"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal Dr. Pranav Nursing Academy 67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019 Mob: 9928080456, 7849875744 Page 1 Chapter 1 BASICS OF REPRODUCTION GERM Cell and its Differentiation: Germ cell dk fuekZ .k Epiblast ;k Yolk Sac ds Ectoderm ls gksrk gS A SRY Gene (Sex determining Region Present on Y Chromosome) Present Absent Spermatogonia Oogonia GERM CELL DIFFERENTIATION: 1) SPERMATOGENESIS: Primordial Germ Cell ds }kjk Spermatid dk fuekZ .k rFkk Spermatids dk Spermatozoa ¼;k Sperm½ esa differentiation spermatogenesis dgykrk gS A Spermatogenesis Puberty ds le; Males esa Testis dh Seminiferous tubules esa Start gksrk gS A Complete Spermatogenesis esa yxHkx 72&74 fnu dk le; yxrk gS A Spermatogonia Enlarge, Mature (Mitosis) Primary Spermatocyte (2n) 1 st Meiotic Division (n) (n) Secondary Spermatocyte (2 in No.) Spermatids (4 in No.) Undergo transformation Spermiogenesis Sperms (4 in No.) ,d spermatgonia ls yxHkx 16 primary spermatocytes dk fuekZ .k gksrk gS A 44 + X Y 44 + X Y 22 + X 22 + Y 22 + Y 22 + X 22 + X 22 + Y

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 1
Chapter 1
BASICS OF REPRODUCTION GERM Cell and its Differentiation:
Germ cell dk fuekZ.k Epiblast ;k Yolk Sac ds Ectoderm ls gksrk gSA
SRY Gene (Sex determining Region Present on Y Chromosome)
Present Absent
Spermatogonia Oogonia
GERM CELL DIFFERENTIATION:
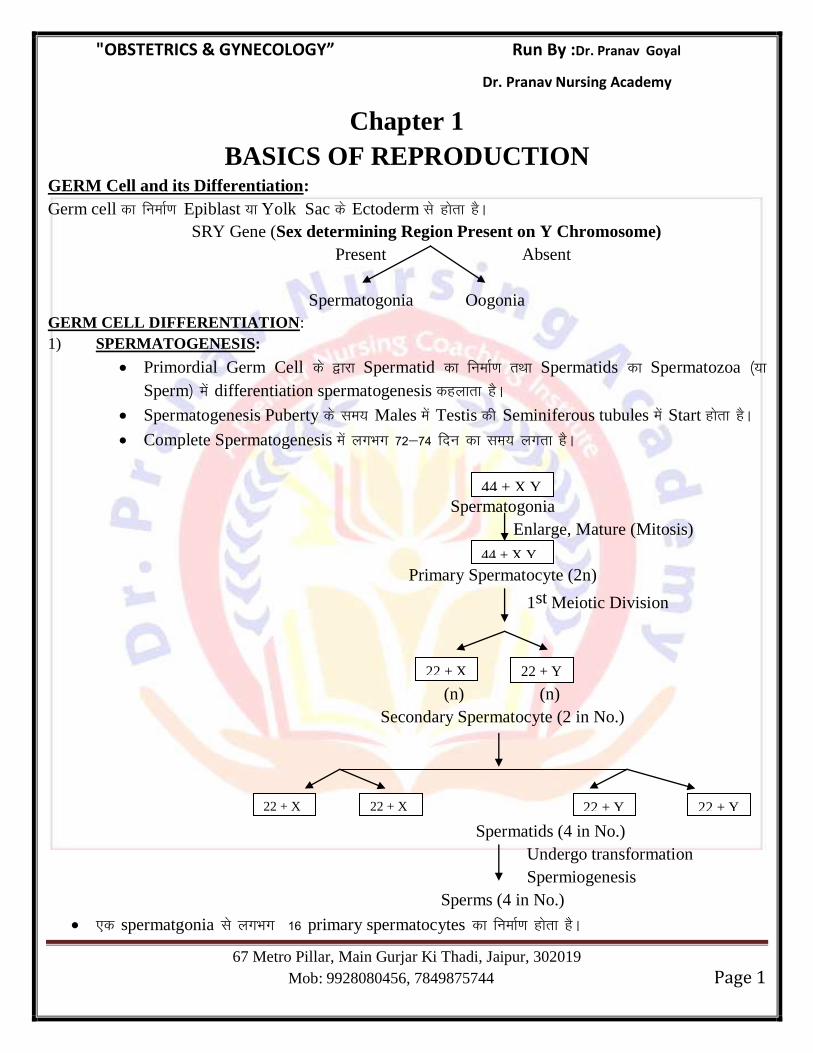
