International Psychogeriatrics: page 1 of 13 C International Psychogeriatric Association 2014 doi:10.1017/S1041610214002361 Open referral policy within a nurse-led memory clinic: patient demographics, assessment scores, and diagnostic profiles ........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................... Melinda Minstrell, 1 Michael Bentley, 1 Hazel Bucher, 2 Martin Morrissey, 2 Carl Higgs, 1 Andrew Robinson 1,3 and Christine Stirling 3 1 Wicking Dementia Research and Education Centre, University of Tasmania, Hobart, Tasmania 7001, Australia 2 Department of Health and Human Services,Tasmania Older Persons Mental Health, 90 Davey Street, Hobart, Tasmania 7000, Australia 3 School of Health Sciences, University of Tasmania, Hobart, Tasmania 7000, Australia ABSTRACT Background: Memory clinics, typically led by multidisciplinary teams and requiring health professional referral, are one means of providing diagnosis and care coordination for dementia. Nurse-led clinics may provide an effective and alternative means to dementia diagnosis, and open referral policies may minimize existing barriers to accessing a diagnosis, but evidence is needed. Methods: Patients attending a one-day per week nurse-led memory clinic over a 25-month period during 2011–2013 (n = 106) completed comprehensive cognitive assessments and were diagnosed by an aged care nurse practitioner. Descriptive statistics detail the demographics, assessment scores, and diagnostic profiles of patients. Comparable data from published literature was identified, and the differences were analyzed qualitatively. Results: One hundred and six patients were assessed with the key differences from other data sets being history of falls more common, higher mean Mini-Mental State Examination scores, and fewer dementia diagnoses. Sixty-four patients (60%) were self-referred to the nurse-led memory clinic, of which 19 (30%) were diagnosed with mild cognitive impairment (MCI) or dementia. Overall, forty-eight patients (45%) received diagnoses of MCI or dementia. Conclusions: An open referral policy led to a high proportion of patients being self-referred, and nearly a third of these were diagnosed with cognitive impairment or dementia. Open referral policies and nurse-led services may overcome some of the barriers to early diagnosis that are currently experienced. Considering an aging population worldwide and the associated increases in cognitive impairment, which benefits from early identification and intervention, this paper provides an alternative model of nurse-led assessment. Key words: memory clinic, nurse practitioner, open referral policy, nurse-led clinic, self-referral, dementia Introduction Timely diagnosis of dementia is important as it enables people with dementia and their families to engage with appropriate treatment and support services, thereby facilitating access to appropriate care pathways (Burns and Iliffe, 2009). Furthermore, cost benefit analyses suggest that the initial costs of diagnosis and early intervention provide “net savings of around US$10,000 per person with dementia across the disease course” (Prince et al., 2011). Correspondence should be addressed to: Christine Stirling, Associate Professor, School of Health Sciences, University of Tasmania, Private Bag 135, Hobart, TAS 7000, Australia. Phone: +61-3-6226-4678; Fax: +61-3-6226- 4690. Email: [email protected]. Received 22 May 2014; revision requested 29 Jun 2014; revised version received 8 Oct 2014; accepted 8 Oct 2014. Around 50–80% of people with dementia are believed to be undiagnosed (Prince et al., 2011) and research suggests that primary care physicians do not regularly screen for, recognize, or discuss dementia with their patients (Millard et al., 2011; van den Dungen et al., 2012). It may be particularly difficult for general practitioners (GPs) to identify individuals with mild dementia due primarily to the lack of symptom severity (Mitchell et al., 2011). Healthcare providers have identified their own knowledge gaps about dementia, including diagnosis, dementia-specific services and/or support services, and the legal rights of patients (Turner et al., 2004; Hansen et al., 2005). In one study, two-thirds of GPs lacked confidence in dementia symptom management (Turner et al., 2004). There are also barriers for patients, carers, and healthcare providers seeking information about

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

International Psychogeriatrics: page 1 of 13 C© International Psychogeriatric Association 2014doi:10.1017/S1041610214002361
Open referral policy within a nurse-led memory clinic: patientdemographics, assessment scores, and diagnostic profiles
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Melinda Minstrell,1 Michael Bentley,1 Hazel Bucher,2 Martin Morrissey,2 Carl Higgs,1
Andrew Robinson1,3 and Christine Stirling3
1Wicking Dementia Research and Education Centre, University of Tasmania, Hobart, Tasmania 7001, Australia2Department of Health and Human Services, Tasmania Older Persons Mental Health, 90 Davey Street, Hobart, Tasmania 7000, Australia3School of Health Sciences, University of Tasmania, Hobart, Tasmania 7000, Australia
ABSTRACT
Background: Memory clinics, typically led by multidisciplinary teams and requiring health professional referral,are one means of providing diagnosis and care coordination for dementia. Nurse-led clinics may provide aneffective and alternative means to dementia diagnosis, and open referral policies may minimize existing barriersto accessing a diagnosis, but evidence is needed.
Methods: Patients attending a one-day per week nurse-led memory clinic over a 25-month period during2011–2013 (n = 106) completed comprehensive cognitive assessments and were diagnosed by an aged carenurse practitioner. Descriptive statistics detail the demographics, assessment scores, and diagnostic profilesof patients. Comparable data from published literature was identified, and the differences were analyzedqualitatively.
Results: One hundred and six patients were assessed with the key differences from other data sets being historyof falls more common, higher mean Mini-Mental State Examination scores, and fewer dementia diagnoses.Sixty-four patients (60%) were self-referred to the nurse-led memory clinic, of which 19 (30%) were diagnosedwith mild cognitive impairment (MCI) or dementia. Overall, forty-eight patients (45%) received diagnoses ofMCI or dementia.
Conclusions: An open referral policy led to a high proportion of patients being self-referred, and nearly athird of these were diagnosed with cognitive impairment or dementia. Open referral policies and nurse-ledservices may overcome some of the barriers to early diagnosis that are currently experienced. Considering anaging population worldwide and the associated increases in cognitive impairment, which benefits from earlyidentification and intervention, this paper provides an alternative model of nurse-led assessment.
Key words: memory clinic, nurse practitioner, open referral policy, nurse-led clinic, self-referral, dementia
Introduction
Timely diagnosis of dementia is important asit enables people with dementia and theirfamilies to engage with appropriate treatmentand support services, thereby facilitating access toappropriate care pathways (Burns and Iliffe, 2009).Furthermore, cost benefit analyses suggest that theinitial costs of diagnosis and early interventionprovide “net savings of around US$10,000 perperson with dementia across the disease course”(Prince et al., 2011).
Correspondence should be addressed to: Christine Stirling, Associate Professor,School of Health Sciences, University of Tasmania, Private Bag 135,Hobart, TAS 7000, Australia. Phone: +61-3-6226-4678; Fax: +61-3-6226-4690. Email: [email protected]. Received 22 May 2014; revisionrequested 29 Jun 2014; revised version received 8 Oct 2014; accepted 8 Oct2014.
Around 50–80% of people with dementia arebelieved to be undiagnosed (Prince et al., 2011)and research suggests that primary care physiciansdo not regularly screen for, recognize, or discussdementia with their patients (Millard et al., 2011;van den Dungen et al., 2012). It may be particularlydifficult for general practitioners (GPs) to identifyindividuals with mild dementia due primarily tothe lack of symptom severity (Mitchell et al.,2011). Healthcare providers have identified theirown knowledge gaps about dementia, includingdiagnosis, dementia-specific services and/or supportservices, and the legal rights of patients (Turneret al., 2004; Hansen et al., 2005). In one study,two-thirds of GPs lacked confidence in dementiasymptom management (Turner et al., 2004).
There are also barriers for patients, carers,and healthcare providers seeking information about
2 M. Minstrell et al.
dementia services and diagnosis, with some familycarers describing “futile searching for informationwithin a seemingly disorganized healthcare system”(Robinson et al., 2009). Open referral policies (self-or health professional referrals) have been proposedto enable people with dementia to “leapfrog”primary care physicians in their requests for timelydiagnosis (Scott and Donnelly, 2005; Robinsonet al., 2009).
Memory clinics can facilitate resolution ofdiagnostic, management, and care coordinationissues by providing a single point of entry todementia services and information. Traditionally,memory clinics are found in high income countries,run by multidisciplinary teams (MDT), includinga core team of clinicians (Jolley et al., 2006;Woodward and Woodward, 2009; Prince et al.,2011). Good links and networks with local servicesand social and healthcare systems are an importanthallmark of memory clinics (Jolley et al., 2006).Woodward and Woodward’s (2009) description of23 Australian memory clinics (most located in thestate of Victoria) identified that neuropsychologists,geriatricians, and nurses were usual clinical staff,with doctors typically undertaking the initialassessment.
