Oral Manifestations of Systemic Diseases Prepared By: Bawar Yahya Ahmed Muhammed Othman College of Dentistry University of Sulaimani

oral manifestation of systemic diseases
Jul 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Oral Manifestations of Systemic Diseases
Prepared By: Bawar Yahya Ahmed Muhammed Othman
College of DentistryUniversity of Sulaimani

• Outline– Endocrine Disorders– Blood Disorders– Immunodeficiency– Oral Manifestations of
Therapy for Oral Cancer– Effects of Drugs on the Oral
Cavity– Oral Manifestations of
Systemic Diseases

• The oral cavity is a mirror that reflects many of the human body's internal
secrets. Some of these manifestations are disease specific and may accompanied
many systemic diseases. It is very important to recognize them and provide
correct diagnosis.

Cardiovascular diseases • The classical risk factors for
cardiovascular disease:
• - hypertension,
• - hyper-cholesteroleamia,
• - cigarette smoking
• Two biological mechanisms that explain the relationship between cardiovascular disease and periodontal disease:
• – Bacteria from periodontal disease may enter the circulation and contribute directly to the atheromatous or thrombotic processes.
• – Systemic factors alter the immune inflammatory process involved in both periodontal and cardiovascular diseases.

Cardiovascular diseaseOral manifestations• Periodontal disease• Lichenoid stomatitis• Xerostomia• Gingival hyperplasia• Hemorrhagic complication

Cardiovascular diseaseOral manifestations• Periodontal disease Cardiovascular patients
with active periodontal disease are 1.5-2.7 more likely to experience a fatal cardiovascular event
-Increased inflammation-Increased bacteremia risk

Cardiovascular disease Oral manifestations
• Lichenoid stomatitis• Various cardiovascular drugs
may induce lichenoid lesions – oral discomfort
• Diuretics• B1-adrenergic blockers• ACE- inhibitors (angiotensin-
converting-enzyme inhibitors)

Cardiovascular diseaseOral manifestations
Dry mouth• Numerous cardiovascular drugs
may reduce salivary function:1. Diuretics2. B1-adrenergic blockers3. Centrally acting sympathetic
agonists• Synergistic affect with other
medications
Cardiovascular disease Oral manifestations• Gingival hyperplasia:1. Calcium-channel blockers are
commonly prescribed2. Gingival enlargement usually
apparent within 1-2 months of therapy
3. Tissue usually firm and painless
4. Overlying inflammation may occur

Cardiovascular diseaseOral manifestations• Hemorrhagic
complication:• Antithrombotic/anti-
coagulant agents increase the risk of
• -petechia(<2mm)• -purpura(>2mm-
<1cm)• -ecchymosis(>1cm)• -hemorrhage

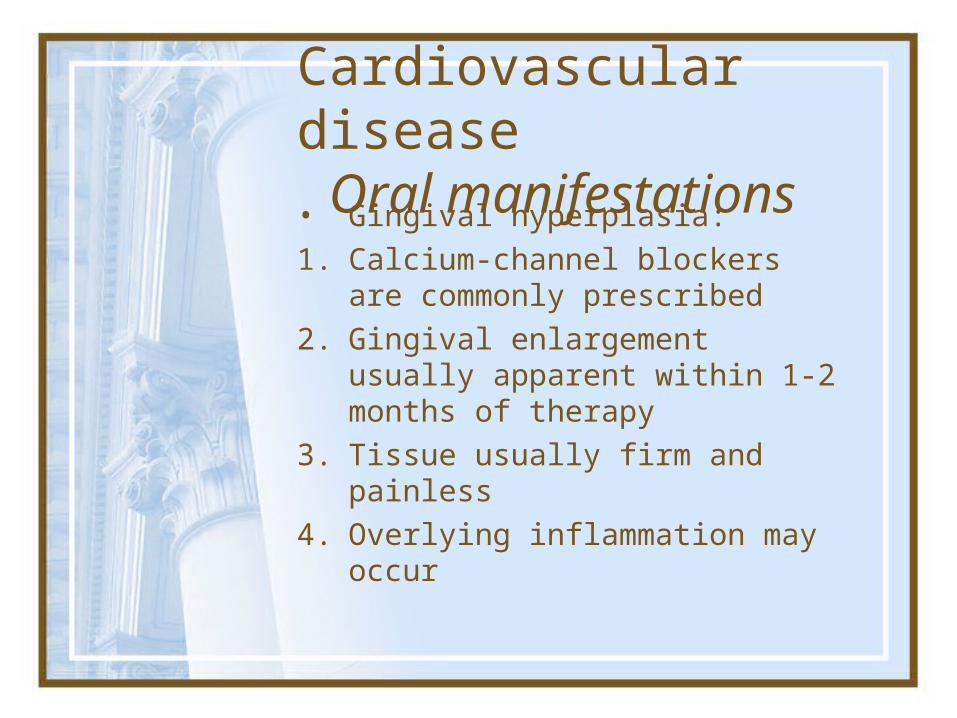
Gingival hyperplasia• Figure 1a: Photograph of a
32-year-old male patient at the time of presentation shows remarkable gingival hyperplasia. The gingival tissue between teeth 11 and 12 resembled an epulis.
• Extraoral examination showed excessive hairiness of the face.
• Desquamation was observed on the patient's back .

