1 Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743 Open access The work of return to work. Challenges of returning to work when you have chronic pain: a meta-ethnography Mary Grant, 1 Joanne O-Beirne-Elliman, 1 Robert Froud, 1,2 Martin Underwood, 1 Kate Seers 3 To cite: Grant M, O-Beirne- Elliman J, Froud R, et al. The work of return to work. Challenges of returning to work when you have chronic pain: a meta-ethnography. BMJ Open 2019;9:e025743. doi:10.1136/ bmjopen-2018-025743 ► Prepublication history and additional material for this paper are available online. To view these files, please visit the journal online (http://dx.doi. org/10.1136/bmjopen-2018- 025743). Received 3 August 2018 Revised 26 February 2019 Accepted 17 April 2019 1 Clinical Trials Unit, University of Warwick, Warwick Medical School, Coventry, UK 2 Department of Health Sciences, Kristiania University College, Oslo, Norway 3 Warwick Research in Nursing, University of Warwick, Warwick Medical School, Coventry, UK Correspondence to Dr Mary Grant; [email protected] Research © Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ. ABSTRACT Aims To understand obstacles to returning to work, as perceived by people with chronic non-malignant pain and as perceived by employers, and to develop a conceptual model. Design Synthesis of qualitative research using meta- ethnography. Data sources Eleven bibliographic databases from inception to April 2017 supplemented by citation tracking. Review methods We used the methods of meta- ethnography. We identified concepts and conceptual categories, and developed a conceptual model and line of argument. Results We included 41 studies. We identified three core categories in the conceptual model: managing pain, managing work relationships and making workplace adjustments. All were influenced by societal expectations in relation to work, self (self-belief, self-efficacy, legitimacy, autonomy and the meaning of work for the individual), health/illness/pain representations, prereturn to work support and rehabilitation, and system factors (healthcare, workplace and social security). A mismatch of expectations between the individual with pain and the workplace contributed to a feeling of being judged and difficulties asking for help. The ability to navigate obstacles and negotiate change underpinned mastering return to work despite the pain. Where this ability was not apparent, there could be a downward spiral resulting in not working. Conclusions For people with chronic pain, and for their employers, navigating obstacles to return to work entails balancing the needs of (1) the person with chronic pain, (2) work colleagues and (3) the employing organisation. Managing pain, managing work relationships and making workplace adjustments appear to be central, but not straightforward, and require substantial effort to culminate in a successful return to work. INTRODUCTION Chronic pain, defined as pain lasting 3 months or more, 1 is a global public health problem affecting one in ten adults. 2 A 2017 mega-ethnography brought together 11 qual- itative evidence syntheses to explore the expe- rience of living with chronic non-malignant pain. 3 Previous reviews have identified the importance of the effect of chronic pain on people’s work life. 4 5 Chronic pain is strongly associated with claiming disability and unem- ployment benefit in Australia 1 and with unemployment in the USA. 6 The obstacles to staying in work for people with musculoskel- etal pain have previously been explored in a meta-ethnography, 7 and factors promoting staying at work are the focus of a previous mixed-methods systematic review. 8 A qualita- tive systematic review of the impact of chronic pain in the workplace 9 takes a broad perspec- tive including impact on employment status, sickness absence and loss of productivity in contrast to a condition and gender-specific literature review focused on work and rehabil- itation for women with fibromyalgia. 10 There is a qualitative research on the perspective of doctors, 11 but this is not considered further in this paper. The lack of focus on return to work for people with chronic non-malignant pain and the perspective of employers presents a knowledge gap in existing reviews. Return to work can refer to the process of returning after a period of sick leave 12 or returning after a period of unemployment. 13 This review uses qualitative evidence synthesis to increase understanding of the obstacles to return to work for people with chronic pain and their employers, and this can then inform inter- vention development to support return to work. 4 14 Strengths and limitations of this study ► This is the first study to present employer and em- ployee perspectives together. ► This study draws together what is known from qual- itative studies to inform practice. ► This study highlights health and illness and pain rep- resentations in relation to return to work. ► Only five studies covered employers’ perspectives, so there are fewer data on employers’ perspectives compared with the perspectives of people with chronic pain. on October 20, 2021 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
The work of return to work. Challenges of returning to work when you have chronic pain: a meta-ethnography
Mary Grant,1 Joanne O-Beirne-Elliman,1 Robert Froud,1,2 Martin Underwood,1 Kate Seers3
To cite: Grant M, O-Beirne-Elliman J, Froud R, et al. The work of return to work. Challenges of returning to work when you have chronic pain: a meta-ethnography. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
► Prepublication history and additional material for this paper are available online. To view these files, please visit the journal online (http:// dx. doi. org/ 10. 1136/ bmjopen- 2018- 025743).
Received 3 August 2018Revised 26 February 2019Accepted 17 April 2019
1Clinical Trials Unit, University of Warwick, Warwick Medical School, Coventry, UK2Department of Health Sciences, Kristiania University College, Oslo, Norway3Warwick Research in Nursing, University of Warwick, Warwick Medical School, Coventry, UK
Correspondence toDr Mary Grant; M. Grant. 2@ warwick. ac. uk
Research
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
AbstrACtAims To understand obstacles to returning to work, as perceived by people with chronic non-malignant pain and as perceived by employers, and to develop a conceptual model.Design Synthesis of qualitative research using meta-ethnography.Data sources Eleven bibliographic databases from inception to April 2017 supplemented by citation tracking.review methods We used the methods of meta-ethnography. We identified concepts and conceptual categories, and developed a conceptual model and line of argument.results We included 41 studies. We identified three core categories in the conceptual model: managing pain, managing work relationships and making workplace adjustments. All were influenced by societal expectations in relation to work, self (self-belief, self-efficacy, legitimacy, autonomy and the meaning of work for the individual), health/illness/pain representations, prereturn to work support and rehabilitation, and system factors (healthcare, workplace and social security). A mismatch of expectations between the individual with pain and the workplace contributed to a feeling of being judged and difficulties asking for help. The ability to navigate obstacles and negotiate change underpinned mastering return to work despite the pain. Where this ability was not apparent, there could be a downward spiral resulting in not working.Conclusions For people with chronic pain, and for their employers, navigating obstacles to return to work entails balancing the needs of (1) the person with chronic pain, (2) work colleagues and (3) the employing organisation. Managing pain, managing work relationships and making workplace adjustments appear to be central, but not straightforward, and require substantial effort to culminate in a successful return to work.
IntroDuCtIonChronic pain, defined as pain lasting 3 months or more,1 is a global public health problem affecting one in ten adults.2 A 2017 mega-ethnography brought together 11 qual-itative evidence syntheses to explore the expe-rience of living with chronic non-malignant pain.3 Previous reviews have identified the importance of the effect of chronic pain on people’s work life.4 5 Chronic pain is strongly
associated with claiming disability and unem-ployment benefit in Australia1 and with unemployment in the USA.6 The obstacles to staying in work for people with musculoskel-etal pain have previously been explored in a meta-ethnography,7 and factors promoting staying at work are the focus of a previous mixed-methods systematic review.8 A qualita-tive systematic review of the impact of chronic pain in the workplace9 takes a broad perspec-tive including impact on employment status, sickness absence and loss of productivity in contrast to a condition and gender-specific literature review focused on work and rehabil-itation for women with fibromyalgia.10 There is a qualitative research on the perspective of doctors,11 but this is not considered further in this paper.
The lack of focus on return to work for people with chronic non-malignant pain and the perspective of employers presents a knowledge gap in existing reviews. Return to work can refer to the process of returning after a period of sick leave12 or returning after a period of unemployment.13 This review uses qualitative evidence synthesis to increase understanding of the obstacles to return to work for people with chronic pain and their employers, and this can then inform inter-vention development to support return to work.4 14
strengths and limitations of this study
► This is the first study to present employer and em-ployee perspectives together.
► This study draws together what is known from qual-itative studies to inform practice.
► This study highlights health and illness and pain rep-resentations in relation to return to work.
► Only five studies covered employers’ perspectives, so there are fewer data on employers’ perspectives compared with the perspectives of people with chronic pain.
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from

2 Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
MethoDsAims and objectivesThis meta-ethnography explores experiences of returning to work, as perceived by people with chronic non-malig-nant pain and by employers, and develops a conceptual model.
study designThere are two main approaches to synthesising qualita-tive research, one that aggregates findings to describe the literature and one that aims to interpret findings and develop a conceptual understanding.4 14 15 Meta-ethnog-raphy is an interpretative form of knowledge synthesis that was chosen for this study in order to both integrate and develop a greater understanding of existing knowledge and identify any other overarching concepts that would explain the data. The seven phases of meta-ethnography are outlined by Noblit and Hare15 and elaborated on by Toye et al.14 These are (1) getting started by identifying the area of interest; (2) deciding what is relevant; (3) reading and rereading the studies; (4) determining how the studies are related, which involves creating a list of key phrases, ideas, metaphors and concepts; (5) translating the studies into one another, where direct comparisons are made and similar concepts are sorted into catego-ries; (6) synthesising the translations, where researchers make sense of the conceptual categories to develop new knowledge and understanding; and (7) expressing the synthesis. A line of argument was constructed by exam-ining how the conceptual categories relate to each other.
Identifying and appraising the review articlesSearch methodsStudy selectionEleven electronic bibliographic databases were searched (Allied and Complementary Medicine (AMED); Applied Social Science Index and Abstracts (ASSIA); The Cumulative Index to Nursing and Allied Health Literature (CINAHL); EMBASE; International Bibliography of the Social Sciences (IBSS); MEDLINE; PsycINFO; Social Services Abstracts; Sociological Abstracts; Web of Science and Westlaw) from inception up until 25 April 2017, supplemented by backward and forward citation tracking using Scopus. These data-bases were considered appropriate because in early scoping work we identified relevant studies in these databases. An academic support librarian undertook the initial search in collaboration with RF in December 2016, and this was updated by MG in April 2017, who continued the screening and selection of papers. The search terms used included ‘Chronic pain’ and ‘Return to work (MeSH) OR Employ-ment OR Employer OR Supported Employment (MeSH)’. In April 2017 two additional search terms were used, ‘pain’ to broaden search as ‘chronic pain’ was not identifying all relevant papers, and ‘qualitative’ as suggested by Shaw et al16 to focus the search on studies with this type of methodology. The search strategy is detailed in online supplementary file 1. All qualitative studies using face-to-face interviews and focus groups which explored perceptions of obstacles to
return to work, in employers and people who were off work, sick-listed and had chronic pain, were included. Non-En-glish-language texts were excluded.
Quality appraisalThe quality of studies was evaluated using the Critical Appraisal Skills Programme (CASP) qualitative assess-ment tool.17 A scoring system was used for CASP (yes=3, can’t tell=2, no=1). A score of 20 or higher indicates the paper is deemed to be of satisfactory quality. The GRADE-CERQual (Grading of Recommendations Assess-ment, Development and Evaluation-Confidence in the level of Evidence from Reviews of Qualitative research) approach was also completed.18 19 Confidence in review findings was assessed based on four components: adequacy of data,20 coherence,21 methodological limita-tions22 and relevance.23
AnalysisInitially, the first 10 papers (in alphabetical order of author) were read by MG, KS and JO-B-E in order to iden-tify key ‘concepts’, the raw data of meta-ethnography.14 These concepts are ideas drawn from the findings of the original papers. They are also known as second-order concepts because they are the authors’ interpretations of the participants’ narratives (known as first-order concepts).24 The participants’ narratives chosen by the author are examples of second-order concepts.14 After reading these 10 papers, the concepts identified by each researcher were amalgamated through discussion and grouped into conceptual categories that the team then worked collaboratively to name. This took place over a series of three meetings. These conceptual categories are third-order concepts insofar as they are the researchers’ interpretations of second-order concepts. All concepts were identified by all three authors (KS, MG, JO-B-E), and even if exact wording differed the concept was the same. This is the way that studies were translated and related to each other. The first author then proceeded to read the rest of the papers and continue this process of analysis. Five additional papers were also read by KS and JO-B-E where MG felt a collaborative discussion would be helpful due to the nature and/or findings of the studies. Thus 25% of papers were checked (n=10), then an additional 10% were checked (ie, 35% in total) to ensure ratings and concepts were in agreement. All the included papers were uploaded to QSR International’s NVivo V.11 soft-ware,25 and nodes were created for the conceptual catego-ries. The next stage was to make sense of these categories through further discussion, make decisions about which were the core categories and develop a line of argument and conceptual model,14 involving a further four meet-ings. Recurring and common concepts were compared across studies,15 where directly comparable (reciprocal translation) together they contributed to our line of argu-ment. We did not find studies that stood in opposition (refutational translation). The line of argument makes a whole of something more than a sum of the parts.15 MG,
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from
3Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
JO-B-E and KS independently drew their own conceptual model before coming together to agree a model, which was revised through several discussions, and the final version is presented in this paper. The culture described by Toye et al26 of a core team that provided a safe envi-ronment in which to freely discuss, agree, disagree and change their position in relation to conceptual analysis was seen as a key strength, laying the foundations for a rigorous review. This approach was adopted in this review. We explored alternative interpretations and explana-tions, including locus of control, navigating relationships, normalising participants’ pain condition and agency but these ideas were not supported as major concepts. Many of these concepts were subsumed in other categories.
Patient and public involvementA patient and public representative was involved in the development of the research funding submission for the overall study as a coapplicant and endorsed the impor-tance of the focus of this meta-ethnography recognising the central nature of obstacles to return to work.