Traditional memory clinics are considered the“gold standard” of dementia diagnosis (Draškovicet al., 2008) and are clearly intensive withnearly five clinical hours spent on each patient(Woodward and Woodward, 2009). However,given the level of under-diagnosis and the projectedincreases in dementia prevalence, sustaining theseclinics is a resourcing challenge (Gladman et al.,2007). Furthermore, some locations may lack theavailability of multidisciplinary clinical staff tocontribute to such a clinic, so alternatives must besought to increase access to dementia diagnosis.
Nurse-led clinics are an alternative means ofdiagnosis that are seeding internationally. Nurse-ledmemory clinics (NLMCs) can potentially providequality diagnostic services while drawing on fewerfinancial and personnel resources. The literaturesupporting nurse-led clinics is growing (Hatchett,2008), and there is increasing use of nurse-ledclinics and services across different health services.Nurse practitioners (NPs) may be particularly wellsuited to lead memory clinics, as NPs completea Master’s level degree and clinical training in aspecific area of nursing. They develop “extendedskills, knowledge and experience in the assessment,planning, implementation, diagnosis and evaluationof care as required” (Gardner et al., 2004).The capacity for NPs to specialize and developcomprehensive knowledge of dementia is a keyaspect of diagnosis (Woodward and Woodward,2009).
Nurses with advanced training have demon-strated their capacity to diagnose cognitiveimpairment in one study. The specialist nurses’structured assessment resulted in a very high degreeof agreement between nurse and MDT diagnoses(Page et al., 2008). Those diagnosed are alsobenefited by earlier linking to appropriate carepathways than those waiting for MDT.
The memory clinic described here differs fromconventional approaches to dementia diagnosis intwo important ways: It is nurse-led, and employsan open referral policy. This is not the first nurse-led memory service to be reported (for example,Mullins and Fitch, 2000), and evidence indicatesthat nurses have capacity to screen for dementia asa preliminary to specialist diagnosis (Seymour et al.,1994; Mullins and Fitch, 2000; Page et al., 2008).However, nurses screening for dementia as opposedto diagnosing dementia is an important distinction.With the exception of the study reported by Scottand Donnelly (2005), the vast majority of nursingservice publications describe nurses screening forMDT memory clinics.
In contrast, the nurse practitioner (NP) withinthe NLMC described here both screens anddiagnoses for dementia while maintaining stronglinks with ongoing dementia care services andspecialists. Although screening tools provide scoringranges which suggest cognitive impairment, aformal diagnosis involves detailed history andphysical examination, observing the patient’spresentation, with additional information benefitsfrom an informant interview (Prince et al.,2011). It is the synthesis of these variouscomponents that enables the diagnosis of cognitiveimpairment/dementia.
However, better information about NLMCs,including the characteristics of those who attend,and the potential influence of an open referralpolicy would help policy makers who are responsiblefor meeting the rising diagnosis demand. Thispaper aims to identify the demographics, assessmentscores, and diagnostic profiles of those attending anNLMC with an open referral policy and to assesshow it differs from other memory clinic profiles.
Methods
DesignThis study collected descriptive data relating todemographics, assessment scores, and diagnosisof consenting consecutive patients attending theNLMC over a 25-month period in 2011–2013. Theclinic was held for one day per week, initially atthe Menzies Research Institute of the Universityof Tasmania (as part of the Wicking Dementia
Open referral to a nurse-led memory clinic 3
Research and Education Centre), and then basedwithin the Older Persons Mental Health Service ofthe Tasmanian Department of Health and HumanServices. The NLMC draws from a primarily urbanpopulation base of approximately 250,000 in greaterHobart, the capital city of Tasmania, Australia.People aged 65 years and older constitute over15% of the greater Hobart population. The studyreceived ethical approval from the Tasmania Healthand Medical Human Research Ethics Committee.This was part of a larger study assessing processes,effectiveness, and impact of the NLMC with the fullprotocol published elsewhere (Bentley et al., 2014).
Historically, dementia diagnosis in this area ofTasmania was typically through geriatricians, GPs,and a specialized state health service (i.e. OlderPersons Mental Health). Geriatricians conducteda memory clinic through the local public hospital(requiring GP referral); this changed to a generalistgeriatric clinic around the same time as the NLMCwas launched with waiting times commonly overthree months.
ParticipantsConsent to participate in the study was obtainedfrom patients attending the memory clinic, andall the attendees agreed to participate (n =106). Twelve patients were excluded; four patientshad missing data, four already had a dementiadiagnosis from a specialist, therefore did notcomplete assessments and only had the “follow-up consultation” (i.e. diagnosis implications), threewere referred to an old aged psychiatrist, and onewas only curious about the NLMC. The “openreferral policy” allowed referrals from a wide rangeof sources, including self-referral.
ProcessPatients were encouraged to bring an accompanyingperson to provide corroboration during theirassessment. (If the NP was concerned aboutpossible dementia based on her investigations andhistory taking, she would contact an informant.However, some patients requested that informantsnot be contacted to protect their privacy.) GPswere asked to forward any blood tests on thepatient’s file from the previous 12 months, andin some cases the usual battery of blood tests hadbeen pre-ordered. The NP only ordered blood testsif patient’s history and presentation, as describedbelow, were suggestive of dementia. Imaging wasordered only when clinically indicated (e.g. MRIfor specific vascular risk), and CT scans were notroutinely ordered.
The NP screened patients using assessment tools(see “Instruments”), conducted a comprehensive
medical history and physical review of each patient,including separate interviews with the patient andaccompanying person, collating this informationwithin a visit summary report. (When patientsattended alone, the NP obtained corroborativehistory via telephone in almost all cases.) This reportdetailed each patient’s diagnosis, recommendationsprovided by the NP, and intentions with respect tofollowing up each case. Assessments required twohours contact time (with patient and family and/orinformant), ranging from 1.5–2.5 hours. Thiscompares with five hours contact time traditionallyallotted by MDT clinics.
The NP’s diagnoses were based on hersynthesis of assessment scores, corroborativehistory, patient presentation, and other aspectsof physical examination using the Diagnosticand Statistical Manual of Mental Disorders, 4thEdition (DSM-IV) diagnostic criteria. Patients werecategorized as having no cognitive impairment, mildcognitive impairment (MCI), or dementia. Otherpossible reasons for the cognitive changes, such asdepression, hypothyroidism, or adverse medicationeffects, were considered in the diagnostic processand excluded by clinical reasoning, supportedby diagnostic tests, physical examination, and athorough history. Patients diagnosed with MCIwere differentiated from those decreed to have adementia by the lack of global cognitive impairmentand/or general functional decline associated withtheir identified cognitive deficits.
Importantly, a collaborative agreement betweenthe NLMC and the Older Persons Mental HealthService of the state health department formed a vitalsupport base and resource for NP, ensuring she wasnot an isolated entity. Specifically, NP diagnoseswere discussed with an old age psychiatrist (posthoc) within the context of a supervisory relationship.As confidence between both individuals grew,cases were only discussed to enable the oldage psychiatrist to commence pharmacologicaltreatments (e.g. cholinesterase inhibitors), or orderbrain scans if necessitated (as NPs across Australiaare not allowed to initiate this care). Complicatedcases (n = 3) were referred for comprehensivespecialist review following initial NLMC triageassessment (and excluded from the research) dueto complex presentations not consistent with theDSM-IV diagnostic framework and/or presentingwith complex past history (e.g. complicated mentalhealth history). The researchers played no role in theclinic, quarantining their involvement to research.
The NLMC was advertised twice during thestudy period: a local newspaper article at the initiallaunch (resulting in 65 referrals), and a small articlein the local GP newsletter in the second year.The clinic was also highlighted in local television
4 M. Minstrell et al.
news items during a visit by a prominent politician.No additional advertisement was undertaken in aneffort to ensure waiting lists were not extensive.
InstrumentsThe assessment battery comprised the followingvalidated and established assessments: Neuropsy-chiatric Inventory Questionnaire (Kaufer et al.,2000); the Australian version of the Addenbrooke’sCognitive Examination – Revised (ACE-R) (Mioshiet al., 2006), which incorporates the Mini-MentalState Examination (MMSE); the short form ofthe Geriatric Depression Survey (Yesavage andSheikh, 1986); the Frontal Assessment Battery(Dubois et al., 2000); the short form of theInformer Questionnaire on Cognitive Decline inthe Elderly (Jorm, 1994); and Frontal BehaviouralInventory (Kertesz et al., 1997). The instrumentswere selected on advice from an old age psychiatristand a neuropsychologist, based on a combination ofthe instruments’ ability to be useful in diagnosis andin research. The researchers do not suggest that thefull assessment battery is required within memoryclinics. However, its use provided more data forcomparison and assisted the NP to refine her ownassessment skills and determine which tools aremost informative to her personally in the diagnosticprocess.
