This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Osteogenic uni- or bilateral form of the guided rapid maxillary expansion
K. AL-OUF, Head of the Oral and Maxillofacial Surgery Unit1, C. KRENKEL, Professor and Head of Oral and
Maxillofacial Surgery Department2, M. Y. HAJEER, Senior Lecturer in Orthodontics3, S. SAKKA, Senior Lecturer in
Oral and Maxillofacial Surgery3
1Central Police Hospital, Damascus, Syria; 2Paracelsus University, Muellner Hauptstr 48, 5020 Salzburg, Austria;3University of Albaath Dental School, Hamah, Syria
SUMMARY. Surgically assisted rapid palatal expansion is an important treatment procedure in patients with con-stricted maxillae. Several surgical methods have been proposed to expand the maxilla bilaterally. A new tech-nique was developed for performing a symmetric or asymmetric maxillary expansion guided by the stabilityof the mid-palatal area employing two osteotomy cuts on either side of mid-palatal suture. A Hyrax-type expan-sion device was used post-operatively. Seventeen patients were included in the study (9 males, 8 females) witha mean age of 30.7 years. Inter-canine and inter-molar widths were evaluated at three assessment intervals: be-fore treatment (T1), immediately after appliance removal (T2) and at six months follow-up (T3). Between T1 andT2, a mean expansion of 7.1 and 9.9 mm was achieved at the canine and molar areas, respectively. The amount ofrelapse measured between T2 and T3 was minimal (a mean value of 0.35 and 0.8 mm at the canine and molarareas, respectively). Asymmetric expansion was performed in 6 patients who exhibited unilateral skeletal con-striction at the initial assessment and these cases appeared stable at T3. The surgical approach described inthe current study enabled rapid maxillary expansion of unilateral and bilateral skeletal constriction cases effec-tively and with good stability. � 2009 European Association for Cranio-Maxillo-Facial Surgery
Keywords: rapid maxillary expansion, palatal osteogenesis, asymmetric expansion
INTRODUCTION
Expansion of the upper jaw cannot be performed by theuse of traditional orthodontic appliances (e.g. Haas orHyrax appliances) when the mid-palatal suture becomestotally ossified (Moss, 1986). Therefore, osteotomiesare indicated to facilitate expansion movements and toavoid overloading the teeth which may be accompaniedby bone resorption (Moss, 1968).
Hippocrates was the first to write about the constrictedupper jaw (Lindorf, 2006). From 1730, several appli-ances were utilized to expand the maxilla. In 1860, DrAngell accomplished a conservative and non-surgicalmaxillary expansion procedure (Angell, 1860). Derichs-weiler described the same procedure in 1950 (Derichs-weiler, 1953, 1958). ‘Rapid’ maxillary expansion wasfirst used and popularized by Haas who employed thistechnique in the treatment of patients with constrictedmaxillary jaws (Haas, 1961, 1980).
For a long time, it has been thought that the median pal-atal suture is the area most resistant to maxillary expan-sion (Morselli, 1997). It has been shown that othersutures might play a similar role to the median palatal su-ture (Isaacson and Murphy, 1964; Isaacson et al., 1969).Several studies demonstrated that the fronto-maxillary,zygomatico-maxillary and pterygo-maxillary sutureswere resistant areas for maxillary expansion procedures(Lines, 1975; Bell and Jacobs, 1979). One study stressedthat the maximum resistance to maxillary expansion camefrom the zygomatic arch (Wertz and Dreskin, 1977).
Steinhauser described a surgical technique in which anosteotomy similar to a Le Fort I osteotomy was per-formed for immediate maxillary widening. Bony seg-ments were moved apart and the resultant space wasfilled by transplanted autologous bone (Steinhauser,1972).
When reviewing the literature, several methods havebeen proposed to perform osteotomies on the maxillarycomplex for maxillary expansion. One of these methodsincluded an osteotomy extending from the piriform aper-ture to the maxillary tuberosity. Expansion could be thenexecuted by ordinary skeletal screws (Timms and Vero,1981). Another method was dependent on an osteotomyin the zygomatic process in conjunction with an osteot-omy in the palatal area (Kaban, 1984), whereas Zoellerand Ullrich performed an osteotomy in zygomatico-max-illary process area in addition to the mid-palatal suture(Zoeller and Ullrich, 1991).
Glassman et al. performed an osteotomy in the facio-maxillary wall starting from the naso-frontal suture andending at the maxillary tuberosity (Glassman et al.,1984). When Schimming et al. applied this method ontheir patients, a case with a fracture in the alveolar ridgeof the maxillary bone was recorded due to the ossifica-tion of the mid-palatal suture (Schimming et al., 2000).
