Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=wjad20 Download by: [University of Liverpool] Date: 01 June 2016, At: 05:56 Journal of Addictive Diseases ISSN: 1055-0887 (Print) 1545-0848 (Online) Journal homepage: http://www.tandfonline.com/loi/wjad20 Assessing the effectiveness and cost-effectiveness of drug intervention programmes: UK case study Brendan J. Collins, Kevin Cuddy & Antony P. Martin To cite this article: Brendan J. Collins, Kevin Cuddy & Antony P. Martin (2016): Assessing the effectiveness and cost-effectiveness of drug intervention programmes: UK case study, Journal of Addictive Diseases, DOI: 10.1080/10550887.2016.1182299 To link to this article: http://dx.doi.org/10.1080/10550887.2016.1182299 Accepted author version posted online: 02 May 2016. Published online: 02 May 2016. Submit your article to this journal Article views: 19 View related articles View Crossmark data

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=wjad20
Download by: [University of Liverpool] Date: 01 June 2016, At: 05:56
Journal of Addictive Diseases
ISSN: 1055-0887 (Print) 1545-0848 (Online) Journal homepage: http://www.tandfonline.com/loi/wjad20
Assessing the effectiveness and cost-effectivenessof drug intervention programmes: UK case study
Brendan J. Collins, Kevin Cuddy & Antony P. Martin
To cite this article: Brendan J. Collins, Kevin Cuddy & Antony P. Martin (2016): Assessing theeffectiveness and cost-effectiveness of drug intervention programmes: UK case study, Journalof Addictive Diseases, DOI: 10.1080/10550887.2016.1182299
To link to this article: http://dx.doi.org/10.1080/10550887.2016.1182299
Accepted author version posted online: 02May 2016.Published online: 02 May 2016.
Submit your article to this journal
Article views: 19
View related articles
View Crossmark data

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 1
Assessing the effectiveness and cost-effectiveness of drug intervention programmes: UK
case study
Brendan J. Collins1, Kevin Cuddy
2, Antony P. Martin
3,*
1Department of Public Health and Policy, University of Liverpool, Liverpool, United Kingdom.
2Centre for Public Health, Liverpool John Moores University, Liverpool, United Kingdom.
3NIHR CLAHRC NWC, University of Liverpool, Liverpool, United Kingdom
*Correspondence to Antony P. Martin. Email: [email protected]
Abstract
Aims: The effectiveness and cost-effectiveness of the UK Drug Interventions Programme (DIP)
which directs adult drug-misusing offenders out of crime and into treatment programmes was
established. Methods: Quality-adjusted life year (QALY) estimates from the UK Drug Treatment
Outcomes Research Study were collected and a cost utility assessment of the DIP was
conducted. Results: Cost-utility assessment confirmed that the DIP is both effective and cost-
effective with an average net cost saving of £668 (£6,207 including one case of homicide).
Conclusions: This study provides evidence that DIPs are cost-effective as they reduce crime,
improve quality of life and reduce subsequent drug use.
Keywords
Drug treatment, crime, cocaine, opiates, quality of life, test on arrest
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 2
Introduction
Drug-related crime is a global challenge. Many problematic drug users in the community find
themselves becoming involved in crime and coming into contact with criminal justice services.