1) SPERMATOGENESIS:
Primordial Germ Cell ds }kjk Spermatid dk fuekZ.k rFkk Spermatids dk Spermatozoa ¼;k
Sperm½ esa differentiation spermatogenesis dgykrk gSA
Spermatogenesis Puberty ds le; Males esa Testis dh Seminiferous tubules esa Start gksrk gSA
Complete Spermatogenesis esa yxHkx 72&74 fnu dk le; yxrk gSA
Spermatogonia
Enlarge, Mature (Mitosis)
Primary Spermatocyte (2n)
1st Meiotic Division
(n) (n)
Secondary Spermatocyte (2 in No.)
Spermatids (4 in No.)
Undergo transformation
Spermiogenesis
Sperms (4 in No.)
,d spermatgonia ls yxHkx 16 primary spermatocytes dk fuekZ.k gksrk gSA
44 + X Y
44 + X Y
22 + X 22 + Y
22 + Y 22 + X 22 + X 22 + Y
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 2
,d primary spermatocyte ls 4 sperms dk fuekZ.k gksrk gSA
vFkkZr~ ,d spermatogonia ls (16 × 4) = 64 sperms dk fuekZ.k gksrk gSA
Spermatids dk maturation mainly epididymis ds caudal part vFkkZr~ Tail of Epididymis esa gksrk gSA
Sperm dk size - 55 microns
Sperm dk life spam - 72 hours.
Ion Responsible for motility of sperm - Calcium.
SPERMIOGENESIS:
bl process ds }kjk spherical vkdkj dk spermatid longitudinal sperm esa convert gks tkrk gSA
bl process esa fuEu changes gksrs gSa%&
Part of Spermatid Part formed in Sperm
Nuclear material Head of Sperm
Golgi Body Acrosomal Cap
Mitochondria Middle Piece
Microtubules / Centrioles Axial Filament / Tail of Sperm.
Sperm esa Rough Endoplasmic Reticulum ugha ik;k tkrk gSA
