25 Onchocerciasis hyperendemic in the Untursn Mountains: the value of recombinant antigens in describing a new transmission area in southern Venezuela Carlos Bottol~z, Andy J. Gillespie 3, SaraiVivas-MartinezL4, Nahir MartinezI, Sandra Manchart2, Maria- Gloria Bas&iezW and Janette E. Bradley316 1Centro Amazbnico para Investigacibn y Control de Enfeermedades Tropicales ‘Simdn Bolivar’, Apartado Postal 59, Puerto Ayacucho 7101, Estaab Amazonas, Ir,nezuela; 2Instituw de Medicina Tropical ‘Dr FtYix P&an0 C.‘, Universidad Central de %ezuela, Apartado Postal 47881, Caracas 1041-A, k?nezuela; 3Department of Biology, Imperial College of Science, Technology and Medicine, Prince Consort Road, London S W7 2BB, UK; 4London School of Hygiene and Tropical Medicine, Keppel Street, London WClE 7HI; UK; 5Wellcome Trust Centre for the Epidemiology of Infectious Disease, University of Oxford, South Parks Road, Oxford OX1 3PS, UK; 6Department of Biolog- ical Sciences, University of Salford, Salford MS 4m UK Abstract A recently described hyperendemic onchocerciasis area, located in the Unturin Mountains (between the Siapa and Orinoco basins) of southernvenezuela was studied using a cocktail of 3 low molecular weight onchocercal recombinant antigens (OvMBWlO, OvMBWl 1, and OvMBW29). The resulting seroepide- miological data were compared with those from a hypoendemic community (Altamira) situated in the northern coastal mountain range. Parasitological (skin biopsy) and serological (enzyme-linked immuno- sorbent assay, ELISA) methods for the specific diagnosis of Onchocerca volvuZus in these 2 very different endemic areas were, respectively, 88% and 96% sensitive in Untursn, and 57% and 91% sensitive in Al- tamira. The mean microfilarial load, the mean optical density (OD), and the seropositivity rates all increased significantly with age in both communities.The serological variables (mean OD and prevalence of anti-O. volvulus antibodies) were both significantly higher in Unturin than in Altamira for children and young adults (aged ~25 years), although above this age no differences between communities were detect- ed. Seroprevalence had already reached 50% in the under 15 year-olds examined at Unturin but was just 5% at Altamira for the same age-class.The prevalence of specific antibodies (mainly a marker of exposure to risk of infection) exceeded 85% in the remaining age-categories at the hyperendemic area. This is in agreement with the high community microfilarial load recorded in Unturhn (>20 mE/mg) and the pres- ence of sclerosing keratitis and hanging groin, suggesting that onchocerciasis is a public health problem in this community. The ELISA test used here, based on a cocktail of 3 low molecular weight onchocercal recombinant antigens, appears, therefore, to constitute a practical tool for the description of endemicity levels in remote areas, particularly given the fact that finger-prick blood samples are routinely taken from children in the Upper Orinoco region for surveys of malaria incidence. Such studies could aid in defining the true extent of the Amazon focus (still unknown) and providing priority indicators for the selection of communities where onchocerciasis control programmes should be implemented. Keywords: onchocerciasis, Onchocerca volvulus, recombinant antigens, seroprevalence, age-profiles, endemicity, Ven- ezuela Introduction Onchocerciasis in the Amazon focus is a severe public health problem among the Venezuelan Yanomam6, causing sclerosing keratitis and blindness in some areas (YARZABAL et al., 1983, 1985b; BOTTO et al., 1984, 1997; BASAIQEZ & YARZABAL, 1989). The geographical distribution of the infection is itself patchy and the af- fected human populations are scattered in isolated areas of the Upper Orinoco rain forest, making the extent of this focus difficult to define. The detection of Onchocerca volvulus microfilariae (mf) by skin biopsy has been the method of choice for both the diagnosis of onchocerciasis and the estimation of worm burden (WHO, 1987). However, parasitologi- cal diagnosis may be insensitive on some occasions such as in pre-patent infection (BRADLEY et al., 1993a), and in hypoendemic foci with low mean microfilarial load (YOSHIMURA et al., 1982) and localities where control measures have been initiated (BRADLEY et al., 1993b). In addition, human populations may become reluctant to be skin-snipped repeatedly during epidemiological surveys and subsequent monitoring of control opera- tions. Recently developed serodiagnostic tests, using onchocercal recombinant antigens, have proved to be very specific (LOBOS etal., ~~~~;BRADLEY etal., 1991; RAMACHANDRAN, 1993) and sensitive under a variety of field situations (BRADLEY et al., 1993a; BRADLEY & UNNASCH,~~~~). The parasitological aspects of a new record of on- Address for correspondence: Dr Carlos Bono A., CAICET, AP 59, Puerto Ayacucho, ZP 7101, Estado Amazonas,Vene- zuela; fax +58 48 21 22 23, e-mail [email protected] chocerciasis have been reported for the Unturhn Moun- tains of south Venezuela, with a microfilarial prevalence of 67% and a community microfilarial load (CMFL) of 24 mElmg (Bo~o et aZ., 1997). This paper describes the use of low molecular weight onchocercal antigens as seroepidemiological tools to compare this hmerendem- ic locality with-a hypoendemic-area in th; northern coastal mountains of Venezuela (BOTTO. 1988‘1. and discusses their usefulness in the assessment of on- chocerciasis endemicity in remote areas. Materials and Methods Study site and parasitological methods A cross-sectional survey was performed in 2 Yanomamij communities located in the Unturti Mountains, between the basins of the Upper Orinoco and the Upper Siapa rivers, with the objectives of as- sessing endemicity levels of human onchocerciasis, ma- laria, and viral hepatitis. Only onchocerciasis results are presented here. Precise location and additional data on these communities have been presented by BO~TO et al. (1997). A sample of 93 individuals (44 females and 49 males; mean age: 32 years) from a total population of 202 was examined. In order to compare the Unturin data with a hypoendemic focus s&died by BOTT’O (1988) and GRILLET et al. (1994). a further samnle of 54 individuals (3 1 females and 23 males; mean age: 28 years) was studied from the locality of Altamira (Cara- bobo State, northern Venezuela). Consent was ob- tained fro& individuals and -community leaders according to the Drocedures outlined in WHO (1993). Parasitol&ical di&nosis and data analyses were can&d out as described in BO~TO et al. (1997).