Moreover, large proportions of prison populations experience problematic drug use and this is
often considered a poor environment to recover. Recently, the UK and other developed countries
have seen an increase in policies aimed at linking drug treatment services with the criminal
justice system.1
Studies have found conflicting evidence as to whether legal pressure is an effective method of
achieving drug treatment success. Some studies from North America have concluded that legal
pressure has a strong and positive impact on treatment entry and also retention, which has led to
positive outcomes.2-4
The US Drug Abuse Treatment Outcome Study highlighted reduced crime
costs following drug treatment in both outpatient and residential settings. Other studies found a
negative impact of legal referral compared with elective referral.5-6
Nevertheless there still
remains a paucity of evidence in favour and against. However, some studies conclude the
possible negative results of a policy of criminal justice referrals into treatment based on
presumptions of need and non-empirical evidence basis.7-8
It has been widely reported that use of certain addictive drugs like heroin and crack cocaine place
a high financial burden on society.9 Given evidence shortage and increasingly constrained
government budgets, it is therefore paramount to continue to evaluate and ensure efficient
allocation of resources. An international literature review compared and contrasted a host of
European schemes and found a lack of consensus remains as to the most effective and cost-
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 3
effective drug intervention programmes. Interventions have been found to vary considerably
between countries such as Austria, Germany and the Netherlands, in terms of choice of
treatment, punishment and imposed treatment-based sentences.10
The Drug Interventions Programme (DIP) was initiated in 2003/04 as part of the UK
Government‟s strategy for combating problematic drug use. Previously, The Crime and Disorder
Act 1998 introduced the Drug Treatment and Testing Orders, a community penalty where drug
users who showed willingness to comply with the conditions of the treatment were compelled
into drug treatment. The DIP has an operational handbook11
which sets out a framework of how
the DIP is implemented. In the DIP, people who have been arrested for „trigger‟ offences such as
drug possession or dealing, or crimes that are often related to drug addiction such as fraud or
acquisitive crime, are saliva tested in the custody suite in the police station for the presence of
cocaine and/or opiate metabolites. If the test is positive, the person is then referred into drug
treatment services. The ambition is that testing on arrest enables early identification of people
who are committing crimes associated with their drug use so that they can be channelled into
drug treatment, and to ensure that drug users who are not charged with an offence are offered a
treatment and support programme. An individual is tested on arrest where they fulfil the
following conditions: are aged 18 or over; are in police custody; and were arrested for a trigger
offence or for an offence where a police officer of Inspector rank or above suspects that opiate or
cocaine use was a causal or contributory factor. Since drug and alcohol commissioning moved
from the NHS to local authorities in April 2013 the DIP has become optional and therefore this
study is pivotal for commissioners who need to decide whether they should continue the DIP.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 4
Moreover, the study provides evidence for the introduction of such drug intervention
programmes across the globe.
The present study followed individuals who were in contact with the DIP across a six month time
period from April to September 2013. The data used in the analysis was drawn from Wirral, a
borough in Merseyside located in the North West of England with a population of approximately
320,000 people. Wirral experienced a significant rise in heroin use from 1982, believed to be
fuelled by high youth unemployment and misinformation with regard to the addictive nature of
the drug.12
Wirral pioneered the “Mersey Model of Harm Reduction” which consisted of opiate
substitution as well as needle and syringe exchange and psychosocial support.13
In 2012 Wirral
was estimated to have the 10th
highest rate of opiate and crack cocaine use out of 151 local
authorities in England.14
During this study Wirral had an older treatment population of around
2,200 mainly opiate, or polydrug opiate and crack users who mainly have an extended history of
drug use of 20 years or more. Crime rates in Wirral peaked in the mid-1980s and fell each year
from 2001 to 2011.15
The analysis was conducted to determine the cost-effectiveness of DIP based on an assessment
of criminal activity and quality of life. This topic is of significant economic importance as the
DIP represents a significant proportion of expenditure for local authorities in England. For the
purposes of the analysis, the hypothesis was that costs of crime will be lower in the 12 months
post DIP assessment than in the 12 months pre assessment. A cost-utility analysis was also
undertaken as it is considered the „gold standard‟ form of evaluation according to NICE (the
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 5
National Institute for Health and Care Excellence, who recommend health and social care
interventions in England and Wales) for assessing the value of public health interventions.16
Methods
The analysis incorporates a broad societal perspective, accounting for the wider impact of crime
on health and quality of life. The transitory pleasure that individuals may experience from using
drugs is characterised as temporary and the analysis considers that average quality of life
improves as individuals confront and attenuate their drug use.
The costs for the DIP were based on an average cost of the whole programme so include the cost
of testing people who did not test positive for drugs. The cost of drug treatment is based on a six
month average for people referred to drug treatment in Wirral. These costs were derived from
service line reporting (SLR) for the services which were both provided by ARCH (Advice,
Rehabilitation, Counselling and Health). ARCH are a not for profit drug treatment provider.
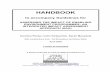
Figure 1 shows relevant costs and outcomes which were included in the analysis. The cost of
£924 for the DIP was based on a total cost of £491,721 for 2012/13 financial year divided by an
estimated 532 people tested (the six month sample of 266 people multiplied by 2). These costs
were made up of having drug testing staff who visited the custody suites including dealing with
repeat offenders and stimulant users (£198k), drug testing materials and laboratory use (£77k),
and GP and prescribing costs (£72k), admin costs (£22k), and costs of engaging with the police
as well as other overheads and management costs (£82k).
