Chapter 16 Oral appliances J.A. Fleetham* and F.R. Almeida # Summary Oral appliances are commonly used for the treatment of snoring and obstructive sleep apnoea–hypopnoea (OSAH). Oral appliances increase the size of the upper airway. Mandibular advancement splints (MAS) are the most widely used type of oral appliance. There is increasing evidence that MAS improve sleepiness, blood pressure and indices of sleep-disordered breathing. Continuous positive airway pressure (CPAP) is more effective than MAS in improving sleepiness, health status and indices of sleep-disordered breathing. CPAP remains the primary treatment for severe OSAH. Current guidelines recommend oral appliances as a primary treatment for patients with mild-to-moderate OSAH. Oral appliances are the best alternative treatment for patients with OSAH who are unwilling or unable to comply with CPAP therapy. Oral appliance therapy may also be indicated as an adjuvant to CPAP when the patient is away from home or electrical power. Oral appliance therapy should be supervised by both medical and dental specialists. MAS should not be recommended for patients with major periodontal disease. Follow-up sleep monitoring is needed to verify the efficacy of oral appliance therapy. Patients treated with oral appliances require long-term medical and dental follow-up care. Keywords: Mandibular advancement device, mandibular advancement splint, obstructive sleep apnoea-hypopneoa, oral appliance, tongue retaining device, snoring *Dept of Medicine, Faculty of Medicine and # Oral health Sciences, Faculty of Dentistry, UBC, Vancouver, BC, Canada. Correspondence: J.A. Fleetham, The Lung Centre, 7th Floor, 2775 Laurel Street, Vancouver, BC V5Z 1M9, Canada, Email [email protected] Eur Respir Mon 2010. 50, 267–285. Printed in UK – all rights reserved. Copyright ERS 2010. European Respiratory Monograph; ISSN: 1025-448x. DOI: 10.1183/1025448x.00025209 O bstructive sleep apnoea–hypopnoea (OSAH) is a common syndrome that is characterised by recurrent episodes of partial or complete upper airway obstruction during sleep. Currently, the primary treatment for OSAH is nasal continuous positive airway pressure (CPAP). However, some patients are unable to tolerate and comply with CPAP on a long-term basis. Oral appliances are now widely used for the treatment of snoring and mild-to-moderate OSAH, both as primary therapy and as an alternative for patients who are unwilling or unable to tolerate CPAP. Oral appliances are a simple, reversible, quiet, and cost-effective therapy for selected patients with OSAH. However, oral appliances as therapy for OSAH remain underutilised. There are a variety of synonyms for oral appliances. In addition to oral, they may be called intraoral, dental or mandibular; instead of appliance, they may be called a device, splint or prosthesis. Oral appliances can be divided into two major types: 1) those that reposition the mandible and the attached tongue, the mandibular advancement splints (MAS) or mandibular advancement device (MAD), 267 J.A. FLEETHAM AND F.R. ALMEIDA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chapter 16
Oral appliancesJ.A. Fleetham* and F.R. Almeida#
SummaryOral appliances are commonly used for the treatment of snoringand obstructive sleep apnoea–hypopnoea (OSAH). Oralappliances increase the size of the upper airway. Mandibularadvancement splints (MAS) are the most widely used type oforal appliance. There is increasing evidence that MAS improvesleepiness, blood pressure and indices of sleep-disorderedbreathing. Continuous positive airway pressure (CPAP) ismore effective than MAS in improving sleepiness, health statusand indices of sleep-disordered breathing. CPAP remains theprimary treatment for severe OSAH. Current guidelinesrecommend oral appliances as a primary treatment for patientswith mild-to-moderate OSAH. Oral appliances are the bestalternative treatment for patients with OSAH who are unwillingor unable to comply with CPAP therapy. Oral appliance therapymay also be indicated as an adjuvant to CPAP when the patientis away from home or electrical power. Oral appliance therapyshould be supervised by both medical and dental specialists.MAS should not be recommended for patients with majorperiodontal disease. Follow-up sleep monitoring is needed toverify the efficacy of oral appliance therapy. Patients treatedwith oral appliances require long-term medical and dentalfollow-up care.
Keywords: Mandibular advancement device, mandibularadvancement splint, obstructive sleep apnoea-hypopneoa, oralappliance, tongue retaining device, snoring
*Dept of Medicine, Faculty ofMedicine and#Oral health Sciences, Faculty ofDentistry, UBC, Vancouver, BC,Canada.
Correspondence: J.A. Fleetham, TheLung Centre, 7th Floor, 2775 LaurelStreet, Vancouver, BC V5Z 1M9,Canada, Email [email protected]
Eur Respir Mon 2010. 50, 267–285.Printed in UK – all rights reserved.Copyright ERS 2010.European Respiratory Monograph;ISSN: 1025-448x.DOI: 10.1183/1025448x.00025209
Obstructive sleep apnoea–hypopnoea (OSAH) is a common syndrome that is characterised byrecurrent episodes of partial or complete upper airway obstruction during sleep. Currently,
the primary treatment for OSAH is nasal continuous positive airway pressure (CPAP). However,some patients are unable to tolerate and comply with CPAP on a long-term basis. Oral appliancesare now widely used for the treatment of snoring and mild-to-moderate OSAH, both as primarytherapy and as an alternative for patients who are unwilling or unable to tolerate CPAP. Oralappliances are a simple, reversible, quiet, and cost-effective therapy for selected patients withOSAH. However, oral appliances as therapy for OSAH remain underutilised. There are a variety ofsynonyms for oral appliances. In addition to oral, they may be called intraoral, dental ormandibular; instead of appliance, they may be called a device, splint or prosthesis. Oral appliancescan be divided into two major types: 1) those that reposition the mandible and the attachedtongue, the mandibular advancement splints (MAS) or mandibular advancement device (MAD),
26
7J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA

and 2) those that hold the tongue forward, the tongue retaining devices (TRD). Prior to treatmentwith any oral appliance, a complete assessment by an experienced physician, within the field, isimportant. Having concluded that treatment with an oral appliance is indicated, the physicianprovides the dentist, who should be knowledgeable in sleep medicine and have skills and experiencein oral appliance therapy, with a written referral and a copy of the sleep diagnostic report. Oralappliances improve OSAH because of an increase in upper airway size, the provision of a stableanterior position of the mandible, advancement of the tongue or soft palate, and possibly by achange in genioglossus muscle activity. Oral appliance therapy for OSAH is a long-termcommitment, so it is important that the appliance must be comfortable for the patient. Finally, as isthe case with CPAP, oral appliances can only be used to treat OSAH in cooperative patients who aremotivated to wear the oral appliance during sleep on a regular and consistent basis every night.
This chapter provides an update to previous recent reviews [1–3] and summarises the recentrecommendations from both the Cochrane Collaboration [4] and the American Academy of SleepMedicine [5]. It provides an overview of the effectiveness of treatment, the predictors of treatmentsuccess, adherence and the potential adverse effects associated with this treatment. It also outlinesa detailed clinical protocol and titration sequence for MAS, since this clinical procedure is oftennot well understood by practitioners new to the field. This chapter only focuses on the use of oralappliances in the adult population. Little is known about the efficacy and side-effects of oralappliances for children without craniofacial abnormalities [6, 7]. Orthodontic treatment forchildren with OSAH and craniofacial anomalies has been shown to be effective not only for thedentition, but also in decreasing respiratory disturbances in children [8, 9].
Appliance
Types of appliances
A large number of different oral appliances are currently available for the treatment of OSAH. Oralappliances increase the size of the upper airway by either advancing the mandible or the tongue. Thereare other minor design differences in currently available oral appliances that may also impact on theirsuccess and treatment adherence. MAS are most widely used and utilise traditional dental techniquesto attach the appliance to both dental arches and maintain the mandible in a forward position.
Figure 1 illustrates some common appliances used for the treatment of sleep apnoea: 1) tonguestabilising device Aveo-TSD1 (Innovative Health Technologies, Christchurch, New Zealand),SomnoDent1 MAS (SomnoMed, Denton, TX, USA), PM Positioner1 (Great Lakes OrthodonticsLtd, Tonawanda, NY, USA), Monoblock appliance (courtesy of M. Marklund, Umea University,Sweden), HerbstTM (Great Lakes Orthodontics Ltd), MDSA1 (Medical Dental Sleep Appliance; R.J. andV.K. Bird Pty Ltd, Melbourne, VIC, Australia) and KlearwayTM (Great Lakes Orthodontics Ltd).Construction usually requires dental impressions, bite registration and fabrication by a dental laboratory.
Some MAS are available in a prefabricated form and are sometimes referred to as ‘‘boil and bite’’[10], but have limited efficacy [11]. These can either be fitted by the patient, themselves, ormoulded to the patient’s teeth in an office setting. Some MAS restrict mouth opening by means ofscrew mechanisms, whereas others allow relatively unhindered movement.
There have been two significant advances in the MAS design over the past 15 yrs. Adjustableappliances that allow the progressive advancement of the mandible, and the use of materials anddesigns that improve intraoral retention, are major improvements. Determining the optimaldegree of mandibular advancement is the most important step when using MAS therapysuccessfully. The amount of anteroposterior mandibular movement, similar to the amount ofCPAP and the speed with which this can be changed, varies considerably between patients. MAShave been developed with an adjustable hinge that allows progressive advancement of themandible, after initial construction, until the optimal mandibular position is achieved. Single-piece or nonadjustable appliances often need to be remade if the initial jaw advancement proves to
26
8O
RA
LA
PP
LIA
NC
ES

be insufficient. MAS sometimesinclude anterior tubes or openingsthat allow for oral breathing orpressure relief. Some oral appliancesfeature a posterior extension of themaxillary component to modify theposition of the soft palate or tongue,but this type of appliance has notbeen widely studied. A subgroupof patients, particularly those whosuffer from sleep bruxism [12],seem to experience jaw discomfortin the morning after wearing a rigid,hard acrylic, single-jaw positionedMAS. MAS have been further devel-oped to allow lateral jaw movement,as well as some degree of vertical jawopening.
There have been major advancesmade in dental materials, whichhave lead to improved flexibilityand strength of thermosensitiveacrylic resin materials. MAS madeof temperature-sensitive material,which the patient can heat in hotwater prior to insertion and thatcool and harden intraorally, pro-vide considerably more retentionthan traditionally designed cold-cure acrylic MAS. The combina-tion of adjustability, lateral andvertical jaw movement, increasedretention and better defined titra-tion protocols, have significantlyimproved the effectiveness of MASover the last decade.