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
25
Onchocerciasis hyperendemic in the Untursn Mountains: the value of recombinant antigens in describing a new transmission area in southern Venezuela
Carlos Bottol~z, Andy J. Gillespie 3, SaraiVivas-MartinezL4, Nahir MartinezI, Sandra Manchart2, Maria- Gloria Bas&iezW and Janette E. Bradley316 1Centro Amazbnico para Investigacibn y Control de Enfeermedades Tropicales ‘Simdn Bolivar’, Apartado Postal 59, Puerto Ayacucho 7101, Estaab Amazonas, Ir,nezuela; 2Instituw de Medicina Tropical ‘Dr FtYix P&an0 C.‘, Universidad Central de %ezuela, Apartado Postal 47881, Caracas 1041-A, k?nezuela; 3Department of Biology, Imperial College of Science, Technology and Medicine, Prince Consort Road, London S W7 2BB, UK; 4London School of Hygiene and Tropical Medicine, Keppel Street, London WClE 7HI; UK; 5 Wellcome Trust Centre for the Epidemiology of Infectious Disease, University of Oxford, South Parks Road, Oxford OX1 3PS, UK; 6Department of Biolog- ical Sciences, University of Salford, Salford MS 4m UK
Abstract A recently described hyperendemic onchocerciasis area, located in the Unturin Mountains (between the Siapa and Orinoco basins) of southernvenezuela was studied using a cocktail of 3 low molecular weight onchocercal recombinant antigens (OvMBWlO, OvMBWl 1, and OvMBW29). The resulting seroepide- miological data were compared with those from a hypoendemic community (Altamira) situated in the northern coastal mountain range. Parasitological (skin biopsy) and serological (enzyme-linked immuno- sorbent assay, ELISA) methods for the specific diagnosis of Onchocerca volvuZus in these 2 very different endemic areas were, respectively, 88% and 96% sensitive in Untursn, and 57% and 91% sensitive in Al- tamira. The mean microfilarial load, the mean optical density (OD), and the seropositivity rates all increased significantly with age in both communities.The serological variables (mean OD and prevalence of anti-O. volvulus antibodies) were both significantly higher in Unturin than in Altamira for children and young adults (aged ~25 years), although above this age no differences between communities were detect- ed. Seroprevalence had already reached 50% in the under 15 year-olds examined at Unturin but was just 5% at Altamira for the same age-class.The prevalence of specific antibodies (mainly a marker of exposure to risk of infection) exceeded 85% in the remaining age-categories at the hyperendemic area. This is in agreement with the high community microfilarial load recorded in Unturhn (>20 mE/mg) and the pres- ence of sclerosing keratitis and hanging groin, suggesting that onchocerciasis is a public health problem in this community. The ELISA test used here, based on a cocktail of 3 low molecular weight onchocercal recombinant antigens, appears, therefore, to constitute a practical tool for the description of endemicity levels in remote areas, particularly given the fact that finger-prick blood samples are routinely taken from children in the Upper Orinoco region for surveys of malaria incidence. Such studies could aid in defining the true extent of the Amazon focus (still unknown) and providing priority indicators for the selection of communities where onchocerciasis control programmes should be implemented.
Keywords: onchocerciasis, Onchocerca volvulus, recombinant antigens, seroprevalence, age-profiles, endemicity, Ven- ezuela
Introduction Onchocerciasis in the Amazon focus is a severe public
health problem among the Venezuelan Yanomam6, causing sclerosing keratitis and blindness in some areas (YARZABAL et al., 1983, 1985b; BOTTO et al., 1984, 1997; BASAIQEZ & YARZABAL, 1989). The geographical distribution of the infection is itself patchy and the af- fected human populations are scattered in isolated areas of the Upper Orinoco rain forest, making the extent of this focus difficult to define.
The detection of Onchocerca volvulus microfilariae (mf) by skin biopsy has been the method of choice for both the diagnosis of onchocerciasis and the estimation of worm burden (WHO, 1987). However, parasitologi- cal diagnosis may be insensitive on some occasions such as in pre-patent infection (BRADLEY et al., 1993a), and in hypoendemic foci with low mean microfilarial load (YOSHIMURA et al., 1982) and localities where control measures have been initiated (BRADLEY et al., 1993b). In addition, human populations may become reluctant to be skin-snipped repeatedly during epidemiological surveys and subsequent monitoring of control opera- tions. Recently developed serodiagnostic tests, using onchocercal recombinant antigens, have proved to be very specific (LOBOS etal., ~~~~;BRADLEY etal., 1991; RAMACHANDRAN, 1993) and sensitive under a variety of field situations (BRADLEY et al., 1993a; BRADLEY & UNNASCH,~~~~).
The parasitological aspects of a new record of on-
Address for correspondence: Dr Carlos Bono A., CAICET, AP 59, Puerto Ayacucho, ZP 7101, Estado Amazonas,Vene- zuela; fax +58 48 21 22 23, e-mail [email protected]
chocerciasis have been reported for the Unturhn Moun- tains of south Venezuela, with a microfilarial prevalence of 67% and a community microfilarial load (CMFL) of 24 mElmg (Bo~o et aZ., 1997). This paper describes the use of low molecular weight onchocercal antigens as seroepidemiological tools to compare this hmerendem- ic locality with-a hypoendemic-area in th; northern coastal mountains of Venezuela (BOTTO. 1988‘1. and discusses their usefulness in the assessment of on- chocerciasis endemicity in remote areas.
Materials and Methods Study site and parasitological methods
A cross-sectional survey was performed in 2 Yanomamij communities located in the Unturti Mountains, between the basins of the Upper Orinoco and the Upper Siapa rivers, with the objectives of as- sessing endemicity levels of human onchocerciasis, ma- laria, and viral hepatitis. Only onchocerciasis results are presented here. Precise location and additional data on these communities have been presented by BO~TO et al. (1997). A sample of 93 individuals (44 females and 49 males; mean age: 32 years) from a total population of 202 was examined. In order to compare the Unturin data with a hypoendemic focus s&died by BOTT’O (1988) and GRILLET et al. (1994). a further samnle of 54 individuals (3 1 females and 23 males; mean age: 28 years) was studied from the locality of Altamira (Cara- bobo State, northern Venezuela). Consent was ob- tained fro& individuals and -community leaders according to the Drocedures outlined in WHO (1993). Parasitol&ical di&nosis and data analyses were can&d out as described in BO~TO et al. (1997).
CARLOS BOTTO ETAL.
Serological methods Venous blood samples were obtained in the field,
transported to the laboratory at 4°C and preserved at -70°C. Levels of onchocerciasis-specific antibodies were determined by the enzyme-linked immunosorbent assay (ELISA), using a cocktail of recombinant low mo- lecular weight antigens (OvMBP/lO. OvMBP/l 1, and OvMBP/293 (BRA~EY eial., 1993a,-1993b). Thebasic ELISA protocol followed that described in BRADLEY et al. (1991, 1993b). Reactivitv of serum samnles to Es- cherkhia coli maltose-binding protein was assessed and deducted from the anti-cocktail results. The negative cut-off value used, 0.03 1, was the mean optical density plus 3 standard deviations of Latin American non-en- demic control sera according to BRADLEY et al. (1993a). All the ELISA tests were performed on sera at a l/200 dilution, which had been determined to be on the linear part of a titration curve obtained using a pool of the higher-responding sera from Unturan. Age-standard- ized mean optical density values and seroprevalence were estimated using the direct method (KIRKWOOD, 1988).
