Spectrum of primary bone grafting in cranio maxillofacial trauma at a tertiary care centre in India Arun Kumar Singh, Devi Prasad Mohapatra 1 , Vijay Kumar Department of Plastic and reconstructive surgery, Chattrapati Shahuji Maharaj Medical University, Lucknow , Uttar Pradesh, 1 Department of Plastic Surgery, Jawaharlal Nehru Institute of Postgraduate Medical Education and Research, Puducherry, India Address for correspondence: Dr. Devi Prasad Mohapatra, Department of Plastic surgery, SS Block, JIPMER, Puducherry, 605006 E-mail: [email protected] ABSTRACT Background: In past several years, traumas following road traffic accidents and other causes have increased, owing to an increase in mechanization and pace of life. These patients frequently have complicated injuries involving soft tissue and the craniofacial skeleton. Assessment of bony injuries and loss of portions of facial skeleton and their management has proved to be a challenge to the reconstructive surgeon. Aims: Primary bone grafting of craniofacial skeletal injuries provides an opportunity for one stage correction of bony defects. The varied spectrum of primary bone grafts for management of craniomaxillofacial injuries are evaluated in this study. Materials and Methods: Patients with a history of acute trauma resulting in facial skeletal injuries with or without bone loss were included in the study. Primary bone grafting was undertaken in situations requiring contour correction, replacement of skeletal losses and for rigid fixation of fracture segments. Olecranon, Iliac crest, ribs, Vascularized as well as nonvascularized outer table calvarial grafts and nonvascularized inner table calvarial grafts were used in this study. Results: Sixty two patients of craniomaxillofacial injury following trauma requiring primary bone grafting were considered in this study. Fifty seven percent of patients (n=32) required primary bone grafting for replacement of bone loss while bone grafting for contour correction was done in twenty three patients. The parietal calvaria overlying the non-dominant hemisphere was used as a source of bone graft in forty-nine patients. Nearly ninety- two percent of the patients were satisfied with the results of primary bone grafting. Conclusions: Functional and aesthetic assessment of each of these patients, managed with primary bone grafting revealed a low rate of disabilities and high percentage of satisfaction in this study. KEY WORDS Bone plate; calvarial bone grafts; craniomaxillofacial trauma; facial fractures; primary bone grafting Original Article Access this article online Quick Response Code: Website: www.ijps.org DOI: 10.4103/0970-0358.81444 BACKGROUND T he incidence of trauma is on the rise and so are the mortality and morbidities associated with it. The aetiology of these injuries vary from road traffic accidents, gunshot injuries, domestic violence, homicidal assault, fall from heights, industrial accidents, Indian Journal of Plastic Surgery January-April 2011 Vol 44 Issue 1 29

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Spectrum of primary bone grafting in cranio maxillofacial trauma at a tertiary care centre in India
Arun Kumar Singh, Devi Prasad Mohapatra1, Vijay KumarDepartment of Plastic and reconstructive surgery, Chattrapati Shahuji Maharaj Medical University, Lucknow , Uttar Pradesh, 1Department of Plastic Surgery, Jawaharlal Nehru Institute of Postgraduate Medical Education and Research, Puducherry, India
Address for correspondence: Dr. Devi Prasad Mohapatra, Department of Plastic surgery, SS Block, JIPMER, Puducherry, 605006 E-mail: [email protected]
ABSTRACT
Background: In past several years, traumas following road traffic accidents and other causes have increased, owing to an increase in mechanization and pace of life. These patients frequently have complicated injuries involving soft tissue and the craniofacial skeleton. Assessment of bony injuries and loss of portions of facial skeleton and their management has proved to be a challenge to the reconstructive surgeon. Aims: Primary bone grafting of craniofacial skeletal injuries provides an opportunity for one stage correction of bony defects. The varied spectrum of primary bone grafts for management of craniomaxillofacial injuries are evaluated in this study. Materials and Methods: Patients with a history of acute trauma resulting in facial skeletal injuries with or without bone loss were included in the study. Primary bone grafting was undertaken in situations requiring contour correction, replacement of skeletal losses and for rigid fixation of fracture segments. Olecranon, Iliac crest, ribs, Vascularized as well as nonvascularized outer table calvarial grafts and nonvascularized inner table calvarial grafts were used in this study. Results: Sixty two patients of craniomaxillofacial injury following trauma requiring primary bone grafting were considered in this study. Fifty seven percent of patients (n=32) required primary bone grafting for replacement of bone loss while bone grafting for contour correction was done in twenty three patients. The parietal calvaria overlying the non-dominant hemisphere was used as a source of bone graft in forty-nine patients. Nearly ninety-two percent of the patients were satisfied with the results of primary bone grafting. Conclusions: Functional and aesthetic assessment of each of these patients, managed with primary bone grafting revealed a low rate of disabilities and high percentage of satisfaction in this study.
