OPEN UNIVERSITY OF MALAYSIA RENAL NURSING – NBNS3504 Dr. S. Nishan Silva (MBBS)

OPEN UNIVERSITY OF MALAYSIA RENAL NURSING – NBNS3504 Dr. S. Nishan Silva (MBBS)
Jan 02, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

OPEN UNIVERSITY OF MALAYSIARENAL NURSING – NBNS3504
Dr. S. Nishan Silva(MBBS)

FUNCTIONS OF THE URINARY SYSTEM
Elimination of waste productsNitrogenous wastes e.g. urea, uric acid, creatinine
ToxinsDrugs

FUNCTIONS OF THE URINARY SYSTEM
Regulate aspects of homeostasisWater balanceElectrolytesAcid-base balance in the blood (pH)Blood pressureRed blood cell productionActivation of vitamin D

ORGANS OF THE URINARY SYSTEM
Figure 15.1a
Kidneys
Ureters
Urinary bladder
Urethra

5

6

7
Transverse sections show retroperitoneal position of kidneys
Note also: liver, aorta muscles on CT
Note layers of adipose (fat), capsule, fascia

8

9
FOR STUDYING
Parts of the kidney:1. Renal pyramid2. Efferent vessel3. Renal artery4. Renal vein5. Renal hilum6. Renal pelvis7. Ureter8. Minor calyx9. Renal capsule10. Inferior renal capsule11. Superior renal capsule12. Afferent vessel13. Nephron14. Minor calyx15. Major calyx16. Renal papilla17. Renal column

10
Kidney has two regionsCortex: outer
Columns of cortex divide medulla into “pyramids”Medulla: inner
Darker, cone-shaped medullary or renal pyramids Parallel bundles of urine-collecting tubules

LOCATION OF THE KIDNEYS
At the level of T12 to L3
Attached to ureters, renal blood vessels, and nerves at renal hilus
On top of each kidney is an adrenal gland

REGIONS OF THE KIDNEY
Figure 15.2b
Renal cortex – outer region
Renal medulla – inside the cortex
Renal pelvis – inner collecting tube

KIDNEY STRUCTURES
Medullary pyramids – triangular regions of tissue in the medulla
Renal columns – extensions of cortex-like material inward
Calyces – cup-shaped structures that funnel urine towards the renal pelvis

NEPHRONS
Main structures of the nephrons
Glomerulus Renal tubule

GLOMERULUS
A specialized capillary bed
Attached to arterioles on both sides (maintains high pressure)
Large afferent arteriole
Narrow efferent arteriole
Figure 15.3c

BLOOD FLOW IN THE KIDNEYS
Figure 15.2c

GLOMERULUS
Capillaries are covered with podocytes from the renal tubule
The glomerulus sits within a glomerular capsule (the first part of the renal tubule)
Figure 15.3c

RENAL TUBULE
Glomerular (Bowman’s) capsule
Proximal convoluted tubule
Loop of HenleDescending limbAscending limbDistal
convoluted tubule
Straight collecting tubule
Figure 15.3b

PERITUBULAR CAPILLARIES
Arise from efferent arteriole of the glomerulus
Normal, low pressure capillaries
Attached to a venule
Cling close to the renal tubule
Reabsorb (reclaim) some substances from collecting tubes

URINE FORMATION PROCESSES
Filtration
Reabsorption
Secretion
Figure 15.4

FILTRATION
Nonselective passive process
Water and solutes smaller than proteins are forced through capillary walls
Blood cells cannot pass out to the capillaries
Filtrate is collected in the glomerular capsule and leaves via the renal tubule

REABSORPTION
Some reabsorption is passive, most is active
Most reabsorption occurs in the proximal convoluted tubule

SECRETION – REABSORPTION IN REVERSE
Some materials move from the peritubular capillaries into the renal tubules
Hydrogen and potassium ionsCreatinine, ureaPenicillin, cocaine, marijuana, many food preservatives, and some pesticides

FORMATION OF URINE
Figure 15.5

CHARACTERISTICS OF URINE USED FOR MEDICAL DIAGNOSIS
Colored somewhat yellow due to the pigment urochrome (from the destruction of hemoglobin) and solutes
Clear
Sterile
Slightly aromatic
Normal pH of around 6
Specific gravity of 1.001 to 1.035

URETERS
Continuous with the renal pelvis
Enter the posterior aspect of the bladder
Run behind the peritoneum
Peristalsis (they contain smooth muscle) aids gravity in urine transport