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 6
The most recent UK data on the unit cost of crimes were adopted from the Integrated Offender
Management toolkit (IOM) which was produced in 2011.17
These costs of crime estimates were
initially produced in 2000 by the Home Office and were updated for crimes against individuals
in 2005.18-19
These figures include costs incurred in anticipation of crime (such as security
expenditure), as a consequence of crime (such as property stolen and emotional or physical
impacts), and in response to crime (costs to the criminal justice system). These Home Office
reports give a detailed breakdown of what proportion of costs are insurance, physical and
emotional impact, health services, property stolen, criminal justice, etc. These costs were inflated
to the time period that individuals were followed up (2012) by increasing them by a factor of
2.38% based on the GDP deflator table from the HM Treasury. The arrests analysed occurred
between April 2011 to September 2013 and a consistent unit cost was selected for each crime to
ensure that the comparison of before and after DIP assessment costs were not skewed by
inflation. There remains a paucity of data as the IOM toolkit and previous unit costs fail to
include a cost for drug offences, which amounts to a significant proportion of the arrests for
which individuals were included in the DIP (11.7% of arrests in the Wirral data). Arrests which
could not be matched to other categories assumed an average cost of £685 based on an academic
case study of Sussex Police.20
Crime costs were matched with arrests for individuals 12 months before and 12 months after
their contact with the DIP. Clearly some individuals are not prosecuted or found guilty of crime
committed, however it was assumed that some of the costs associated with the arrest still
occurred. However it has been estimated that only 29% of crimes are detected (but those detected
are likely to be the more serious crimes), so any cost of crime estimate should theoretically be
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 7
inflated to take into account those crimes that are not detected.21
Based on this figure, it can be
assumed that for each crime that is detected, individuals commit an average of 2-3 crimes which
are not. Nationally, approximately 83% of individuals prosecuted for crimes were found guilty in
2013; however, this varies by type of crime group.22
The highest unit cost per crime is for homicide at £1.8million which was considered an outlier
and therefore caution was taken in the analysis as even a small number of homicides would skew
the average costs. The analysis of average costs was carried out including and excluding
homicides to observe how it would impact upon the results. Appendix 1 shows the arrest reason
and associated costs.
In the analysis, average QALYs gained from the Drug Treatment Outcome Study (DTORS) were
used.23-24
The DTORS cost effectiveness study was essentially a before and after study, where
baseline utility scores were extrapolated. This study measured outcomes for drug users across
England, however it should be noted that it experienced a high drop-out rate. Of the individuals
recruited to the study, 35% had criminal justice involvement, and 62% had used heroin and 44%
crack cocaine in the 4 weeks prior to the interview. The quality of life information in the DTORS
was calculated using the Short Form 12 (SF-12) survey instrument.
Both the costs of crime and estimated QALY differences were measured over a 12 month time
horizon so no discounting rate was applied for costs or outcomes. A subgroup analysis of
differences between crime rates before and after the DIP was conducted according to gender;
those testing positive for cocaine only, opiates only and both cocaine and opiates; and by test
outcome groups. These test outcomes were „no further contact‟ which meant that the staff had no
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 8
further contact with the individual, often because they refused any assessment; where an
assessment was made of the individuals‟ needs in terms of drug treatment and they were
sometimes given a brief intervention; and where a care plan was made with the individual for
their ongoing needs surrounding drug treatment.
In addition, measures of quality of life, psychological and physical health from the Treatment
Outcomes Profiles (TOPs) were analysed. This was for cross-sectional data from ARCH for two
financial years, 2011/12 and 2012/13. There was no recognised approach to mapping scores on
the TOPs to utility scores, otherwise this would have been included in the economic evaluation.