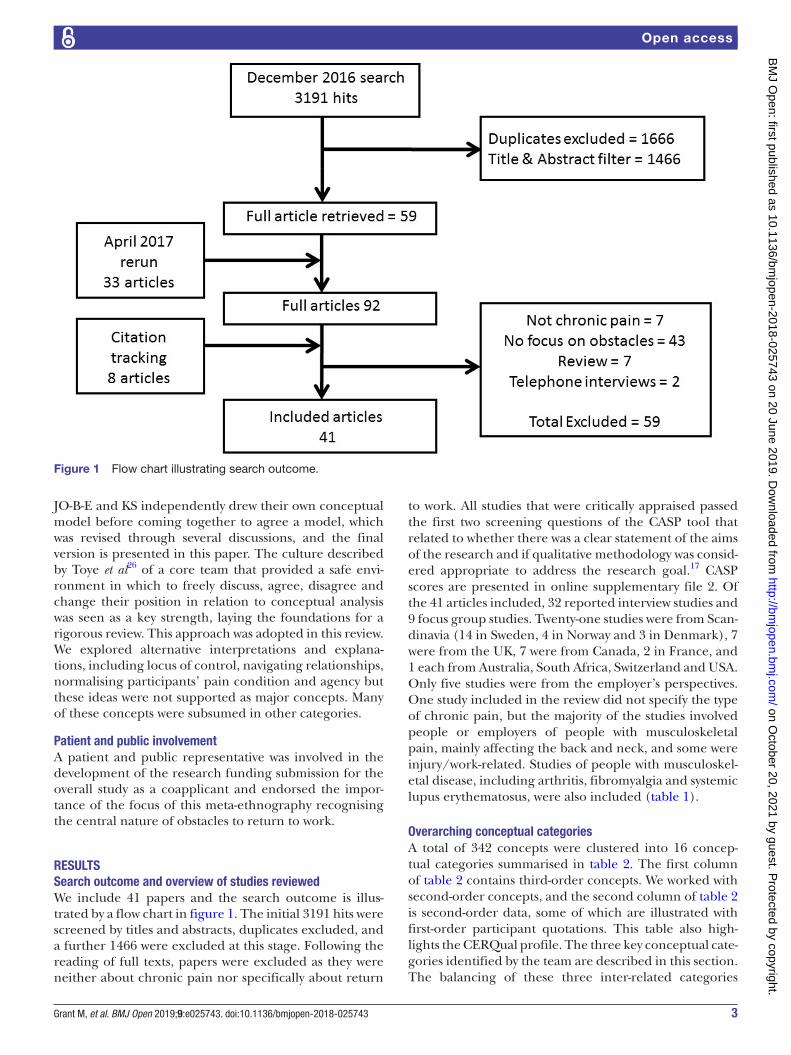
resultssearch outcome and overview of studies reviewedWe include 41 papers and the search outcome is illus-trated by a flow chart in figure 1. The initial 3191 hits were screened by titles and abstracts, duplicates excluded, and a further 1466 were excluded at this stage. Following the reading of full texts, papers were excluded as they were neither about chronic pain nor specifically about return
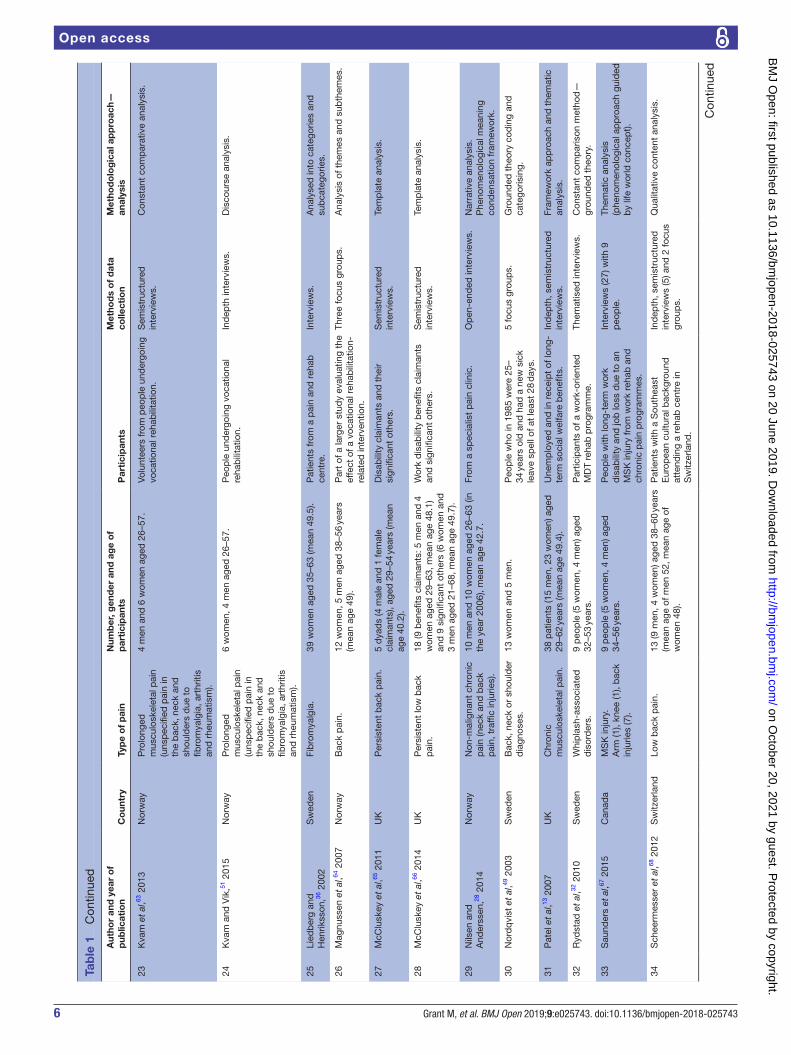
to work. All studies that were critically appraised passed the first two screening questions of the CASP tool that related to whether there was a clear statement of the aims of the research and if qualitative methodology was consid-ered appropriate to address the research goal.17 CASP scores are presented in online supplementary file 2. Of the 41 articles included, 32 reported interview studies and 9 focus group studies. Twenty-one studies were from Scan-dinavia (14 in Sweden, 4 in Norway and 3 in Denmark), 7 were from the UK, 7 were from Canada, 2 in France, and 1 each from Australia, South Africa, Switzerland and USA. Only five studies were from the employer’s perspectives. One study included in the review did not specify the type of chronic pain, but the majority of the studies involved people or employers of people with musculoskeletal pain, mainly affecting the back and neck, and some were injury/work-related. Studies of people with musculoskel-etal disease, including arthritis, fibromyalgia and systemic lupus erythematosus, were also included (table 1).
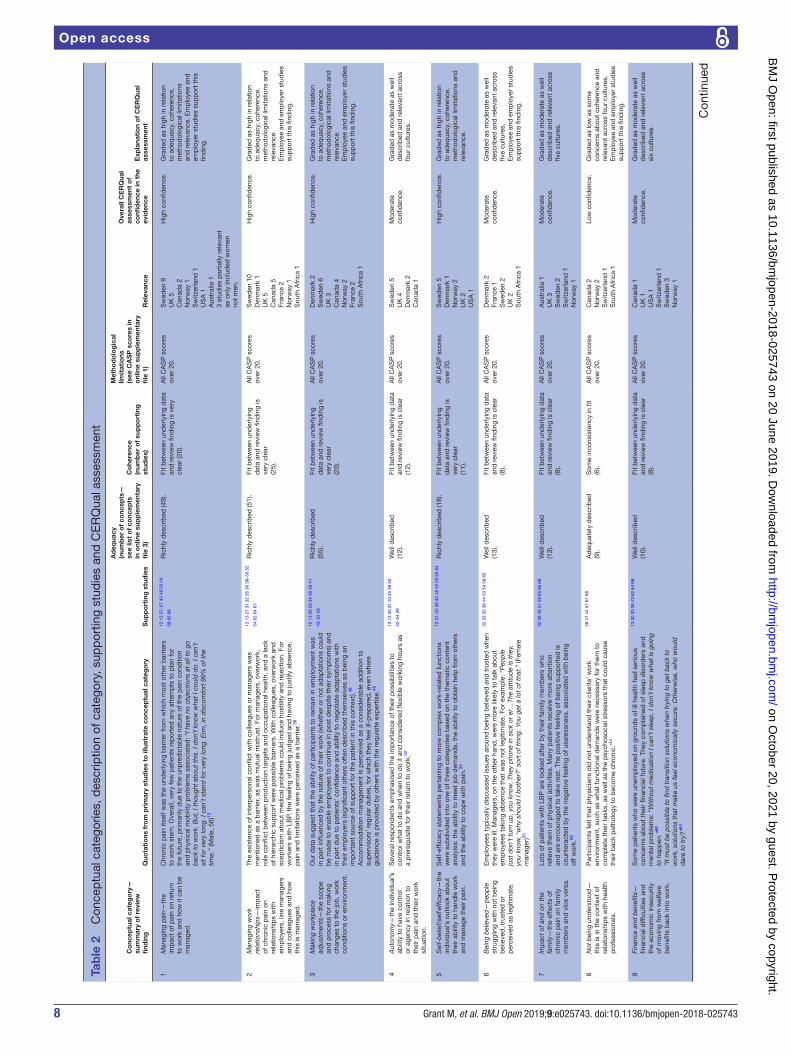
overarching conceptual categoriesA total of 342 concepts were clustered into 16 concep-tual categories summarised in table 2. The first column of table 2 contains third-order concepts. We worked with second-order concepts, and the second column of table 2 is second-order data, some of which are illustrated with first-order participant quotations. This table also high-lights the CERQual profile. The three key conceptual cate-gories identified by the team are described in this section. The balancing of these three inter-related categories
Figure 1 Flow chart illustrating search outcome.
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from

4 Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
Tab
le 1
D
escr
iptio
n of
incl
uded
stu
die
s
Aut
hor
and
yea
r o
f p
ublic
atio
nC
oun
try
Typ
e o
f p
ain
Num
ber
, gen
der
and
ag
e o
f p
arti
cip
ants
Par
tici
pan
tsM
etho
ds
of
dat
a co
llect
ion
Met
hod
olo
gic
al a
pp
roac
h—an
alys
is
1A
hlst
rom
et
al,12
201
7S
wed
enN
eck
pai
n.16
wom
en, m
ean
age
of 5
4.P
eop
le w
ith h
isto
ry o
f lon
g-te
rm
sick
leav
e in
hum
an s
ervi
ce
orga
nisa
tions
.
Inte
rvie
ws.
Con
stru
ctiv
ist
grou
nded
the
ory
app
roac
h.
2A
nder
sen
et a
l,42 2
014
Den
mar
kB
ack
or u
pp
er b
ody.
4 m
en a
nd 3
wom
en a
ged
33–
57.
Par
ticip
ants
in c
hron
ic p
ain
self-
man
agem
ent
pro
gram
me
or t
ailo
red
phy
sica
l act
ivity
p
rogr
amm
e.
Sem
istr
uctu
red
in
terv
iew
s.S
yste
mat
ic t
ext
cond
ensa
tion—
them
atic
cro
ss-c
ase
anal
ysis
.
3A
ngel
et
al,53
201
2D
enm
ark
Low
bac
k p
ain.
20 (6
5% w
omen
), m
ean
age
of 4
6.P
artic
ipan
ts o
f cou
nsel
ling
inte
rven
tion
add
ress
ing
wor
kpla
ce
bar
riers
and
phy
sica
l act
ivity
.
Sem
istr
uctu
red
clin
ical
in
terv
iew
s.N
arra
tive
anal
ysis
.
4A
shb
y et
al,58
201
0A
ustr
alia
Chr
onic
low
bac
k p
ain.
11 m
en a
ged
23–
59.
Par
ticip
ants
in a
wor
k ha
rden
ing
pro
gram
me.
Sem
istr
uctu
red
inte
rvie
ws
(eth
nogr
aphi
c).
Them
atic
con
tent
ana
lysi
s.
5B
rook
s et
al,48
201
3E
ngla
ndP
ersi
sten
t, n
on-
spec
ific
low
bac
k p
ain
of a
t le
ast
12 w
eeks
in
dur
atio
n.
6 w
omen
and
3 m
en.
Wor
king
par
ticip
ants
(5) a
ged
45–
52
(mea
n 49
.2).
Une
mp
loye
d p
artic
ipan
ts (4
) age
d
51–6
3 (m
ean
57) a
nd t
heir
sign
ifica
nt
othe
rs.
Par
ticip
ants
from
hos
pita
l pai
n m
anag
emen
t cl
inic
.S
emis
truc
ture
d
inte
rvie
ws.
Tem
pla
te a
naly
sis
styl
e of
the
mat
ic
anal
ysis
.
6B
uus
et a
l,59 2
015
Den
mar
kLo
w b
ack
pai
n.25
(56%
wom
en) (
mea
n ag
e 46
.8).
Peo
ple
who
had
rec
eive
d
coun
selli
ng in
terv
entio
n d
esig
ned
to
mot
ivat
e th
em t
o ch
ange
wor
k ro
utin
es a
nd e
xerc
ise.
Sem
istr
uctu
red
in
terv
iew
s.In
terp
reta
tive
them
atic
ana
lysi
s.
7C
oole
et
al,45
201
0U
KLo
w b
ack
pai
n.13
wom
en a
nd 1
2 m
en a
ged
22–
58 y
ears
(mea
n ag
e 44
.7).
