Pediatr Surg lnt (1987) 2:216-222 Pediatric Surgery International © Springer-Vertag 1987 Oesophageal atresia without fistula- anastomosis or replacement? N. A. Myers, s. w. Beasley, A. W. Auldist, M. Kent, V. Wright*, and P. Chetcuti Department of Surgery, Royal Children's Hospital, Flemington Road, Parkville, Victoria 3052, Australia Abstract. At the Royal Children's Hospital, Mel- bourne, 553 babies with oesophageal atresia and/ or tracheo-oesophageal fistula have been admit- ted during the past 39 years; 36 (6.5%) of these had oesophageal atresia without a tracheo-oeso- phageal fistula. Definitive surgery was performed in 27 patients: the primary definitive procedure was oesophageal anastomosis in 15 and oesopha- geal replacement in 12. Aspects of diagnosis and selection of the most appropriate treatment mo- dality are discussed, with the results of treatment presented. Our current policy is to perform an oesophageal anastomosis whenever possible, and this has been successful in 7 of the last t 1 patients. Key words: Oesophageat atresia - Gasless abdo- men - Oesophageal replacement - Long gap Introduction Oesophageal atresia without an accompanying tracheo-oesophageal fistula is a relatively rare anomaly and varies between 5% and 10% in most reported series of patient~ with oesophageal atre- sia and tracheo-oesophageal fistula [1, 2, 5, 6, 10, ll, 14, 15, 17, 19, 20, 24, 26, 33, 35, 38]. Many centres therefore have a limited experience of the anomaly; at the Royal Children's Hospital in Melbourne there have been 36 patients who have had atresia without fistula. Thus, we have aver- aged tess than one patient a year during a period which has seen many advances in neonatal care. *Present address: Queen Elizabeth Hospital for Children, Hackney Road, London E2 8PS, UK. Offprint requests to: N.A. Myers Despite these advances and increasing experience controversy still exists as to the most appropriate management of the condition [3, 4, 7, 9, 12, 13, 25, 27, 28, 32]. This paper reports our experience and suggests a protocol which may assist in deter- mining whether primary anastomosis or replace- ment is appropriate. Materials and methods During the period 1948 - 1986, a total of 553 babies with oeso- phageal atresia and/or tracheo-oesophageal fistula were ad- mitted to the Royal Children's Hospital, Melbourne. Oe- sophageal atresia without fistula was seen in 36 (6.5%) of these (Table I). Much of the data was collected prospectively by one of the authors (NAM) and supplemented by careful review of each patient's hospital records. Table 1. 553 patients with oesophageal atresia and/or tracheo- oesophageal fistula (1948- 1986) Oesophageal atresia with distal tracheo-oesophageal fistula Oesophageal atresia with proximal tracheo-oesophageal fistula Oesophageal atresia with proximal and distal tracheo-oesophageal fistula Oesophageal atresia without fistula Tracheo-oesophageal fistula ("H') Total 475 11 1 36 30 553 Results Polyhydramnios was present in 34 patients. Birth weight ranged from 1.6 to 3.6 kg (mean = 2.3 kg). One or more associated congenital anomalies were re¢ognised in 21 patients (Table 2). Of 3 t pa- tients in whom the gestation was recorded, t7 (55%) were tess than 37 weeks-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pediatr Surg lnt (1987) 2:216-222 Pediatric Surgery
International © Springer-Vertag 1987
Oesophageal atresia without fistula- anastomosis or replacement?
N. A. Myers, s . w . Beasley, A. W. Auldist, M. Kent, V. Wright*, and P. Chetcuti
Department of Surgery, Royal Children's Hospital, Flemington Road, Parkville, Victoria 3052, Australia
Abstract. At the Royal Children's Hospital, Mel- bourne, 553 babies with oesophageal atresia and / or tracheo-oesophageal fistula have been admit- ted during the past 39 years; 36 (6.5%) of these had oesophageal atresia without a tracheo-oeso- phageal fistula. Definitive surgery was performed in 27 patients: the primary definitive procedure was oesophageal anastomosis in 15 and oesopha- geal replacement in 12. Aspects of diagnosis and selection of the most appropriate treatment mo- dality are discussed, with the results of treatment presented. Our current policy is to perform an oesophageal anastomosis whenever possible, and this has been successful in 7 of the last t 1 patients.
Key words: Oesophageat atresia - Gasless abdo- men - Oesophageal replacement - Long gap
Introduction
Oesophageal atresia without an accompanying tracheo-oesophageal fistula is a relatively rare anomaly and varies between 5% and 10% in most reported series of patient~ with oesophageal atre- sia and tracheo-oesophageal fistula [1, 2, 5, 6, 10, l l , 14, 15, 17, 19, 20, 24, 26, 33, 35, 38]. Many centres therefore have a limited experience of the anomaly; at the Royal Children's Hospital in Melbourne there have been 36 patients who have had atresia without fistula. Thus, we have aver- aged tess than one patient a year during a period which has seen many advances in neonatal care.
*Present address: Queen Elizabeth Hospital for Children, Hackney Road, London E2 8PS, UK. Offprint requests to: N.A. Myers
Despite these advances and increasing experience controversy still exists as to the most appropriate management of the condition [3, 4, 7, 9, 12, 13, 25, 27, 28, 32]. This paper reports our experience and suggests a protocol which may assist in deter- mining whether primary anastomosis or replace- ment is appropriate.
Materials and methods
During the period 1948 - 1986, a total of 553 babies with oeso- phageal atresia and/or tracheo-oesophageal fistula were ad- mitted to the Royal Children's Hospital, Melbourne. Oe- sophageal atresia without fistula was seen in 36 (6.5%) of these (Table I).