Bell and Epker performed a surgical cut similar to LeFort I osteotomy, in which all the facial bony structureswere cut in addition to the osteotomy that was performedin the mid-palatal suture area (Bell and Epker, 1976).Then expansion was accomplished gradually and bone
160
Journal of Cranio-Maxillo-Facial Surgery (2010) 38, 160e165
� 2009 European Association for Cranio-Maxillo-Facial Surgery
doi:10.1016/j.jcms.2009.03.011, available online at http://www.sciencedirect.com
Author's personal copy
deposited in a way similar to the osteogenesis proceduresdescribed by Ilizarov in medicine (the treatment of bonelengthening of ends) (Ilizarov, 1990; McCarthy et al.,1992).
Moreselli used a minor surgical procedure to performmaxillary expansion and thought that the mid-palatal su-ture did not play a primary role when expanding the max-illa (Morselli, 1997). When Mommaerts et al. applieda similar approach using endoscopically assisted corticot-omies to perform transpalatal osteodistraction, theyfound that the operative time as well as both percentageand nature of complications were similar to those experi-enced with ‘open-sky transpalatal distraction’ with lesspronounced oedema (Mommaerts et al., 2008).
Stroemberg and Holm, after a longitudinal follow-upof patients with maxillary expansion, found that the in-ter-molar width was increased by a mean amount of7.1 mm, whereas the inter-canine width was increaseda mean amount of 4.8 mm. They found that the mid-pal-atal suture might remain unossified for a long time(Stromberg and Holm, 1995).
Lindorf applied selective weakening procedures to thefacial bones and used mini-plates to create what could becalled ‘semi-stabilization’. In addition, he employed in-ter-maxillary elastics to guide the expansion procedure(Lindorf, 2006).
It has been noted from the literature review that severalsurgical approaches to maxillary expansion as well asseveral opinions about the most suitable lines of osteoto-mies have been proposed. The aim of the current paper isto describe and evaluate a modification of the conven-tional method of surgically assisted rapid maxillary ex-pansion by the application of two osteotomies on eitherside of the mid-palatal suture which is followed by ordi-nary maxillary widening and bone formation. This tech-nique is referred to as ‘‘Osteogenic Uni- or BilateralForm of Rapid Maxillary Expansion’’ (OUF-RME).
MATERIALS AND METHODS
Subjects
Seventeen patients (8 females and 9 males) with skeletaltransverse discrepancies in the maxilla were treated be-tween 2005 and 2008 at the Department of Oral andMaxillofacial Surgery at Paracelsus Medical University,Salzburg (Austria) as well as at the Department of Oraland Maxillofacial Surgery at Police Hospital in Damas-cus (Syria). The average patient age was 30.7 years.Mandibular prognathism was diagnosed in 13 patientswhereas maxillary retrognathism occurred in 12 patients,with 8 patients being diagnosed as having both skeletalabnormalities. All patients exhibited skeletal posteriorcrossbite either uni- or bilaterally. Orthodontic bracketswere placed on the anterior teeth in 14 cases pre-opera-tively, whereas 3 cases just underwent orthodontic treat-ment post-operatively.
Ligation options between the upper six teeth dependedon the treatment plan. A Hyrax-type expansion appliancewas used with four bands on the upper first premolarsand upper first molars.
OUF-RME surgical technique
The procedure was performed under general anaesthesiaand local infiltration with a vasoconstrictor (Adrenaline,1:100,000 concentration) which was applied on both sidesof the oral vestibule. Oral intubation was used for generalanaesthesia since the surgical osteotomies were per-formed through the nasal cavity floor and not from the pal-atal area. The palatal mucosa was kept intact throughoutthe procedure. An incision was made in the mucosal mem-brane and the periosteum in the depth of the vestibule.This incision extended from the first molar on the rightside to the first molar on the other side. Soft tissueswere dissected at the canine fossa as well as the maxillarytuberosity. Dissection was also made along the floor of thenasal cavity towards the soft palate. Intra-operatively, thepatient was given intravenous antibiotics.