Table 1. Mean optical density values in sera from 2 Venezuelan localities of different onchocerciasis endemicity using an ELISA based on a cocktail of 3 0. volvulus recombinant antigens ~OvMBWlO. OvMBPlll and OvMBW29) - .
Age-group Altamira Unturan (years) (Hypoendemic) (Hyperendemic) P value
Cl5 n
0% 0.004
14 0.21 co.05 0.056
AMOD SE
~25
&lOD SE
225
:MOD SE
245
LOD SE
30 32 0.03 0.43 CO.001 0.027 0.080
0?4 0.116
61 0.77 NS 0.663
11 0.94 0.148
NS 0.096
The geometric mean numbers of mf/mg in the whole population (Williams’ mean microfihu-ial density (WMMD), WIJ.LIAMS, 1937) and in the nonulation aged >2O’;ears (CMEL, F&MME et al., l-98*9) were calculated for both hypo- and hyperendemic localities as described by BOITO et al. (1997). The ELISA results
n=sample size; AMOD=arithmetic mean of optical density val- ues; SE=standard error; -probability value (a=0.05); NS=not significant.
1.6, I were computed as arithmetic mean optical densities (AMODs). Comparison of AMOD values was carried out by means of the 2-sample t-test for normally distributed data or the Mann-Whitnev U-test (MWU) for data departing from normality. DifiPrences between prevalences were tested by the x2 test with Yates’ correction when necessary, and possible trends in seroprevalence were explored by means of the x2 test for trends. The non-parametric Spearman rank test (I& was used to examine correlations between different variables. These analyses were carried out with Statgraphics@ (Statistical Graphics System, ver. 4.0, Western Michigan Universitv and Software Technoloav Support Center, USA). -
--
1.4 - 0
1.2 - 8 1.0 0 -
SO.6 - 0 0
0 0 0.6 -
0.4 4 0
Results The AMOD of onchocercal-specific antibodies was
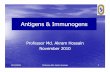
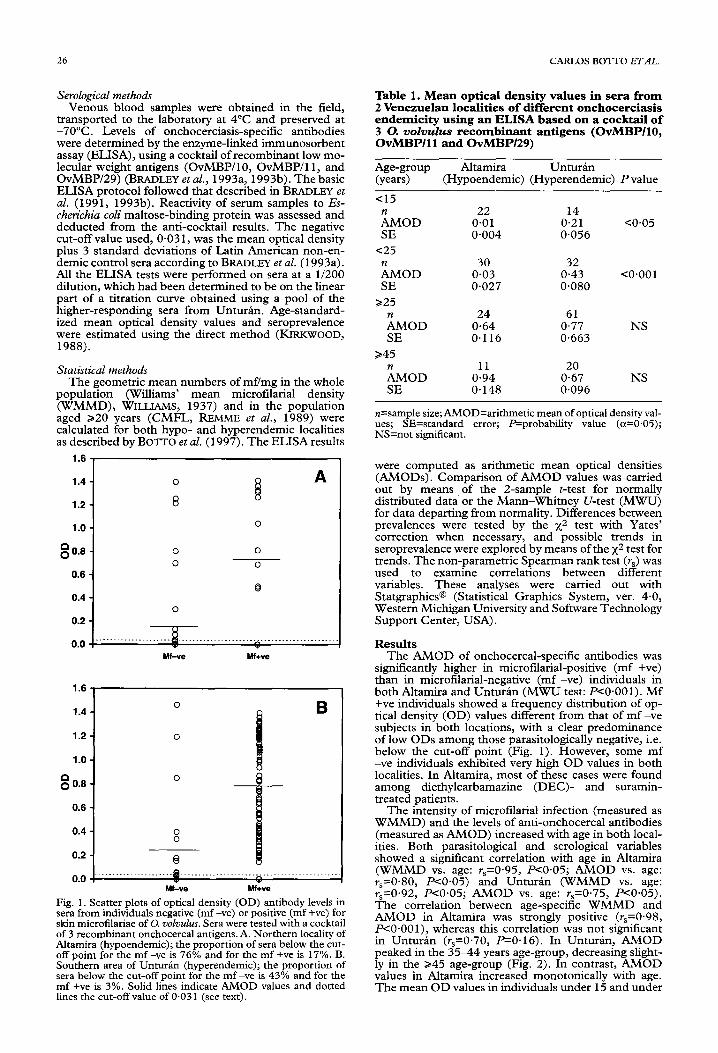
sienificantlv higher in microfilarial-nositive (mf +ve) t&n in m&rofillarial-negative (mf -;e) individuals in both Altamira and Unturan (MWU test: P<O.OOl). Mf +ve individuals showed a frequency distribution of op- tical density (OD) values different horn that of mf -ve subjects in both locations, with a clear predominance of low ODs among those parasitologically negative, i.e. below the cut-off point (Fig. 1). However, some mf -ve individuals exhibited very high OD values in both localities. In Altamira, most of these cases were found among diethylcarbamazine (DEC)- and suramin- treated patients.