The other major type of oralappliance available is the TRD ortongue stabiliser device (TSD),which keeps the tongue in ananterior position during sleep bymeans of negative pressure in a softplastic bulb. It fits over both the mandibular and maxillary arches and has a flange that is placedbetween the lips and teeth, keeping the appliance stable in the mouth. This appliance was one ofthe first to be developed and is available in both a fabricated and prefabricated form [13–15]. It hasrecently been evaluated for dentate patients [16]. It is mainly used in edentulous patients and is theoral appliance of choice for patients with no teeth, limited anterior-posterior mandibularmovement or a very large tongue.
Mechanisms of action
The majority of oral appliances are designed to maintain the mandible and/or tongue in a protrudedposture, thereby preventing upper airway obstruction during sleep. Proposed mechanisms of action
a) b)
c) d)
e)
g) h)
f)
Figure 1. Different types of oral appliances used for the treatmentof obstructive sleep apnoea–hypopnoea. a) Aveo-TSD1 (InnovativeHealth Technologies, Christchurch, New Zealand). b) SomnoDent1
MAS (SomnoMed, Denton, TX, USA). c) PM positioner1 (GreatLakes Orthodontics Ltd, Tonawanda, NY, USA). d) Monoblockappliance (courtesy of M. Marklund, Umea University, Sweden).e) HerbstTM (Great Lakes Orthodontics Ltd). f) MDSA1 (MedicalDental Sleep Appliance; R.J. and V.K. Bird Pty Ltd, Melbourne, VIC,Australia). g) KlearwayTM (Great Lakes Orthodontics Ltd), lateralview. h) KlearwayTM, hinge view.
26
9J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA

for oral appliances include increased upper airway size, decreased upper airway collapsibility,activation of upper airway dilator muscles, and stabilisation of mandibular posture.
Several different upper airway-imaging techniques have been used to assess changes in upperairway size and function with oral appliances in patients with OSAH. These imaging techniquesinclude cephalometry, computed tomography (CT), magnetic resonance imaging (MRI) andvideoendoscopy [17]. Voluntary mandibular and tongue protrusion have been shown to increaseupper airway size and alter upper airway shape, particularly in the velopharynx, in subjects withand without OSAH [18]. Several studies have demonstrated an increase in the anteroposteriordiameter of the upper airway following MAS insertion [19–21], an example is shown in figure 2.This increase was predominantly in the oropharynx and hypopharynx, but some studies have alsosuggested an effect on the velopharynx [22]. Nonadjustable MAS constructed in the mostadvanced position without causing discomfort or at 75% of mandibular advancement, have shownan increase in the total volume of the upper airway and cross-sectional areas of the retropalataland retroglossal regions using CT [23, 24]. Two studies, which used MRI, showed that withmandibular advancement the velopharynx cross-sectional area and volume increases, and that thischange was predominantly attributed to an increase in the lateral dimensions [25, 26]. Theseupper airway changes were associated with an increase in lower anterior facial height, higherposition of the hyoid, lateral displacement of the parapharyngeal fat pads away from the airwayand anterior positioning of the base of tongue muscles [26].
Almost all of these upper-airway imaging studieshave been performed during wakefulness and it isunknown whether the same changes occur duringsleep. MAS have also been shown to increase upperairway muscle tone, which may also contribute toan increased upper airway patency [27].
Contradictions
MAS normally requires at least eight teeth in eachof the maxillary and mandibular arches to supportthe appliance in the absence of advanced period-ontal disease. Furthermore, the patient should beable to advance their mandible by at least 5 mmwithout discomfort.
Temporomandibular joint disease is common inpatients with OSAH [28] and should not beconsidered as a contraindication. The concernabout MAS treatment in patients with tempor-omandibular joint disease was raised because ofmild initial and transitory side-effects of MAS wear,such as pain in the temporomandibular joint andmasticatory muscles. It is important to determine,during the clinical exam, whether there is any noiseand/or pain in the temporomandibular joint, thedegree of mandibular movement and any mastica-tory muscle tenderness. When temporomandibularjoint disease was assessed with MRI, MAS appearednot to cause or increase temporomandibular jointdisease over a 1-yr treatment period [29]. Fur-thermore, if MAS are used in combination withmandibular physiotherapy, patients with previous
a)
b)
Figure 2. Lateral cephalometry of a malepatient a) without and b) with a mandibularadvancement oral appliance. Note the advance-ment of the mandible and an increase in the sizeof the velopharynx with the mandibular advance-ment oral appliance (b).
27
0O
RA
LA
PP
LIA
NC
ES

temporomandibular disease are able to use MAS [30].Therefore, the presence of temporomandibular diseaseis not currently a contraindication for MAS treatment.
Sleep bruxism has been reported to be more prevalentin patients with OSAH [12, 31], and MAS treatmentcan be used in patients with bruxism. The MAS canhelp prevent tooth wear and has been associated with aremarkable reduction in sleep bruxism motor activityin patients with OSAH [32]. Finally, bruxism occlusalsplints have been shown to exacerbate OSAH [33].
Treatment optimisation
The optimisation of MAS treatment is quite differentfrom CPAP treatment, which can either be performedduring polysomnography (PSG) or with an automaticCPAP machine. Patients may not be able to initiallytolerate the degree of mandibular advancementrequired to completely relieve the OSAH. There are avariety of studies that show how the decrease inapnoea/hypopnoea index (AHI) is dependent upon theamount of mandibular advancement (figs 3 and 4) [19, 34–37]. MAS cannot easily be tried for asingle night to predict treatment success and patient adherence, and may require up to 6 monthsof progressive mandibular advancement.
One study has used a prefabricated boil and bite mandibular advancement appliance as a screeningtool for MAS therapy [11]. This randomised controlled cross-over study found that aprefabricated appliance had a 31% compliance failure, whereas a custom-made appliance showedonly a 6% compliance failure. The prefabricated appliance showed an exceptionally high totalfailure rate of 69%, while the failure rate of the custom-made appliance was 40%. The studyconcluded that prefabricated boil and bite appliances cannot be recommended as a therapeuticoption, nor can they be used as a tool to identify good candidates for MAS therapy.
Several studies have evaluated whether titration of mandibular advancement during PSG could beused to optimise MAS treatment, similar to CPAP titration [38–42]. The first study of overnighttitration used MAS that was removed from the patient’s mouth and adjusted manually [38]. Othertitration studies have used a temporary appliance that can be adjusted by either waking or notwaking the patient [39, 40]. The MAS was advanced either manually, after the removal of thetemporary appliance [41], by using either a hydraulic system [39], or by remote control of amotorised system [40]. These studies had mixed results in predicting the amount of mandibularadvancement needed for successful MAS therapy. Overnight titration of MAS remains anexperimental approach and the technology for remote controlled advancement is not yet widelyavailable.
The efficacy of titration and timing for repeat-sleep monitoring concerning MAS titrationsrequires further study. KRISHNAN et al. [42] have shown that although 55% of patients achievesuccessful self-titration at home, another 32% can reach success with further PSG-guided titration.ALMEIDA et al. [43] showed that titration at night can improve the results, after the usual clinicaladvancement of the MAS, by up to 35%. The protocol is simple to implement in the sleeplaboratory, with the technologist asking the patient to advance the appliance in 1-mm incrementsif the patient continues to snore or have persistent apnoea, hypopnoea or arterial oxygendesaturation episodes. However, the patients should not be woken more than three times per nightin order to achieve an adequate total sleep time.
250
200
150
100
50
300
0
Cro
ss-s
ectio
nal a
rea
of v
elop
hary
nx m
m2
#
#
Pre PostInsertion of MAS
●
●
●
●●●
●●●
●●●●●
●●
●
●
●●●●●●●●
●●
Figure 3. Increase in cross-sectional areaof the velopharynx after the insertion of amandibular advancement splint (MAS).#: median values. n515 and p,0.005.Reproduced from [19] with permission fromthe publisher.
27
1J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA
Effectiveness
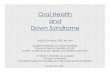
The treatment of OSAH shouldalways be individualised for eachpatient and the future goal is todevelop customised treatment,based on each patient’s phenotype.The patient’s age, occupation,severity of symptoms, body massindex, comorbid disease, lifestyleand treatment-outcome expecta-tions, may all influence the OSAHtreatment decision taken. Approxi-mately 50% of patients achieve aAHI f10 events?h-1 with MAStreatment [1], and it is often thepatient’s preferred choice of treat-ment over CPAP. Although not asefficacious as CPAP, oral appli-ances should be considered first-line treatment in patients withmild-to-moderate OSAH and whoprefer oral appliances to CPAP, arenot appropriate candidates forCPAP, or fail treatment attemptswith CPAP or treatment with be-havioural measures. Patients withsevere OSAH should always have aninitial trial of nasal CPAP becausegreater effectiveness has been shownwith this treatment than with oralappliances [5]. Despite MAS ther-
apy being less effective in severe OSAH, HENKE et al. [44] suggested that severity of OSAH and thesite of airway closure should not be used to exclude patients from MAS treatment.