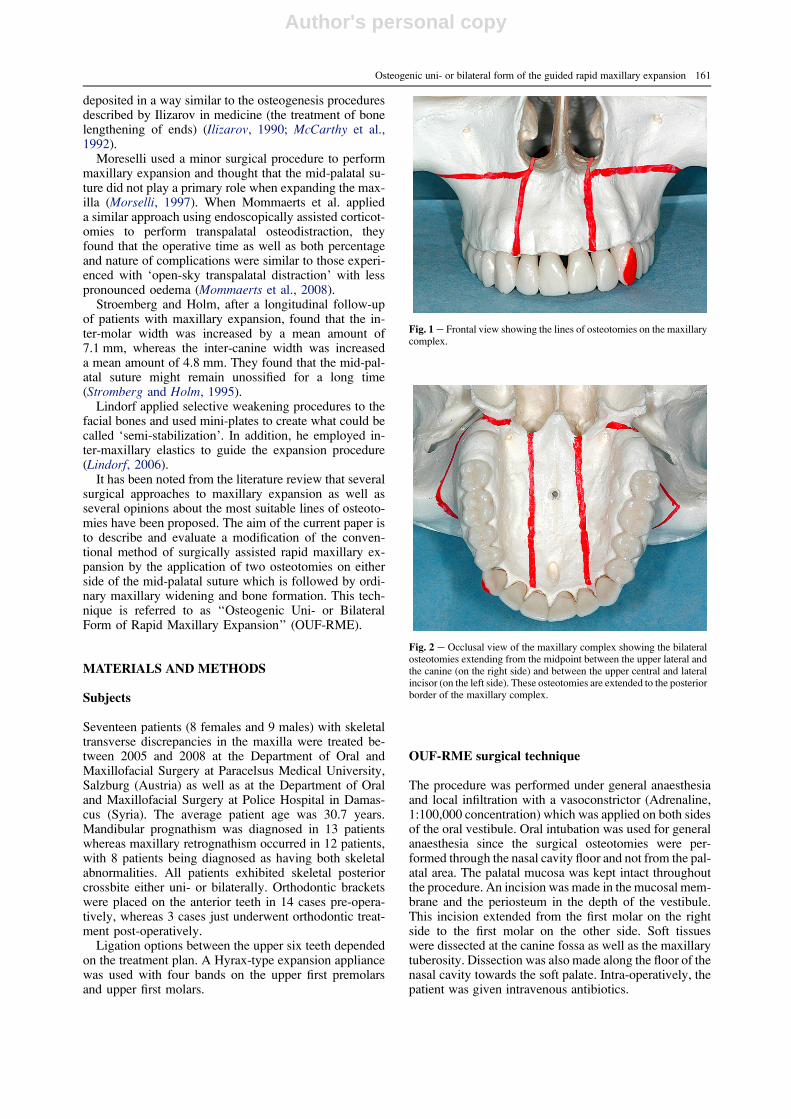
Fig. 1 e Frontal view showing the lines of osteotomies on the maxillarycomplex.
Fig. 2 e Occlusal view of the maxillary complex showing the bilateralosteotomies extending from the midpoint between the upper lateral andthe canine (on the right side) and between the upper central and lateralincisor (on the left side). These osteotomies are extended to the posteriorborder of the maxillary complex.
Osteogenic uni- or bilateral form of the guided rapid maxillary expansion 161
Author's personal copy
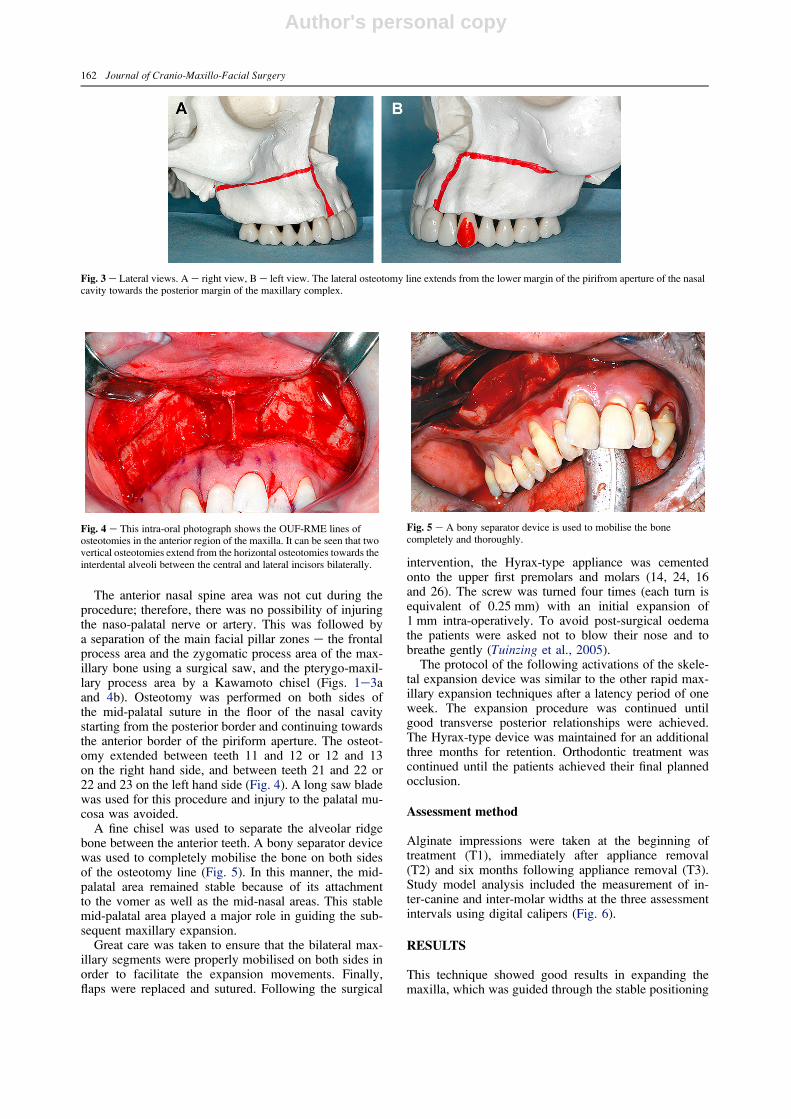
The anterior nasal spine area was not cut during theprocedure; therefore, there was no possibility of injuringthe naso-palatal nerve or artery. This was followed bya separation of the main facial pillar zones e the frontalprocess area and the zygomatic process area of the max-illary bone using a surgical saw, and the pterygo-maxil-lary process area by a Kawamoto chisel (Figs. 1e3aand 4b). Osteotomy was performed on both sides ofthe mid-palatal suture in the floor of the nasal cavitystarting from the posterior border and continuing towardsthe anterior border of the piriform aperture. The osteot-omy extended between teeth 11 and 12 or 12 and 13on the right hand side, and between teeth 21 and 22 or22 and 23 on the left hand side (Fig. 4). A long saw bladewas used for this procedure and injury to the palatal mu-cosa was avoided.
A fine chisel was used to separate the alveolar ridgebone between the anterior teeth. A bony separator devicewas used to completely mobilise the bone on both sidesof the osteotomy line (Fig. 5). In this manner, the mid-palatal area remained stable because of its attachmentto the vomer as well as the mid-nasal areas. This stablemid-palatal area played a major role in guiding the sub-sequent maxillary expansion.
Great care was taken to ensure that the bilateral max-illary segments were properly mobilised on both sides inorder to facilitate the expansion movements. Finally,flaps were replaced and sutured. Following the surgical
intervention, the Hyrax-type appliance was cementedonto the upper first premolars and molars (14, 24, 16and 26). The screw was turned four times (each turn isequivalent of 0.25 mm) with an initial expansion of1 mm intra-operatively. To avoid post-surgical oedemathe patients were asked not to blow their nose and tobreathe gently (Tuinzing et al., 2005).
The protocol of the following activations of the skele-tal expansion device was similar to the other rapid max-illary expansion techniques after a latency period of oneweek. The expansion procedure was continued untilgood transverse posterior relationships were achieved.The Hyrax-type device was maintained for an additionalthree months for retention. Orthodontic treatment wascontinued until the patients achieved their final plannedocclusion.
