Open Fractures Dr. KB LEE Department of O&T Queen Elizabeth Hospital AADO

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Open Fractures
Dr. KB LEEDepartment of O&T
Queen Elizabeth HospitalAADO

Introduction
Management of open fractureClinical casesSummary

Management of Open Fracture

Open Fracture
Fracture communicates through a traumatic wound to surrounding environment Resulting in contamination & soft tissue envelope disruption

Open Fracture
A big wound not communicating with fracture ≠ open fractureEven a small wound communicating withfracture ≡ open fracture (compound fracture)
Open Fracture
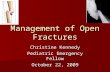
High energyOutcome depends extent of soft tissue injuryTreatment of soft tissue trauma with contamination Primarily importantTreatment of skeletal injury Secondary

Gustilo Classification (1976, 1984)
III
III
< 1cm Clean wound, minimal comminution> 1cm Mod. contamination / Moderate comminution> 10cm High contamination / Soft tissue damage(Including all segmental #, farmyard injuries, # in
contaminated environment, gunshot)
a
b
c
Soft tissue crushed / flapped / lacerated, comminuted #, adequate coverageExtensive soft tissue injury, periosteal stripping, exposure of bone, inadequate coverageV. severe loss of coverage, vascular injury

Gustilo Classification: Typing Pitfalls
Problem of inter-observer varianceTyping can only be attempted after initial debridement and irrigation Typing often Up-graded subsequently when flaps necrosed, or skin graft failed - requiring local or free flaps - Grade IIIB.
Does Typing reliably guide treatment??Can Typing guide prognosis??

Classification: Gustilo & Anderson
5-50High energy>10III
2-5Moderate energy1-10II
0-2Low energy<1I
Infection rate (%)
Energy of trauma(Soft tissue crush & fracture comminution)
Size(cm)
Type

Classification:Gustilo & Anderson
4225-50Repairable vascular injury
IIIC
1610-50Periosteal stripping, wound coverage required
IIIB
05-10Adequate soft tissue coverage
IIIA
Amputation rate (%)
Infection rate (%)
DescriptionSubclass
Type III Open Fracture
It is not “a fracture with a wound”It is “a wound resulting from high energy trauma, complicated with a Fracture”First priority is to deal with the Wound,and then minimize complications arising from the fracture.

Objectives of Open Fracture Mx
Prevent infectionPromote fracture healingRestore function

Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery

ATLS:Save the Life First
Resuscitation: ABC

ATLS:Then Save the Limb
Recognize & treat the limb threatening conditions
Traumatic amputation
Vascular insufficiency
Compartment syndrome

Limb Specific Management:Initial Management
Make detailed assessment & documentation, take clinical photoInitial cleansing if possibleSterile cover - do not open until in OTImmediate systemic antibioticsOT as soon as fasted enough for GA or regional anesthesia - It is an Emergency! (But 6-hr rule controversial) Analyze needs, prioritize aims, plan, and plan for the worst
Take them seriously!

Assess and document wound location, size, contamination - photoDebridement and copious lavage (6 - 10 L.), discard loose fragments Preserve flaps - esp. where local flaps are not readily available: distal 1/3 of tibia and beyond.Stabilize fracture – Ext. Fix. or NailDo NOT close woundGreat demand on appropriate decision making and surgical proficiency - experienced surgical team makes a difference!
Limb Specific Management: First Operation “EOT”

Prevent Infection: Wound Debridement & Lavage
Remove all devitalized tissue, debis, loose fragments & foreign bodyNS / antiseptic irrigation:copious pulsatile lavage (6-10 L)+/- 2nd look debridement every 24-72 hrs until completely clean Wound left open & daily dressing
1st debridement 2nd debridement

Lavage
Wound irrigation is the key to prevent infectionDecrease bacterial load and remove foreign body“Copious”, PulsatileControversy: NS, antiseptic, antibiotic, soap

Prevent Infection:IV Antibiotics
Broad spectrum cephalosporin (Gm +ve & -ve)Zinacef
+/- Aminoglycoside (Gm - ve) Gentamicin
+/- Metronidazole (anaerobes)Flagyl
No optimal regimen!Depends onwound condition !!
≠

Prevent Infection:Local Antibiotics
Antibiotic loaded beads:1. High local concentration2. Temporary spacer

Prevent Infection:Tetanus Prophylaxis
As a routinePreviously immunized
toxoid boosterNot immunized
toxoid + immune globulin

Fracture Stabilization:Optimize Fracture Healing
Reasonable reductionStable fixationDynamize and weight bear at appropriate timeBone graftBring in blood supply
Fracture Stabilization:TemporarilyAim:1. maintain bony alignment & length2. reduction of dead space3. improve circulation & lymphatic drainage 4. facilitate wound care5. pain control

Fracture Stabilization:Temporarily
Standard: External FixationQuick & easyMinimal invasiveGood stabilityPrevent infection
Should leave room for wound care & future reconstruction
Temporarily stabilization

Ext Fix generally more forgiving, esp. for tibiaMore room for adjustments and revisionsTyping of open fracture not easy, a lot of inter-observer differences - Big trouble if under-typed and nailed Much quicker if proficient, but long learning curveMore prone to delayed and mal-union if Ext Fix used as definitive treatmentBut open femur # is safe with primary nailing
Fracture Stabilization:Temporary Ext. Fix. vs Nailing

Fracture Stabilization:Definite
Usually done after wound conditions ( infection & coverage ) stabilized Exchange to internal fixation(plate / IM nail) ORKeep external fixationTiming & method depends on fracture pattern & wound conditions

Conversion of Ext. Fix. to Reamed Nailing
Tibia - generally not later than one weekFor I, II and IIIA #’sOne stage or “cooling” periodBetter access for flap surgeryLess prone to delayed or mal-unionGenerally more acceptable to patientsShorter hospital stayOnly if fracture location and type amenable to nailing
IM Nail Conversionin Long Bone Fractures
When?Less than 3wks without inflammation :
immediate internal fixationMore than 3wks :
limb temporarily stabilized in cast for 8-10 days prevent infection

Reamed or Unreamed Nailing?
Controversial in terms of infection, nonunion & re-operation rateTheoretical advantage with unreamed -preserving blood supplyMore nail or screw breakageProblems: Ex Fix > Unreamed > ReamedFew bones large enough!Reamed nailing generally safe for IIIA or below.
Early Soft Tissue Coverage:Initial Flap Preservation
Esp. where local flaps are not readily available: distal 1/3 of tibia and beyondDon’t jeopardise blood supply by insertion of pins, drains etc. thro’ the flapNo tensionMinimise soft tissue motion - to enhance regeneration of microvasculature - skeletal immobilisation