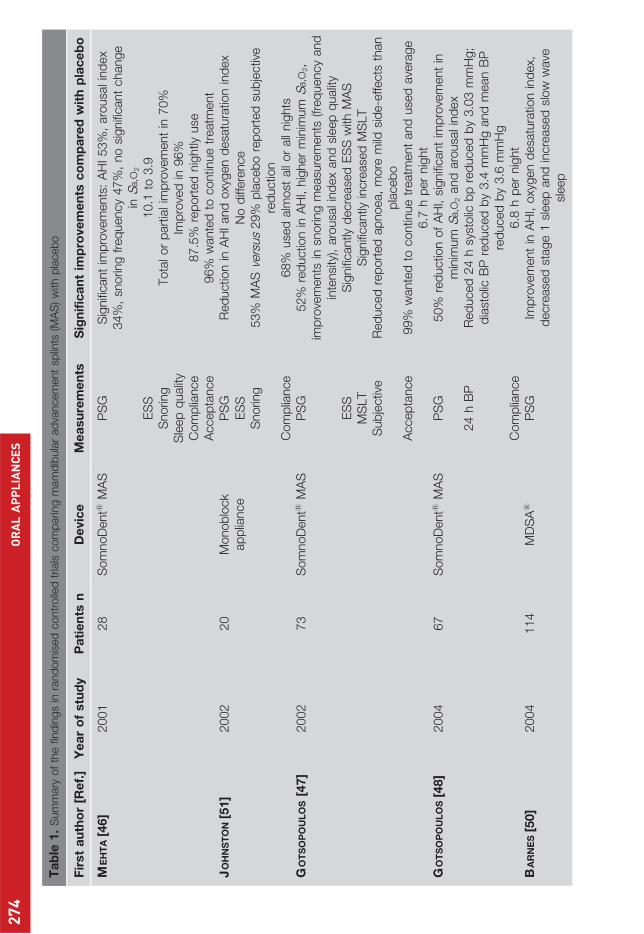
In the first practice parameters paper by the American Sleep Disorder Association,on the efficacyof oral appliance treatment for OSAH, published in 1995 [45], the majority of the data were fromuncontrolled case series studies, which were subject to study design issues such as regression to themean, and selection and reporting bias. The second practice parameters paper by the AmericanAcademy of Sleep Medicine was published in 2006 [5], and included six randomised, controlledtrials comparing MAS with an inactive control [4, 46–49]. Furthermore, there are approximatelyten randomised controlled trials comparing MAS with CPAP, and 12 studies comparing differenttypes of oral appliances.
MAS versus placebo
There are six randomised controlled trials on 375 patients comparing active MAS with control oralappliances [46–51], and there are two randomised controlled trials on 39 patients comparingTRD with placebo [52, 53]. MAS has been shown to significantly improve objective sleepmeasurements, such as AHI, arousal index, snoring and in some but not all studies, arterial oxygendesaturation. MAS have also been shown to improve objective measurements for sleepiness whenexamined using the multiple sleep latency test [47], but not the multiple vigilance test [50]. MASimproved subjective measurements of sleepiness (Epworth Sleepiness Scale) in all but one study [51].
ΔCSA
mm
2ΔC
SA %
ΔAHI
a) 100
50
0
-50
200b)
150
100
50
0
-50-10 0 40302010
●
●
●●
●●
●
●
●
●
●
●●
●
●
●
● ●
●
●● ●
●
●
●
●
●
●●
●
Figure 4. Relationship between the change in apnoea/hypopnoeaindex (DAHI) and a) the absolute (r50.64, p50.01) and b) theproportional (r50.64, p50.01) change in cross-sectional area(DCSA) of the velopharynx, following the insertion of a mandibularadvancement splint. Reproduced from [19] with permission from thepublisher.
27
2O
RA
LA
PP
LIA
NC
ES
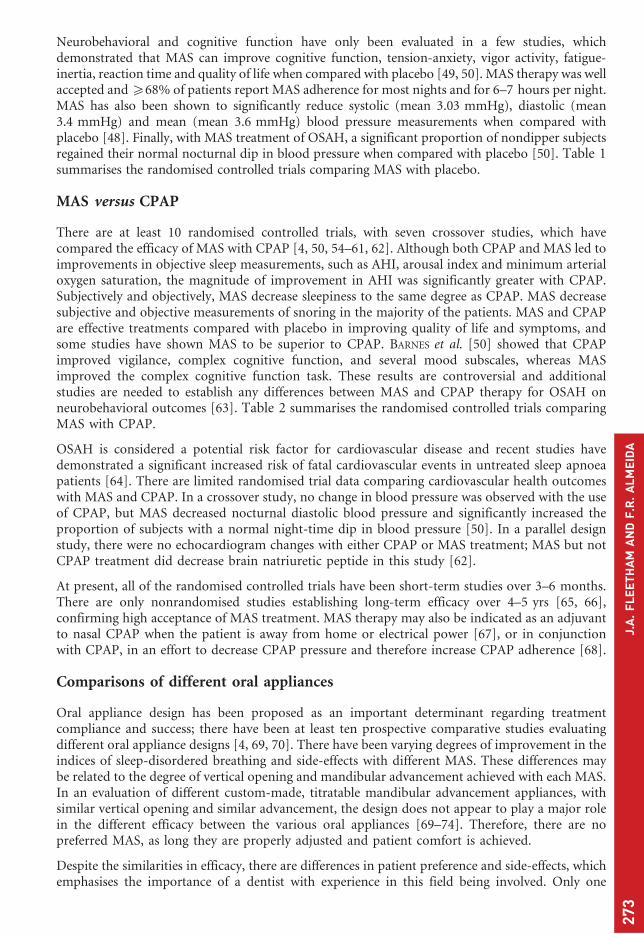
Neurobehavioral and cognitive function have only been evaluated in a few studies, whichdemonstrated that MAS can improve cognitive function, tension-anxiety, vigor activity, fatigue-inertia, reaction time and quality of life when compared with placebo [49, 50]. MAS therapy was wellaccepted and o68% of patients report MAS adherence for most nights and for 6–7 hours per night.MAS has also been shown to significantly reduce systolic (mean 3.03 mmHg), diastolic (mean3.4 mmHg) and mean (mean 3.6 mmHg) blood pressure measurements when compared withplacebo [48]. Finally, with MAS treatment of OSAH, a significant proportion of nondipper subjectsregained their normal nocturnal dip in blood pressure when compared with placebo [50]. Table 1summarises the randomised controlled trials comparing MAS with placebo.
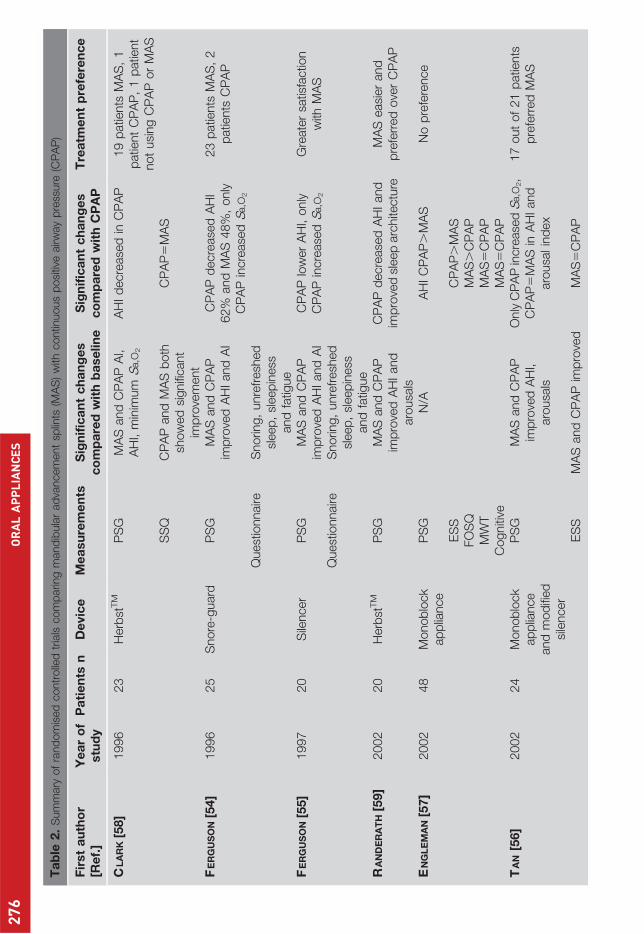
MAS versus CPAP
There are at least 10 randomised controlled trials, with seven crossover studies, which havecompared the efficacy of MAS with CPAP [4, 50, 54–61, 62]. Although both CPAP and MAS led toimprovements in objective sleep measurements, such as AHI, arousal index and minimum arterialoxygen saturation, the magnitude of improvement in AHI was significantly greater with CPAP.Subjectively and objectively, MAS decrease sleepiness to the same degree as CPAP. MAS decreasesubjective and objective measurements of snoring in the majority of the patients. MAS and CPAPare effective treatments compared with placebo in improving quality of life and symptoms, andsome studies have shown MAS to be superior to CPAP. BARNES et al. [50] showed that CPAPimproved vigilance, complex cognitive function, and several mood subscales, whereas MASimproved the complex cognitive function task. These results are controversial and additionalstudies are needed to establish any differences between MAS and CPAP therapy for OSAH onneurobehavioral outcomes [63]. Table 2 summarises the randomised controlled trials comparingMAS with CPAP.
OSAH is considered a potential risk factor for cardiovascular disease and recent studies havedemonstrated a significant increased risk of fatal cardiovascular events in untreated sleep apnoeapatients [64]. There are limited randomised trial data comparing cardiovascular health outcomeswith MAS and CPAP. In a crossover study, no change in blood pressure was observed with the useof CPAP, but MAS decreased nocturnal diastolic blood pressure and significantly increased theproportion of subjects with a normal night-time dip in blood pressure [50]. In a parallel designstudy, there were no echocardiogram changes with either CPAP or MAS treatment; MAS but notCPAP treatment did decrease brain natriuretic peptide in this study [62].
At present, all of the randomised controlled trials have been short-term studies over 3–6 months.There are only nonrandomised studies establishing long-term efficacy over 4–5 yrs [65, 66],confirming high acceptance of MAS treatment. MAS therapy may also be indicated as an adjuvantto nasal CPAP when the patient is away from home or electrical power [67], or in conjunctionwith CPAP, in an effort to decrease CPAP pressure and therefore increase CPAP adherence [68].
Comparisons of different oral appliances
Oral appliance design has been proposed as an important determinant regarding treatmentcompliance and success; there have been at least ten prospective comparative studies evaluatingdifferent oral appliance designs [4, 69, 70]. There have been varying degrees of improvement in theindices of sleep-disordered breathing and side-effects with different MAS. These differences maybe related to the degree of vertical opening and mandibular advancement achieved with each MAS.In an evaluation of different custom-made, titratable mandibular advancement appliances, withsimilar vertical opening and similar advancement, the design does not appear to play a major rolein the different efficacy between the various oral appliances [69–74]. Therefore, there are nopreferred MAS, as long they are properly adjusted and patient comfort is achieved.
Despite the similarities in efficacy, there are differences in patient preference and side-effects, whichemphasises the importance of a dentist with experience in this field being involved. Only one
27
3J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA
Ta
ble
1.