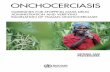
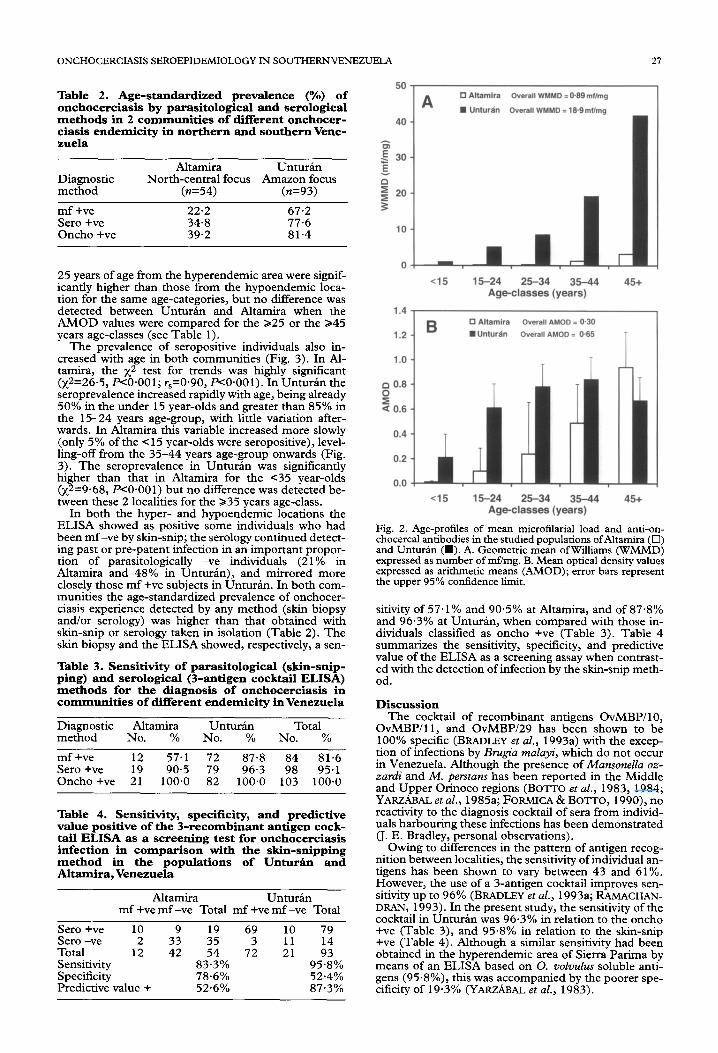
The intensitv of microfilarial infection (measured as WMMD) and-the levels of anti-onchocercal antibodies (measured as AMOD) increased with age in both local- ities. Both parasitological and serol&ical variables showed a significant correlation with age in Altamira (WMMD vs. age: r,=O.95, P~0.05; AMOD vs. age: ;,=0.80, PcO.05) a”nd Unturan (WMMD vs. age: rpO.92, EYO.05: AMOD vs. aee: r~O.75, PcO.05). The correlation. between age-siec&c WkMD and AMOD in Altamira was strongly positive (r,=O.98, P<O.OOl), whereas this correlation was not significant in Unturan (r,=O.70, -0.16). In Unturan, AMOD peaked in the 35-44 years age-group, decreasing slight- ly in the 245 age-group (Fig. 2). In contrast, AMOD values in Altamira increased monotonically with age. The mean OD values in individuals under 15 and under
..-
1.4
1.2
1.0
8 0.6
0.6
0.4 8 0.2 Q
0.0 ! 0.--.--...-.-.---..---,----------...--...-J
Mf-ve Mf+ve
Fig. 1. Scatter plots of optical density (OD) antibody levels in sera from individuals negative (mf -ve) or positive (mf +ve) for skin microfilariae of 0. VOZVUZUS. Sera were tested with a cocktail of 3 recombinant onchocercal antigens. A. Northern locality of Altamira (hypoendemic); the proportion of sera below the cut- off noint for the mf -ve is 76% and for the mf +ve is 17%. B. Southern area of Unturan (hyperendemic); the proportion of sera below the cut-off point for the mf -ve is 43% and for the mf +ve is 3%. Solid lines indicate AMOD values and dotted lines the cut-off value of 0.03 1 (see text).
ONCHOCERCIASIS SEROEPIDEMIOLOGY IN SOUTHERNVENEZUELA 2-l
Table 2. Age-standardized prevalence (%) of onchocerciasis by parasitological and serological methods in 2 communities of different onchocer- ciasis endemicity in northern and southern Vene- zuela
Diagnostic method
mf +ve Sero +ve Oncho +ve
Altamira Unturin North-central focus Amazon focus
(n=54) (n=93)
22.2 67.2 34.8 77.6 39.2 81.4
25 years of age from the hyperendemic area were signif- icantly higher than those from the hypoendemic loca- tion for the same age-categories, but no difference was detected between Unturhn and Altamira when the AMOD values were compared for the 225 or the 345 years age-classes (see Table 1).
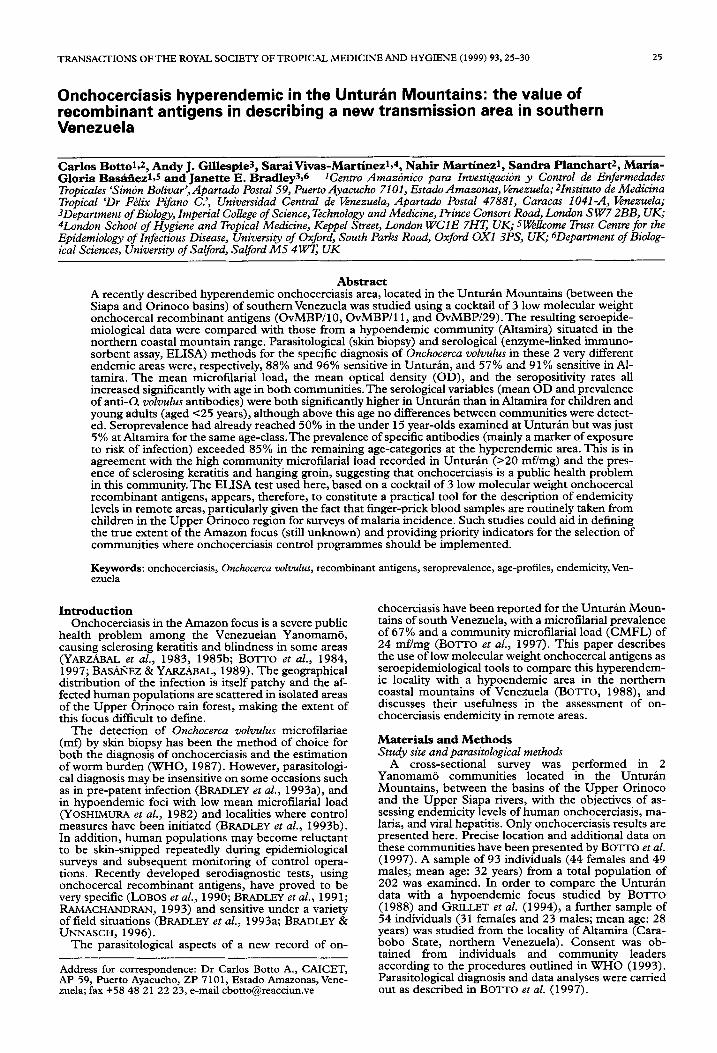
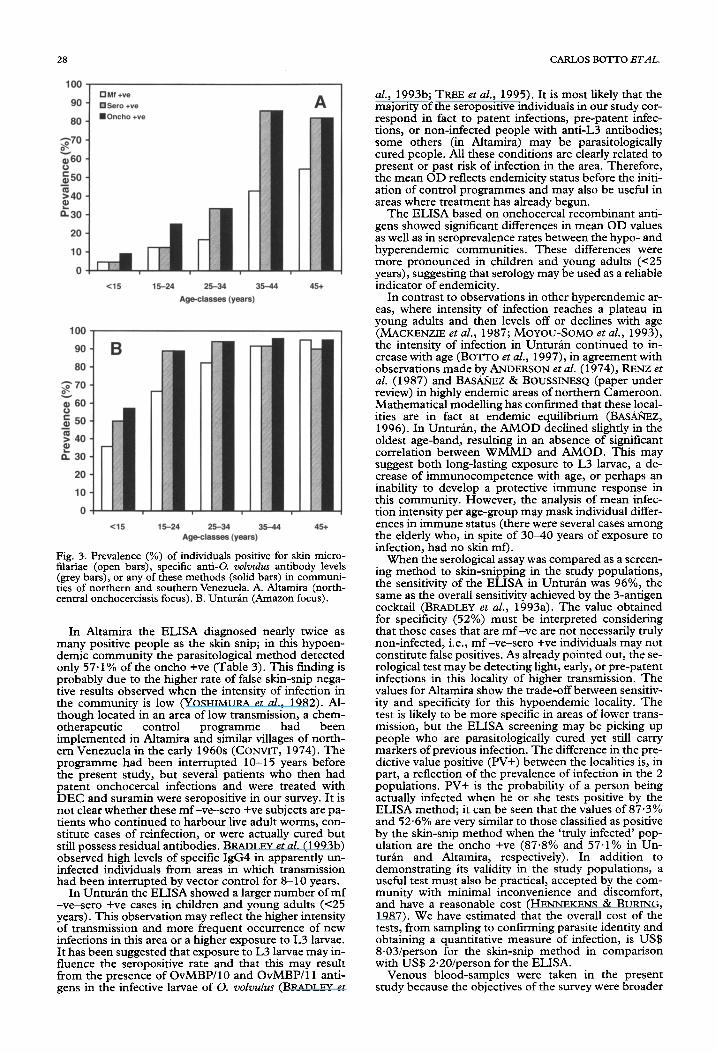
The prevalence of seropositive individuals also in- creased with age in both communities (Fig. 3). In Al- tamira, the x2 test for trends was highly significant (~2~26.5, P<O.OOl; r,=O.90, F<O.OOl). In Unturln the seroprevalence increased rapidly with age, being already 50% in the under 15 year-olds and greater than 85% in the 15-24 years age-group, with little variation after- wards. In Altamira this variable increased more slowly (only 5% of the c 15 year-olds were seropositive), level- ling-off from the 35-44 years age-group onwards (Fig. 3). The seroprevalence in Unto&n was significantly higher than that in Altamira for the <35 year-olds (x2=9.68, RO.001) but no difference was detected be- tween these 2 localities for the 235 years age-class.
In both the hyper- and hypoendemic locations the ELISA showed as positive some individuals who had been mf-ve by skin-snip; the serology continued detect- ing past or pre-patent infection in an important propor- tion of parasitologically -ve individuals (21% in Altamira and 48% in Unturin), and mirrored more closely those mf +ve subjects in UnturPn. In both com- munities the age-standardized prevalence of onchocer- ciasis experience detected by any method (skin biopsy and/or serology) was higher than that obtained with skin-snip or serology taken in isolation (Table 2). The skin biopsy and the ELISA showed, respectively, a sen-