Endocrine Disorders
• Hyperpituitarism• Hyperthyroidism• Hypothyroidism• Hyperparathyroidism• Diabetes Mellitus• Addison Disease

Diabetes
• Type 1 diabetes is usually diagnosed in childhood. Many patients are diagnosed when they are older than age 20. In this disease, the body makes little or no insulin. Daily injections of insulin are needed. The exact cause is unknown. Genetics, viruses, and autoimmune problems may play a role.
• Type 2 diabetes is far more common than type 1. It makes up most of diabetes cases. It usually occurs in adulthood, but young people are increasingly being diagnosed with this disease. The pancreas does not make enough insulin to keep blood glucose levels normal, often because the body does not respond well to insulin. Many people with type 2 diabetes do not know they have it, although it is a serious condition. Type 2 diabetes is becoming more common due to increasing obesity and failure to exercise.

Risk factors for diabetes
• There are many risk factors for type 2 diabetes, including:
-Age over 45 years -A parent, brother, or sister with
diabetes -Gestational diabetes or delivering a
baby weighing more than 9 pounds -Heart disease -High blood cholesterol level -Obesity -Not getting enough exercise -Polycystic ovary disease (in women) -Previous impaired glucose tolerance
Diabetes mellitus presented with an ulcerating rash

Symptoms of diabetes
• Patients with type 1 diabetes usually develop symptoms over a short period of time. The condition is often diagnosed in an emergency setting
• Symptoms of type 1 diabetes:
1. Fatigue 2. Increased thirst 3. Increased urination 4. Nausea 5. Vomiting 6. Weight loss in spite
of increased appetite
• Type 2 diabetes develops slowly, some people with high blood sugar experience no symptoms at all.
• Symptoms of type 2 diabetes:
1. Blurred vision 2. Fatigue 3. Increased appetite 4. Increased thirst 5. Increased
urination

Oral lesions at diabetes
FIGURE 1. Lingual view of mandibular incisors of a 60-year-oldfemale with poorly controlled type 2 diabetes. The HbA1c value at initialexamination was 13.9%. Multiple periodontal abscesses (teeth 22, 23, 25,26, and 27) with severe inflammation and bone loss can be seen.
Figure 2. Radiograph of the same sextant shown in Figure 1.Severe bone loss can be noted on tooth 2.

Complications of Diabetes• 1. Eye Disease• 2. Kidney Disease• 3. Cardiovascular Disease• 4. Neuropathy• 5. Foot Problems• 6. Susceptibility to Dental
disease, especially periodontal (gum) infections.
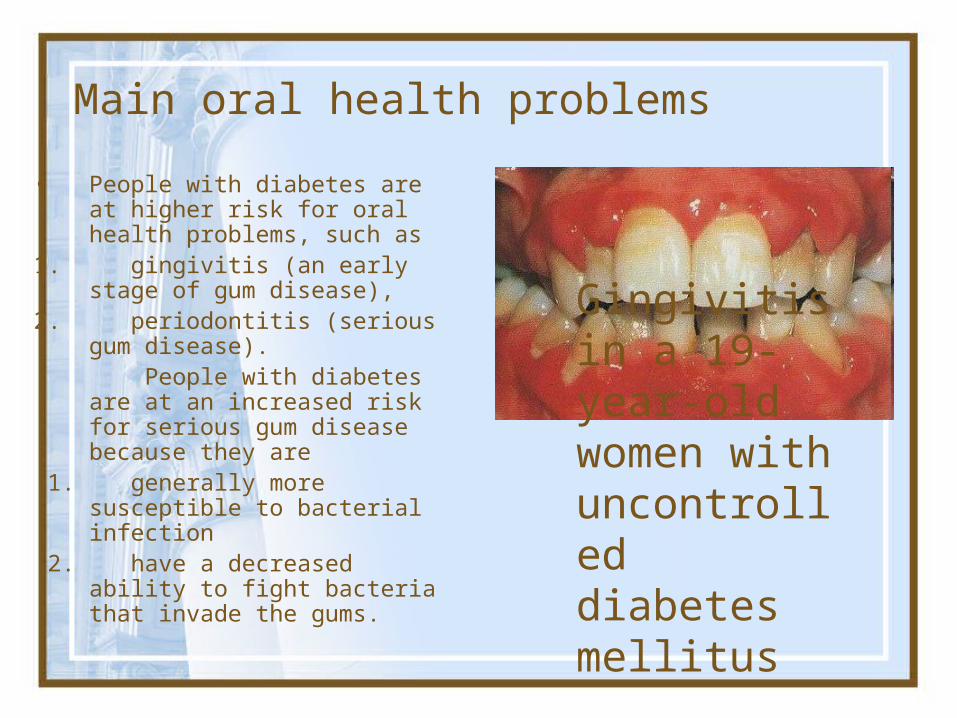
Main oral health problems
• People with diabetes are at higher risk for oral health problems, such as
1. gingivitis (an early stage of gum disease),
2. periodontitis (serious gum disease).
People with diabetes are at an increased risk for serious gum disease because they are
1. generally more susceptible to bacterial infection
2. have a decreased ability to fight bacteria that invade the gums.
Gingivitis in a 19-year-old women with uncontrolled diabetes mellitus