KEY WORDS
Bone plate; calvarial bone grafts; craniomaxillofacial trauma; facial fractures; primary bone grafting
Original Article
Access this article onlineQuick Response Code:
Website:
www.ijps.org
DOI:
10.4103/0970-0358.81444
BACKGROUND
The incidence of trauma is on the rise and so are the mortality and morbidities associated with it. The aetiology of these injuries vary from road
traffic accidents, gunshot injuries, domestic violence, homicidal assault, fall from heights, industrial accidents,
Indian Journal of Plastic Surgery January-April 2011 Vol 44 Issue 129

Singh et al.: Primary bone grafting in cranio maxillofacial trauma
and miscellaneous causes, including blast injuries from fire crackers and domestic gas cylinder bursts. These patients frequently have complicated injuries involving the soft tissue and the craniofacial skeleton. Earlier most of the injuries were under diagnosed and treated at local hospital levels. The extent of bony injuries could not be assessed properly and such patients presented late with the resultant complications. The results were most disastrous in children, where the undiagnosed and mistreated injuries resulted in severe facial abnormalities, because of the dynamic growing structural nature of the pediatric facial skeleton. A proper referral system with availability of tertiary level care, has today resulted in the timely intervention for all such injuries, with accurate diagnosis, comprehensive evaluation, and definitive management. Assessment of bony injuries and loss of portions of facial skeleton has proved to be a challenge to the plastic surgeon from the reconstruction point of view. Autogenous bone grafts have been used extensively in reconstructive surgery of the craniofacial region for a long time. The use of autogenous primary bone grafts for the management of bony injuries with contour defects or concomitant loss of skeleton is a more recent promising technique for the management of craniomaxillofacial injuries, in the acute setting. The advantages of using bone grafts are manifold. They help in the early restoration of bone volume, with correction of the deformity. The varied spectrum in the use of primary bone grafts during the management of craniofacial injuries has been evaluated in the present study.
MATERIALS AND METHODS
This study was conducted in the Department of Plastic and Reconstructive Surgery, of our hospital, in association with trauma centre. Sixty-two patients of craniomaxillofacial injuries were considered in this study from November 2007 to November 2009. All patients with a history of acute trauma resulting in facial soft tissue and skeletal fractures with or without bone loss were included in the study. Few patients were excluded from this study. These were, first, patients with associated multisystem trauma, including intra-abdominal, intra-thoracic, skeletal system, and intracranial injuries; second, patients with craniofacial injuries who had been managed previously with bone grafting and needed further management; third, patients with associated life-threatening illnesses including cardio-respiratory diseases, musculoskeletal pathologies, neurological diseases, and finally patients who did not give consent for the procedure.
