Optimized Multidisciplinary Care Teams Enhance Antiretroviral Therapy Adherence --What We Know Michael Horberg, MD MAS FACP Director, HIV/AIDS Kaiser Permanente Executive Director Research, Mid-Atlantic Permanente Medical Group Clinical Lead, HIV/AIDS, Care Management Institute Vice-Chair, HIV Medicine Association HIVI HIV Initiative of Kaiser Permanente and Care Management Institute

Optimized Multidisciplinary Care Teams Enhance Antiretroviral Therapy Adherence --What We Know Michael Horberg, MD MAS FACP Director, HIV/AIDS Kaiser Permanente.
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Optimized Multidisciplinary Care Teams Enhance Antiretroviral Therapy
Adherence--What We Know
Michael Horberg, MD MAS FACPDirector, HIV/AIDS Kaiser PermanenteExecutive Director Research, Mid-Atlantic Permanente Medical GroupClinical Lead, HIV/AIDS, Care Management InstituteVice-Chair, HIV Medicine Association
HIVI HIV Initiative of Kaiser Permanente and Care Management Institute

Why The Care Team as Necessary?
• Doctors don’t always discuss adherence with the patient or don’t emphasize it enough Nachega, IAPAC/NIMH 2011; Golin, JGIM, 2004
• Patient treatment adherence is not static over time Leading to changes in viral control over time (Mugavero,
IAPAC/NIMH 2011)
• Care necessities evolve over time drug-drug interactions, co-morbidities do too These impact adherence also
• Structural issues can impact adherence Including transportation, ease of refills
Slide 2
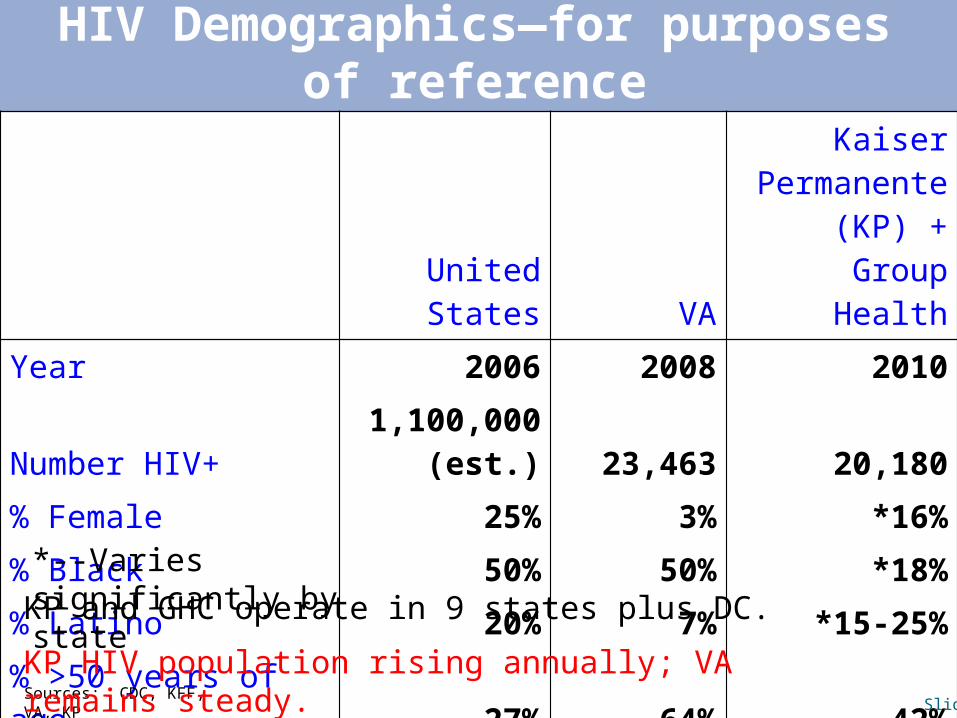
HIV Demographics—for purposes of reference
United States VA
Kaiser Permanente (KP)
+ Group Health
Year 2006 2008 2010
Number HIV+ 1,100,000 (est.) 23,463 20,180
% Female 25% 3% *16%
% Black 50% 50% *18%
% Latino 20% 7% *15-25%
% >50 years of age 27% 64% 42%
Sources: CDC, KFF, VA, KP
*--Varies significantly by state
Slide 3
KP and GHC operate in 9 states plus DC.
KP HIV population rising annually; VA remains steady.