A statistical model was constructed using MS Excel Visual Basic for Applications. This model
was a client level Monte Carlo simulation model which was bootstrapped for 10,000 hypothetical
clients where each time a random scenario was drawn from the data distributions. A Monte Carlo
simulation was performed to investigate and quantify the uncertainty associated with the results
of our analysis. This information provides the decision-maker with a range of possible outcomes
and the probabilities that they would occur for any choice of action. A Monte Carlo simulation
demonstrates the extreme outcome possibilities and frequency of those outcomes. An overall
point estimate was then calculated from the 10,000 random walks through the model and the
results were modelled over the 12 month time horizon. Table 1 shows a list of parameters for the
model. In short, all parameters were randomly sampled from assigned probability distributions.
However, in the absence of data distributions for individual costs for the DIP and for drug
treatment, an estimate of around 20% variance was used to characterise uncertainty for those
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 9
parameters in the model. Because there was one homicide case which has a very high cost, this
was excluded from the analysis but included as an additional separate scenario.
Findings
Differences in Offending
The main types of offences committed by the 266 people in contact with the DIP were
acquisitive and drugs offences. Overall there was a significant reduction in offending of 52% in
the 12 months post-test period compared with the 12 months pre-test period (F [1,263] = 58.035,
p < 0.001). Moreover, there was a reduction in economic costs across individuals who had tested
positive for cocaine, opiates and both (see Table 2). Those individuals who were care planned by
the DIP team following their arrest showed the most substantial reduction in offences pre-test
and post-test. However, there were no statistically significant differences between the three
groups in terms of change in the number of offences pre-test to post-test (F [2,263] = 1.931, ns).
This absence of statistical significance in part may be explained by the smaller sample size due
to the subgroup analysis (see Table 3).
Differences in Health & Quality of Life Outcomes
Treatment Outcomes Profiles (TOPs) are self-reported profiles of drug use, crime and other
outcomes. In the dataset it was not possible to conclusively filter for clients identified through
the DIP, therefore criminal justice referrals were used as a proxy. This included arrest referral,
DIP, DRR [drug rehabilitation requirement], criminal justice other, CARAT [counselling
assessment referral advice and throughcare], prison and probation. In practice, the majority of
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 10
these clients would have passed through the DIP. In a cross section of 1,806 criminal justice
clients in Wirral, the average TOPs psychological health status was 24.7% higher at treatment
exit than treatment start, physical health was 12.4% higher, and quality of life was 31.1% higher
(see Figure 2). These differences were all statistically significant (p<0.001).
Difference in Crime Costs
The crime costing analysis included 264 out of 266 clients; 2 clients could not be matched with
the data and were therefore excluded. The average crime costs were found to be 43% lower in
the 12 months post DIP, or 77% lower when the one case of homicide was included (Table 2).
The data for costs of crime did not follow a normal distribution so a non-parametric Wilcoxon
signed ranks test was used. The difference in costs between 12 months pre and 12 months post
DIP was statistically significant (p<0.0001) with 209 out of 264 clients having lower crime costs,
42 had higher crime costs, and 13 had the same crime costs. This difference was significant with
and without the one homicide case (p<0.0001).
Economic Model Results
Overall, the DIP was found to be cost effective with an average net cost saving of £668 (or
£6,207 including one case of homicide). Using the QALY estimates from the DTORS, the
service was found to be dominant against a do-nothing alternative, meaning it had a lower net
cost and higher average QALYs gained (Table 4).
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 11
Discussion
There is a considerable shortage of evidence with regard to the efficacy and cost-effectiveness of
Drug Intervention Programmes throughout the world. Existing evidence has been found to be
conflicting and the interpretation of the transferability of programmes requires caution.
Intervention effectiveness has been found to be partially dependent upon permutations of formal
and informal legal pressure, alongside types of interventions. Moreover, the methods and nature
of diversion from the criminal justice system to treatment varies considerably. Arrest referral
schemes such as the DIP in England and Wales provides a voluntary treatment referral system
from within the criminal justice setting to largely community-based prescribing services.