A detailed preoperative assessment including a clinical
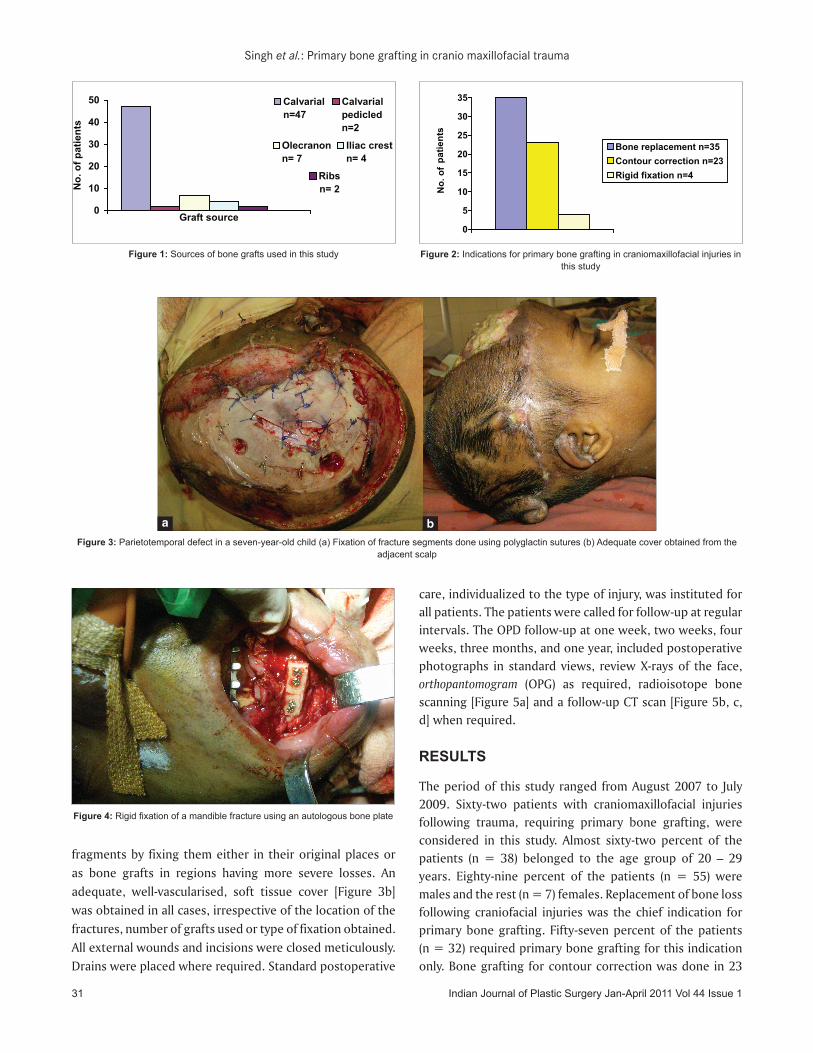
examination and radiological evaluation was carried out in each patient, to ascertain the need for primary bone grafting. The patients were operated under either general or loco-regional anesthesia depending on either the severity of the injury, age of the patient, or the expected duration of surgery. The fractures involving the faciomaxillary skeleton were approached through the existing lacerations, where present, or through standard incisions like subciliary, gingivobuccal sulcus or coronal in cases of closed injuries. Bone grafts were harvested from different sites including the calvaria, olecranon process of the ulna, ribs, and iliac crest using the standard approaches. Bone grafts in the form of vascularised as well as non-vascularised outer table calvarial grafts, non-vascularised inner table calvarial grafts, bone chips, bone dust, split ribs, and partial thickness olecranon grafts, were used for skeletal correction for patients in this study [Figure 1]. The inner table of the calvarium was harvested and used as a bone graft in patients having head injuries, who required concurrent cranioplasty. The calvarial bone graft was preferred in a majority of cases due to proximity to the affected site, abundance, and ease of harvest. Ribs were used as primary grafts where the cranial loss was extensive. The olecranon bone graft was preferred for the nasal dorsum overlay. The indications for primary bone grafting were correction of skeletal contour abnormalities, replacement of bone losses, and rigid fixation of the fracture segments [Figure 2]. These grafts were either placed as an onlay graft or an inlay graft without any rigid fixation, or with an interfragmentary fixation using stainless steel wiring, or delayed absorbable synthetic braided sutures (polyglactin 910) or screws and miniplates. The inlay graft method was used for covering the frontal and maxillary sinuses where comminution and bone loss of the anterior wall had occurred. Here the edges of the bone graft were just wedged into the margins of the sinus wall. Where the sinus wall fracture had resulted in comminution of the bone without any bone loss and only a contour defect, the bone graft was placed as an onlay without any fixation. By doing this, it was ensured that the bone graft was lying snugly in the soft tissue pocket in close contact to the bone. Interfragmentary fixation of bone chips in children was performed with polyglactin sutures [Figure 3a]. This obviated the need for removal of the hardware at a later date. Some fractures were reduced and skeletal stability was achieved with the bone graft fixed with screws to the fracture segments, where the bone graft behaved as an autologous bone plate. This method was utilized for unilateral mandibular body fractures [Figure 4]. In all patients with comminuted craniofacial fractures, an attempt was made to utilize the bone
Indian Journal of Plastic Surgery Jan-April 2011 Vol 44 Issue 1 30
Singh et al.: Primary bone grafting in cranio maxillofacial trauma
fragments by fixing them either in their original places or as bone grafts in regions having more severe losses. An adequate, well-vascularised, soft tissue cover [Figure 3b] was obtained in all cases, irrespective of the location of the fractures, number of grafts used or type of fixation obtained. All external wounds and incisions were closed meticulously. Drains were placed where required. Standard postoperative
care, individualized to the type of injury, was instituted for all patients. The patients were called for follow-up at regular intervals. The OPD follow-up at one week, two weeks, four weeks, three months, and one year, included postoperative photographs in standard views, review X-rays of the face, orthopantomogram (OPG) as required, radioisotope bone scanning [Figure 5a] and a follow-up CT scan [Figure 5b, c, d] when required.