Sum
mary
of
the
find
ings
inra
nd
om
ised
contr
olle
dtr
ials
com
parin
gm
am
dib
ula
rad
vancem
ent
splin
ts(M
AS
)w
ithp
laceb
o
Fir
st
au
tho
r[R
ef.
]Y
ea
ro
fstu
dy
Pa
tie
nts
nD
evic
eM
ea
su
rem
en
tsS
ign
ific
an
tim
pro
ve
me
nts
co
mp
are
dw
ith
pla
ce
bo
ME
HT
A[4
6]
2001
28
Som
noD
ent1
MA
SP
SG
Sig
nifi
cant
imp
rove
ments
:A
HI53%
,aro
usa
lin
dex
34%
,sn
orin
gfr
eq
uency
47%
,no
signifi
cant
change
inS
a,O
2
ES
S10.1
to3.9
Snorin
gTota
lor
part
ialim
pro
vem
ent
in70%
Sle
ep
qualit
yIm
pro
ved
in96%
Com
plia
nce
87.5
%re
port
ed
nig
htly
use
Accep
tance
96%
wante
dto
contin
ue
treatm
ent
JO
HN
ST
ON
[51]
2002
20
Monob
lock
ap
plia
nce
PS
GR
ed
uctio
nin
AH
Iand
oxy
gen
desa
tura
tion
ind
ex
ES
SN
od
iffere
nce
Snorin
g53%
MA
Sve
rsus
29%
pla
ceb
ore
port
ed
sub
jectiv
ere
ductio
nC
om
plia
nce
68%
use
dalm
ost
all
or
all
nig
hts
GO
TS
OP
OU
LO
S[4
7]
2002
73
Som
noD
ent1
MA
SP
SG
52%
red
uctio
nin
AH
I,hig
her
min
imum
Sa,O
2,
imp
rove
ments
insn
orin
gm
easu
rem
ents
(freq
uency
and
inte
nsi
ty),
aro
usa
lin
dex
and
sleep
qualit
yE
SS
Sig
nifi
cantly
decre
ase
dE
SS
with
MA
SM
SLT
Sig
nifi
cantly
incre
ase
dM
SLT
Sub
jectiv
eR
ed
uced
rep
ort
ed
ap
noea,
more
mild
sid
e-e
ffects
than
pla
ceb
oA
ccep
tance
99%
wante
dto
contin
ue
treatm
ent
and
use
dave
rage
6.7
hp
er
nig
ht
GO
TS
OP
OU
LO
S[4
8]
2004
67
Som
noD
ent1
MA
SP
SG
50%
red
uctio
nof
AH
I,si
gnifi
cant
imp
rove
ment
inm
inim
um
Sa,O
2and
aro
usa
lin
dex
24
hB
PR
ed
uced
24
hsy
stolic
bp
red
uced
by
3.0
3m
mH
g;
dia
stolic
BP
red
uced
by
3.4
mm
Hg
and
mean
BP
red
uced
by
3.6
mm
Hg
Com
plia
nce
6.8
hp
er
nig
ht
BA
RN
ES
[50]
2004
114
MD
SA
1P
SG
Imp
rove
ment
inA
HI,
oxy
gen
desa
tura
tion
ind
ex,
decre
ase
dst
age
1sl
eep
and
incre
ase
dsl
ow
wave
sleep
27
4O
RA
LA
PP
LIA
NC
ES
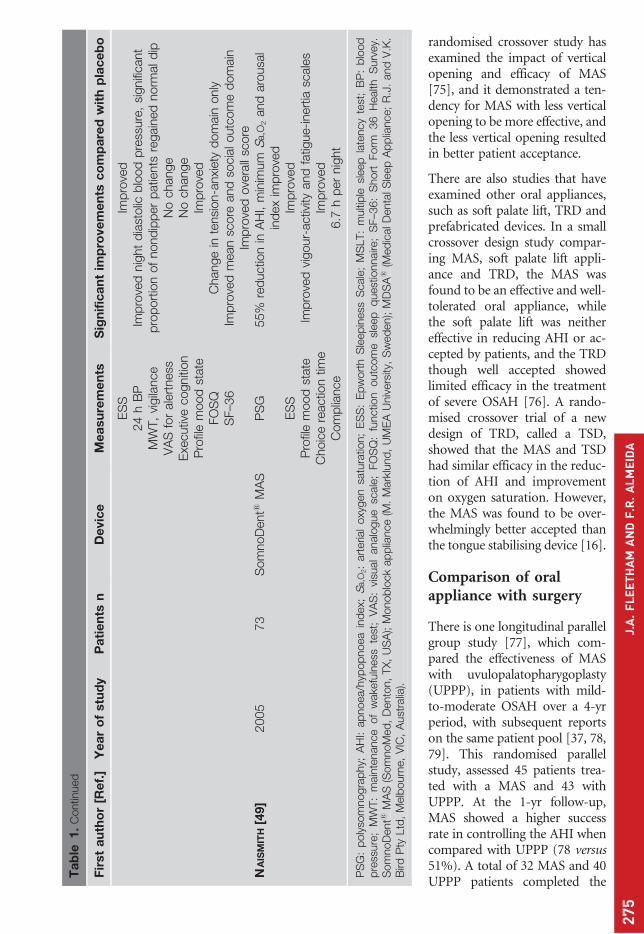
randomised crossover study hasexamined the impact of verticalopening and efficacy of MAS[75], and it demonstrated a ten-dency for MAS with less verticalopening to be more effective, andthe less vertical opening resultedin better patient acceptance.
There are also studies that haveexamined other oral appliances,such as soft palate lift, TRD andprefabricated devices. In a smallcrossover design study compar-ing MAS, soft palate lift appli-ance and TRD, the MAS wasfound to be an effective and well-tolerated oral appliance, whilethe soft palate lift was neithereffective in reducing AHI or ac-cepted by patients, and the TRDthough well accepted showedlimited efficacy in the treatmentof severe OSAH [76]. A rando-mised crossover trial of a newdesign of TRD, called a TSD,showed that the MAS and TSDhad similar efficacy in the reduc-tion of AHI and improvementon oxygen saturation. However,the MAS was found to be over-whelmingly better accepted thanthe tongue stabilising device [16].
Comparison of oralappliance with surgery
There is one longitudinal parallelgroup study [77], which com-pared the effectiveness of MASwith uvulopalatopharygoplasty(UPPP), in patients with mild-to-moderate OSAH over a 4-yrperiod, with subsequent reportson the same patient pool [37, 78,79]. This randomised parallelstudy, assessed 45 patients trea-ted with a MAS and 43 withUPPP. At the 1-yr follow-up,MAS showed a higher successrate in controlling the AHI whencompared with UPPP (78 versus51%). A total of 32 MAS and 40UPPP patients completed the
Ta
ble
1.
Contin
ued
Fir
st
au
tho
r[R
ef.
]Y
ea
ro
fstu
dy
Pa
tie
nts
nD
evic
eM
ea
su
rem
en
tsS
ign
ific
an
tim
pro
ve
me
nts
co
mp
are
dw
ith
pla
ce
bo
ES
SIm
pro
ved
24
hB
PM
WT,
vigila
nce
Imp
rove
dnig
ht
dia
stolic
blo
od
pre
ssure
,si
gnifi
cant
pro
port
ion
of
nond
ipp
er
patie
nts
regain
ed
norm
ald
ipV
AS
for
ale
rtness
No
change
Exe
cutiv
ecogniti
on
No
change
Pro
file
mood
state
Imp
rove
dFO
SQ
Change
inte
nsi
on-a
nxi
ety
dom
ain
only
SF–3
6Im
pro
ved
mean
score
and
socia
loutc
om
ed
om
ain
Imp
rove
dove
rall
score
NA
ISM
ITH
[49]
2005
73
Som
noD
ent1
MA
SP
SG
55%
red
uctio
nin
AH
I,m
inim
um
Sa,O
2and
aro
usa
lin
dex
imp
rove
dE
SS
Imp
rove
dP
rofil
em
ood
state
Imp
rove
dvi
gour-
activ
ityand
fatig
ue-inert
iasc
ale
sC
hoic
ere
actio
ntim
eIm
pro
ved
Com
plia
nce
6.7
hp
er
nig
ht
PS
G:
poly
som
nogra
phy;
AH
I:ap
noea/h
ypop
noea
ind
ex;
Sa,O
2:
art
eria
loxy
gen
satu
ratio
n;
ES
S:
Ep
wort
hS
leep
iness
Scale
;M
SLT:
multi
ple
sleep
late
ncy
test
;B
P:
blo
od
pre
ssure
;M
WT:
main
tenance
of
wake
fuln
ess
test
;V
AS
:vi
sual
analo
gue
scale
;FO
SQ
:fu
nctio
noutc
om
esl
eep
quest
ionnaire
;S
F–3
6:
Short
Form
36
Health
Surv
ey.
Som
noD
ent1
MA
S(S
om
noM
ed
,D
ento
n,
TX
,U
SA
);M
onob
lock
ap
plia
nce
(M.
Mark
lund
,U
ME
AU
niv
ers
ity,
Sw
ed
en);
MD
SA
1(M
ed
icalD
enta
lS
leep
Ap
plia
nce;
R.J
.and
V.K
.B
irdP
tyLtd
,M
elb
ourn
e,
VIC
,A
ust
ralia
).
27
5J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA
Ta
ble
2.
Sum
mary
of
rand
om
ised
contr
olle
dtr
ials
com
parin
gm
and
ibula
rad
vancem
ent
splin
ts(M
AS
)w
ithcontin
uous
posi
tive
airw
ay
pre
ssure
(CP
AP
)
Fir
st
au
tho
r[R
ef.