Much of the data was collected prospectively by one of the authors (NAM) and supplemented by careful review of each patient's hospital records.
Table 1. 553 patients with oesophageal atresia and/or tracheo- oesophageal fistula (1948- 1986)
Oesophageal atresia with distal tracheo-oesophageal fistula
Oesophageal atresia with proximal tracheo-oesophageal fistula
Oesophageal atresia with proximal and distal tracheo-oesophageal fistula
Oesophageal atresia without fistula
Tracheo-oesophageal fistula ("H')
Total
475
11
1
36
30
553
Results
Polyhydramnios was present in 34 patients. Birth weight ranged from 1.6 to 3.6 kg (mean = 2.3 kg). One or more associated congenital anomalies were re¢ognised in 21 patients (Table 2). Of 3 t pa- tients in whom the gestation was recorded, t7 (55%) were tess than 37 weeks-
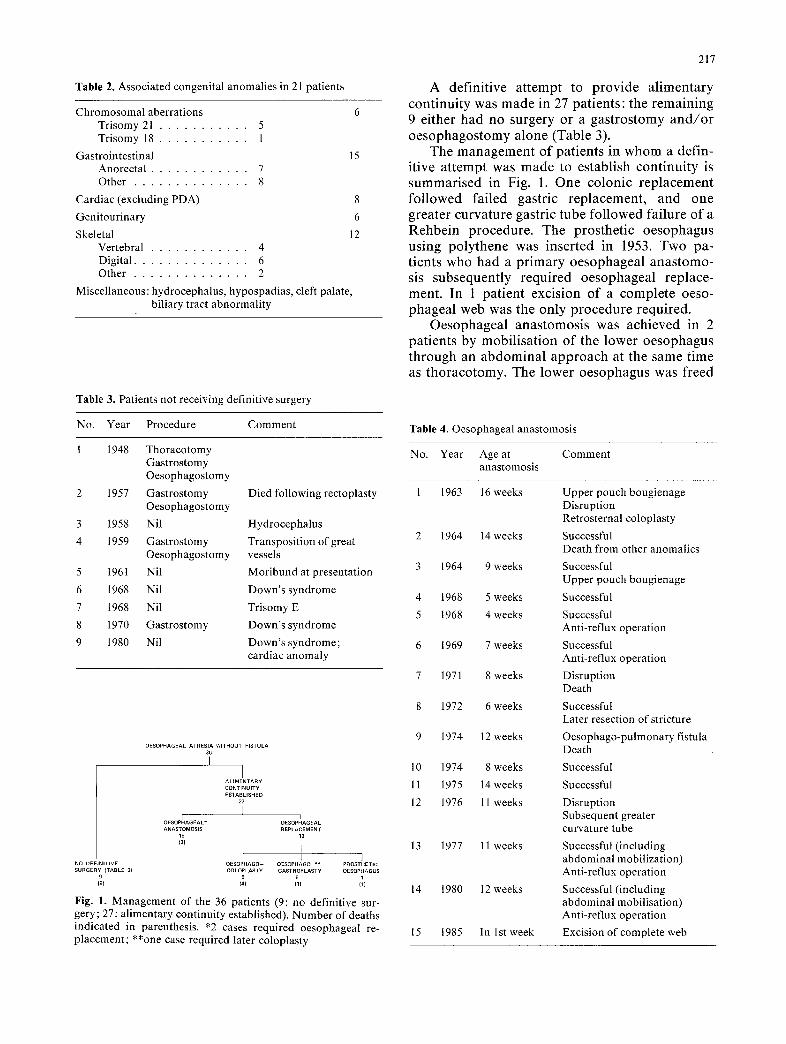
Table 2. Associated congenital anomalies in 21 patients
Chromosomal aberrations 6 Trisomy 21 . . . . . . . . . . . 5 Trisomy 18 . . . . . . . . . . . 1
Gastrointestinal 15 Anorectal . . . . . . . . . . . . 7 Other . . . . . . . . . . . . . . 8
Cardiac (excluding PDA) 8
Genitourinary 6
Skeletal 12 Vertebral . . . . . . . . . . . . 4 Digital . . . . . . . . . . . . . . 6 Other . . . . . . . . . . . . . . 2
Miscel laneous:hydrocephalus, hypospadias, cleft palate, biliary tract abnormali ty
Table 3. Patients not receiving definitive surgery
No. Year Procedure Comment
1 1948 Thoracotomy Gastrostomy Oesophagostomy
2 1957 Gastrostomy Oesophagostomy
1958 Nil
1959 Gastrostomy Oesophagostomy
1961 Nil
1968 Nil
1968 Nil
1970 Gastrostomy
1980 Nil
Died following rectoplasty
Hydrocephalus
Transposition of great vessels
Moribund at presentation
Down's syndrome
Trisomy E
Down°s syndrome
Down's syndrome; cardiac anomaly
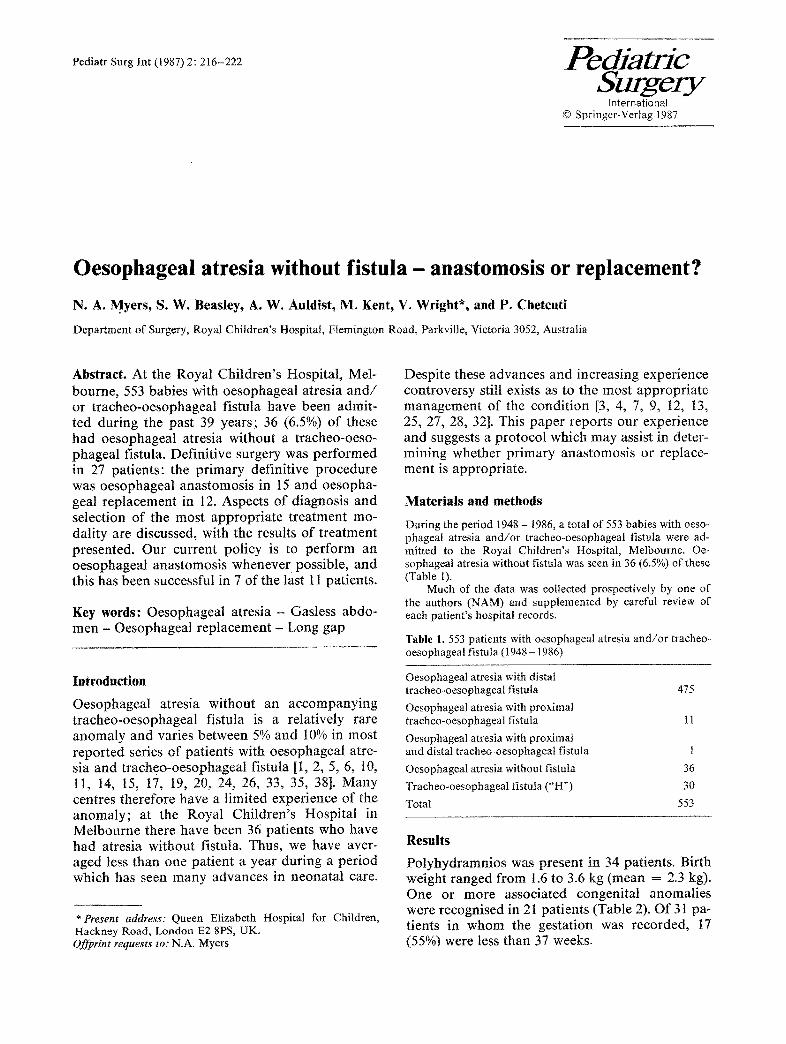
0ESOPHAGEAL ATRESIA WITHOUT FISTULA 38 I
I ALIMENTARY CONTINUITY ESTABLISHED
27
OESOPIHAGEAL * OESOPHIAGEAL ANASTOMOSIS REPLACEMENT
15 12
~3~ 1 I NO DEFINITIVE OESOPHAGO- OESOPHAGO ** PROSTHETIC SURGERY (TABLE 3} COLOPLAST¥ GASTROPLASTY OESOPHAGUS
9 5 6 1 (9) (4) (1 ) (1)
Fig. 1. Management of the 36 patients (9: no definitive sur- gery; 27: alimentary continuity established). Number of deaths indicated in parenthesis. *2 cases required oesophageal re- placement; **one case required later coloplasty
217
