1 Copyright © CAMH 2011 Copyright © CAMH 2011 OPIOID BASICS For RNAO October 24, 2013 Lori Naylor, RSW Developed in collaboration with the Centre for Addiction and Mental Health, Timiskaming Addictions and Mental Health, Sandy Hill Community Health Centre Oasis Program Copyright © CAMH 2011 Copyright © CAMH 2011 Learning Objectives Increase knowledge and understanding about: • What opioids are • Problematic use • Who is using opioids • Risk and protective factors • Health promotion • Opioids and pregnancy • Treatment approaches • Overdose prevention • Supporting Full Recovery • Opiate Substitution Therapies 2 Copyright © CAMH 2011 Copyright © CAMH 2011 3 What are Opioids? ?

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Copyright © CAMH 2011Copyright © CAMH 2011
OPIOID BASICSFor RNAO
October 24, 2013Lori Naylor, RSW
Developed in collaboration with the Centre for Addiction and Mental Health,
Timiskaming Addictions and Mental Health, Sandy Hill Community Health Centre Oasis Program
Copyright © CAMH 2011Copyright © CAMH 2011
Learning Objectives
Increase knowledge and understanding about:• What opioids are
• Problematic use
• Who is using opioids
• Risk and protective factors
• Health promotion
• Opioids and pregnancy
• Treatment approaches
• Overdose prevention
• Supporting Full Recovery
• Opiate Substitution Therapies2
Copyright © CAMH 2011Copyright © CAMH 2011
3
What are Opioids?
?
2
Copyright © CAMH 2011Copyright © CAMH 2011
Opioids:
• Are psychoactive chemicals that work by binding to our natural opioid receptors.
• Are types of painkillers, or analgesics, that are sometimes called “narcotic pain relievers.”
• Have positive effects associated with their analgesic qualities.
• Have risks associated with misuse and with the drug’s depressant qualities.
4
“Opiate” is a synonym for “opioid.” True / False
Copyright © CAMH 2011Copyright © CAMH 2011
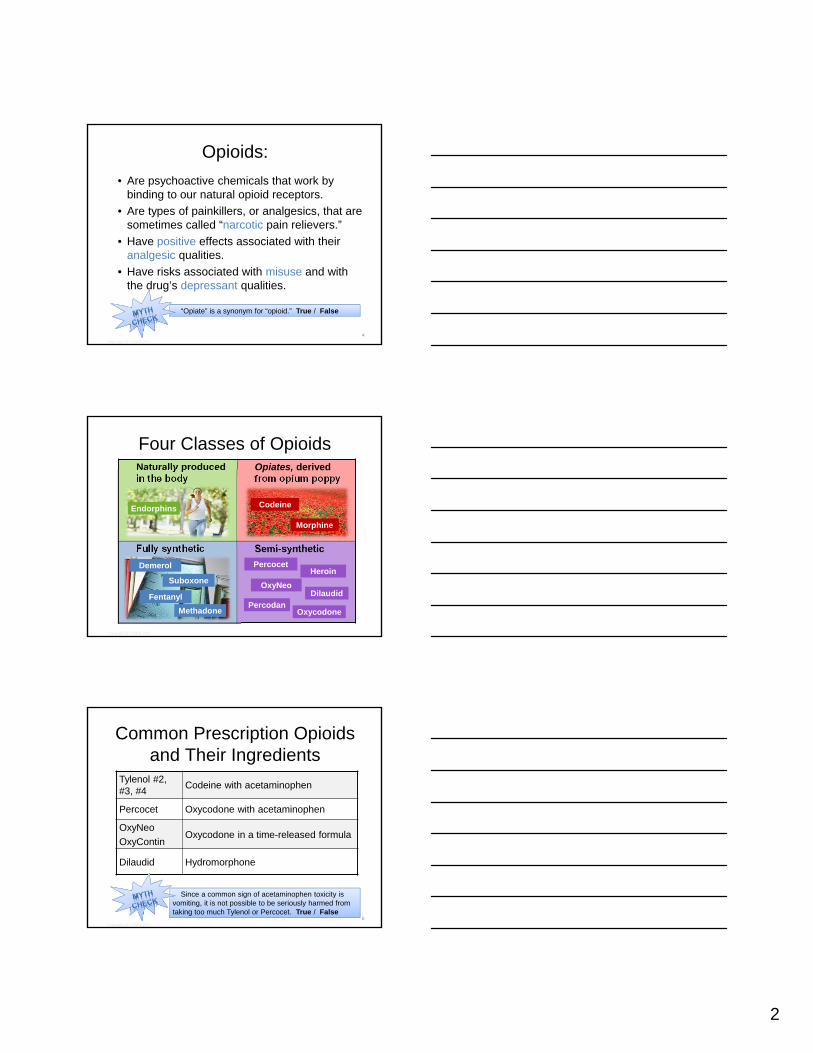
Four Classes of Opioids Naturally produced in the body
Opiates, derived from opium poppy
Fully synthetic Semi-synthetic
HeroinPercocet
Oxycodone
DilaudidOxyNeo
PercodanFentanyl
Suboxone
Methadone
Demerol
Endorphins
Morphine
Codeine
Copyright © CAMH 2011Copyright © CAMH 2011
