigraphy. Semin Nucl Med 1992; 22:292–294.
39 Seabold JE, Nepola JV, Marsh JL, Hawes DR, Justin EP, Ponto JA, et al.Postoperative bone marrow alterations: potential pitfalls in the diagnosis ofosteomyelitis with 111In-labeled leukocyte scintigraphy. Radiology 1991;180:741–747.
40 Seabold JE, Forstrom LA, Schauwecker DS, Brown ML, Datz FL, McAfee JG,et al. Procedure guideline for indium-111-leucocyte for suspected infection/inflammation. Society of Nuclear Medicine. J Nucl Med 1997; 6:997–1001.
41 Datz FL, Thorne DA. Cause and significance of cold bone defects on indium-111-labeled leucocyte imaging. J Nucl Med 1987; 28:820–823.
42 Palestro CJ, Kim CK, Swyer AJ, Capozzi JD, Solomon RW, Goldsmith SJ.Total-hip arthroplasty: periprosthetic indium111-labeled leukocyte activityand complementary technetium-99m–sulfur colloid imaging in suspectedinfection. J Nucl Med 1990; 31:1950–1955.
43 Prandini N, Feggi LM, Massari L. 99mTc-HMPAO-WBC three phasesscintigraphy in secondary osteomyelitis.Q J Nucl Med 1996; 40(suppl 1):55.
44 Prandini N, Feggi L, Panareo S, Massari L, Galla A, Penazzi V. Leukocytescintigraphy with 99mTc-HMPAO a ten years experience. Nucl MedCommun 1999; 20, 10:970.
45 Datz FL, Thorne DA. Effect of antibiotic therapy on sensitivity of 111In-labeledleukocytes scans. J Nucl Med 1986; 27:1849–1853.
46 Lew DP, Waldvogel FA. Use of quinolones in osteomyelitis and infectedorthopaedic prosthesis. Drugs 1999; 58(suppl 2):85–91.
47 Galanakis N, Giamarellou H, Moussas T, Dounis E. Chronic osteomyelitiscaused by multiresistant Gram-negative bacteria: evaluation of treatmentwith newer quinolones after prolonged follow-up. J Antimicrob Chemother1997; 39:241–246.
48 Marone P, Concia E, Andreoni M, Suter F, Cruciani M. Treatment of boneand soft tissue infections with teicoplanin. J Antimicrob Chemother 1990;25:435–439.
49 Lovering AM, Zhang J, Bannister GC, Lankester BJ, Brown JH, Narendra G,MacGowan AP. Penetration of linezolid into bone, fat, muscle andhaematoma of patients undergoing routine hip replacement. J AntimicrobChemother 2002; 50:73–77.
50 Birmingham MC, Rayner CR, Meagher AK, Flavin SM, Batts DH, SchentagJJ. Linezolid for the treatment of multidrug-resistant, gram-positive infections:experience from a compassionate-use program. Clin Infect Dis 2003;36:159–168. E-pub 3 Jan 2003.
51 Rehm SJ, Graham DR, Srinath L, Prokocimer P, Richard MP, Talbot GH.Successful administration of quinupristin/dalfopristin in the outpatientsetting. J Antimicrob Chemother 2001; 47:639–645.
52 Summers M, Misenhimer GR, Antony SJ. Vancomycin-resistantEnterococcus faecium osteomyelitis: successful treatment withquinupristin–dalfopristin. South Med J 2001; 94:353–355.
53 Conrad DA, Williams RR, Couchman TL, Lentnek AL. Efficacy of aztreonamin the treatment of skeletal infections due to Pseudomonas aeruginosa. RevInfect Dis 1991; 13(suppl 7):S634–S639.
54 Mader JT, Shirtliff ME, Bergquist SC, Calhoun J. Antimicrobial treatment ofchronic osteomyelitis [Review]. Clin Orthop Relat Res 1999; 360:47–65.
55 Tice AD, Hoaglund PA, Shoultz DA. Outcomes of osteomyelitis amongpatients treated with outpatient parenteral antimicrobial therapy. Am J Med2003; 114:723–728.
56 Swiontkowski MF, Hanel DP, Vedder NB, Schwappach JR. A comparison ofshort- and long-term intravenous antibiotic therapy in the postoperativemanagement of adult osteomyelitis. J Bone Joint Surg Br 1999; 81:1046–1050.