]Y
ea
ro
fstu
dy
Pa
tie
nts
nD
evic
eM
ea
su
rem
en
tsS
ign
ific
an
tc
ha
ng
es
co
mp
are
dw
ith
ba
se
lin
eS
ign
ific
an
tc
ha
ng
es
co
mp
are
dw
ith
CP
AP
Tre
atm
en
tp
refe
ren
ce
CL
AR
K[5
8]
1996
23
Herb
stTM
PS
GM
AS
and
CP
AP
AI,
AH
I,m
inim
um
Sa,O
2
AH
Id
ecre
ase
din
CP
AP
19
patie
nts
MA
S,
1p
atie
nt
CP
AP
,1
patie
nt
not
usi
ng
CP
AP
or
MA
SS
SQ
CP
AP
and
MA
Sb
oth
show
ed
signifi
cant
imp
rove
ment
CP
AP
5M
AS
FE
RG
US
ON
[54]
1996
25
Snore
-guard
PS
GM
AS
and
CP
AP
imp
rove
dA
HIand
AI
CP
AP
decre
ase
dA
HI
62%
and
MA
S48%
,only
CP
AP
incre
ase
dS
a,O
2
23
patie
nts
MA
S,
2p
atie
nts
CP
AP
Quest
ionnaire
Snorin
g,
unre
fresh
ed
sleep
,sl
eep
iness
and
fatig
ue
FE
RG
US
ON
[55]
1997
20
Sile
ncer
PS
GM
AS
and
CP
AP
imp
rove
dA
HIand
AI
CP
AP
low
er
AH
I,only
CP
AP
incre
ase
dS
a,O
2
Gre
ate
rsa
tisfa
ctio
nw
ithM
AS
Quest
ionnaire
Snorin
g,
unre
fresh
ed
sleep
,sl
eep
iness
and
fatig
ue
RA
ND
ER
AT
H[5
9]
2002
20
Herb
stTM
PS
GM
AS
and
CP
AP
imp
rove
dA
HIand
aro
usa
ls
CP
AP
decre
ase
dA
HIand
imp
rove
dsl
eep
arc
hite
ctu
reM
AS
easi
er
and
pre
ferr
ed
ove
rC
PA
P
EN
GL
EM
AN
[57]
2002
48
Monob
lock
ap
plia
nce
PS
GN
/AA
HIC
PA
P.
MA
SN
op
refe
rence
ES
SC
PA
P.
MA
SFO
SQ
MA
S.
CP
AP
MW
TM
AS
5C
PA
PC
ogniti
veM
AS
5C
PA
PT
AN
[56]
2002
24
Monob
lock
ap
plia
nce
and
mod
ified
sile
ncer
PS
GM
AS
and
CP
AP
imp
rove
dA
HI,
aro
usa
ls
Only
CP
AP
incre
ase
dS
a,O
2,
CP
AP
5M
AS
inA
HIand
aro
usa
lin
dex
17
out
of
21
patie
nts
pre
ferr
ed
MA
S
ES
SM
AS
and
CP
AP
imp
rove
dM
AS
5C
PA
P
27
6O
RA
LA
PP
LIA
NC
ES

Ta
ble
2.
Contin
ued
Fir
st
au
tho
r[R
ef.
]Y
ea
ro
fstu
dy
Pa
tie
nts
nD
evic
eM
ea
su
rem
en
tsS
ign
ific
an
tc
ha
ng
es
co
mp
are
dw
ith
ba
se
lin
eS
ign
ific
an
tc
ha
ng
es
co
mp
are
dw
ith
CP
AP
Tre
atm
en
tp
refe
ren
ce
BA
RN
ES
[50]
2004
114
MD
SA
1P
SG
MA
Sand
CP
AP
imp
rove
dA
HIand
Sa,O
2,
decre
ase
dst
age
1sl
eep
and
incre
ase
dsl
ow
wave
sleep
CP
AP
.M
AS
36%
patie
nts
MA
S
ES
SIm
pro
ved
CP
AP
5M
AS
44%
patie
nts
CP
AP
MW
TIm
pro
ved
CP
AP
5M
AS
FO
SQ
Imp
rove
dFO
SQ
only
MA
Sb
ett
erth
an
pla
ceb
oP
VT
lap
ses
MA
Sd
ecre
ase
dd
iast
olic
BP
CP
AP
.M
AS
BP
MA
S.
CP
AP
,only
with
MA
Sa
signifi
cant
pro
port
ion
of
nond
ipp
er
sub
jects
regain
ed
noctu
rnal
dip
HO
EK
EM
A[6
1]
2007
48
TA
P1
Sexu
alfu
nctio
nN
oim
pro
vem
ent
MA
S5
CP
AP
N/A
para
llelst
ud
yH
OE
KE
MA
[60]
2007
20
TA
P1
PS
GM
AS
and
CP
AP
imp
rove
dA
HI,
min
Sa,O
2
MA
S5
CP
AP
N/A
para
llelst
ud
y
ES
SC
PA
Pand
MA
Sb
oth
decre
ase
dM
AS
5C
PA
P
Driv
ing
perf
orm
ance
CP
AP
and
MA
Sb
oth
imp
rove
dM
AS
5C
PA
P
HO
EK
EM
A[6
2]
2008
28
TA
P1
NT-p
ro-B
NP
MA
Ssh
ow
ed
imp
rove
ment
Only
MA
Sim
pro
ved
NT-p
ro-B
NP
N/A
para
llelst
ud
y
PS
Gp
oly
som
nogra
phy;
AI:
ap
noea
ind
ex;
AH
I:ap
noea/h
ypop
noea
ind
ex;
Sa,O
2,:
art
eria
loxy
gen
satu
ratio
n;
SS
Q:
sleep
sym
pto
ms
quest
ionnaire
;ES
S:
Ep
wort
hsl
eep
iness
scale
;FO
SQ
:fu
nctio
noutc
om
esl
eep
quest
ionnaire
;M
WT:
main
tenance
of
wake
fuln
ess
test
;P
VT:
psy
chom
oto
rvi
gila
nce
task
;B
P:
blo
od
pre
ssure
;N
A:
nonap
plic
ab
le;
NT-
pro
-BN
P:
am
ino-t
erm
inalfr
agm
ent
of
pro
-bra
innatr
iure
ticp
ep
tide.
Herb
stTM
(Gre
at
Lake
sO
rthod
ontic
sLtd
,Tonaw
and
a,
NY
,U
SA
).
27
7J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA

4-yr follow-up [65]. According to predetermined criteria for OSAH (apnoea index (AI) o5 orAHIo10 events?h-1), 63% of the patients in the MAS group attained normalisation after 4 yrs, aproportion that was significantly higher than the 33% among the patients in the UPPP group. Thisstudy suggests that MAS was more effective than UPPP in improving indices of sleep-disorderedbreathing. However, the significance of this finding is questionable, as there is no definitive evidence ofthe effectiveness of this type of corrective upper airway surgery. MAS have also been used ascombination therapy in patients who have had an unsuccessful response to UPPP [80].
Cardiovascular health
There are two randomised controlled trials with intention-to-treat analysis [48, 50] and threenonrandomised prospective studies [81–83] in which MAS treatment of OSAH has been shown toreduce blood pressure measurements. These changes are primarily in diastolic blood pressure andre-establishing the nocturnal dip. One study found a correlation between the improvement in AHIand a decrease in blood pressure after MAS treatment [81]. Another study, found that there wasno change in blood pressure with CPAP, whereas MAS significantly improved the nocturnaldiastolic blood pressure and increased the proportion of subjects with a normal night-time dip inblood pressure [50]. In the evaluation of biomarkers for oxidative stress and inflammation, onestudy has shown that treatment with MAS improves cardiovascular pathophysiologic factors, suchas endothelial function after 3 months and 1 yr of MAS treatment [84]. The endothelial functionin the MAS group was not different from a reference non-OSA group. A year of treatment resultedin a normalisation of malondialdehyde levels and a decrease in thiobarbituric acid-reactivesubstance levels, despite residual sleep-disordered breathing (average AHI of 19 events?h-1). In aparallel study, comparing MAS with CPAP, MAS improved amino-terminal fragment of pro-brainnatriuretic peptide [64].
Partner health status
Partners of patients with OSAH have impaired health status, probably due to sleep fragmentationrelated to the patient’s loud snoring and restless sleep pattern. Treatment of patients with snoringand OSAH might be beneficial, not only for the patient, but for the bed partner and the couplerelationship. MCARDLE et al. [85] reported significant impairment in sleep quality of OSAH bedpartners without improvement in objective sleep quality after treatment with CPAP. In contrast,DOHERTY et al. [86], showed significant improvements in bed partner health status followingCPAP. In one study sleep changed to better or much better in 64.1% of the bed partners followingMAS treatment for OSAH [87] in another report, an improvement in intimate relationships andsexual activity following MAS treatment for OSAH was seen [71].
Treatment
Predictors of treatment success
A variety of clinical, physiological and PSG variables have been identified as possible predictors ofMAS treatment success [88–91]. It has been suggested that, a younger patient [92, 93] with a lowerAHI [46, 88, 93], a smaller neck circumference [50], a lower body mass index [91] and positionalOSAH [86, 92, 94] would be more likely to achieve treatment success with MAS. Patients whoachieve a greater degree of mandibular advancement have the highest decrease in AHI [35, 95],and females have higher success rates than males. Treatment success may be inversely related topre-treatment severity, but this relationship may just be a function of the definition of treatmentsuccess, although one study has shown that the higher the AHI pre-treatment, the greater thedecrease in AHI that could be achieved [44].
Several upper airway skeletal and soft tissue measurements made from pre-treatment lateralcephalometry have been shown to be associated with treatment success. These include a more
27
8O
RA
LA
PP
LIA
NC
ES

micrognathic or retrognathic mandible, small soft palate and tongue and larger retropalatal area[19, 50, 96, 97]. Upper airway fluoroscopy has also been proposed as a technique to guidesuccessful MAS therapy. A hypopharyngeal site of obstruction may be associated with a bettertreatment outcome. A study of upper airway MRI during a Muller manoeuvre, together withmandibular advancement, has shown that improvement in upper airway patency correlates withtreatment success [98]. However, there is considerable overlap between good and poor treatmentresponse in these studies. More recently, physiological assessments of nasal resistance andpulmonary function have shown to be of some predictive value [99, 100]. The utility of anytreatment recommendation for MAS based on clinical features, OSAH severity or upper airwayanatomy is still questionable and requires prospective validation.
Treatment adherance
The treatment adherence and side-effects of oralappliance treatment differ depending on the typeof the appliance, disease severity and patient supervision [101, 102]. Adherence is usuallymeasured subjectively, with the exception of one study in which a compliance monitor indicatedthat the MAS was worn for a mean of 6.8 h per night [103]. Self-reported treatment adherence hasbeen reported as high as 96% for patients using MAS .75% of the nights and 80% of patientsusing MAS .75% of each night [54].