Spermiogenesis esa yxHkx 14 days dk le; yxrk gSA
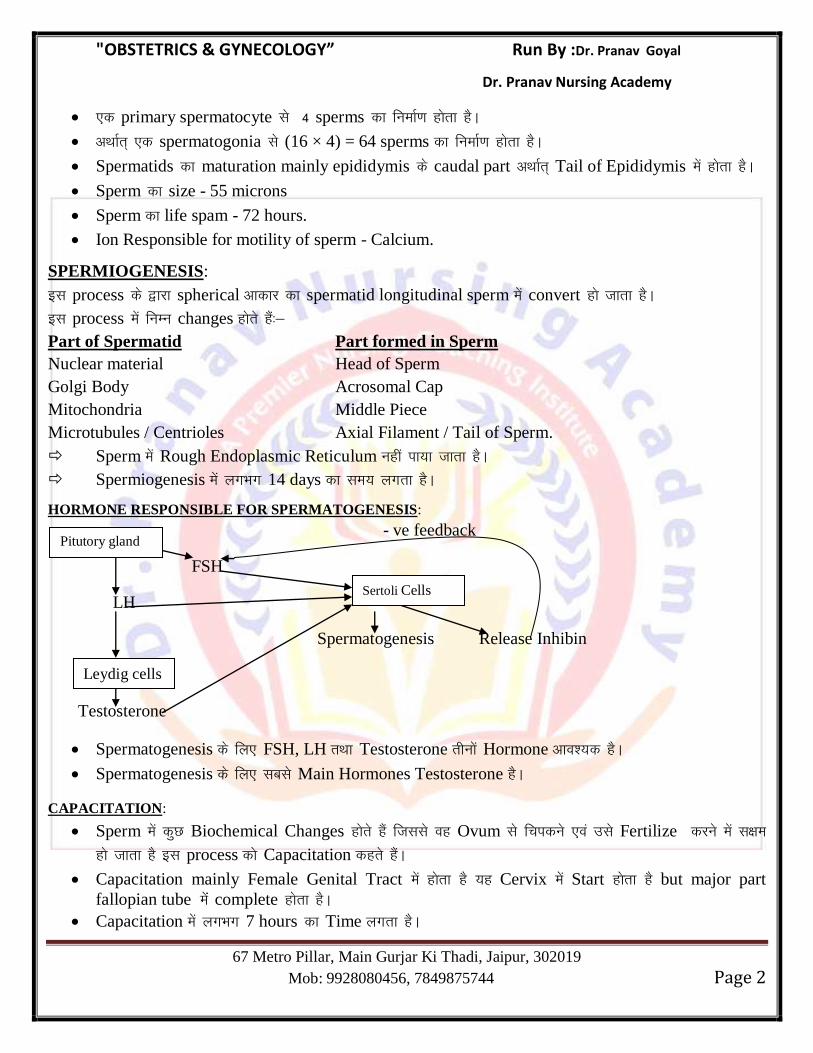
HORMONE RESPONSIBLE FOR SPERMATOGENESIS:
- ve feedback
FSH
LH
Spermatogenesis Release Inhibin
Testosterone
Spermatogenesis ds fy, FSH, LH rFkk Testosterone rhuksa Hormone vko’;d gSA
Spermatogenesis ds fy, lcls Main Hormones Testosterone gSA
CAPACITATION:
Sperm esa dqN Biochemical Changes gksrs gSa ftlls og Ovum ls fpidus ,oa mls Fertilize djus esa l{ke
gks tkrk gS bl process dks Capacitation dgrs gSaA
Capacitation mainly Female Genital Tract esa gksrk gS ;g Cervix esa Start gksrk gS but major part
fallopian tube eaas complete gksrk gSA
Capacitation esa yxHkx 7 hours dk Time yxrk gSA
Pitutory gland
Leydig cells
Sertoli Cells
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 3
Capacitation ds ckn sperm iwjh rjg ls Mature rFkk Hypermobile gks tkrk gSA
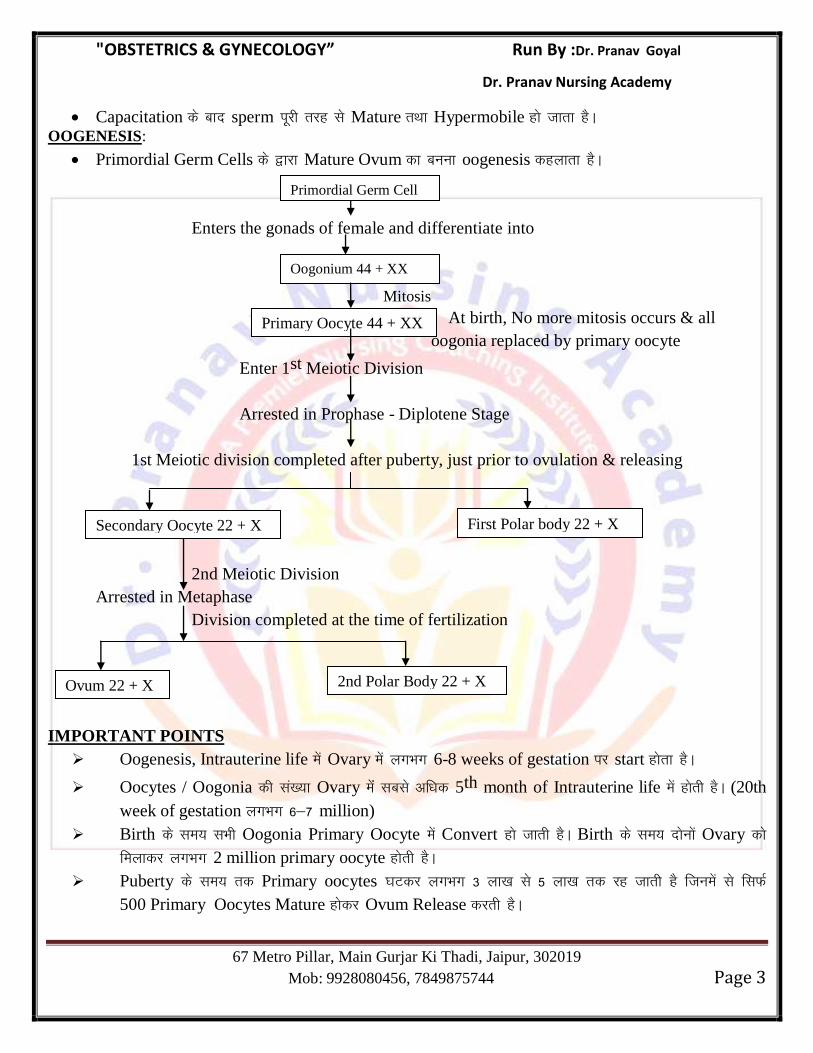
OOGENESIS:
Primordial Germ Cells ds }kjk Mature Ovum dk cuuk oogenesis dgykrk gSA
Enters the gonads of female and differentiate into
Mitosis
At birth, No more mitosis occurs & all
oogonia replaced by primary oocyte
Enter 1st Meiotic Division
Arrested in Prophase - Diplotene Stage
1st Meiotic division completed after puberty, just prior to ovulation & releasing
2nd Meiotic Division
Arrested in Metaphase
Division completed at the time of fertilization
IMPORTANT POINTS
Oogenesis, Intrauterine life esa Ovary esa yxHkx 6-8 weeks of gestation ij start gksrk gSA
