ON CHLOROFORM AND OTHER ANAESTHETICS THEIR ACTION AND ADMINISTRATION BY JOHN SNOW, M.D. Licentiate of the Royal College of Physicians {Continued from page 467) In the Experiments 24 and 25, related half grown. Ten or twelve drops of chloro- above, the animals were first made form were put into a short bent metal tube, insensible by vapour of moderate strength, lined with bibulous paper, which formed in order to keep them quiet for the appli- part of an inhaler, and one end of the tube cation of the stethoscope whilst the was applied to the animal's nose, which stronger vapour was inhaled, but when closed it. The guineapig consequently animals are made to breathe air contain- breathed backwards and forwards through ing ten per cent, or so of vapour of chloro- the tube, which was, moreover, warm from form from the first, death takes place in being held in the hand. It struggled at the same manner, i.e., by the direct action first, endeavouring to get away from Dr. of the chloroform on the heart. Under Sibson, who held it; but in twenty or these circumstances the creatures die thirty seconds it became quiet; and suddenly, after a brief interval of agitation observing that the conjunctiva was insen- and excitement, without previous insensi- sible, I withdrew the chloroform, and the bility. This is what has happened in some guineapig was laid on the table. We of the accidents from chloroform to be remarked that the breathing was very related further on; whilst in many cases slow; and scarcely had this remark been death has happened after a longer or made, when it ceased altogether, three or shorter period of insensibility. four inspirations only having been made In many of the fatal cases of inhalation since the inhalation was left off. Dr. of chloroform the alarming symptoms Sibson proceeded immediately to open the commenced whilst the patient was still body; but as soon as he had divided the inhaling, but in a considerable number integuments of the chest the animal began there was no sign of danger until after to make some convulsive gasping inspira- the inhalation had been left off; and tions during which the mouth was widely this is a result which may be imitated on opened, and we observed that the dia- animals. The two following experiments, phragm acted alone, the ribs being pressed which were made at Dr. Sibson's on inwards by the atmosphere. The heart December 27th, 1849, illustrate this point, was not contracting at all when the peri- Experiment 29. The subject of this cardium was first opened; but in a few experiment was a young guineapig, about moments the auricles began to contract 498 by guest on July 29, 2016 http://bja.oxfordjournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ON CHLOROFORM AND OTHER ANAESTHETICS
THEIR ACTION AND ADMINISTRATION
BY
JOHN SNOW, M.D.
Licentiate of the Royal College of Physicians
{Continued from page 467)
In the Experiments 24 and 25, related half grown. Ten or twelve drops of chloro-above, the animals were first made form were put into a short bent metal tube,insensible by vapour of moderate strength, lined with bibulous paper, which formedin order to keep them quiet for the appli- part of an inhaler, and one end of the tubecation of the stethoscope whilst the was applied to the animal's nose, whichstronger vapour was inhaled, but when closed it. The guineapig consequentlyanimals are made to breathe air contain- breathed backwards and forwards throughing ten per cent, or so of vapour of chloro- the tube, which was, moreover, warm fromform from the first, death takes place in being held in the hand. It struggled atthe same manner, i.e., by the direct action first, endeavouring to get away from Dr.of the chloroform on the heart. Under Sibson, who held it; but in twenty orthese circumstances the creatures die thirty seconds it became quiet; andsuddenly, after a brief interval of agitation observing that the conjunctiva was insen-and excitement, without previous insensi- sible, I withdrew the chloroform, and thebility. This is what has happened in some guineapig was laid on the table. Weof the accidents from chloroform to be remarked that the breathing was veryrelated further on; whilst in many cases slow; and scarcely had this remark beendeath has happened after a longer or made, when it ceased altogether, three orshorter period of insensibility. four inspirations only having been made
In many of the fatal cases of inhalation since the inhalation was left off. Dr.of chloroform the alarming symptoms Sibson proceeded immediately to open thecommenced whilst the patient was still body; but as soon as he had divided theinhaling, but in a considerable number integuments of the chest the animal beganthere was no sign of danger until after to make some convulsive gasping inspira-the inhalation had been left off; and tions during which the mouth was widelythis is a result which may be imitated on opened, and we observed that the dia-animals. The two following experiments, phragm acted alone, the ribs being pressedwhich were made at Dr. Sibson's on inwards by the atmosphere. The heartDecember 27th, 1849, illustrate this point, was not contracting at all when the peri-
Experiment 29. The subject of this cardium was first opened; but in a fewexperiment was a young guineapig, about moments the auricles began to contract
498
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
ON CHLOROFORM AND OTHER ANAESTHETICS 499,
rhythmically. The lungs were of a lightred colour.
Experiment 30. Another guineapig ofthe same age was treated in the samemanner, except that I removed the tubefrom the nose for a short time betweenevery two or three inspirations, in order tosee if I could not make it insensible in thisway without a fatal result. In half aminute or so the animal no longer requiredto be held, but lay on the table withoutmaking any resistance, the conjunctivabeing still sensible, and some motion of thelimbs, apparently voluntary, remaining.It only inhaled once after Dr. Sibsonceased to hold it, and whilst in the statejust described, and then only for two orthree inspirations. After this it appearedquite insensible, and no more chloroformwas given. It breathed at first naturally,except more slowly and gently than beforethe inhalation; but the breathing becameslower, and ceased altogether about aquarter of a minute after the inhalationhad been left off. The body was openedimmediately. When the pericardium wasopened, the auricles were observed to con-tract slightly, and the contractions in-creased after their exposure to the air.
The amount of vapour in the airbreathed by these two guineapigs is notknown, but there is no doubt that it wasupwards of eight per cent.