Other oral problems associated to diabetes include:
• thrush, • an infection
caused by fungus that grows in the mouth,
• dry mouth which can cause soreness, ulcers, infections and cavities.
Inflamed, papulonodular hyperplasia of the gingiva in a diabetic patient

Oral Complications of Diabetes
• Periodontitis• Increased rate of
dental caries• Xerostomia• Salivary
dysfunction• Burning mouth
and tongue • Candidiasis• Cheilosis• Glossodynia• Lichen Planus
• Oral changes associated with diabetes include cheilosis, mucosal drying, burning mouth and tongue, diminished salivary flow, alterations in the flora of the oral cavity and increased rate of dental caries. Periodontal changes include enlarged gingiva, sessile or pedunculated gingival polyps, polypoid gingival proliferations, abscess formation, periodontitis, and loosened teeth. Periodontal disease in diabetics follows no consistent or distinct pattern.

Clinical Features and Oral Manifestations of Hyperpituitarism
• Affects both men and women, most commonly during the fourth decade of life– Patients experience poor vision, light sensitivity,
enlargement of hands and feet, and an increase in rib size.
• Facial changes– Enlargement of maxilla and mandible may cause
separation of teeth and malocclusion.– Frontal bossing and an enlargement of nasal
bones may lead to deepening of voice.• Mucosal changes
– May have thickened lips and macroglossia

Clinical Features and Oral Manifestations of Hyperpituitarism (cont.)

Salivary Dysfunction & Xerostomia
• Salivary Hypofunction/ Dry mouth Dry mouth (xerostomia) occurs when the
salivary glands are not functioning properly resulting in decreased saliva. Saliva not only aids in digestion, but is a necessary factor in oral health because it also helps to keep your mouth moist and prevent tooth decay. Diabetic neuropathy can also affect the salivary glands.
• Polyuria
• Topical treatments:1. fluoride containing mouthrinses2. salivary substitutes

Periodontal Disease
• Increased prevalence of PerioDisease
• Decreased healing in poorly controlled DM
• Management of periodontal disease may help improve glycemic control

Dental Caries• Increased
prevalence of dental caries
• Salivary hyperglycemia

Oral Candidiasis
• Opportunistic fungal infection commonly associated with hyperglycemia.
• Salivary dysfunction compromise immune function.
• Salivary hyperglycemia provide substrate for fungal growth

Burning Mouth Syndrome
Burning mouth syndrome is a condition with no determined cause and is characterized by a chronic burning pain in your mouth. This burning sensation can be severe, feeling much the same as scalding and can affect the overall areas of your mouth such as your tongue, gums, lips, inside of your cheeks, and the roof of your mouth. Although BMS has no known cause and finding treatment may by difficult, most people can bring it under control by working with an oral health specialist.

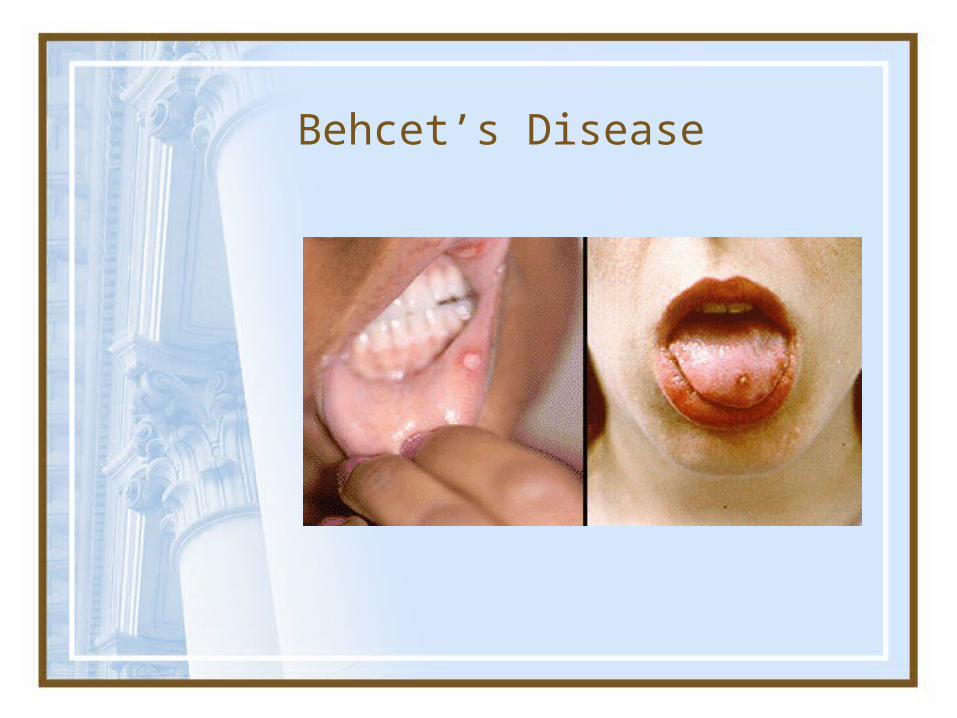
Behcet’s Syndrome
• Chronic multisystemic inflammatory disorder.• The exact cause is unclear, although an
immunogenetic basis is suggested.• It is more common in males (5–10 times), and
the onset is usually in the 20–30 years age group.
• Incidence in Asian/Middle Eastern countries - 1/10,000• Male to Female ratio 16-24:1• The major clinical diagnostic criteria for the
disease are: (a) Recurrent oral ulcerations (aphthae) (b) Recurrent genital ulcerations (c) Ocular lesions (conjunctivitis, reduced visual
acuity (d) Skin lesions (papules, pustules,ulcers)• The oral lesions are the herald of this disease
and are usually 6mm or smaller and resolve within 1-3 weeks. Aphthous ulcerations are the most common oral presentation