RESULTS
The period of this study ranged from August 2007 to July 2009. Sixty-two patients with craniomaxillofacial injuries following trauma, requiring primary bone grafting, were considered in this study. Almost sixty-two percent of the patients (n = 38) belonged to the age group of 20 – 29 years. Eighty-nine percent of the patients (n = 55) were males and the rest (n = 7) females. Replacement of bone loss following craniofacial injuries was the chief indication for primary bone grafting. Fifty-seven percent of the patients (n = 32) required primary bone grafting for this indication only. Bone grafting for contour correction was done in 23
Figure 3: Parietotemporal defect in a seven-year-old child (a) Fixation of fracture segments done using polyglactin sutures (b) Adequate cover obtained from the adjacent scalp
a b
Figure 4: Rigid fixation of a mandible fracture using an autologous bone plate
Calvarial n=47
Calvarial pedicled n=2
Olecranon n= 7
Iliac crest n= 4
Ribsn= 2
0
10
20
30
40
50
Graft source
No.
of p
atie
nts
Figure 1: Sources of bone grafts used in this study
0
5
10
15
20
25
30
35
No.
of
patie
nts
Bone replacement n=35Contour correction n=23Rigid fixation n=4
Figure 2: Indications for primary bone grafting in craniomaxillofacial injuries in
this study
Indian Journal of Plastic Surgery Jan-April 2011 Vol 44 Issue 131

Singh et al.: Primary bone grafting in cranio maxillofacial trauma
patients. Contour correction was performed in patients having impacted zygomatic body fractures, comminuted fractures of the frontal region, and anterior wall maxillary fractures. A bone graft was used for the purpose of rigid fixation of fracture segments, as an autologous bone plate, in four patients. Two of these patients had unilateral mandibular body fractures, one had a segmental mandibular body fracture with bone loss, and one of these patients had a mandibular parasymphyseal fracture. Thirty-two percent of the patients (n = 20) were operated under regional and local anesthesia. Patients with extensive injuries, including panfacial fractures, and children and patients expected to have prolonged surgery were considered and taken up for surgery under general anesthesia. The parietal calvaria overlying the non-dominant hemisphere was used as a source of bone graft in 49 patients. Two of these were vascularised, based on the superficial temporal artery. The calvarial graft was harvested in a few patients from the inner table of the calvaria, removed during craniectomy for the management of associated intracranial injuries [Figure 6]. The olecranon bone grafts were preferred for nasal dorsum correction and used in seven patients. Split ribs were used as grafts for the correction of bone loss in the parietotemporal region, in
two patients. The iliac crest outer table cortical graft was used in four patients for either restoration of the contour or replacement of bone loss. In addition bone dust and bone chips obtained during cranial bone graft harvest were also utilized for resurfacing of the residual defects during surgery over the craniofacial skeleton [Figure 7].