Oocytes / Oogonia dh la[;k Ovary eaas lcls vf/kd 5th month of Intrauterine life esa gksrh gSA (20th
week of gestation yxHkx 6&7 million)
Birth ds le; lHkh Oogonia Primary Oocyte esa Convert gks tkrh gSA Birth ds le; nksuksa Ovary dks
feykdj yxHkx 2 million primary oocyte gksrh gSA
Puberty ds le; rd Primary oocytes ?kVdj yxHkx 3 yk[k ls 5 yk[k rd jg tkrh gS ftuesa ls flQZ
500 Primary Oocytes Mature gksdj Ovum Release djrh gSA
Primordial Germ Cell
Oogonium 44 + XX
Primary Oocyte 44 + XX
First Polar body 22 + X Secondary Oocyte 22 + X
Ovum 22 + X 2nd Polar Body 22 + X
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 4
Birth ds le; lHkh Primary Oocyte esa Growth, Diplotene Stage of Prophase esa Arrest gks tkrh gS
tks fd Meiosis Division dh ,d stage gSA
Ovary esa Primary Oocyte pkjksa vksj ls Follicular cells }kjk f?kjk gksrk gS ftls Primordial Follicle
dgrs gSaA
Puberty ds le; Mid Cycle Preovulutory Surge gksrk gS (LH Surge) ftlls Meiosis iqu% Start gksrk
gS rFkk Ovulution ds Just igys Complete gksrk gS vFkkZr~ Meiosis-I ,d Hormonal Dependent
Process gS tks fd LH Hormone ij depend gksrk gSA
Primary Oocyte ls Secondary Oocyte dk cuuk Ovulution dgykrk gSA
Secondary oocyte cuus ds ckn immediate 2nd Meiotic Division Start gksrk gS यह
metaphase stage arrest ह ह A Fertilization स य 2
nd meiotic division complete ह ह 2nd
polar body ovum
release ह ह A Size of Mature Ovum - 120 - 130 Micron (Largest cell in Body)
Life Spam of Ovum - 12-24 hours.