FATAL CASES OF INHALATION OF
CHLOROFORM
If it were possible for a medical man to*mistake or disregard the symptoms ofapproaching danger, and to go on exhibit-ing vapour of chloroform, diluted to a
proper strength, till the death of the:patient, this event would take place slowlyand gradually, as in Experiment 23,related above, and every other experimentin which the air did not contain more thanfive per cent, of vapour. The action o£the heart would survive the respiration;,there would be a great tendency to spon-taneous recovery, and the patient wouldbe easily restored by artificial respiration,if it were performed whilst the heart wasstill acting; as I have always found it to besuccessful in animals under these circum-stances.
In examining the recorded cases of fatal,inhalation of chloroform, we shall find,,however, that they have none of them,taken place in this gradual manner; butthat in all cases the fatal symptoms, if notthe actual death, have come on verysuddenly. Dr. Sibson was, I believe, thefirst to point out that, in the fatal cases ofinhalation of chloroform, death was causedby its paralysing the heart; but he was notat that time aware of the physical con-ditions under which this agent may act:directly on the heart. In commenting onthe first four deaths from chloroform, hesays: * " In all the four cases it is manifestthat the immediate cause of the instan-taneous death lay in the heart. The heart,,influenced by the poison, ceased to con-tract, not from the cessation of respiration,,for the heart in asphyxia will beat fromone to three minutes after respiration hasceased, but from immediate death of theheart. There is no doubt a combinationof causes operating to destroy the heart's-contractile power: the mental influencethe congestion in the systemic, and that in
* London Medical Gazette, vol. xlii, 1848, p. 109.
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
500 BRITISH JOURNAL OF ANAESTHESIA
the pulmonary capillaries, will all have amaterial influence." And further on he.says: "We are obliged, then, from theexperience of these cases, to conclude, thatin man the death is usually instantaneous,and due, as every instantaneous death is,to paralysis of the heart. In animals the•death is usually due to paralysis of themuscles of respiration. It is chiefly owingto the superior control of the mind overthe body in man, that in him the poisonacts on the heart more than in dogs."
I had been long aware that chloroformwas capable of paralysing the heart inanimals; and, indeed, that sulphuric etherwould do so when it could reach the heartin sufficient quantity;* and soon after Dr.Sibson's remarks I was able to ascertainand point out the strength of the vapourwhich will produce this effect, and howone may avoid the risk of it, by having thevapour sufficiently diluted, f The greaternumber of experimenters who have killedanimals with chloroform have found thatthe action of the heart continued after thebreathing ceased; but they did not either•control or ascertain the proportion whichthe vapours of chloroform bore to theinspired air. In Mr. Thomas Wakley's•experiments the action of the heart con-tinued after the breathing had ceased; andthis was the case in a great number ofexperiments performed by a Commissionwhich reported to the Society of Emula-tion of Paris, in 1855.t
This Commission came to the conclu-sion that, in all instances in which animalsare killed by chloroform, the action of theheart survives the respiration; but they
* On the Inhalation of the Vapour of Ether, p. 82.t Medical Gazette, vol. xlii, p. 415.tSee l'Union M<dicale, 1855, No. 13.
might have administered chloroform to anequal number of human patients withoutany one of them being cut off by suddenparalysis of the heart. If animals wereusually to die suddenly of paralysis of theheart, when the chloroform is given in amanner similar to what may be called itsordinary administration to patients, weshould be at a loss to know how this agentcould be used at all. It is only reasonableto suppose that, in experiments so conduc-ted, that mode of death should usually bemet with which would occur to the humansubject, if the chloroform were continued,in the disregard of dangerous symptoms,till death should ensue. I have, indeed,been informed of several instances inwhich animals died in a sudden, and whatwas thought an unaccountable manner,whilst chloroform was given to preventthe pain and struggles which would beoccasioned by physiological experiments.In these cases there is no doubt the heartwas paralysed; but the experimenters wereoften too intent on other matters to observethe circumstance. By a proper arrange-ment of circumstances, however, one mayproduce at will the event in animals whichoccurs, in fact, so very rarely to a patient,although it may at any time happen ifgreat caution, guided also by rightprinciple, is not used.
Air, when saturated only at 60° Fah.,contains 12 per cent of vapour ofchloroform, and at 70° 19 per cent;and 8 or 10 per cent, in the inspired air iscapable, as we have seen, of causingsudden death by paralysing the heart; but
' in practice the air is usually far from beingsaturated, in passing over a handkerchiefor similar material, even at the tempera-ture at which it is inhaled; and this is
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
ON CHLOROFORM AND OTHER ANESTHETICS 501
generally lowered considerably by theabsorption of caloric by the chloroform, asit changes its condition from a liquid to avapour. Moreover, air strongly chargedwith vapour of chloroform is not easy tobreathe, owing to its pungency; and thephysiological knowledge and close atten-tion of every medical man who administersthis medicine causes him to withdraw itimmediately on the least appearance ofdanger.