Table 3. Sensitivity of parasitological (skin-snip- ping) and serological (3-antigen cocktail ELISA) methods for the diagnosis of onchocerciasis in communities of different endemicity in Venezuela
Diagnostic Altamira Unturin Total method No. % No. % No. %
mf +ve 12 57.1 72 87.8 84 81.6 Sero +ve 19 90-5 79 96-3 98 95.1 Oncho +ve 21 100.0 82 100.0 103 100.0
Table 4. Sensitivity, specificity, and predictive value positive of the 3-recombinant antigen cock- tail ELISA as a screening test for onchocerciasis infection in comparison with the skin-snipping method in the populations of Unturti and Altamira, Venezuela
Altamira Unturhn mf +ve mf -ve Total mf +ve mf -ve Total
Sero +ve 10 9 19 69 10 79 Sero -ve 2 33 35 3 Total 12 42 54 72 :: ;; Sensitivity 83.3% 95.8% Specificity 78.6% 52.4% Predictive value + 52.6% 87.3%
“” I A 0 Altamlra Overall WMMD =099mtlmg
n Unturh7 Overall WMMD = 19.9mf/ma
40 -
8
g 30- 5
g $
20-
10 -
O- - r 15-24 2534 35-44 45+
Agwzlasses (years)
0 0.6 -
2 a 0.6 -
0.4 -
0.2 -
0.0 -I
cl5 15-24 25-34 35-44 Age-classes (years)
45+
Fig. 2. Age-profiles of mean microflarial load and anti-c chocercal antibodies in the studied populations ofAltamira ( ;, and Untudn (I). A. Geometric mean of Williams (WMMD) expressed as number of mflmg. B. Mean optical density values expressed as arithmetic means (AMOD); error bars represent the upper 95% confidence limit.
sitivity of 57.1% and 90.5% at Altamira, and of 87.8% and 96.3% at UnturPn, when compared with those in- dividuals classified as oncho +ve (Table 3). Table 4 summarizes the sensitivity, specificity, and predictive value of the ELISA as a screening assay when contrast- ed with the detection of infection by the skin-snip meth- od.
Discussion The cocktail of recombinant antigens OvMBlWO,
OvMBWll, and OvMBIY29 has been shown to be 100% specific (BRADLEY et al., 1993a) with the excep- tion of infections by Brugia malayi, which do not occur in Venezuela. Although the presence of Mansonella oz- zardi and M. perstans has been reported in the Middle and Upper Orinoco regions (BO?TO et al., 1983, 1984; YARZ.&AL et al., 1985a; FORMICA & BOTTO, 1990), no reactivity to the diagnosis cocktail of sera from individ- uals harbouring these infections has been demonstrated (J. E. Bradley, personal observations).
Owing to differences in the pattern of antigen recog- nition between localities, the sensitivity of individual an- tigens has been shown to vary between 43 and 61%. However, the use of a 3-antigen cocktail improves sen- sitivity up to 96% (BRADLEY et al., 1993a; RAMACHAN- DRAN, 1993). In the present study, the sensitivity of the cocktail in Unturin was 96.3% in relation to the oncho +ve (Table 3), and 95.8% in relation to the skin-snip +ve (Table 4). Although a similar sensitivity had been obtained in the hyperendemic area of Sierra Parima by means of an ELISA based on 0. volvulus soluble anti- gens (95.8%), this was accompanied by the poorer spe- cificity of 19.3% (YARZABAL et al., 1983).
28 CARLOS BOTI-0 ETAL.
c;;70 a ;60 250 e
?40 s! a30
20
10
0
<15 15-24 25-34
60
20
10
0
Cl5
Age-classas (years)
15-24 25-34 Aga-classas (yaws)
A
35-44
-I
45+
-I
Fig. 3. Prevalence (%) of individuals positive for skin micro- filariae (open bars), specific anti-Q VOZVUZUS antibody levels (grey bars), or any of these methods (solid bars) in communi- ties of northern and southern Venezuela. A. Altamira (north- central onchocerciasis focus). B. UnturBn (Amazon focus).