Peo
ple
offe
red
MD
T b
ack
pai
n re
hab
ilita
tion
and
con
cern
ed a
bou
t ab
ility
to
wor
k d
ue t
o lo
w b
ack
pai
n.
Sem
istr
uctu
red
in
terv
iew
s.Th
emat
ic a
naly
sis.
8C
outu
et
al,37
201
0C
anad
aP
ersi
sten
t m
uscu
losk
elet
al p
ain—
bac
k p
ain
(10)
, up
per
ex
trem
ities
(4),
mix
ed
(2).
10 m
en a
nd 6
wom
en a
ged
25–
56
(mea
n ag
e 40
).W
orke
rs r
efer
red
to
wor
k re
hab
p
rogr
amm
e.S
emis
truc
ture
d
inte
rvie
ws.
Nar
rativ
e ap
pro
ach—
cont
ent
anal
ysis
.
9C
outu
et
al,60
201
1C
anad
aM
SD
-rel
ated
pai
n fo
r m
ore
than
12
wee
ks a
ccep
ted
an
d c
omp
ensa
ted
b
y Q
ueb
ec W
orke
rs’
Com
pen
satio
n B
oard
.B
ack
pai
n (1
0), u
pp
er
extr
emiti
es (4
), m
ixed
(2
).
16 w
orke
rs: 1
0 m
en, 6
wom
en, a
ged
25
–56
year
s (m
ean
age
40).
Ref
erre
d t
o ev
iden
ce-b
ased
wor
k re
hab
pro
gram
me
by
a th
ird-p
arty
p
ayer
.
Sem
istr
uctu
red
in
terv
iew
s.C
onte
nt a
naly
sis.
10C
outu
et
al,61
201
3C
anad
aM
SD
-rel
ated
pai
n fo
r m
ore
than
12
wee
ks a
ccep
ted
an
d c
omp
ensa
ted
b
y Q
ueb
ec W
orke
rs’
Com
pen
satio
n B
oard
.B
ack
pai
n (8
), up
per
ex
trem
ities
(2),
bot
h (2
).
12 w
orke
rs (8
men
and
4 w
omen
) age
d
25–5
6 (m
ean
age
31) a
nd 5
clin
icia
ns.
Par
ticip
ants
from
wor
kers
sta
rtin
g a
wor
k re
hab
pro
gram
me
at a
ho
spita
l res
earc
h ce
ntre
.
Mul
tiple
cas
e st
udy
des
ign:
sem
istr
uctu
red
in
terv
iew
s w
ith w
orke
rs
and
reh
ab c
linic
ians
at
four
poi
nts
in t
ime.
Them
atic
ana
lysi
san
d c
onst
ant
com
par
ison
met
hod
(g
roun
ded
the
ory)
.
Con
tinue
d
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from

5Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
Aut
hor
and
yea
r o
f p
ublic
atio
nC
oun
try
Typ
e o
f p
ain
Num
ber
, gen
der
and
ag
e o
f p
arti
cip
ants
Par
tici
pan
tsM
etho
ds
of
dat
a co
llect
ion
Met
hod
olo
gic
al a
pp
roac
h—an
alys
is
11C
rook
s,43
200
7C
anad
aM
SD
(fib
rom
yalg
ia,
arth
ritis
, RA
, OA
, lup
us).
18 w
omen
age
d 2
6–69
(mea
n ag
e 44
).W
omen
who
dev
elop
ed M
SD
whi
le
invo
lved
in t
he la
bou
r m
arke
t.In
dep
th in
terv
iew
s.Th
emat
ic a
naly
sis.
12D
ionn
e et
al,50
201
3C
anad
aW
ork-
dis
ablin
g b
ack
pai
n.W
orke
rs w
ith w
ork-
dis
ablin
g b
ack
pai
n.9=
retu
rned
to w
ork
(7 m
en, 2
wom
en)
aged
30–
59.
10=
not r
etur
ned
or
rece
ntly
ret
urne
d (7
m
en, 2
wom
en) a
ged
30–
60+
.
Rec
ruite
d t
hrou
gh n
ewsp
aper
ad
vert
s.Fo
cus
grou
ps
(2).
Con
tent
ana
lysi
s.
13E
dén
et
al,52
200
7S
wed
enM
SD
(typ
e no
t sp
ecifi
ed).
17 in
div
idua
ls (2
men
, 15
wom
en) a
ged
41
–62
year
s.P
eop
le g
oing
bac
k to
wor
k b
y m
eans
of t
he S
wed
ish
‘res
ting
dis
abili
ty p
ensi
on’.
Inte
rvie
ws.
Ind
uctiv
e an
alys
is r
elev
ant
to
rese
arch
que
stio
n.
14*
Fass
ier
et a
l,38 2
015
Fran
ceLo
w b
ack
pai
n.3
emp
loye
rs, 1
man
ager
and
1 w
orke
r.R
ecru
ited
from
wor
kpla
ces
with
hi
gh r
ates
of a
bse
nce
for
low
b
ack
pai
n—ca
r m
aker
, ass
ocia
tion
pro
vid
ing
hom
e se
rvic
es fo
r th
e d
epen
den
t an
d t
wo
univ
ersi
ty
hosp
itals
.
Inte
rvie
ws
and
focu
s gr
oup
s.Q
ualit
ativ
e co
nten
t an
alys
is.
15G
ard
and
San
db
erg,
40 1
998
Sw
eden
Mus
culo
skel
etal
pai
n (s
houl
der
, nec
k an
d lo
w
bac
k p
ain)
for
at le
ast
1 ye
ar w
ith a
per
iod
of
at le
ast
4 w
eeks
dur
ing
that
tim
e.
10 p
atie
nts
(9 w
omen
, 1 m
an) a
ged
30
–54
year
s (m
ean
age
47).
Peo
ple
sic
k-lis
ted
with
m
uscu
losk
elet
al p
ain.
Inte
rvie
ws
with
a lo
w
deg
ree
of s
truc
ture
.P
heno
men
olog
ical
str
uctu
ral
anal
ysis
.
16G
lava
re e
t al
,54 2
012
Sw
eden
Long
-ter
m
mus
culo
skel
etal
pai
n (w
hip
lash
, fib
rom
yalg
ia,
nerv
e in
jury
(nec
k),
arth
rosi
s of
the
foot
).
11 (8
wom
en a
nd 3
men
) age
d 2
2–58
(m
edia
n ag
e 39
).P
artic
ipan
ts in
a m
ultip
rofe
ssio
nal
pai
n re
hab
pro
gram
me
follo
wed
b
y a
coac
hed
wor
k-tr
aini
ng
pro
gram
me.
Them
atis
ed r
esea
rch
inte
rvie
ws.
Gro
und
ed t
heor
y—co
nsta
nt
com
par
ativ
e m
etho
d.
17*
Gra
talo
up e
t al
,47 2
016
Fran
ceS
uper
viso
rs o
f peo
ple
w
ith m
uscu
losk
elet
al
dis
ord
ers.
Em
plo
yees
’ sup
ervi
sors
(61
char
ge
nurs
es, a
nd h
ead
nur
ses
sup
ervi
sing
on
e or
mor
e w
orke
rs w
ith r
estr
ictio
ns
for
heav
y lif
ting
or r
epet
itive
m
ovem
ents
).
Sta
ff fr
om 3
pub
lic h
osp
itals
.12
focu
s gr
oup
s (c
harg
e nu
rses
and
hea
d n
urse
s se
par
ate)
.
Them
atic
qua
litat
ive
anal
ysis
by
cons
tant
com
par
ison
, eac
h fo
cus
grou
p a
naly
sed
bef
ore
the
next
hel
d.
18H
anss
on e
t al
,30 2
001
Sw
eden
Sp
ine-
rela
ted
pai
n.5
peo
ple
(4 w
omen
and
1 m
an) a
ged
51
–64
(med
ian
55).
Peo
ple
gra
nted
dis
abili
ty p
ensi
on
in 1
996.
Inte
rvie
ws
cond
ucte
d a
s co
nver
satio
ns—
app
roac
h b
ased
on
sym
bol
ic
inte
ract
ioni
sm.
Bas
ed o
n gr
ound
ed t
heor
y.
19H
anss
on e
t al
,34 2
006
Sw
eden
Nec
k or
low
bac
k p
ain
(sp
ine-
rela
ted
pai
n).
33 (2
0 w
omen
and
13
men
) age
d
32–6
1 ye
ars
(med
ian
age
48).
Sic
k-lis
ted
par
ticip
ants
.Q
ualit
ativ
e in
terv
iew
s.Q
ualit
ativ
e an
alys
is.
20Jo
hans
son
et a
l,62 1
997
Sw
eden
Und
efine
d
mus
culo
skel
etal
pai
n d
isor
der
s.
20 fe
mal
e p
atie
nts
aged
21–
61.
Wom
en s
ick-
liste
d d
ue t
o M
SD
in
urb
an h
ealth
cen
tre.
Rep
eate
d t
hem
atic
in
terv
iew
s.G
roun
ded
the
ory.
21Ju
uso
et a
l,27 2
016
Sw
eden
Fib
rom
yalg
ia.
15 w
omen
age
d 3
8–64
(med
ian
54).
From
a r
ehab
ilita
tion
cent
re (4
), as
soci
atio
ns fo
r rh
eum
atis
m a
nd
FM (1
1).
Ind
epth
qua
litat
ive
inte
rvie
ws.
Her
men
eutic
ap
pro
ach.
22K
alsi
et
al,31
201
6U
KC
hron
ic p
ain
(typ
e no
t sp
ecifi
ed).
17 p
atie
nts
(8 m
en, 9
wom
en) a
ged
18
–65+
, but
maj
ority
(14/
17) w
ere
18–3
4.
Pat
ient
s at
tend
ing
a 3-
wee
k, h
igh-
inte
nsity
pai
n m
anag
emen
t p
rogr
amm
e.
Sem
istr
uctu
red
focu
s gr
oup
dis
cuss
ion.
Them
atic
ana
lysi
s.
Tab
le 1
C
ontin
ued
Con
tinue
d
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from
6 Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
Aut
hor
and
yea
r o
f p
ublic
atio
nC
oun
try
Typ
e o
f p
ain
Num
ber
, gen
der
and
ag
e o
f p
arti
cip
ants
Par
tici
pan
tsM
etho
ds
of
dat
a co
llect
ion
Met
hod
olo
gic
al a
pp
roac
h—an
alys
is
23K
vam
et
al,63
201
3N
orw
ayP
rolo
nged
m
uscu
losk
elet
al p
ain
(uns
pec
ified
pai
n in
th
e b
ack,
nec
k an
d
shou
lder
s d
ue t
o fib
rom
yalg
ia, a
rthr
itis
and
rhe
umat
ism
).
4 m
en a
nd 6
wom
en a
ged
26–
57.
Volu
ntee
rs fr
om p
eop
le u
nder
goin
g vo
catio
nal r
ehab
ilita
tion.
Sem
istr
uctu
red
in
terv
iew
s.C
onst
ant
com
par
ativ
e an
alys
is.
24K
vam
and
Vik
,51 2
015
Nor
way
Pro
long
ed
mus
culo
skel
etal
pai
n (u
nsp
ecifi
ed p
ain
in
the
bac
k, n
eck
and
sh
ould
ers
due
to
fibro
mya
lgia
, art
hriti
s an
d r
heum
atis
m).
6 w
omen
, 4 m
en a
ged
26–
57.
Peo
ple
und
ergo
ing
voca
tiona
l re
hab
ilita
tion.
Ind
epth
inte
rvie
ws.
Dis
cour
se a
naly
sis.
25Li
edb
erg
and
Hen
rikss
on,36
200
2S
wed
enFi
bro
mya
lgia
.39
wom
en a
ged
35–
63 (m
ean
49.5
).P
atie
nts
from
a p
ain
and
reh
ab
cent
re.
Inte
rvie
ws.
Ana
lyse
d in
to c
ateg
orie
s an
d
sub
cate
gorie
s.
26M
agnu
ssen
et
al,64
200
7N
orw
ayB
ack
pai
n.12
wom
en, 5
men
age
d 3
8–56
yea
rs
(mea
n ag
e 49
).P
art
of a
larg
er s
tud
y ev
alua
ting
the
effe
ct o
f a v
ocat
iona
l reh
abili
tatio
n-re
late
d in
terv
entio
n.
Thre
e fo
cus
grou
ps.
Ana
lysi
s of
the
mes
and
sub
them
es.
27M
cClu
skey
et
al,65
201
1U
KP
ersi
sten
t b
ack
pai
n.5
dya
ds
(4 m
ale
and
1 fe
mal
e cl
aim
ants
), ag
ed 2
9–54
yea
rs (m
ean
age
40.2
).
Dis
abili
ty c
laim
ants
and
the
ir si
gnifi
cant
oth
ers.
Sem
istr
uctu
red
in
terv
iew
s.Te
mp
late
ana
lysi
s.
28M
cClu
skey
et
al,66
201
4U
KP
ersi
sten
t lo
w b
ack
pai
n.18
(9 b
enefi
ts c
laim
ants
: 5 m
en a
nd 4
w
omen
age
d 2
9–63
, mea
n ag
e 48
.1)
and
9 s
igni
fican
t ot
hers
(6 w
omen
and
3
men
age
d 2
1–68
, mea
n ag
e 49
.7).
Wor
k d
isab
ility
ben
efits
cla
iman
ts
and
sig
nific
ant
othe
rs.
Sem
istr
uctu
red
in
terv
iew
s.Te
mp
late
ana
lysi
s.