Assessment method
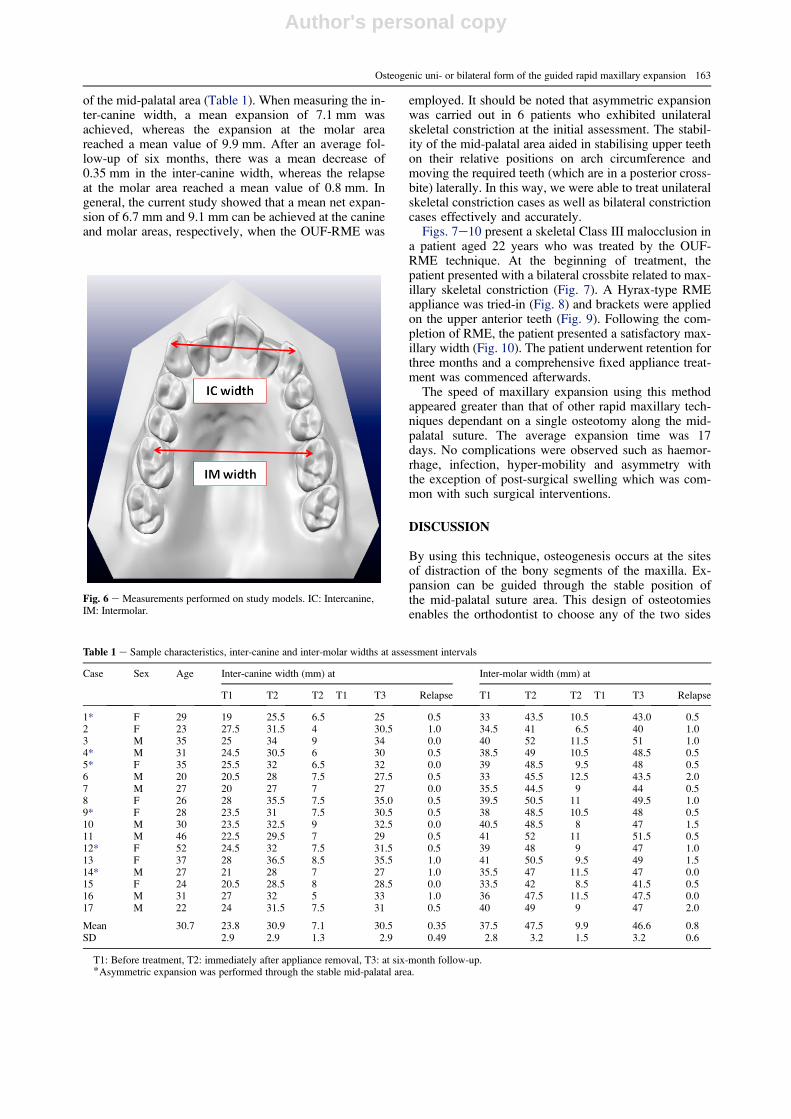
Alginate impressions were taken at the beginning oftreatment (T1), immediately after appliance removal(T2) and six months following appliance removal (T3).Study model analysis included the measurement of in-ter-canine and inter-molar widths at the three assessmentintervals using digital calipers (Fig. 6).
RESULTS
This technique showed good results in expanding themaxilla, which was guided through the stable positioning
Fig. 3 e Lateral views. A e right view, B e left view. The lateral osteotomy line extends from the lower margin of the pirifrom aperture of the nasalcavity towards the posterior margin of the maxillary complex.
Fig. 4 e This intra-oral photograph shows the OUF-RME lines ofosteotomies in the anterior region of the maxilla. It can be seen that twovertical osteotomies extend from the horizontal osteotomies towards theinterdental alveoli between the central and lateral incisors bilaterally.
Fig. 5 e A bony separator device is used to mobilise the bonecompletely and thoroughly.
162 Journal of Cranio-Maxillo-Facial Surgery
Author's personal copy
of the mid-palatal area (Table 1). When measuring the in-ter-canine width, a mean expansion of 7.1 mm wasachieved, whereas the expansion at the molar areareached a mean value of 9.9 mm. After an average fol-low-up of six months, there was a mean decrease of0.35 mm in the inter-canine width, whereas the relapseat the molar area reached a mean value of 0.8 mm. Ingeneral, the current study showed that a mean net expan-sion of 6.7 mm and 9.1 mm can be achieved at the canineand molar areas, respectively, when the OUF-RME was
employed. It should be noted that asymmetric expansionwas carried out in 6 patients who exhibited unilateralskeletal constriction at the initial assessment. The stabil-ity of the mid-palatal area aided in stabilising upper teethon their relative positions on arch circumference andmoving the required teeth (which are in a posterior cross-bite) laterally. In this way, we were able to treat unilateralskeletal constriction cases as well as bilateral constrictioncases effectively and accurately.