Case 1. The first death from chloro-form was that of Hannah Greener, whichoccurred at Winlaton, near Newcastle, onthe 28th of January, 1848. The patientwas a girl of 15, who required to have thenail of the great toe removed. A similaroperation had been performed on the otherfoot, in the previous November in theNewcastle Infirmary, when ether wasadministered with a satisfactory result.The following is the account of the acci-dent by Dr. Meggison, who administeredthe chloroform: " She appeared to dreadthe operation, and fretted a good deal: infact, she commenced sobbing on our enter-ing the house, and continued so untilseated in the operating chair, and com-mencing the inhalation, which was donefrom a handkerchief on which a teaspoon-ful of chloroform had been poured. Afterdrawing her breath twice, she pulled myhand from her mouth. I told her toput her hands on her knees, and breathequietly, which she did. In about half aminute, seeing no change in breathing, oralteration of pulse, I lifted her arm, whichI found rigid. I looked at the pupil andpinched her cheek and, finding her insen-sible, requested Mr. Lloyd to begin theoperation. At the termination of the
C
semilunar incision she gave a kick ortwitch, which caused me to think thechloroform had not sufficient effect. I wasproceeding to apply more to the handker-chief, when her lips, which had beenpreviously of a good colour, becamesuddenly blanched, and she spluttered atthe mouth, as if in epilepsy. I threw downthe handkerchief, dashed cold water in herface, and gave her some internally,followed by brandy, without, however, theleast effect, not the slightest attempt at arally being made. We laid her on thefloor, opened a vein in her arm, and thejugular vein, but no blood flowed. Thewhole process of inhalation, operation,venesection, and death, could not, I shouldsay, have occupied more than twominutes."*
An examination of the body was madethe day after death by Sir John Fife andDr. Glover, who reported as follows: —" The body was that of a well-grownfemale of about fifteen years of age. . . .On opening the chest, the lungs were notcollapsed. One or two very slightadhesions were encountered on separatingthem from the walls of the chest. Theexternal appearance of both lungs, overthe whole surface, but especially in theinferior portions, was that of organs in avery high state of congestion. They weremottled with patches of a deep purple,blueish, or scarlet hue. They were every-where crepitant. Along the outer andinterior border of both lungs, particularlyof the upper lobe of the left lung, wereseveral emphysematous bubbles of smallsize. . . . The pulmonary tissue was filledwith bloody froth, which was also found
* London Medical Gazette, vol. xli, p. 255.
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
502 BRITISH JOURNAL OF ANAESTHESIA
in the interior of the bronchi, mixed withmucus. There was no appearance ofhepatization. On examining the larynxand trachea, the epiglottis was foundreddened at the summit, of a vermilionhue. The mucous membrane of thelarynx was redder than natural—mottledwith vascular patches. The sinuses of thelarynx contained a good deal of darkmucus. The oesophagus was healthy. Thestomach was distended with food. Someof the veins were more distinct than usual.The heart contained dark fluid blood inboth its cavities: very little in the left. Itsstructure, and that of the great vessels nearit, quite healthy. The brain, externallyand internally, was more congested thanusual; and the ventricles contained rathermore than the usual quantity of serum."*
Sir John Fife and Dr. Glover expressedthe opinion that chloroform caused deathby producing congestion of the lungs.After the further experience which hasbeen gained respecting chloroform, thisopinion of the mode in which it causeddeath, in the above case, would probablynot now be offered. Indeed, in similarcases which have since occurred, the sameopinion has not been advanced and as thelungs were crepitant throughout, in theabove case, it is probable that the con-gestion was not greater than is commonlymet with in cases of sudden death withouthaemorrhage. Dr. Simpson published hisopinion, immediately after this caseoccurred, that it was not caused by the
• Opus cit., p. 253.
chloroform, but by the brandy which wasgiven when the alarming symptoms cameon; but Dr. Meggison replied that only ateaspoon of brandy was given; that it wasswallowed, though with difficulty; thatthere were no symptoms of choking fromit; and that the girl was without pulsewhen it was given, f
From the lips becoming suddenlyblanched in the above case, there is everyreason to conclude that the heart wassuddenly paralysed. The patient breathedfor a little time after this, and was able toswallow, though with difficulty. Theprocess of inhalation occupied only a littlemore than half a minute in Dr. Meggi-son's estimation; yet he appeared to thinkthat the fluid drachm of chloroform whichhe had put on the handkerchief hadevaporated; for he was about to applymore when the alarming symptomsappeared. But supposing only one-thirdof the drachm was actually inhaled intothe lungs in the half minute, the vapourwould necessarily be in a highly concen-trated state—probably twenty cubicinches of vapour in 200 cubic inches ofair, which would be adequate to occasionthe result which happened. In the shortspace of about half a minute, the bloodcould not be uniformly impregnated withthe vapour; only a portion of it could passthrough the lungs in the time; yet, as thepatient was rendered insensible, this por-tion must necessarily have been highlycharged with vapour.
t Opus cit, p. 341.
(To be continued)
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
WORLD CONGRESS OF ANAESTHESIOLOGISTS, 1955
THERE will be unanimous agreement Mr. Suiirhoff was followed by Mr.among all, whatever their nationality or Zwyndrecht an Alderman of the Haguethe relative profundity of their interest in who welcomed the delegates on behalf ofanaesthesia, that this first World Congress the Burgomaster and Corporation. Prof,of Anaesthesiologists held at Schevenin- Dr. E. Grzegorzewski of the World Healthgen was an enormous success. From the Organization, which had taken thestately opening in the Hall of Knights greatest interest in the planning for the(Ridderzaal) at the Hague to those final World Congress and World Federation,impressive moments in the CentralSessions Hall of the Kurhaus whenthe World Federation of Societiesof Anaesthesiologists was founded, thoseattending were kept busy, interestedand entertained. The Great Hall ofthe Ridderzaal, an ancient 13th-centurycastle, where the Queen of the Nether-lands annually carries out the stateopening of her Parliament, with its vastbeamed roof and candelabra, remindedmany of the great hall at Lincoln's Innwhere the Association of Anaesthetists ofGreat Britain and Ireland held its Dinnerin 1946 to celebrate the centenary of thediscovery of Ether Anaesthesia. Here theCongress was formerly declared open byMr. J. G. Suurhoff, Her Majesty'sMinister of Social Affairs and PublicHealth. In his opening remarks Mr.Suurhoff drew attention to the wide scopeof this specialty. Advances in anaesthesiahad not only led to tremendous advancesin surgery, particularly of the heart and Kurhaus at Scheveningen and in thelungs., but the skill and knowledge of the mornings the delegates divided into twopractitioners in this specialty had been groups to attend papers and discussions inapplied to useful purpose in the treatment the two smaller North and South Sessionof poliomyelitis and to assist in the modern Halls. A special delight at these sessionstreatment of the pyschiatric patient. were the beautiful floral decorations of
503
pointed out that anaesthesia had been andstill was a major public problem in manyparts of the world. It could be regardedas " the preventive discipline to allbranches of medicine where surgicalintervention is required". In splendid,truly statesmanlike speeches delivered infour languages Dr. G. R. Ritsema vanEck, President of the Organizing Com-mittee emphasized that all the efforts ofdelegates and congressioners during theweek must be directed to the one end—toserve mankind in the relief of suffer-ing. He particularly welcomed thescientists and surgeons who might beassociated with anaesthetists in the variousnational societies to whom "we owe somuch and whom we regard as our greatestfriends".