AnalysisResearchers extracted data from visit summaryreports and entered it into SPSS version 19.0.0.1 foranalyses. The data were arranged in the followingcategories: (1) patient background characteristics;(2) medical history; (3) lifestyle factors; and(4) assessments. Simple descriptive statistics werecalculated across participant groups in this study todescribe demographics, assessments, and diagnosis.Missing data were low (and more likely due to thedifficulties of clinical history taking than biases onthe part of the NP who collected the data). In casen � 106, valid percentage was used. Comparisonswere made with similar studies, but as the studiesvaried considerably, no quantitative analysis wasundertaken to describe these differences.
Comparison studiesSix studies, described in seven papers providedsuitable comparisons with this data. Studies wereselected based on the publication of similar datacategories for comparison (e.g. demographics,assessment scores, and diagnostic profiles), ideallyin the assessment of memory clinics or services.The comparison studies were held in Australiaand the United Kingdom, where assessments wereeither clinic- or home-based. In only one case was
a nurse solely responsible for diagnosis, and thiswas limited to an initial diagnosis which was laterassessed by the clinic’s MDT (Page et al., 2008). Allcomparison study memory clinics or services reliedmostly on referrals from medical professionals. Onestudy across two papers provided normative data ofindividuals previously diagnosed with either MCI ordementia (Ellis et al., 2009; Sona et al., 2012). Whilecomparison groups are useful, research cohorts maynot be a representative of dementia service users.
Results
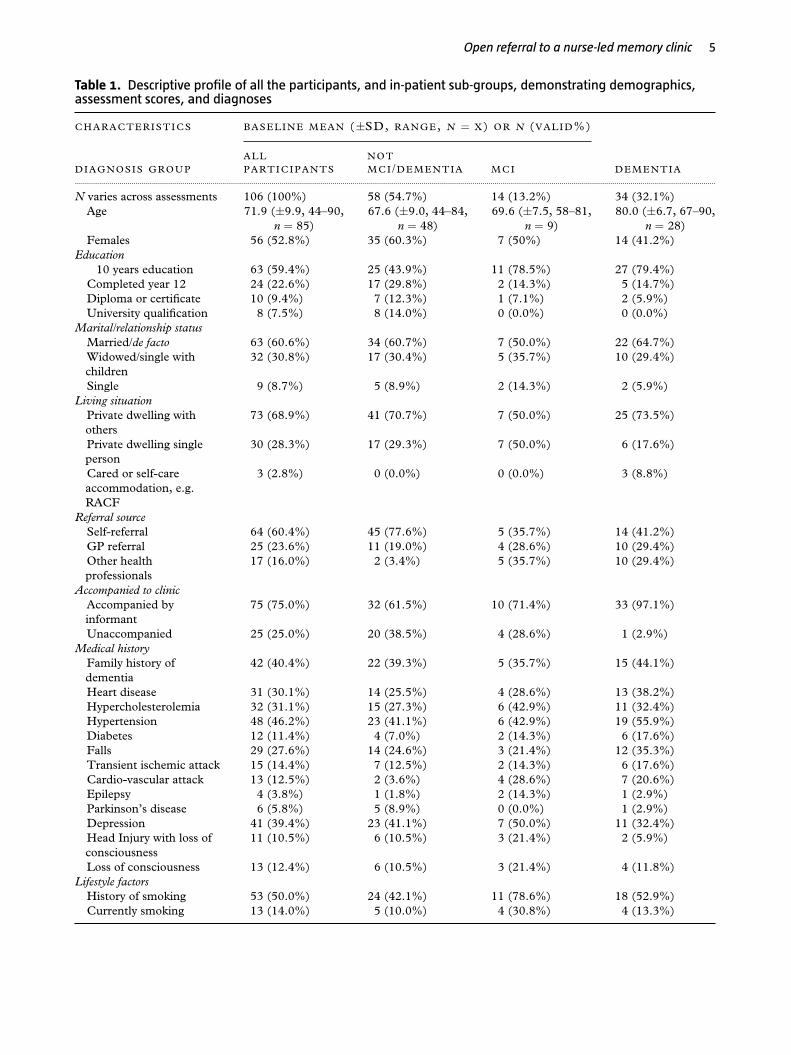
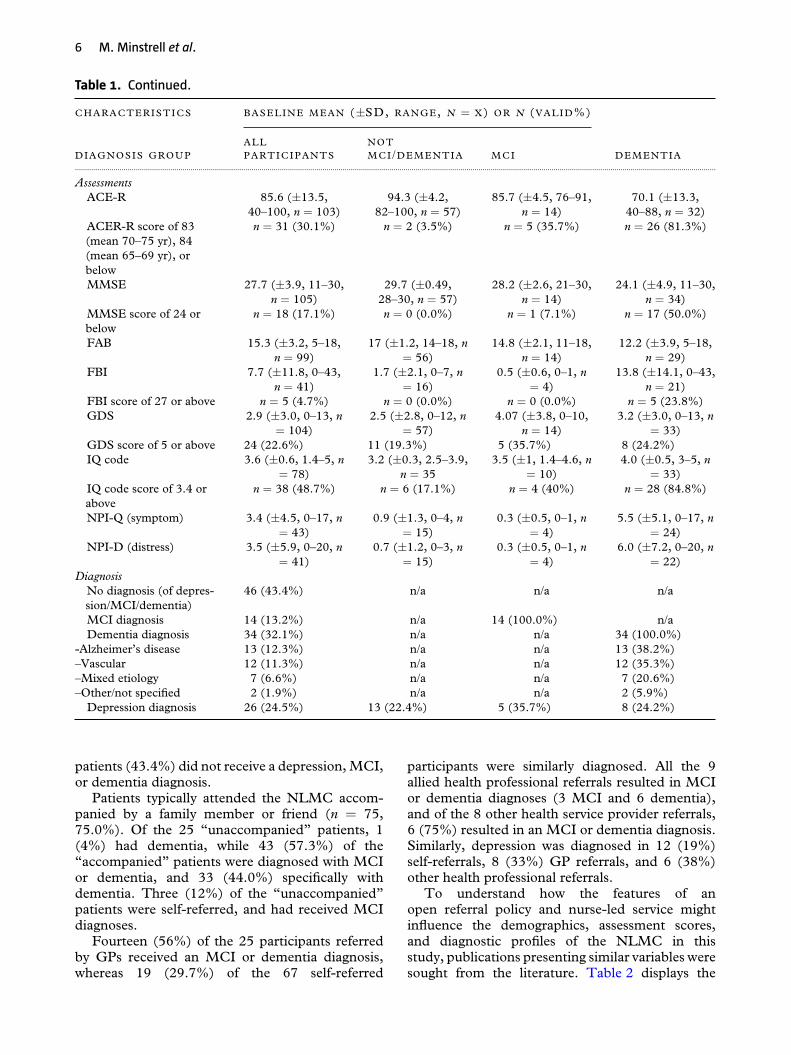
Table 1 presents the demographics, assessmentscores, and diagnostic profiles of 106 participantsin this study. Participants had a mean age of71.9 years (±9.9, 44–90, n = 85), 87 participants(82.0%) had 12 or less years of education, 63 parti-cipants (60.6%) were in a married or de factorelationship, and 56 (52.8%) were women.Medical histories of patients most commonlyincluded hypertension (46.2%), family historyof dementia (40.4%), depression (39.4%), andhypercholesterolemia (31.1%). Fifty-three patients(50%) had a history of smoking, and 30 (28.3%)lived alone in a private dwelling. Patients mostlyself-referred (60.4%) to the NLMC, but referralswere also received from GPs (23.6%) and otherhealth professionals (16.0%), including specialistsand allied health professionals. Mean ACE-R scorewas 85.60 (±13.5, 40–100, n = 103) out of 100for all patients, while mean MMSE score was27.69 (±3.9, 11–30, n = 105) out of 30. MeanACE-R and MMSE scores were lower for patientsdiagnosed with MCI and dementia. Twenty-fourpatients (22.6%) scored 5 or more on GeriatricDepression Scale (GDS).