A definitive attempt to provide alimentary continuity was made in 27 patients: the remaining 9 either had no surgery or a gastrostomy and /o r oesophagostomy alone (Table 3).
The management of patients in whom a defin- itive attempt was made to establish continuity is summarised in Fig. 1. One colonic replacement followed failed gastric replacement, and one greater curvature gastric tube followed failure of a Rehbein procedure. The prosthetic oesophagus using polythene was inserted in 1953. Two pa- tients who had a primary oesophageal anastomo- sis subsequently required oesophageal replace- ment. In 1 patient excision of a complete oeso- phageal web was the only procedure required.
Oesophageal anastomosis was achieved in 2 patients by mobilisation of the lower oesophagus through an abdominal approach at the same time as thoracotomy. The lower oesophagus was freed
Table 4. Oesophageal anastomosis
No. Year Age at Comment anastomosis
1 1963 16 weeks
2 1964 14 weeks
3 1964 9 weeks
4 1968 5 weeks
5 1968 4 weeks
6 1969 7 weeks
7 1971 8 weeks
8 1972 6 weeks
9 1974 12 weeks
10 1974 8 weeks
11 1975 14 weeks
12 1976 11 weeks
13 1977 11 weeks
14 1980 12 weeks
15 1985 In 1st week
Upper pouch bougienage Disruption Retrosternal coloplasty
Successful Death from other anomalies
Successful Upper pouch bougienage
Successful
Successful Anti-reflux operation
Successful Anti-reflux operation
Disruption Death
Successful Later resection of stricture
Oesophago-pulmonary fistula Death
Successful
Successful
Disruption Subsequent greater curvature tube
Successful (including abdominal mobilization) Anti-reflux operation
Successful (including abdominal mobilisation) Anti-reflux operation
Excision of complete web
218
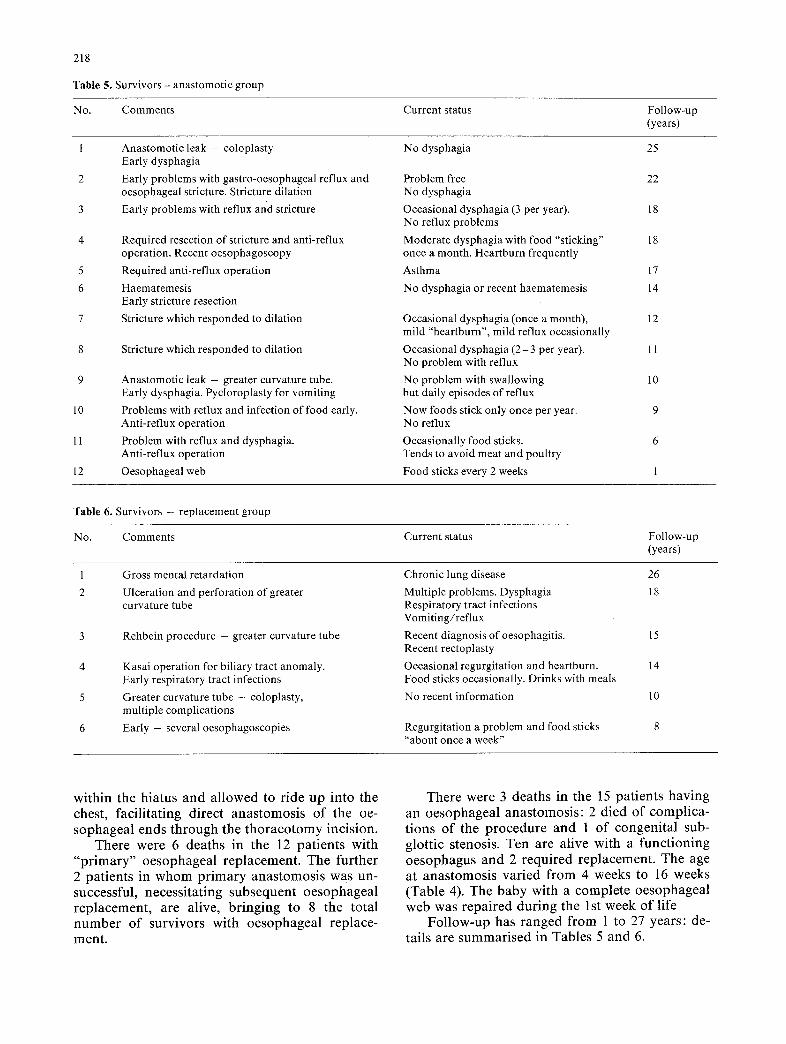
Table 5, Survivors - anastomotic group
No. Comments Current status Follow-up (years)
1 Anastomotic leak - coloplasty No dysphagia 25 Early dysphagia
2 Early problems with gastro-oesophageal reflux and 22 oesophageal stricture. Stricture dilation
3 Early problems with reflux and stricture 18
4 18
5 17
6 14
7 12
8 11
9 10
10 9
11 6
12 1
Required resection of stricture and anti-reflux operation. Recent oesophagoscopy
Required anti-reflux operation
Haematemesis Early stricture resection
Stricture which responded to dilation
Stricture which responded to dilation