Whereas, the USA drug court referrals deal mainly with individuals charged with drug-related
offences and more commonly refer the individual to an abstinence-based residential programme.9
Constrained governmental budgets exist in Europe, North America and worldwide. Increasingly,
a stronger evidence-base of cost-effectiveness is now required for the adoption or continuation of
national spending on drug intervention programmes and other national programmes. This
economic evaluation has demonstrated that the Drug Interventions Programme is likely to be
cost effective in reducing future crime. This will be achieved by engaging individuals in drug
treatment programmes and other services such as housing and money advice as many drug users
often face several socioeconomic challenges.25
Crime can be reduced by challenging drug user
behaviour and creating opportunities and motivating individuals to move to an alternative
lifestyle where drug use and crime do not feature.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 12
The overall volume of offending by Wirral residents in the sample reduced by 52% post DIP
positive drug test. National research from 2007 suggested a 26% reduction in crime post-DIP and
if national figures are still similar, this implies that the DIP in Wirral is associated with a greater
reduction in crime than nationally.11
Taking into account net costs and social value of benefits
(using a willingness to pay threshold of £20,000 per QALY) the cost-benefit ratio would be
£2.26 for every £1 spent, or £6.33 where homicide was included. As a comparison, in the
DTORS study (which had a one year time horizon and did not include the DIP), average net
benefit ratio was £2.50 for every £1 spent. In addition, the earlier NTORS study adopted a longer
4 year time horizon and the cost-benefit ratio was estimated at £9.50 in benefits for every £1
spent.26
It should be noted that there is limited evidence for what can be considered a clinically
important difference in QALYs for drug treatment. A cancer study concluded that 0.11 QALYs
is a clinically important difference, which is greater than the average difference from the DTORS
used in this analysis.27
It should be noted that Wirral is an area with a history of drug problems and still there remains a
significant population of drug users. This factor, combined with its long history of drug treatment
services may mean that services in Wirral are expected to be more cost effective and efficient
than similar services in other areas of the UK as service provision has existed for a long time and
at scale. Overall, this analysis is useful in informing national and international decision-making
surrounding drug test on arrest schemes. However, as the richness of this crime data is not
available for other drug and alcohol treatment services, the present study has limited comparison
with other services in terms of cost effectiveness through preventing crime.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 13
The present study included people tested for opiates, cocaine or both. Opiates would include
prescription drugs such as tramadol and codeine as well as street heroin and methadone. In
addition, the testing process did not differentiate between powder cocaine and crack cocaine. It
may be that some powder cocaine users are more likely to be recreational or weekend drug users
whereas crack cocaine users are more likely to be addicts and to commit acquisitive crime to
fund their addiction as inhalation of crack cocaine produces greater dopamine system down-
regulation leading to greater addiction.28
In individuals who tested positive for cocaine, 46% had
only one arrest in the 12 months pre-test and of these, 79% of these had no arrests in the 12
months post-test which may indicate that many individuals arrested for drugs possession may not
have been arrested again regardless of DIP contact.
The QALY estimates used were from the DTORS study, which may not accurately reflect the
reality of the quality of life benefits for clients who have been through the DIP. The change in
TOPS data over time suggests that individuals who are identified through the DIP show a
significant improvement in quality of life. The TOPs quality of life scores showed a 31%
improvement between treatment start and treatment exit, which if translated into QALYs could
enhance the cost-effectiveness of the DIP. However, unlike other quality of life questionnaires
such as the EQ-5D, SF-12 and Health Utility Index, there is currently no standard method for
converting the TOPs scores into QALYs.28
Since the health and quality of life questions on the
TOPs follow other questions which relate to drug use and crime, there may have been a social
desirability effect of clients wanting to please their key workers by giving them positive answers
to the questions on the TOPs. Additionally, it should be noted that this analysis adopted a one
year time horizon and so the actual benefits may be greater when assessed over a longer
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 14
duration. However, as the DIP is essentially a way of channelling people away from crime into
drug treatment, the benefits cannot be attributed to the DIP alone, as it is part of a complex
integrated system of criminal justice, and drug and alcohol treatment.
Due to the nature of the data analysed in this study and issues regarding regression to the mean,
uncertainty analysis was conducted. Clients who had no further DIP contact still showed a
reduction in crime. In addition, there may also be a small proportion of clients who were in
custody in the 12 months after assessment and were therefore less likely to commit crimes.
However, there is also the probability that once individuals are known to the police they are
more likely to be rearrested for crimes in the future which would result in an increase in arrest
rates. The DTORS cost effectiveness study was also a before and after study, which may
underestimate the QALY gains from drug treatment, as without drug treatment, individual
quality of life may have declined rather than been stable. It may not be considered ethical or
practical to run randomised controlled trials in drug treatment, but there may be scope for more
robust research designs such as cluster randomised controlled trials or natural trials in future.