Early Soft Tissue CoverageUsually within 3 days to 1 week to prevent nosocomial infection (main source of infection in open #) and improve outcomeBalanced by soft tissue tension & infectionMethods: - Delayed 1° closure- Skin graft (PTSG, full thickness)- Flap (local, free) bring in blood supply
Soleal flap

Vacuum Assisted Closure (VAC)
Accelerating wound healing by reducing chronic edema, increasing local blood flow and enhancing granulation tissue formationApplied after each irrigation & debridementuntil wound is clean (about 10-20 days)Promising modality, but need additional studies

Management of Bone Defect
Depends on size & site of defect
Bone graft Bone transportBone defect
OR
Shortening
OR

Management of Bone DefectBone Graft
Autograft / allograft / artificial boneCortical / cancellousVascularised / nonvascularised

Bone Grafting
I & II #’s generally do not require bone graft - dynamise at 6 - 12 weeks.
III #’s - YES, but not before 6 weeks.No segmental defect - graft if no callus by 12w.Segmental defect < 2cm, graft at 6 weeksSegmental defect > 2cm, bone transport

Recombinant Human Bone Morphogenetic Protein-2 (rhBMP-2)
Reduce secondary procedures, hardware failure & wound infectionFaster fracture healing & wound healingNeed further studies

Management of Bone Defect
Bone transport Ilizarov

Rehabilitation:Minimize Disability
Avoid immobilizing jointsAvoid transfixion of muscle or tendonsEarly mobilizationMaintenance exercisesPsychological supportPrevent sores

Management Protocol

Complications
InfectionDelayed unionNon-union

Amputation:Guideline
Nonviable limbNonfunctional limbLife-theatening limbToo extensive & prolonged reconstruction MESS >7
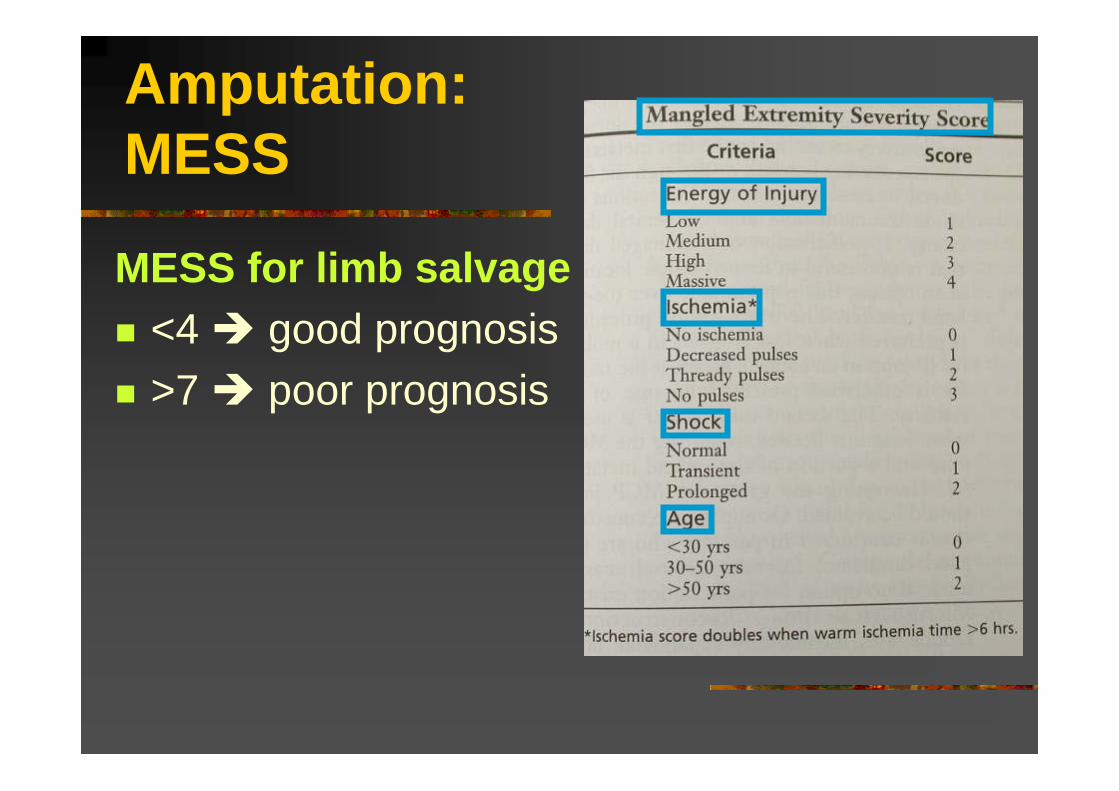
Amputation:MESS
MESS for limb salvage<4 good prognosis>7 poor prognosis


Open Fractures
Clinical Cases

Salvageable Limb
Case 1

Female / 25 yr / RTA (motorbike)

Limb threatening condition !
Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery

RevascularizationDebridementExternal fixation

Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flapMx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery
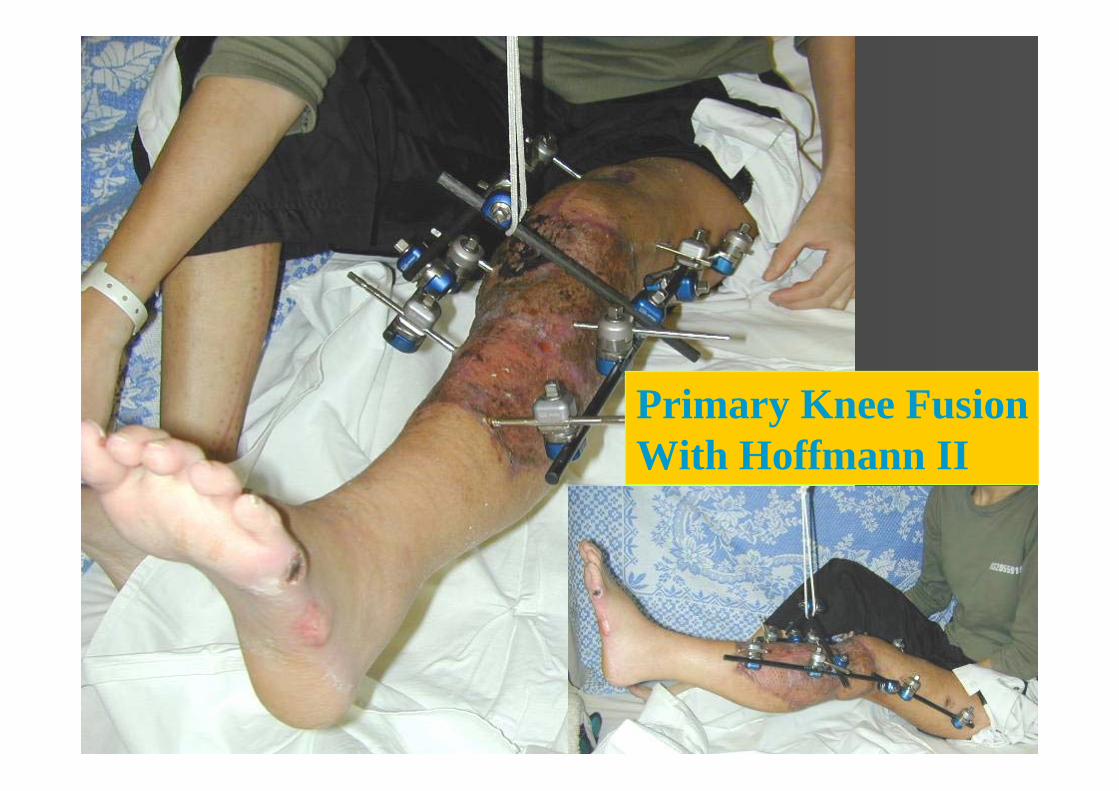
Primary Knee FusionWith Hoffmann II

Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery


Non-salvagable Limb
Case 2

Knocked down by a car MESS=7
M/54


Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery



Day 1, 2nd Debridement, Two Pins Added

What next ?
Keep fixator, skin graft, wait for bone healing ?
BKA ?

MESS
Very high energy : 4Age 54 : 2Transient shock : 1Limb ischaemia : 0
Total: 7 / 14Amputation recommended for score of >= 7.

What next ?
Keep fixator, skin graft, wait for bone healingBKA
Change to Ring Fixation to buy more time

Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery

Day 3
Hybrid Fixatorwith tensioned wire

Soft tissue defect anticipated!

Local antibiotics:Gentamicin beads
Bone defect also anticipated!

Day 10: Complicated with Infection despite Repeated Debridement
Agreed to BKA

Conversion to Nailing
Case 3

Antero-lateral view, Right leg
Antero-medial close-up viewRight leg
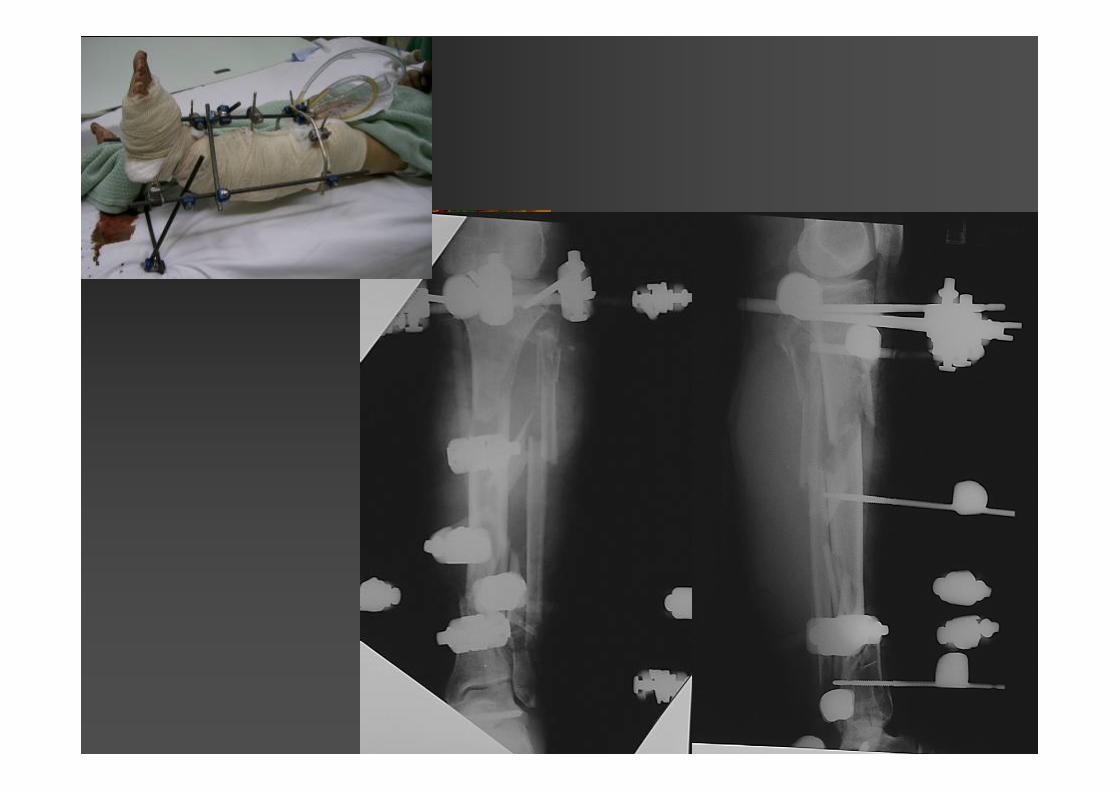
M/51
RTABilateral open fracture tibia .Left side Grade IIRight side IIIB.


Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery

Initial Treatment
Day 0: debridement, lavage, ex fix both sides, bridging across the ankle.Day 4: lavaged againDay 6:
Left side converted to IM nail.Right side: ex fix revised. Ex fix fixing distal
tibial segment instead of bridging across ankle joint. Further lavage.
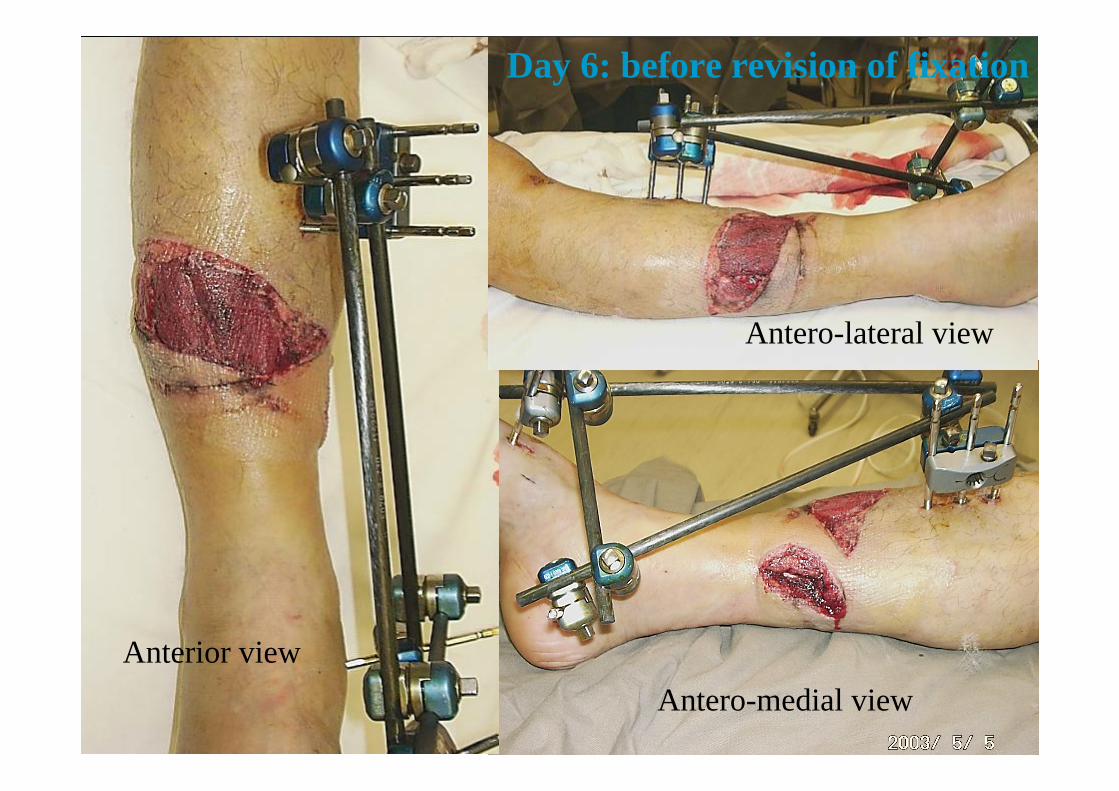
Antero-lateral view
Anterior viewAntero-medial view
Day 6: before revision of fixation

Small area of exposed bone
Day 6: after revision of fixation
Anterior view

Antero-medial view
This wound communicates with posterior surface of tibia.
Exposed bone

Close up view of exposed bone


Subsequent Development
Day 10: SSG of wounds.SSG taken and all wounds became closed.4 week: Autogenous cancellous bone graft onto antero-lateral aspect of fracture site.
Patient discharged to KH. Refused Exogen treatment.

Opposite (Left) Tibia

Initial Management
Debridement, lavage, Ex fix on admission.Repeat debridement and lavage on D2 & D4Conversion to AO IM Nail on Day 6Wounds closed

Day 9
Left Leg

11 weeks
Left Leg

11 weeks
Right Leg
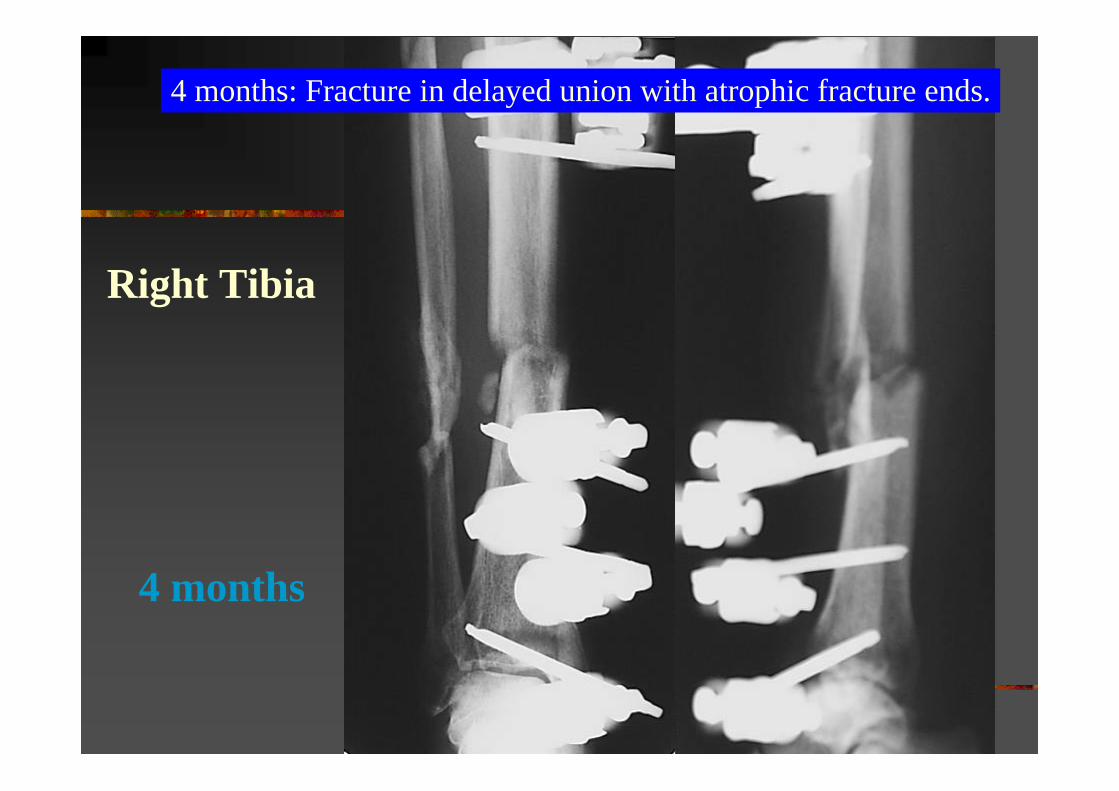
4 months
4 months: Fracture in delayed union with atrophic fracture ends.
Right Tibia

4 months
Right Leg

4 months
Right Leg

4 Months
Fixator removedFracture grossly unstable: even the fibula is not united yetPin tracts debrided and over-drilledApplication of short-leg cast with windows for pin hole dressing
Right Leg

Pin tracts “rested”for 4 weeks.
5 months
Resection of fibula, IC nail fixation of tibia with compression.
Right Leg

5 months
Started on Exogen
Right Leg

2 weeks
8 weeks 14 weeksRight Leg

2 weeks 8 weeks 14 weeks
Right Leg

22 weeks
Right Leg

22 weeks

One and a half year

Day 3 10 weeks 30 weeksLeft Leg

Day 3 10 weeks 30 weeksLeft Leg

Conversion to Nailing
Case 4

M/23
Ex-member of Hong Kong Badminton teamWorks as Badminton coachStudent at City UniversitySustained severe injuries when his motorbike was hit by a car.

Open wounds at the left leg.