Common Prescription Opioids and Their Ingredients
6
Tylenol #2, #3, #4
Codeine with acetaminophen
Percocet Oxycodone with acetaminophen
OxyNeo
OxyContinOxycodone in a time-released formula
Dilaudid Hydromorphone
Since a common sign of acetaminophen toxicity is vomiting, it is not possible to be seriously harmed from taking too much Tylenol or Percocet. True / False

3
Copyright © CAMH 2011Copyright © CAMH 2011
Other Prescription Opioids and Their Ingredients
MS Contin, M-Eslon Morphine
Duragesic patch Fentanyl
Talwin Pentazocine
Demerol Meperidine
7
Copyright © CAMH 2011Copyright © CAMH 2011
Intended Use of Opioids:
1) Physical pain management
2) Treatment of addiction to other opioids
8
Copyright © CAMH 2011Copyright © CAMH 2011
9
Understanding Pain: What to do about it in less than five minutes? (5 min) http://www.youtube.com/watch?v=4b8oB757DKc
More resources about pain:
Non-pharmacologic Therapy and Chronic Pain (54 min)https://camh.adobeconnect.com/_a829238269/p41da49y1da/?launcher=false&fcsContent=true&pbMode=normal
Chronic Pain and Treatment (51 min) https://camh.adobeconnect.com/_a829238269/p2z32qxd7w7/?launcher=false&fcsContent=true&pbMode=normal
4
Copyright © CAMH 2011Copyright © CAMH 2011
10
Problematic Use
Photo credit: http://www.flickr.com/photos/robbrucker/
Copyright © CAMH 2011Copyright © CAMH 2011
“There is a relationship between the amount of opioid medicine prescribed in Canada and the increasing level of opioid abuse and opioid-related deaths among youth in Ontario.”
(Dhalla, Mamdani, Sivilotte, Kopp, Qureshi & Juurlink, 2009)
11
Copyright © CAMH 2011Copyright © CAMH 2011
What are the risks of opioid use/abuse?
12
• Dependence
• Addiction
• Overdose
• Withdrawal
• Health risks
• Diversion
Most people who use opioids go on to develop dependence or addiction. True / False
5
Copyright © CAMH 2011Copyright © CAMH 2011
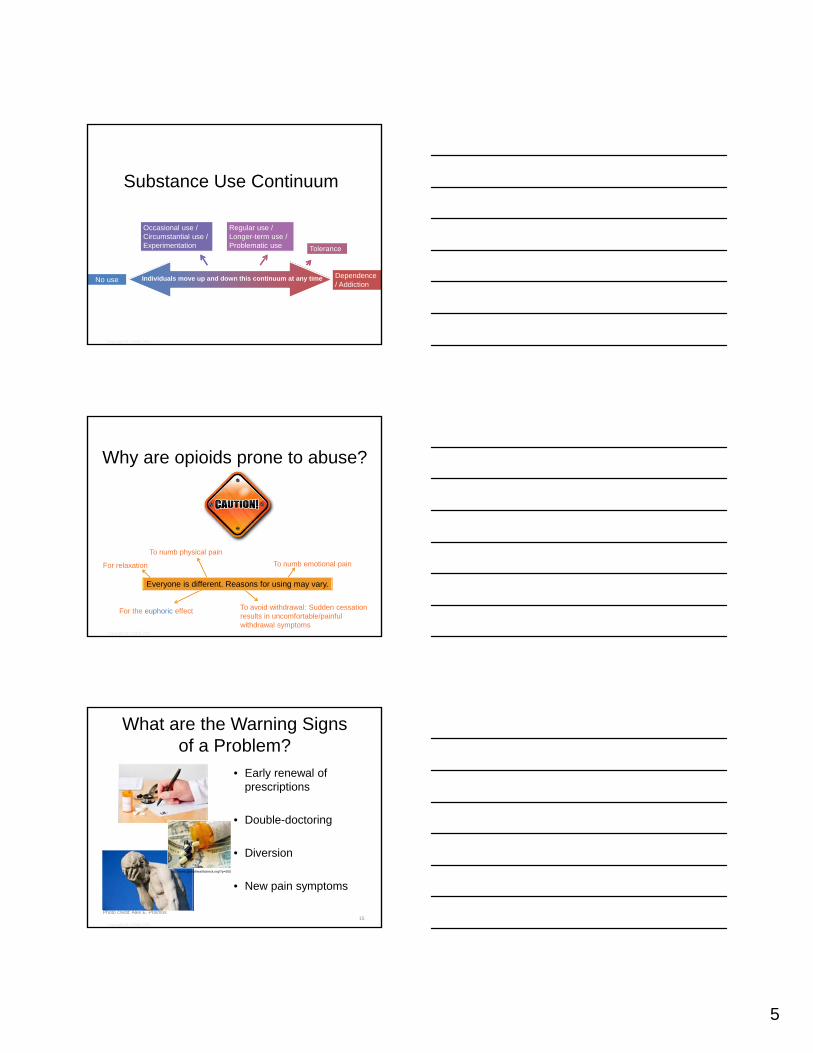
Substance Use Continuum
Individuals move up and down this continuum at any timeNo use Dependence / Addiction
Occasional use / Circumstantial use /Experimentation
Regular use / Longer-term use / Problematic use Tolerance
Copyright © CAMH 2011Copyright © CAMH 2011
Why are opioids prone to abuse?