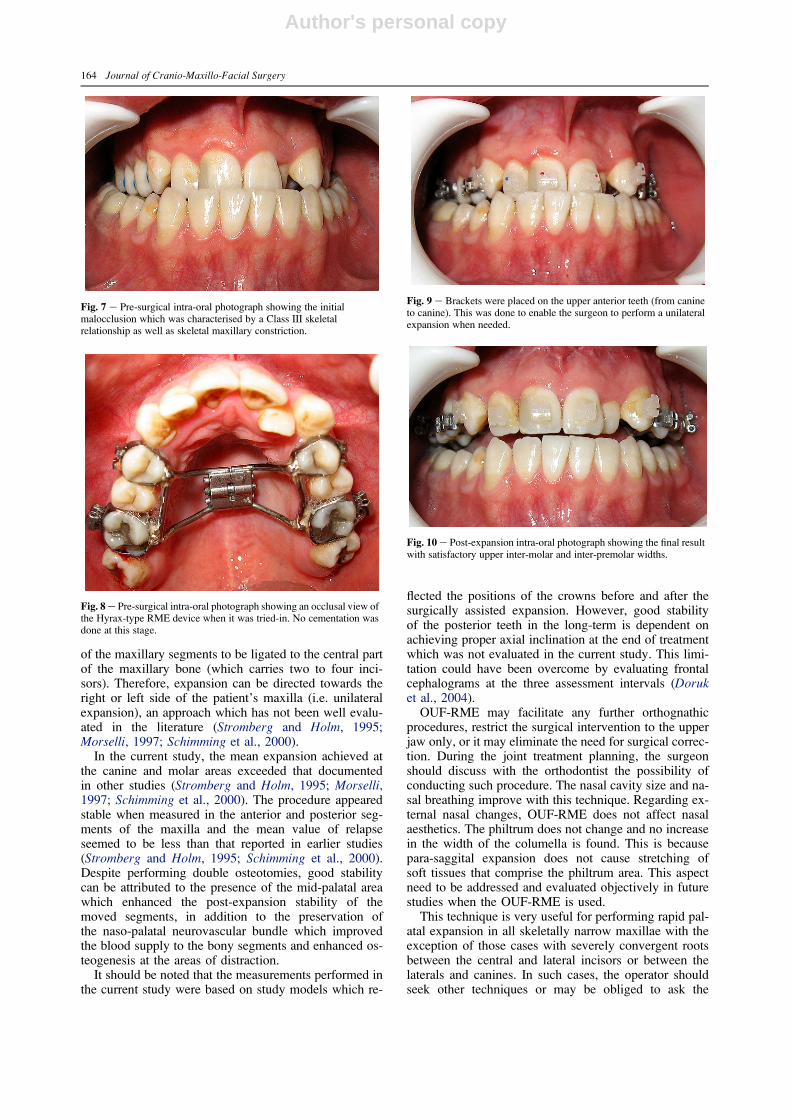
Figs. 7e10 present a skeletal Class III malocclusion ina patient aged 22 years who was treated by the OUF-RME technique. At the beginning of treatment, thepatient presented with a bilateral crossbite related to max-illary skeletal constriction (Fig. 7). A Hyrax-type RMEappliance was tried-in (Fig. 8) and brackets were appliedon the upper anterior teeth (Fig. 9). Following the com-pletion of RME, the patient presented a satisfactory max-illary width (Fig. 10). The patient underwent retention forthree months and a comprehensive fixed appliance treat-ment was commenced afterwards.
The speed of maxillary expansion using this methodappeared greater than that of other rapid maxillary tech-niques dependant on a single osteotomy along the mid-palatal suture. The average expansion time was 17days. No complications were observed such as haemor-rhage, infection, hyper-mobility and asymmetry withthe exception of post-surgical swelling which was com-mon with such surgical interventions.
DISCUSSION
By using this technique, osteogenesis occurs at the sitesof distraction of the bony segments of the maxilla. Ex-pansion can be guided through the stable position ofthe mid-palatal suture area. This design of osteotomiesenables the orthodontist to choose any of the two sides
Fig. 6 e Measurements performed on study models. IC: Intercanine,IM: Intermolar.
Table 1 e Sample characteristics, inter-canine and inter-molar widths at assessment intervals
Case Sex Age Inter-canine width (mm) at Inter-molar width (mm) at
T1 T2 T2� T1 T3 Relapse T1 T2 T2� T1 T3 Relapse
1* F 29 19 25.5 6.5 25 �0.5 33 43.5 10.5 43.0 �0.52 F 23 27.5 31.5 4 30.5 �1.0 34.5 41 6.5 40 �1.03 M 35 25 34 9 34 0.0 40 52 11.5 51 �1.04* M 31 24.5 30.5 6 30 �0.5 38.5 49 10.5 48.5 �0.55* F 35 25.5 32 6.5 32 0.0 39 48.5 9.5 48 �0.56 M 20 20.5 28 7.5 27.5 �0.5 33 45.5 12.5 43.5 �2.07 M 27 20 27 7 27 0.0 35.5 44.5 9 44 �0.58 F 26 28 35.5 7.5 35.0 �0.5 39.5 50.5 11 49.5 �1.09* F 28 23.5 31 7.5 30.5 �0.5 38 48.5 10.5 48 �0.510 M 30 23.5 32.5 9 32.5 0.0 40.5 48.5 8 47 �1.511 M 46 22.5 29.5 7 29 �0.5 41 52 11 51.5 �0.512* F 52 24.5 32 7.5 31.5 �0.5 39 48 9 47 �1.013 F 37 28 36.5 8.5 35.5 �1.0 41 50.5 9.5 49 �1.514* M 27 21 28 7 27 �1.0 35.5 47 11.5 47 0.015 F 24 20.5 28.5 8 28.5 0.0 33.5 42 8.5 41.5 �0.516 M 31 27 32 5 33 1.0 36 47.5 11.5 47.5 �0.017 M 22 24 31.5 7.5 31 �0.5 40 49 9 47 �2.0
Mean 30.7 23.8 30.9 7.1 30.5 �0.35 37.5 47.5 9.9 46.6 �0.8SD 2.9 2.9 1.3 2.9 0.49 2.8 3.2 1.5 3.2 0.6
T1: Before treatment, T2: immediately after appliance removal, T3: at six-month follow-up.*Asymmetric expansion was performed through the stable mid-palatal area.