Sixty participants (56.6%) received a diagnosisfrom the NLMC; 47 (44.3%) with MCI ordementia, and a further 13 (22.4%) were diagnosedwith depression without cognitive impairment.(Twenty-four (92%) of the 26 patients diagnosedwith depression had a GDS score of greaterthan or equal to 5.) Of note, nine of the13 diagnosed with depression without cognitiveimpairment were self-referred (69%). Fourteenpatients (13.2%) received an MCI diagnosis and 34(32.1%) received a dementia diagnosis. Of the 34patients diagnosed with dementia, 12 (35.3%) werediagnosed with vascular dementia, and 13 (38.2%)with Alzheimer’s disease. The NP did not identifyclients presenting with diagnostic criteria suggestiveof fronto-temporal dementia, Lewy Body Disease,or other less common dementia types during thestudy period. Overall, 26 patients (24.5%) werediagnosed with depression. Less than half of the
Open referral to a nurse-led memory clinic 5
Table 1. Descriptive profile of all the participants, and in-patient sub-groups, demonstrating demographics,assessment scores, and diagnoses
C H A R A C T E R I S T I C S BA S E L I N E M E A N (±SD, RANGE, N = X) OR N (V A L I D%)
DIAGNOSIS GROUPA L LP A R T I C I P A N T S
NOTMCI/D E M E N T I A M C I DE M E N T I A
............................................................................................................................................................................................................................................................................................................................
N varies across assessments 106 (100%) 58 (54.7%) 14 (13.2%) 34 (32.1%)Age 71.9 (±9.9, 44–90,
n = 85)67.6 (±9.0, 44–84,
n = 48)69.6 (±7.5, 58–81,
n = 9)80.0 (±6.7, 67–90,
n = 28)Females 56 (52.8%) 35 (60.3%) 7 (50%) 14 (41.2%)
Education�10 years education 63 (59.4%) 25 (43.9%) 11 (78.5%) 27 (79.4%)Completed year 12 24 (22.6%) 17 (29.8%) 2 (14.3%) 5 (14.7%)Diploma or certificate 10 (9.4%) 7 (12.3%) 1 (7.1%) 2 (5.9%)University qualification 8 (7.5%) 8 (14.0%) 0 (0.0%) 0 (0.0%)
Marital/relationship statusMarried/de facto 63 (60.6%) 34 (60.7%) 7 (50.0%) 22 (64.7%)Widowed/single withchildren
32 (30.8%) 17 (30.4%) 5 (35.7%) 10 (29.4%)
Single 9 (8.7%) 5 (8.9%) 2 (14.3%) 2 (5.9%)Living situation
Private dwelling withothers
73 (68.9%) 41 (70.7%) 7 (50.0%) 25 (73.5%)
Private dwelling singleperson
30 (28.3%) 17 (29.3%) 7 (50.0%) 6 (17.6%)
Cared or self-careaccommodation, e.g.RACF
3 (2.8%) 0 (0.0%) 0 (0.0%) 3 (8.8%)
Referral sourceSelf-referral 64 (60.4%) 45 (77.6%) 5 (35.7%) 14 (41.2%)GP referral 25 (23.6%) 11 (19.0%) 4 (28.6%) 10 (29.4%)Other healthprofessionals
17 (16.0%) 2 (3.4%) 5 (35.7%) 10 (29.4%)
Accompanied to clinicAccompanied byinformant
75 (75.0%) 32 (61.5%) 10 (71.4%) 33 (97.1%)
Unaccompanied 25 (25.0%) 20 (38.5%) 4 (28.6%) 1 (2.9%)Medical history
Family history ofdementia
42 (40.4%) 22 (39.3%) 5 (35.7%) 15 (44.1%)
Heart disease 31 (30.1%) 14 (25.5%) 4 (28.6%) 13 (38.2%)Hypercholesterolemia 32 (31.1%) 15 (27.3%) 6 (42.9%) 11 (32.4%)Hypertension 48 (46.2%) 23 (41.1%) 6 (42.9%) 19 (55.9%)Diabetes 12 (11.4%) 4 (7.0%) 2 (14.3%) 6 (17.6%)Falls 29 (27.6%) 14 (24.6%) 3 (21.4%) 12 (35.3%)Transient ischemic attack 15 (14.4%) 7 (12.5%) 2 (14.3%) 6 (17.6%)Cardio-vascular attack 13 (12.5%) 2 (3.6%) 4 (28.6%) 7 (20.6%)Epilepsy 4 (3.8%) 1 (1.8%) 2 (14.3%) 1 (2.9%)Parkinson’s disease 6 (5.8%) 5 (8.9%) 0 (0.0%) 1 (2.9%)Depression 41 (39.4%) 23 (41.1%) 7 (50.0%) 11 (32.4%)Head Injury with loss ofconsciousness
11 (10.5%) 6 (10.5%) 3 (21.4%) 2 (5.9%)
Loss of consciousness 13 (12.4%) 6 (10.5%) 3 (21.4%) 4 (11.8%)Lifestyle factors
History of smoking 53 (50.0%) 24 (42.1%) 11 (78.6%) 18 (52.9%)Currently smoking 13 (14.0%) 5 (10.0%) 4 (30.8%) 4 (13.3%)
6 M. Minstrell et al.
Table 1. Continued.
C H A R A C T E R I S T I C S BA S E L I N E M E A N (±SD, RANGE, N = X) OR N (V A L I D%)
DIAGNOSIS GROUPA L LP A R T I C I P A N T S
NOTMCI/D E M E N T I A M C I DE M E N T I A
............................................................................................................................................................................................................................................................................................................................
AssessmentsACE-R 85.6 (±13.5,
40–100, n = 103)94.3 (±4.2,
82–100, n = 57)85.7 (±4.5, 76–91,
n = 14)70.1 (±13.3,
40–88, n = 32)ACER-R score of 83(mean 70–75 yr), 84(mean 65–69 yr), orbelow
n = 31 (30.1%) n = 2 (3.5%) n = 5 (35.7%) n = 26 (81.3%)
MMSE 27.7 (±3.9, 11–30,n = 105)
29.7 (±0.49,28–30, n = 57)
28.2 (±2.6, 21–30,n = 14)
24.1 (±4.9, 11–30,n = 34)
MMSE score of 24 orbelow
n = 18 (17.1%) n = 0 (0.0%) n = 1 (7.1%) n = 17 (50.0%)
FAB 15.3 (±3.2, 5–18,n = 99)
17 (±1.2, 14–18, n= 56)
14.8 (±2.1, 11–18,n = 14)
12.2 (±3.9, 5–18,n = 29)
FBI 7.7 (±11.8, 0–43,n = 41)
1.7 (±2.1, 0–7, n= 16)
0.5 (±0.6, 0–1, n= 4)
13.8 (±14.1, 0–43,n = 21)
FBI score of 27 or above n = 5 (4.7%) n = 0 (0.0%) n = 0 (0.0%) n = 5 (23.8%)GDS 2.9 (±3.0, 0–13, n
= 104)2.5 (±2.8, 0–12, n
= 57)4.07 (±3.8, 0–10,
n = 14)3.2 (±3.0, 0–13, n
= 33)GDS score of 5 or above 24 (22.6%) 11 (19.3%) 5 (35.7%) 8 (24.2%)IQ code 3.6 (±0.6, 1.4–5, n
= 78)3.2 (±0.3, 2.5–3.9,
n = 353.5 (±1, 1.4–4.6, n
= 10)4.0 (±0.5, 3–5, n
= 33)IQ code score of 3.4 orabove
n = 38 (48.7%) n = 6 (17.1%) n = 4 (40%) n = 28 (84.8%)
NPI-Q (symptom) 3.4 (±4.5, 0–17, n= 43)
0.9 (±1.3, 0–4, n= 15)
0.3 (±0.5, 0–1, n= 4)
5.5 (±5.1, 0–17, n= 24)
NPI-D (distress) 3.5 (±5.9, 0–20, n= 41)
0.7 (±1.2, 0–3, n= 15)
0.3 (±0.5, 0–1, n= 4)
6.0 (±7.2, 0–20, n= 22)
DiagnosisNo diagnosis (of depres-sion/MCI/dementia)
46 (43.4%) n/a n/a n/a
MCI diagnosis 14 (13.2%) n/a 14 (100.0%) n/aDementia diagnosis 34 (32.1%) n/a n/a 34 (100.0%)
-Alzheimer’s disease 13 (12.3%) n/a n/a 13 (38.2%)–Vascular 12 (11.3%) n/a n/a 12 (35.3%)–Mixed etiology 7 (6.6%) n/a n/a 7 (20.6%)–Other/not specified 2 (1.9%) n/a n/a 2 (5.9%)
Depression diagnosis 26 (24.5%) 13 (22.4%) 5 (35.7%) 8 (24.2%)
patients (43.4%) did not receive a depression, MCI,or dementia diagnosis.