Treatment adherence varies between each oral appliance type and appears better with mandibularadvancement rather than tongue retaining appliance or boil and bite type appliances. 40% of non-adherence occurs within the first 6 months [104]. The most common reasons to stop using theappliance are discomfort and/or because the patient finds it cumbersome (46%) and it has no orlittle effect (36%).
Adherence rates vary widely between studies with a minimum of 4% to a maximum of 82% ofadherence after 1 yr of treatment [78]. Adherence rates appear to decrease with the duration ofuse. In a study of 630 patients, MARKLUND et al. [88] described an adherence of 75% of the patientsafter 12 months of treatment. After a 2–5-yr follow-up period, studies have revealed adherencerates from 48% up to 90% [105–107], and this has been reported as 60% at 1 yr and 48% at 2 yrs.Previous experience with nasal CPAP suggests that self-reported treatment adherence tends tooverestimate actual use. Studies with CPAP have identified that subjective adherence is oftenhigher than objective adherence. Therefore, until there is an adherence monitor available for oralappliance therapy, caution should be taken in the reporting of subjective oral appliance adherence.Table 3 provides a summary of studies evaluating oral appliance adherence rates after a minimumof 1-yr treatment plan.
Side-effects
The main reasons for discontinuing treatment have been reported to be insufficient reduction ofsnoring and the presence of side-effects [95]. Most side-effects caused by MAS are usuallydescribed as mild and transient, most frequently reported as dry mouth, excessive salivation,mouth or teeth discomfort, muscle tenderness and jaw stiffness. Significant and persistenttemporomandibular joint (TMJ) problems are rare [1]. One study evaluated the TMJ of sevenpatients, using MRI, over a mean period of 11 months and concluded that MAS, in the titratedposition, appeared to be innocuous to the TMJ in OSA patients [95]. Excessive salivation, mouthdryness, morning-after occlusal changes and discomfort in the gums, teeth or jaw are commonside-effects in the first weeks of MAS therapy, but usually resolve with time [104, 109]. Morepersistent and severe side-effects, which include TMJ dysfunction and dental crown damage,appear uncommon [108]. MAS adjustment can decrease side-effects by reducing pressure on theanterior teeth and excessive mandibular advancement. Side-effects vary between the types of oralappliance used, with tongue pain occurring in tongue retention appliances and gagging associatedwith appliances that have a maxillary component to modify soft palate position. Long-term side-effects are more recently described evaluating oral appliance side-effects over a period of more
27
9J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA

than 5 yrs. ALMEIDA and co-workers [109, 110], using a titratable MAS, demonstrated that MASused for a mean period of 7.3 yrs have a significant impact on occlusal and dental structures.Changes observed in craniofacial structures were mainly related to significant tooth movements.MARKLUND [109] observed that the frequent use of a single piece MAS with full occlusal coveragefor 5 yrs resulted in median reductions in overjet and overbite of 0.6 mm in patients with eithersnoring or OSAH. Table 4 summarises the long-term side-effects of MAS on occlusalmeasurements [111–114].
Cost
The cost of oral-appliance therapy varies depending on the types of oral appliances used and theextent and expertise of the dental supervision. Consensus opinion indicates that a prefabricatedoral appliance can range from J35 to J75 and custom made oral appliances range from J75 toover J700 [1]. Oral appliances usually remain effective for 2–5 yrs, but they can break and requireeither repair or replacement. Dental service fees vary greatly between J150–1,800, depending onthe time spent caring for the patient and geographical economical factors. Costs can equal orexceed those associated with nasal CPAP therapy. There is increasing evidence that both oralappliances and nasal CPAP are cost-effective treatments for OSAH [115, 116].
Treatment recommendations
A Cochrane systematic review performed a variety of meta-analyses on data from 16 randomisedcontrolled trials involving 745 patients available up to 2005, and concluded that there was
Table 3. Adherence rates of mandibular advancement splints in selected studies that evaluated adherenceafter a minimum of 1 year
First author [Ref.] Year of study Interval months Patients n Comliance rateWCS/BCS
MCGOWN [101] 2001 22 166 42/56DORT [102] 2004 22 110 40/57MARKLUND [88] 2004 12 630 75/76DE ALMEIDA [104] 2005 68 544 30/64MARKLUND [108] 2006 60 450 56/56GINDRE [34] 2008 17 66 82/82
WCS: worst case scenario, which relates to an analysis interpretation of patients who did not return thequestionnaires as compliance failures. BCS: best case scenario, which relates only to the percentage ofpatients who responded to the questionnaire.
Table 4. Long-term side-effects of mandibular advancement stent on occlusal measurements
First author [Ref.] Year ofstudy
Patients n Intervalyears
Change in OBmm
Change in OJmm
MARKLUND [66] 2001 75 2.5 -0.5 -0.6ROBERTSON [111] 2001 100 2.5 -1.02 -1.06ROSE [112] 2002 34 2.5 -1.1 -1.3GHAZAL [113] 2008 24 2.5 3.2 2.5ALMEIDA [109, 110] 2006 70 7.6 -1.9/-2.8 -1.2/-2.6MARKLUND [108] 2006 450 5.4 -0.6 -0.6HAMMOND [114] 2007 64 2.1 -0.3 -0.2
OB: overbite, vertical overlapping of upper teeth over lower teeth. OJ: overjet, horizontal projection of upperteeth beyond the lower teeth.
28
0O
RA
LA
PP
LIA
NC
ES

increasing evidence that oral appliances improve subjective sleepiness and sleep-disorderedbreathing compared with control appliances [4]. However, it recommended that until there wasmore definitive evidence on the effectiveness of oral appliance compared with CPAP, oralappliance therapy should be restricted to patients with mild, symptomatic OSAH and thosepatients who are unwilling or unable to comply with CPAP therapy. The American Academy ofSleep Medicine [5] reviewed similar data to the Cochrane Collaboration and recommended thatoral appliances were indicated for use in patients with mild–moderate OSAH who prefer them toCPAP, or who do not respond to, are not appropriate candidates for, or who fail treatment withCPAP. They recommended CPAP therapy whenever possible for patients with severe OSAH.
These practice parameters emphasise the importance of a combined medical and dental approachto oral appliance treatment. MAS therapies should not be used in patients who have majorperiodontal disease. Follow-up sleep monitoring is needed to verify the efficacy of oral appliancetherapy. OSAH is a chronic disease and therefore patients treated with oral appliances requirelifelong follow-up to monitor patient adherence, long-term dental follow-up, evaluations of theoral appliance deterioration or maladjustment, and evaluation of the health of the oral structuresand integrity of the occlusion.
Statement of Interest
None declared.
References1. Ferguson KA, Cartwright R, Rogers R, et al. Oral appliances for snoring and sleep apnea: A review. Sleep 2006; 29:
244–262.
2. Fleetham JA. Sleep Apnea: Oral appliances. In: Laurent GJ, Shapiro SD, eds. Encyclopedia of Respiratory
Medicine. Volume 40. Elsevier Ltd, London, 2007; pp. 67–70.
3. Hoffstein V. Review of oral appliances for treatment of sleep-disordered breathing. Sleep Breath 2007; 11: 1–22.
4. Lim J, Lasserson TJ, Fleetham J, et al. Oral appliances for obstructive sleep apnea. Cochrane Database Syst Rev
2006; I: CD004435.
5. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive
sleep apnea with oral appliances: An update for 2005. Sleep 2006; 29: 240–243.
6. Nelson S, Kulnis R. Snoring and sleep disturbance among children from an orthodontic setting. Sleep Breath
2001; 5: 63–70.
7. Carvalho FR, Lentini-Oliveira D, Machado MA, et al. Oral appliances and functional orthopaedic appliances for
obstructive sleep apnoea in children. Cochrane Database Syst Rev 2007; 2: CD005520.
8. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea
syndrome. Sleep 2004; 27: 761–766.
9. Cozza P, Polimeni A, Ballanti F. A modified monobloc for the treatment of obstructive sleep apnoea in paediatric
patients. Eur J Orthod 2004; 26: 523–530.
10. Schmidt-Nowara WW, Meade TE, Hays MB. Treatment of snoring and obstructive sleep apnea with a dental
orthosis. Chest 1991; 99: 1378–1385.
11. Vanderveken OM, Devolder A, Marklund M, et al. Comparison of a custom-made and a thermoplastic oral
appliance for the treatment of mild sleep apnea. Am J Respir Crit Care Med 2008; 178: 197–202.
12. Sjoholm TT, Lowe AA, Miyamoto K, et al. Sleep bruxism in patients with sleep-disordered breathing. Arch Oral
Biol 2000; 45: 889–896.
13. Cartwright RD, Samelson CF. The effects of a nonsurgical treatment for obstructive sleep apnea. The tongue-
retaining device. JAMA 1982; 248: 705–709.
14. Cartwright RD. Predicting response to the tongue retaining device for sleep apnea syndrome. Arch Otolaryngol
1985; 111: 385–388.
15. Cartwright R, Stefoski D, Caldarelli D, et al. Toward a treatment logic for sleep apnea: the place of the tongue
retaining device. Behav Res Ther 1988; 26: 21–26.
16. Deane SA, Cistulli PA, Ng AT, et al. Comparison of mandibular advancement splint and tongue stabilizing device
in obstructive sleep apnea: a randomized controlled trial. Sleep 2009; 32: 648–653.
17. Fleetham JA. Upper airway imaging in relation to obstructive sleep apnea. In: Phillipson EA, Bradley TD, eds.
Clinics in Chest Medicine. Breathing Disorders in Sleep. Saunders, Philadelphia PA, 1992; pp. 399–416.
18. Ferguson KA, Love LL, Ryan CF. Effect of mandibular and tongue protrusion on upper airway size during
wakefulness. Am J Respir Crit Care Med 1997; 151: 1748–1754.
28
1J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA

19. Ryan CF, Love LL, Peat D, et al. Mandibular advancement oral appliance therapy for obstructive sleep apnea:
Effect on awake calibre of the velopharynx. Thorax 1999; 54: 972–977.
20. Eveloff SE, Rosenberg CL, Carlisle CC, et al. Efficacy of a Herbst mandibular advancement device in obstructive
sleep apnea. Am J Respir Crit Care Med 1994; 149: 905–909.
