OCULAR MANIFESTATIONS OF HIV INFECTION DR MD SHAHID MANZOOR AMUIO, ALIGARH

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
OCULAR MANIFESTATIONS OF
HIV INFECTION
DR MD SHAHID MANZOORAMUIO, ALIGARH
INTRODUCTION Human immunodeficiency virus infection / acquired
immunodeficiency syndrome (HIV/AIDS) is
a disease of the human immune system caused by
infection with human immunodeficiency
virus (HIV).
leads to gradual decrease in CD4+ T lymphocytes
causing subsequent opportunistic infections and
neoplasia.
70-75% of patients infected with HIV will develop
some form of ocular involvement.
Ocular manifestations of HIV/AIDS
Direct infection by HIV,
Opportunistic infections
Neoplasia and
Drug related
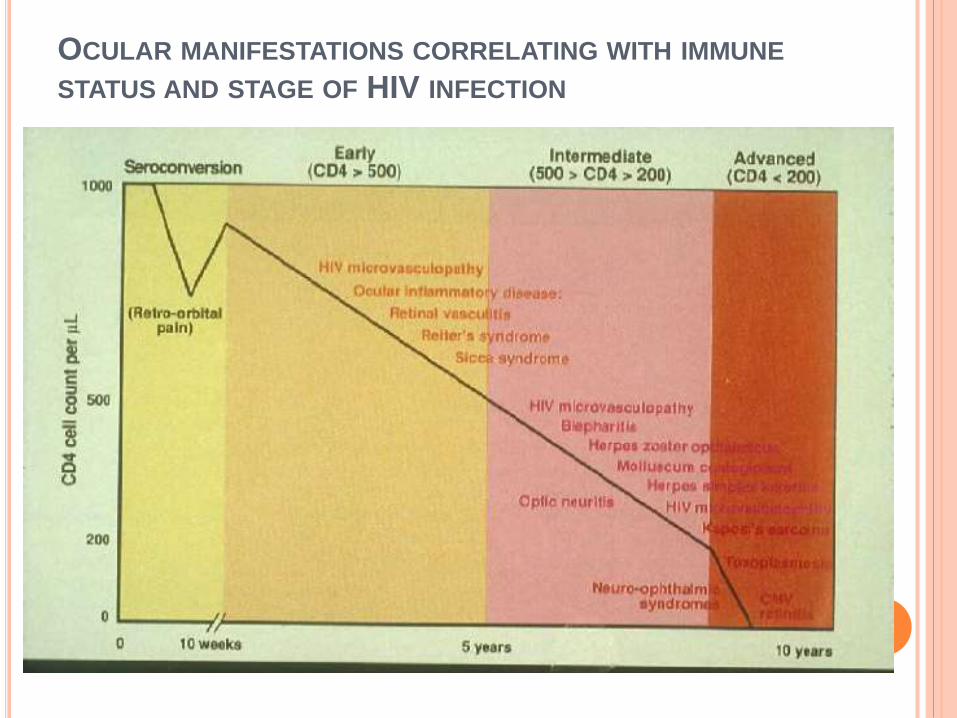
OCULAR MANIFESTATIONS CORRELATING WITH IMMUNE
STATUS AND STAGE OF HIV INFECTION