Defects over the frontal region following comminuted fractures or bone loss in compounding injuries were replaced with calvarial outer table grafts [Figure 8]. Smaller parietotemporal defects were resurfaced with calvarial outer table non-vascularised grafts. In two patients, larger defects were replaced with split rib grafts [Figure 9]. In twelve patients, blowout fractures of the orbit were resurfaced with calvarial outer table non-vascularised grafts. The outer table of the ilium was used as a plate to resurface the orbital floor defect in one patient. Six calvarial outer table grafts were used to resurface contour defects of the zygoma, following impacted zygomatic fractures in patients presenting late. Of these, two were vascularised grafts based on the superficial temporal artery. Olecranon grafts were used in fractures involving the nasal dorsum. The outer table of the parietal calvaria was used for improving the dorsal nasal contour in two patients and for
a b
c dFigure 5: Postoperative photographs demonstrating (a) radionucleide (Tc99m
MDP) scanning at three months, demonstrating osteoblastic activity in the bone graft (Black Arrow) (b) CT scan image at one-year follow-up showing incorporation of the bone graft in the defect (White arrow), (c) and (d) 3-D reconstruction of the CT scan of the same patient in a one-year follow-up
Figure 6: Extracorporeal bone graft harvest from the inner table of the parietal calvarium in progress
Figure 7: Bone dust used as slurry to cover the residual defects following cranioplasty in acute craniofacial trauma
Indian Journal of Plastic Surgery Jan-April 2011 Vol 44 Issue 1 32

Singh et al.: Primary bone grafting in cranio maxillofacial trauma
replacement of bone loss over the maxillary anterior wall in one. Mandible body and parasymphseal fractures were fixed with contoured bone plates designed from the calvarial outer table and screws. Five calvarial outer table non-vascularised grafts were used for this purpose.
The incidence of donor site complications was eleven percent (n = 7). Bone graft donor site complications included pain over the donor site, contour defect, and fracture of the bone graft during harvest. Pain was most commonly associated with the ribs, iliac crest, and olecranon harvest. The contour defect was noted following the iliac crest harvest, while the graft fracture occurred during the calvarial graft harvest. Recipient-site complications included graft fracture, infection, contour abnormalities, and resorption. These were seen in
eight patients. The graft fracture was noted in patients during
a follow-up CT scan. Persistent infection in the recipient site
in one patient required graft and hardware removal. This
patient had a compound fracture of the mandibular body
opening into the skin, and had presented late. The average
postoperative hospital stay for frontal and parietal fractures
was seven days. Fractures located in the midface required a
hospital stay averaging 7 – 15 days. This was attributed to
the presence of associated injuries, tracheostomy or other
systemic injuries. Nearly ninety-two percent of the patients
were satisfied with the results [Figures 10 and 11].
Figure 9: A parietotemporal skeletal defect in an eight-year-old female child resurfaced with split rib grafts
Figure 10: Photographs showing (a) patient with a ten-day-old injury, showing ptosis and enopthalmos on the right side, (b) and (c) radiographs demonstrating complex comminuted fracture of the orbital floor, maxillary
wall, and zygoma (d) six-month follow-up photograph showing an improved functional and aesthetic result, with replacement of the orbital floor with
calvarial bone graft
Figure 8: Frontal defect in a adult male (7a) Primary calvarial outer table bone graft for resurfacing the defect, and (7b) Immediate postoperative result
a b
Figure 11: (a) Preoperative photograph of a patient with zygomaticomaxillary injury on the right side, (b) and (c upper) intraoperative photographs
demonstrating calvarial bone graft harvest and open reduction and internal fixation using the bone graft over the anterior maxillary wall, (c lower) schematic depiction of the outline of the bone graft (yellow arrow) and
miniplates and screws (red arrows), (d) and (e) postoperative views at the first week showing improved zygomatic projection and dental occlusion, (f) follow-up photograph at 18 months showing maintenance of the midface height and
aesthetic results
a
b
c
d
e f
a b
c d
Indian Journal of Plastic Surgery Jan-April 2011 Vol 44 Issue 133

Singh et al.: Primary bone grafting in cranio maxillofacial trauma
DISCUSSION