Moreover, it would also be useful to conduct comparative evaluations in other regions with
different population profiles in order to better assess the wider cost effectiveness of DIPs in the
UK. In addition, it would be interesting to compare the change in crime and drug treatment rates
between areas that retain the DIP and areas that decommission it; however it may be that areas
that decommission the DIP will already have fewer problems associated with drugs and crime.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 15
Summary
This is a pivotal study as it is the first time a cost utility analysis has been carried out on the Drug
Interventions Programme. This analysis used data from Wirral, a local authority area in England
and the results have wider implications for the rest of the UK and internationally. The evaluation
adopted a societal perspective of the Drug Interventions Programme, where individuals who
were arrested for trigger offences were tested for drugs and referred into drug treatment. The
results of the analysis provide further evidence of the cost-effectiveness of the programme. The
analysis concludes that the drug intervention programme successfully reduces economic costs of
crime and also increases quality of life of individuals included in the DIP.
Acknowledgements
In conducting this research, AM was supported by the National Institute of Health Research
Collaboration for Leadership in Applied Health Research and Care North West Coast (NIHR
CLAHRC NWC). The views expressed are those of the authors and not necessarily those of the
NHS, the NIHR or the Department of Health.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 16
References
1. Osborne A. Future delivery of the Drug Interventions Programme: Do the benefits justify the
costs? Journal of Forensic and Legal Medicine 2013; 816-820.
2. Berkowitz G, Brindis C, Clayson Z, Peterson S. Options for recovery: promoting success
among women mandated to treatment. J Psychoactive Drugs 1996;28:31–8.
3. Collins JJ, Allison M. Legal coercion and retention in drug-abuse treatment. Hosp
Community Psychiatry 1983;34:1145–9.
4. Pompi KF, Resnick J. Retention of court-referred adolescents and young-adults in the
therapeutic-community. Am J Drug Alcohol Abuse 1987;13:309–25.
5. Harford RJ. Effects of legal pressure on prognosis for treatment of drug-dependence. Am J
Psychiatry 1976;133:1399–404.
6. Howard DL, McCaughrin WC. The treatment effectiveness of outpatient substance misuse
treatment organizations between court-mandated and voluntary clients. Subst Use Misuse
1996;31:895–926.
7. Wild TC. Social control and coercion in addiction treatment: towards evidence-based policy
and practice. Addiction 2006;101:40–9.
8. Wild TC, Newton-Taylor B, Ogborne AC, Mann R, Erickson P, MacDonald S. Attitudes
toward compulsory substance abuse treatment: a comparison of the public, counselors,
probationers and judges‟ views. Drugs: Educ Prev Pol 2001;8:33–45.
9. Hayhurst KP, Leitner M, Davies L, Flentje R, Millar T, Jones A, King C, Donmall M, Farrell
M, Fazel S, Harris R, Hickman M, Lennox C, Mayet S, Senior J, Shaw J. The effectiveness
and cost-effectiveness of diversion and aftercare programmes for offenders using class A
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 17
drugs: a systematic review and economic evaluation. Health Technology Assessment 2015;
No. 19.6.
10. Stevens A, Berto D, Heckmann W, Kerschl V, Oeuvray K, Van Ooyen M, et al. Quasi-
compulsory treatment of drug dependent offenders: an international literature review. Subst
Use Misuse 2005;40:269–83.
11. Home Office (2011) Drug Interventions Programme Operational Handbook.
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/118069/DIP-
Operational-Handbook.pdf (accessed 12th January 2016).
12. Parker HJ, Bakx K, Newcombe R. Living With Heroin: The Impact of a Drug Epidemic on
an English Community. 1988. Milton Keynes: Open University Press.
13. Ashton JR, Seymour H. Public Health and the origins of the Mersey Model of Harm
Reduction. Intern J Drug Policy 2010; 21:94–96.
14. Hay G, Gannon M, MacDougall J, Eastwood C, Williams K, Millar T. Opiate and crack
cocaine use: A new understanding of prevalence. Drugs: Education, Prevention and Policy
2010; 17(2):135-147.