Osteogenic uni- or bilateral form of the guided rapid maxillary expansion 163
Author's personal copy
of the maxillary segments to be ligated to the central partof the maxillary bone (which carries two to four inci-sors). Therefore, expansion can be directed towards theright or left side of the patient’s maxilla (i.e. unilateralexpansion), an approach which has not been well evalu-ated in the literature (Stromberg and Holm, 1995;Morselli, 1997; Schimming et al., 2000).
In the current study, the mean expansion achieved atthe canine and molar areas exceeded that documentedin other studies (Stromberg and Holm, 1995; Morselli,1997; Schimming et al., 2000). The procedure appearedstable when measured in the anterior and posterior seg-ments of the maxilla and the mean value of relapseseemed to be less than that reported in earlier studies(Stromberg and Holm, 1995; Schimming et al., 2000).Despite performing double osteotomies, good stabilitycan be attributed to the presence of the mid-palatal areawhich enhanced the post-expansion stability of themoved segments, in addition to the preservation ofthe naso-palatal neurovascular bundle which improvedthe blood supply to the bony segments and enhanced os-teogenesis at the areas of distraction.
It should be noted that the measurements performed inthe current study were based on study models which re-
flected the positions of the crowns before and after thesurgically assisted expansion. However, good stabilityof the posterior teeth in the long-term is dependent onachieving proper axial inclination at the end of treatmentwhich was not evaluated in the current study. This limi-tation could have been overcome by evaluating frontalcephalograms at the three assessment intervals (Doruket al., 2004).
OUF-RME may facilitate any further orthognathicprocedures, restrict the surgical intervention to the upperjaw only, or it may eliminate the need for surgical correc-tion. During the joint treatment planning, the surgeonshould discuss with the orthodontist the possibility ofconducting such procedure. The nasal cavity size and na-sal breathing improve with this technique. Regarding ex-ternal nasal changes, OUF-RME does not affect nasalaesthetics. The philtrum does not change and no increasein the width of the columella is found. This is becausepara-saggital expansion does not cause stretching ofsoft tissues that comprise the philtrum area. This aspectneed to be addressed and evaluated objectively in futurestudies when the OUF-RME is used.
This technique is very useful for performing rapid pal-atal expansion in all skeletally narrow maxillae with theexception of those cases with severely convergent rootsbetween the central and lateral incisors or between thelaterals and canines. In such cases, the operator shouldseek other techniques or may be obliged to ask the
Fig. 7 e Pre-surgical intra-oral photograph showing the initialmalocclusion which was characterised by a Class III skeletalrelationship as well as skeletal maxillary constriction.
Fig. 8 e Pre-surgical intra-oral photograph showing an occlusal view ofthe Hyrax-type RME device when it was tried-in. No cementation wasdone at this stage.
Fig. 9 e Brackets were placed on the upper anterior teeth (from canineto canine). This was done to enable the surgeon to perform a unilateralexpansion when needed.
Fig. 10 e Post-expansion intra-oral photograph showing the final resultwith satisfactory upper inter-molar and inter-premolar widths.
164 Journal of Cranio-Maxillo-Facial Surgery

Author's personal copy
orthodontist to perform some pre-surgical space creationfor interdental osteotomies.
CONCLUSION
The OUF-RME has been shown to be effective in per-forming uni- or bilateral rapid maxillary expansion in pa-tients with constricted maxillary bases. The achievedexpansion has been shown to be stable during follow-up.