The academic sessions'of the Congressreached a very high standard in severalinstances. They were held in the after-noons in the large Central Hall in the
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
504 BRITISH JOURNAL OF ANAESTHESIA
the stage and rostra, and the excellentarrangement that had been made fortranslation.
On each chair were headphonesthrough which, by the simple adjustmentof a switch the words of the speaker couldbe heard in English, French and German.Although (not surprisingly) the translatorshad a little difficulty with some of themore technical papers, the arrangementsworked on the whole splendidly andadded very greatly to the success of theCongress.
The speakers had been allottedvarious times for their papers which werestrictly enforced. This occasionally ledto some embarrassment and, perhapsmore unfortunately, to readers hurryingunduly through communications. Inone case an interesting paper was"cut off", after about one-third of itscourse through a misunderstanding.These incidents, however, were theprice, and probably a very small one,which had to be paid for the necessarylimitation of the more voluble speakers.
It was to be expected that the mainthemes of this gathering would be Hypo-thermia, Hypotension, and the RelaxantDrugs. It would be quite invidious todraw attention to any few of the manycommunications given, but the programmeof papers listed below shows the widevariety of the fare offered. Certainly theydemonstrated the contrasting approachesmade to the problems of anaesthesia.
Not the least interesting features werethe three " Panel-Discussions ". At these,questions previously written in wereanswered by a panel of four experts on thesubject under consideration, presided overby a moderator. One recalls with
pleasure Professor Pask's lucid answersand deft dealing with an obscure questionon carbon dioxide and also the eloquenceof Professor Beecher. It was clear that allpresent did not agree with the latter's pro-nouncement that the only two advances inanaesthesia in the last two decades whichhad permitted the surgeon to do what hadhitherto been impossible were Hypo-tension and Hypothermia.
The social side of the Congress was wellup to the standard of its more seriousaspects. The weather on the whole wasexcellent except for one morning andafternoon of rain, and the admirablebathing facilities were greatly appreciated.Each afternoon there was an excursion forAssociate Members to the various attrac-tive and historically interesting featuresin the neighbourhood. In addition therewas a dance and variety show in the HotelWitte Burg in the Hague, one feature ofwhich was attractive folk dancing innational costume. This was an eveningof complete relaxation and convivialitywhich will long be remembered by thosepresent. The closing Congress Dinnerwas held at the Palace Hotel, Schevenin-gen.
The climax of this outstanding Congresswas the General Assembly of the variousnational delegates and of the Congres-sioners in the Central Hall of the Kurhausat which was formed the World Federa-tion of National Societies of Anaesthesio-logists. On the stage delegates from themajority of countries in the world sat oneither side of Dr. Harold Griffiths, whohad been the chairman of the InterimCommittee responsible for the planningof the World Federation. Dr. Goldblat(Belgium), Secretary of the Interim Com-
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
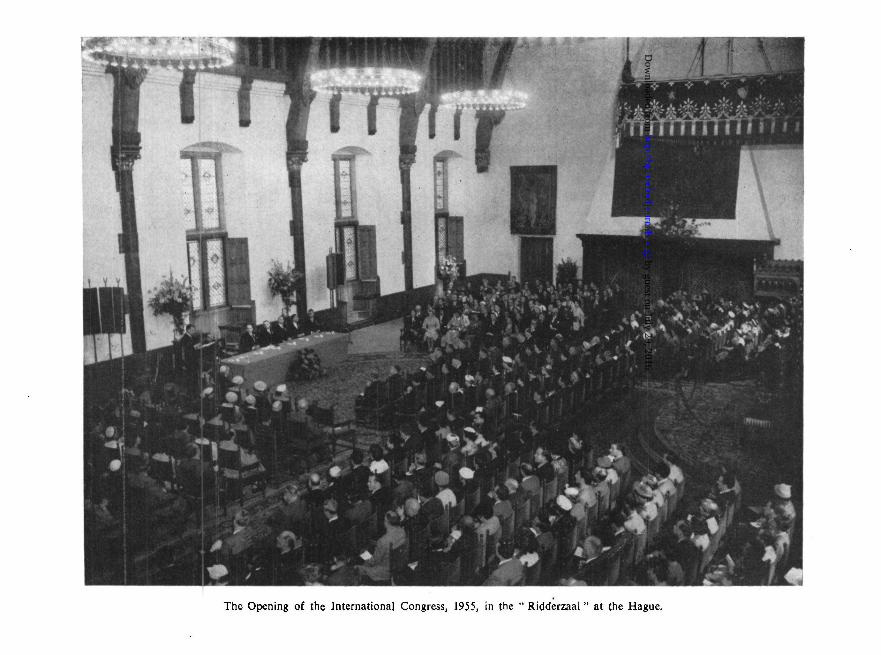
The Opening of the International Congress, 1955, in the " Ridderzaal" at the Hague.