URINARY BLADDER
Figure 15.6
Smooth, collapsible, muscular sac
Temporarily stores urine

URINARY BLADDER
Trigone – three openingsTwo from the uretersOne to the urethrea
Figure 15.6

URINARY BLADDER WALL
Composed of three layers:Outer layer – loose connective tissue covered on the upper surface by the peritoneum
Middle layer - three layers of smooth muscle (detrusor muscle)
Inner layer - mucosa made of transitional epithelium
Walls are thick and folded in an empty bladder, can expand significantly without increasing internal pressure


31
THE URETHRASmooth muscle with inner mucosa Changes from transitional through stages to stratified squamous near
end Drains urine out of the bladder and body
Male: about 20 cm (8”) longFemale: 3-4 cm (1.5”) long Short length is why females have more urinary tract infections than
males - ascending bacteria from stool contamination
Urethra____
urethra

32
Urethral sphincters Internal: involuntary sphincter of smooth muscleExternal: skeletal muscle inhibits urination voluntarily until proper time (levator anni muscle also helps voluntary constriction)
Males: urethra has three regions (see right)
1. Prostatic urethra__________
2. Membranous urethra____
3. Spongy or penile urethra_____
_________trigone
female

URETHRA
Release of urine is controlled by two sphincters
Internal urethral sphincter (involuntary)External urethral sphincter (voluntary)

URETHRA GENDER DIFFERENCES
LocationFemales – along wall of the vagina and opens to the outside at the urethral meatus between the labia minora.
Males – through the prostate and penis
FunctionFemales – only carries urineMales – carries urine and is a passageway for sperm cells


STORAGE REFLEXES
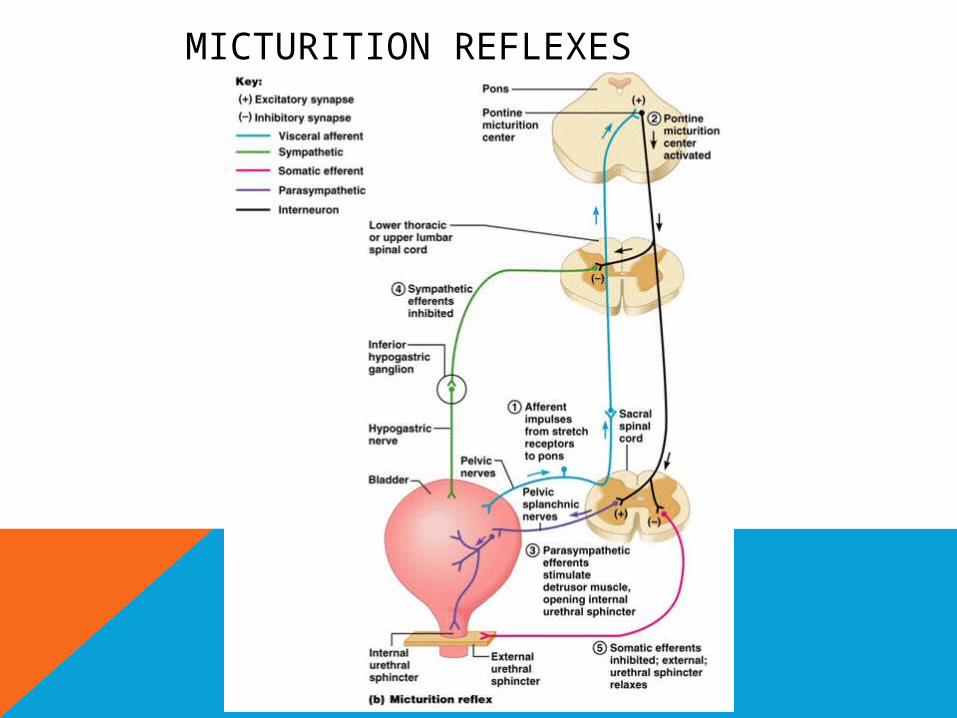
MICTURITION REFLEXES

38
Micturition AKA:
Voiding Urinating Emptying the bladder
(See book for diagramexplanation p 701)
KNOW:Micturition center of brain:
pons(but heavily influenced by
higher centers) Parasympathetic: to voidSympathetic: inhibits
micturition

URINE
ANALYSIS

COLLECTION OF URINE
Early morning sample-qualitative
Random sample- routine24hrs sample- quantitativeMidstream sample-UTIPost prandial sample-D.M