To numb physical pain
To numb emotional pain
For the euphoric effect
For relaxation
To avoid withdrawal: Sudden cessation results in uncomfortable/painful withdrawal symptoms
Everyone is different. Reasons for using may vary.
Copyright © CAMH 2011Copyright © CAMH 2011
15
What are the Warning Signs of a Problem?
• Early renewal of prescriptions
• Double-doctoring
• Diversion
• New pain symptoms
Photo credit: Alex E. Proimos
http://www.globalhealthcheck.org/?p=505

6
Copyright © CAMH 2011Copyright © CAMH 2011
Diarrhea
InsomniaExhaustion
Chills, shivering, clammy skin Muscle cramps and spasms /Body aches / Bone aches
Sweating
Anxiety / restlessness / agitationDepression / hopelessness
What are the Withdrawal Effects?
• They are uncomfortable but not life threatening.
• They usually subside after a week.
• They often drive people to use again.
• They can occur even after first use.
16
Copyright © CAMH 2011Copyright © CAMH 2011
What is Tolerance?
• It’s the need for higher doses for the same effect.
• Tolerance increases the risk of physical and psychological dependence.
Note: Since tolerance for euphoria increases more rapidly than respiratory depression, individuals may continue to seek the euphoria of the drug while ignoring overdose cues (i.e. slowed breathing). This puts them at risk of overdose.
Copyright © CAMH 2011Copyright © CAMH 2011
What does Addiction Impact?
Leisure
Emotional health
Physical health
Family relationships
Social relationships
Legal status
Education
Employment
Finances
Determining whether drug use is a problem isn’t always about how often or how much it is used but more about how it is negatively impacting various life areas.
7
Copyright © CAMH 2011Copyright © CAMH 2011
Who Is Using Opioids?
19
Copyright © CAMH 2011Copyright © CAMH 2011
20
“Ontario is in the midst of a public health crisis—a crisis stemming from the inappropriate prescribing, dispensing and illicit use of opioids and other narcotics."
- Dr. Jack Mandel, PresidentCollege of Physicians and Surgeons of Ontario(September 2010)
Copyright © CAMH 2011Copyright © CAMH 2011
Opioid Use in Ontario
Between 1991 and 2009, the number of prescriptions in Ontario for oxycodone drugs rose by 850%.*
Between 1991 and 2004, deaths in Ontario from opioid use doubled from 13.7 deaths per million residents to 27.2 deaths per million.*
In 2009–2010, MOHLTC spent $156 million on narcotics for Ontario Drug Benefit Program recipients, $54 million on OxyContin alone.**
21
$*(Dhalla, I., et al, 2009)**CBC investigative report (CBC Radio 1, 1730 hour News, June 2, 2009)
8
Copyright © CAMH 2011Copyright © CAMH 2011
Opioid Use in Ontario
Between 2000 and 2004, controlled‐release oxycodone increased from 3.8% to 55.4% of the total opioid admissions.
Long‐acting oxycodone was associated with a five‐fold increase in oxycodone‐related mortality.
22
Note: Since March 2012, OxyContin began being removed from the market in Ontario and has been delisted from the Ontario Drug Benefit Program.
Copyright © CAMH 2011Copyright © CAMH 2011
Prescription Opioid Misuse
Prescriptions opioid misuse has been Ontario’s fastest‐growing problem substance, and the third top presenting problem substance for new admissions (DATIS, 2012).
Due to discontinuing OxyContin in 2012, DATIS expects to be observing a different trend.
Image: http://www.datis.ca/newsarchive.php#27
Copyright © CAMH 2011Copyright © CAMH 2011
Entering Treatment
24
9
Copyright © CAMH 2011Copyright © CAMH 2011
Opioid misuse among general population in Ontario
(Lalomiteanu et al,2012)
Mouse-over this text for analysis
Copyright © CAMH 2011Copyright © CAMH 2011
Reported Use among Youth (Ages 19-24)
Therefore, when assessing and treating, it is important to speak to females about the nature of their drug use.
Copyright © CAMH 2011Copyright © CAMH 2011
Ontario Student Drug Use and Health Survey
Past Year Use 2011
Alcohol 55%
Cannabis 22%
Opioid pain relievers (NM) 14%
Cigarettes 9%
Stimulants (NM) 4%
Sedatives (NM) 2%
www.camh.net
NM = non-medical

10
Copyright © CAMH 2011Copyright © CAMH 2011
Ontario Student Drug Use and Health Survey 2011
• Approximately 14% of Ontario students in Grades 7–12 report using prescription opioid pain relievers such as Tylenol #3 and Percocet for non-medical purposes
• Almost 67% report obtaining the drugs from home
28
Copyright © CAMH 2011Copyright © CAMH 2011
Resources For Parents
Key messages on
how to prevent problems:1) Build healthy relationships
2) Clear rules – never take someone’s else’s medicine
3) Store opioids in safe secure place and keep track of pills
4) Clean out medicine cabinet at least once a year
5) Get help early – call Drug and Alcohol Helpline 1.800.565.8603
Youth and prescription painkillers: What parents need to knowhttp://knowledgex.camh.net/amhspecialists/resources_families/Documents/YouthandMisuse%20E.pdf
Copyright © CAMH 2011Copyright © CAMH 2011
About Percs, Oxys and other Pain Pillshttp://knowledgex.camh.net/amhspecialists/resources_families/Documents/about_percs_oxys.pdf
11
Copyright © CAMH 2011Copyright © CAMH 2011
Risk and ProtectiveFactors*
*Remember, these don’t have a simple cause-and-effect relationship.