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
506 BRITISH JOURNAL OF ANAESTHESIA
mittee, then gave the report of the Com-mittee on Credentials to the Assembly,which had approved of the credentials ofthe following delegates:
DelegatesArgentine: Dr. M. Alarcon, Dr. G. VarelaAustralia: Dr. N. JamesAustria: Dr. O. MayrhoferBelgium: Dr. A. GoldblatBrazil: Dr. O. BastosCanada: Dr. H. R. Griffiths, Dr. R. A. GordonChile: Dr. L. C. GuarderasColumbia: Dr. G. DelgadoCuba: Dr. Corbcllo-Denmark: Dr. O. SechcrFinland: Dr. E. O. TurpeinenFrance: Dr. J. Boureau, Dr. P. JaquenardGermany: Dr. R. FreyGreat Britain: Dr. W. Low, Dr. G. Organe, Dr.
J. Gillies, Dr. R. ShackletonIndia: Prof. S. TalwalkarIsrael: Dr. FoldesItaly: Prof. E. CiocattoNetherlands: Dr. C. Ritsema van EckNorway: Dr. I. LundPortugal: Dr. E. Lopes-SoaresSouth Africa: Dr. RobertsSweden: Dr. T. GordhSwitzerland: Dr. K. ZimmermannSpain: Dr. D. MontonUruguay: Dr. A. CanellasVenezuela: Dr. C. Hogi
ObserversCzechoslovakia: Dr. H. KadlicGreece: Dr. S. CouremenosNew Zealand: Dr. A. SlaterU.S.A.: Dr. L. WrightU.S.S.R.: Dr. ZeitzenYugoslavia: Dr. A. Longhino
The Constitution and Bye-laws asdrawn up and approved by the InterimCommittee were then unanimouslyadopted, after which Dr. H. Griffithsannounced: "The baby is now born".For legal reasons this Constitution and
Bye-laws are registered in the Dutchlanguage. The Nominations Committeethen put forward their nominations forthe World Federation which were asfollows:
PresidentProfessor H. R. GRIFFITHS (Canada)
V ice-PresidentsDr. C. RITSEMA VAN ECK (Holland)Dr. A. GOLDBLAT (Belgium)Dr. R. FREY (Germany)Dr. CURBELLO (Cuba)
Secretary-TreasurerDr. GEOFFREY ORGANE (Great Britain)
Owing to the fact that the Secretary-Treasurer could no longer serve as aNational Delegate, being supranationalin his duties, Dr. Cecil Gray took his placein the British Delegation.
After his election as President, Dr.Griffiths expressed his appreciation of thegreat honour that had been done him andreviewed the history of the formation ofthis World Federation. He paid tributeto the inspiration of Professor Monot andDr. Thalheimer, whose enthusiasm at the1951 Congress in Paris had led to theformation of the Interim Committee. Itwas a result of the many deliberations ofthis Interim Committee over the last fouryears which had now culminated in thepresent formation of this internationalbody. He thanked particularly Dr. Gold-blat, the Secretary of the Interim Com-mittee, for all his work during the deliber-ations. After his election as Secretary-Treasurer, Dr. Geoffrey Organe expressedhis appreciation of the honour. If. histitle to this post depended on the numberof countries he had visited he was wellqualified, as since the war he had travelled
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
WORLD CONGRESS OF ANAESTHESIOLOGISTS, 1955 507
to fourteen countries in four continents.He said he regarded war as " the greatestfutility", and considered it was alwaysthe result of misunderstanding. The bestway to avoid misunderstanding was to getto know each other better and he was surethat the World Federation had an impor-tant part to play in this respect. It wasnot the purpose of the new Federation tointerfere in the affairs of any country orof any National Society of Anaesthesiolo-gists. It would be its duty to give helpwhen help was required and in this hewould serve to the best of his ability. Heintended as soon as it was possible to visitthe member countries to get to know thembetter. He paid tribute to Dr. Goldblatwho had been assiduous in his capacity asSecretary of the Interim Committee.
The election of the Executive Com-mittee followed and the following dele-gates were elected:
Dr. J. BoureauDr. E. CiocattoDr. J. GilliesDr. A. GoldblatDr. A. Gonzales VarelaDr. T. GordhDr. R. A. GordonDr. H. R. GriffithDr. N. R. JamesDr. O. MayrhoferDr. R. P. W. ShackletonDr. Zairo VieiraDr. S. G. Talwalkar (co-opted)Dr. Ritsema van Eck (co-opted)
It was unanimously agreed to send atelegram to Her Majesty the Queen of theNetherlands, expressing the gratitude andloyalty of those present for having sogenerously given her patronage to theCongress.
The time and place of the next Inter-national Congress were left for an earlydecision by the Executive Committee.
LIST OF LECTURESPhysiologyProf. Dr. T. Sj0strand, Stockholm: "Blood
Volume and Regulation of Circulation." ,Prof. E. A. Pask, Newcastle upon Tyne.: " Tech-
nique for Assessing the Central RespiratoryDepression in the Presence of Muscle Re-laxants."
Dr. G. RodewaM, Hamburg, Dr. R. Beer, Mar-burg : " Haemoxytensiometry."
Dr. R. F. Woolmer, Bristol: "The Role of theAnaesthetist in the Treatment of BulbarPoliomyelitis and Tetanus."
Dr. H. C. Churchill-Davidson, London: "AcuteMassive Pulmonary Collapse."
Dr. P. R. Bromage, Chichester, Portsmouth:" Blood pressure and Vital Capacity."
Dr. R. P. Harbord, Leeds: " Pulmonary Ventila-tion during Anaesthesia."
Dr. B. Sommer Pedersen, Hiller0d: " Anaesthesiaand Stress."
Dr. J. D. Robertson, Edinburgh: " Some Effectsof Anaesthetics on the Reflex Regulation ofthe Circulation."
Prof. Dr. P. Knoefel, Louisville: "The RenalCirculation in Anaesthesia."
Dr. J. L. McClung, U.S.N.R., Dr. G. C. Sutton,U.S.N.R., Dr. D. M. Little, U.S.N.R.:" Measurements of the Mechanical and Elec-trical Events of the Cardiac Cycle; (1) EtherAnaesthesia."