Clean Catch

Specimen Collection
Supra-pubic Needle Aspiration

24 HOUR URINE SAMPLE
1. For quantitative estimation of proteins
2. For estimation of vanillyl mandelic acid, 5-hydroxyindole acetic acid, metanephrines
3. For detection of AFB in urine
4. For detection of microalbuminuria


URINARY VOLUME
Normal = 600-1550ml
Polyuria- >2000ml
Oliguria-<400ml
Anuria-complete cessation of urine(<200ml)
Nocturia-excretion of urine by a adult of >500ml with a specific gravity of <1.018 at night (characteristic of chronic glomerulonephritis)

COLOR & APPEARANCE
Normal= clear & pale yellow
1. Colourless- dilution, diabetes mellitus, diabetes insipidus, diuretics
2. Milky-purulent genitourinary tract infection, chyluria
3. Orange-fever, excessive sweating
4. Red-beetroot ingestion,haematuria
5. Brown/ black- alkaptunuria, melanin

URINARY PH/ REACTION
Reaction reflects ability of kidney to maintain normal hydrogen ion concentration in plasma & ECF
Normal= 4.6-8
Tested by- 1.litmus paper
2. pH paper
3. dipsticks

ODOUR
Normal= aromatic due to the volatile fatty acids
Ammonical – bacterial action
Fruity- ketonuria

SPECIFIC GRAVITY
Depends on the concentration of various solutes in the urine.
Measured by-urinometer
- refractometer
- dipsticks

URINOMETER
Take 2/3 of urinometer container with urine
Allow the urinometer to float into the urine
Read the graduation at the lowest level of urinary meniscus
Correction of temperature & albumin is a must.
Urinometer is calibrated at 15or 200cSo for every 3oc increase/decrease
add/subtract 0.001For 1gm/dl of albumin add0.001


CHEMICAL EXAMINATION
ProteinsSugarsKetone bodiesBilirubinBile saltsUrobilinogenBlood

MICROSCOPIC EXAMINATION
Microscopic urinalysis is done simply pouring the urine sample into a test tube and centrifuging it (spinning it down in a machine) for a few minutes. The top liquid part (the supernatant) is discarded. The solid part left in the bottom of the test tube (the urine sediment) is mixed with the remaining drop of urine in the test tube and one drop is analyzed under a microscope

CRYSTALS IN URINE
Crystals in acidic urine
Uric acid
Calcium oxalate
Cystine
Leucine
Crystals in alkaline urine
Ammonium magnesium phosphates(triple phosphate crystals)
Calcium carbonate

CRYSTALS

CASTS
Urinary casts are cylindrical aggregations of particles that form in the distal nephron, dislodge, and pass into the urine. In urinalysis they indicate kidney disease. They form via precipitation of Tamm-Horsfall mucoprotein which is secreted by renal tubule cells.

TYPES OF CASTS
Acellular casts
Hyaline casts
Granular casts
Waxy casts
Fatty casts
Pigment casts
Crystal casts
Cellular casts
Red cell casts
White cell casts
Epithelial cell cast

GRANULAR CASTS
Granular casts can result either from the breakdown of cellular casts or the inclusion of aggregates of plasma proteins (e.g., albumin) or immunoglobulin light chains
indicative of chronic renal disease


Microscopic Examination Granular Cast

Microscopic Examination WBCs Cast

Microscopic Examination RBCs Cast -
Histology

Chemical AnalysisUrine
DipstickGlucoseGlucose
BilirubinBilirubin
KetonesKetones
Specific GravitySpecific Gravity
BloodBlood
pHpH
ProteinProtein
UrobilinogenUrobilinogen
NitriteNitrite
Leukocyte EsteraseLeukocyte Esterase

BLOOD ANALYSIS
(Of creatinine)
Glomerulofiltration Rate

ESTIMATED GFR
GFR Calculatorhttp://easycalculation.com/medical/gfr.php

RENAL SCAN

RENAL ARTERIOGRAM

INTRAVENOUS PYELOGRAM

RENAL BIOPSY

PYELO
NEPHRIT
I
S
70

ETIOLOGY❏ usually ascending microorganisms, most often
bacteria
❏ in females with uncomplicated pyelonephritis usually E. coli
❏ causative microorganisms are usually E. coli, Klebsiella, Proteus, Serratia, Pseudomonas, Enterococcus, and S. aureus
❏ if S. aureus is found, suspect bacteremic spread from a distant focus (e.g. septic emboli in infective endocarditis) and suspect (possible multiple intra-renal microabscesses or perinephric abscess)
71