References
Angell EH: Treatment of irregularities of the permanent or adult tooth.Dental Cosmos 1: 540e547, 1860
Bell WH, Epker BN: Surgical-orthodontic expansion of the maxilla.Am J Orthod 70(5): 517e528, 1976
Bell WH, Jacobs JD: Surgical-orthodontic correction of horizontalmaxillary deficiency. J Oral Surg 37(12): 897e902, 1979
Derichsweiler H: Die Gaumennaht Erweiterung. Fortschr Kieferorthop14: 405e415, 1953
Derichsweiler H: Die Gaumennaht Erweiterung. Stuttghart: HansaVerlag, 1958
Doruk C, Bicakci AA, Basciftci FA, Agar U, Babacan H: Acomparison of the effects of rapid maxillary expansion and fan-typerapid maxillary expansion on dentofacial structures. Angle Orthod74(2): 184e194, 2004
Glassman AS, Nahigian SJ, Midway JM, Aronowitz HI: Conservativesurgical orthdontic adult rapid palatal expansion: sixteen cases. AmJ Orthod 86: 207e213, 1984
Haas AJ: Rapid palatal expansion of the maxillary dental arch andnasal cavity by opening the midfacial sutures. Angle Orthod 31:73e90, 1961
Haas AJ: Long-term posttreatment evaluation of rapid palatalexpansion. Angle Orthod 50(3): 189e217, 1980
Ilizarov GA: Clinical application of the tension-stress effect for limblengthening. Clin Orthop Relat Res 250: 8e26, 1990
Isaacson RJ, Murphy D: Some effects of rapid maxillary expansion incleft lip and palate patients. Angle Orthod 34: 143e154, 1964
Isaacson RJ, Wood JL, Ingram AH: Forces produced by rapidmaxillary expansion. Angle Orthod 34: 256e269, 1969
Kaban LB: Surgical orthdontic correction of transverse maxillarydeficiency: a simplified approach, discussion. Plast Reconstr Surg73: 67e68, 1984
Lindorf H: Die chirurgisch gesteuerte maxillare expansion (GME) durchselektive Schwachung der Gesichtspfeiler. ZMK 22: 6e20, 2006
Lines PA: Adult rapid maxillary expansion with corticotomy. Am JOrthod 67(1): 44e56, 1975
McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH:Lengthening the human mandible by gradual distraction. PlastReconstr Surg 89(1): 1e8, 1992
Mommaerts MY, Collado J, Mareque BJ: Morbidity related to ‘‘endo-corticotomies’’ for transpalatal osteodistraction. J CraniomaxillofacSurg 36(4): 198e202, 2008
Morselli PG: Surgical maxillary expansion: a new minimally invasivetechnique. J Craniomaxillofac Surg 25(2): 80e84, 1997
Moss JP: Rapid expansion of the maxillary arch. II. Indications forrapid expansion. J Pract Orthod 2: 215e223, 1968
Moss JP: Rapid expansion of the maxillary arch. I. J Pract Orthod 2:165e171, 1986
Schimming R, Feller KU, Herzmann K, Eckelt U: Surgical andorthodontic rapid palatal expansion in adults using Glassman’stechnique: retrospective study. Br J Oral Maxillofac Surg 38(1):66e69, 2000
Steinhauser EW: Midline splitting of the maxilla for correction ofmalocclusion. J Oral Surg 30(6): 413e422, 1972
Stromberg C, Holm J: Surgically assisted, rapid maxillary expansion inadults. A retrospective long-term follow-up study.J Craniomaxillofac Surg 23(4): 222e227, 1995
Timms DJ, Vero D: The relationship of rapid maxillary expansion tosurgery with special reference to midpalatal synostosis. Br J OralSurg 19(3): 180e196, 1981
Tuinzing DB, Greebe RB, Dorenbos J, Van Der Kwast WAM: Surgicalorthodontics: diagnosis and treatment, Amsterdam: Harry RansomHumanities Research Center, 2005
Wertz R, Dreskin M: Midpalatal suture opening: a normative study.Am J Orthod 71(4): 367e381, 1977
Zoeller J, Ullrich H: Die Kombinierte chirurgischkieferorthopadischeGaumennahterweiterung im Erwachsenenalter. FortschrKieferorthop 52: 61e65, 1991
Dr K. AL-OUFP.O. Box 25821DamascusSyria
Tel.: +963 115419706Fax: +963 112221843E-mail: [email protected]
Paper received 9 November 2008Accepted 28 March 2009
Osteogenic uni- or bilateral form of the guided rapid maxillary expansion 165
Related Documents





![Welcome [iinfacts.cespu.pt]...Patients with Unilateral and Bilateral Maxillary Incisor Agenesis. Journal of Prosthodontics. 2015, 24:366-372. Acknowledgements: This work was supported](https://static.cupdf.com/doc/110x72/60fd8ead8cfd56001f53d0f4/welcome-patients-with-unilateral-and-bilateral-maxillary-incisor-agenesis.jpg)