15. Office of National Statistics (ONS). Crime statistics: CSEW open data table - Personal Crime
Prevalence, 2012. http://www.ons.gov.uk/ons/publications/re-reference-
tables.html?edition=tcm%3A77-265883 (accessed August 20, 2015).
16. NICE. Methods for the development of NICE public health guidance (third edition), 2012.
http://publications.nice.org.uk/PMG4, (accessed August 20, 2015).
17. Home Office. Revisions made to the multipliers and unit costs of crime used in the Integrated
Offender Management Value for Money Toolkit, 2011.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 18
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/97813/IOM-
phase2-costs-multipliers.pdf (accessed August 20, 2015).
18. Brand S, Price R. The economic and social costs of crime. Home Office Research Study 217.
London: Home Office, 2000.
http://webarchive.nationalarchives.gov.uk/20110218135832/rds.homeoffice.gov.uk/rds/pdfs/
hors217.pdf (accessed August 20, 2015).
19. Dubourg R, Hamed J. Estimates of the economic and social costs of crime in England and
Wales: Costs of crime against individuals and households, 2003/04. Home Office Online
Report, 2005. London: Home Office.
http://webarchive.nationalarchives.gov.uk/20100413151441/http://www.homeoffice.gov.uk/r
ds/pdfs05/rdsolr3005.pdf (accessed August 20, 2015).
20. Sheffield Hallam University. A Break-even Analysis of the delivery of Integrated Offender
Management in Sussex, 2012.
http://www.sussexcriminaljusticeboard.org.uk/media/476235/iom_sussex_evaluation.pdf
(accessed August 20, 2015).
21. Ministry of Justice. Criminal Justice Statistics Quarterly, March 2013.
https://www.gov.uk/government/statistics/criminal-justice-statistics-quarterly-march-2013
(accessed August 20, 2015).
22. Smith K, Taylor P, Elkin M. Crimes detected in England and Wales 2012/13 (Second
edition) Home Office HOSB, 2013.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 19
23.
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/224037/ho
sb0213.pdf (accessed August 20, 2015).
24. Davies L, Jones A, Vamvakas G, Dubourg R, Donmall M. The Drug Treatment Outcomes
Research study (DTORS): Cost-effectiveness analysis. Home Office Research Report 25,
2009.
25. Brouwer WB, Culyer AJ, Van Exel N, Rutten FF. Welfarism vs. extra-welfarism. J of health
economics 2008; 27(2):325-338.
26. Boys A, Marsden J, Griffiths P, Strang J. Drug use functions predict cocaine‐related
problems in young people. Drug Alcohol Review 2000; 19(2):181-190.
27. Godfrey C, Stewart D, Gossop M. Economic analysis of costs and consequences of the
treatment of drug misuse: 2-year outcome data from the National Treatment Outcome
Research Study (NTORS). Addiction 2004; 99(6):697–707.
28. Walters SJ, Brazier JE. Comparison of the minimally important differences for two health
state utility measures: EQ-5D and SF-6D. Quality of life research 2005; 14(40):1523-1532.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 20
Appendix 1. Arrest reason and matched crime type and unit cost.
Arrest Reason Crime type Unit Cost 2012 Other Theft Theft -- not vehicle £781 [Blank] [Mainly „warrant‟] <other arrests> £685 Drugs Possess Class A <other arrests> £685 Other Non-Crime <other arrests> £685 Drunk and Disorderly <other arrests> £685 Drugs Possess Class B <other arrests> £685 Burglary Dwelling Burglary in a dwelling £4,018 Breach of the Peace <other arrests> £685 Drugs Possess W/I Supply Class A <other arrests> £685 Burglary Other Burglary not in a dwelling £4,718 S.47 Assault Other wounding £10,024 Criminal Damage Criminal damage
(personal)
£1,078 Other Violence Against Person Common assault £1,792 Theft Of Vehicle Theft of vehicle £5,088 Other Crime <other arrests> £685 S.39 Assault Common assault £1,792 Robbery Robbery -- personal £9,020 Theft From Vehicle Theft from vehicle £1,059 Disorder - Other <other arrests> £685 Traffic OPL <other arrests> £685 S.18 Wounding Serious wounding £26,360 Fraud and Forgery <other arrests> £685 Drugs Supply Class A <other arrests> £685 Disorder - Serious <other arrests> £685 Drugs Produce Class B <other arrests> £685 Going Equipped for Stealing <other arrests> £685 Drugs Possess W/I Supply Class B <other arrests> £685 Handling Stolen Goods <other arrests> £685 Aggravated Vehicle Taking Theft of vehicle £5,088 S.20 Wounding Other wounding £10,023 Traffic General <other arrests> £685 Aggravated Burglary Dwelling Burglary in a dwelling £4,018 Sexual Offence Sexual offences £37,831 Burglary in a dwelling Burglary in a dwelling £4,018 Drugs Other <other arrests> £685 Violence against the person Common assault £1,792 Drugs Supply Class B <other arrests> £685 Homicide Homicide £1,816,918 All others <other arrests> £685
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 21
Table 1. Parameters for Wirral DIP Cost Utility Model.