Dr. G. Moricca, Dr. L. Manni, Rome: " Electro-and Balistocardiographic Studies on Patientssubmitted to Various Types of AnaestheticInduction."
Dr. Sadi Sun, Aksaray, Istanbul: "Anaesthesiain Intra-thoracic Surgery without CO,Absorption (High Flow Technique)."
Dr. H. Gopfert, Heidelberg: "Observations onthe Physiology of Respiration in Experimentswith' rapid-action' COS Analysers."
Dr. H. Hornicke, Hannover, Dr. J. Stoffregen,Heidelberg: "Comparison of Pressure-breathing and Positive-Negative Breathing inExperiments with Animals."
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
508 BRITISH JOURNAL OF ANAESTHESIA
Dr. F. R. Gusterson, Worthing: " Tonsillectomyin Children " (with film).
Dr. G. Arezio, Pavia: " Influence of Glucose-1-phosphate on the modifications of the Elec-trocardiogram in Anaesthesia."
Dr. D. Carbonera, Dr. V. Freyrie, Pavia: "Res-piratory Insufficiencies in Anaesthesia."
Dr. L. Barth, Berlin-Buch: "Left-right Differ-ences, during Pulmonary Ventilation in Inter-mitted Pressure-breathing in the openThorax."
Dr. H. Oehmig, Dr. J. Stoffregen, Heidelberg:" On a New Apparatus to StimulateExpectorations."
Dr. D. Mendelsohn, Philadelphia: " Electro-cardiographic and Blood Pressure Changesduring and following Biliary Tract Surgery."
Dr. S. A. Klein, The Hague: "Some Physio-logical Considerations on the Administra-tion of Oxygen during General Anaesthesia,especially in the Elderly Patient."
Dr. R. E. Mansfield, London: " The Control ofSecretions in Thoracic Surgery."
Dr. B. A. Sellick, London: "The Control ofCardiac Rhythm during Heart-Surgery."
Prof. Dr. A. Quevauviller, Dr. O. Blanpin, Paris:" The Influence of Fluids on Local Anaes-thesia."
Artificial Hibernation and Hypothermia.Dr. P. Huguenard, Paris: " The Protection against
Stress by Means of Hypometabolism.Physiology and Methods."
Prof. Dr. E. Ciocatto, Turin: " PhysiopathologicalStudies during Hypothermia in Man."
Prof. R. W. Virtue, Denver: "The ClinicalAspects and the Technique of Hypothermia."
Dr. T. C. Gray, Liverpool: " Metabolic Responsesto Trauma Inflicted during Hypothermia."
Dr. B. G. B. Lucas, London: " Hypothermia."Dr. H. M. Laborit, Paris: "The Notion of a
Functional Thermic Optimum in ArtificialHibernation."
Dr. G. Soares Bairao, Dr. A. P. de Almeida, Dr.A. V. Lorenzo, Dr. C. Sawaya, Dr. R.Tenuto, Sao Paulo: " A few Data about ourExperience in the Hospital das Clinicas ofSao Paulo with Artificial Hibernation andNeuroplegy."
Prof. H. M. Ausherman, Dr. W. K. Nowill, Dr.S. Boyarsky, Dr. H. E. Hall, Dr. M. Bour-geois-Gavardin, Durham, N. Car.: " Physio-logic Variations during Induced Hypother-mia in the Dog."
Dr. M. Battezzati, Dr. C. Taddei, Dr. P. Mosetti,Dr. G. B. Gemma, Geneva: " Hypothermiaand Extracorporeal Circulation with Exclu-sion of Heart and Lungs."
Dr. L. H. Wright, New York: " Hypothermia forCardiac Surgery."
Dr. S. M. H. Holmdahl, Uppsala: "The Toler-ance of the Dog under Hypothermia toRespiratory Acidosis."
Dr. L. E. Gelin, Dr. B. Lofstrom, Lund: "OnPeripheral Circulation in deep Hypothermia."
Dr. H. C. Slocum, Dr. C. W. Hughes, Dr. P.Schafer, Dr. T. G. Barilla, Washington, D.C. :" The Influence of Pentobarbital and Thio-pental on the Tolerance of the HypothermicDog-heart to Ventricular Fibrillation."
Dr. E. Grafin von Liittichau, Mannheim: " In-duced Hypothermia (Laborit) as an aid in theTreatment of Severest Shock."
Dr. O. H. Just, Berlin: " Clinical Experiences inExtreme Induced Hypothermia."
Dr. J. Cahn, Paris: " Physiology of ArtificialHibernation."
Dr. J. du Cailar, Montpellier: " Artificial Hiber-nation by means of the Methoniums."
Dr. V. G. Longo, Rome: " Effects of Chlorpro-mazine on Electroencephalographic andbehavioural reactions due to HypothalmusStimulations in the Rabbit" (with film).
Dr. J. Thuillier, Paris: " Evaluation of theAnalgetics in the Animal by means ofTensiometry " (with film).
Dr. Nicola Cocchia, Dr. Renato Cuoculo, Naples:" Hibernation therapy in Surgery for aorticTransplants."
Dr. J. Bimar, Marseille: "The Combination ofHydergin-Diparcol in Hibernation and po-tentiated Anaesthesia."
Dr. L. Campan, Toulouse: " Hypersensibility toHibernotherapy."
Dr. P. Jaquenoud, Dr. J. Mercier, Dr. L. Hartung,Dr. M. Gavan, Marseilles: " Oxygen Con-sumption and Neuroplegic Drugs."
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
WORLD CONGRESS OF ANAESTHESIOLOGISTS, 1955 509
Dr. C. Horatz, Hamburg: " Hypothermia andArtificial Hibernation." .
Dr. G. Hossli, Zurich: " Artificial Respiration(continuous) and Hypothermia in severeWound Tetanus."