29N
ilsen
and
And
erss
en,28
201
4N
orw
ayN
on-m
alig
nant
chr
onic
p
ain
(nec
k an
d b
ack
pai
n, t
raffi
c in
jurie
s).
10 m
en a
nd 1
0 w
omen
age
d 2
6–63
(in
the
year
200
6), m
ean
age
42.7
.Fr
om a
sp
ecia
list
pai
n cl
inic
.O
pen
-end
ed in
terv
iew
s.N
arra
tive
anal
ysis
.P
heno
men
olog
ical
mea
ning
co
nden
satio
n fr
amew
ork.
30N
ord
qvi
st e
t al
,49 2
003
Sw
eden
Bac
k, n
eck
or s
houl
der
d
iagn
oses
.13
wom
en a
nd 5
men
.P
eop
le w
ho in
198
5 w
ere
25–
34 y
ears
old
and
had
a n
ew s
ick
leav
e sp
ell o
f at
leas
t 28
day
s.
5 fo
cus
grou
ps.
Gro
und
ed t
heor
y co
din
g an
d
cate
goris
ing.
31P
atel
et
al,13
200
7U
KC
hron
ic
mus
culo
skel
etal
pai
n.38
pat
ient
s (1
5 m
en, 2
3 w
omen
) age
d
29–6
2 ye
ars
(mea
n ag
e 49
.4).
Une
mp
loye
d a
nd in
rec
eip
t of
long
-te
rm s
ocia
l wel
fare
ben
efits
.In
dep
th, s
emis
truc
ture
d
inte
rvie
ws.
Fram
ewor
k ap
pro
ach
and
the
mat
ic
anal
ysis
.
32R
ydst
ad e
t al
,32 2
010
Sw
eden
Whi
pla
sh-a
ssoc
iate
d
dis
ord
ers.
9 p
eop
le (5
wom
en, 4
men
) age
d
32–5
3 ye
ars.
Par
ticip
ants
of a
wor
k-or
ient
ed
MD
T re
hab
pro
gram
me.
Them
atis
ed in
terv
iew
s.C
onst
ant
com
par
ison
met
hod
—gr
ound
ed t
heor
y.
33S
aund
ers
et a
l,67 2
015
Can
ada
MS
K in
jury
.A
rm (1
), kn
ee (1
), b
ack
inju
ries
(7).
9 p
eop
le (5
wom
en, 4
men
) age
d
34–5
6 ye
ars.
Peo
ple
with
long
-ter
m w
ork
dis
abili
ty a
nd jo
b lo
ss d
ue t
o an
M
SK
inju
ry fr
om w
ork
reha
b a
nd
chro
nic
pai
n p
rogr
amm
es.
Inte
rvie
ws
(27)
with
9
peo
ple
.Th
emat
ic a
naly
sis
(phe
nom
enol
ogic
al a
pp
roac
h gu
ided
b
y lif
e w
orld
con
cep
t).
34S
chee
rmes
ser
et a
l,68 2
012
Sw
itzer
land
Low
bac
k p
ain.
13 (9
men
, 4 w
omen
) age
d 3
8–60
yea
rs
(mea
n ag
e of
men
52,
mea
n ag
e of
w
omen
48)
.
Pat
ient
s w
ith a
Sou
thea
st
Eur
opea
n cu
ltura
l bac
kgro
und
at
tend
ing
a re
hab
cen
tre
in
Sw
itzer
land
.
Ind
epth
, sem
istr
uctu
red
in
terv
iew
s (5
) and
2 fo
cus
grou
ps.
Qua
litat
ive
cont
ent
anal
ysis
.
Tab
le 1
C
ontin
ued
Con
tinue
d
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from

7Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
Aut
hor
and
yea
r o
f p
ublic
atio
nC
oun
try
Typ
e o
f p
ain
Num
ber
, gen
der
and
ag
e o
f p
arti
cip
ants
Par
tici
pan
tsM
etho
ds
of
dat
a co
llect
ion
Met
hod
olo
gic
al a
pp
roac
h—an
alys
is
35S
haw
and
Hua
ng,33
200
5U
SA
Occ
upat
iona
l low
bac
k p
ain.
Focu
s gr
oup
: 28
peo
ple
(15
men
, 13
wom
en) a
ged
31–
65 (m
ean
age
46).
Inte
rvie
wee
s: 2
3 p
eop
le (1
1 m
en, 1
2 w
omen
) age
d 2
5–64
(mea
n ag
e 42
.6).
Focu
s gr
oup
par
ticip
ants
: peo
ple
re
cent
ly (<
6 m
onth
s) r
etur
ned
to
wor
k af
ter
inju
ry r
esp
ond
ing
to
new
spap
er a
dve
rt.
Inte
rvie
w p
artic
ipan
ts: p
atie
nts
refe
rred
by
phy
sios
from
co
llab
orat
ing
OH
net
wor
k.
Focu
s gr
oup
and
in
terv
iew
s.C
onte
nt a
naly
sis.
36S
jöst
röm
et
al,29
201
1S
wed
enM
SK
dis
ord
ers—
m
ainl
y b
ack
and
nec
k p
ain.
10 p
eop
le (7
wom
en, 3
men
) age
d
29–6
1 (m
ean
age
48).
Att
end
ed a
reh
ab p
rogr
amm
e an
d
still
on
full-
time
sick
leav
e 2
year
s af
ter
com
ple
tion.
Sem
istr
uctu
red
in
terv
iew
s.Q
ualit
ativ
e co
nten
t an
alys
is.
37S
oeke
r et
al,44
200
8S
outh
Afr
ica
Bac
k in
jury
.26
peo
ple
(18
men
, 8 w
omen
) age
d
18–6
0.S
elec
ted
by
rand
om s
amp
ling
from
a
hosp
ital r
ehab
dep
artm
ent.
Focu
s gr
oup
s.Q
ualit
ativ
e an
alys
is.
38*
Sok
larid
is e
t al
,41 2
010
Can
ada
Low
bac
k p
ain—
wor
k-re
late
d in
jury
.59
sta
keho
lder
s in
clud
ing
6 in
jure
d
wor
kers
and
5 s
mal
l and
9 la
rge
emp
loye
rs.
Vario
us c
onta
cts
of t
he r
esea
rch
team
.9
focu
s gr
oup
s.G
roun
ded
the
ory
app
roac
h.
39S
vens
son
et a
l,39 2
010
Sw
eden
Bac
k ne
ck o
r sh
ould
er
dia
gnos
is.
13 w
omen
and
5 m
en.
Peo
ple
age
d 2
5–34
yea
rs o
ld in
19
85 a
nd h
ad a
new
sic
k le
ave
spel
l of a
t le
ast
28 d
ays.
5 fo
cus
grou
ps.
Des
crip
tive
and
exp
lora
tive
met
hod
of
ana
lysi
s.
40*
Will
iam
s-W
hitt
et
al,46
201
6C
anad
aLo
w b
ack
pai
n.23
sup
ervi
sors
.S
uper
viso
rs o
f bac
k-in
jure
d
wor
kers
from
11
Can
adia
n or
gani
satio
ns.
Sem
istr
uctu
red
, ind
epth
in
terv
iew
s.C
onst
ruct
ivis
t gr
ound
ed t
heor
y p
rinci
ple
s.
41*
Wyn
ne-J
ones
et
al,35
201
1W
ales
Mus
culo
skel
etal
pai
n.18
em
plo
yees
with
MS
K p
ain
(8 m
en,
10 w
omen
), m
ean
age
49.7
.20
man
ager
s (1
0 m
en, 1
0 w
omen
), m
ean
age
44.8
.
Two
larg
e p
ublic
sec
tor
orga
nisa
tions
.S
emis
truc
ture
d
inte
rvie
ws.
Them
atic
ana
lysi
s.
*Em
plo
yer
stud
ies.
FM, fi
bro
mya
lgia
; MD
T, m
ulti-
dis
cip
linar
y; M
SD
, mus
culo
skel
etal
dis
ord
ers;
MS
K, m
uscu
losk
elet
al; O
A, o
steo
arth
ritis
; OH
, occ
upat
iona
l hea
lth; R
A, r
heum
atoi
d a
rthr
itis.
Tab
le 1
C
ontin
ued
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from
8 Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
Tab
le 2
C
once
ptu
al c
ateg
orie
s, d
escr
iptio
n of
cat
egor
y, s
upp
ortin
g st
udie
s an
d C
ER
Qua
l ass
essm
ent
Co
ncep
tual
cat
ego
ry—
sum
mar
y o
f re
view
fi
ndin
gQ
uota
tio
ns f
rom
pri
mar
y st
udie
s to
illu
stra
te c
onc
eptu
al c
ateg
ory
Sup
po
rtin
g s
tud
ies
Ad
equa
cy(n
umb
er o
f co
ncep
ts—
see
list
of
conc
epts
in
onl
ine
sup
ple
men
tary
fi
le 3
)
Co
here
nce
(num
ber
of
sup
po
rtin
g
stud
ies)
Met
hod
olo
gic
al
limit
atio
ns(s
ee C
AS
P s
core
s in
o
nlin
e su
pp
lem
enta
ry
file
1)
Rel
evan
ce
Ove
rall
CE
RQ
ual
asse
ssm
ent
of
confi
den
ce in
the
ev
iden
ceE
xpla
nati
on
of
CE
RQ
ual
asse
ssm
ent
1M
anag
ing
pai
n—th
e im
pac
t of
pai
n on
ret
urn
to w
ork
and
how
it c
an b
e m
anag
ed.
Chr
onic
pai
n its
elf w
as t
he u
nder
lyin
g b
arrie
r fr
om w
hich
mos
t ot
her
bar
riers
to
wor
k st
em. O
vera
ll, v
ery
few
pat
ient
s re
por
ted
any
att
emp
ts t
o p
lan
for
the
futu
re, p
rimar
ily d
ue t
o th
e un
pre
dic
tab
le n
atur
e of
the
pai
n co
nditi
on
and
phy
sica
l mob
ility
pro
ble
ms
asso
ciat
ed: “
I hav
e no
ob
ject
ions
at
all t
o go
b
ack
to w
ork.
But
, I t
houg
ht a
bou
t th
is. I
don
’t kn
ow w
hat
I cou
ld d
o. I
can’
t si
t fo
r ve
ry lo
ng. I
can
’t st
and
for
very
long
. Erm
, in
dis
com
fort
99%
of t
he
time.
” (M
ale,
56)
13
12 1
3 27
–37
40 4
8 50
54
58 6
5 68
Ric
hly
des
crib
ed (4
9).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is v
ery
clea
r (2
0).
All
CA
SP
sco
res
over
20.
Sw
eden
9U
K 5
Can
ada
2N
orw
ay 1
Sw
itzer
land
1U
SA
1A
ustr
alia
13
stud
ies
par
tially
rel
evan
t as
onl
y in
clud
ed w
omen
no
t m
en.
Hig
h co
nfid
ence
.G
rad
ed a
s hi
gh in
rel
atio
n to
ad
equa
cy, c
oher
ence
, m
etho
dol
ogic
al li
mita
tions
an
d r
elev
ance
. Em
plo
yee
and
em
plo
yer
stud
ies
sup
por
t th
is
find
ing.
2M
anag
ing
wor
k re
latio
nshi
ps—
imp
act
of c
hron
ic p
ain
on
rela
tions
hip
s w
ith
emp
loye
rs, l
ine
man
ager
s an
d c
olle
ague
s an
d h
ow
this
is m
anag
ed.
The
exis
tenc
e of
inte
rper
sona
l con
flict
with
col
leag
ues
or m
anag
ers
was
m
entio
ned
as
a b
arrie
r, as
was
mut
ual m
istr
ust.
For
man
ager
s, o
verw
ork,
ro
le c
onfli
ct b
etw
een
pro
duc
tion
targ
ets
and
occ
upat
iona
l hea
lth, a
nd a
lack
of
hie
rarc
hic
sup
por
t w
ere
pos
sib
le b
arrie
rs. W
ith c
olle
ague
s, o
verw
ork
and
sc
eptic
ism
ab
out
med
ical
pro
ble
ms
coul
d in
duc
e ho
stili
ty a
nd r
ejec
tion.
For
w
orke
rs w
ith L
BP,
the
feel
ing
of b
eing
jud
ged
and
hav
ing
to ju
stify
ab
senc
e,
pai
n an
d li
mita
tions
wer
e p
erce
ived
as
a b
arrie
r.38
12 1
3 27
31
32 3
5 36
38–
50 5
2
54 6
2 64
67
Ric
hly
des
crib
ed (5
1).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is
very
cle
ar(2
5).
All
CA
SP
sco
res
over
20.
Sw
eden
10
Den
mar
k 1
UK
5C
anad
a 5
Fran
ce 2
Nor
way
1S
outh
Afr
ica
1
Hig
h co
nfid
ence
.G
rad
ed a
s hi
gh in
rel
atio
n to
ad
equa
cy, c
oher
ence
, m
etho
dol
ogic
al li
mita
tions
and
re
leva
nce.
Em
plo
yee
and
em
plo
yer
stud
ies
sup
por
t th
is fi
ndin
g.
3M
akin
g w
orkp
lace
ad
just
men
ts—
the
scop
e an
d p
roce
ss fo
r m
akin
g ch
ange
s to
the
job
, wor
k co
nditi
ons
or e
nviro
nmen
t.