KP Non-NQF HIV Quality Measures
non-NQF Measures: All Sites Combined: 2007, 2008, 2009KPCO and KPHI data not available for 2007
55.4
88.6
27.1
61.8
93.8
59.3
88.8
25.7
60.5
94.0
61.7
87.5
25.6
62.4
94.3
0102030405060708090
100
HIV Testing Among STI Positives
(3 STI)
CD4 Measured in 90 days of Identified HIV+
CD4 < 200 Among Newly
Diagnosed HIV+
Adherenceto ART ≥90%
Median ARTAdherence
Perc
ent
2007 2008 2009

Our Non-NQF HIV Quality Measures
non-NQF Measures: All Sites Combined: 2007, 2008, 2009KPCO and KPHI data not available for 2007
55.4
88.6
27.1
61.8
93.8
59.3
88.8
25.7
60.5
94.0
61.7
87.5
25.6
62.4
94.3
0102030405060708090
100
HIV Testing Among STI Positives
(3 STI)
CD4 Measured in 90 days of Identified HIV+
CD4 < 200 Among Newly
Diagnosed HIV+
Adherenceto ART ≥90%
Median ARTAdherence
Perc
ent
2007 2008 2009
Care coordination key here.
Many person effort necessary—not justthe physician!

Our NQF/NCQA HIV Quality Performance
NQF Endorsed Measures--KP Performance
76.886.3
68.0
86.892.9
79.385.8
65.6
89.294.4
77.885.5
65.9
90.5 94.5
0.010.020.030.040.050.060.070.080.090.0
100.0
Retention In Care
CD4 Measured
PCP Prophylaxis
On HIV Treatment
HIV RNA <75/mL
Metric
Perc
ent S
ucce
ss
2007
2008
2009
Many team efforts here also.
Outcomes are a team effort.

(Re-)New Interest in “Medical Home”
• Emphasis on integrated, multi-disciplinary care (MDCT) HIV Specialist (ID or primary care) as “specialty leader” Case manager and care management Can be physically in one place or connected by technology
Linkage to inpatient and outpatient care, lab, pharmacy services, consults
• Has been an element in HIV care Essentially, how KP practices HIV medicine Ryan White C clinics, VA also
• Not much research Some research but pre-combination ART (Le, 1998, Sherer, 2002)
HIV specialist improved outcomes (Kitahata 2000, Delgado 2003)
HIV clinical pharmacist (Horberg 2007)
Slide 7

Multidisciplinary Care Team Components (1)
Potential Components: NOTE: Need for local considerations always
• HIV Specialist Can be Infectious Disease Specialist Or Primary Care with extended experience with HIV Care
• Care Coordination Often an RN, but not necessarily Consider PA, clinical pharmacist, other
• HIV Clinical Pharmacist• Nurse Case Manager
Slide 8

Multidisciplinary Care Team Components (2)
• Social Work Benefits Coordination Access to outside services
?Housing ?Legal
• Health Educator• Nutrition Service• Transportation Specialist• Identified Specialists in other disciplines
Oncology Gastroenterology
• Mental HealthSlide 9

KP: Provider Experience and Outcomes
•IF antiretroviral naïve: ↑ panel size has modest
effect on adherence and odds BLQ at 12 month
Years of provider experience or specialty no association
Significant association with ARV class (NNRTI) and year started greatest impact
•IF antiretroviral experienced:
↑ years provider experience associated with ↑ adherence and odds BLQ
No association with panel size or specialty
Significant association with older age, Caucasian, MSM, initiation after 2000Horberg, Hurley, Towner, Allerton, Tang, Catz, Silverberg, Quesenberry, IDSA Abstract 1131, 2010; IAS Abstract MOPE464,
2011
Observational cohort data
Slide 10

Clinical Pharmacists: Roles
• Can have many roles Adherence and adverse effect counseling Manage adverse effects and drug-drug interactions Ombudsman with dispense pharmacies Research staff Potentially case management
• Physicians average 13 minutes entire course of a patient’s care discussing adherence while pharmacists spend 0.5-1.5 hours per visit discussing adherence
Older data, need to update And this was adherence to antiretroviral medications
only
Golin, JGIM, 2004; Geletko, Am J Hlth Sys Pharm, 2002;Rathbun, Clin Ther, 2005

HIV Clinical Pharmacists Study
ARV Naïve ARV Experienced
12 Month
--Continuous Outcome +6.5% (.06) [NOTE: Far greater impact on poorer subpopulation]
+3.1% (.34)
-- OR ≥90% 1.23 (.47) 1.02 (.92)
24 Month
--Continuous Outcomes +8.7% (.01) +3.0% (.40)/ +10.6% (.001)*
--OR ≥90% 3.88 (<.0001) 1.39 (.29)/ 2.49 (.002)*
*--1st value is 0-50 patients; 2nd value is 51+ patients
• 3538 patients evaluated—1571 antiretroviral naïve and 1967 experienced patients
Adherence Results (multivariate analysis, p value):
Horberg, Hurley, Silverberg, Quesenberry, Kinsman, JAIDS, 2007; 44:531-539