A ) ADNEXAL MANIFESTATIONS
B) ANTERIOR SEGMENT MANIFESTATION
C) POSTERIOR SEGMENT MANIFESTATIONS
D) NEURO-OPHTHALMIC MANIFESTATIONS
E) ORBITAL MANIFESTATIONS
F) DRUG-RELATED OCULAR TOXICITY IN HIV-
INFECTED PATIENTS
A) ADNEXAL MANIFESTATIONS
1) Herpes zoster ophthalmicus (HZO)
2) Kaposi sarcoma
3) Molluscum contagiosum
4) Conjunctival microvasculopathy
1) HERPES ZOSTER OPHTHALMICUS
5-15% of HIV patients.
Reactivation of a latent infection by VZV in the
dorsal root of trigeminal nerve .
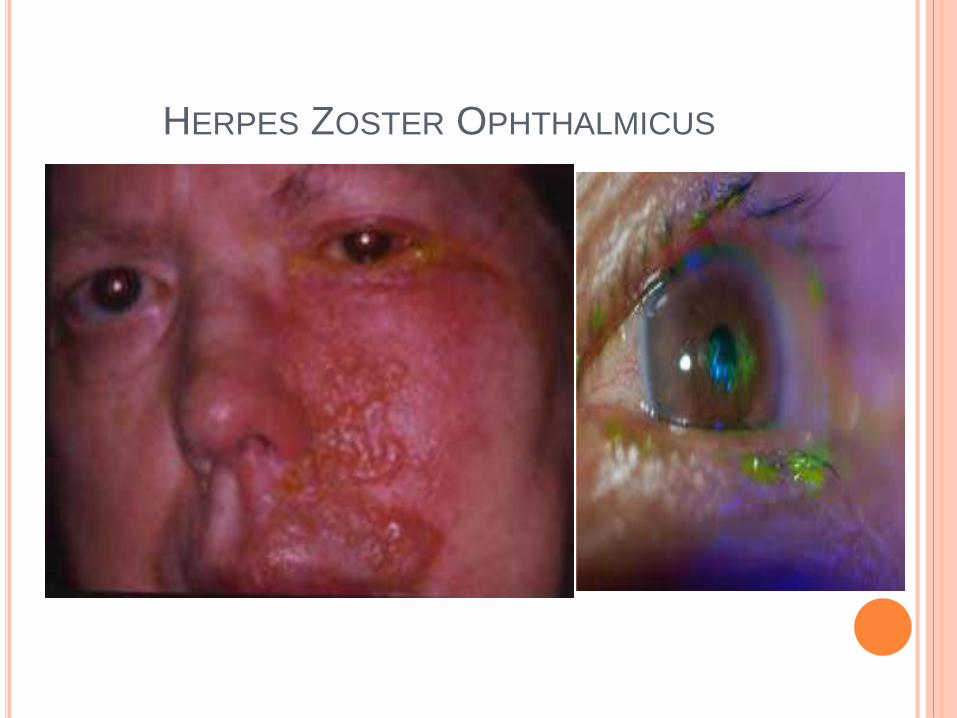
Manifests with a painful maculo -papulo -vesicular
rash .
Involves the upper lid and does not cross the
midline.
Keratitis, scleritis, uveitis, retinitis, or cns
involvement
Cranial nerve palsies
HERPES ZOSTER OPHTHALMICUS
HERPES ZOSTER OPHTHALMICUS
Intravenous acyclovir 10 mg/kg 3 times per day for
7 days,
followed by oral acyclovir 800 mg to 1 g 5 times per
day for an additional 7 days.
This regimen is most effective when started within
72 hours of onset of the vesicular lesions.
This treatment reduces the frequency of
recurrences.
2) KAPOSI SARCOMA
25% of HIV patients.
Human herpes virus type 8
Mesenchymal-derived vascular neoplasm.
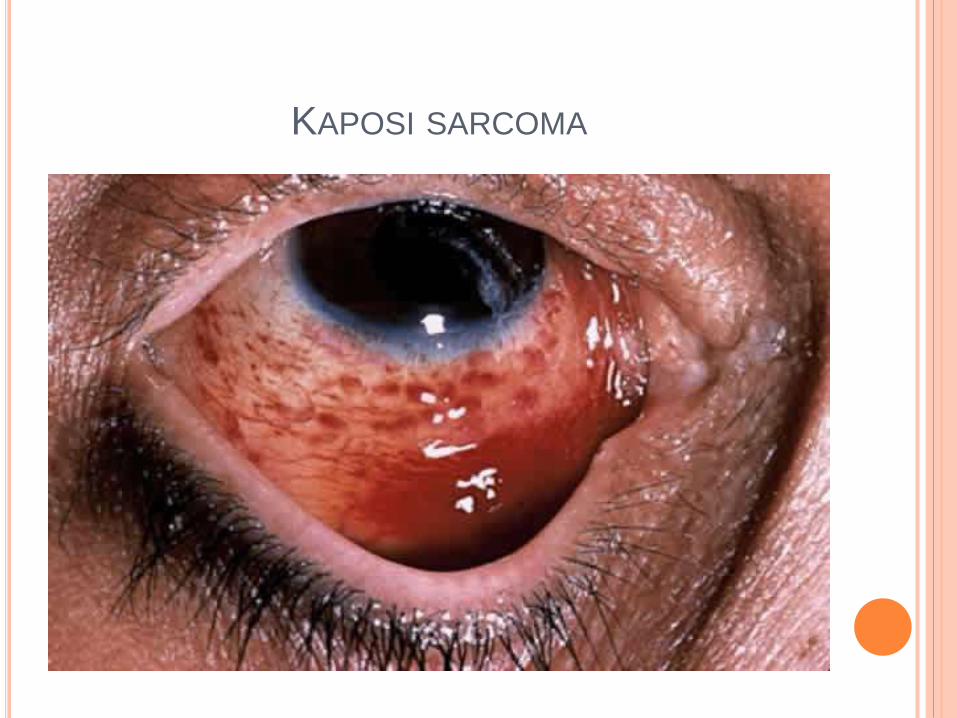
Manifests with a violet-brown , non-tender nodule.
Eyelid and conjunctival Kaposi sarcoma tend to mimic chalazion and localized subconjunctivalhemorrhage, respectively.
It can progress rapidly to other sites such as the gastrointestinal tract and CNS
Complications of ocular Kaposi sarcoma include trichiasis and entropion formation. .

KAPOSI SARCOMA
KAPOSI SARCOMA

KAPOSI SARCOMA
Radiation therapy
Intralesional chemotherapy with
vinblastine, alpha interferon, and liposomal
daunorubicin.
Surgical excision of the tumor.

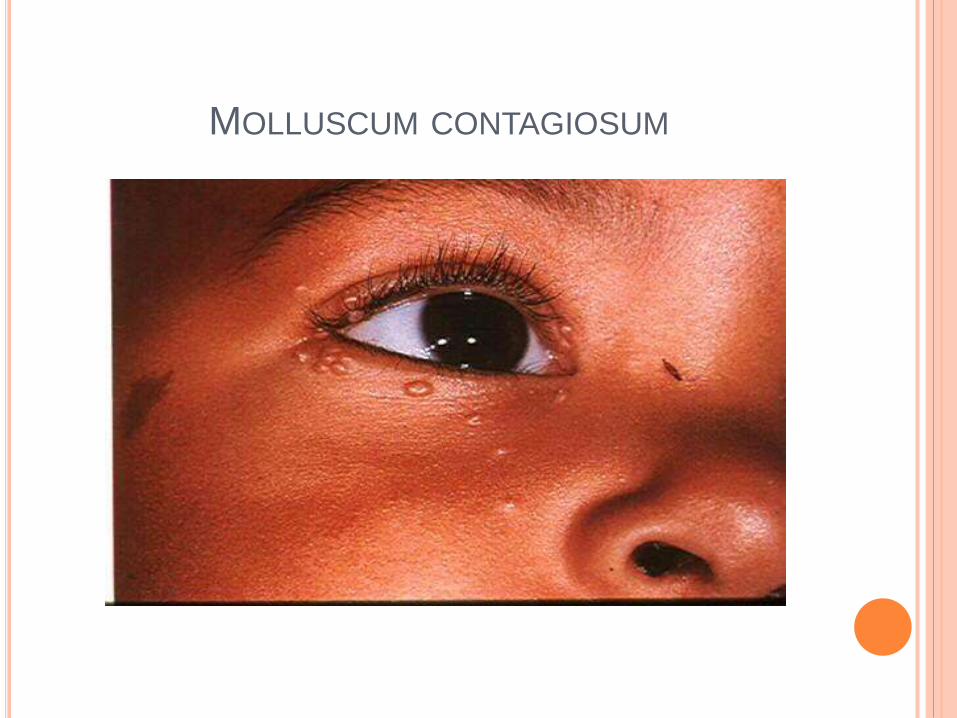
3) MOLLUSCUM CONTAGIOSUM
20% of HIV patients
It is a highly contagious dermatitis caused by DNA
poxvirus, and it may affect mucous membranes as
well as skin.
Manifests with multiple, small, painless, umbilicated
lesions which produce a waxy discharge when
pressured.
A self-limiting disease with spontaneous resolution
taking months to years.
MOLLUSCUM CONTAGIOSUM