57 Ceri H, Olson ME, Stremick C, Read RR, Morck D, Buret A. The CalgaryBiofilm Device: new technology for rapid determination of antibioticsusceptibilities of bacterial biofilms. J Clin Microbiol 1999; 37:1771.
58 Anderl JN, Zahller J, Roe F, Stewart PS. Role of nutrient limitation andstationary phase existence in Klebsiella pneumoniae biofilm resistance toampicillin and ciprofloxacin. Antimicrob Agents Chemother 2003; 47:1251–1256.
59 Buchholz HW, Elson RA, Hengelbrecht E, Lodenkaemper H, Roettger J,Siegel A. Management of deep infection of total hip replacement. J BoneJoint Surg 1981; 63-B:342–353.
60 Wilde AH, Ruth JT. Two stages reimplantation in infected total kneearthroplasty. Clin Orthop 1988; 236:23–35.
61 Ghisellini F, Ceffa R. Trattamento delle infezioni di protesi articolari. Roma:Mediprint Ed.; 1997.
62 Cerretani D, Giorgi G, Fornara P, Bocchi L, Neri L, Ceffa R, et al. The ‘invitro’ elution characteristics of vancomycin combined with imipenem–cilastatin in acrylic bone cements: A pharmacokinetic study. J Arthroplast2002; 17:5.
63 Gomis M, Barberan J, Sanchez B, Khorrami S, Borja J, Garcia-Barbal J. Oralofloxacin versus parenteral imipenem–cilastatin in the treatment ofosteomyelitis. Rev Esp Quimioter 1999; 12:244–249.
64 Mader JT, Ortiz M, Calhoun JH. Update on the diagnosis and management ofosteomyelitis [Review]. Clin Podiatr Med Surg 1996; 13:701–724.
65 Boutin RD, Brossmann J, Sartoris DJ, Reilly D, Resnick D. Update onimaging of orthopaedic infections. Orthop Clin North Am 1998; 29:41–66.
66 Atkinson RN, Paterson DC, Morris LL, Savage JP. Bone scintigraphy indiscitis and related disorders in children. Aust NZ J Surg 1978; 48:374–377.
67 Lazzeri E, Manca M, Molea N, Marchetti S, Consoli V, Bodei L, et al. Clinicalvalidation of the avidin/indium-111 biotin approach for imaging infection/inflammation in orthopaedic patients. Eur J Nucl Med 1999; 26:606–614.
68 De Winter F, Gemmel F, Van Laere K, De Winter O, Poffijn B, Dierckx RA,Van de Wiele C. 99mTc-ciprofloxacin planar and tomographic imaging for thediagnosis of infection in the postoperative spine: experience in 48 patients.Eur J Nucl Med Mol Imaging 2004; 31:233–239.
69 Gratz S, Dorner J, Oestmann JW, Opitz M, Behr T, Meller J, et al. 67Ga-citrate and 99Tcm-MDP for estimating the severity of vertebral osteomyelitis.Nucl Med Commun 2000; 21:111–120.
70 Lazzeri E, Pauwels EK, Erba PA, Volterrani D, Manca M, Bodei L, et al.Clinical feasibility of two-step streptavidin/111In-biotin scintigraphy inpatients with suspected vertebral osteomyelitis. Eur J Nucl Med MolImaging 2004; 31:1505–1511. E-pub 6 July 2004.
71 Love C, Patel M, Lonner BS, Tomas MB, Palestro CJ. Diagnosing spinalosteomyelitis: a comparison of bone and Ga-67 scintigraphy and magneticresonance imaging. Clin Nucl Med 2000; 25:963–977.
72 Prandini N, Feggi L, Panareo S, Ciprian A, Massari L, Galla A, et al. 99mTc-ciprofloxacin in the imaging of central bone infections. Nucl Med Commun2001; 22:1156–1157.
660 Nuclear Medicine Communications 2006, Vol 27 No 8
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Related Documents



![RESEARCH ARTICLE Open Access Staphylococcus aureus … · osteomyelitis [9-11], that clinical osteomyelitis isolates of S. aureus are capable of forming biofilms in vitro [12-14],](https://static.cupdf.com/doc/110x72/5e2dbd77b609da091e164f06/research-article-open-access-staphylococcus-aureus-osteomyelitis-9-11-that-clinical.jpg)