Copyright © CAMH 2011Copyright © CAMH 2011
Risk Factors
• Life events / environmental stressors
• Psychological vulnerabilities (personality traits)
• Other illness and medications
Note: If we are aware of risk factors we can target prevention and education specifically to these areas.
Copyright © CAMH 2011Copyright © CAMH 2011
Protective Factors
• Personal and social competence
• Feeling in control of one’s life
• Optimism
• Ability to detach from conflict
• Willingness to seek support
12
Copyright © CAMH 2011Copyright © CAMH 2011
Populations at greater risk
• Adolescents
• Older adults
• People with a family history or personal history of substance use issues
• People with a personal history of mood or anxiety disorders
(Kahan et al, 2011)
Copyright © CAMH 2011Copyright © CAMH 2011
Concurrent Disorders
From Ontario data, non‐medical prescription opioid use has been reported to be significantly higher among those reporting elevated psychological distress (Shield et al., 2011)
Mental health problems
Substance use problems
(Shield et al., 2011)
Copyright © CAMH 2011Copyright © CAMH 2011
Health Promotion
Aimed at empowering individuals
to improve their health

13
Copyright © CAMH 2011Copyright © CAMH 2011
Health Promotion Strategies
Strengthening community
actions
Developing personal skills
Reorienting health services
Creating supportive
environments
Building healthy public policy
Copyright © CAMH 2011Copyright © CAMH 2011
Social Determinants of Health
38(Dahlgren & Whitehead, 1991)
Copyright © CAMH 2011Copyright © CAMH 2011
What Works?• Building resiliency and protective factors
• Balancing health and safety
• Setting goals based on evidence / best practices
• Using a comprehensive approach (a range of strategies)
• Supporting collaborations (sectors, governments, NGOs)
• Addressing the determinants of health
• Using a population health approach
Opioid Basics: Health Promotion, Prevention and Harm Reduction Approacheshttp://camh.adobeconnect.com/p9j5z4mefu5/
14
Copyright © CAMH 2011Copyright © CAMH 2011
Opioids and Pregnancy
Note: Opioids cross the placenta.
Copyright © CAMH 2011Copyright © CAMH 2011
Risks of Withdrawal
Risks to fetuses and infants:• Withdrawal has the same physical