MOLLUSCUM CONTAGIOSUM
MOLLUSCUM CONTAGIOSUM
Molluscum contagiosum lesions of the skin can be
treated with
Excision (with or without curettage)
Cryotherapy
Topical agents- phenol and trichloroacetic acid.

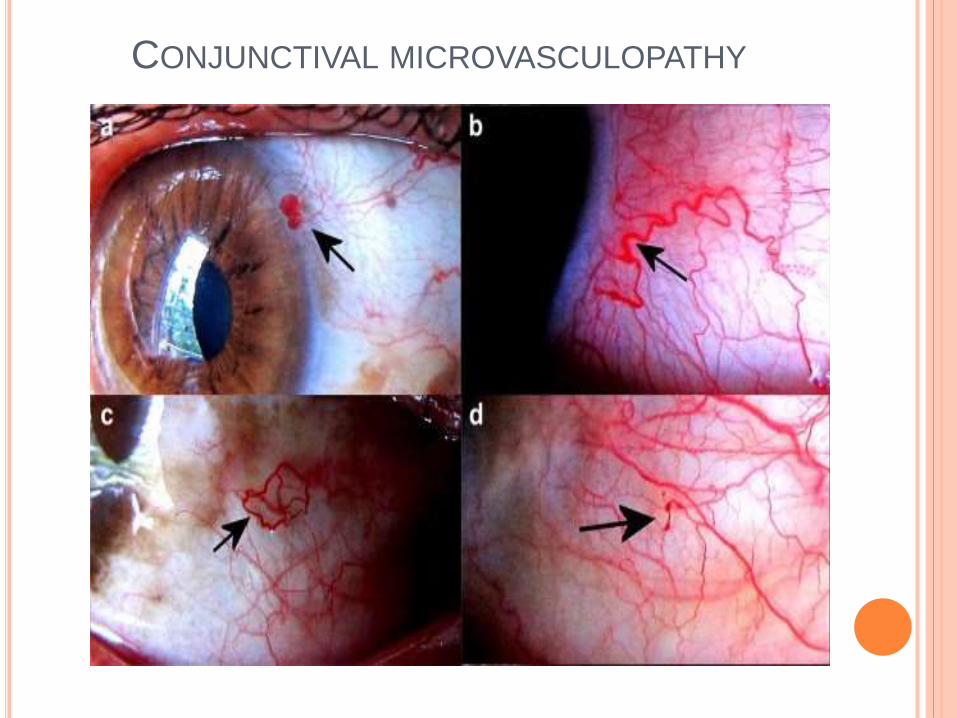
4) CONJUNCTIVAL MICROVASCULOPATHY
70 - 80% of HIV patients
Increased plasma viscosity
immune-complex deposition are believed to be
involved and
Direct infection of the conjunctival vascular
endothelium by HIV.
These changes include segmental vascular
dilation and narrowing, microaneurysm
formation, and appearance of comma-shaped
vascular fragments.
CONJUNCTIVAL MICROVASCULOPATHY
B) ANTERIOR SEGMENT MANIFESTATIONS
More than 50% of HIV-positive patients
Common symptoms include irritation, pain,
photophobia, redness and decreased vision
1)Keratoconjunctivitis sicca
2) Keratitis
3) Iridocyclitis
1) KERATOCONJUNCTIVITIS SICCA
10-20% of patients who are HIV positive.
The etiology is related to HIV-mediated
inflammation and damage of the accessory and
major lacrimal glands.
Patients complain of burning uncomfortable red
eyes.
Artificial tears and
lubricating ointment.