Patients typically attended the NLMC accom-panied by a family member or friend (n = 75,75.0%). Of the 25 “unaccompanied” patients, 1(4%) had dementia, while 43 (57.3%) of the“accompanied” patients were diagnosed with MCIor dementia, and 33 (44.0%) specifically withdementia. Three (12%) of the “unaccompanied”patients were self-referred, and had received MCIdiagnoses.
Fourteen (56%) of the 25 participants referredby GPs received an MCI or dementia diagnosis,whereas 19 (29.7%) of the 67 self-referred
participants were similarly diagnosed. All the 9allied health professional referrals resulted in MCIor dementia diagnoses (3 MCI and 6 dementia),and of the 8 other health service provider referrals,6 (75%) resulted in an MCI or dementia diagnosis.Similarly, depression was diagnosed in 12 (19%)self-referrals, 8 (33%) GP referrals, and 6 (38%)other health professional referrals.
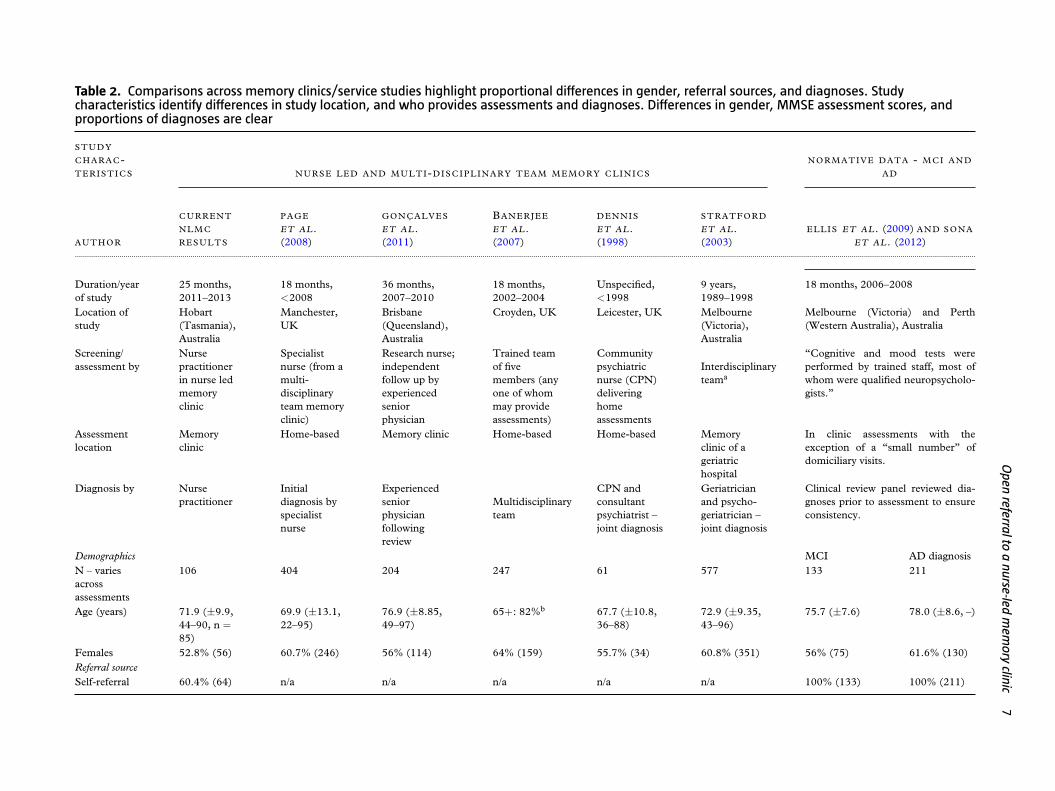
To understand how the features of anopen referral policy and nurse-led service mightinfluence the demographics, assessment scores,and diagnostic profiles of the NLMC in thisstudy, publications presenting similar variables weresought from the literature. Table 2 displays the
Open
referraltoa
nurse-ledm
emory
clinic7
Table 2. Comparisons across memory clinics/service studies highlight proportional differences in gender, referral sources, and diagnoses. Studycharacteristics identify differences in study location, and who provides assessments and diagnoses. Differences in gender, MMSE assessment scores, andproportions of diagnoses are clear
STUDY
C H A R A C-TERISTICS NURSE LED AND MULTI-DISCIPLINARY TEAM MEMORY CLINICS
NORMATIVE DATA - MCI A ND
A D
AUTHOR
CURRENT
NLMC
RESULTS
PAGE
ET AL.(2008)
GONÇALVES
ET AL.(2011)
BANERJEE
ET AL.(2007)
DENNIS
ET AL.(1998)
STRATFORD
ET AL.(2003)
ELLIS ET AL. (2009) AND SONA
ET AL. (2012)............................................................................................................................................................................................................................................................................................................................................................................................................................................................
Duration/yearof study
25 months,2011–2013
18 months,<2008
36 months,2007–2010
18 months,2002–2004
Unspecified,<1998
9 years,1989–1998
18 months, 2006–2008
Location ofstudy
Hobart(Tasmania),Australia
Manchester,UK
Brisbane(Queensland),Australia
Croyden, UK Leicester, UK Melbourne(Victoria),Australia
Melbourne (Victoria) and Perth(Western Australia), Australia
Screening/assessment by
Nursepractitionerin nurse ledmemoryclinic
Specialistnurse (from amulti-disciplinaryteam memoryclinic)
Research nurse;independentfollow up byexperiencedseniorphysician
Trained teamof fivemembers (anyone of whommay provideassessments)
Communitypsychiatricnurse (CPN)deliveringhomeassessments
Interdisciplinaryteama
“Cognitive and mood tests wereperformed by trained staff, most ofwhom were qualified neuropsycholo-gists.”
Assessmentlocation
Memoryclinic
Home-based Memory clinic Home-based Home-based Memoryclinic of ageriatrichospital
In clinic assessments with theexception of a “small number” ofdomiciliary visits.
Diagnosis by Nursepractitioner
Initialdiagnosis byspecialistnurse
Experiencedseniorphysicianfollowingreview
Multidisciplinaryteam
CPN andconsultantpsychiatrist –joint diagnosis
Geriatricianand psycho-geriatrician –joint diagnosis
Clinical review panel reviewed dia-gnoses prior to assessment to ensureconsistency.
Demographics MCI AD diagnosisN – variesacrossassessments
106 404 204 247 61 577 133 211
Age (years) 71.9 (±9.9,44–90, n =85)
69.9 (±13.1,22–95)
76.9 (±8.85,49–97)
65+: 82%b 67.7 (±10.8,36–88)
72.9 (±9.35,43–96)
75.7 (±7.6) 78.0 (±8.6, –)
Females 52.8% (56) 60.7% (246) 56% (114) 64% (159) 55.7% (34) 60.8% (351) 56% (75) 61.6% (130)Referral sourceSelf-referral 60.4% (64) n/a n/a n/a n/a n/a 100% (133) 100% (211)
8M
.Minstrelletal.
Table 2. Continued.
STUDY
C H A R A C-TERISTICS NURSE LED AND MULTI-DISCIPLINARY TEAM MEMORY CLINICS
NORMATIVE DATA - MCI A ND
A D
AUTHOR
CURRENT
NLMC
RESULTS
PAGE et al.(2008)
GONÇALVES
ET AL.(2011)
BANERJEE
ET AL.(2007)
DENNIS
ET AL.(1998)
STRATFORD
ET AL.(2003)
ELLIS ET AL. (2009) AND SONA
ET AL. (2012)............................................................................................................................................................................................................................................................................................................................................................................................................................................................