Initial debridementand Hoffmann II External Fixation

Before and after initial external fixation

Day 3, fixation revised


Injured limb supported and raised on the fixatorframe to facilitate nursing care, surgery, and drainage.

Skin graft

4 weeks

Fixation removed (already the 9th operation).Pin holes “rested” for 4 weeks.

8 weeks after injury
IC Tibial nail inserted.

6 months after nailing
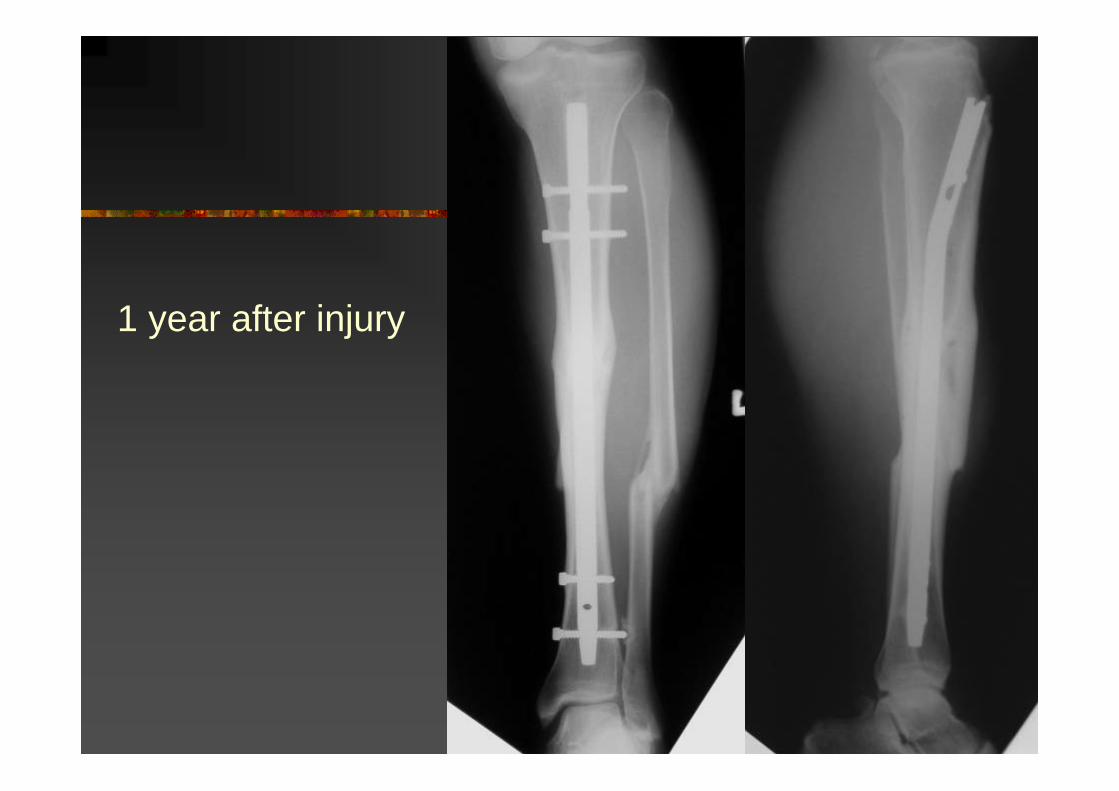
1 year after injury

Two years after injuryIM Nail removed12 operations in totalFull range at the kneeKnee instability due to PCL rupture (pending reconstruction)Minimal pain at the injured limbResumed badminton coaching part-timeResumed university studies

2 years after injury


Infected Open Fracture
Case 5

M/50
Type IIIA open fracture of distal tibia Also with fractures in the tarsals and metatarsalsCrushed by metal board


Initial treatment on Day 0
Debridement, LavageExternal fixationiv Antibiotics

Day 2Wound looked clean and healthy, not much stripping of bone.Reamed IM nail using Osteo IC tibialnail, static lockWound debrided, lavaged, SSGClinical photo just before SSG ...


Day 11
ORIF of foot fractures calcaneal via lateral incision;navicular via medial incision
Foot and ankle quite swollen prior to this, skin quite precarious on lateral side.SSG on open wound had taken well.


Infection!
Redness and discharge started at lateral foot wound, then the medial wound,Stitches taken off for drainagethen the wound over the patella tendon became red as well.MRSA

Day 23, Day 39
Wounds debrided and debrided

Progress
Patella tendon wound gradually got betterFoot wounds still bad Foot wounds gradually healed up after exposure and removal of some implantsBy 8 weeks, just prior to discharging home, collection found at antero-medial aspect of fracture site!

Day 59
Incision and drainage of abscessIncision at antero-medial aspect.Abscess cavity extended to postero-medial aspect of fracture, communicating

10 weeks
Loosening of distal fixation detected, fracture went into valgus & recurvatum

10 weeks

Subsequent Management(11 weeks)
Removal of nail, overreaming, hybrid external fixation,Debridement of wound and fracture site, intramedulary gentamycin beads,plating of fibula


After wound closure


2 May 2003

12 weeks


15 weeks (3 weeks after hybrid fixation)
Autogenous cancellous bone graft laid onto anterior aspect of inter-osseous membrane at the level of the fracture

Exogen
Started on 4 weeks after hybrid fixationDaily standard dose

18 weeks(6 weeks afterhybrid)

11 weeks after hybrid

11 weeks after hybrid
Pin tracts okay.On touch down walking.“Early callus”palpable along antero-medial aspect of tibia.

14 weeks

14 weeks

14 weeks

17 weeks after hybrid
External Fixator removed
Patient advised to keep 20% weight bearing

23 weeks

35 weeks from hybrid fixation11 months after injury
Stick walking 30 min, unaided 10 min.

43 weeks from hybrid fixation13 months after injury

Delayed Union
Case 6

Male / 16
Traffic Accident
Type II Open Wound
Single injury

Initial Management (Day 0)
DebridementFree fragments discardedLavage (9 litres of NS)External fixationAntibiotics
Day 2
DebridementLavage (9 L. of NS)

Day 5
DebridementLavage (9 L. of NS)Removal of External fixatorG-K Tibial Nail - static lockSoleal Flap + Skin graft

10 days afternailing

8 weeks afternailing

9 Weeks after Nailing
Postero-lateral bone graftAutogenous cancellousbone laid on the interosseous membraneTo induce cross union

10 days afterbone graft

10 weeks afterbone graft

Dynamisationperformed 5 months afternailing (3 months afterbone graft).