KERATOCONJUNCTIVITIS SICCA
2) INFECTIOUS KERATITIS
Main etiology –
Viral (VZV and HSV )- most frequent but less
severe
Bacterial and
less frequent but more severe.
Fungal keratitis
The most common fungal organism is Candida,
especially in intravenous drug users and Fusarium
and Aspergillus species .
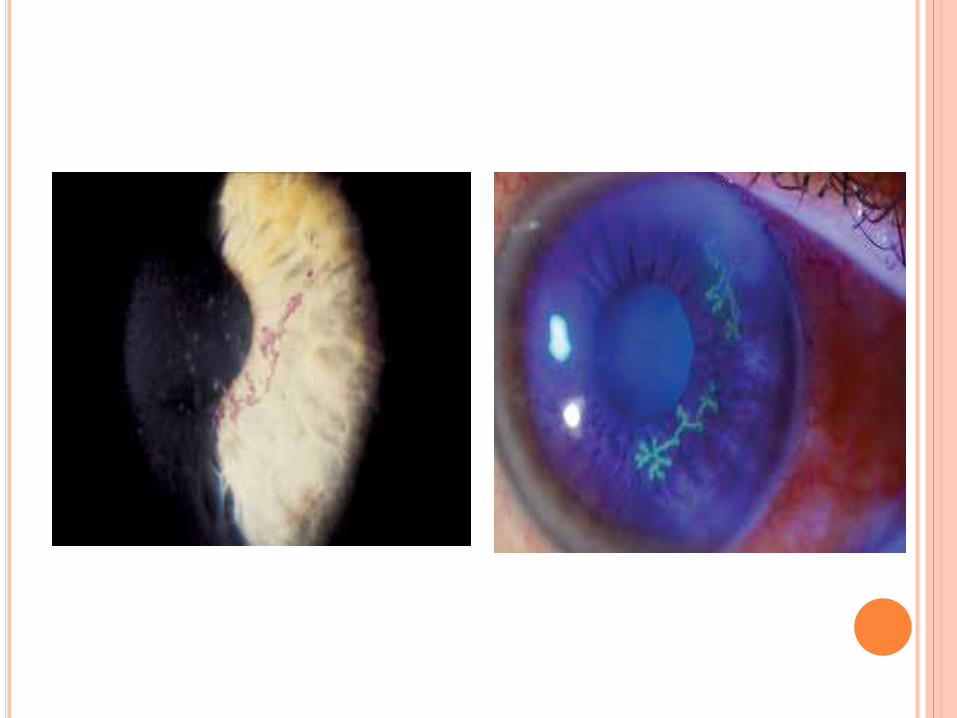
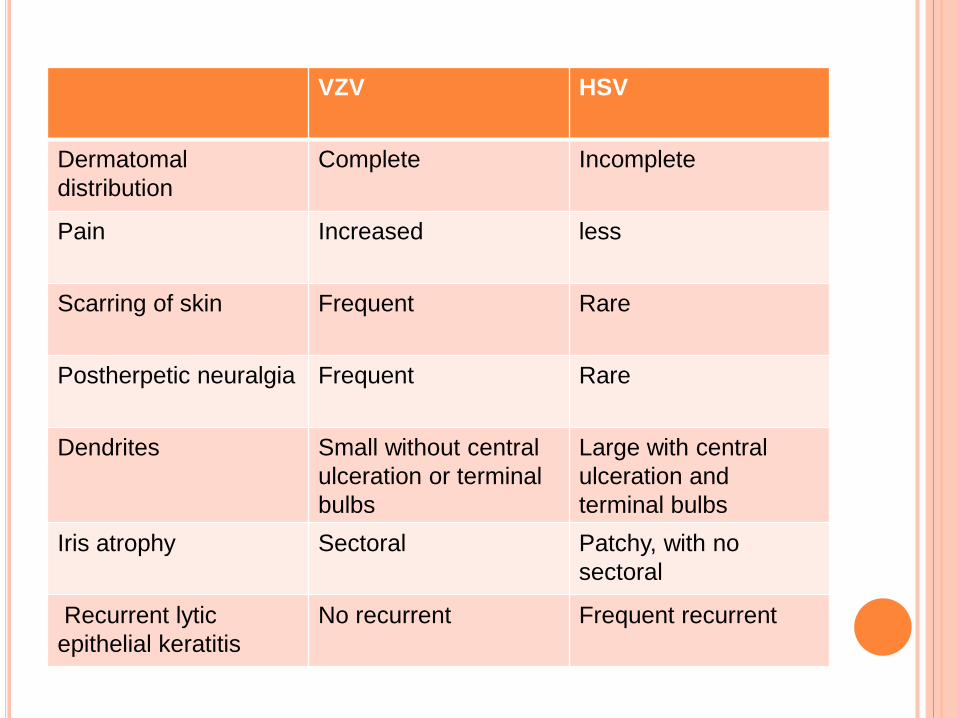
VZV HSV
Dermatomal
distribution
Complete Incomplete
Pain Increased less
Scarring of skin Frequent Rare
Postherpetic neuralgia Frequent Rare
Dendrites Small without central
ulceration or terminal
bulbs
Large with central
ulceration and
terminal bulbs
Iris atrophy Sectoral Patchy, with no
sectoral
Recurrent lytic
epithelial keratitis
No recurrent Frequent recurrent
VARICELLA-ZOSTER VIRUS KERATITIS
Recommended treatment is
Oral acyclovir 800 mg 5 times per day or famciclovir
125-500 mg 3-5 times per day.
Chronic treatment may be required for VZV
keratitis. This usually minimizes symptoms and
shortens the duration of viral shedding.
Severe disciform stromal keratitis - treated with
topical corticosteroids.
HERPES SIMPLEX VIRUS KERATITIS
Debridement of HSV epithelial keratitis with a dry cotton-
tipped applicator or a cellulose sponge can hasten
resolution and decrease the load of infectious virus and
viral antigens.
Medical treatment includes acyclovir topical 3%
ointment 5 times daily for 14 days or oral dosage form
400 mg 5 times daily for 7 days; or famciclovir 500 mg
by mouth 3 times daily for 7 days.
HSV neurotrophic keratopathy is a condition that
should be managed with nonpreserved lubricants,
eyelid patching, bandage contact lenses, and
sometimes autologous serum and nerve growth factor.