GP referral 23.6% (25) 100% (404) “mainly” (p.789)
100% (247) 82% (50) >80% n/a n/a
Other healthprofessionals
16.0% (17) n/a n/a 18% (11) not specified n/a n/a
AssessmentsMMSE 27.69 (±3.9,
11–30)25.31(±4.81)
22.28 (±5.33,4–30)c
22.5 (±5.7) 21 (±7.2,3–30)
19.8 (±6.1,0–30)
26.2 (±2.6, –) 19 (±5.2, –)
GDS 2.93 (±3.0,0–13)
3.71 (±3.53) 3.99 (±3.2,0–15)
3.4 (±3.2) (Notpublished)
n/a 2.0 (±1.8) 2.9 (±2.2)
DiagnosesNo depres-sion/MCI/dementiadiagnosis
43.4% (46) 8.5% (34)d 3% (6)e 30% (74) 15% (9) 4.9% (28)f n/a n/a
Depressiondiagnosis
25.0% (26) 13.9% (56) 5% (10)g Not specified 11.5% (7) 6.7% (39)h Not specified Not specified
MCIdiagnosis
13.2% (14) 35.4% (143)i 13% (27)j Excludedk Not specified Excludedl 100% (133) n/a
Dementiadiagnosism
32.1% (34) 42.3% (171) 75% (152) 64% (156) 60.6% (37) 64% (369) n/a 100% (211)
Notes: aThe team included a psychiatrist, geriatrician, social worker, nurse, occupational therapist, speech pathologist, and neuropsychologist.bAge data provided as age in parentheses.cStandardized Mini-Mental State Examination (SMMSE) administered rather than MMSE; however results are comparable.dCombined categories of “no problem identified” and “none of the above.”eSubjective memory complaints.fStratford et al. (2003) combine patients diagnosed as “normal” and with “functional psychiatric disorders,” which does not include those diagnosed with “organic cognitive impairment.”gIncludes anxiety.hCalculated by summing diagnosis categories “depressive episode (single)” and “recurrent depressive disorder.”iMCI or VCI.jMCI and cognitive impairment no dementia (CIND).kWhile similar data for these categories were published in these articles, these cases were excluded from comparison as they were not referred to as MCI and did not match our definition.lAs above.mWhere an overall dementia diagnosis figure has not been provided, sub-diagnoses (e.g. Alzheimer’s disease, vascular dementia and so forth) have been combined.
Open referral to a nurse-led memory clinic 9
published results of the studies most suitable forcomparison with this study’s results.
The participants in this study were generallysimilar to those of other memory clinic studies;however, this study had a smaller proportion offemale patients (52.8% as compared with a rangeof 56–64%). Patients in this study had lowereducation levels than a dementia research cohort,yet similar levels to another Australian memoryclinic study. Specifically, 87 (82%) patients had12 years or less of education in this study, ascompared with 79% within another Australianstudy (Gonҫalves et al., 2011), and 59% ofthe Australian Imaging, Biomarkers and Lifestyle(AIBL) study’s dementia cohort (Sona et al., 2012).Gonҫalves et al. (2011) only presented data frommemory clinic attendees who were accompanied byan informant, and reported finding a correlationbetween accompanied attendees and an increasedlikelihood of cognitive impairment diagnosis.
Medical histories of patients varied as well.Specifically, the participants of this study hadrelatively high proportions of falls in their medicalhistory, and a history of depression was similarand/or more common than other reports. A historyof falls was reported by 29 (27.6%) of the NLMCparticipants as compared with 15% within anotherservice (Page et al., 2008). A medical history ofdepression was reported for 41 (39.4%) patientsin this study as compared with 39.9% from theother nurse-based clinic (Page et al., 2008), and23.3% and 27% of AIBL’s MCI and AD cohortsrespectively.
Referral sources were strikingly different fromother memory clinics. Over 80% of the referralswere from GPs in other memory clinic studies,whereas the NLMC had 25 (23.6%) GPreferrals. Similarly, Australian memory clinicsreportedly received the majority of referrals frommedical professionals and/or services: GPs (59%),other external doctors (16%), affiliated services(13%), and self-referrals (12%) (Woodward andWoodward, 2009).
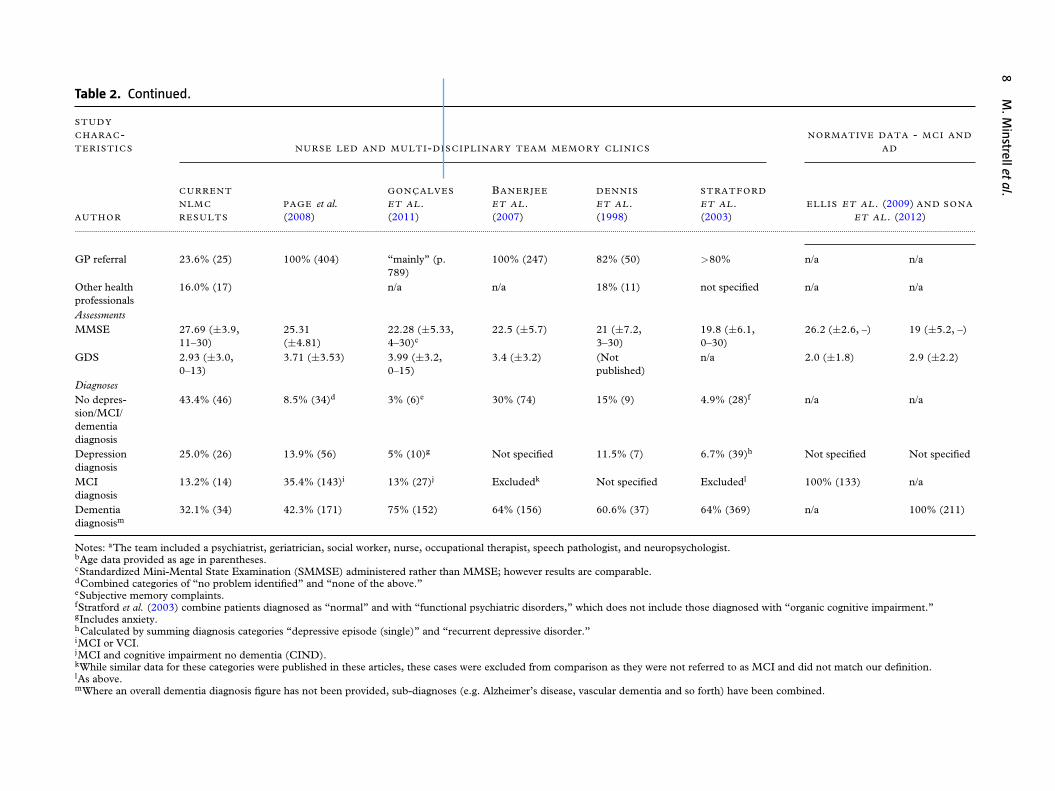
This study reported proportionally fewerdementia diagnoses than previous studies. Whileother studies demonstrated 61 to 75% of patientsbeing diagnosed with dementia (Dennis et al.,1998; Stratford et al., 2003; Banerjee et al., 2007;Gonҫalves et al., 2011), our study identified only34 patients (32.1%) with dementia, although theproportion of dementia diagnosis from healthprofessional referrals was higher (47.6%). The mostsimilar proportions were reported by Page et al.(2008), who reported 42% of the cases receivingdementia diagnosis, while a typical Australianmemory clinic profile was calculated to be 48%(Woodward and Woodward, 2009).
This study had a similar proportion of MCIdiagnosis as Gonҫalves et al. (2011), yet both hadsmaller proportions than Page et al. (2008; 13.2%and 13% as compared with 35.4%). A typicalAustralian memory clinic profile was calculated tobe 20% (Woodward and Woodward, 2009). Thisstudy had the highest proportion of patients whodid not receive a diagnosis of depression, MCI,or dementia (43.4%), with one study reporting30% (Banerjee et al., 2007) and the remainingreporting 15% or less. Yet, NLMC participantsexpressed less depression symptoms – as per theirGDS scores (2.93 compared with 3.4–3.99) – thanother memory clinic studies (Banerjee et al., 2007;Page et al., 2008; Gonҫalves et al., 2011).
NLMC patients diagnosed with MCI (n =14) received relatively high MMSE scores. Uponreviewing these cases, the NP reported determiningan MCI diagnosis through a fuller picture for eachpatient rather than relying on any one assessmentscore. This review demonstrated the importance offactors other than screening tests (mainly detailedcorroborative history and integrating results frompatient presentation at interview and physical exam)in arriving at a cognitive impairment diagnosis.
In comparison to the AIBL study cohorts,participants diagnosed with dementia and MCI inthis study had higher MMSE scores. Specifically,those diagnosed with MCI and dementia in thisstudy had MMSE scores of 28.2 (±2.6) and 24.1(±4.9) as compared with those in the AIBL study26.2 (±2.6) and 19 (±5.2) (Ellis et al., 2009; Sonaet al., 2012).
Discussion
The results discussed here are descriptive patterns,and not significant statistically. The relativelylow sample size needs to be acknowledgedwhen interpreting these results. Other studylimitations include the naturalistic setting, thelimited published data available for comparison,and the inclusion of two distinct but relatedprocesses (i.e. nurse-led and open referral policy)makes it difficult to clarify the contribution ofeach process toward the outcomes identified. Thedifferent demographics, assessment scores, anddiagnostic profiles of patients from the NLMCwhen compared with more traditional memoryclinics may however warrant further study asdementia prevalence increases. The differencesmay have resulted from the open referral policyand/or having an NP conduct both assessmentsand diagnoses; and some possible reasons for thesedifferences are discussed below.