Our
dat
a su
gges
t th
at t
he a
bili
ty o
f par
ticip
ants
to
rem
ain
in e
mp
loym
ent
was
in
par
t in
fluen
ced
by
the
natu
re o
f the
ir w
ork
(whe
ther
or
not
adap
tatio
ns c
ould
b
e m
ade
to e
nab
le e
mp
loye
es t
o co
ntin
ue in
pos
t d
esp
ite t
heir
sym
pto
ms)
and
in
par
t d
ue t
o p
atie
nts’
con
fiden
ce a
nd a
bili
ty t
o ne
gotia
te a
dap
tatio
ns w
ith
thei
r em
plo
yers
(sig
nific
ant
othe
rs o
ften
des
crib
ed t
hem
selv
es a
s b
eing
an
imp
orta
nt s
ourc
e of
sup
por
t fo
r th
e p
atie
nt in
thi
s co
ntex
t).48
Acc
omm
odat
ion
man
agem
ent
is p
erce
ived
as
a co
nsid
erab
le a
dd
ition
to
sup
ervi
sors
’ reg
ular
dut
ies,
for
whi
ch t
hey
feel
ill-
pre
par
ed, e
ven
whe
re
guid
ance
is p
rovi
ded
by
othe
rs w
ith t
he r
equi
site
exp
ertis
e.46
12 1
3 28
29
34 3
6 38
41
43–5
3 59
Ric
hly
des
crib
ed(5
5).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is
very
cle
ar(2
0).
All
CA
SP
sco
res
over
20.
Den
mar
k 2
Sw
eden
6U
K 3
Can
ada
4N
orw
ay 2
Fran
ce 2
Sou
th A
fric
a 1
Hig
h co
nfid
ence
.G
rad
ed a
s hi
gh in
rel
atio
n to
ad
equa
cy, c
oher
ence
, m
etho
dol
ogic
al li
mita
tions
and
re
leva
nce.
Em
plo
yee
and
em
plo
yer
stud
ies
sup
por
t th
is fi
ndin
g.
4A
uton
omy—
the
ind
ivid
ual’s
ab
ility
to
have
con
trol
or
age
ncy
in r
elat
ion
to
thei
r p
ain
and
the
ir w
ork
situ
atio
n.
Sev
eral
res
pon
den
ts e
mp
hasi
sed
the
imp
orta
nce
of t
heir
pos
sib
ilitie
s to
co
ntro
l wha
t to
do
and
whe
n to
do
it an
d c
onsi
der
ed fl
exib
le w
orki
ng h
ours
as
a p
rere
qui
site
for
thei
r re
turn
to
wor
k.52
12 1
3 30
31
40 4
5 48
50
52–5
4 59
Wel
l des
crib
ed(1
2).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is c
lear
(12)
.
All
CA
SP
sco
res
over
20.
Sw
eden
5U
K 4
Den
mar
k 2
Can
ada
1
Mod
erat
e co
nfid
ence
.G
rad
ed a
s m
oder
ate
as w
ell
des
crib
ed a
nd r
elev
ant
acro
ss
four
cul
ture
s.
5S
elf-
bel
ief/
self
effic
acy—
the
ind
ivid
ual’s
out
look
ab
out
thei
r ab
ility
to
hand
le w
ork
and
man
age
thei
r p
ain.
Sel
f-ef
ficac
y st
atem
ents
per
tain
ing
to m
ore
com
ple
x w
ork-
rela
ted
func
tions
w
ere
sub
div
ided
into
one
of t
hree
cat
egor
ies
bas
ed o
n th
e th
emat
ic c
onte
nt
anal
ysis
: the
ab
ility
to
mee
t jo
b d
eman
ds,
the
ab
ility
to
obta
in h
elp
from
oth
ers
and
the
ab
ility
to
cop
e w
ith p
ain.
33
12 3
1–33
39
40 4
8 52
53
63 6
4R
ichl
y d
escr
ibed
(18)
.Fi
t b
etw
een
und
erly
ing
dat
a an
d r
evie
w fi
ndin
g is
ve
ry c
lear
(11)
.
All
CA
SP
sco
res
over
20.
Sw
eden
5D
enm
ark
1N
orw
ay 2
UK
2U
SA
1
Hig
h co
nfid
ence
.G
rad
ed a
s hi
gh in
rel
atio
n to
ad
equa
cy, c
oher
ence
, m
etho
dol
ogic
al li
mita
tions
and
re
leva
nce.
6B
eing
bel
ieve
d—
peo
ple
st
rugg
ling
with
not
bei
ng
bel
ieve
d, t
rust
ed o
r p
erce
ived
as
legi
timat
e.
Em
plo
yees
typ
ical
ly d
iscu
ssed
issu
es a
roun
d b
eing
bel
ieve
d a
nd t
rust
ed w
hen
they
wer
e ill
. Man
ager
s, o
n th
e ot
her
hand
, wer
e m
ore
likel
y to
tal
k ab
out
emp
loye
es t
akin
g ab
senc
e th
at w
as n
ot le
gitim
ate.
For
exa
mp
le: “
Peo
ple
ju
st d
on’t
turn
up
, you
kno
w. T
hey
pho
ne in
sic
k or
er…
The
attit
ude
is t
hey,
yo
u kn
ow, ‘
why
sho
uld
I b
othe
r?’ s
ort
of t
hing
. You
get
a lo
t of
tha
t.”
(Fem
ale
man
ager
)35
32 3
3 35
38
44 5
3 54
59
65W
ell d
escr
ibed
(13)
.Fi
t b
etw
een
und
erly
ing
dat
a an
d r
evie
w fi
ndin
g is
cle
ar(8
).
All
CA
SP
sco
res
over
20.
Den
mar
k 2
Fran
ce 1
Sw
eden
2U
K 2
Sou
th A
fric
a 1
Mod
erat
e co
nfid
ence
.G
rad
ed a
s m
oder
ate
as w
ell
des
crib
ed a
nd r
elev
ant
acro
ss
five
cultu
res.
Em
plo
yee
and
em
plo
yer
stud
ies
sup
por
t th
is fi
ndin
g.
7Im
pac
t of
and
on
the
fam
ily—
the
effe
cts
of
chro
nic
pai
n on
fam
ily
mem
ber
s an
d v
ice
vers
a.
Lots
of p
atie
nts
with
LB
P a
re lo
oked
aft
er b
y th
eir
fam
ily m
emb
ers
who
re
lieve
the
m o
f phy
sica
l act
iviti
es. M
any
pat
ient
s re
ceiv
e m
ore
atte
ntio
n an
d a
re e
ncou
rage
d t
o ta
ke r
est.
The
pos
itive
feel
ing
of b
eing
sup
por
ted
is
coun
tera
cted
by
the
nega
tive
feel
ing
of u
sele
ssne
ss, a
ssoc
iate
d w
ith b
eing
of
f wor
k.68
32 3
6 48
51
58 6
5 66
68
Wel
l des
crib
ed(1
3).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is c
lear
(8).
All
CA
SP
sco
res
over
20.
Aus
tral
ia 1
UK
3S
wed
en 2
Sw
itzer
land
1N
orw
ay 1
Mod
erat
e co
nfid
ence
.G
rad
ed a
s m
oder
ate
as w
ell
des
crib
ed a
nd r
elev
ant
acro
ss
five
cultu
res.
8N
ot b
eing
und
erst
ood
—th
is is
in t
he c
onte
xt o
f re
latio
nshi
ps
with
hea
lth
pro
fess
iona
ls.
Par
ticip
ants
felt
that
phy
sici
ans
did
not
und
erst
and
the
ir cl
ient
s’ w
ork
envi
ronm
ent,
suc
h as
wha
t fu
nctio
nal d
eman
ds
wer
e ne
cess
ary
for
them
to
com
ple
te t
heir
task
s, a
s w
ell a
s th
e p
sych
osoc
ial s
tres
sors
tha
t co
uld
cau
se
thei
r b
ack
pat
holo
gy t
o b
ecom
e ch
roni
c.’44
28 4
1 44
51
61 6
8A
deq
uate
ly d
escr
ibed
(9).
Som
e in
cons
iste
ncy
in fi
t(6
).A
ll C
AS
P s
core
s ov
er 2
0.C
anad
a 2
Nor
way
2S
witz
erla
nd 1
Sou
th A
fric
a 1
Low
con
fiden
ce.
Gra
ded
as
low
as
som
e co
ncer
ns a
bou
t co
here
nce
and
re
leva
nt a
cros
s fo
ur c
ultu
res.
Em
plo
yee
and
em
plo
yer
stud
ies
sup
por
t th
is fi
ndin
g.
9Fi
nanc
e an
d b
enefi
ts—
finan
cial
diffi
culti
es a
nd
the
econ
omic
inse
curit
y of
mov
ing
from
wel
fare
b
enefi
ts b
ack
into
wor
k.
Som
e p
atie
nts
who
wer
e un
emp
loye
d o
n gr
ound
s of
ill h
ealth
had
ser
ious
co
ncer
ns a
bou
t th
eir
finan
cial
futu
re. T
hey
com
pla
ined
of s
leep
dis
ord
ers
and
m
enta
l pro
ble
ms:
“W
ithou
t m
edic
atio
n I c
an’t
slee
p. I
don
’t kn
ow w
hat
is g
oing
to
hap
pen
.”68
“It
mus
t b
e p
ossi
ble
to
find
tra
nsiti
on s
olut
ions
whe
n tr
ying
to
get
bac
k to
w
ork,
sol
utio
ns t
hat
mak
e us
feel
eco
nom
ical
ly s
ecur
e. O
ther
wis
e, w
ho w
ould
d
are
to t
ry?”
64
13 3
0 33
36
43 6
2 64
68
Wel
l des
crib
ed(1
0).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is c
lear
(8).
All
CA
SP
sco
res
over
20.
Can
ada
1U
K 1
US
A 1
Sw
itzer
land
1S
wed
en 3
Nor
way
1
Mod
erat
e co
nfid
ence
.G
rad
ed a
s m
oder
ate
as w
ell
des
crib
ed a
nd r
elev
ant
acro
ss
six
cultu
res.
Con
tinue
d
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from
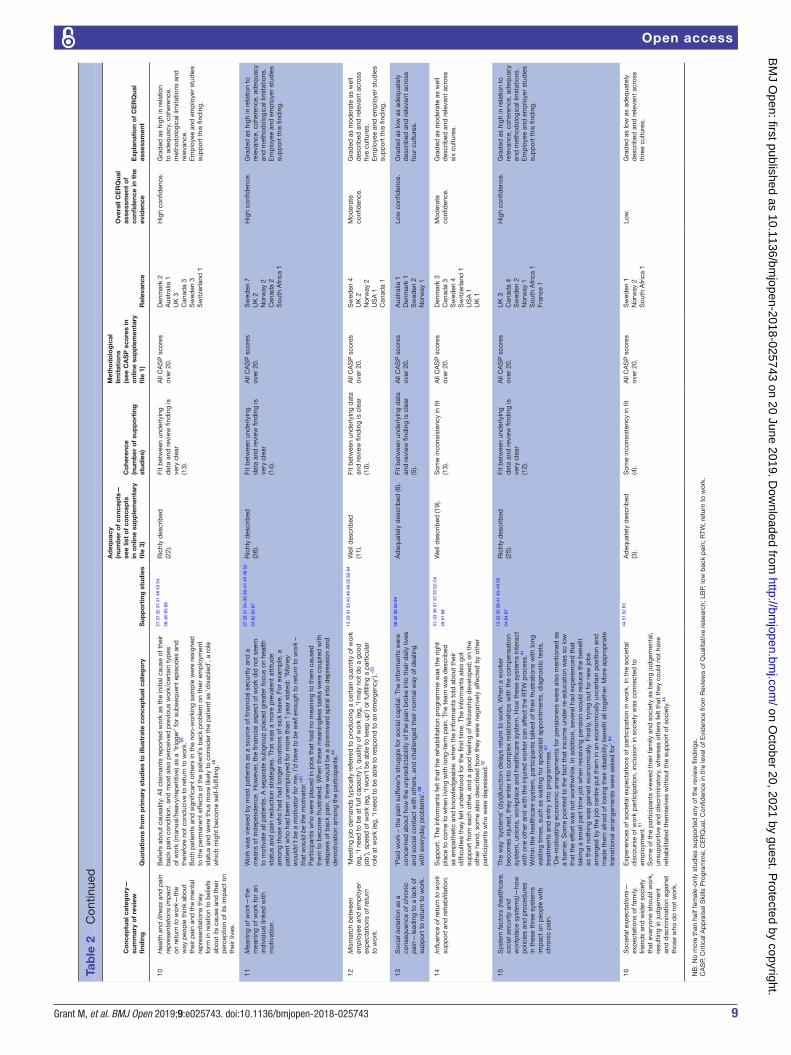
9Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
Co
ncep
tual
cat
ego
ry—
sum
mar
y o
f re
view
fi
ndin
gQ
uota
tio
ns f
rom
pri
mar
y st
udie
s to
illu
stra
te c
onc
eptu
al c
ateg
ory
Sup
po
rtin
g s
tud
ies
Ad
equa
cy(n
umb
er o
f co
ncep
ts—
see
list
of
conc
epts
in
onl
ine
sup
ple
men
tary
fi
le 3
)
Co
here
nce
(num
ber
of
sup
po
rtin
g
stud
ies)
Met
hod
olo
gic
al
limit
atio
ns(s
ee C
AS
P s
core
s in
o
nlin
e su
pp
lem
enta
ry
file
1)
Rel
evan
ce
Ove
rall
CE
RQ
ual
asse
ssm
ent
of
confi
den
ce in
the
ev
iden
ceE
xpla
nati
on
of
CE
RQ
ual
asse
ssm
ent
10H
ealth
and
illn
ess
and
pai
n re
pre
sent
atio
ns im
pac
t on
ret
urn
to w
ork—
the
way
peo
ple
thi
nk a
bou
t th
eir
pai
n an
d t
he m
enta
l re
pre
sent
atio
ns t
hey
form
in r
elat
ion
to b
elie
fs
abou
t its
cau
se a
nd t
heir
per
cep
tion
of it
s im
pac
t on
th
eir
lives
.