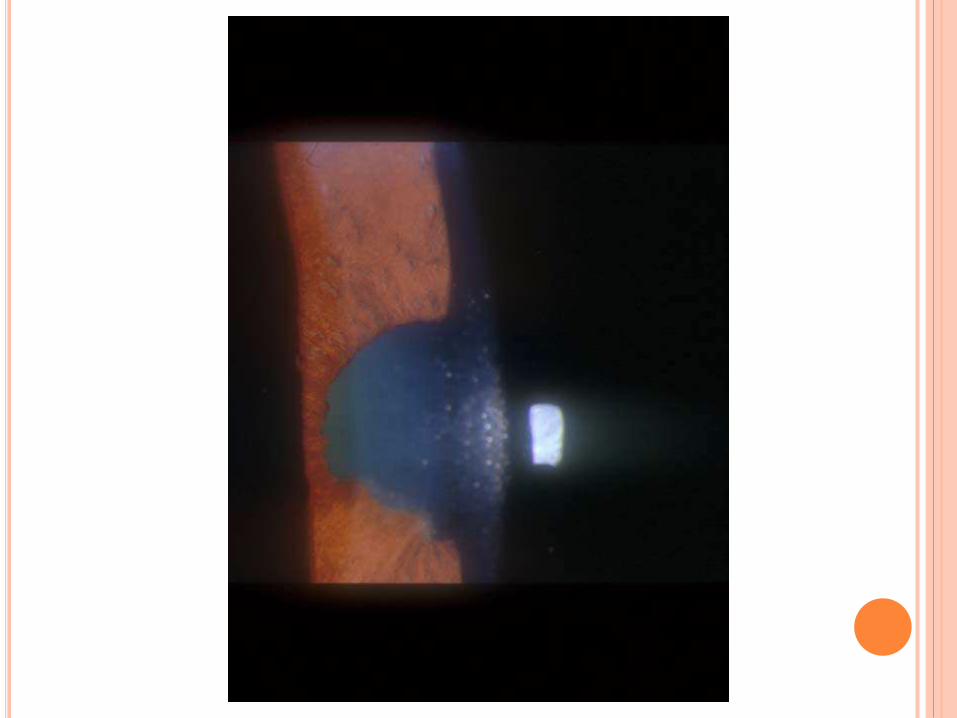
3) IRIDOCYCLITIS
The etiology of iridocyclitis in HIV-positive
patients includes sequelae of retinitis,
retinochoroiditis, and drug toxicity ( rifabutin,
cidofovir), secondary to direct toxic effect upon
the non-pigmented epithelium of the ciliary
body.
Mild iridocyclitis associated with viral retinitis
due to CMV,HSV, VZV.
Severe, seen in association with ocular
toxoplasmosis, tuberculosis, syphilis, or bacterial
or fungal retinitis.
Treatment
Topical corticosteroid drops are used frequently
but with extreme caution and with proper
antimicrobial coverage when infection is
suspected.
If toxicity from the medication is suspected, the
dose should be tapered or the causative agent
should be discontinued.
C) POSTERIOR SEGMENT MANIFESTATIONS
Posterior segment structures involved in HIV-
positive patients include the retina, choroid, and
optic nerve head.
50% of patients who are HIV positive.
Symptoms are floaters, flashing lights, visual field
defect, and decreased visual acuity.
Presence of an afferent pupillary defect strongly
suggests significant retinal or optic nerve
involvement.
Diagnoses often are based on clinical evidence
seen on funduscopic examinations.
POSTERIOR SEGMENT MANIFESTATIONS
1) HIV retinopathy
2) HIV-related retinochoroiditis
1) HIV RETINOPATHY
50-70% of HIV-infected patients
Arteriolar occlusion in HIV retinal
microvasculopathy leads to interruption of the
axoplasmic flow and the subsequent
accumulations of axoplasmic debris, which
manifests as cotton-wool spots.
Increased plasma viscosity, immune-complex
deposition, and a direct cytopathic effect of the
virus on the retinal vascular endothelium are
believed to be involved.
asymptomatic and transient, but it may contribute to
the optic nerve atrophy seen in many of the
patients. Common findings may include the
following:
Cotton-wool spots
Intraretinal hemorrhages
Roth spots (white-centered hemorrhages)
Retinal microaneurysms
No treatment is indicated for HIV retinopathy.
These patients require observation only.