72

73

CLINICAL PRESENTATION
❏ rapid onset (hours to a day)
❏ lethargic and unwell, fever, tachycardia, shaking, chills, nausea and vomiting, myalgias
❏ marked CVA or flank tenderness; possible abdominal pain on deep palpation
❏ symptoms of lower UTI may be absent (urgency, frequency, dysuria)
❏ may have symptoms of Gram negative sepsis
74

INVESTIGATIONS
❏ urine dipstick: +ve for leukocytes and nitrites, possible hematuria
❏ microscopy: > 5 WBC/HPF in unspun urine or > 10 WBC/HPF in spun urine, bacteria
❏ Gram stain: Gram negative rods, Gram positive cocci
❏ culture: > 105 colony forming units (CFU)/mL in clean catch midstream urine or > 102 CFU/mL in suprapubic aspirate or catheterized specimen
❏ CBC and differential: leukocytosis, high % neutrophils
❏ blood cultures: may be positive in 20% of cases, especially in S. aureus infection
❏ consider investigation of complicated pyelonephritis: if fever, pain, leukocytosis not resolving with treatment within 72 hr, if male patient, or if there is history of urinary tract abnormalities (abdo /pelvis U/S, CT for renal abscess, spiral CT for stones, cystoscopy)
75

76

COMPLICATIONS
Chronicity
Bacteraemia or Septicaemia
77

TREATMENT❏ uncomplicated pyelonephritis with mild
symptoms
• 14 day course of TMP/SMX (trimethoprim-sulfamethoxazole) or fluoroquinolone or third generation cephalosporin
• start with IV for several days and then switch to PO (can then be treated as outpatient)
❏ patient more than mildly symptomatic or complicated pyelonephritis in the setting of stone obstruction is an urologic emergency (placing patient at risk of kidney loss or septic shock)
• start broad spectrum IV antibiotics until cultures return (imipenem or emropenem or piperacillin /tazobactam or ampicillin+gentamicin) and treat 2-3 weeks
• follow-up cultures 2-4 weeks after stopping treatment
❏ if no improvement in 48-72 hr, need to continue on IV antibiotics, assess for complicated pyelonephritis or possible renal or perinephric abscess
78

79
GLOMERULONEPHRITIS

80
Electron micrograph of a normal glomerular capillary loop showing the fenestrated endothelial cell (Endo), the glomerular basement membrane (GBM), and the epithelial cells with its interdigitating foot processes (arrow). The GBM is thin and no electron dense deposits are present. Two normal platelets are seen in
the capillary lumen. Courtesy of Helmut Rennke, MD.

81
Capillary Space
Endothelium
Urinary Space
GBM
Podocyte
FILTRATION MEMBRANE – ELECTRON MICRO.
MD consult

82
Electron micrograph in dense deposit disease (DDD) showing dense, ribbon-like appearance of subendothelial and intramembranous material (arrow) and narrowing of the capillary lumen due to proliferation of cells (double arrow). Courtesy of Helmut Rennke, MD.

83
POSSIBLE CLINICAL MANIFESTATIONS
Proteinuria – asymptomatic
Haematuria – asymptomatic
Hypertension
Nephrotic syndrome
Nephritic syndrome
Acute renal failure
Rapidly progressive renal failure
End stage renal failure

84
DIAGNOSIS
Look for clues History
Haematuria Proteinuria Azotemia azote – nitrogen A – without Zoe – life “The gas does not support life” (French chemists Gayton de Morveau
(1737-1816) and Antoine Lavoisier (1743-1794) )
McCarthy ET, November 2008

NEPHROTIC SYNDROME
Nephrotic syndrome (NS) results from increased permeability of Glomeulrar basement membrane (GBM) to plasma protein.
It is clinical and laboratory syndrome characterized by massive proteinuria, which lead to hypoproteinemia ( hypo-albuminemia), hyperlipidemia and pitting edema.
(4-increase, 1-decrease).