Clinical features• Minor clinical features may also be present, e. g.,
arthritis, arthralgia, vein thrombosis, arterial occlusion and aneurysms, central nervous system involvement, pulmonary, renal, and gastrointestinal manifestations.
• The diagnosis is mainly made on clinical grounds. For accurate diagnosis, recurrent oral ulcerations plus two of the other four major criteria must be present.
• Differential diagnosis Recurrent aphthous ulcers, erythema multiforme, Stevens–Johnson syndrome.
• Treatment– Tetracycline solution oral swish and swallow 4x daily has shown to
improve aphthous ulcers– Topical steroids for both oral and genital lesions– Systemic steroids have been shown to improve acute symptoms,
but do not slow progression or prevent recurrence• KEY TO DIAGNOSIS: Clinical

Behçet Disease

ADDISON'S DISEASE
• An Adrenal Cortical insufficiency.• This disease causes an increased
production of melanin, resulting in melanotic macules in the oral mucosa.
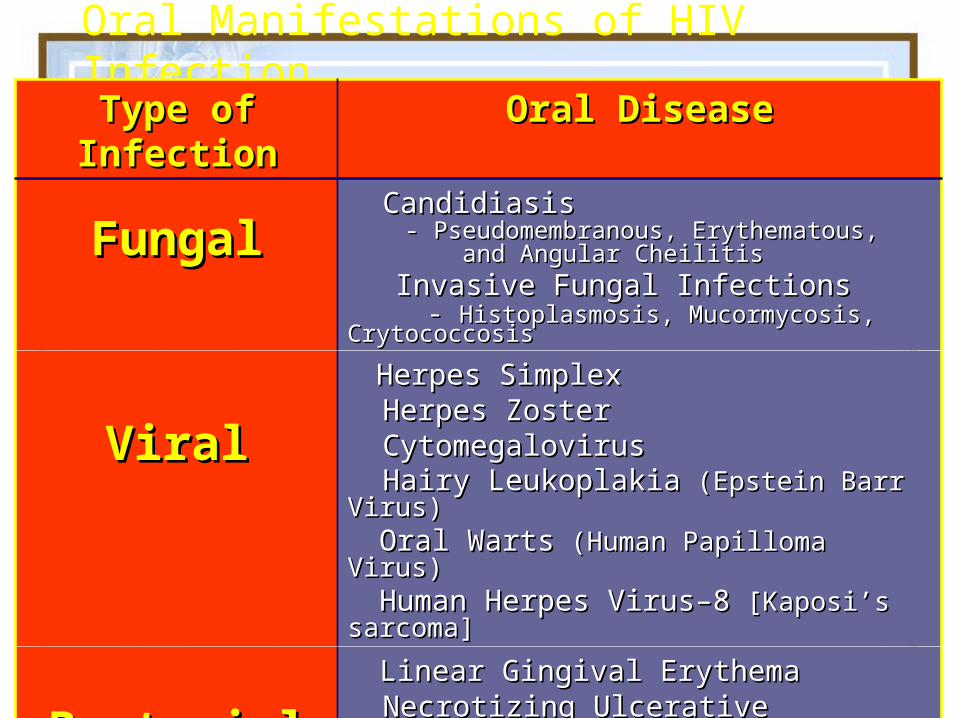
Oral Manifestations of HIV Infection
Type of Type of InfectionInfection
Oral DiseaseOral Disease
FungalFungal CandidiasisCandidiasis - Pseudomembranous, Erythematous, - Pseudomembranous, Erythematous, and Angular Cheilitisand Angular Cheilitis Invasive Fungal InfectionsInvasive Fungal Infections - - Histoplasmosis, Mucormycosis, Histoplasmosis, Mucormycosis, CrytococcosisCrytococcosis
ViralViral
Herpes SimplexHerpes Simplex Herpes ZosterHerpes Zoster CytomegalovirusCytomegalovirus Hairy LeukoplakiaHairy Leukoplakia (Epstein Barr Virus) (Epstein Barr Virus) Oral WartsOral Warts (Human Papilloma Virus) (Human Papilloma Virus) Human Herpes Virus–8Human Herpes Virus–8 [Kaposi’s [Kaposi’s sarcoma]sarcoma]
BacterialBacterial Linear Gingival ErythemaLinear Gingival Erythema Necrotizing Ulcerative PeriodontitisNecrotizing Ulcerative Periodontitis Tuberculosis* Tuberculosis* Mycobacterium avium complex*Mycobacterium avium complex* Bacillary angiomatosis*Bacillary angiomatosis*