Dr. S. A. Mason, Sanderstead, Surrey: "TheHypotensive Technique and Artificial Hiber-nation for the Fenestration-operation."
HypotensionDr. M. Bozza, Milan: " Resperine as an Aid in
controlled Arterial and Cerebral Hypotensionin Neurosurgery."
Dr. J. P. Payne, London: " Histamine Releaseduring Controlled Hypotension with Arfo-nad."
Dr. W. N. Rollason, Hull: " The Electrocardio-gram in Hypotensive Anaesthesia."
Dr. G. Carstensen: Wiirzburg: " Damage to theKidneys and Anaesthesia."
Dr. B. Haid, Innbruck: " Our experiences withInduced Hypotension during Five Years."
Dr. F. Becker, Wiirzburg: " Induced Hypoten-sion with Arfonad and Kidney-function."
Dr. P. G. Sironi, Milan: " Observations on hypo-tensive Activity of Resperine in Anaesthesiafor the Micro-surgery of the Ear."
Dr. L. Marogna, Sassari: " Fatal Haemorrhageafter potentiated Anaesthesia and InducedHypotension."
Dr. B. Paradis, Quebec: " Physiological andClinical Considerations on Induced Hypo-tension in Anaesthesia."
Dr. M. B. S. Silva Araiijo, Oporto: " Ganglio-plegics."
Dr. F. M. Meisner-Biilow, Stuttgart: " InducedHypotension in Haemorrhage " (with film).
Dr. H. C. Voorhoeve, Rijswijk, The Hague:" Controlled Hypotension in GynaecologicalOperations " (with film)
Dr. J. Gillies, Edinburgh: " Spinal Block andHypotension."
Dr. D. E. Hale, Cleveland: " T h e History andRational of Induced Hypotension."
Dr. E. Kern, Paris: "Analysis of 600 Observa-tions on Induced Hypotension."
Dr. G. E. H. Enderby, London: "Safety inhypotensive Anaesthesia."
Dr. St. Kubicki, Berlin: " Electro-corticographicDerivations in Hypotension."
Dr. K. Wiemers, Dr. E. Kaniak, Freiburg: " TheInfluence of Phenothiazines on the Toleranceto Ischaemia of the Rabbit-heart."
Dr. E. Gadermann, Hamburg: " Induced Hypo-tension in Heart-surgery."
Dr. P. Pellmont, Basle: "The Pharmacology ofthe Ganglionplegks in Connection with Hy-potension."
Free SubjectsDr. M. D. Leigh, Los Angeles: "Paediatric
Anaesthesia."Prof. Dr. R. A. Hingson, Cleveland: " T h e
Reserve Midget Portable AnaesthesiaMachine, Resuscitator and Oxygen Inhalatoras the Vehicle for Non-explosive cyclopro-pane/helium/oxygen Anaesthesia."
Dr. W. Block: Hamburg: " On the Relation ofThiobarbiturates to the Fat Metabolism."
Dr. L. Havers, London: " Controlled Hypoten-sion by Extradural Spinal Block UnderChlorpromazine Cover."
Dr. W. Bakhoum, Dr. S. F. Mankarious, Cairo:" Desoxycortisone in the Treatment of Post-spinal Anaesthesia Headache."
Dr. R. L. Rodriguez-Cantu, Mexico: " FineNeedle Technique in Spinal Anaesthesia."
Dr. H. Ruppert, Berlin: "The Changes in theMotility of the Uterus in Extradural SpinalAnaesthesia."
Dr. G. Hoflehner, Steyr: "Cerebral DamageCaused by Anaesthesia and the ConsequencesThereof."
Dr. J. T. Hayward-Butt, Durban, S.A.: " Kemi-thal Sodium. Review of 50,000 Administra-tions."
Dr. J. Bark, Tubingen: " Bronchoscopy and Bron-chography under Anaesthesia."
Dr. K. L. Schober, Halle: " Experimental Eluci-dation of the Mode of Action of PeriduralAnaesthesia."
Dr. H. Wendl, Hamburg: " Anaesthesia forCaesarean section."
Dr. C. Matteucci, Sassari: " 1,000 EpiduralBlocks."
Dr. V. Keating, Jamaica: " Anaesthetic Problemsin a Tropical Country."
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
510 BRITISH JOURNAL OF ANAESTHESIA
Dr. B. R. Margolius, New York: "The phantartrate on Respiration during Nitrous-oxide-oxygen Anaesthesia."
Dr. M. Swerdlow, Manchester; Dr. F. F. Fokles,Pittsburg; Dr. L. A. Pirk, New Jersey: " TheUse of Nisentil and Levallorphan to Supple-ment Nitrous-oxide-oxygen Anaesthesia."
Dr. P. Drury Byrne, Dublin: " Modified Electro-convulsive Therapy."
Dr. R. D. Levis, London: " The transference ofthiopentone and some Relaxants across thePlacenta."
Dr. R. Bryce-Smith, Oxford: " Bronchoscopy forthe Anaesthetist."
Dr. N. Guardagni, Los Angeles: " Steroid Anaes-thesia in Surgery."
Dr. P. Mundeleer, Brussels: " Anaesthesia inThoracic Surgery."
Muscle Relaxants
Dr. R. J. Hodges, Portsmouth: " SuxamethoniumTolerance and Pseudocholinesterase Levelsin Children."
Dr. J. Bullough, Chislehurst: " Five Years con-tinuous use of Dimethyl-tubocurarine in5,000 Cases."
Dr. J. K. Harper, London: " The Relaxants in EyeSurgery with special reference to Intra-ocularManipulations."
Prof. W. W. Mushin, Cardiff: " Further Experi-mental Studies of Gallamine-triethiodide inMan."
Dr. S. Thesleff, Lund: "The Mode of Neuro-muscular-block caused by Acetylcholine,Decamethonium and Succinylcholine."