NEPHROTIC CRITERIA:-
*Massive proteinuria: qualitative proteinuria: 3+ or 4+, quantitative proteinuria : more than 40 mg/m2/hr in children (selective).
*Hypo-proteinemia : total plasma proteins < 5.5g/dl and serum albumin : < 2.5g/dl.
*Hyperlipidemia: serum cholesterol : > 5.7mmol/L
*Edema: pitting edema in different degree

NEPHRITIC CRITERIA
-Hematuria: RBC in urine (gross hematuria)
-Hypertension: ≥130/90 mmHg in school-age children ≥120/80 mmHg in preschool-age children ≥110/70 mmHg in infant and toddler’s children
-Azotemia ( renal insufficiency ) : Increased level of serum BUN 、 Cr-Hypo-complementemia: Decreased level of serum c3
Oliguria, Oedema, Albuminurea

CLASSIFICATION:
A-Primary Idiopathic NS (INS): majority
The cause is still unclear up to now. Recent 10 years ,increasing evidence has suggested that INS may result from a primary disorder of T– cell function.
Accounting for 90% of NS in child. mainly discussed.
B-Secondary NS:
NS resulted from systemic diseases, such as anaphylactoid purpura , systemic lupus erythematosus, HBV infection.
C-Congenital NS: rare
*1st 3monthe of life ,only treatment renal transplantation

SECONDARY NS Drug,Toxic,Allegy: mercury, snake venom, vaccine, pellicillamine,
Heroin, gold, NSAID, captopril, probenecid, volatile hydrocarbons
Infection: APSGN, HBV, HIV, shunt nephropathy, reflux nephropathy, leprosy, syphilis, Schistosomiasis, hydatid disease
Autoimmune or collagen-vascular diseases: SLE, Hashimoto’s thyroiditis,, HSP, Vasculitis
Metabolic disease: Diabetes mellitus
Neoplasma: Hodgkin’s disease, carcinoma ( renal cell, lung, neuroblastoma, breast, and etc)
Genetic Disease: Alport syn, Sickle cell disease, Amyloidosis, Congenital nephropathy
Others: Chronic transplant rejection, congenital nephrosclerosis

IDIOPATHIC NS (INS): PATHOLOGY:-
Minimal Change Nephropathy (MCN): <80%The glomeruli appear normal basically Under
Light microscopy, and Under Immunofluorescence
*under Electron microscopy – fusion of the foot processes of the podocytes
(2) Non—MCN : < 20%*Mesangial proliferative glomerulonephritis
(MsPGN): about 10%*Focal segmental glomerulosclerosis (FSGS): 5%*Membranous Nephropathy (MN) : 2% *Membrane proliferative glomerulonephritis
(MPGN) : 1% *Others : rare,Cresent glomerulonephritis

CLINICAL MANIFESTATION:-
IN MCNS , The male preponderance of 2:1
: 1.Main manifestations:
Edema (varying degrees) is the common symptomLocal edema: edema in face , around eyes( Periorbital swelling) , in
lower extremities. Generalized edema (anasarca), edema in penis and scrotum.
2-Non-specific symptoms:
Fatigue and lethargyloss of appetite, nausea and vomiting ,abdominal pain , diarrhea
body weight increase, urine output decrease pleural effusion (respiratory distress)



INVESTIGATIONS:-
1-Urine analysis:-
A-Proteinuria : 3-4 + SELECTIVE.
b-24 urine collection for protein>40mg/m2/hr for children
c- volume: oliguria (during stage of edema formation)
d-Microscopically:-
microscopic hematuria 20%, large number of hyaline cast

INVESTIGATIONS:-
2-Blood:A-serum protein: decrease >5.5gm/dL , Albumin levels are low ( < 2.5gm/dL).
B-Serum cholesterol and triglycerides: Cholesterol > 5.7mmol/L (220mg/dl).
C-- ESR↑ > 100mm/hr during activity phase
.3.Serum complemen: Vary with clinical type.
4.Renal function
.

KIDNEY BIOPSY:-
Considered in:
1-Secondary N.S
2-Frequent relapsing N.S
3-Steroid resistant N.S
4- Hematuria
5-Hypertension
6- Low GFR

COMPLICATIONS OF NS:-
1-Infections:Infections is a major complication in children with NS. It frequently trigger relapses.
Nephrotic pt are liable to infection because :A-loss of immunoglobins in urine.B-the edema fluid act as a culture medium.C-use immunosuppressive agents.
D- malnutrition
The common infection : URI, peritonitis, cellulitis and UTI may be seen.
Organisms: encapsulated (Pneumococci, H.influenzae), Gram negative (e.g E.coli

COMPLICATION …
Vaccines in NS;-
polyvalent pneumococcal vaccine (if not previously immunized) when the child is in remission and off daily prednisone therapy.
Children with a negative varicella titer should be given varicella vaccine.