Parameter Distribution Mean Standard
deviation
Cost of crime -- 12
months before DIP
contact
Skewed - bootstrapped
from data
£2,728 £7,261
Cost of crime - 12
months after DIP
contact
Skewed - bootstrapped
from data
£4,762 £7,328
Cost of DIP Normal -- estimate based
on local data
£924 £200
Cost of drug
treatment
Normal - estimated based
on local data
£429 £100
QALYs gained Normal -- from DTORS 0.05 0.201
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 22
Table 2. Differences in crime volume and costs for Wirral DIP clients, 12 months before
and 12 months after DIP contact, by drug tested positive for (excludes homicide).
Drug tested
positive for
Number
of clients
12 months pre test 12 months post test Difference 12 months
post - 12 months pre test
Mean N
offences
Mean cost
of offences
Mean N
offences
Mean
cost of
offences
Difference
in mean N
offences
Difference
in mean
cost of
offences
Both
(Cocaine &
Opiates)
54 3.69 £5,560 2.76 £4,246 -0.93 -£1,314
Cocaine 166 2.63 £4,808 1.02 £2,570 -1.61 -£2,238
Opiates 46 2.8 £3,348 1.09 £1,334 -1.71 -£2,014
Total 266 2.88 £4,708 1.38 £2,697 -1.5 -£2,011
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 23
Table 3. Wirral Residents Testing Positive in the DIP -- Number of Trigger Offences.
Groups Compared Mean Number of Offences Difference
(pre -- post)
Significance
12 months
pre test
12 months
post test
Overall (n = 266) 2.8759 1.3835 1.4924 p < 0.001
Assessed (n = 68) 2.2647 1.3088 0.9559 Not
statistically
significant Care Planned (n = 141) 2.6809 0.9858 1.6951
No further DIP Contact
(n = 57)
4.0877 2.4561 1.6316
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 24
Table 4. Wirral Drugs Intervention Programme - Economic modelling results.
Outcome Average 2.5% lower limit 97.5% higher limit Average
(including
homicide)
Cost of crime - before £4,824 £685 £22,584 £10,226
Cost of crime - after £2,802 £0 £22,621 £2,666
Cost of DIP £923 £532 £1,318 £922
Cost of drug treatment £431 £239 £627 £430
QALYs gained 0.052 0.449 -0.348 0.052
Net costs (cost of treatment less cost savings) -£668 -£20,875 £21,225 -£6,207
ICER (compared to do-nothing alternative) Dominates Dominates Dominated Dominates
Dominates = less costly and more effective; Dominated = more costly and less effective
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 25
1
2
Inputs (Costs)
Cost of the DIP
Cost of drug
treatment
Outputs (benefits)
Reduction in cost of crime
Financial cost to
individual victims
(insurance, time, lost
output etc)
Monetary value of
human cost (QALY loss)
to victims
Preventative, police & CJS
costs
Benefits to
offenders
Monetary value of QALYs
gained from drug
treatment
Figure 1. Costs and outcomes included in the present study.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 26
Figure 2. Average Treatment Outcome Profile psychological health, physical health and
quality of life scores at treatment start, review and treatment exit, 2011/12 to 2012/13
(financial years). Scores out of 20. Shown with 95% confidence intervals. N = 1806.
Dow
nloa
ded
by [
Uni
vers
ity o
f L
iver
pool
] at
05:
56 0
1 Ju
ne 2
016
Related Documents