21. Lowe A, Fleetham J, Ryan F, et al. Effects of a mandibular repositioning appliance used in the treatment of
obstructive sleep apnea on tongue muscle activity. In: Issa FG, Suratt PM, Remmers JE, eds. Sleep and
Respiration. Wiley-Liss, New York, 1990: pp. 395–405.
22. Ng AT, Gotsopoulos H, Qian J, et al. Effect of oral appliance therapy on upper airway collapsibility in obstructive
sleep apnea. Am J Respir Crit Care Med 2003; 168: 238–241.
23. Sam K, Lam B, Ooi CG, et al. Effect of a non-adjustable oral appliance on upper airway morphology in
obstructive sleep apnoea. Respir Med 2006; 100: 897–902.
24. Kyung SH, Park YC, Pae EK. Obstructive sleep apnea patients with the oral appliance experience pharyngeal size
and shape changes in three dimensions. Angle Orthod 2005; 75: 15–22.
25. Zhao X, Liu Y, Gao Y. Three-dimensional upper-airway changes associated with various amounts of mandibular
advancement in awake apnea patients. Am J Orthod Dentofacial Orthop 2008; 133: 661–668.
26. Chan ASLSK, Schwab RJ, Zeng B, et al. The effect of mandibular advancement on upper airway structure in
obstructive sleep apnoea. Sleep Biol Rhythms 2009; 7: Suppl. 1, A17.
27. Adachi S, Lowe AA, Tsuchiya M, et al. Genioglossus muscle activity and inspiratory timing in obstructive sleep
apnea. Am J Orthod Dentofacial Orthop 1993; 104: 138–145.
28. Cunali PA, Almeida FR, Santos CD, et al. Prevalence of temporomandibular disorders in obstructive sleep apnea
patients referred for oral appliance therapy. J Orofac Pain 2009; 23: 339–344.
29. de Almeida FR, Bittencourt LR, de Almeida CI, et al. Effects of mandibular posture on obstructive sleep apnea
severity and the temporomandibular joint in patients fitted with an oral appliance. Sleep 2002; 25: 507–513.
30. Cunali PA, Almeida FR, Santos CD, et al. Mandibular exercises improve mandibular advancement device therapy
for obstructive sleep apnoea. Sleep Breath 2010; [Epub ahead of print DOI: 10.1007/s11325-010-0428-2].
31. Ohayon MM, Li KK, Guilleminault C. Risk factors for sleep bruxism in the general population. Chest 2001; 119:
53–61.
32. Landry ML, Rompre PH, Manzini C, et al. Reduction of sleep bruxism using a mandibular advancement device:
an experimental controlled study. Int J Prosthodont 2006; 19: 549–556.
33. Gagnon Y, Mayer P, Morisson F, et al. Aggravation of respiratory disturbances by the use of an occlusal splint in
apneic patients: a pilot study. Int J Prosthodont 2004; 17: 447–453.
34. Gindre L, Gagnadoux F, Meslier N, et al. Mandibular advancement for obstructive sleep apnea: dose effect on
apnea, long-term use and tolerance. Respiration 2008; 76: 386–392.
35. Kato J, Isono S, Tanaka A, et al. Dose-dependent effects of mandibular advancement on pharyngeal mechanics
and nocturnal oxygenation in patients with sleep-disordered breathing. Chest 2000; 117: 1065–1072.
36. Fleury B, Rakotonanahary D, Petelle B, et al. Mandibular advancement titration for obstructive sleep apnea:
optimization of the procedure by combining clinical and oximetric parameters. Chest 2004; 125: 1761–
1767.
37. Tegelberg A, Walker-Engstrom ML, Vestling O, et al. Two different degrees of mandibular advancement with a
dental appliance in treatment of patients with mild to moderate obstructive sleep apnea. Acta Odontol Scand
2003; 61: 356–362.
38. Raphaelson MA, Alpher EJ, Bakker KW, et al. Oral appliance therapy for obstructive sleep apnea syndrome:
progressive mandibular advancement during polysomnography. Cranio 1998; 16: 44–50.
39. Petelle B, Vincent G, Gagnadoux F, et al. One-night mandibular advancement titration for obstructive sleep
apnea syndrome: a pilot study. Am J Respir Crit Care Med 2002; 165: 1150–1153.
40. Tsai WH, Vazquez JC, Oshima T, et al. Remotely controlled mandibular positioner predicts efficacy of oral
appliances in sleep apnea. Am J Respir Crit Care Med 2004; 170: 366–370.
41. Kuna ST, Giarraputo PC, Stanton DC, et al. Evaluation of an oral mandibular advancement titration appliance.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 101: 593–603.
42. Krishnan V, Collop NA, Scherr SC. An evaluation of a titration strategy for prescription of oral appliances for
obstructive sleep apnea. Chest 2008; 133: 1135–1141.
43. Almeida FR, Parker J, Hodges J, et al. Effect of a titration polysomnogram on treatment success with a
mandibular repositioning appliance. J Clin Sleep Med 2009; 5: 198–204.
44. Henke KG, Frantz DE, Kuna ST. An oral elastic mandibular advancement device for obstructive sleep apnea. Am
J Respir Crit Care Med 2000; 161: 420–425.
45. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances, Sleep 1995; 18:
511–513.
46. Mehta A, Qian J, Petocz P, et al. A randomized, controlled study of a mandibular advancement splint for
obstructive sleep apnea. Am J Respir Crit Care Med 2001; 163: 1457–1461.
47. Gotsopoulos H, Chen C, Qian J, et al. Oral appliance therapy improves symptoms in obstructive sleep apnoea
syndrome. A randomised controlled trial. Am J Respir Crit Care Med 2002; 166: 743–748.
48. Gotsopoulos H, Kelly JJ, Cistulli PA. Oral appliance therapy reduces blood pressure in obstructive sleep apnea: A
randomized, controlled trial. Sleep 2004; 27: 934–941.
28
2O
RA
LA
PP
LIA
NC
ES

49. Naismith SL, Winter VR, Hickie IB, et al. Effect of oral appliance therapy on neurobehavioral functioning in
obstructive sleep apnea: a randomized controlled trial. J Clin Sleep Med 2005; 1: 374–380.
50. Barnes M, McEvoy RD, Banks S, et al. Efficacy of positive airway pressure and oral appliance in mild to moderate
obstructive sleep apnea. Am J Respir Crit Care Med 2004; 170: 656–664.
51. Johnston CD, Gleadhill IC, Cinnamond MJ, et al. Mandibular advancement appliances and obstructive sleep
apnoea: a randomized clinical trial. Eur J Orthod 2002; 24: 251–262.
52. Dort L, R Brant, A randomized, controlled, crossover study of a noncustomized tongue retaining device for sleep
disordered breathing. Sleep Breath 2008; 12: 369–373.
53. Ono T Lowe AA, Ferguson KA, et al. A tongue retaining device and sleep-state genioglossus muscle activity in
patients with obstructive sleep apnea. Angle Orthod 1996; 66: 273–280.
54. Ferguson KA, Ono T, Lowe AA, et al. A randomized crossover study of an oral appliance versus nasal-continuous
positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest 1996; 109: 1269–1275.
55. Ferguson KA, Ono T, Lowe AA, et al. A short term controlled trial of an adjustable oral appliance for the
treatment of mild to moderate obstructive sleep apnoea. Thorax 1997; 52: 362–368.
56. Tan YK, L’Estrange PR, Luo YM, et al. Mandibular advancement splints and continuous positive airway pressure
in patients with obstructive sleep apnoea: a randomized cross-over trial. Eur J Orthod 2002; 24: 239–249.
57. Engleman HM, McDonald JP, Graham D, et al. Randomized crossover trial of two treatments for sleep apnea/
hypopnea syndrome: Continuous positive airway pressure and mandibular repositioning splint. Am J Respir Crit
Care Med 2002; 166: 855–859.
58. Clark GT, Blumenfeld I, Yoffe N, et al. A crossover study comparing the efficacy of continuous positive airway
pressure with anterior mandibular positioning devices on patients with obstructive sleep apnea. Chest 1996; 109:
1477–1483.
59. Randerath WJ, Heise M, Hinz R, et al. An individually adjustable oral appliance versus continuous positive airway
pressure in mild-to-moderate obstructive sleep apnea syndrome. Chest 2002; 122: 569–575.
60. Hoekema A, Stegega B, Bakker M, et al. Simulated driving in obstructive sleep apnoea-hypopnoea; effects of oral
appliances and continuous positive airway pressure. Sleep Breath 2007; 11: 129–138.
61. Hoekema A, Stel AL, Stegenga B, et al. Sexual function and obstructive sleep apnea-hypopnea: a randomized
clinical trial evaluating the effects of oral-appliance and continuous positive airway pressure therapy. J Sex Med
2007; 4: 1153–1162.
62. Hoekema A, Voors AA, Wijkstra PJ, et al. Effects of oral appliances and CPAP on the left ventricle and natriuretic
peptides. Int J Cardiol 2008; 128: 232–239.
63. Naismith S, Winter V, Gotsopoulos H, et al. Neurobehavioral functioning in obstructive sleep apnea: differential
effects of sleep quality, hypoxemia and subjective sleepiness. J Clin Exp Neuropsychol 2004; 26: 43–54.
64. Marin JM, Carrizo SJ, Vicente E, et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-
hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet
2005; 365: 1046–1053.
65. Walker-Engstrom ML, Tegelberg A, Wilhelmsson B, et al. 4-year follow-up of treatment with dental appliance or
uvulopalatopharyngoplasty in patients with obstructive sleep apnea: a randomized study. Chest 2002; 121: 739–746.
66. Marklund M, Sahlin C, Stenlund H, et al. Mandibular advancement device in patients with obstructive sleep
apnea: Long-term effects on apnea and sleep. Chest 2001; 120: 162–169.
67. Smith DM, Stradling JR. Can mandibular advancement devices be a satisfactory substitute for short term use in
patients on nasal continuous positive airway pressure? Thorax 2002; 57: 305–308.
68. Denbar MA. A case study involving the combination treatment of an oral appliance and auto-titrating CPAP
unit. Sleep Breath 2002; 6: 125–128.
69. Hans MG, Nelson S, Luks VG, et al. Comparison of two dental devices for treatment of obstructive sleep apnea
syndrome (OSAS). Am J Orthod Dentofacial Orthop 1997; 111: 562–570.