effects on the fetus as it does on the woman.
• Neonatal Abstinence Syndrome (NAS) – occurring in some infants born to mothers who are dependent on opioids
Risks to the mother:• Withdrawal is also associated with
placental abruption and could be life-threatening for the mother.
Opioids in Pregnancy
If tapering has to be done:
• The safest time is between 14 and 32 weeks*
• The dose should be tapered at a rate of:
• No more than 10% reduction per day*
• No more than 5-10 mg per week as an outpatient, or
• No more than 1-2 mg per day as an inpatient
• Switch to an immediate release preparation at the end of the taper to allow for finer titration*
Prenatal
Monitor closely and stop tapering if any adverse consequences are reported!

15
Copyright © CAMH 2011Copyright © CAMH 2011
During Pregnancy
Minimize withdrawal
Prevent relapses
Use maintenance medications
Copyright © CAMH 2011Copyright © CAMH 2011
Safety Considerations
Provide prenatal care and psychosocial treatment
Monitor for partner’s use of drugs and/or violence in the relationship
Consider taking action if the child is at risk under the Child and Family Services Act
Poly-drug use and tobacco (high risk for SIDS)
Copyright © CAMH 2011Copyright © CAMH 2011
45
For more information and resources on opioids and pregnancy, visit: https://knowledgex.camh.net/opioid_alert/2012/Pages/pregnancy_pro_april32012.aspx
Management of Perinatal Opioid Addictionhttp://camh.adobeconnect.com/p3uznlolk6k/
Resources on Treating Pregnant Clients with Opiate
Addictions
16
Copyright © CAMH 2011Copyright © CAMH 2011
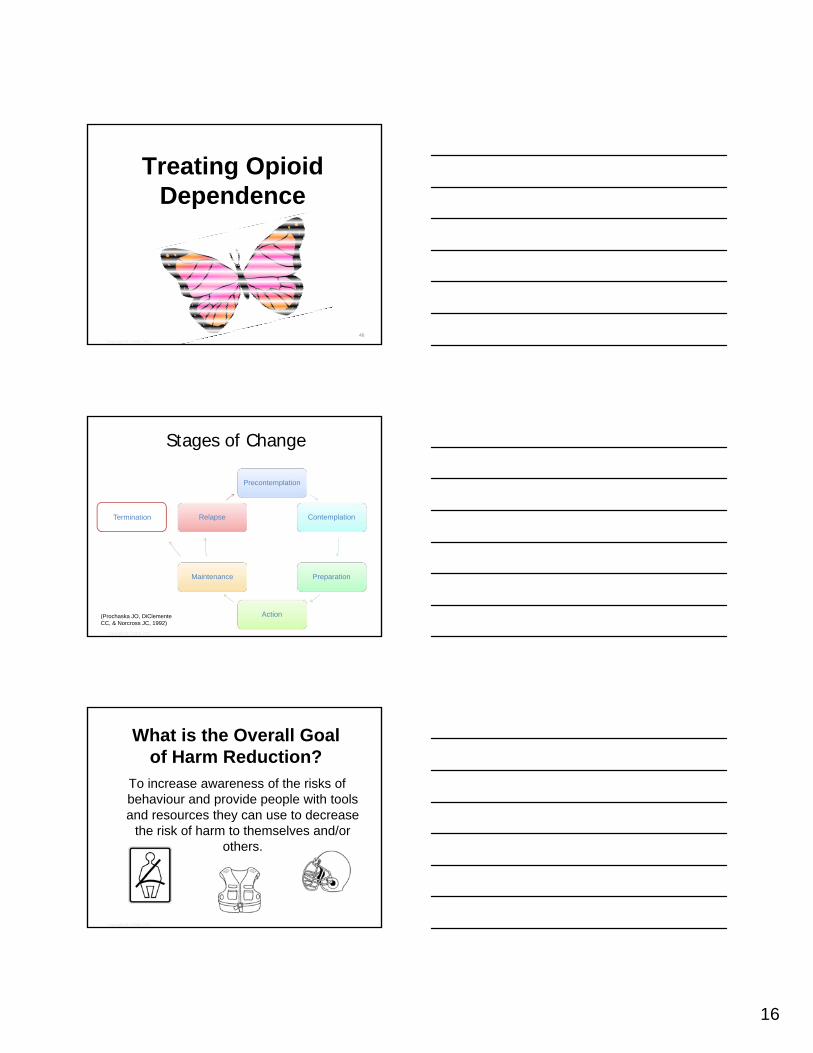
Treating Opioid Dependence
46
Copyright © CAMH 2011Copyright © CAMH 2011
(Prochaska JO, DiClemente CC, & Norcross JC, 1992)
Stages of Change
Precontemplation
Contemplation
Preparation
Action
Maintenance
RelapseTermination
Copyright © CAMH 2011Copyright © CAMH 2011
What is the Overall Goal of Harm Reduction?
To increase awareness of the risks of behaviour and provide people with tools and resources they can use to decrease
the risk of harm to themselves and/or others.
17
Copyright © CAMH 2011Copyright © CAMH 2011
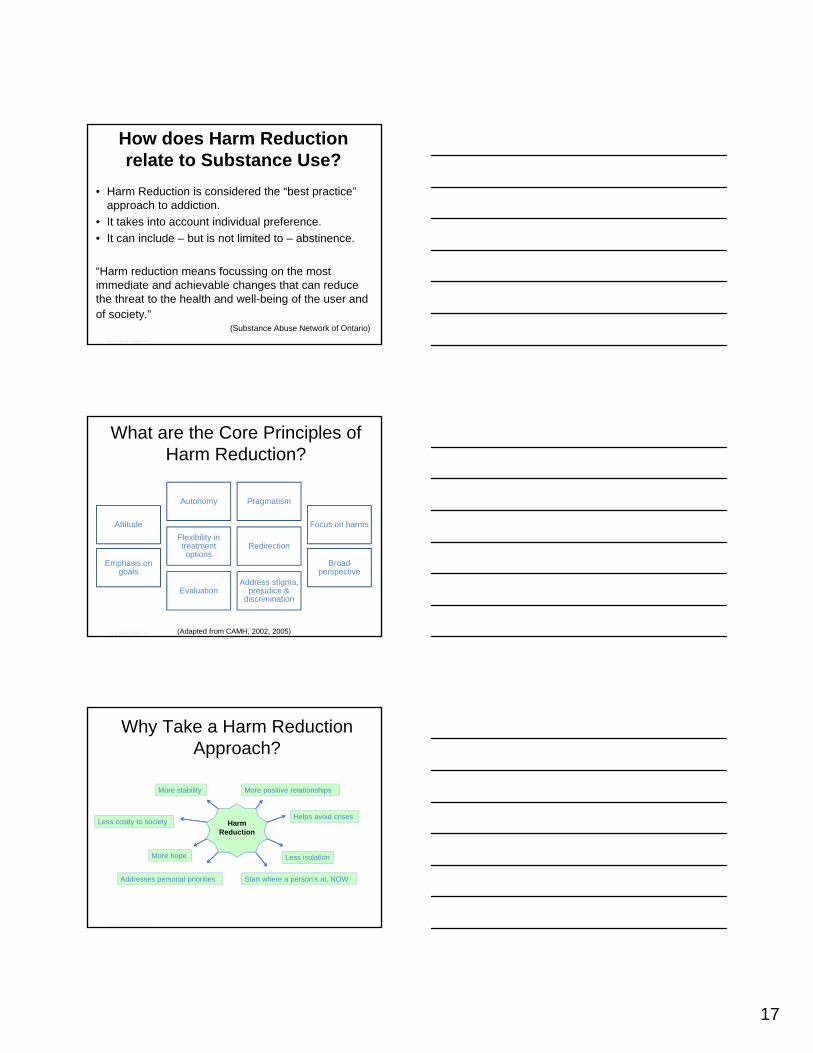
How does Harm Reduction relate to Substance Use?