Anastomotic leak - greater curvature tube. Early dysphagia. Pycloroplasty for vomiting
Problems with reflux and infection of food early. Anti-reflux operation
Problem with reflux and dysphagia. Anti-reflux operation
Oesophageal web
Problem free No dysphagia
Occasional dysphagia (3 per year). No reflux problems
Moderate dysphagia with food "sticking" once a month. Heartburn frequently
Asthma
No dysphagia or recent haematemesis
Occasional dysphagia (once a month), mild "heartburn", mild reflux occasionally
Occasional dysphagia (2 - 3 per year). No problem with reflux
No problem with swallowing but daily episodes of reflux
Now foods stick only once per year. No reflux
Occasionally food sticks. Tends to avoid meat and poultry
Food sticks every 2 weeks
Table 6. Survivors - replacement group
No. Comments Current status Follow-up (years)
Gross mental retardation
Ulceration and perforation of greater curvature tube
Rehbein procedure - greater curvature tube
Kasai operation for biliary tract anomaly. Early respiratory tract infections
Greater curvature tube - coloplasty, multiple complications
Early - several oesophagoscopies
Chronic lung disease 26
Multiple problems. Dysphagia 18 Respiratory tract infections Vomiting/reflux
Recent diagnosis of oesophagitis. 15 Recent rectoplasty
Occasional regurgitation and heartburn. 14 Food sticks occasionally. Drinks with meals
No recent information 10
Regurgitation a problem and food sticks "about once a week"
within the hiatus and allowed to ride up into the chest, facilitating direct anastomosis of the oe- sophageal ends through the thoracotomy incision.
There were 6 deaths in the 12 patients with "primary" oesophageal replacement. The further 2 patients in whom primary anastomosis was un- successful, necessitating subsequent oesophageal replacement, are alive, bringing to 8 the total number of survivors with oesophageal replace- ment.
There were 3 deaths in the 15 patients having an oesophageal anastomosis: 2 died of complica- tions of the procedure and 1 of congenital sub- glottic stenosis. Ten are alive with a functioning oesophagus and 2 required replacement. The age at anastomosis varied from 4 weeks to 16 weeks (Table 4). The baby with a complete oesophageal web was repaired during the 1st week of life
Follow-up has ranged from 1 to 27 years: de- tails are summarised in Tables 5 and 6.