Bel
iefs
ab
out
caus
ality
. All
clai
man
ts r
epor
ted
wor
k as
the
initi
al c
ause
of t
heir
bac
k p
ain
cond
ition
, and
mos
t al
so p
erce
ived
pre
viou
s w
ork/
cert
ain
typ
es
of w
ork
(man
ual/h
eavy
/rep
etiti
ve) a
s a
‘trig
ger’
for
sub
seq
uent
ep
isod
es a
nd
ther
efor
e no
t co
nduc
ive
to r
etur
n to
wor
k.65
Bot
h p
atie
nts
and
sig
nific
ant
othe
rs in
the
non
-wor
king
sam
ple
wer
e re
sign
ed
to t
he p
erm
anen
t ef
fect
s of
the
pat
ient
’s b
ack
pro
ble
m o
n th
eir
emp
loym
ent
stat
us a
nd w
ere
thus
mor
e lik
ely
to c
onsi
der
the
pat
ient
as
‘dis
able
d’,
a ro
le
whi
ch m
ight
bec
ome
self-
fulfi
lling
.48
27 3
1 32
37
41 4
8 53
54
58–6
0 65
68
Ric
hly
des
crib
ed(2
2).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is
very
cle
ar(1
3).
All
CA
SP
sco
res
over
20.
Den
mar
k 2
Aus
tral
ia 1
UK
3C
anad
a 3
Sw
eden
3S
witz
erla
nd 1
Hig
h co
nfid
ence
.G
rad
ed a
s hi
gh in
rel
atio
n to
ad
equa
cy, c
oher
ence
, m
etho
dol
ogic
al li
mita
tions
and
re
leva
nce.
Em
plo
yee
and
em
plo
yer
stud
ies
sup
por
t th
is fi
ndin
g.
11M
eani
ng o
f wor
k—th
e m
eani
ng o
f wor
k fo
r an
in
div
idua
l lin
ked
with
m
otiv
atio
n.
Wor
k w
as v
iew
ed b
y m
ost
pat
ient
s as
a s
ourc
e of
fina
ncia
l sec
urity
and
a
mea
ns o
f ind
epen
den
ce. H
owev
er, t
he fi
nanc
ial a
spec
t of
wor
k d
id n
ot s
eem
to
mot
ivat
e al
l pat
ient
s. A
sep
arat
e su
bgr
oup
pla
ced
gre
ater
focu
s on
hea
lth
stat
us a
nd p
ain
red
uctio
n st
rate
gies
. Thi
s w
as a
mor
e p
reva
lent
att
itud
e am
ong
thos
e w
ho h
ad h
ad lo
nger
dur
atio
ns o
f sic
k le
ave.
For
exa
mp
le, a
p
atie
nt w
ho h
ad b
een
unem
plo
yed
for
mor
e th
an 1
yea
r st
ated
: “M
oney
w
ould
n’t
be
a m
otiv
ator
for
me,
I’d
hav
e to
be
wel
l eno
ugh
to r
etur
n to
wor
k –
that
wou
ld b
e th
e m
otiv
ator
.”31
Par
ticip
ants
who
wer
e p
lace
d in
job
s th
at h
ad n
o m
eani
ng t
o th
em c
ause
d
them
to
bec
ome
frus
trat
ed. W
hen
thes
e m
eani
ngle
ss t
asks
wer
e co
uple
d w
ith
rela
pse
s of
bac
k p
ain,
the
re w
ould
be
a d
ownw
ard
sp
iral i
nto
dep
ress
ion
and
d
emot
ivat
ion
amon
g th
e p
artic
ipan
ts.44
27 2
8 31
34–
36 3
9–41
44
46 5
2
54 6
2 63
67
Ric
hly
des
crib
ed(2
6).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is
very
cle
ar(1
4).
All
CA
SP
sco
res
over
20.
Sw
eden
7U
K 2
Nor
way
2C
anad
a 2
Sou
th A
fric
a 1
Hig
h co
nfid
ence
.G
rad
ed a
s hi
gh in
rel
atio
n to
re
leva
nce,
coh
eren
ce, a
deq
uacy
an
d m
etho
dol
ogic
al li
mita
tions
.E
mp
loye
e an
d e
mp
loye
r st
udie
s su
pp
ort
this
find
ing.
12M
ism
atch
bet
wee
n em
plo
yee
and
em
plo
yer
exp
ecta
tions
of r
etur
n to
wor
k.
‘Mee
ting
job
dem
and
s ty
pic
ally
ref
erre
d t
o p
rod
ucin
g a
cert
ain
qua
ntity
of w
ork
(eg,
‘I n
eed
to
be
at fu
ll ca
pac
ity’),
qua
lity
of w
ork
(eg,
‘I m
ay n
ot d
o a
good
jo
b’),
sp
eed
of w
ork
(eg,
‘I w
on’t
be
able
to
keep
up
’) or
fulfi
lling
a p
artic
ular
ro
le a
t w
ork
(eg,
‘I n
eed
to
be
able
to
resp
ond
to
an e
mer
genc
y’).’
33
13 2
9 31
33
40 4
6 49
52
63 6
4W
ell d
escr
ibed
(11)
.Fi
t b
etw
een
und
erly
ing
dat
a an
d r
evie
w fi
ndin
g is
cle
ar(1
0).
All
CA
SP
sco
res
over
20.
Sw
eden
4U
K 2
Nor
way
2U
SA
1C
anad
a 1
Mod
erat
e co
nfid
ence
.G
rad
ed a
s m
oder
ate
as w
ell
des
crib
ed a
nd r
elev
ant
acro
ss
five
cultu
res.
Em
plo
yee
and
em
plo
yer
stud
ies
sup
por
t th
is fi
ndin
g.
13S
ocia
l iso
latio
n as
a
cons
eque
nce
of c
hron
ic
pai
n—le
adin
g to
a la
ck o
f su
pp
ort
to r
etur
n to
wor
k.
‘Pai
d w
ork
– th
e p
ain
suffe
rer’s
str
uggl
e fo
r so
cial
cap
ital.
The
info
rman
ts w
ere
conc
erne
d a
bou
t ho
w t
he u
npre
dic
tab
ility
of t
he p
ain
bro
ke in
to t
heir
dai
ly li
ves
and
soc
ial c
onta
ct w
ith o
ther
s, a
nd c
halle
nged
the
ir no
rmal
way
of d
ealin
g w
ith e
very
day
pro
ble
ms’
.28
28 3
2 36
58
59A
deq
uate
ly d
escr
ibed
(6).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is c
lear
(5).
All
CA
SP
sco
res
over
20.
Aus
tral
ia 1
Den
mar
k 1
Sw
eden
2N
orw
ay 1
Low
con
fiden
ce.
Gra
ded
as
low
as
adeq
uate
ly
des
crib
ed a
nd r
elev
ant
acro
ss
four
cul
ture
s.
14In
fluen
ce o
f ret
urn
to w
ork
sup
por
t an
d r
ehab
ilita
tion.
Sup
por
t. T
he in
form
ants
felt
that
the
reh
abili
tatio
n p
rogr
amm
e w
as t
he r
ight
p
lace
to
com
e to
whe
n liv
ing
with
long
-ter
m p
ain.
The
tea
m w
as d
escr
ibed
as
em
pat
hetic
and
kno
wle
dge
able
: whe
n th
e in
form
ants
tol
d a
bou
t th
eir
diffi
culti
es t
hey
felt
und
erst
ood
for
the
first
tim
e. T
he in
form
ants
als
o go
t su
pp
ort
from
eac
h ot
her,
and
a g
ood
feel
ing
of fe
llow
ship
dev
elop
ed; o
n th
e ot
her
hand
, som
e al
so d
escr
ibed
how
the
y w
ere
nega
tivel
y af
fect
ed b
y ot
her
par
ticip
ants
who
wer
e d
epre
ssed
.32
31–3
3 36
37
42 5
0 52
–54
59 6
1 68
Wel
l des
crib
ed (1
9).
Som
e in
cons
iste
ncy
in fi
t(1
3).
All
CA
SP
sco
res
over
20.
Den
mar
k 3
Can
ada
3S
wed
en 4
Sw
itzer
land
1U
SA
1U
K 1
Mod
erat
e co
nfid
ence
.G
rad
ed a
s m
oder
ate
as w
ell
des
crib
ed a
nd r
elev
ant
acro
ss
six
cultu
res.
15S
yste
m fa
ctor
s (h
ealth
care
, so
cial
sec
urity
and
w
orkp
lace
sys
tem
s)—
how
p
olic
ies
and
pro
ced
ures
in
the
se t
hree
sys
tem
s im
pac
t on
peo
ple
with
ch
roni
c p
ain.
The
way
‘sys
tem
s’ (d
ys)fu
nctio
n d
elay
s re
turn
to
wor
k. W
hen
a w
orke
r b
ecom
es in
jure
d, t
hey
ente
r in
to c
omp
lex
rela
tions
hip
s w
ith t
he c
omp
ensa
tion
syst
em, u
nion
s, w
orkp
lace
and
hea
lthca
re s
yste
m. H
ow t
hese
sys
tem
s in
tera
ct
with
one
oth
er a
nd w
ith t
he in
jure
d w
orke
r ca
n af
fect
the
RTW
pro
cess
.41
With
in t
he h
ealth
care
sys
tem
, par
ticip
ants
tal
ked
of t
heir
frus
trat
ions
with
long
w
aitin
g tim
es, s
uch
as w
aitin
g fo
r sp
ecia
list
app
oint
men
ts, d
iagn
ostic
tes
ts,
trea
tmen
ts a
nd e
ntry
into
pro
gram
mes
.67
‘De-
mot
ivat
ing
econ
omic
arr
ange
men
ts fo
r p
ensi
oner
s w
ere
also
men
tione
d a
s a
bar
rier.
Som
e p
oint
ed t
o th
e fa
ct t
hat
inco
me
und
er r
e-ed
ucat
ion
was
so
low
th
at t
he e
ffort
was
not
wor
thw
hile
. In
add
ition
, sev
eral
had
exp
erie
nced
tha
t ta
king
a s
mal
l par
t tim
e jo
b w
hen
rece
ivin
g p
ensi
on w
ould
red
uce
the
ben
efit
so t
hat
noth
ing
was
gai
ned
eco
nom
ical
ly. F
inal
ly, t
ryin
g ou
t fo
r ne
w jo
bs
arra
nged
by
the
job
cen
tre
put
the
m in
an
econ
omic
ally
unc
erta
in p
ositi
on a
nd
mad
e th
em a
frai
d o
f los
ing
thei
r d
isab
ility
ben
efit
all t
oget
her.
Mor
e ap
pro
pria
te
tran
sitio
nal a
rran
gem
ents
wer
e as
ked
for’
.64
13 3
2 35
38
41 4
3–45
50
54 6
4 67
Ric
hly
des
crib
ed(2
5).
Fit
bet
wee
n un
der
lyin
g d
ata
and
rev
iew
find
ing
is
very
cle
ar(1
2).
All
CA
SP
sco
res
over
20.
UK
3C
anad
a 4
Sw
eden
2N
orw
ay 1
Sou
th A
fric
a 1
Fran
ce 1
Hig
h co
nfid
ence
.G
rad
ed a
s hi
gh in
rel
atio
n to
re
leva
nce,
coh
eren
ce, a
deq
uacy
an
d m
etho
dol
ogic
al li
mita
tions
.E
mp
loye
e an
d e
mp
loye
r st
udie
s su
pp
ort
this
find
ing.
16S
ocie
tal e
xpec
tatio
ns—
exp
ecta
tions
of f
amily
, fr
iend
s an
d w
ider
soc
iety
th
at e
very
one
shou
ld w
ork,
re
sulti
ng in
jud
gem
ent
and
dis
crim
inat
ion
agai
nst
thos
e w
ho d
o no
t w
ork.
Exp
erie
nces
of s
ocie
tal e
xpec
tatio
ns o
f par
ticip
atio
n in
wor
k. In
the
soc
ieta
l d
isco
urse
of w
ork
par
ticip
atio
n, in
clus
ion
in s
ocie
ty w
as c
onne
cted
to
emp
loym
ent.
51
Som
e of
the
par
ticip
ants
vie
wed
the
ir fa
mily
and
soc
iety
as
bei
ng ju
dge
men
tal,
unsu
pp
ortiv
e an
d d
iscr
imin
ator
y, w
here
as o
ther
s fe
lt th
at t
hey
coul
d n
ot h
ave
reha
bili
tate
d t
hem
selv
es w
ithou
t th
e su
pp
ort
of s
ocie
ty.44
44 5
1 52
63
Ad
equa
tely
des
crib
ed(3
).S
ome
inco
nsis
tenc
y in
fit
(4).
All
CA
SP
sco
res
over
20.