• Harm Reduction is considered the “best practice” approach to addiction.
• It takes into account individual preference.
• It can include – but is not limited to – abstinence.
“Harm reduction means focussing on the most immediate and achievable changes that can reduce the threat to the health and well-being of the user and of society.”
(Substance Abuse Network of Ontario)
Copyright © CAMH 2011Copyright © CAMH 2011
What are the Core Principles of Harm Reduction?
Attitude
Autonomy Pragmatism
Focus on harms
Emphasis on goals
Flexibility in treatment options
Redirection
Broad perspective
Evaluation Address stigma,
prejudice & discrimination
(Adapted from CAMH, 2002, 2005)
Copyright © CAMH 2011Copyright © CAMH 2011
Why Take a Harm Reduction Approach?
Harm Reduction
Harm Reduction
More positive relationshipsMore positive relationships
Less isolationLess isolation
Addresses personal prioritiesAddresses personal priorities
More stabilityMore stability
More hopeMore hope
Helps avoid crisesHelps avoid crisesLess costly to societyLess costly to society
Start where a person’s at, NOWStart where a person’s at, NOW
18
Copyright © CAMH 2011Copyright © CAMH 2011
Overdose Prevention / What is Naloxone?
• It can prevent death in the case of an opioid overdose.
• It acts as an opioid inverse agonist.
• It is commonly administered/self-administered intravenously.
Note: While Naloxone was included in overdose prevention kits distributed to agencies in Ontario in 2012-13 by the Ontario Harm Reduction Distribution Program (OHRDP), the MOHLTC is now looking into alternative Naloxone delivery models for Ontario due to regulatory issues.
Photo credit: Toronto Public Health
Copyright © CAMH 2011Copyright © CAMH 2011
What are Some Treatment Approaches?
• Controlled use
• Tapering
• Withdrawal management (residential or community)
• Opiate Substitution therapies (ie. Methadone and Suboxone)
• Alternative Therapies
53
Supporting Opioid Addiction Through Adjunct Therapieshttp://camh.adobeconnect.com/p1920sa9u9f/
Copyright © CAMH 2011Copyright © CAMH 2011
Controlled Use
• Taking drugs “as prescribed”
• Involves some tapering
• Makes use of alternative pain management strategies, such as
– Acupuncture, TENS
– hot/cold compresses
– physical activity
– relaxation
– distraction
54
19
Copyright © CAMH 2011Copyright © CAMH 2011
Supported Tapering/Withdrawal
• Slowly decreasing opioid use with the intent to quit
• The ideal approach includes planning with the client, the service provider/physician, and a support person
• The client is monitored closely throughout the tapering process and meets frequently with the service provider
55
Copyright © CAMH 2011Copyright © CAMH 2011
Preparing for Withdrawal
56
Supports
Consider the “whole person”when putting supports in place
(E.g. Does the person need mental health supports,
spiritual supports, physical supports?)
Explore self-help options, peer support and family/friend
support
Education
Ensure the client knows that there’s a high risk of overdose if the person relapses to the original dose (due to there being a loss of tolerance
following withdrawal).
Educate client about the withdrawal process, and prepare an “at home kit” of what might be
helpful for them.
Develop a solid practical plan based on resources available to the person, including:
Copyright © CAMH 2011Copyright © CAMH 2011
Other Strategies for Successful Withdrawal
• Prepare a safe and comfortable environment
• Ensure access to a support person
• Get lots of rest
• Decrease noise levels
• Cool clothing
• Warm compresses
• Baths
• Stay hydrated by drinking water
• Consult with a physician about medications that can support withdrawal symptoms
57
20
Copyright © CAMH 2011Copyright © CAMH 2011
Supporting Full Recovery
Full recovery requires a continuum of care including:
•Initial contact
•Stabilization
•Withdrawal Management
•Treatment (in or out-patient)
•After care
•Relapse prevention
•Education and on-going support
•Alternatives for pain management if necessary
•Adjunct Therapy support
58
Copyright © CAMH 2011Copyright © CAMH 2011
3 Common Substitution Treatment Options
1. Methadone
2. Buprenorphine
3. Suboxone
Copyright © CAMH 2011Copyright © CAMH 2011
What is METHADONE?
60
21
Copyright © CAMH 2011Copyright © CAMH 2011
Methadone
• A long-acting oral opiate analgesic
• Given in the appropriate dose to opioid-dependent patients
– Dose is usually once daily
– Suppresses symptoms of opioid withdrawal for 24-36 hours
– Reduces cravings
– Does not induce sedation, intoxication or euphoria at the correct dose
– Reduces pain for short periods of time
– Cross-tolerance to other opiates61
Copyright © CAMH 2011Copyright © CAMH 2011
Components of a Successful MMT Program
• MMT = Methadone Maintenance Treatment
• Counselling which involves education and support for both the client and his/her family
• Urine drug screens
• Integrated medical, counselling and administrative services
• Availability of a variety of psychosocial services if required
• Highly trained staff and involvement of support people
• Long term involvement from clients(Methadone Research Drug Guide, 2006) 62
Copyright © CAMH 2011Copyright © CAMH 2011
Benefits of MMT
• Decreased illicit drug use
• Decreased criminal activity
• Improved employment rates
• Improved psychological status
• Decreased mortality (11x less)
• Suppression of withdrawal symptoms
• Reduced craving for opiates
• Does not induce sedation or euphoria
63
22
Copyright © CAMH 2011Copyright © CAMH 2011
Who is Methadone helpful for?