D i s c u s s i o n
Until the 1960s, oesophageal anastomosis in oe- sophageal atresia without fistula was considered impossible and the standard management in- volved establishment of a salivary fistula in the neck as a cervical oesophagostomy. In 1965 Koop and Hamilton [16, 22] introduced the concept of "staged" management for oesophageal atresia with distal fistula, advocating early gastrostomy
219
followed by a period of waiting before oesopha- geal anastomosis. This concept was extended to the baby with atresia without fistula. Preservation of the upper pouch produced new problems: the baby had to remain in hospital; there was risk of aspiration from accumulation of saliva in the upper pouch; and the child could not "sham feed". Aspiration was reduced by instituting an intensive programme of nursing care, attention to the posture of the baby, and continuous or fre-
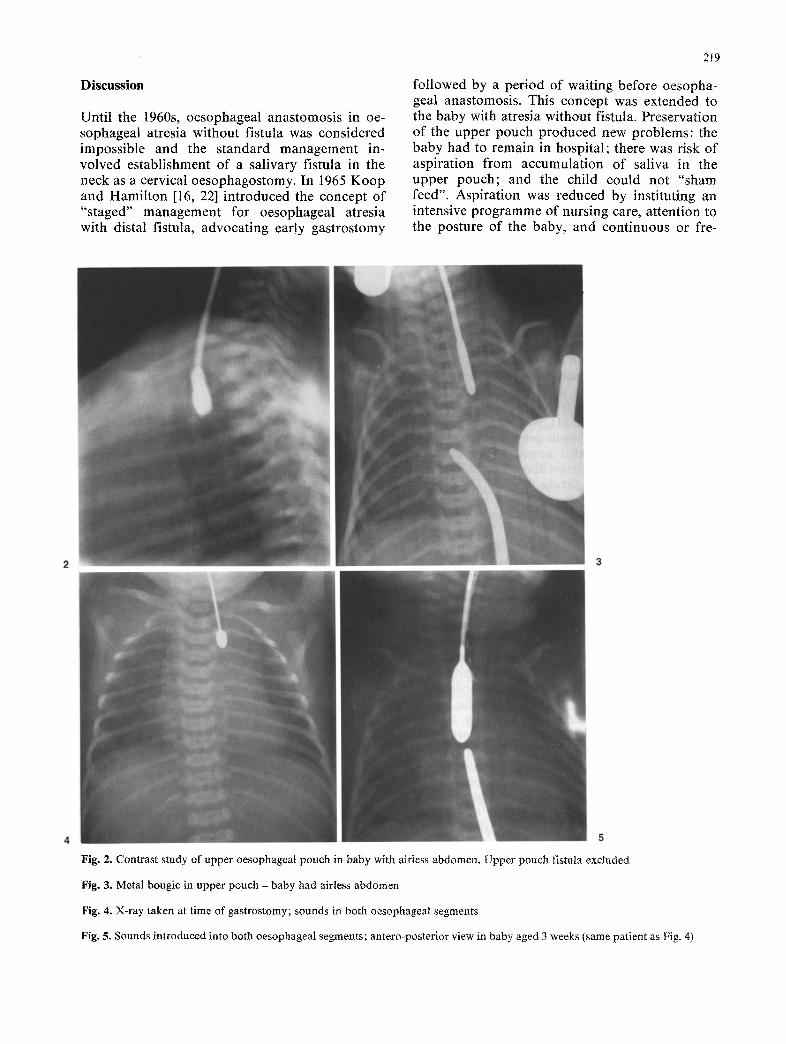
Fig. 2. Contrast study of upper oesophageal pouch in baby with airless abdomen, Upper pouch fistula excluded
Fig. 3. Metal bougie in upper pouch - baby had airless abdomen
Fig. 4. X-ray taken at time of gastrostomy; sounds in both oesophageal segments
Fig. 5. Sounds introduced into both oesophageal segments; antero-posterior view in baby aged 3 weeks (same patient as Fig. 4)
220
quent suction of the upper pouch. If further eval- uation showed that oesophageal anastomosis was not feasible, a cervical oesophagostomy was per- formed. In 1963 upper pouch bougienage was in- troduced. In retrospect, we believe that the main advantage of bougienage was to encourage upper pouch preservation in babies who would other- wise have had a cervical oesophagostomy.
The use of upper pouch bougienage as first de- scribed by Howard and Myers [21] led to the de- velopment of other techniques such as Rehbein's Olive technique [29, 30], electro-magnetic bougie- nage [18], and circular myotomy [23, 31, 34, 36, 37, 39], each of which had its proponents. We no longer perform bougienage, but do encourage large bolus gastrostomy feeds with the object of promoting gastro-oesophageal reflux in the belief that spontaneous growth of the lower oesophageal segment may be increased by reflux.
Once a child with oesophageal atresia has been shown to have a gasless abdomen two ques- tions need answering: (1) is there a proximal tracheo-oesophageal fistula present? This is de- monstrated by a careful upper pouch contrast study and in our experience about one in four will have an upper-pouch fistula [8]; and (2) what is the length of the gap between the oesophageal ends and is it such that a primary anastomosis can be performed?
The gap between the oesphageal segments in isolated oesophageal atresia tends to be much greater than when a tracheo-oesophageal fistula is present. However, we know from our own experi- ence that direct end-to-end oesophageal anasto- mosis is possible in many of these patients and has been successfully performed in 7 of our last 11 patients.