10 M. Minstrell et al.
The male–female split in this study’s patientbase reflects the expected proportion of dementiaprevalence for participant’s age (Prince, 2008),but the proportion of males was higher comparedwith most other reported studies. Being malehas been linked with limited health literacy andassociated with decreased healthcare access (Sudoreet al., 2006). While men’s adherence to traditionalmasculinity may deter their health seeking behaviormore broadly, it is possible that the NP’s perceiveddiminished position of power was less threateningto men (Boman and Walker, 2010). Thus, theNP clinic model may provide a more acceptableassessment entry point for men than traditionalmedical and clinic services.
Low education levels have also been linked todiminished healthcare access, even in countriesproviding universal care (Adler and Newman, 2002;Sudore et al., 2006); thus, the low education levelsof NLMC participants in this study is of interest.Previous research has demonstrated that individualswith less education and income use fewer specialistservices (Adler and Newman, 2002); therefore thenon-specialist environment of the NLMC in thisstudy and the research nurse in the Gonҫalves et al.(2011) study may have been more acceptable and/oraccessible to them. It may be that those with lowereducation levels felt more comfortable visiting anurse for assessment rather than a doctor, specialist,or MDT.
The nurse-led feature of this memory clinicmight have also influenced patient’s attendancemore broadly. Informal feedback from the NPsuggests that patients were more comfortablebringing subtle issues to an NP earlier than toa doctor (e.g. “not enough changes to bother adoctor”). This fits with a growing body of literaturethat shows patients’ comfort in communicating withnurses compared with doctors (Williams and Jones,2006).
This study highlights the importance ofpublishing fuller data sets for others to makecomparisons, as it was difficult to locate fullpublished data sets. Unfortunately, this meant thatone of the few means of comparison was screeningassessment scores, which are only part of thediagnostic picture. The most commonly availableassessment scores for comparison were the MMSEand GDS, which fit with Woodard and Woodward’s(2009) finding that the MMSE and clock drawingare the most common assessment tools used inAustralian memory clinics.
However, while the MMSE may be commonas it is accessible and easy to administer, itsreliability has been questioned, as patients withpresentations and clinical histories indicative ofdementia may still score highly (Terpening et al.,
2011) as did our study participants. Our studyparticipants may have had higher MMSE scoresbecause patients with early symptoms were able toreceive a timely and full assessment as a result ofself-referral. Higher MMSE scores for self-referredpatients compared with GP-referred patients werefound in another memory clinic study (Barker et al.,1994), while the majority of patients from anothernurse-led self-referral service were diagnosed withmild to moderate cognitive impairment (Scottand Donnelly, 2005). The open referral policy ofthis NLMC likely meant that its patients gainedentrance when they may have experienced delayedaccess elsewhere due to poor physician recognitionskill as noted by Mitchell et al. (2011).
Self-referral may have also been the reason whylower percentage of dementia diagnosis was foundin this study. While the NP-screened referrals toensure potential patients were genuinely concernedabout memory changes, many ultimately hadsubjective memory concerns. However, there wasoften a family history of dementia, and patientswere genuinely worried and needed reassurance.For example, one GP referred two patients whoneeded confirmation that they were aging normally.The NLMC provided an avenue for patient’sconcerns being addressed when GPs were unable toprovide this service or expertise, or when patientsrequired further reassurance as was the case withthese patients. In addition, the NLMC playeda role in promoting brain health, and providinginformation on how to minimize risk factors fordeveloping dementia. A follow-up study of patientsattending this clinic revealed that some attendedto benchmark their own aging as compared withthe rest of society (Stirling et al., 2013), thus itis intuitive that self-referred patients would havea lower dementia incidence than those referredby health professionals. Patients referred by healthprofessionals are likely to have been experiencingsymptoms and/or seeking diagnosis for longer, andlikely to typically have more pronounced symptoms.It is also possible that a proportion of those whowere described as normal may have had a differentoutcome if they underwent a fuller diagnosticassessment commonly utilized in more traditionalmemory clinics.
The lower proportion of dementia diagnosiscould also be partly because some spouses undergoassessment themselves in order to encourage theirpartner. The NP was aware of at least three patientsattending the NLMC in an effort to encouragespouse with a cognitive impairment concern toattend as well. Therefore, a small proportion ofparticipants attended with a concern about theirpartner’s cognition. Although this can be construedas a downfall, it can also be viewed as an evidence

Open referral to a nurse-led memory clinic 11
that an open referral policy within an accessiblenon-threatening diagnostic service may providean important avenue to overcome some of thechallenges to diagnosis, i.e. partners and familymembers experiencing difficulty broaching theirconcerns with – and/or prompting assessmentsof – individuals they suspect may have cognitiveimpairment and/or dementia.
The NLMC also diagnosed depression withinthis study, both with and without MCI or dementia.The number of self-referred patients diagnosed withdepression without cognitive impairment suggeststhat the NLMC model can help to identifydepression in the wider community.
As over half of the patients were not diagnosedwith dementia, MCI, or depression, this doesraise the question of whether this memory clinicformat is viable or worthwhile. Such a decisionmay require a value judgment and economicanalysis. In the case of the NLMC, the financialoutlay for services was relatively low (requiringan NP, room, and administrative staff to bookappointments), with the NP assessing two patientsand following up with one patient on an averageday. Even when staffing costs are lower thantraditional memory clinics, there are considerablecost implications of having a lower percentageof attendees diagnosed with dementia. However,this type of memory clinic can increase accessto the diagnostic process to assist in managingthe ever increasing need for dementia assessment.Furthermore, patients without diagnosis are lessresource-intensive (e.g. one visit as comparedwith two visits), and NLMC attendance providesopportunities for health promotion, learning aboutaging, and reassurance. Future studies comparingthe dementia diagnostic rate in an NLMC with GP-only referrals could be informative. Further researchcould also identify the impact and cost-effectivenessof the clinic across the spectrum of services andpatient experiences (including depression). Thebenefits of early diagnosis may offset the costsassociated with assessing individuals without MCIor dementia (Getsios, 2012).
Overall, this study suggests that an open referralpolicy may lower diagnostic barriers for males, andthose with lower levels of education, potentiallyreaching those from lower socioeconomic groups(although the data were not collected). It mayalso be possible that the nurse-led feature ofthis memory clinic diminished patient-drivenbarriers to accessing diagnosis. A further possiblebenefit of open referral is that it allows earlieridentification of MCI. National dementia strategiesof high-income countries consistently identify earlydiagnosis and intervention as key policy priorities
(Prince et al., 2011). This outcome needs to becarefully considered by policy makers as there isdisagreement over what an MCI diagnosis implies,as conversion rates to dementia are still tentative.Notwithstanding this, MCI diagnoses may beparticularly relevant to future care when improvedprediction of conversion from MCI to dementia isfound through potential future use of biomarkers,for example.
In conclusion, this study found that differingmemory clinic features – specifically an openreferral policy and being nurse-led – although notsignificantly associated with patient profiles, diddemonstrate some unusual patterns that suggestthese features may facilitate diagnoses of MCI anddementia.
The authors recommend that the future researchinvestigates and publishes more patient data(e.g. referral source), as this information canhelp others to understand the type of patientsand services that are described as well asproviding data for comparison. In addition, futurestudies should assess whether NLMCs are indeedeffective. While the present evidence points to theeffectiveness of nurses to diagnose dementia, furtherresearch could build the evidence and increaseconfidence in NLMCs, specifically if NP’s cognitiveimpairment diagnoses are consistent with those ofspecialists, who have been diagnosing dementiamore traditionally.
Conflict of interest
None.
Description of authors’ roles
Christine Stirling led the chief investigators indesigning the study, obtaining funding, overseeingthe data analysis, and paper writing. Chiefinvestigators Martin Morrissey, Hazel Bucher,and Andrew Robinson assisted in designingthe study and obtaining funding, and providedcritical feedback on the paper. Hazel Bucheralso implemented the assessment procedures andcollected the data. Carl Higgs inputted and analyzedthe data, and assisted in writing the paper. MichaelBentley imputed data and provided critical feedbackon the paper. Melinda Minstrell analyzed the data,and took the lead on writing this paper through thepresentation of data and ideas. All authors assistedin revising the paper.