COMPLICATION…..
2-Hypercoagulability (Thrombosis).
Hypercoagulability of the blood leading to venous or arterial thrombosis:
Hypercoagulability in Nephrotic syndrome caused by: 1-Higher concentration of I,II, V,VII,VIII,X and fibrinogen
2- Lower level of anticoagulant substance: antithrombin III
3-decrease fibrinolysis.
4-Higher blood viscosity
5- Increased platelet aggregation
6- Overaggressive diuresis

3-ARF: pre-renal and renal
4- cardiovascular disease :-Hyperlipidemia, may be a risk factor for cardiovascular disease.
5-Hypovolemic shock
6-Others: growth retardation, malnutrition, adrenal cortical insufficiency

GENERAL THERAPY:-
Hospitalization:- for initial work-up and evaluation of treatment.
Activity: usually no restriction , except
massive edema,heavy hypertension and infection.
Diet Hypertension and edema: Low salt diet (<2gNa/ day) only during period of edema or salt-free diet. Severe edema: Restricting fluid intake
Avoiding infection: very important.
Diuresis: Hydrochlorothiazide (HCT) : 2mg/kg.d
Antisterone : 2 ~ 4mg/kg.d
Dextran : 10 ~ 15ml/kg , after 30 ~ 60m,
followed by Furosemide (Lasix) at 2mg/kg .

INDUCTION USE OF ALBUMIN:-
Albumin + Lasix (20 % salt poor)
1-Severe edema
2-Ascites
3-Pleural effusion
4-Genital edema
5-Low serum albumin

CORTICOSTEROID—PREDNISONE THERAPY:-
Prednisone tablets at a dose of 60 mg/m2/day (maximum daily dose, 80 mg divided into 2-3 doses) for at least 4 consecutive weeks.
After complete absence of proteinuria, prednisone dose should be tapered to 40 mg/m2/day given every other day as a single morning dose.
The alternate-day dose is then slowly tapered and discontinued over the next 2-3 mo.

TREATMENT OF RELAPSE IN NS:
Many children with nephrotic syndrome will experience at least 1 relapse (3-4+proteinuria plus edema).
daily divided-dose prednisone at the doses noted earlier (where he has the relapse) until the child enters remission (urine trace or negative for protein for 3 consecutive days).
The pred-nisone dose is then changed to alternate-day dosing and tapered over 1-2 mo.

ACCORDING TO RESPONSE TO PREDNISONE THERAPY:
*Remission: no edema, urine is protein free for 5 consecutive days.
* Relapse: edema, or first morning urine sample contains > 2 + protein for 7 consecutive days.
*Frequent relapsing: > 2 relapses within 6 months (> 4/year).
*Steroid resistant: failure to achieve remission with prednisolone given daily for 28 days.

ALTERNATIVE AGENT:-
When can be used:
Steroid-dependent patients, frequent relapsers, and steroid-resistant patients.
Cyclophosphamide Pulse steroids
Cyclosporin A
Tacrolimus
Microphenolate

107
Diseases PSGN IgA Nephropathy MPGN RPGN
Age and Sex All ages, mean 7 years, 2:1 male
2:1 male, 15-35 yrs 6:1 male, 15-30 yrs Mean 51yrs, 2:1 male
Clinical Manifestations 90% 50% 90% 90%
Acute nephritic syndrome
Occasionally 50% Rare rare
Asymptomatic haematuria
10-20% Rare Rare 10-20%
Nephrotic syndrome 70% 30-50% Rare 25%
Hypertension 50% Rare 50% 60%
Acute renal failure Latent 1-3 weeks Follows viral infection Pul haemorrhage, iron def
none
Lab findings ASOT IgA +anti GBM membrane + ANCA
Positive streptozyme IgA in dermal caps
C3-C9 N C1 and C4
Immunogenetics HLA B12
Light microscopy Diffuse proliferation Focal proliferation Focal- diffuse crescentic Crescentic GN
Immunoflourescence Granular IgG and C3 Diffuse mesangial IgA Linear IgG and C3 No immune complexes
Electron microscopy Subepithelial humps Mesangial deposits No deposits No deposits
Prognosis 95% cure5% progress
Slow progression in 25-50 years
75% stabilise or improve if treated early
75% stabilise or improve if treated early
Treatment Supportive None established Plasman exchange, cyclosphosphamide, steroids
Pulsed steroid therpy


Related Documents