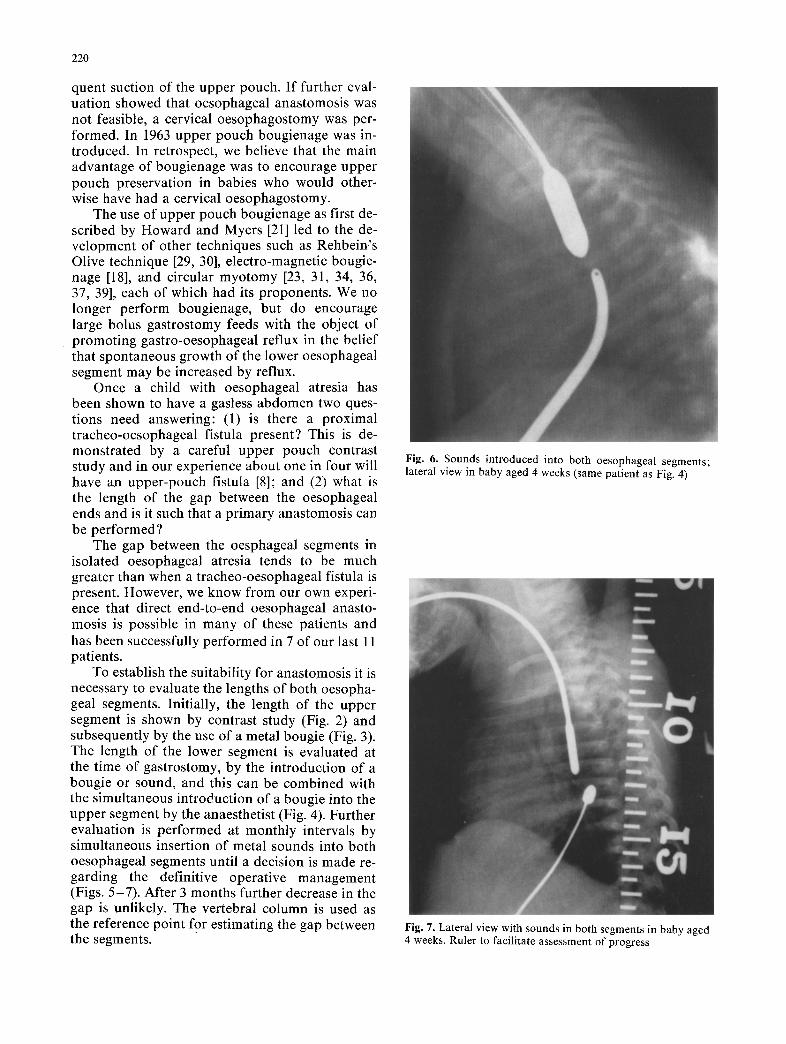
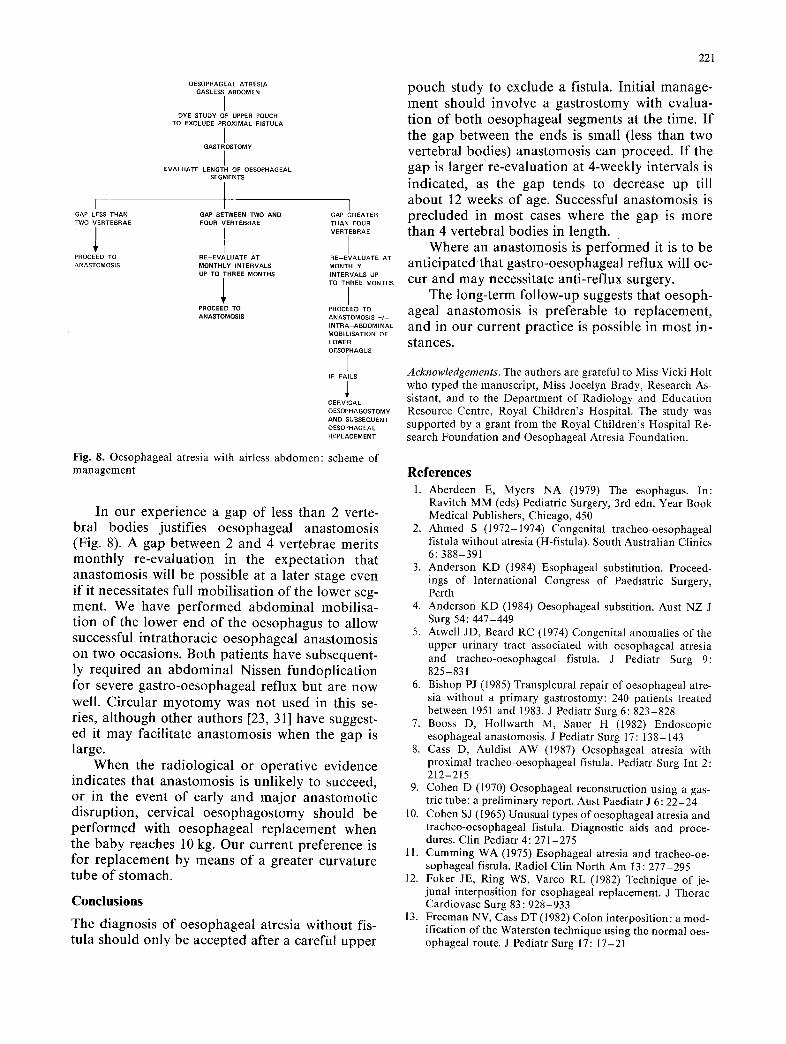
To establish the suitability for anastomosis it is necessary to evaluate the lengths of both oesopha- geal segments. Initially, the length of the upper segment is shown by contrast study (Fig. 2) and subsequently by the use of a metal bougie (Fig. 3). The length of the lower segment is evaluated at the time of gastrostomy, by the introduction of a bougie or sound, and this can be combined with the simultaneous introduction of a bougie into the upper segment by the anaesthetist (Fig. 4). Further evaluation is performed at monthly intervals by simultaneous insertion of metal sounds into both oesophageal segments until a decision is made re- garding the definitive operative management (Figs. 5-7). After 3 months further decrease in the gap is unlikely. The vertebral column is used as the reference point for estimating the gap between the segments.