One of the earliest reports of bone grafting was in 1668; when Van Meekeren reported the use of canine calvarial bone to repair a cranial defect in a Russian soldier[1]. Ollier published his experiments with bone grafting and emphasized the importance of the periosteum[2]. Macewen demonstrated the use of autogenous rib grafts for the repair of mandible defects[2]. Barth suggested the term ‘creeping substitution’ as the method of osseous regeneration after bone grafting[3]. Mowlem popularized the use of cancellous bone grafting in various clinical conditions[4]. Mau_claire, in 1908, discussed the use of the ilium to correct skull bone defects. This procedure was later popularized by Dingman and Clintock.[5] The calvarium was first used as an osteocutaneous flap by Muller and Koning in 1890. In 1920, Lecene described the use of split skull grafts in cranial reconstruction. Tessier popularized several harvesting techniques and uses of calvarial grafts[3]. The use of bone grafts in the surgery of the face has been reviewed by Converse and Campbell,[6] and in the reconstruction of a defective mandible by Branemark.[7] Bone grafts are frequently required in the management of complex wounds of the face, whether for replacement of true loss of bone (avulsive injuries) or in cases wherein comminuted and misplaced fragments need to be replaced or reinforced.[8,9]
Several anatomical types of bone grafts are used in surgery. Most of these types of grafts have been discussed by Burwel (1994) and Czitrom and Gross (1992)[10,11]. Skull bone grafting has been used in primary and secondary correction deformities of the craniofacial areas.[8,9] The bone used for grafting may be cortical, cancellous or corticocancellous. The cancellous bone provides more space for faster revascularization. The cortical bone provides the best form of consolidation. The corticocancellous bone provides the best of both types of grafts[10,12]. The sources of bone grafts mentioned in various literatures include the ribs, iliac crest, calvarial bone, and tibia. Calvarial bone grafts can be developed into blocks, chips, paste, shaving grafts, and vascularised outer table grafts[8]. Blocks can be cut according to the defect to be reconstructed. Bone chips are harvested as particulate bone and placed into the defect[13]. Rapid vascularization is followed by solidification and incorporation of the graft. This process may take up to a year. The extracorporeal harvest of the bone graft from the inner table for craniofacial reconstruction, has limited mention in literature[14,15]. Greene and colleagues have harvested and utilized bone dust from the inner surface of the calvarial bone flap during cranioplasty, for coverage of
osseous defects[13]. Blocks of inner table grafts are harvested from the calvarial bone flap during cranioplasty and utilized to replace the missing bone. The frontal and upper cranial bone flaps are readily available sources for the inner table bone graft harvest, to restore continuity and contour of the frontal skeleton and orbital rim, as well as for facial skeletal reconstruction. The extracorporeal inner table calvarial bone graft harvest is not associated with the additional blood loss and other complications of the calvarial bone harvest like penetration of the inner table with dural puncture or inadvertent puncture of the dural venous sinuses, which leads to profuse hemorrhage. Bone paste can also be used to pack residual defects, cracks and crevices after bone grafting. Bone grafts have been used as autologous bone plates for the rigid fixation of fracture segments, especially in the mandible.[16]
Reconstruction of the facial skeleton with bone grafts gained popularity in World War I. The surgical dogma was against early or primary bone grafting and it stipulated waiting until soft tissue healing had occurred. More recently the use of bone grafts in the early setting has gained popularity. Gruss and colleagues have published extensively on their success with early bone grafting to stabilize and support soft tissues, and to decrease scar contracture and distortion.[17] At present, many surgeons advocate the use of primary bone grafting in the midface[17,18]. Some surgeons also advocate immediate bone grafting of mandible defects[19]. According to a recent study[20] high density porous polyethylene (HDPP) was a frequently utilized material for reconstruction in facial fractures, although it is not immediately clear whether HDPP had been utilized for reconstruction of the facial skeleton, in the acute setting, in this study. Immediate bone grafting for craniomaxillofacial trauma, helps in the early restoration of bone volume along with correction of the deformity and also reduces the need for reconstruction using synthetic materials at a later period. Primary bone grafting for craniofacial skeletal injuries appears to be a simple procedure, which could be accomplished with limited instrumentation in an emergency set-up in most of the patients. The functional and aesthetic assessment of each of the patients managed with immediate autologous bone grafting revealed a low rate of disabilities and high degree of satisfaction, in this study.