3 months afterdynamisation

5 months afterdynamisation,
removal of prox. screws

2 year 8 months after injury.
Delayed union is common in open fracture even after BG

Soft Tissue Defect requiring Flap Coverage
Case 7

M/64
DM, HT, Schizophrenia, Parkinson, Chronic smokerLive with family, walk unaided RTA: knocked down by a taxi
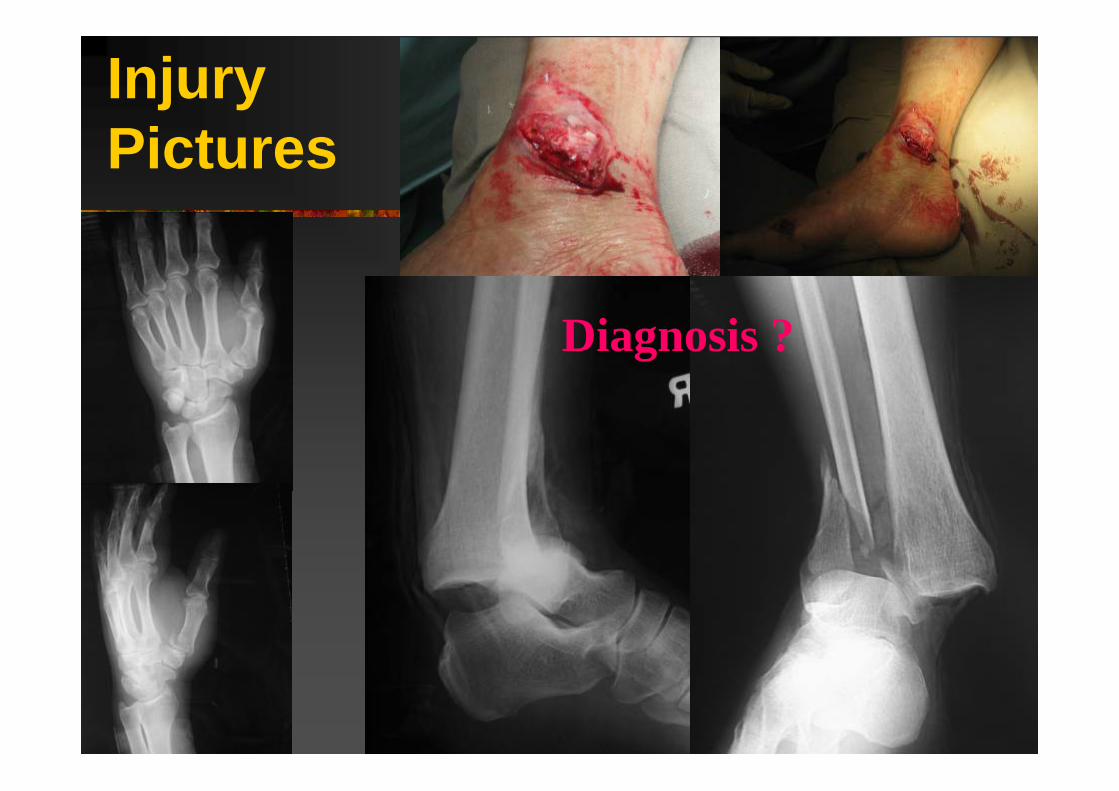
Injury Pictures
Diagnosis ?

Diagnosis
Open fracture dislocation of right ankle1. Type IIIb: perosteal stripping without vascular
deficit2. # medial & lateral malleolus
Closed extra-articular # of base of left 1st MC
Management Plan ?

Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery

Day 0
Ankle: Debridement + External FixationThumb: CR + K-wire + dynacast

Day 0
Intra-op: right knee haemathrosis noticed No gross laxityBetter x-ray showed PCL injury

Day 1
Wound: soft tissue necrosis2nd look debridementCross knee external fixation for PCL

Day 3
Wound: purulent collection drained, necrosis debrided until healthy viable tissue seen , non-viable medial malleolus free fragment also removed Large soft tissue defect with bone & joint exposed
What next ?
Chest infection & Fever

What next ?
Bone exposed !
Joint exposed !
Infection set in !

Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery

Soft TissueReconstruction Ladder
Delayed 1° closure X too much skin loss2° intention by granulation ?? too big & too longSkin graft X bare bone exposedFlap: Free ?? 64 yr old, DM, HT, schizophrenia, chronic smoker, chest infectionFlap: Local- Random X not reliable
- Pedicled Options ?

Local Pedicled Flap for Foot & Ankle Region
Supra-malleolar Medial saphenousMedial plantarMedialis pedisPeroneus brevisExtensor brevisCross-leg
All are technically demanding with variable result !

Reconstruction aroundDistal leg, Ankle & Heel
Technically demandingLimited option for local muscle flap & random skin flap in distal LL, which sacrificing major arteries Free flap more classic BUT
1. lengthy operation 2. Microvascular expertise3. Contraindication for microsurgery: old age,
heavy smoker, poor medical condition

Reverse Sural Flap
Fasciocutaneous flap depends on superficial sural artery of peroneal arteryPedicle: superficial & deep fascia, sural nerve, short sapehnous vein & superficial sural arteryFlap proper: skin island , subcutaneous tissue & fasciaFor reconstruction of soft tissue defect around distal leg, ankle, heel & dorsum of foot