2) HIV-RELATED RETINOCHOROIDITIS
Viruses are the MC
CMV , VZV and, less commonly HSV .
Bacterial causes include Mycobacterium
tuberculosis and Treponema pallidum (syphilis).
Parasitic causes include Toxoplasma gondii and
Pneumocystis jiroveci
Fungal causes include Candida, Cryptococcus
neoformans, and Histoplasma capsulatum, as
well as, Sporothrix, and Aspergillus species.
Cytomegalovirus retinitis
Acute Retinal Necrosis
Progressive Outer Retinal Necrosis
(Varicella-Zoster Retinitis)
Toxoplasma Retinochoroiditis
Tuberculosis.
CYTOMEGALOVIRUS RETINITIS
Most common cause of intraocular infection
Usually in CD4 < 50/microlitre
Painless, progressive loss of vision
It presents with a wide range of clinical
appearances, from cotton wool to confluent areas
of full thickness retinal necrosis.
Infection spreads centrifugally from that focus
with advancement of lesion borders toward the
fovea like “brushfire” pattern at a median rate of
24 μm/day.
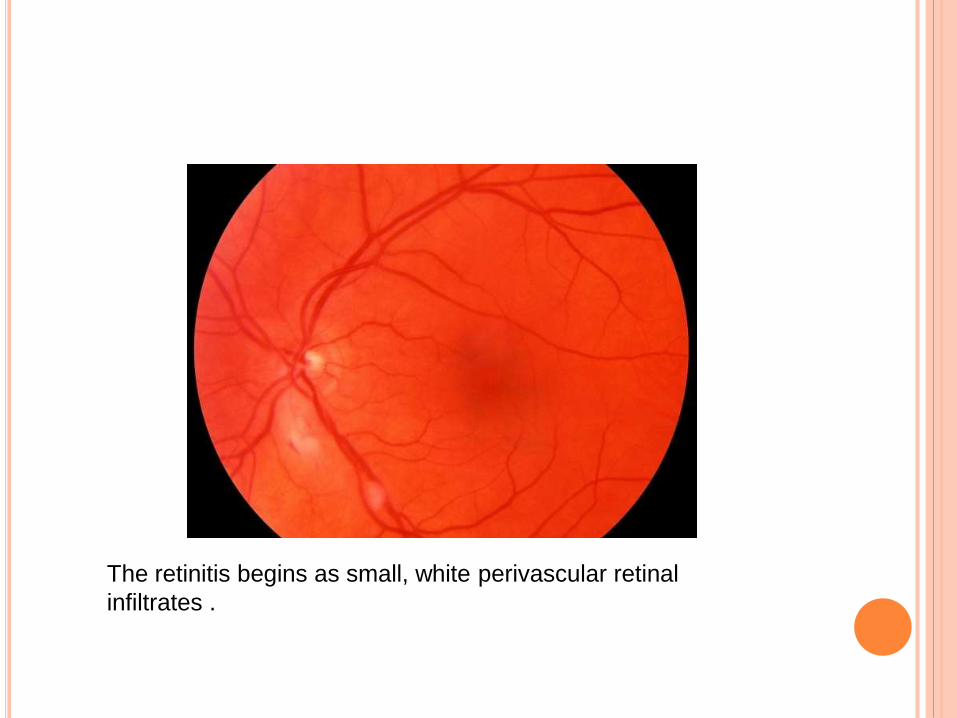
The retinitis begins as small, white perivascular retinal
infiltrates .
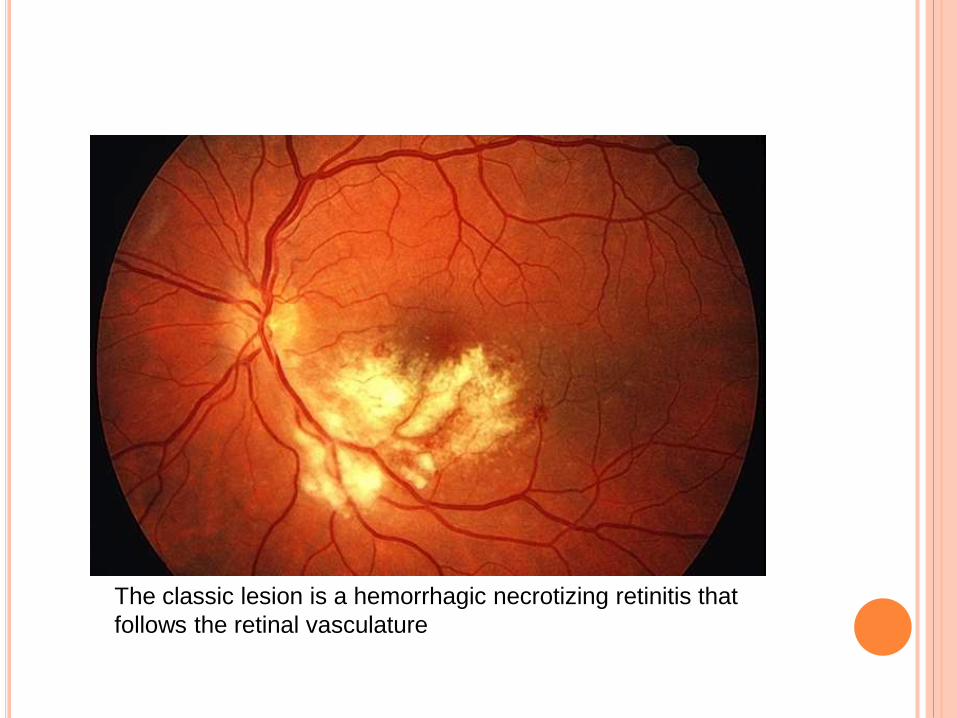
The classic lesion is a hemorrhagic necrotizing retinitis that
follows the retinal vasculature