Oral Manifestations of HIV Infection
Type of Type of LesionLesion
Oral DiseaseOral Disease
NeoplastNeoplast
icic
Kaposi’s Sarcoma (KS) [HHV-8]Kaposi’s Sarcoma (KS) [HHV-8]
LymphomaLymphoma
Squamous Cell Carcinoma*Squamous Cell Carcinoma*
OtherOther HIV-associated Necrotizing HIV-associated Necrotizing
UlcerationUlceration
HIV-Salivary Gland HIV-Salivary Gland Disease/XerostomiaDisease/Xerostomia
Immune Thrombocytopenic Immune Thrombocytopenic Purpura*Purpura*
Abnormalities of Mucosal Abnormalities of Mucosal PigmentationPigmentation

Fungal Infections: Candidiasis
• Pseudomembraneous Candidiasis
• White “curd-like” raised material that wipes off
• Erythematous / Atrophic Candidiasis
• Mucosal erythema and/or patchy depapillation of the tongue
• Hyperplastic Candidiasis• White/red hyperplastic lesions
• Angular Cheilitis• Erythema and/or fissuring-ulceration at the corner of
the mouth

Pseudomembraneous Candidiasis

Atrophic / Erythematous Candidiasis

Hyperplastic Candidiasis

Angular Cheilitis
Oral manifestations of patients with hyperthyroidism
• -accelerated dental eruption in children,
• -maxillary or mandibular osteoporosis, • -enlargement of extraglandular
thyroid tissue, • -increased susceptibility to caries and
periodontal disease,• -burning mouth syndrome,• -development of connective-tissue
diseases such as Sjorgen’s syndrome or systemic lupus erythematosus.
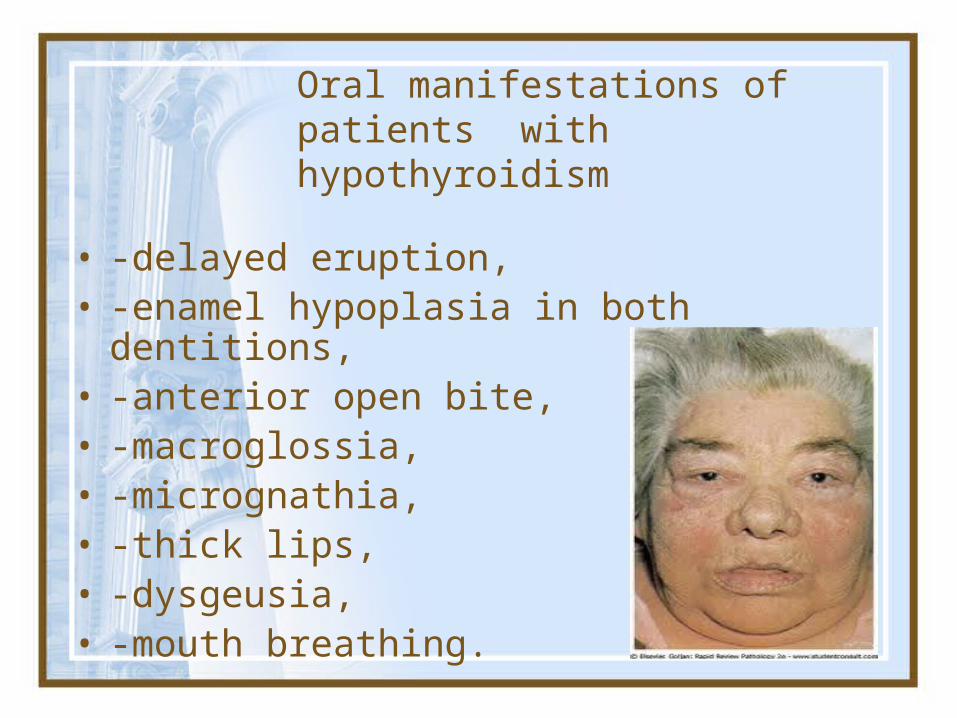
Oral manifestations of patients with hypothyroidism
• -delayed eruption,• -enamel hypoplasia in both dentitions,• -anterior open bite,• -macroglossia,• -micrognathia,• -thick lips,• -dysgeusia,• -mouth breathing.

Oral manifestations of patients with hyperparathyroidism• 1. Dental abnormalities: -widened pulp
chambers; -development defects; -alterations in dental
eruption -weak teeth -maloclussions• 2. Brown tumor• 3. Loss of bone density• 4. Soft tissue
calcifications

Hyperparathyroidism (cont.)
Oral manifestations of patients with hypoparathyroidism
• 1. Dental abnormalities:• -enamel hypoplasia in horizontal lines;• -poorly calcified dentin;• -widened pulp chambers;• -dental pulp calcifications;• -shortened roots;• -hypodontia;• -delay or cessation of dental development.• 2. Mandibular tori• 3. Chronic candidiasis• 4. Paresthesia of the tongue or lips• 5. Alteration in facial muscles

Iron Deficiency Anemia
– (pg. 295)• An insufficient amount of iron is supplied
to bone marrow for red blood cell development.– May occur as a result of deficient iron intake,
blood loss from heavy menstrual bleeding or chronic gastrointestinal bleeding, poor iron absorption, or an increased requirement for iron in situations such as pregnancy or infancy
• Plummer-Vinson syndrome may result from long standing iron deficiency anemia.– Includes dysphagia, atrophy of the upper
alimentary tract, and a predisposition to developing oral cancer