Sw
eden
1N
orw
ay 2
Sou
th A
fric
a 1
Low
.G
rad
ed a
s lo
w a
s ad
equa
tely
d
escr
ibed
and
rel
evan
t ac
ross
th
ree
cultu
res.
NB
: No
mor
e th
an h
alf f
emal
e-on
ly s
tud
ies
sup
por
ted
any
of t
he r
evie
w fi
ndin
gs.
CA
SP,
Crit
ical
Ap
pra
isal
Ski
lls P
rogr
amm
e; C
ER
Qua
l, C
onfid
ence
in t
he le
vel o
f Evi
den
ce fr
om R
evie
ws
of Q
ualit
ativ
e re
sear
ch; L
BP,
low
bac
k p
ain;
RTW
, ret
urn
to w
ork.
Tab
le 2
C
ontin
ued
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from
10 Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
and the way they are influenced by other factors appear to be central to negotiating a successful return to work. The scope for managing pain and making adjustments in the workplace can be influenced by the quality of the relationship an individual has with their employer and/or line manager and what is feasible within a particular work setting. The remaining 13 conceptual categories are described in more detail in online supplementary file 3. The concepts within each conceptual category are presented in online supplementary file 4.
Managing painPain was seen as a major obstacle to return to work.27–29 A plethora of strategies to manage it were described,28–33 including use of sick leave.12 34
They used the strategies doing a little at a time, taking continuous breaks, working slower and being aware of body posture and workloads. These strategies im-proved their endurance and prevented further pain.32
However, the strain of living with chronic pain meant fatigue also became a problem and low-energy levels prevented work return.29
Pain developed and became continuous, was easi-ly provoked by work tasks and relatively resistant to pain-controlling strategies. Life became strenuous and energy was reduced.30
The impact of pain on performance35 and ability to attend and travel to work,36 along with the fear of pain exacerbation,31 37 were also problematic.
Managing work relationshipsInterpersonal conflict and mutual mistrust can arise between people with pain and their employers and colleagues,38 39 and if relationships with supervisors are perceived as poor then this is demotivating in relation to work return.40 Employers with few employees expressed reservations about how far to push an employee for fear of upsetting them and causing them to be off sick for longer than necessary.41 Managers in a public sector study appeared to be walking a fine line between supporting employees, making sure colleagues were not adversely affected and that services were delivered.35 Asking for help was perceived as frustrating by people in pain, and incurred feelings of inadequacy and negativity.42 Some struggled in their interaction with employers and tended to be passive, not believing their views were listened to, or valued, which led to difficulties in sustaining work return.12 Unsympathetic employer attitude and a lack of understanding of the person’s experience of pain were seen as major obstacles to work return,13 31 32 43 44 but those employers with personal experience of pain were perceived as more sympathetic and empathic.45 46
One of the important employment related obstacles is the perception that employers have limited under-standing about pain due to ignorance and a lack of awareness. However, patients do acknowledge that
chronic pain is difficult to understand without per-sonal experience.13
Team management responsibilities of regulating tension between colleagues were perceived as challenging when work restrictions for those with pain caused unequal work distribution, leading to a sense of injustice.47
However, if duties were reduced indefinitely, with no extra cover, workers might feel that they were bur-dening their colleagues. There were doubts as to how long their colleagues support might continue.45
Making workplace adjustmentsAn economic climate of austerity was perceived as an obstacle to work due to reduced job availability and a competitive job market.13 Reorganisations and rational-isation in the workplace meant jobs had changed and become more demanding and potentially difficult to adapt for people with a pain condition.36 In this situation, age was also seen as influential, with some feeling they were too old to retrain for a different kind of job.13 44
The type of job influenced work return decisions, with physical work being perceived as more challenging with pain44 47 and more highly skilled work providing greater scope for flexibility and adaptation.48
Modifying work hours and days is a potential accom-modation for women who develop musculoskeletal diseases, but it is only appropriate in certain work en-vironments where such flexibility is allowed.43
People with chronic pain often felt they were not consulted or involved in the decision making about work-place redeployment or adjustment, and when desired modifications were not possible they could not return to work.43–45 48 Managers’ attitudes and efforts,46 combined with effective routine methods of regular communica-tion of changes made to colleagues,49 were seen as ways of improving the success of workplace adjustments. Managers did not always have the resources or know what options would be available for making these adjustments and saw the planning of these accommodations as an additional demand on their time.46 Managers also felt that information about work restrictions from occupa-tional health was not always realistic in the work setting and therefore difficult to implement.47
Many charge and head nurses complained that oc-cupational physicians formulated unrealistic restric-tions that were impossible to respect due to work organization.47
A number of workplace adjustments were felt to be helpful, including flexible hours or a reduction in hours, but were not always forthcoming.36 43 48 The possibility of a gradual return to work,50 working from home or participating in a job sharing programme43 was also seen as helpful by people in chronic pain. Changes to the job itself, including physical adjustments and a reduction in
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from

11Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
job demands, were not always feasible, for example in a nursing,43 nursing assistant role36 or a preschool teaching role.51
line of argumentA line of argument was constructed by examining how the conceptual categories relate to each other. A flow diagram/conceptual model was then developed (figure 2).
This conceptual model of return to work is now explained, going anticlockwise from (1) to (7).1. The underpinning foundation lies in the cultural ex-
pectation within society that people should work and contribute to the economy. Societal expectations are manifested within institutions, families and the media.
2. Societal and family expectations influence the individ-ual’s sense of self and what work means to each per-son. Meaning can relate to financial remuneration, re-wards or survival, and meeting of social, cognitive and achievement needs or purpose in life. The individual’s level of self-belief and autonomy will both play a part in how much agency and control can be exerted over pain and the work situation.
3. The way someone thinks about their pain and the mental representation they create will also influence their behaviour and the possibility of returning to work. People’s perceptions of whether pain is a long-term disability could influence whether they feel able to work and thus their return to work decisions, where-
as someone who has accepted the pain as part of their life and adapts may be more likely to consider return to work.
4. Some studies in the review evaluated prereturn to work support or rehabilitation programmes, and not being understood by health professionals was cited as an ob-stacle. In the same way, not being believed or being judged by people in the workplace was also perceived to make return to work challenging.
5. The three key tenets of return to work are managing pain, managing work relationships and making work-place adjustments. Tension exists between these three facets and they can be influenced by a mismatch be-tween the individual and the employer expectations, difficulties asking for help and system factors in the workplace, and health and social security systems.
6. Individuals must negotiate a wide range of obstacles and navigate change.
7. This could result in a downward spiral (and not work-ing) at one end of a continuum through to an upward spiral of mastering return to work despite pain.
DIsCussIonIn this meta-ethnography we identified obstacles to return to work for people with chronic pain centred around three key conceptual categories: managing pain, managing work relationships in the workplace and making workplace adjustments. The dynamic relationship
Figure 2 Conceptual model: the work of return to work. This conceptual model of return to work is explained in the text, going anticlockwise from (1) to (7).
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from

12 Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
between these three closely linked categories appears to be highly influential in navigating change and over-coming obstacles individuals with chronic pain face. The ability to manage pain and negotiate workplace adjust-ments can be affected by the strength of relationships with employer and colleagues and what is practicable in the work environment.
The concepts of health and pain representations and the role of significant others and their thinking about pain and return to work do not appear to be highlighted by previous reviews. Another neglected area is the influ-ence of prereturn to work support or rehabilitation. The employer perspective is missing in earlier reviews which have focused on the experience of people with chronic pain. Only five of the included studies were conducted with employers, so there is still limited research with this group despite people with pain emphasising the impor-tance of employer attitudes and knowledge in the return to work process.49
Some studies that were included in the review appear to suggest that those people with chronic pain who manage to stay in work have different characteristics from those who are unable to do so. This is seen in part to be connected with their cognitive appraisal of their pain and whether they are able to adapt.31 37 It has been proposed that in those who do not return to work, their pain repre-sentation of ‘abnormal pain’ becomes crystallised with their goal of pain elimination firmly intact, whereas those who returned to work began to perceive pain as ‘the new normal’ and something they learn to live with.37 Edén et al52 described three different adaptation patterns: the go-getter, realist and indifferent. They proposed the pessimistic and passive outlook of the latter type meant work return was less likely. Passivity in the interaction with stakeholders like the employer was found to be linked with reduced drive to return to work.12 Angel et al53 and Dionne et al50 also found passivity in relation to pain was not helpful when addressing workplace obstacles.
The provision of professional individualised support and coaching in the workplace was seen to be valuable in the work return process,54 and this concept supports the idea of developing work-based interventions to help people with chronic pain return to work.
When comparing findings with previous reviews that have highlighted obstacles to return to work, similarities include fears of not being able to fulfil employer expec-tations, not being believed by colleagues and financial concerns.4 Worries for the future, including financial and job security, were also uncovered by MacNeela et al.5 Strain on the family relationships, including those with partners and children,4 and gender differences regarding role as carer or breadwinner were revealed.5 Unsatisfying rela-tionships with health professionals where people felt they were not being listened to and frustrations with limita-tions of medical treatment were other common features.5 Social withdrawal as a result of pain was highlighted in both of these reviews.4 5 A struggle for legitimacy with colleagues and stigma in the workplace was highlighted
by Toye et al7 and Froud et al.4 This review also drew atten-tion to the system not supporting return to work due to a lack of dialogue between employers, occupational health and the health system to facilitate a gradual return with appropriate adjustments.
The collaborative team approach to conceptual anal-ysis increased the rigour of the review.14 Independently drawing flow diagrams to illustrate the conceptual model and then coming together to amalgamate these through discussion and debate, combined with checking all concepts had been included, ensured this process was thorough.
The CERQual assessments indicated there was a high level of confidence in the findings for managing pain, managing work relationships, managing the work-place, self-belief, health and illness representations, the meaning of work and system factors. Although we have used CERQual, we found we agreed with many comments on its use by Toye et al,55 namely that for relevance, studies rated as partially or indirectly relevant could also contain helpful concepts. They suggest ‘gravitational pull’ of an idea may be important. They argue providing clear infor-mation about concepts is critical, and we have provided this in online supplementary files 3 and 4. They also note for adequacy. ‘The power of concepts to make us think, however, is not based on quantity of data included’. We agree when looking at coherence that inconsistent find-ings do not necessarily call the findings into question. It may be one study has developed an insight not consid-ered in other studies. No tool can guarantee confidence in findings, and authors still need to carefully consider rigour issues.
ImplicationsThis review identifies obstacles faced by people with chronic pain in returning to work after a period of sick leave or unemployment and can be used to inform the development of a return to work intervention. The focus of such intervention should be working collaboratively with the person who has chronic pain and the employer to explore ways of addressing managing pain, managing work relationships and making workplace adjustments. The way in which the different factors work together either to enhance or inhibit return to work is highly individual, and clinicians will need to assess what is most important for the person and employer with whom they are working. This intervention could be located in commu-nity/primary healthcare and delivered by case managers, for example, occupational therapists or occupational health nurses working alongside general practitioners. Alternatively it could be delivered by employment special-ists working in employment services and trained in pain management strategies. This type of intervention would provide support tailored to the specific needs of people with chronic pain. Discussion may be needed between the employer, the employee and the case manager to enable exploration of the ways in which obstacles to return to work might be overcome. This collaborative approach
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from

13Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
has the potential to improve healthcare services and change workplace culture and is the kind of innovation envisioned by the UK government in their 10-year plan for people with long-term health conditions to realise their working potential.56
limitationsIt is apparent that more research is required from the employer’s perspective. The five studies included in the review were from the perspective of employers working in car making, university hospitals, home care provision for disabled people in France,38 public hospitals in France,47 and National Health Service Trust and local authority in Wales.35 The Canadian study that included small and large employers did not specify the nature of the industry in which they were engaged.41
It is likely that the reviewers’ backgrounds and experi-ences had an impact on synthesis findings. The authors came from healthcare professional and non-healthcare professional backgrounds, and these backgrounds and experiences of chronic pain provided certain lenses, which we would expect to influence our understanding.
At the time we did this work, the eMERGe Reporting Guidance for meta-ethnography57 had not been published. They were published close to the end of the peer review process for this paper.
ConClusIonsThe navigation of obstacles to return to work for people with chronic pain and their employers entails balancing the needs of the person with chronic pain, colleagues and the employing organisation. The influence of health and pain representations the person formulates has not been emphasised in previous reviews. Managing pain, managing relationships in the workplace and making adjustments are central to achieving a successful return to work, and these can be hard work for the person with chronic pain.
Acknowledgements We would like to thank Samantha Johnson, Academic Support Librarian (Medicine, Life Sciences and Psychology) at the University of Warwick, for her help with initial literature search and helpful guidance during the updated search process. We would like to thank Debs Smith, patient and public involvement representative, who participated in developing the research protocol as a coapplicant.
Contributors KS, RF and MU made a substantial contribution to the design of the study. MG and KS were responsible for acquisition, and MG, KS and JO-B-E were responsible for analysis and interpretation of the data. MG drafted the first, subsequent and final versions, and KS, JO-B-E, RF and MU revised all versions for important intellectual content and approved the final version. All authors agree to be accountable for the accuracy and integrity of the work.
Funding This research is part of the RISE (Return to work with Individualised Supported Employment) feasibility study supported by the Versus Arthritis charity (project number 9401), and the funder has had no involvement in this paper.