In Altamira the ELISA diagnosed nearly twice as many positive people as the skin snip; in this hypoen- demic community the parasitological method detected only 57.1% of the oncho +ve (Table 3). This finding is probably due to the higher rate of false skin-snip nega- tive results observed when the intensity of infection in the community is low (YOSHIMURA et al., 1982). Al- though located in an area of low transmission, a chem- otherapeutic control programme had been implemented in Altamira and similar villages of north- em Venezuela in the early 1960s (CONVIT, 1974). The programme had been interrupted lo-15 years before the present study, but several patients who then had patent onchocercal infections and were treated with DEC and suramin were seropositive in our survey. It is not clear whether these mf -ve-sero +ve subjects are pa- tients who continued to harbour live adult worms, con- stitute cases of reinfection, or were actually cured but still uossess residual antibodies. BRADLEY et al. (1993b) obs&ved high levels of specific IgG4 in apparently un- infected individuals from areas in which transmission had been interrupted by vector control for 8-10 years.
In Unturin the ELISA showed a larger number of mf -ve-sero +ve cases in children and young adults (~25 years). This observation may reflect the higher intensity of transmission and more frequent occurrence of new infections in this area or a higher exposure to L3 larvae. It has been suggested that exposure to L3 larvae may in- fluence the seropositive rate and that this may result from the presence of OvMBP/lO and OvMBP/l 1 anti- gens in the infective larvae of 0. volvulus (BRADLEY et
al., 1993b; TREE et al., 1995). It is most likely that the majority of the seropositive individuals in our study cor- responci in fact to patent infections, pre-patent Infec- tions, or non-infected neonle with anti-L3 antibodies; somk others (in Alta&r$ may be parasitologically cured people. All these conditions are clearly related to present or past risk of infection in the area. Therefore, the mean OD reflects endemicity status before the initi- ation of control programmes and may also be useful in areas where treatment has already begun.
The ELISA based on onchocercal recombinant anti- gens showed significant differences in mean OD values as well as in seroprevalence rates between the hypo- and hyperendemic communities. These differences were more pronounced in children and young adults (c25 years), suggesting that serology may be used as a reliable indicator of endemicity.
In contrast to observations in other hyperendemic ar- eas, where intensity of infection reaches a plateau in young adults and then levels off or declines with age WACKENZIE et al., 1987; MOYOU-SOMO et al., 19931, t‘he intensity of infection-in Unturan continueh to i& crease with gge (Bo~o et al., 1997), in agreement with observations made bv ANDERSON et al. (19741, RENZ et al. (1987) and BAS.&EZ & BoUssINESh (paper under review) in highly endemic areas of northern Cameroon. Mathematical modelline has confirmed that these local- ities are in fact at enldemic equilibrium (BAsAGEz, 19961. In Unturln. the AMOD declined sliahtlv in the oldesi age-band, resulting in an absence of-sihificant correlation between WMMD and AMOD. This may suggest both long-lasting exposure to L3 larvae, a de- crease of immunocompetence with age, or perhaps an inability to develop a protective immune response in this community. However, the analysis of mean infec- tion intensity per age-group may mask individual differ- ences in immune status (there were several cases among the elderly who, in spite of 30-40 years of exposure to infection, had no skin mQ.
When the serological assay was compared as a screen- ing method to skin-snipping in the study populations, the sensitivity of the ELISA in UnturBn was 96%, the same as the overall sensitivity achieved by the 3-antigen cocktail (BRADLEY et al., 1993a). The value obtained for specificity (52%) must be interpreted considering that those cases that are mf -ve are not necessarily truly non-infected, i.e., mf -ve-sero +ve individuals may not constitute false positives. As already pointed out, the se- rological test may be detecting light, early, or pre-patent infections in this locality of higher transmission. The values for Altamira show the trade-off between sensitiv- itv and snecificitv for this hvDoendemic localitv. The t&t is likely to be more spec& in areas of lowe; trans- mission, but the ELISA screening may be picking up people who are parasitologically cured yet still carry markers of previous infection. The difference in the pre- dictive value positive (PV+) between the localities is, in part, a reflection of the prevalence of infection in the 2 populations. PV+ is the probability of a person being actually infected when he or she tests positive by the ELISA method; it can be seen that the values of 87.3% and 52.6% are very similar to those classified as positive by the skin-snip method when the ‘truly infected’ pop- ulation are the oncho +ve (87.8% and 57.1% in Un- turPn and Altamira, respectively). In addition to demonstrating its validity in the study populations, a useful test must also be practical, accepted by the com- munity with minimal inconvenience and discomfort, and have a reasonable cost (HENNEKENS & BURING, 1987). We have estimated that the overall cost of the tests, from sampling to confirming parasite identity and obtaining a quantitative measure of infection, is US$ 8.03/person for the skin-snip method in comparison with US$ 2.20/person for the ELISA.
Venous blood-samples were taken in the present study because the objectives of the survey were broader
ONCHOCERCIASIS SEROEPIDEMIOLOGY IN SOUTHERNVENEZUELA 29
than those of assessing onchocerciasis endemicity alone. Filter-paper finger-prick blood samples would clearly be more practical and readily accepted. In fact, finger- prick blood samples are routinely taken for malaria di- agnosis and treatment in several isolated Yanomamij villages of southern Venezuela with the support of the community, who acknowledge the severity of the malar- ial problem in the area (700 cases per 1000 people an- nually). The usefulness and validity of the test with filter-paper samples are being evaluated at present (by S. Vivas-Martinez) .
In conclusion, the low molecular weight onchocercal recombinant antigens used here appear to be a practical tool for the description of endemicity in isolated re- gions. In this study a seroprevalence rate 250% was ob- served in all age-classes for the hyperendemic location. This community exhibits sclerosing keratitis and hang- ing groin (BOTTO et al., 1997), and a CMFL 220 mf/ mg, indicating that onchocerciasis is an important pub- lic health problem in the area (REMME et al., 1989). The seroprevalence in the < 15 year-olds from Unturin was 10 times as high as that recorded for this age-class in Al- tamira. The existence of these clear-cut differences would facilitate description of levels of endemicity in new areas by studying sera from the cl 5 years age- group, possibly through finger-prick filter-paper sam- ples in surveys integrated into routine malaria control activities. A high seroprevalence rate in children could serve as an ind<cator of local and intense transmission. This mav aid the selection of communities for further parasitolbgical surveys, administration of treatment, and subsequent epidemiological surveillance.
Acknowledgements We are grateful for the financial assistance of the World
Bank/UNDP (grant no. Ven-96002), and the logistic support of the Venezuelan OffIce for Indigenous Affairs (DAI), the Up- per Orinoco Health District (Drs M. Magris, A. Tami and L. Castro). and of the Venezuelan Air Force. M. G. B. is suuuort- ed by he Wellcome Trust. We also thank the Royal Society and the British Council for support through their exchange programmes with Latin America.