Clinical Features and Oral Manifestations of Iron Deficiency Anemia
– (pg. 295)• Often asymptomatic, may have
nonspecific symptoms such as weakness and fatigue– In severe cases may see angular cheilitis,
pallor of oral tissue, and an erythematous, smooth, painful tongue

Clinical Features and Oral Manifestations of Iron Deficiency Anemia (cont.)
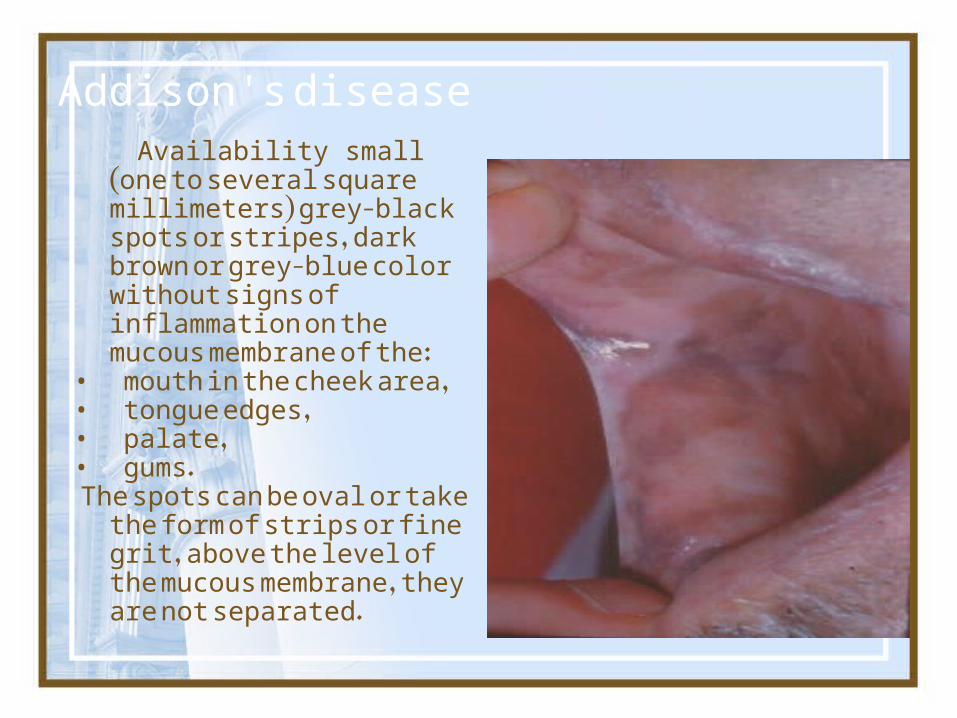
Addison's disease Availability small (one to several
square millimeters) grey-black spots or stripes, dark brown or grey-blue color without signs of inflammation on the mucous membrane of the:
• mouth in the cheek area, • tongue edges, • palate, • gums. The spots can be oval or take the
form of strips or fine grit, above the level of the mucous membrane, they are not separated.

Pernicious Anemia
– (pgs. 295-296)• Probably an autoimmune
disorder in most situations– May be caused by removal of the
stomach, gastric cancer, or gastritis• Caused by a deficiency in
intrinsic factor– Intrinsic factor is secreted by
parietal cells in the stomach; it is necessary for absorption of vitamin B12

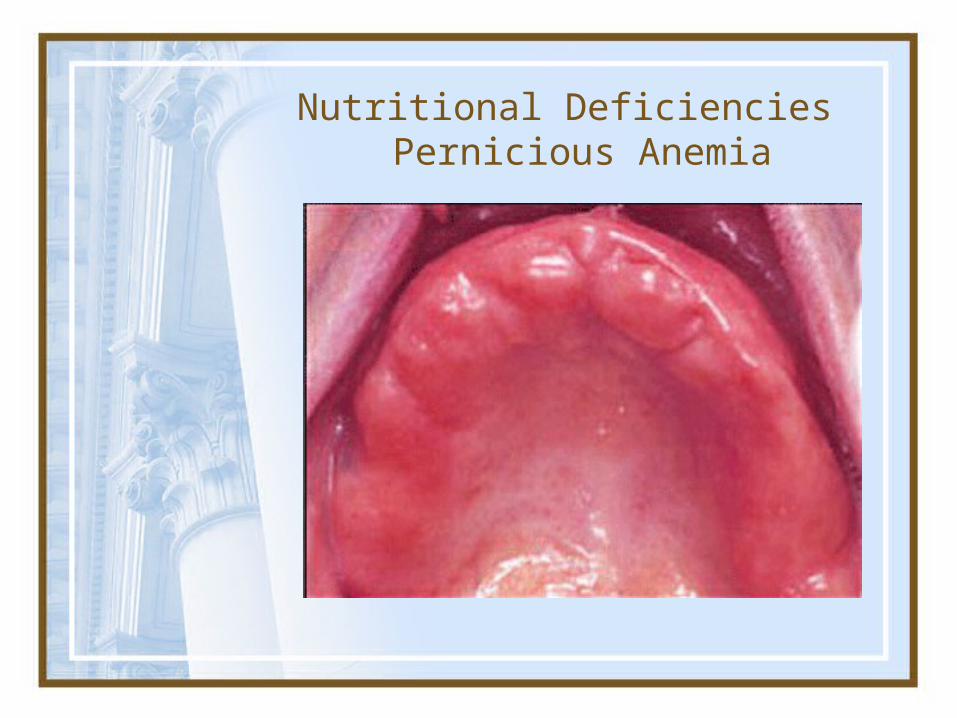
Clinical Features and Oral Manifestations of Pernicious Anemia
– (pgs. 295-296)• Weakness, pallor, and fatigue on
exertion– May see nausea, dizziness, diarrhea,
abdominal pain, loss of appetite, and weight loss
– Angular cheilitis, mucosal pallor, painful atrophic and erythematous mucosa, mucosal ulceration, loss of papillae on the dorsum of the tongue, and burning and painful tongue