Competing interests RF is chief investigator on the Versus Arthritis grant from which this project was funded. He has published multiple papers on chronic pain, some of which are referenced in this paper. RF and MU are part of an academic partnership with Serco related to return-to-work initiatives. RF and MU are directors and shareholders of Clinvivo, a university spin-out company that provides data collection services for health services research. MU was Chair of the NICE
Accreditation Advisory Committee until March 2017 for which he received a fee. He is chief investigator or coinvestigator on multiple previous and current research grants from the UK National Institute for Health Research and Versus Arthritis, and is a coinvestigator on grants funded by the Australian NHMRC. He is an NIHR Senior Investigator. He has received travel expenses for speaking at conferences from the professional organisations hosting the conferences. He is a coinvestigator on a study receiving support in kind from OrthoSpace. He has accepted an honorarium from CARTA. He is an editor of the NIHR journal series, and a member of the NIHR Journal Editors Group, for which he receives a fee. KS is an investigator in multiple previous and current research grants from the UK National Institute for Health Research and Versus Arthritis. She has received travel and accommodation expenses for speaking at conferences from the professional organisations hosting the conferences. She has published multiple papers on pain, some of which are referenced in this paper.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This is a qualitative systematic review, so there are no primary research data. We have tried to include all relevant data for the qualitative systematic review in the supplementary files. Any other reasonable requests will be considered on a case-by-case basis by MG (lead author; email: M. Grant. 2@ warwick. ac. uk).
open access This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https:// creativecommons. org/ licenses/ by/ 4. 0/.
reFerenCes 1. Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a
prevalence study. Pain 2001;89:127–34. 2. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC
Public Health 2011;11:770. 3. Toye F, Seers K, Hannink E, et al. A mega-ethnography of eleven
qualitative evidence syntheses exploring the experience of living with chronic non-malignant pain. BMC Med Res Methodol 2017;17:116.
4. Froud R, Patterson S, Eldridge S, et al. A systematic review and meta-synthesis of the impact of low back pain on people's lives. BMC Musculoskelet Disord 2014;15:50.
5. MacNeela P, Doyle C, O'Gorman D, et al. Experiences of chronic low back pain: a meta-ethnography of qualitative research. Health Psychol Rev 2015;9:63–82.
6. Johannes CB, Le TK, Zhou X, et al. The prevalence of chronic pain in United States adults: results of an Internet-based survey. J Pain 2010;11:1230–9.
7. Toye F, Seers K, Allcock N, et al. A synthesis of qualitative research exploring the barriers to staying in work with chronic musculoskeletal pain. Disabil Rehabil 2016;38:566–72.
8. de Vries HJ, Brouwer S, Groothoff JW, et al. Staying at work with chronic nonspecific musculoskeletal pain: a qualitative study of workers' experiences. BMC Musculoskelet Disord 2011;12:126.
9. Patel AS, Farquharson R, Carroll D, et al. The impact and burden of chronic pain in the workplace: a qualitative systematic review. Pain Pract 2012;12:578–89.
10. Henriksson CM, Liedberg GM, Gerdle B. Women with fibromyalgia: work and rehabilitation. Disabil Rehabil 2005;27:685–94.
11. Wainwright E, Wainwright D, Keogh E, et al. Fit for purpose? Using the fit note with patients with chronic pain: a qualitative study. Br J Gen Pract 2011;61:e794–e800.
12. Ahlstrom L, Dellve L, Hagberg M, et al. Women with Neck Pain on Long-Term Sick Leave-Approaches Used in the Return to Work Process: A Qualitative Study. J Occup Rehabil 2017;27:92–105.
13. Patel S, Greasley K, Watson PJ. Barriers to rehabilitation and return to work for unemployed chronic pain patients: a qualitative study. Eur J Pain 2007;11:831–40.
14. Toye F, Seers K, Allcock N, et al. Meta-ethnography 25 years on: challenges and insights for synthesising a large number of qualitative studies. BMC Med Res Methodol 2014;14:80.
15. Noblit GW, Hare RD. Meta-Ethnography: synthesizing qualitative studies. Newbury Park, Calif: Sage, 1988.
16. Shaw RL, Booth A, Sutton AJ, et al. Finding qualitative research: an evaluation of search strategies. BMC Med Res Methodol 2004;4:5.
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from

14 Grant M, et al. BMJ Open 2019;9:e025743. doi:10.1136/bmjopen-2018-025743
Open access
17. CASP. Critical appraisal skills programme qualitative assessment tool 2018. 2018 http:// media. wix. com/ ugd/ dded87_ 29c5 b002 d993 42f7 88c6 ac67 0e49f274. pdf [Accessed 6 Jan 2018].
18. Lewin S, Booth A, Glenton C, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings: introduction to the series. Implement Sci 2018;13(Suppl 1):2.
19. Lewin S, Bohren M, Rashidian A, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings-paper 2: how to make an overall CERQual assessment of confidence and create a Summary of Qualitative Findings table. Implement Sci 2018;13(Suppl 1):10.
20. Glenton C, Carlsen B, Lewin S, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings-paper 5: how to assess adequacy of data. Implement Sci 2018;13(Suppl 1):14.
21. Colvin CJ, Garside R, Wainwright M, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings-paper 4: how to assess coherence. Implement Sci 2018;13(Suppl 1):13.
22. Munthe-Kaas H, Bohren MA, Glenton C, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings-paper 3: how to assess methodological limitations. Implement Sci 2018;13(Suppl 1):9.
23. Noyes J, Booth A, Lewin S, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings-paper 6: how to assess relevance of the data. Implement Sci 2018;13(Suppl 1):4.
24. Schutz A. Concept and theory formation in the social sciences. J Philos 1954;51:257–73.
25. NVivo 11 [program]: QSR International Pty Ltd. 2012. 26. Toye F, Seers K, Allcock N, et al. 'Trying to pin down jelly' - exploring
intuitive processes in quality assessment for meta-ethnography. BMC Med Res Methodol 2013;13:46.
27. Juuso P, Skär L, Sundin K, et al. The Workplace Experiences of Women with Fibromyalgia. Musculoskeletal Care 2016;14:69–76.
28. Nilsen G, Anderssen N. Struggling for a normal life: work as an individual self-care management strategy among persons living with non-malignant chronic pain. Work 2014;49:123–32.
29. Sjöström R, Melin-Johansson C, Asplund R, et al. Barriers to and possibilities of returning to work after a multidisciplinary rehabilitation programme. A qualitative interview study. Work 2011;39:243–50.
30. Hansson M, Boström C, Harms-Ringdahl K. Living with spine-related pain in a changing society—a qualitative study. Disabil Rehabil 2001;23:286–95.
31. Kalsi P, Turkistani W, Sykes C, et al. “Work is a beautiful thing…” Exploring attitudes towards employment in chronic pain (CP) patients attending a pain management programme (PMP). J Vocat Rehabil 2016;44:97–107.
32. Rydstad M, Schult ML, Löfgren M. Whiplash patients' experience of a multimodal rehabilitation programme and its usefulness one year later. Disabil Rehabil 2010;32:1810–8.
33. Shaw WS, Huang YH. Concerns and expectations about returning to work with low back pain: identifying themes from focus groups and semi-structured interviews. Disabil Rehabil 2005;27:1269–81.
34. Hansson M, Boström C, Harms-Ringdahl K. Sickness absence and sickness attendance–what people with neck or back pain think. Soc Sci Med 2006;62:2183–95.
35. Wynne-Jones G, Buck R, Porteous C, et al. What happens to work if you're unwell? Beliefs and attitudes of managers and employees with musculoskeletal pain in a public sector setting. J Occup Rehabil 2011;21:31–42.
36. Liedberg GM, Henriksson CM. Factors of importance for work disability in women with fibromyalgia: an interview study. Arthritis Rheum 2002;47:266–74.
37. Coutu MF, Baril R, Durand MJ, et al. Transforming the meaning of pain: an important step for the return to work. Work 2010;35:209–19.
38. Fassier JB, Durand MJ, Caillard JF, et al. Results of a feasibility study: barriers and facilitators in implementing the Sherbrooke model in France. Scand J Work Environ Health 2015;41:223–33.
39. Svensson T, Müssener U, Alexanderson K. Sickness absence, social relations, and self-esteem: a qualitative study of the importance of relationships with family, workmates, and friends among persons initially long-term sickness absent due to back diagnoses. Work 2010;37:187–97.
40. Gard G, Sandberg AC. Motivating factors for return to work. Physiother Res Int 1998;3:100–8.
41. Soklaridis S, Ammendolia C, Cassidy D. Looking upstream to understand low back pain and return to work: psychosocial factors as the product of system issues. Soc Sci Med 2010;71:1557–66.
42. Andersen LN, Kohberg M, Herborg LG, et al. "Here we're all in the same boat"–a qualitative study of group based rehabilitation for sick-listed citizens with chronic pain. Scand J Psychol 2014;55:333–42.
43. Crooks VA. Women's experiences of developing musculoskeletal diseases: employment challenges and policy recommendations. Disabil Rehabil 2007;29:1107–16.
44. Soeker MS, Wegner L, Pretorius B. I'm going back to work: back injured clients' perceptions and experiences of their worker roles. Work 2008;30:161–70.
45. Coole C, Watson PJ, Drummond A. Low back pain patients' experiences of work modifications; a qualitative study. BMC Musculoskelet Disord 2010;11:277.
46. Williams-Whitt K, Kristman V, Shaw WS, et al. A Model of Supervisor Decision-Making in the Accommodation of Workers with Low Back Pain. J Occup Rehabil 2016;26:366–81.
47. Grataloup M, Massardier-Pilonchéry A, Bergeret A, et al. Job Restrictions for Healthcare Workers with Musculoskeletal Disorders: Consequences from the Superior's Viewpoint. J Occup Rehabil 2016;26:245–52.
48. Brooks J, McCluskey S, King N, et al. Illness perceptions in the context of differing work participation outcomes: exploring the influence of significant others in persistent back pain. BMC Musculoskelet Disord 2013;14:48.
49. Nordqvist C, Holmqvist C, Alexanderson K. Views of laypersons on the role employers play in return to work when sick-listed. J Occup Rehabil 2003;13:11–20.
50. Dionne CE, Bourbonnais R, Frémont P, et al. Obstacles to and facilitators of return to work after work-disabling back pain: the workers' perspective. J Occup Rehabil 2013;23:280–9.
51. Kvam L, Vik K. Discourses of participation in work among men and women in vocational rehabilitation. J Occup Sci 2015;22:345–57.
52. Edén L, Andersson HI, Ejlertsson G, et al. Characteristics of disability pensioners returning to work: an interview study among individuals with musculoskeletal disorders. Disabil Rehabil 2007;29:1720–6.
53. Angel S, Jensen LD, Gonge BK, et al. Patients' interpretations of a counselling intervention for low back pain: a narrative analysis. Int J Nurs Stud 2012;49:784–92.
54. Glavare M, Löfgren M, Schult ML. Between unemployment and employment: experience of unemployed long-term pain sufferers. Work 2012;43:475–85.
55. Toye F, Seers K, Barker K. A meta-ethnography of health-care professionals’ experience of treating adults with chronic non-malignant pain to improve the experience and quality of health care. Health Serv Deliv Res 2018;6:1–106.
56. Department of Work and Pensions DoH. Improving lives. The future of Work, Health and Disability: HMSO, 2017.
57. France EF, Cunningham M, Ring N, et al. Improving reporting of meta-ethnography: the eMERGe reporting guidance. BMC Med Res Methodol 2019;19:25.
58. Ashby S, Richards K, James C. The effect of fear of movement on the lives of people with chronic low back pain. Int J Ther Rehabil 2010;17:232–43.
59. Buus N, Jensen LD, Maribo T, et al. Low back pain patients' beliefs about effective/ineffective constituents of a counseling intervention: a follow-up interview study. Disabil Rehabil 2015;37:936–41.
60. Coutu MF, Baril R, Durand MJ, et al. Health and illness representations of workers with a musculoskeletal disorder-related work disability during work rehabilitation: a qualitative study. J Occup Rehabil 2011;21:591–600.
61. Coutu MF, Baril R, Durand MJ, et al. Clinician-patient agreement about the work disability problem of patients having persistent pain: why it matters. J Occup Rehabil 2013;23:82–92.
62. Johansson EE, Hamberg K, Lindgren G, et al. "How could I even think of a job?"–Ambiguities in working life in a group of female patients with undefined musculoskeletal pain. Scand J Prim Health Care 1997;15:169–74.
63. Kvam L, Eide AH, Vik K. Understanding experiences of participation among men and women with chronic musculoskeletal pain in vocational rehabilitation. Work 2013;45:161–74.
64. Magnussen L, Nilsen S, Råheim M. Barriers against returning to work–as perceived by disability pensioners with back pain: a focus group based qualitative study. Disabil Rehabil 2007;29:191–7.
65. McCluskey S, Brooks J, King N, et al. The influence of 'significant others' on persistent back pain and work participation: a qualitative exploration of illness perceptions. BMC Musculoskelet Disord 2011;12:236.
66. McCluskey S, Brooks J, King N, et al. Are the treatment expectations of 'significant others' psychosocial obstacles to work participation for those with persistent low back pain? Work 2014;48:391–8.
67. Saunders SL, MacEachen E, Nedelec B. Understanding and building upon effort to return to work for people with long-term disability and job loss. Work 2015;52:103–14.
68. Scheermesser M, Bachmann S, Schämann A, et al. A qualitative study on the role of cultural background in patients' perspectives on rehabilitation. BMC Musculoskelet Disord 2012;13:5.
on October 20, 2021 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2018-025743 on 20 June 2019. D
ownloaded from
Related Documents