Fluffy retinal infiltrates and necrosis are associated with scattered
hemorrhages, this creates what has been called the "scrambled eggs and
ketchup“or ‘pizza pie appearance of severe CMVR
TREATMENT
Oral Valganciclovir.
Oral ,Intravenous, and Intravitreal ganciclovir.
Intravenous and Intravitreal Foscarnet or
combined intravenous Ganciclovir and Foscarnet
Intravenous Cidofovir
Inhibiting CMV DNA polymerase.
CYTOMEGALOVIRUS RETINITIS
Valganciclovir is the drug of choice for the
treatment of CMV retinitis.
Induction is 900 mg twice a day and then 900 mg
once a day for maintenance.
For ganciclovir, start induction with 5 mg/kg IV
every 12 hours for 14 days, then change to a
maintenance IV dose of 5 mg/kg/day for 7 days.
myelosuppression
CYTOMEGALOVIRUS RETINITIS
Foscarnet
Induction with 60 mg/kg IV every 8 hours for 14
days.
Maintenance IV dose of 90-120 mg/kg/day.
Hydration with 1000 mL of isotonic sodium
chloride solution is recommended because of
renal toxicity associated with foscarnet.
CYTOMEGALOVIRUS RETINITIS
Cidofovir
Induction dose - 5 mg/kg IV over 1 hour once
weekly for 2 weeks.
Maintenance dose - 5 mg/kg over 1 hour once
every other week.
Renal toxicity, Iritis and Ocular hypotony.
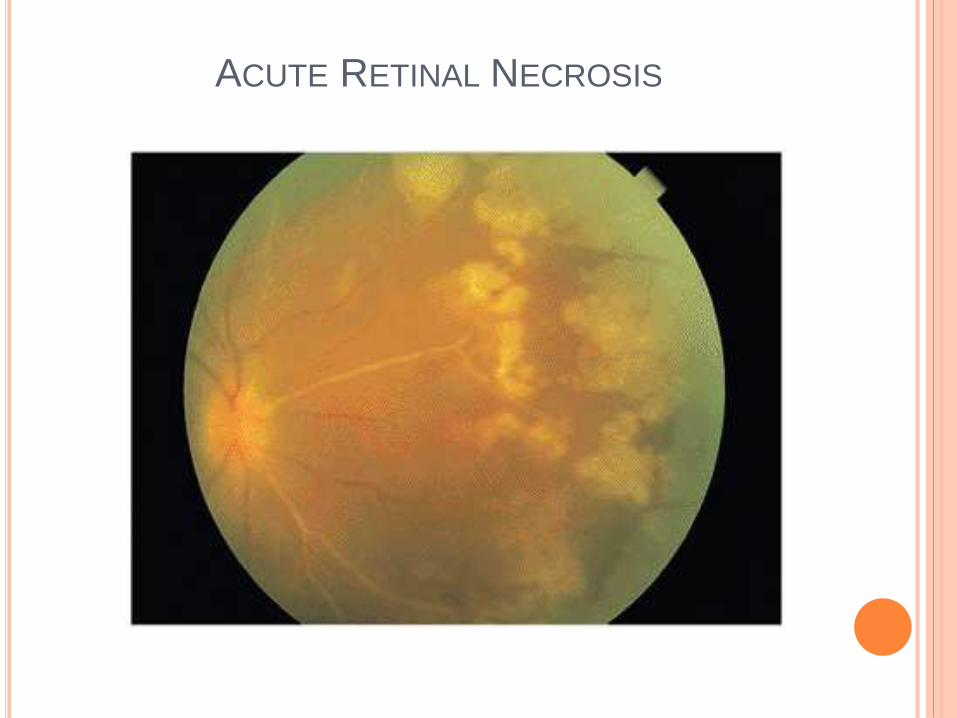
ACUTE RETINAL NECROSIS
It is a fulminant retinal vaso-occlusive necrotizing
retinitis , usually due to Varicella-Zoster infection,
can also be caused by Herpes Simplex virus or
Cytomegalovirus.
The retina shows small, necrotic yellowish lesions in
the periphery, which rapidly spread into a larger
confluent white area, most often involving the entire
peripheral retina, and then progress toward the
posterior pole.
Optic neuritis and retinal detachment are frequent complications.
ACUTE RETINAL NECROSIS
ACUTE RETINAL NECROSIS
Acute retinal necrosis (ARN) frequently is
complicated by anterior uveitis, retinal and
choroidal vasculitis, vitritis, and papillitis.
Episcleritis, scleritis, or optic neuropathy.
are treated with high doses of intravenous
aciclovir or famciclovir, combined with laser
treatment to prevent retinal detachment
PROGRESSIVE OUTER RETINAL NECROSIS
(VARICELLA-ZOSTER RETINITIS)
It is is a rapidly progressive, necrotizing retinitis
caused by Varicella Zoster virus, without vitritis
or retinal vasculitis.
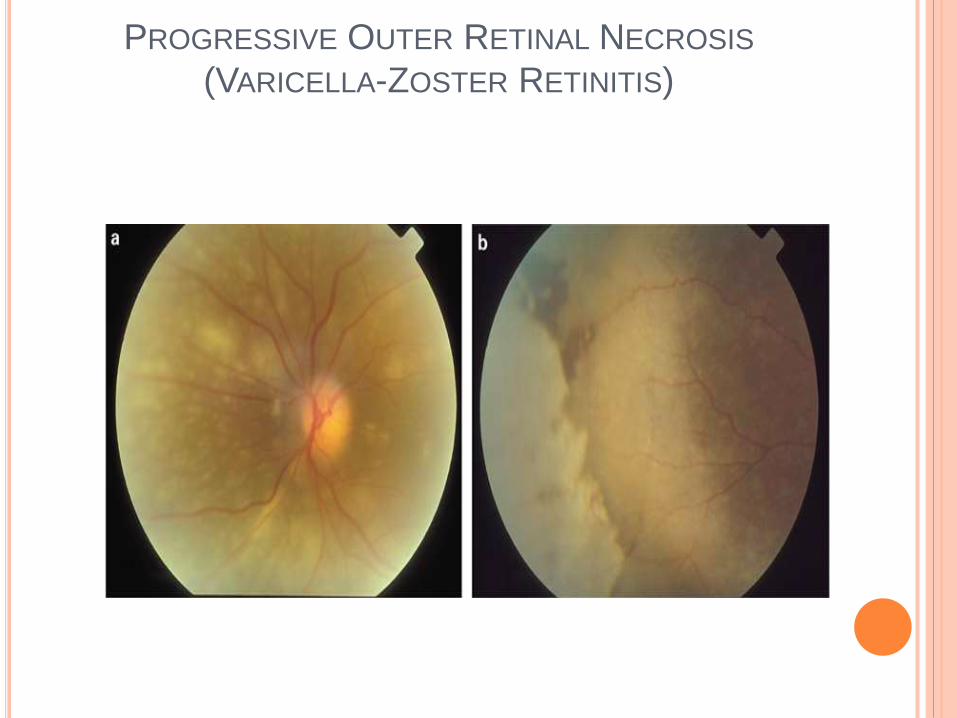
The retina shows typically a white lesion
(multifocal, deep to the retina, opaque, and
patchy) with no haemorrhages or exudates.
Typically, the lesions start from the posterior
pole and spread with extreme rapidity to involve
the entire retina.

PROGRESSIVE OUTER RETINAL NECROSIS
(VARICELLA-ZOSTER RETINITIS)
PROGRESSIVE OUTER RETINAL NECROSIS
(VARICELLA-ZOSTER RETINITIS)
PROGRESSIVE OUTER RETINAL NECROSIS
Treatment is often unsatisfactory and usually
requires combination of Ganciclovir and Aciclovir.
The prognosis is very poor and retinal
detachment is common.
TUBERCULOSIS
The most common ocular manifestation is
anterior uveitis and disseminated choroiditis.
Manifests as areas of necrosis surrounded by
mononuclear and giant cells.
unifocal or multifocal yellowish, grayish, or
whitish choroiditis, mostly in the posterior pole.