Fig. 6. Sounds introduced into both oesophageal segments; lateral view in baby aged 4 weeks (same patient as Fig. 4)
Fig. 7. Lateral view with sounds in both segments in baby aged 4 weeks. Ruler to facilitate assessment of progress
221
I GAP LESS THAN TWO VERTEBRAE
PROCEED TO ANASTOMOSIS
OESOPHAGEAL ATRESIA GASLESSARDOMEN
DYE STUDY OF UPPER POUCH TO EXCLUDE PROXIMAL FISTULA
GASTROSTOM¥
I EVALUATE LENGTH OF OESOPHAGEAL
SEGMENTS
t GAP BETWEEN TWO AND FOUR VERTEBRAE
RE-EVALUATE AT MONTHLY INTERVALS UP TO THREE MONTHS
1 PROCEED TO ANASTOMOSIS
I GAP GREATER THAN FOUR VERTEBRAE
I RE-EVALUATE AT MONTHLY INTERVALS UP TO THREE MONTHS
I PROCEED TO ANASTOMOSIS +/-- INTRA ABDOMINAL MOBILISATION OF LOWER OESOPHAGUS
I IF FAILS
CERVICAL OESOPHAGOSTOMY AND SUBSEQUENT OESOPHAGEAL REPLACEMENT
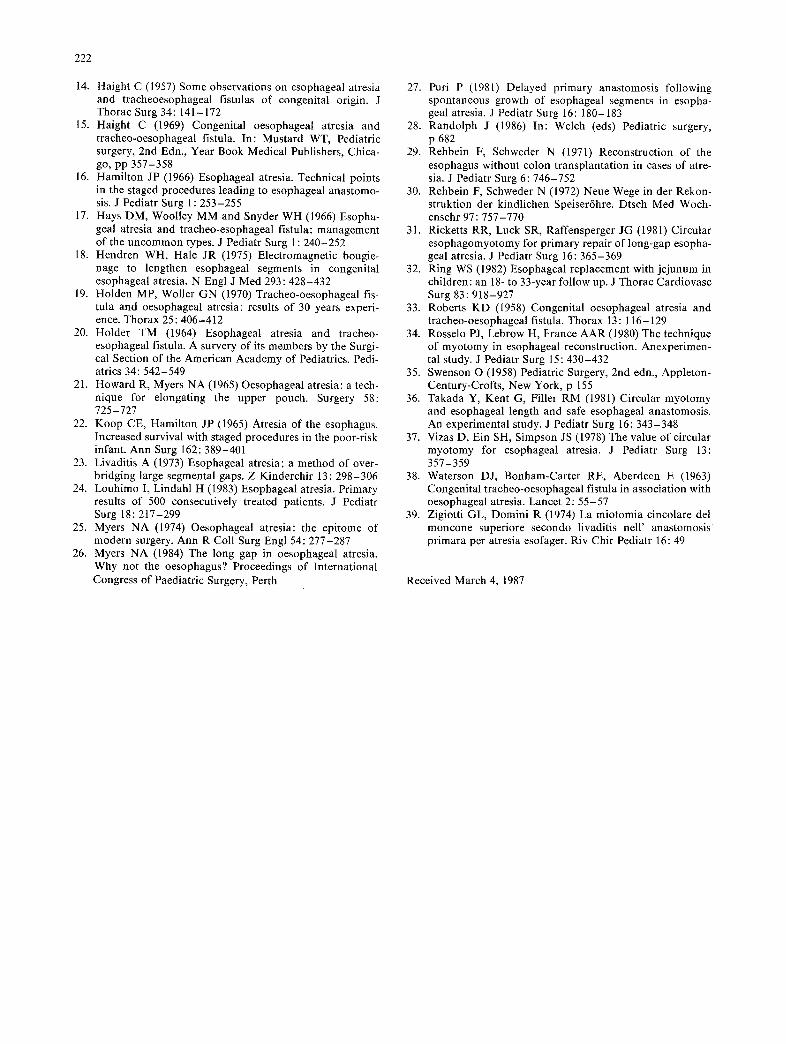
Fig. 8. Oesophageal atresia with airless abdomen: scheme of management
In our experience a gap of less than 2 verte- bral bodies justifies oesophageal anastomosis (Fig. 8). A gap between 2 and 4 vertebrae merits monthly re-evaluation in the expectation that anastomosis will be possible at a later stage even if it necessitates full mobilisation of the lower seg- ment. We have performed abdominal mobilisa- tion of the lower end of the oesophagus to allow successful intrathoracic oesophageal anastomosis on two occasions. Both patients have subsequent- ly required an abdominal Nissen fundoplication for severe gastro-oesophageal reflux but are now well. Circular myotomy was not used in this se- ries, although other authors [23, 31] have suggest- ed it may facilitate anastomosis when the gap is large.
When the radiological or operative evidence indicates that anastomosis is unlikely to succeed, or in the event of early and major anastomotic disruption, cervical oesophagostomy should be performed with oesophageal replacement when the baby reaches 10 kg. Our current preference is for replacement by means of a greater curvature tube of stomach.
C o n c l u s i o n s
The diagnosis of oesophageal atresia without fis- tula should only be accepted after a careful upper
pouch study to exclude a fistula. Initial manage- ment should involve a gastrostomy with evalua- tion of both oesophageal segments at the time. If the gap between the ends is small (less than two vertebral bodies) anastomosis can proceed. If the gap is larger' re-evaluation at 4-weekly intervals is indicated, as the gap tends to decrease up till about 12 weeks of age. Successful anastomosis is precluded in most cases where the gap is more than 4 vertebral bodies in length.
Where an anastomosis is performed it is to be anticipatedthat gastro-oesophageal reflux will oc- cur and may necessitate anti-reflux surgery.
The long-term follow-up suggests that oesoph- ageal anastomosis is preferable to replacement, and in our current practice is possible in most in- stances.
Acknowledgements. The authors are grateful to Miss Vicki Holt who typed the manuscript, Miss Jocelyn Brady, Research As- sistant, and to the Department of Radiology and Education Resource Centre, Royal Children's Hospital. The study was supported by a grant from the Royal Children's Hospital Re- search Foundation and Oesophageal Atresia Foundation.