Clinical Features and Oral Manifestations of Pernicious Anemia (cont.)
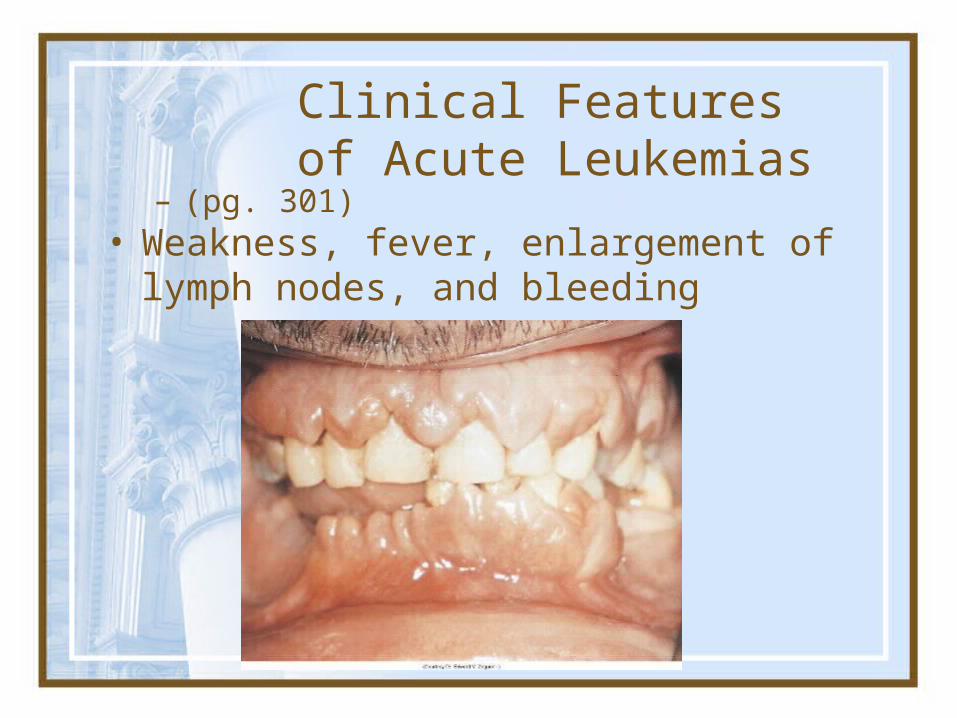
Clinical Features of Acute Leukemias
– (pg. 301)• Weakness, fever, enlargement of
lymph nodes, and bleeding

Oral Manifestations of Acute Leukemias• Gingival enlargement• Oral infection• Bleeding gums, petechiae
and ecchymosis

Diagnosis and Treatment of Acute Leukemias• Laboratory findings include elevated
white blood cell count, anemia, and low platelet count
• Treatment – Bone marrow transplant

Oral Manifestations of Therapy for Oral Cancer• Radiation Therapy
• Chemotherapy

Oral Manifestations of Therapy for Oral Cancer (cont.)• Oral cancer can be treated with
surgery, radiation therapy, or chemotherapy, or a combination.

Radiation Therapy
• The patient often experiences mucositis during radiation therapy.– Mucositis begins about the
second week of therapy and subsides a few weeks after its completion.
– It is painful and appears as an erythematous and ulcerated mucosa.
– The patients may have difficulty eating, pain on swallowing, and loss of taste.

• Destruction of major salivary glands may result in xerostomia– The patient is prone to rampant caries and oral
candidiasis.– They also are prone to osteoradionecrosis.
Radiation Therapy (cont.)Radiation Therapy (cont.)

• Patients should have an oral evaluation before radiation therapy of the head and neck.– Potential sources for oral infection and
teeth with a questionable prognosis should be removed.
• The hygienist can help with– Fluoride application– Patient education– Frequent follow-up appointments
Radiation Therapy (cont.)Radiation Therapy (cont.)

Chemotherapy
• Drugs used for cancer chemotherapy affect basal cells of the epithelium.– Mucositis and oral ulceration are
common complications.• A decrease in all blood cells may
occur– Lowered RBC counts can lead to anemia.– Lowered WBC counts can lead to
infections.– Lowered platelets can lead to bleeding
problems.