Patients should be given isoniazid (INH) 300 mg
orally daily, rifampin 600 mg orally daily, and
pyrazinamide 25-35 mg/kg orally daily for 2 months;
then, continue with INH and rifampin for an
additional 7 months.
Drug resistance is most common with streptomycin
and INH; however, this may be minimized by the
use of multiple bactericidal antituberculous drugs.
Pyridoxine 25 mg orally daily usually is added to the
regimen to prevent peripheral neuritis.
TOXOPLASMA RETINOCHOROIDITIS
The usual ocular lesion of toxoplasmosis is a
focal necrotizing retinitis, with white infiltration
and surrounding retinal edema.
Unlike in immunocompetent patients, HIV
infected patients often have bilateral and
multifocal disease associated with anterior
uveitis and vitritis with no pigmented scars
adjacent to the areas of retinal necrosis.
Toxoplasmosis in immunocompromised patients
is not self-limiting as it is in imunocompetent
patients.
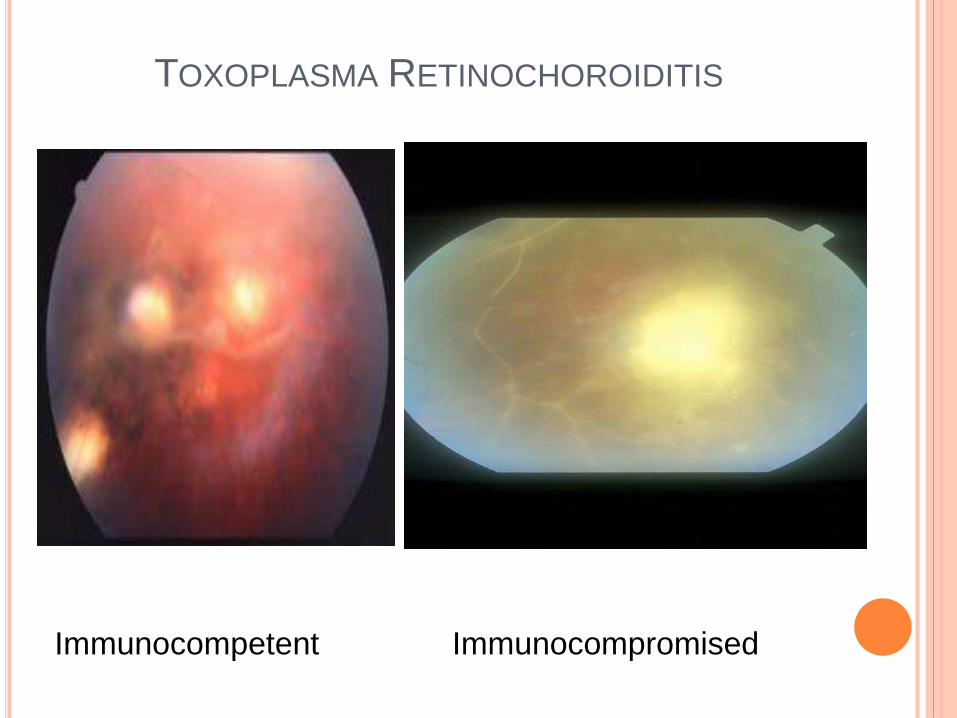
TOXOPLASMA RETINOCHOROIDITIS
Immunocompetent Immunocompromised
TOXOPLASMA RETINOCHOROIDITIS
For active retinochoroiditis within 2-3 mm of the
disc or fovea, which threatens vision, or peripheral
lesion associated with severe vitritis, start first-line
therapy for 3-6 weeks, as follows:
(1) pyrimethamine 75 mg PO load,25 mg PO twice
daily, plus,
(2) folinic acid 3-5 mg PO twice weekly (to reduce
the adverse effect of bone marrow toxicity of
pyrimethamine), and
(3) sulfadiazine 2 g PO load, then 1 g PO 4 times
daily.
D) NEURO-OPHTHALMOLOGIC
MANIFESTATIONS
10-15% of patients who are infected with HIV
common causes of neuro-ophthalmologic
manifestations include
Meningitis,
Meningeal and Parenchymal Lymphoma,
Neurosyphilis, and
Toxoplasmosis.
Neuro-ophthalmologic manifestations include
Papilledema due to increased intracranial
pressure.
Optic neuritis,
Cranial nerve palsies,
Ocular motility disorders, and
Visual field defects
TREATMENT
Radiation and Chemotherapy for Lymphoma
Specific antibiotics for Infectious causes
Systemic steroids are indicated in severe cases of
optic neuritis (high dose, short course).
E) ORBITAL MANIFESTATIONS
The most common complications include
Orbital lymphoma,
Orbital cellulitis due to Aspergillus infection and
Orbital Kaposi's sarcoma
Lymphomas are treated with radiation and
chemotherapy, whereas orbital cellulitis is
amenable to systemic antibiotics.

F) OCULAR MANIFESTATION OF HIV
INFECTION IN CHILDREN
Fewer ocular manifestations of HIV infection
and an especially low incidence of CMV retinitis.
The reason for this difference is unknown, but
may relate to an altered immune response to HIV
or a lower prevalence of CMV seropositivity in
children.
HIV-infected children are, however, at increased
risk for neurodevelopmental delay, a condition
often associated with neuro-ophthalmic
complications.

A fetal AIDS-associated embryopathy,
with downward obliquity of the eyes,
prominent palpebral fissures,
hypertelorism, and
blue sclerae, has also been described

G) OCULAR TOXICITY OF ANTIRETROVIRAL
DRUGS
Rifabutin- intraocular inflammation uveitis- 33%
Cidofovir- uveitis and intraocular hypotony - 25- 30%
Didanosine- retinal pigment epithelial abnormalities;
mottling and hypertrophy accompanied by overall
decreased retinal function .
Gancyclovir & Acyclovir- corneal epithelial inclusion
termed corneal lipidosis.
Lastly, long-term Atovaquone can corneal subepithelial
deposits.
These adverse effects are dose related and resolve
following discontinuation of the drug, with the exception
of the abnormal retinal pigment epithelial changes.
THANK YOU
Related Documents