HIV Clinical Pharmacists Study (2)
ARV Naïve ARV Experienced
Hospital Days ↑67% (<.0001) [NOTE: Far greater impact on poorer subpopulation] / ↑10% (.36)*
↓14% (.008)/↓38% (<.0001)*
ER Visits ↓2% (.89) ↓18% (.05)
Office Visits ↓12% (<.0001) [NOTE: Far greater impact on poorer subpopulation] / ↓1% (.71)*
↓22% (<.0001) / ↑3% (.16)*
*--1st value is 0-50 patients; 2nd value is 51+ patients
Utilization Results:
Slide 13

HIV Multidisciplinary Care Team Study (1)
• Research Question: What components of the HIV MDCT in combination are
associated with the greatest increases in adherence?
• Retrospective analysis of HIV+ patients in KP California (11,411) initiating a new ART regimen from 1996-2006. ARV Naïve: 7,597 patients ARV Experienced: 3,814 patients
• Measured 12 month adherence to ART regimen using pharmacy dispense/refill records
Horberg, Hurley, Towner, Allerton, Tang, Catz, Silverberg, Quesenberry, Treatment Adherence Conference, 2011

HIV Multidisciplinary Care Team Study (2)
Primary Predictor—Exposure to MDCT component by medical center (26):•HIV Specialist (y/n)•Nurse Case Manager•Non-Nurse Care Coordinator•Clinical Pharmacist•Social Work/Benefits Counselor•Dietician•Mental Health
Other Predictor Variables•Age•Gender•Race/Ethnicity (White, Black, Latino, Other)•HIV Risk (MSM, IDU, Heterosexual)•HCV+•ART Regimen Class•ARV Experienced•Year this ART regimen was initiated (temporal trend)•Medical Center (cluster variable)•Provider (cluster variable)
Slide 15

HIV Multidisciplinary Care Team Study (3)
• Classification and regression tree approach (recursive partitioning) to ascertain potential MDCT compositions associated with maximal mean ART adherence (CART Pro 6.0®, Salford Systems, San Diego, CA)
• From above, potential combinations tested in adjusted* mixed linear regression to determine which associated with maximal ART adherence
*--Clustering by medical center, provider, patient. Adjusted for ART experience, age, gender, race/ethnicity, HIV risk, HCV+, ART regimen class, temporal trend

HIV MDCT Study (4): Recursive Partitioning
* p < 0.05
Multiple team combinations possible with significant effect.
First branch is clinicalpharmacist.

HIV MDCT Study (5): Teams Determined from RPMDCT below not significantly different between them
Team Composition
Mean Adjusted Percent Increase
Adherence 95% Confidence Interval p Value
Specialist Only 74.4% 72.2-76.8%
Clinical Pharmacist Only +3.3% +0.1 to +5.8% 0.01
Pharmacist + non-RN care coordinator +8.1% +2.7 to +13.4% 0.003
Nurse + Social Work/Benefits +7.5% +5.4 to+9.7% <0.001
HIV Specialist + Mental Health +6.5% +2.6 to +10.4% 0.001
Pharmacist + Social Work/Benefits +5.7% +4.0 to +7.4% <0.001
Slide 18

CC = (0)
TerminalNode 1
Class = 0Class Cases %
0 1740 57.31 1295 42.7W = 3035.00
N = 3035
CC = (1)
TerminalNode 2
Class = 1Class Cases %
0 84 36.51 146 63.5
W = 230.00N = 230
RNCCCM = (0)
Node 3Class = 0
CC = (0)Class Cases %
0 1824 55.91 1441 44.1W = 3265.00
N = 3265
SWBC = (0)
TerminalNode 3
Class = 0Class Cases %
0 219 56.21 171 43.8
W = 390.00N = 390
SWBC = (1)
TerminalNode 4
Class = 1Class Cases %
0 648 46.31 752 53.7W = 1400.00
N = 1400
RNCCCM = (1)
Node 4Class = 1
SWBC = (0)Class Cases %
0 867 48.41 923 51.6W = 1790.00
N = 1790
RX = (0)
Node 2Class = 0
RNCCCM = (0)Class Cases %
0 2691 53.21 2364 46.8W = 5055.00
N = 5055
SWBC = (1)
TerminalNode 5
Class = 0Class Cases %
0 1148 51.41 1084 48.6W = 2232.00
N = 2232
SWBC = (0)
TerminalNode 6
Class = 1Class Cases %
0 299 41.61 420 58.4
W = 719.00N = 719
MH = (0)
Node 7Class = 0
SWBC = (1)Class Cases %
0 1447 49.01 1504 51.0W = 2951.00
N = 2951
MH = (1)
TerminalNode 7
Class = 1Class Cases %
0 426 40.61 624 59.4W = 1050.00
N = 1050
CC = (0)
Node 6Class = 1
MH = (0)Class Cases %
0 1873 46.81 2128 53.2W = 4001.00
N = 4001
CC = (1)
TerminalNode 8
Class = 1Class Cases %
0 972 41.31 1383 58.7W = 2355.00
N = 2355
RX = (1)
Node 5Class = 1
CC = (0)Class Cases %
0 2845 44.81 3511 55.2W = 6356.00
N = 6356
Node 1Class = 0
RX = (0)Class Cases %
0 5536 48.51 5875 51.5W = 11411.00
N = 11411
CC onlyp<0.05
RX=clinical pharmacist
RNCCCM=nurse case manager
CC=non-RN case coordinator
SWBC=social work/benefits counselor
MH=mental health worker
Reference group is HIV specialist only
Ref.RNCCM only RNCCM
+ SWBC
RX + SWBCRX onlyp<0.05
RX + MH
RX + CC
This Can Be Applied to Other Outcomes– Odds Maximal Viral Control
Horberg, Hurley, Towner, Allerton, Tang, Catz, Silverberg, Quesenberry, IAS Abstract MOPE422, 2011