12 M. Minstrell et al.
Acknowledgments
The authors gratefully acknowledge The MasonFoundation – Judith Jane Mason and Harold Stan-nett Williams Memorial Foundation, administeredby ANZ Trustees for their grant supporting theNLMC research. From July 2011, the clinic wasfunded by a project grant from the CommonwealthDepartment of Health and Ageing. This is anAustralian Government initiative trialing agedcare nurse practitioner models. These sequentialsources of funding were supplemented throughoutby in-kind contributions from the TasmanianDepartment of Health and Human Services in theway of professional supervision for the NP. Theauthors also sincerely thank the NLMC patients andtheir families for participating, and the reviewersand editorial teams for their constructive feedback.
References
Adler, N. E. and Newman, K. (2002). Socio-economicdisparities in health: pathways and policies. Health Affairs,21, 60–76.
Banerjee, S., Willis, R., Matthews, D., Contell, F.,Chan, J. and Murray, J. (2007). Improving the quality ofcare for mild to moderate dementia: an evaluation of theCroydon Memory Service Model. International Journal ofGeriatric Psychiatry, 22, 782–788.
Barker, A., Carter, C. and Jones, R. (1994). Memoryperformance, self-reported memory loss and depressivesymptoms in attenders at a GP-referral and a self-referralmemory clinic. International Journal of Geriatric Psychiatry,9, 305–311.
Bentley, M., Minstrell, M., Bucher, H., Morrissey, M.,Robinson, A. and Stirling, C. (2014). A case studyevaluation protocol to assess processes, effectiveness andimpact of a nurse practitioner-led memory clinic. Health, 6,748–756.
Boman, E. K. O. and Walker, G. A. (2010). Predictors ofmen’s health care utilization. Psychology of Men &Masculinity, 11, 113–122.
Burns, A. and Iliffe, S. (2009). Dementia. British MedicalJournal, 338, 467–471.
Dennis, M., Furness, L., Lindesay, J. and Wright, N.(1998). Assessment of patients with memory problemsusing a nurse-administered instrument to detect earlydementia and dementia subtypes. International Journal ofGeriatric Psychiatry, 13, 405–409.
Draškovic, I., Vernooij-Dassen, M., Verhey, F.,Scheltens, P. and Rikkert, M. O. (2008). Developmentof quality indicators for memory clinics. InternationalJournal of Geriatric Psychiatry, 23, 119–128.
Dubois, B., Slachevsky, A., Litvan, I. and Pillon, B.(2000). The FAB: a frontal assessment battery at bedside.Neurology, 55, 1621–1626.
Ellis, K. A. et al. (2009). The Australian Imaging,Biomarkers and Lifestyle (AIBL) study of aging:methodology and baseline characteristics of 1112
individuals recruited for a longitudinal study of Alzheimer’sdisease. International Psychogeriatrics, 21, 672–687.
Gardner, G., Carryer, J., Dunn, S. and Gardner, A.(2004). Nurse Practitioner Standards Project. Report toAustralian Nursing and Midwifery Council, PositionStatement on Advanced Nursing Practice. Brisbane,Australia: Royal College of Nursing (RCNA).
Getsios, D. (2012). An economic evaluation of earlyassessment for Alzheimer’s disease in the United Kingdom.Alzheimer’s & Dementia, 8, 22–30.
Gladman, J. R. F., Jones, R. G., Radford, K., Walker, E.and Rothera, I. (2007). Person-centred dementia servicesare feasible, but can they be sustained? Age and Ageing, 36,171–176.
Gonҫalves, D., Arnold, E., Appadurai, K. and Byrne,G. J. (2011). Case finding in dementia: comparative utilityof three brief instrumentss in the memory clinic setting.International Psychogeriatrics, 23, 788–796.
Hansen, E., Robinson, A., Mudge, P. and Crack, G.(2005). Barriers to the provision of care for people withdementia and their carers in a rural community. AustralianJournal of Primary Health, 11, 72–79.
Hatchett, R. (2008). Nurse-led clinics: 10 essential steps tosetting up a service. Nursing Times, 104, 62–64.
Jolley, D., Benbow, S. M. and Grizzell, M. (2006).Memory clinics. Postgraduate Medical Journal, 82,199–206.
Jorm, A. F. (1994). A short form of the InformantQuestionnaire on Cognitive Decline in the Elderly(IQCODE): development and cross-validation.Psychological Medicine, 24, 145–153.
Kaufer, D. I. et al. (2000). Validation of the NPI-Q, a briefclinical form of the neuropsychiatric inventory. Journal ofNeuropsychiatry and Clinical Neurosciences, 12, 233–239.
Kertesz, A., Davidson, W. and Fox, H. (1997). Frontalbehavioral inventory: diagnostic criteria for frontal lobedementia. Canadian Journal of Neurological Sciences, 24,29–36.
Millard, F. B., Kennedy, R. L. and Baune, B. T. (2011).Dementia: opportunities for risk reduction and earlydetection in general practice. Australian Journal of PrimaryHealth, 17, 89–94.
Mioshi, E., Dawson, K., Mitchell, J., Arnold, R. andHodges, J. R. (2006). The Addenbrooke’s CognitiveExamination Revised (ACE-R): a brief cognitive testbattery for dementia screening. International Journal ofGeriatric Psychiatry, 21, 1078–1085.
Mitchell, A. J., Meader, N. and Pentzek, M. (2011).Clinical recognition of dementia and cognitive impairmentin primary care: a meta-analysis of physician accuracy. ActaPsychiatrica Scandinavica, 124, 165–183.
Mullins, J. and Fitch, F. (2000). Diagnosis by request: aself-referral memory clinic. Journal of Dementia Care, 8,30–31.
Page, S., Hope, K., Bee, P. and Burns, A. (2008). Nursesmaking a diagnosis of dementia – a potential change inpractice? International Journal of Geriatric Psychiatry, 23,27–33.
Prince, M. (2008). The Prevalence of Dementia Worldwide.Alzheimer’s Disease International Factsheet. London:Alzheimer’s Disease International.

Open referral to a nurse-led memory clinic 13
Prince, P. M., Bryce, D. R. and Ferri, D. C. (2011).World Alzheimer Report 2011: The Benefits of Early Diagnosisand Intervention. London: Institute of Psychiatry, King’sCollege.
Robinson, A., Elder, J., Emden, C., Lea, E., Turner, P.and Vickers, J. (2009). Information pathways intodementia care services. Dementia, 8, 17–37.
Scott, D. and Donnelly, M. (2005). The early identificationof cognitive impairment. Dementia, 4, 207–232.
Seymour, J., Saunders, P., Wattis, J. P. and Daly, L.(1994). Evaluation of early dementia by a trained nurse.International Journal of Geriatric Psychiatry, 9, 37–42.
Sona, A. et al. (2012). Predictors of rapid cognitive decline inAlzheimer’s disease: results from the Australian Imaging,Biomarkers and Lifestyle (AIBL) study of ageing.International Psychogeriatrics, 24, 197–204.
Stirling, C., Campbell, B., Bentley, M., Bucher, H. andMorrissey, M. (2013). A qualitative study of patients’experiences of a nurse-led memory clinic. Dementia.Epublished ahead of print, doi:10.1177/1471301213512841
Stratford, J. A., LoGiudice, D., Flicker, L., Cook, R.,Waltrowicz, W. and Ames, D. (2003). A memory clinicat a geriatric hospital: a report of 577 patients assessed with
the CAMDEX over 9 years. Australian & New ZealandJournal of Psychiatry, 37, 319–326.
Sudore, R. L. et al. (2006). Limited literacy in older peopleand disparities in health and healthcare access. Journal ofthe American Geriatrics Society, 54, 770–776.
Terpening, Z., Cordato, N. J., Hepner, I. J., Lucas, S. K.and Lindley, R. I. (2011). Utility of the Addenbrooke’sCognitive Examination – Revised for the diagnosis ofdementia syndromes. Australasian Journal on Ageing, 30,113–118.
Turner, S. et al. (2004). General practitioners’ knowledge,confidence and attitudes in the diagnosis and managementof dementia. Age and Ageing, 33, 461–467.
van den Dungen, P. et al. (2012). The accuracy of familyphysicians’ dementia diagnoses at different stages ofdementia: a systematic review. International Journal ofGeriatric Psychiatry, 27, 342–354.
Williams, A. and Jones, M. (2006). Patients’ assessments ofconsulting a nurse practitioner: the time factor. Journal ofAdvanced Nursing, 53, 188–195.
Woodward, M. C. and Woodward, E. (2009). A nationalsurvey of memory clinics in Australia. InternationalPsychogeriatrics, 21, 696–702.
Yesavage, J. A. and Sheikh, J. I. (1986). GeriatricDepression Scale (GDS): recent evidence and developmentof a shorter version. Clinical Gerontologist, 5, 165–173.
Related Documents