70. Lawton HM, Battagel JM, Kotecha B. A comparison of the Twin Block and Herbst mandibular advancement
splints in the treatment of patients with obstructive sleep apnoea: A prospective study. Eur J Orthod 2005; 27:
82–90.
71. Gauthier L, Laberge L, Beaudry M, et al. Efficacy of two mandibular advancement appliances in the management
of snoring and mild-moderate sleep apnea: a cross-over randomized study. Sleep Med 2009; 10: 329–336.
72. Ghazal A, Sorichter S, Jonas I, et al. A randomized prospective long-term study of two oral appliances for sleep
apnoea treatment. J Sleep Res 2009; 18: 321–328.
73. Bloch KE, Iseli A, Zhang JN, et al. A randomized, controlled crossover trial of two oral appliances for sleep apnea
treatment. Am J Respir Crit Care Med 2000; 162: 246–251.
74. Lamont J, Baldwin DR, Hay KD, et al. Effect of two types of mandibular advancement splints on snoring and
obstructive sleep apnoea. Eur J Orthod 1998; 20: 293–297.
75. Pitsis AJ, Darendeliler MA, Gotsopoulos H, et al. Effect of vertical dimension on efficacy of oral appliance therapy
in obstructive sleep apnea. Am J Respir Crit Care Med 2002; 166: 860–864.
76. Barthlen GM, Brown LK, Wiland MR, et al. Comparison of three oral appliances for treatment of severe
obstructive sleep apnea syndrome. Sleep Med 2000; 1: 299–305.
77. Wilhelmsson B, Tegelberg A, Walker-Engstrom ML, et al. A prospective randomized study of a dental appliance
compared with uvulopalatopharyngoplasty in the treatment of obstructive sleep apnoea. Acta Otolaryngol 1999;
119: 503–509.
28
3J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA
78. Walker-Engstrom ML, Wilhelmsson B, Tegelberg A, et al. Quality of life assessment of treatment with dental
appliance or UPPP in patients with mild to moderate obstructive sleep apnoea. A prospective randomized 1-year
follow-up study. J Sleep Res 2000; 9: 303–308.
79. Tegelberg A, Wilhelmsson B, Walker-Engstrom ML, et al. Effects and adverse events of a dental appliance for
treatment of obstructive sleep apnoea. Swed Dent J 1999; 23: 117–126.
80. Millman RP, Rosenberg CL, Carlisle CC, et al. The efficacy of oral appliances in the treatment of persistent sleep
apnea after uvulopalatopharyngoplasty. Chest 1998; 113: 992–996.
81. Yoshida K. Effect on blood pressure of oral appliance therapy for sleep apnea syndrome. Int J Prosthodont 2006;
19: 61–66.
82. Otsuka R, Ribeiro de Almeida F, Lowe AA, et al. The effect of oral appliance therapy on blood pressure in patients
with obstructive sleep apnea. Sleep Breath 2006; 10: 29–36.
83. Andren A, Sjoquist M, Tegelberg A. Effects on blood pressure after treatment of obstructive sleep apnoea with a
mandibular advancement appliance - a three-year follow-up. J Oral Rehabil Oct 2009; 36: 719–725.
84. Itzhaki S, Dorchin H, Clark G, et al. The effects of 1-year treatment with a Herbst mandibular advancement splint
on obstructive sleep apnea, oxidative stress, and endothelial function. Chest 2007; 131: 740–749.
85. McArdle N, Kingshott R, Engleman HM, et al. Partners of patients with sleep apnoea/hypopnoea syndrome:
effect of CPAP treatment on sleep quality and quality of life. Thorax 2001; 56: 513–518.
86. Doherty LS, Kiely JL, Lawless G, et al. Impact of nasal continuous positive airway pressure therapy on the quality
of life of bed partners of patients with obstructive sleep apnea syndrome. Chest 2003; 124: 2209–2214.
87. Bates CJ, McDonald JP. Patients’ and sleeping partners’ experience of treatment for sleep-related breathing
disorders with a mandibular repositioning splint. Br Dent J 2006; 200: 95–101.
88. Marklund M, Stenlund H, Franklin KA. Mandibular advancement devices in 630 men and women with
obstructive sleep apnea and snoring: Tolerability and predictors of treatment success. Chest 2004; 125:
1270–1278.
89. Ng AT, Qian J, Cistulli PA. Oropharyngeal collapse predicts treatment response with oral appliance therapy in
obstructive sleep apnea. Sleep 2006; 29: 666–671.
90. Horiuchi A, Suzuki M, Ookubo M, et al. Measurement techniques predicting the effectiveness of an oral
appliance for obstructive sleep apnea hypopnea syndrome. Angle Orthod 2005; 75: 1003–1011.
91. Otsuka R, Almeida FR, Lowe AA, et al. A comparison of responders and nonresponders to oral appliance therapy
for the treatment of obstructive sleep apnea. Am J Orthod Dentofacial Orthop 2006; 129: 222–229.
92. Liu Y, Park YC, Lowe AA, et al. Supine cephalometric analyses of an adjustable oral appliance used in the
treatment of obstructive sleep apnea. Sleep Breath 2000; 4: 59–66.
93. Liu Y, Lowe AA, Fleetham JA, et al. Cephalometric and physiologic predictors of the efficacy of an adjustable oral
appliance for treating obstructive sleep apnea. Am J Orthod Dentofacial Orthop 2001; 120: 639–647.
94. Yoshida K. Influence of sleep posture on response to oral appliance therapy for sleep apnea syndrome. Sleep 2001;
24: 538–544.
95. de Almeida FR, Bittencourt LR, de Almeida CI, et al. Effects of mandibular posture on obstructive sleep apnea
severity and the temporomandibular joint in patients fitted with an oral appliance. Sleep 2002; 25: 507–513.
96. Mayer G, Meier-Ewert K. Cephalometric predictors for orthopaedic mandibular advancement in obstructive
sleep apnoea. Eur J Orthod 1995; 17: 35–43.
97. Otsuka R, Almeida FR, Lowe AA, et al. A comparison of responders and nonresponders to oral appliance therapy
for the treatment of obstructive sleep apnea. Am J Orthod Dentofacial Orthop 2006; 129: 222–229.
98. Sanner BM, Heise M, Knoben B, et al. MRI of the pharynx and treatment efficacy of a mandibular advancement
device in obstructive sleep apnoea syndrome. Eur Respir J 2002; 20: 143–150.
99. Zeng B, Ng AT, Darendeliler MA, et al. Use of flow-volume curves to predict oral appliance treatment outcome
in obstructive sleep apnea. Am J Respir Crit Care Med 2007; 175: 726–730.
100. Zeng B, Ng AT, Qian J, et al. Influence of nasal resistance on oral appliance treatment outcome in obstructive
sleep apnea. Sleep 2008; 31: 543–547.
101. McGown AD, Makker HK, Battagel JM, et al. Long-term use of mandibular advancement splints for snoring and
obstructive sleep apnoea: a questionnaire survey. Eur Respir J 2001; 17: 462–466.
102. Dort LC, J Hussein, Snoring and obstructive sleep apnea: compliance with oral appliance therapy. J Otolaryngol
2004; 33: 172–176.
103. Lowe AA, Sjoholm TT, Ryan CF, et al. Treatment, airway and compliance effects of a titratable oral appliance.
Sleep 2000; 23: Suppl. 4, S172–S178.
104. de Almeida FR, Lowe AA, Tsuiki S, et al. Long-term compliance and side effects of oral appliances used for the
treatment of snoring and obstructive sleep apnea syndrome. J Clin Sleep Med 2005; 1: 143–152.
105. Yoshida K. Effects of a mandibular advancement device for the treatment of sleep apnea syndrome and snoring
on respiratory function and sleep quality. Cranio 2000; 18: 98–105.
106. Clark GT, Sohn JW, Hong CN. Treating obstructive sleep apnea and snoring: assessment of an anterior
mandibular positioning device. J Am Dent Assoc 2000; 131: 765–771.
107. Pantin CC, Hillman DR, Tennant M. Dental side effects of an oral device to treat snoring and obstructive sleep
apnea. Sleep 1999; 22: 237–240.
108. Marklund M. Predictors of long-term orthodontic side effects from mandibular advancement devices in patients
with snoring and obstructive sleep apnea. Am J Orthod Dentofacial Orthop 2006; 129: 214–221.
28
4O
RA
LA
PP
LIA
NC
ES

109. Almeida FR, Lowe AA, Otsuka R, et al. Long-term sequelae of oral appliance therapy in obstructive sleep apnea
patients: Part 2. Study-model analysis. Am J Orthod Dentofacial Orthop 2006; 129: 205–213.
110. Almeida FR, Lowe AA, Sung JO, et al. Long-term sequellae of oral appliance therapy in obstructive sleep apnea
patients: Part 1. Cephalometric analysis. Am J Orthod Dentofacial Orthop 2006; 129: 195–204.
111. Robertson CJ. Dental and skeletal changes associated with long-term mandibular advancement. Sleep 2001; 24:
531–537.
112. Rose EC, Barthlen GM, Staats R, et al. Therapeutic efficacy of an oral appliance in the treatment of obstructive
sleep apnea: a 2-year follow-up. Am J Orthod Dentofacial Orthop 2002; 121: 273–279.
113. Ghazal A, Jonas IE, Rose EC. Dental side effects of mandibular advancement appliances - a 2-year follow-up.
J Orofac Orthop 2008; 69: 437–447.
114. Hammond RJ, Gotsopoulos H, Shen G, et al. A follow-up study of dental and skeletal changes associated with
mandibular advancement splint use in obstructive sleep apnea. Am J Orthod Dentofacial Orthop 2007; 132:
806–814.
115. Ayas NT, FitzGerald JM, Fleetham JA, et al. Cost-effectiveness of continuous positive airway pressure for
moderate to severe obstructive sleep apnea hypopnea. Arch Intern Med 2006; 166: 977–984.
116. Sadatsafavi M, Marra C, Ayas N, et al. Cost-effectiveness of oral appliances in the treatment of obstructive sleep
apnea-hypopnea. Sleep Breath 2009; 13: 241–252.
28
5J.
A.
FL
EE
TH
AM
AN
DF
.R.
AL
ME
IDA
Related Documents