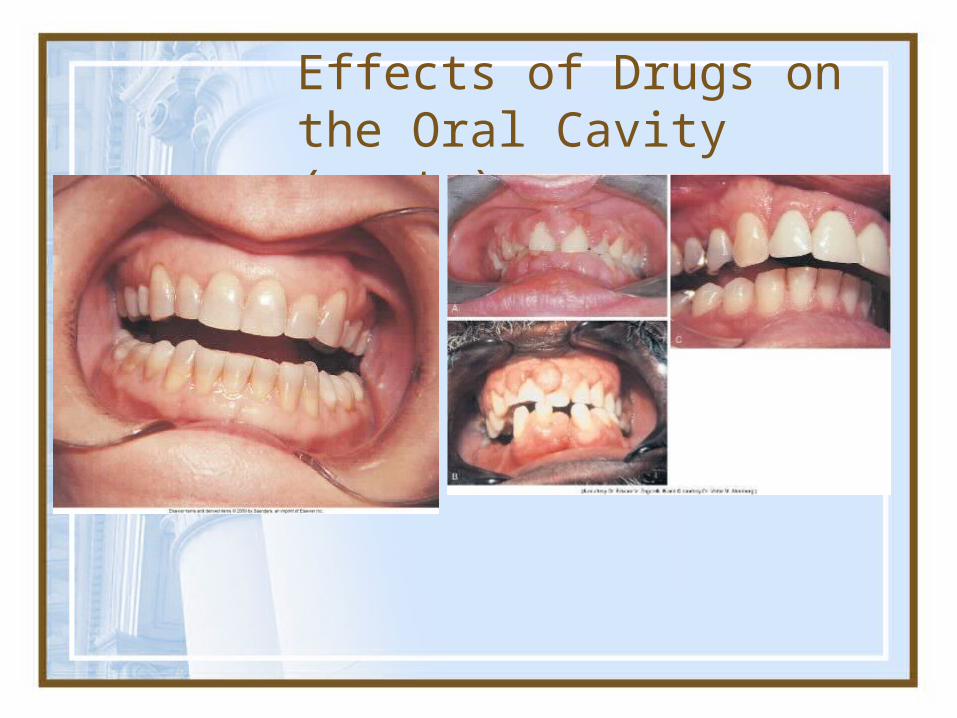
Effects of Drugs on the Oral Cavity
Blood pressure drugs, antianxiety medications, antipsychotic medications, and antihistamines can cause xerostomia.
• Prednisone suppresses the immune system and can lead to candidiasis and oral infections.
• Antibiotics may increase risk of candidiasis.

Effects of Drugs on the Oral Cavity (cont.)
Effects of Drugs on the Oral Cavity (cont.)

Effects of Drugs on the Oral Cavity (cont.)
• Tetracycline can cause tooth discoloration.
• Phenytoin and nifedipine can cause gingival enlargement.
• Cyclosporine may cause gingival enlargement.

Addison's disease
Addison's disease results from a chronic insufficiency of the adrenal cortex.
The first signs of the disease may be: - pigmentation of the skin and mucous
membranes due to excessive deposition of melanin in the connective tissue and epithelial cells. Pigmentation of the skin appears in the areas exposed to light (the face, the back surface of the hands). As the disease progresses the skin become light brown or bronze color.
-possible fatigue, gastrointestinal
disturbances (nausea, vomiting, diarrhea, abdominal pain), headache, memory loss, weight loss.

Addison's diseaseThe most common symptoms are fatigue, lightheadedness upon standing or while upright, muscle weakness, fever, weight loss, difficulty in standing up, anxiety, nausea, vomiting, diarrhea, headache, sweating, changes in mood and personality, joint and muscle pains.

Addison's disease is differentiated from:-multiple melanotic macules, -smoker’s melanosis, -Peutz-Jeghers syndrome, -heavy metal poisoning, -postinflammatory hyperpigmentation, -congenital pigmentation of the oral mucosa, which is observed in some nations Fig. the band-like grayish blue pigmentation of the maxillary and mandibular anterior gingiva after using drugs that include antimalarial agents .
*
Addison's disease
• Treatment: -replace the missing or low levels of cortisol
(hydrocortisone) • Prognosis:-Prognosis for patients appropriately treated with
hydrocortisone and aldosterone is excellent. These patients can expect to enjoy a normal lifespan.
-Without treatment, or with substandard treatment, patients are always at risk of developing Addisonian crisis.

Fungal Infections

Viral Infections-Herpes

Viral Infections-HIV
Behcet’s Disease

Sjögren’s Syndrome
Nutritional DeficienciesPernicious Anemia

Conclusions
• The mucosal surface that is the oral cavity may provide insight into the immune function of the patient.
• Differential diagnosis is important as many disorders may manifest themselves similarly in the buccal area.
ReferencesGreenspan, JS. "Sentinelsand Signposts: the
Epidemiology and Significance of the Oral Manifestations of HIV disease." Oral Diseases May 1997: S13-17.
McCance, Kathryn L., and Sue E. Huether. Pathophysiology The Biologiv Basis for Disease in Adults and Children. 4th ed. St. Louis: Mosby, 2002
Bologna, Jean L., Joseph L. Jorizzo, and Ronald P. Rapini. Dermatology. Spain: Mosby, 2003.
Edwards, Brooks S. Amyloidosis. 2 Aug. 2005. Mayo Clinic. 26 Dec. 2005 <http://www.mayoclinic.com/health/amyloidosis/DS00431>.
Related Documents