Advantage
Great mobility & versatility with wide arc of rotation (90°-180°): from distal leg to heel to forefootQuick (2 hrs, one-stage), easy (minimal expertise) & reliable (constant anastomosis)Safe, without sacrificing important artery or structure, no major donor morbidityExcellent durability even for heel coverageSuitable for all age group from pediatrics to elderly
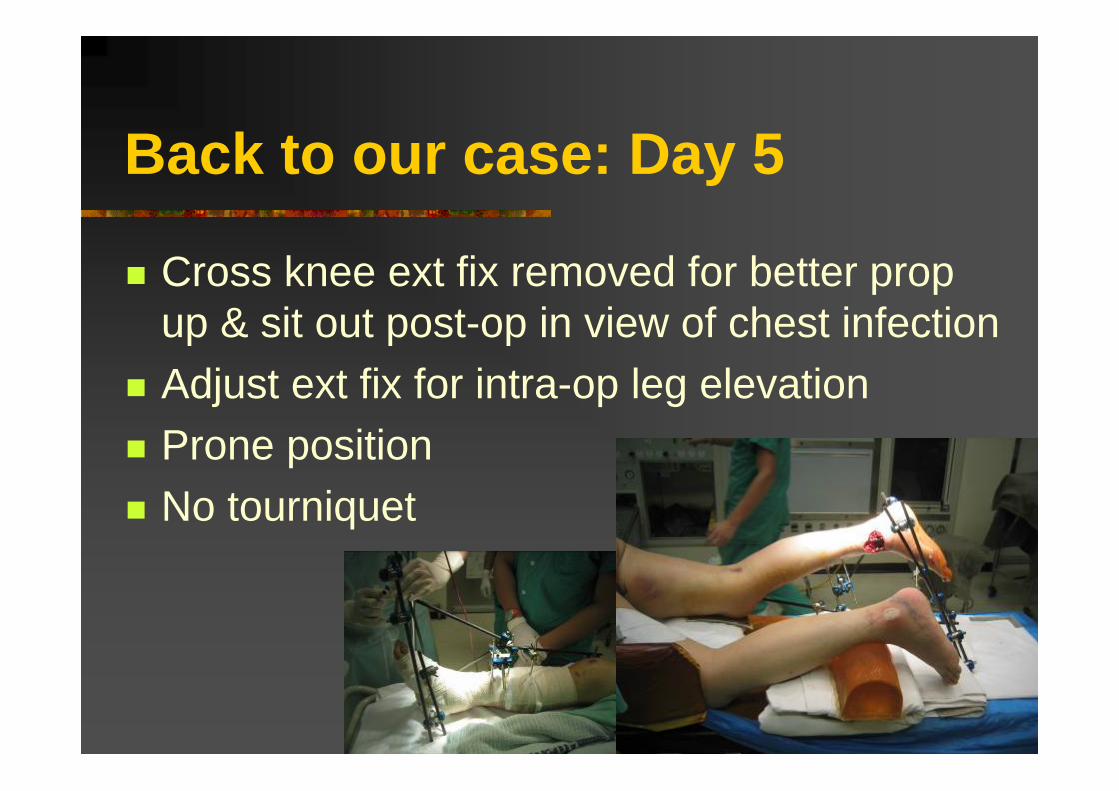
Back to our case: Day 5
Cross knee ext fix removed for better prop up & sit out post-op in view of chest infection Adjust ext fix for intra-op leg elevationProne positionNo tourniquet
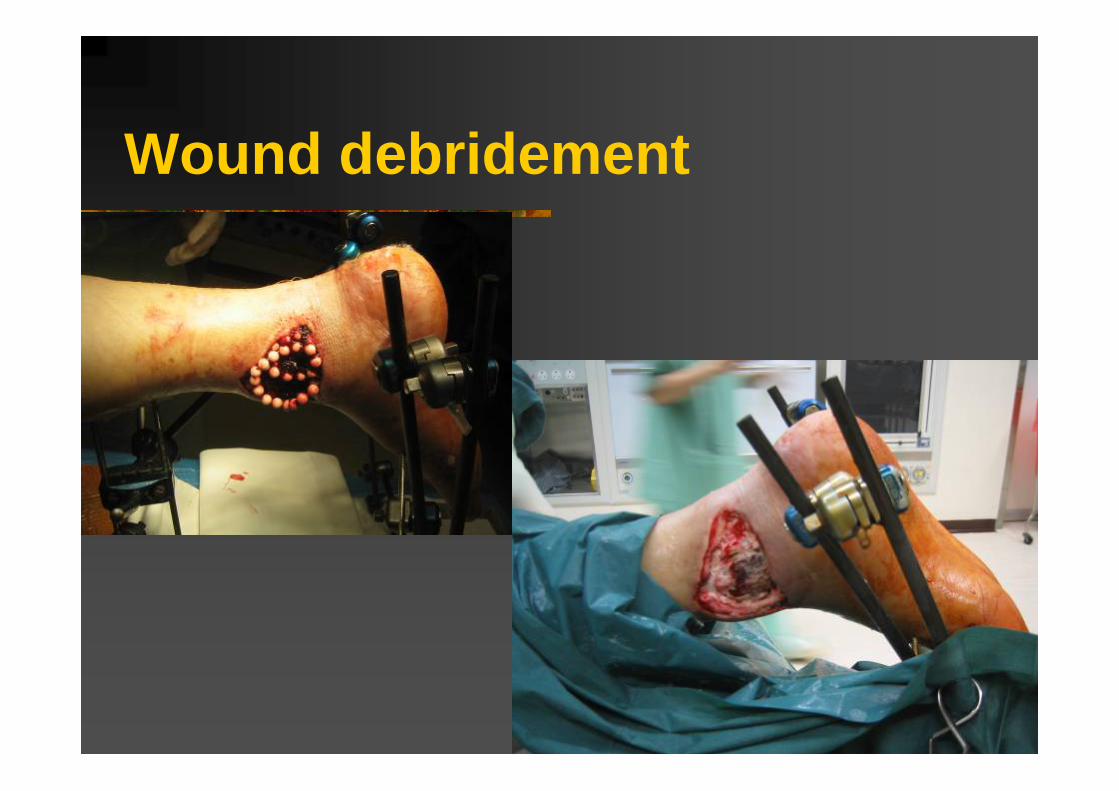
Wound debridement

PlanningA line at halfway between Achilles tendon & lateral malleolus, from ankle to midline between two heads of gastrocnemiusMark the most distal point of dissection: 7cm above tip of lateral malleolusMark the pedicle & adjacent fasciaMark the skin island of flap

Identify the Pedicle
Skin incision over pedicleSkin undermined to explore the pedicle and adjacent 1-2cm fascia on each side

Fasciocutaneous Flap Dissection
Identify & ligate the sural nerve & adjacent short sapheouns vein at proximal margin

Pedicle Dissection
Dissect the flap including the deep fascia covering gastrocnemius muslcePedicle dissected including adjacent fascia, about 1-2 cm on each side

Flap transfer to cover defect

Donor site closure
Donor coverage: PTSGIncision for pedicle: primary suturePedicle coverage: PTSG

Flap 5 weekPost injury 6 week

10 Weeks

High Successful Rate even with Risk factors
Age>40PVDVenous insufficiencyDMHeavy smokerPoorly compliant patient

SUMMARY

Open Fracture
Fracture communicates through a traumatic wound to surrounding environment Resulting in contamination & soft tissue envelope disruption

Open Fracture
High energyOutcome depends extent of soft tissue injuryTreatment of soft tissue trauma withcontamination Primarily importantTreatment of skeletal injury Secondary

Type III Open Fracture
It is not “a fracture with a wound”It is “a wound resulting from high energy trauma, complicated with a Fracture”First priority is to deal with the Wound,and then minimize complications arising from the fracture.
Objectives of Open Fracture Mx
Prevent infectionPromote fracture healingRestore function

Principles of ManagementATLS: Save life first, then save limbPrevent infection: Wound debridement & lavage,IV / local antibiotics, Tetanus prophylaxisFracture stabilization: Temporarily & definiteEarly soft tissue coverage: Initial flap preservation, delayed 1° suture, secondary intention, skin graft, flap Mx of bone defect: Shortening, bone graft / transportRehabilitation: to minimize disability & optimize functional recovery

Complications
InfectionDelayed unionNon-union

Open Fracture Management
Analyze needs, prioritize aims, plan, and plan for the worstTake them seriously!