References Anderson, J., Fuglsang, H., Hamilton, P. J. S. & Marshall, T
F, de C. (1974). Studies on onchocerciasis in the United Cameroon RepLblic. II. Comparison of onchocerciasis in rain-forest and Sudan savanna. Transactions of the Row1 Soci- ety of Tropical Medicine and Hygiene, 68,209:222. -
BasBiiez, M. G. (1996). Density-dependent processes in the transmission of human onchocerciasis with particular refer- ence to the Onchocerca-Simulium interaction. PhD thesis, Imperial College of Science,Technology and Medicine, Uni- versity of London, UK.
BasPiiez, M. G. & YarzBbal, L. (1989). Onchocerciasis in the Sierra Parima and Upper Orinoco regions, FederalTerritory of Amazonas, Venezuela. In: Parasitic Diseases: Treatment and Control, Miller, M. J. & Love, E. J. (editors). Florida: CRC Press, chapter 31, pp. 231-256.
Botto, C. ( 1988). Epidemiologia de la Oncocercosti en una Comu- nidad Yanomami de la Sierra Parima, Alto Orinoco, y en una Comunidad Compesina de la Cordillera de la Costa: una Con- tribucidn a la Patogeografia Regional.Trabajo de Ascenso, Fac- ultad de Medicina. Caracas: Universidad Central de Venezuela.
Bono, C., YarzPbal, A., Lugo, E., Arango, M. & Yarzibal, L. (1983). Aspectos epidemiol6gicos de la mansonelosis en el Territorio Federal Amazonas. Venezuela. In: Las FiZuriasis Humanas en el Territorio kederal Amazonas, Venezuela, Yarzhbal, L., Holmes, R., BasPiiez, M. G., Petralanda, I., Bono, C., Arango, M. & Schkolnik, S. (editors). Caracas: PROICET-Amazonas, Publicaci6n Cientifica no. 2, pp. 21-40.
Botto, C., Arango, M. &YaxzBbal, L. (1984). Onchocerciasis in Venezuela: prevalence of microfilaraemia in Amerindians and morphological characteristics of the microfilariae from the Upper Orinoco focus. Tropenmedizin und Parasitologik, 35, 167-173. _ _ _ _
Bono, C., Planchart, S., Martinez, N., Castro, L., Gelrud, A., Vivas, L. & Grillet, M. E. (1997). Onchocerciasis hyperen- demic in the Unturen mountains: an extension of the en-
demic region in southern Venezuela. Transactions of the Royal Society of Tropical Medicine and Hygiene, 91, 150-l 52.
Bradley, J. E. & Unnasch, T. R. (1996). Molecular approaches to the diagnosis of onchocerciasis. Advances in Parasitology, 37,57-106.
Bradley, J. E., Helm, R., Lahaise, M. & Maizels, R. M. (1991). cDNA clones of Onchocerca volwulus low molecular weight antigens provide immunologically specific clones. Molecular and Biochemical Parasitology, 46, 219-228.
Bradley, J. E., Trenholme, K., Gillespie, A., Guderian, R., Ti- tanii. V.. Karam. M. & McRevnolds. L. (1993a). A cocktail of ;&ombinant’antigens pro;ide a sensitive se;odiagnostic test for onchocerciasis. American Journal of Tropical Medicine and Hygiene, 48,198-204.
Bradley, J. E., Gillespie, A. J., Trenholme, K. R. & Karam, M. (1993b). The effects of vector control on the antibody re- snonse to antigens of Onchocerca ~olvulus. Parasitolozv, 106, $63-370. -
Convit, J. (1974). Onchocerciasis in Venezuela. In: Research and Control of Onchocerciasis in the Western Hemisphere. Wash- ington DC: Pan American Health Organization, Scientific Publication no. 298, pp. 105-l 11.
Formica. S. & Bono. C. (19901. Filariasis focus due to Mun- , . sonella ozzardi and Mansone& perstans in the Amazon Feder- al Territory of Venezuela. Journal of Tropical Medicine and Hygiene, 93, 160-165.
Grillet, M. E., Botto, C., Basiiiez, M. G. & Barrera, R. (1994). Vector competence of Simulium metallicum s.1. (Diptera: Simuliidae) in two endemic areas of human onchocerciasis in northern Venezuela. Annals of Tropical Medicine and Para- sitology, 88, 65-75.
Hennekens, C. H. & Buring, J. E. (1987). Epidemiology in Med- icine. Boston: Little, Brown and Company.
Kirkwood, B. R. (1988). Essentials of Medical Statistics. Oxford: Blackwell Scientific Publications.
Lobos, E., Altmann, M,, Mengod, G., Weiss, N., Rudin, W. & Karam, M. (1990). Identification of an Onchocerca volvulus cDNA encoding a low molecular weight antigen uniquely recognized by onchocerciasis patient sera. Molecular and Bio- chemical Parasitology, 39, 135-145.
Mackenzie, C. D., Williams, J. F., O’Day, J., Ghalal, I., Flokhart, H. A. & Sisley, B. M. (1987). Onchocerciasis in southwestern Sudan: parasitological and clinical characteris- tics. American .‘fournal of Tropical Medicine and Hygiene, 36, 371-382. -
Moyou-Somo, R., Enyong, I? A., Fobi, G., Dinga, J. S., Laf- leur, C., Agnamey, P., Ngosso, A. & Mpoudi-Ngolle, E. (1993). A study of onchocerciasis with severe skin and eye lesions in a hyperendemic zone in the forest of southwestern Cameroon: clinical, parasitologic and entomologic findings. Americanrournal of Tropical Medicine and Hygiene, 48, 14-l 9.
Ramachandran, C. I?. (1993). Improved immunodiagnostic tests to monitor onchocerciasis control programmes-a multicenter effort. Parasitology Today, 9,76-79.
Remme, J., Dadzie, K.Y., Rolland, A. & Thylefors, B. (1989). Ocular onchocerciasis and intensity of infection in the com- munity. I. West African Savannah. Tropical Medicine and Para- sitologj, 40, 340-347.
Renz, A., Wenk, I’., Anderson, J. & Fuglsang, H. (1987). Srud- ies on the dynamics of transmission of onchocerciasis in a Sudan-savanna area of North Cameroon. V. What is a toler- able level of annual transmission potential? Annals of Tropical Medicine and Parasitology, 81,263-274.
Tree,T. I., Gillespie, A. J., Shepley, K. J., Blaxter, M. L.,Tuan, R. S. & Bradley, J. E. (1995). Characterisation of an immu- nodominant glycoprotein antigen of Onchocerca volvulus with homologues in other filarial nematodes and Cuenorhabditis el- egans. Molecular and Biochemical Parasitology, 69, 185-l 95.