• Those who have tried other treatment options who may be more motivated to try MMT because of past failings
• Those with persistent pain who are able to commit to the treatment regime *
• Individuals with a safe stable living environment
• Individuals who able to get to the clinic or pharmacy without difficulty
• Individuals who are motivated to commit to a long term program **
• Individuals who have support from a family member or case manager
64
Copyright © CAMH 2011Copyright © CAMH 2011
Methadone Dispensing
• Daily oral dose is administered at a pharmacy
• Administration is supervised by a nurse or a pharmacist
• Policies and professional/client contracts are in place to ensure safety and adherence to program
65
Copyright © CAMH 2011Copyright © CAMH 2011
What is a “Carry” and what are the general guidelines?
• A ‘carry’ is a take-home dose of methadone
• Not recommended in first 2 months of treatment
• Client will receive 1 extra carry/week for each month of the program if there are no issues
• Maximum 6 carries/week
(Methadone Maintenance Treatment Program Standards and Guidelines, 2011)
66
23
Copyright © CAMH 2011Copyright © CAMH 2011
How does MMT help improve lives?
• More effective in retaining client in treatment
• More effective in the suppression of opioid use
• Reduced drug-related criminal behaviours
• Reduced mortality rates among individuals receiving treatment
• Improved physical and mental health
• Reduced risk behaviours for HIV, HCV, and STI’s
• Improved pregnancy outcomes
• Improved social functioning and quality of life
(Health Canada, 2013, Mattick et. Al., 2003)
67
Copyright © CAMH 2011Copyright © CAMH 2011
68
Methadone Summary
Methadone is effective
It is a long-acting opioid agonist that is administered daily
Treatment is very specific to the individual
There is a high risk of relapse if treatment is discontinued, and withdrawal symptoms can be severe
The induction period is a particularly dangerous time
With long term supports in place, treatment outcomes are very good
Some individuals will use methadone for the rest of their lives
Copyright © CAMH 2011Copyright © CAMH 2011
What is BUPRENORPHINE?
69
24
Copyright © CAMH 2011Copyright © CAMH 2011
Buprenorphine
• Buprenorphine is a partial agonist
• Alternative to Methadone
• Blocks effects of opioids to help reduce cravings
• Suppresses withdrawal symptoms for a duration of approximately 6-12 hours with relief in about 15 minutes
• Lower potential for abuse/overdose risk
70
Copyright © CAMH 2011Copyright © CAMH 2011
What is SUBOXONE?
71
Copyright © CAMH 2011Copyright © CAMH 2011
Suboxone
• Suboxone is a partial opioid agonist• Contains naloxone to deter injection• Theoretically, less severe withdrawal than
methadone• Clients often state that suboxone feels less
emotionally addictive than methadone• There is a ceiling on Suboxone activity making it
safer• Not suitable for those who need a high dose to
avoid withdrawal

25
Copyright © CAMH 2011Copyright © CAMH 2011
Resources mentioned in this tutorial:
Brochures
About Percs, Oxys and other Pain Pills: http://knowledgex.camh.net/amhspecialists/resources_families/Documents/about_percs_oxys.pdf
Youth and prescription painkillers: What parents need to know: http://knowledgex.camh.net/amhspecialists/resources_families/Documents/YouthandMisuse%20E.pdf
Videos
Prescription for Addiction: https://knowledgex.camh.net/videos/Pages/prescription_addiction.aspx
Understanding Pain: What to do about it in less than five minutes? http://www.youtube.com/watch?v=4b8oB757DKc
Webinars
Management of Perinatal Addiction: http://camh.adobeconnect.com/p3uznlolk6k
Supporting Opioid Recovery with Adjunct Therapies: http://camh.adobeconnect.com/p1920sa9u9f/Chronic Pain and Treatment:
https://camh.adobeconnect.com/_a829238269/p2z32qxd7w7/?launcher=false&fcsContent=true&pbMode=normal
Management of Perinatal Opioid Addiction: http://camh.adobeconnect.com/p3uznlolk6k/
Copyright © CAMH 2011Copyright © CAMH 2011
References
74
CAMH. CAMH and Harm Reduction. 2002. Available at: http://knowledgex.camh.net/amhspecialists/resources_families/Pages/harm_reduction.aspx
CAMH. Fundamentals of Addiction On-line course, Characteristics of Harm Reduction. 2005. Available at: http://www.camh.net/education/online_courses_webinars/mha101/introtoaddiction/Introduction_to_Addiction.htm
Canadian Guideline for Safe and Effective Use of Opioids for chronic non-cancerous pain: http://nationalpaincentre.mcmaster.ca/opioid
College of Physicians and Surgeons of Ontario. Avoiding Abuse, Achieving a Balance: Tackling the Opioid Public Health Crisis. 2010. Available at: http://www.cpso.on.ca/uploadedFiles/policies/positions/Opioid%20report%20final.pdf
Dhalla IA, Mamdani MM, Sivilotte ML, Kopp A, Qureshi O, Juurlink DN. Prescribing of opioid analgesics and related mortality before and after the introduction of long-acting oxycodone. CMJ 2009; 181:891-6.