Dr. A. Vitale, Naples: "The Effect of Musclerelaxation on potassium-metabolism."
Dr. S. Johanson, Dr. W. Hougs, Hellerup: " TheInteraction of Benzoquinonium with otherCurarizing Substances."
Dr. R. Frey, Heidelberg: " A Short-actingmuscle relaxant belonging to the CurareGroup. PrestonaL"
Dr. H. Briicke, Murzzuschlag: " A very ActiveMuscle Relaxant. Imbretil."
Dr. R. Rizzi, Venice: " Muscle Relaxation andMortality in Surgery."
Dr. T. Gordh, Dr. O. v Dardel, Stockholm:" The Results in a 2-year Period usingSuccinylcholine Iodide in Anaesthesia."
Dr. S. Schotz, Philadelphia: "Technique ofextremely light Analgesia Plus Muscle Re-laxants in Major Cardiac Surgery" (withfilm).
Dr. G. G. Nahas, Paris: " Experimental Defibri-lation " (with film),
Dr. R. Bronnimann, Dr. H. Stimemann, Bern:" Experimental Tetanus by Tetanus-toxin and
the Curares."Dr. N. Cocchio, Dr. Fr. Portolano, Naples:
" Tardily absorbable d-Tubocurarine inAnaesthesia."
Dr. R. Brodowsky, Paris; Dr. T. Lada, Lille:" Mediatorial (anaethocurarium) Muscle Re-laxant and Potentiating other Curares.Clinical use, Evaluation."
Prof. Dr. M. J. Dallemagne, Liege: " Modes ofaction of Carnitine and its derivatives on themotor-end-plates and Ganglionic Synapsis."
Dr. M. Hanquet, Liege: " Reciprocal Antagonis-tic action in Man of the Curaremimetics andAcetylcholinomimetics."
Dr. H. L'Allemand, Giessen: " Haemodynamicsof the lung Circulation in diffusion Respira-tion under Oxygen and under gradualHypoxia."
Dr. H. Gross, Dr. E. Kepes, Dr. D. Young, Dr.D. Enselberg, New York: " Electrocardio-graphic changes during anaesthesia for Mitral-commissurotomy."
Dr. E. Lopes-Soares, Dr. C. M. Medres, Dr. R.LaFeria, Lisbon: " Results of 1,500 generalanaesthetics with pentothal-tubarine-pro-caine."
Dr. H. Keszler, Prague: " Pathogenisis and Treat-ment of Laryngeal Spasm."
Dr. A. G. ElGohary, Cairo: "The Status ofAnaesthesia in the Middle East."
Dr. J. Pastorovd, Prague: " The Present state ofCzechoslovac Anaesthesia."
Dr. M. B. de Oleaga Alarc6n, Buenos Aires:" Potentiated Anaesthesia in EndothoracicSurgery."
Prof. D. Bovet, Rome: " Chemical structure andPharmacodynamic Activities of the Naturaland Synthetic Curares."
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
WORLD CONGRESS OF ANAESTHESIOLOGISTS, 1955 511
Prof. W. D. Paton, London: " T h e Mode ofAction of neuro-muscular blocking agents."
Dr. F. F. Foldes, Pittsburgh: " The fate of MuscleRelaxants."
TeachingDr. H. Reinhold, Dr. J. v. d. Walk, Brussels:
" The Teaching of Anaesthesiology."Prof. Dr. S. M. Campbell, Toronto: "The
Teaching of Anaesthesia in a Canadian Uni-versity."
Dr. N. R. James, Melbourne: "Basic Principlesin the Teaching of Anaesthesia."
Dr. J. G. Fairer, London: "The Use of Visualaids in Teaching the Principles of Anaes-thesia."
Prof. H. Griffith, Montreal: " The Teaching ofAnaesthesiology."
Dr. E. Wain0 Andersen, Dr. W. Dam, Dr. E.Husfekit, Dr. B. Ibsen, Dr. J. Kirchnoff, Dr.H. Ruben, Dr. O. Secher, Copenhagen:" Teaching and Preliminary Results."
BOOK REVIEW
Erlebtes aus der Thoraxchirurgie (1st edition). ByProfessor Dr. Rudolph Nissen, Director ofthe University Surgical Clinic, Basle. Pub-lished by Georg Thieme Verlag, Stuttgart.Pp. 65. Price D.M.14.40.
This delightful booklet is the substance of theMitchell Banks Memorial Lecture on " TheRomance of Thoracic Surgery " delivered by theauthor at the University of Liverpool two yearsago. In the space of some 12 pages, Dr. Nissenrapidly flits through the temples of ThoracicSurgery, lighting a small candle at each of thenumerous shrines en route. The story is afascinating one, and confirms once again howrecent are so many aspects of thoracic surgery,which we take for granted and which havebecome routine today. He pays but modest tributeto the contributions of modern anaesthesia to thisbranch of surgery. Mention might well have beenmade of some of the pioneers of Thoracic Anaes-thesia within our own memory and time, and
without whom the giants of surgery he describesmight well have remained pigmies. Nissen wasa former pupil of Sauerbruch and it says muchin his objectivity ,when he speaks of his formerchief as follows: " SaueTbruch rejected onprinciple the idea of setting up anaesthesia as abranch in its own right. . . . His voice wassufficiently influential in the Continent to holdup a development there from which in othercountries, thoracic surgery was to benefit morethan any other."
The second half of the booklet consists ofexcellently reproduced portraits, and of nowhistorical and classical articles covering thedevelopment of thoracic surgery. British-surgeonsare well to the fore and portraits and reproduc-tions of papers are shown of Morriston Davies,Henry Souttar and Russell Brock. For thosewhose German is imperfect a nearly completetranslation of the lecture was published in theAmerican Journal of Surgery, 1955, 89, 9.
W. W. Mushin
by guest on July 29, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
Related Documents