CONCLUSION
Immediate autologous bone grafting for the management of complex craniofacial skeletal injuries is an attractive option. The sources of autologous bone grafts are plenty. With the availability of such a modality in the armamentarium
Indian Journal of Plastic Surgery Jan-April 2011 Vol 44 Issue 1 34

Singh et al.: Primary bone grafting in cranio maxillofacial trauma
Source of Support: Nil, Conflict of Interest: None declared.
of the reconstructive surgeon, a vastly improved outcome in the management of craniofacial skeletal injuries can be expected.
REFERENCES
1. Macewen W. The growth of bone. New York: Glasgow J Maclehose and sons; 1912.
2. Shebadi SE. Skull reconstruction with bone dust. Br J Plast Surg 1970;23:227.
3. Tessier P. Autogenous bone grafts taken from the calvarium for facial and cranial applications. Clin Plast Surg 1982;9:531.
4. Mowlem R. Bone grafting. Br J Plast Surg 1963;16:293.5. Dingman R.O. Iliac bone cranioplasty. Plast Reconstr Surg,
1952, 9, 130-1396. Converse J.M., Campbell R.M. Bone grafts in surgery of the face,
Surg Clin North Am,1954, Apr, 375-4017. Branemark PI, Lindstrom J, Hallen O, Briene U, Jeppeson PH,
Ohman A. Reconstruction of the defective mandible. Scand J Plast Reconstr Surg 1975;9:116-28.
8. Jackson IT, Adham M, Bite U, Marx R. Update On cranial bone grafts in craniofacial surgery. Ann Plast Surg 1987;18:37.
9. Jackson IT, Helden G, Marx R. Skull bone grafts in maxillofacial and craniofacial surgery. J Oral Maxillofac Surg 1986;44:949-55.
10. Burwell RG. History of bone grafting and bone substitutes with special reference to osteogenic conduction. In: Urist MR, O’Connor BT, Burwell RG, editors. Bone grafts and derivatives. Oxford: Butterworth Heinemann; 1994.
11. Czitrom AA, Gross AE. Allografts in orthopaedics practice. Baltimore: Williams and Wilkins; 1992.
12. Clark N, Birely B, Manson PN, Slezak S, Kolk CV, Robertson B.
High energy ballistic and avulsive facial injuries: classification, patterns and an algorithm for primary reconstruction. Plast Reconstr Surg 1996;98:583-601.
13. Greene AK, Proctor M, Rogers GF. Primary grafting with autologous cranial particulate bone prevents osseus defects following frontoorbital advancement. Plast Reconstr Surg 2007;120:1603.
14. Singh AK, Mohapatra DP, Kumar V. The inner table calvarial bone graft harvest: A source of primary bone graft in the management of craniomaxillofacial skeletal injuries. Eur J Plast Surg 2010;33:297-301.
15. Jackson I. Commentary on “The inner table calvarial bone graft harvest: A source of primary bone graft in the management of craniomaxillofacial skeletal injuries”. Eur J Plast Surg 2010;33:305.
16. Singh AK, Mohapatra DP, Kumar V. Rigid internal fixation of mandibular fractures using autologous bone grafts: The autologous bone plate. Eur J Plast Surg 2010;33:163-7.
17. Gruss JS, Mackinnon SE, Kassell EE, Copper PW. The role of primary bone grafting in complex craniomaxillofacial trauma. Plast Reconstr Surg 1985;15:17-24.
18. Manson PN, Crawley WA, Yaremchuk MJ, Rochman GM, Hoopes JE, French JH Jr. Midface fractures: advantages of immediate extended open reduction and bone grafting. Plast Reconstr Surg 1985;76:1.
19. Kusiak JF, Zins JE, Whitaker LA. The early revascularization of membranous bone. Plast Reconstr Surg 1985;76:510-6.
20. Hwang K, You SH. Analysis of facial bone fractures: An 11- year study of 2094 patients. Indian J Plast Surg 2010;43:42-8.
Dispatch and return notification by E-mail The journal now sends email notification to its members on dispatch of a print issue. The notification is sent to those members who have provided their email address to the association/journal office. The email alerts you about an outdated address and return of issue due to incomplete/incorrect address.
If you wish to receive such email notification, please send your email along with the membership number and full mailing address to the editorial office by email.
Indian Journal of Plastic Surgery Jan-April 2011 Vol 44 Issue 135
Related Documents