CC = (0)
TerminalNode 1
Class = 0Class Cases %
0 1740 57.31 1295 42.7W = 3035.00
N = 3035
CC = (1)
TerminalNode 2
Class = 1Class Cases %
0 84 36.51 146 63.5
W = 230.00N = 230
RNCCCM = (0)
Node 3Class = 0
CC = (0)Class Cases %
0 1824 55.91 1441 44.1W = 3265.00
N = 3265
SWBC = (0)
TerminalNode 3
Class = 0Class Cases %
0 219 56.21 171 43.8
W = 390.00N = 390
SWBC = (1)
TerminalNode 4
Class = 1Class Cases %
0 648 46.31 752 53.7W = 1400.00
N = 1400
RNCCCM = (1)
Node 4Class = 1
SWBC = (0)Class Cases %
0 867 48.41 923 51.6W = 1790.00
N = 1790
RX = (0)
Node 2Class = 0
RNCCCM = (0)Class Cases %
0 2691 53.21 2364 46.8W = 5055.00
N = 5055
SWBC = (1)
TerminalNode 5
Class = 0Class Cases %
0 1148 51.41 1084 48.6W = 2232.00
N = 2232
SWBC = (0)
TerminalNode 6
Class = 1Class Cases %
0 299 41.61 420 58.4
W = 719.00N = 719
MH = (0)
Node 7Class = 0
SWBC = (1)Class Cases %
0 1447 49.01 1504 51.0W = 2951.00
N = 2951
MH = (1)
TerminalNode 7
Class = 1Class Cases %
0 426 40.61 624 59.4W = 1050.00
N = 1050
CC = (0)
Node 6Class = 1
MH = (0)Class Cases %
0 1873 46.81 2128 53.2W = 4001.00
N = 4001
CC = (1)
TerminalNode 8
Class = 1Class Cases %
0 972 41.31 1383 58.7W = 2355.00
N = 2355
RX = (1)
Node 5Class = 1
CC = (0)Class Cases %
0 2845 44.81 3511 55.2W = 6356.00
N = 6356
Node 1Class = 0
RX = (0)Class Cases %
0 5536 48.51 5875 51.5W = 11411.00
N = 11411
CC onlyp<0.05
RX=clinical pharmacist
RNCCCM=nurse case manager
CC=non-RN case coordinator
SWBC=social work/benefits counselor
MH=mental health worker
Reference group is HIV specialist only
Ref.RNCCM only RNCCM
+ SWBC
RX + SWBCRX onlyp<0.05
RX + MH
RX + CC
This Can Be Applied to Other Outcomes– Odds Maximal Viral Control
First branch is clinical pharmacist.
Different results when stratified by ARV status.
Discussion of MDCT Study Results
• First study to consider all elements of HIV MDCT interactively
• Clinical pharmacist is significantly associated with adherence improvement Confirms prior study
• Multiple combinations (5) are associated with significantly improved adherence Compared to HIV specialist only
• Likely some confounding by indication
Slide 21

Next Research Questions/Steps
• Test MDCT optimized teams in prospective study Also in different healthcare systems
• Do these teams also improve other outcomes? Accessing Care Retention in Care Mortality
• Who are the key personnel for linkage to care? Especially in non-integrated care systems
• What services are not addressed by these teams?
Slide 22

Thank you!
The great work continues.(Paraphrased from Angels in America)
Related Documents