WHO (1987). World Health Organization Expert Committee on Onchocerciasis. Third Report. Geneva: World Health Organi- zation,Technical Report Series, no. 752.
WHO (1993). International Ethical Guidelines for Biomedical Re- search Involving Human Subjects. Geneva: World Health Or- ganization.
Williams, C. B. (1937). The use of logarithms in the interpre- tation of certain entomological problems. Annuls of Applied Biology, 24,404-414.
YarzPbal, L., Arango, M., Bono, C., Jaimes, J. L., SBnchez- Beaujon, R. & Raga, L. M. (1983). Nuevas observaciones sobre la endemia oncocerc6sica de la Sierra de Parima,T. F. Amazonas, Venezuela. 1n:Las Filariasis Humanas en el Terri- torio Federal Amazonas, Venezuela, YarzPbal, L., Holmes, R., Basifiez, M. G., Petralanda, I., Bono, C., Arango, M. & Schkolnik, S. (editors). Caracas: PROICET-Amazonas, Publicaci6n Cientifica no. 2, pp. 3-19.

30
Yarzabal, L., Ba&iiez, M. G., Ramirez-Perez, J., Ramirez, A., Botto, C. &Yarzabal, A. (1985a). Experimental and natural infection of Simulium sanchezi by Mansonella ozzardi in the Middle Orinoco region ofVenezuela. Transactions of the Royal Society of Tropical Medicine and Hygiene, 79,29-33.
Yanabal, L., Botto, C., Arango, M., Raga, L. M.,Wong, F., Al- lan, R., Jaimes, J. L. & Sanchez-Beaujon, R. (1985b). Epi- demiological aspects of onchocerciasis in the Sierra Parima, Federal Territory of Amazonas, Venezuela. In: La Oncocerco- sis en Amdrica,YarzPbal, L., Botto, C. & Allan, R. (editors). Caracas: Ediciones CAICET, Publication Cientifica no. 3,
CARLOS BOlTO ETAL.
pp. 43-63. Yoshimura,T, Hashiguchi,Y., Kawabata, M., Flores C., 0. F.,
Gudiel, 0. 0. & Mazariegos L., E. C. (1982). Prevalence and incidence of onchocerciasis as baseline data for evalua- tion of vector control in San Vicente Pacaya, Guatemala. Transactions of the Royal Society of Tropical Medicine and Hy- giene, X,48-53.
Received 9 October 1997; revised 26 August 1998; accepted for publication 8 September 1998
TRANSACTIONS OF THE ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENE (1999) 93,30-3 1
1 Short Report 1
HIV-2 status in southern India
R. Kannangz$, S. Ramalingam’, R. C. Ca;til.lo’, E g E&m&; J. John , G. Sridharan and
. . ‘Department of Clinical Virology, Christian Medical College Hospital, Vellore 632004, India; ‘Department of Molecular Microbiology and Immunology, The Johns Hopkins School of Hygiene and Public Health, Baltimore, Maryland 21205, USA
Keywords: human imrmmodeficiency virus type 2, epidemiol- ogy, seroprevalence, India
Human immunodeficiency virus type 2 (HIV-2) was first described in Senegal in 1985 and was initially believed to be restricted to West African countries (BRAIN et al., 1985). In this region, prevalence measured by serological testing ranges from 0.2% to 25% among different populations, and is generally higher in prosti- tutes (RANKI, 1997). Among European countries, Por- tugal has a high prevalence rate for HIV-2, which accounts for lo- 12% of all HIV infections (KANKI, 1997). In Asia, most of the HIV-2 cases have been reported from Indian port cities. The first report of HIV-2 infection in western India was from Mumbai in 1991 (RUBSAMEN-WAIGMANN et al., 1991). HIV-2 infections were reported in Madras and Vishakapatnam in southern India in 1993 (BABU et al., 1993). The routes of transmission of HIV-2 in the human population are the same as for HIV-l, although transmission in West Africa appears to be less efficient (KANKI, 1997). There is some evidence that infection with HIV-2 may interfere
with HIV-l infection, offering a level of cross-protection (AABY et al., 1997).
We analysed immunoblot results of the years 1993 through 1997 to assess the burden of infection with HIV- 2. Samples were obtained from several sources within the Christian Medical College Hospital in Vellore, Tamil- nadu, a major regional health care centre. The primary sources were the Infectious Disease Clinic, the STD clinic and individual physicians, all referring patients for testing at the Department of Clinical Virology. Samples positive by enzyme-linked immunosorbent assay (ELI- SA) were confirmed using the HIV blot 2.2 (GeneLabs, Singapore) or INNOLIA (Innogenetics, Belgium) kits. HIV blot 2.2 and INNOLIA contain gp36 bands for the specific detection of HIV-2. Of a total of 3986 ELISA- positive samples tested during the 5-year period, 3040 were found to be positive for HIV upon immunoblot testing. Among the HIV-positive samples, 96.2% were reactive to HIV-l alone, 2.1% to both HIV- 1 and HIV-2, and l-7% to HIV-2 alone. Yearly immunoblot data from 1993 to 1997 are presented in Table 1.
Earlier reports from western Indian states such as Maharashtra and Goa showed a high prevalence of HIV- 2 infection. Among a group of high-risk individuals in Mumbai, 4% of all HIV-positive patients were infected with HIV-2, and 17% had dual HIV- 1 and -2 infections. In Goa, HIV-2 accounted for 33% of all HIV infections (RUBSAMEN-WAIGMANN et al., 1994). The geographical distribution of our patient population is shown in Table 2. The southern state ofAndhra Pradesh contributed the maximum number of HIV-2 positive samples.
Our data show a relatively low (when compared to HIV-l) but continuous circulation of HIV-2 in southern India. Initially, in 1993 and 1994, the prevalence of HIV- 2-infected individuals was higher than those dually infected with HIV-l and HIV-2. However, at present, dual infection with these viruses is showing a higher prevalence. This may be due to the slower heterosexual
Table 1. Immunoblot data for HIV infection in and around Vellore in 1993-97
Year
1993 1994 1995 1996 1997 Total
Total positive
253 645 708 747 687
3040
HIV-l HIV-2 HIV-l and HIV-2
No. (%I No. (“/I No. (%I
237 9 7 627 15 3 690 8 10 711 11 25 658 10 19
2923 53 (1.7) 64
Address for correspondence: David H. Schwartz, Department of Molecular Microbiology and Immunology, The Johns Hop- kins School of Hygiene and Public Health, 6 15 N. Wolfe Street, Baltimore, MD 21205, USA; phone +l 410 955-3175, fax +l 410 955-0105, e-mail [email protected]
transmission of this virus because of the lower infectivity potential. Given the stable prevalence of HIV-2 in this region (at least as determined by serology), it will be important to initiate prospective studies of disease progression and relative risk for subsequent HIV-l
Related Documents