References 1. Aberdeen E, Myers NA (1979) The esophagus. In:
Ravitch MM (eds) Pediatric Surgery, 3rd edn. Year Book Medical Publishers, Chicago, 450
2. Ahmed S (1972-1974) Congenital tracheo-oesophageal fistula without atresia (H-fistula). South Australian Clinics 6:388-391
3. Anderson KD (1984) Esophageal substitution. Proceed- ings of International Congress of Paediatric Surgery, Perth
4. Anderson KD (1984) Oesophageal substition. Aust NZ J Surg 54:447-449
5. Atwell JD, Beard RC (1974) Congenital anomalies of the upper urinary tract associated with oesophageal atresia and tracheo-oesophageal fistula. J Pediatr Surg 9: 825-831
6. Bishop PJ (1985) Transpleural repair of oesophageal atre- sia without a primary gastrostomy: 240 patients treated between 1951 and 1983. J Pediatr Surg 6:823-828
7. Booss D, Hollwarth M, Sauer H (1982) Endoscopic esophageal anastomosis. J Pediatr Surg 17: 138-143
8. Cass D, Auldist AW (1987) Oesophageal atresia with proximal tracheo-oesophageal fistula. Pediatr Surg Int 2: 212-215
9. Cohen D (1970) Oesophageal reconstruction using a gas- tric tube: a preliminary report. Aust Paediatr J 6:22-24
10. Cohen SJ (1965) Unusual types of oesophageal atresia and tracheo-oesophageal fistula. Diagnostic aids and proce- dures. Clin Pediatr 4:271-275 Cumming WA (1975) Esophageal atresia and tracheo-oe- sophageal fistula. Radiol Clin North Am 13:277-295 Foker JE, Ring WS, Varco RL (1982) Technique of je- junal interposition for esophageal replacement. J Thorac Cardiovasc Surg 83:928-933 Freeman NV, Cass DT (1982) Colon interposition: a mod- ification of the Waterston technique using the normal oes- ophageal route. J Pediatr Surg 17:17-21
11.
12.
13.
222
14. Haight C (1957) Some observations on esophageal atresia and tracheoesophageal fistulas of congenital origin. J Thorac Surg 34: 141-172
15. Haight C (1969) Congenital oesophageal atresia and tracheo-oesophageal fistula. In: Mustard WT, Pediatric surgery, 2nd Edn., Year Book Medical Publishers, Chica- go, pp 357-358
16. Hamilton JP (1966) Esophageal atresia. Technical points in the staged procedures leading to esophageal anastomo- sis. J Pediatr Surg 1 : 253-255
17. Hays DM, Woolley MM and Snyder WH (1966) Esopha- geal atresia and tracheo-esophageal fistula: management of the uncommon types. J Pediatr Surg 1 : 240-252
18. Hendren WH, Hale JR (1975) Electromagnetic bougie- nage to lengthen esophageal segments in congenital esophageal atresia. N Engl J Med 293:428-432
19. Holden MP, Woller GN (1970) Tracheo-oesophageal fis- tula and oesophageal atresia: results of 30 years experi- ence. Thorax 25:406-412
20. Holder TM (1964) Esophageal atresia and tracheo- esophageal fistula. A survery of its members by the Surgi- cal Section of the American Academy of Pediatrics. Pedi- atrics 34:542-549
21. Howard R, Myers NA (1965) Oesophageal atresia: a tech- nique for elongating the upper pouch. Surgery 58: 725-727 Koop CE, Hamilton JP (1965) Atresia of the esophagus. Increased survival with staged procedures in the poor-risk infant. Ann Surg 162:389-401 Livaditis A (1973) Esophageal atresia; a method of over- bridging large segmental gaps. Z Kinderchir 13:298-306 Louhimo I, Lindahl H (1983) Esophageal atresia. Primary results of 500 consecutively treated patients. J Pediatr Surg 18:217-299 Myers NA (1974) Oesophageal atresia: the epitome of modern surgery. Ann R Coll Surg Engl 54:277-287 Myers NA (1984) The long gap in oesophageal atresia. Why not the oesophagus? Proceedings of International Congress of Paediatric Surgery, Perth
22.
23.
24.
25.
26.
27. Puri P (1981) Delayed primary anastomosis following spontaneous growth of esophageal segments in esopha- geal atresia. J Pediatr Surg 16: 180-183
28. Randolph J (1986) In: Welch (eds) Pediatric surgery, p 682
29. Rehbein F, Schweder N (1971) Reconstruction of the esophagus without colon transplantation in cases of atre- sia. J Pediatr Surg 6:746-752
30. Rehbein F, Schweder N (1972) Neue Wege in der Rekon- struktion der kindlichen Speiser6hre. Dtsch Med Woch- enschr 97 : 757-770
31. Ricketts RR, Luck SR, Raffensperger JG (1981)Circular esophagomyotomy for primary repair of long-gap esopha- geal atresia. J Pediatr Surg 16:365-369
32. Ring WS (1982) Esophageal replacement with jejunum in children: an 18- to 33-year follow up. J Thorac Cardiovasc Surg 83:918-927
33. Roberts KD (1958) Congenital oesophageal atresia and tracheo-oesophageal fistula. Thorax 13 : 116-129
34. Rosselo PJ, Lebrow H, France AAR (1980) The technique of myotomy in esophageal reconstruction. Anexperimen- tal study. J Pediatr Surg 15:430-432
35. Swenson O (1958) Pediatric Surgery, 2nd edn., Appleton- Century-Crofts, New York, p 155
36. Takada Y, Kent G, Filler RM (1981) Circular myotomy and esophageal length and safe esophageal anastomosis. An experimental study. J Pediatr Surg 16:343-348
37. Vizas D, Ein SH, Simpson JS (1978) The value of circular myotomy for esophageal atresia. J Pediatr Surg 13: 357-359
38. Waterson DJ, Bonham-Carter RE, Aberdeen E (1963) Congenital tracheo-oesophageal fistula in association with oesophageal atresia. Lancet 2:55-57
39. Zigiotti GL, Domini R (1974) La miotomia cincolare del moncone superiore secondo livaditis nell' anastomosis primara per atresia esofager. Riv Chit Pediatr 16:49
Received March 4, 1987
Related Documents