Thank You
The End

Principle of External Fixation

External Fixator
External device (outside the skin) Stabilizes the bone fragments through pins or wires connected to bars, tubes or rings

Types of External Fixator
Pin fixators (Schanz pins / Steinmenn pins)Ring fixators (tensioned wires)Hybrid fixators (wires and pins)

Pin FixatorsAO Orthofix
Stryker: Hoffmann II

Ring & Hybrid Fixators
AO Orthofix
Half pin
Tensioned wire
Stryker: Tenxor

AO Mini
Mini- FixatorsStryker:Hoffmann Compact

IlizarovRing Fixator

Components of External Fixator
Pin / WireClampRod
Straight and U rods
Pin-to-ClampClamp-to-Rod
Pin-to-Rod
Different Combinations !

Frame Classification
1 Unilateral1A Unilateral uniplanar1B Unilateral biplanar
2 Bilateral2A Bilateral uniplanar2B Bilateral biplanar (3D)
3 Modular

Unilateral uniplanar
Bilateral uniplanar
Unilateral biplanar
Bilateral biplanar (3D)
Frame Classification
Modular

Safe Soft Tissue Corridor
Avoid vessels, nerves & tendons

Advantages
• Provides low-risk stable fixation- minimal additional soft tissue trauma
• Adjustable- allowing translation, rotation, angulation, and axial
adjustments• Provides access to the extremity
- for wound care and reconstructive surgery. • Technically easy to perform
- apply quickly

Disadvantages
Bulk of the device Discomfort Need for daily pin carePin tract infection Delay union/ nonunionMalunionTethering of muscle & tendonLimitation of the joint movement

Biomechanics of External Fixator
Stability of frame depends on1. Pin size2. Number of pins3. Pin location4. Bone-frame distance
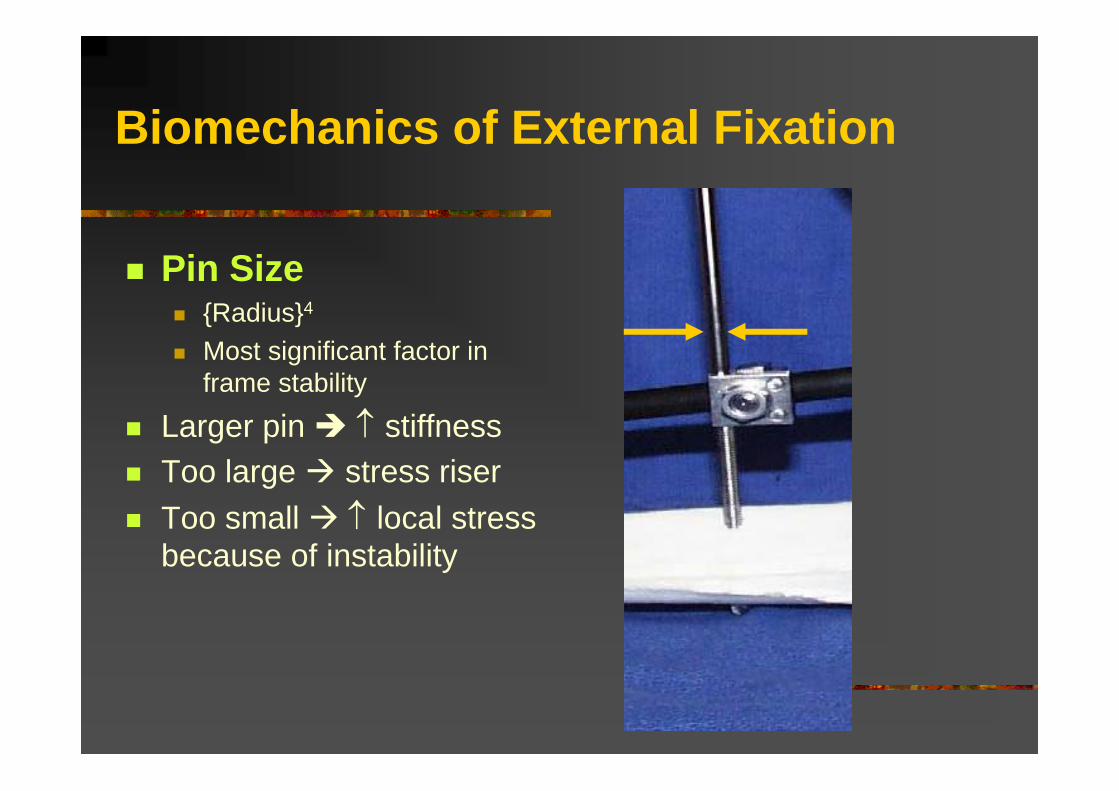
Biomechanics of External Fixation
Pin Size{Radius}4
Most significant factor in frame stability
Larger pin ↑ stiffness Too large stress riserToo small ↑ local stress because of instability

Biomechanics of External Fixation
Number of Pins More pins more stable

Biomechanics of External Fixation
Pin LocationAvoid zone of injury or future ORIFPins close to fracture as possiblePins spread far apart in each fragment

Biomechanics of External Fixation
Bone-Frame DistanceCloser better

Factors Affecting Construct Stiffness

Biomechanics of External FixationSUMMARY OF EXTERNAL FIXATOR STABILITY:
Can make a fixator more stable by:1] Increasing the pin diameter.2] Increasing the number of pins.3] Increasing the spread of the pins.4] Multiplanar fixation.5] Reducing the bone-frame distance.6] Predrilling & cooling during insertion (↓ thermal necrosis).7] Radially preload pins.8] 90° tensioned wires.9] Stacked frames.
**but a very rigid frame is not always good.

How to improve stability of this frame

•More pins
•More rods
•Better position of rods
•Bilateral biplanar frame
Much better now !

Complications of Ext. Fix.
Pin loosening Pin tract infection
• Malunion• Delayed or non-union• Neurovascular injury• Fracture through the hole• Failure of fixation

Application of External FixationAny fracture
Open fracturePolytraumaComminuted metaphyseal fracturePaediatric fracture
• Bone transport • Limb lengthening • Angular correction • Soft tissue reconstruction • Contractures
Related Documents