Drug and Alcohol Treatment Information System (DATIS) – CAMH. Substance Abuse Statistical Tables - Fiscal Year 2007/2008 To Fiscal Year 2011/2012. 2012. Available at: http://www.datis.ca/pub/reports/DATIS%20Substance%20Abuse%20Statistical%20Tables%20FY200708%20to%20FY201112.pdf
Copyright © CAMH 2011Copyright © CAMH 2011
75
ReferencesFischer G, et al. (2000). Treatment of opioid-dependent pregnant women with buprenorphine. Addiction. 95(2): 239-244
Fishbain, D.A., Cole B, Lewis J., Rosomoff HL., Rosomoff RS What percentage of chronic nonmalignant pain patients exposed to chronic opioid analgesic therapy develop abuse/addiction and/or aberrant drug-related behaviors? A structured evidence-based review Pain Med2008 May-Jun;9(4):444-59.
Harrison, Susan, Carver, Virginia Eds.(2004) Alcohol and Drug Problems: A Practical Guide for Counsellors 3rd Edition. Toronto: Centre for Addiction and Mental Health 2004
Health Canada, Retrieved from website May 2013 from Literature Review – Methadone Maintenance Treatment: http://www.hc-sc.gc.ca/hc-ps/pubs/adp-apd/methadone/effectiveness-efficacite-eng.php
Ialomiteanu AR, Adlaf EM, Hamilton H & Mann RE. CAMH Monitor eReport: Addiction and Mental Health Indicators Among Ontario Adults, 1977-2011 CAMH Research Document Series No. 35. 2012. Toronto: Centre for Addiction and Mental Health.
Johnson R, et al. (2003). Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 70(2 Suppl): S87-S101
Kahan M, Wilson L, Mailis-Gagnon A, Srivastava A. Canadian guideline for safe and effective use of opioids for chronic noncancer pain. Clinical summary for family physicians. Part 2: special populations. Can Fam Physician. 2011; 57:1269–76.
26
Copyright © CAMH 2011Copyright © CAMH 2011
Lacroix L, et al. (2004). Buprenorphine in pregnant opioid dependent women: first results of a prospective study. Addiction. 99: 209-214
Mattick RP, Kimber J, Breen C, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database of Systematic Reviews 2008;CD002207(April 16). Johnson RE, et al. (2001) Buprenorphine treatment of pregnant opioid-dependent women: maternal and neonatal outcomes. Drug Alcohol Depend.; 63: 97- 103
Methadone Maintenance Treatment, Client Handbook, Centre for Addiction and mental Health 2003
Methadone Maintenance Treatment: Program Standards and Clinical Guidelines, February 2011. Retrieved from the College of Physicians and and Surgeons Website: http://www.cpso.on.ca/uploadedFiles/members/MMT-Guidelines.pdf
Methadone Research Web Guide December 2006. Revised from: Methadone Maintenance Treatment: Translating Research Into Policy (1995) prepared by the National Institute on Drug Abuse (NIDA) International Program.
Ottawa Charter,http://health.qld.gov.au/atod/documents/atod_prev_statement.pdf 2009Paglia-Boak A, Adlaf EM, Mann RE. Drug use among Ontario students, 1977-2011: Detailed OSDUHS findings. CAMH Research Document Series No. 32. 2011. Toronto, ON: Centre for Addiction and Mental Health.
Prochaska JO, DiClemente CC & Norcross JC. In search of how people change: Applications to addictive behaviors. American Psychologist. 1992; 47(9), 1102-1114
References
Copyright © CAMH 2011Copyright © CAMH 2011
77
Queensland Health Population Health Plan 2007–2012) Prevention Statement: December 2009Selby, P. & Kahan, M. (2008). Methadone Maintenance: A Physician's Guide to Treatment (2nd ed.). Toronto: Centre for Addiction and Mental Health.
Shield KD, Ialomiteanu A, Fischer B, Mann RE, Rehm J: Non-medical use of prescription opioids among Ontario adults: data from the 2008/2009 CAMH monitor. Can J Public Health 2011, 102(5):330-335.
Whitehead M & Dahlgren G. What can we do about inequalities in health? Lancet, 1991; 338: 1059-1063.
References
Related Documents










![JMartello.pptx [Read-Only] - IntNSA · 2018-12-06 · Jennifer Martello, DNP, RN, FNP-BC University of Pittsburgh School of Nursing Capstone Committee Chair Dr. Brenda Cassidy, DNP,](https://static.cupdf.com/doc/110x72/5f9390583bf6b522112215bd/read-only-intnsa-2018-12-06-jennifer-martello-dnp-rn-fnp-bc-university.jpg)