FERTILIZATION:
Fertilization ,d Process gS ftlds }kjk Male Pronucleus ,oa Female Pronucleus vkil esa feydj
Zygote cukrs gSaA
Fertilization Fallopian Tube ds Ampula okys Part esa gksrk gSA
Male rFkk Female Pronucleus ds Fusion ds fy;s Fertilin uked Gene Responsible gksrk gSA
Fertilization ds ckn Zygote Fallopian Tube esa 3 fnu rd jgrk gS rFkk blesa Cell Division gksrk jgrk gSA
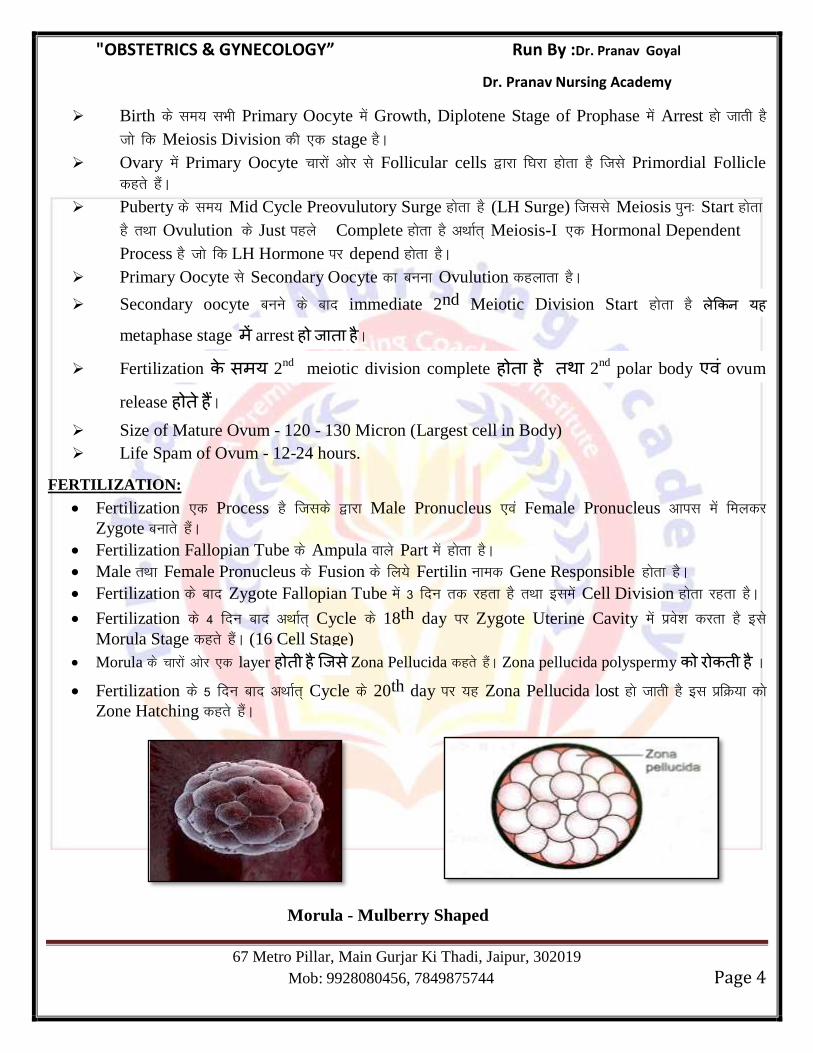
Fertilization ds 4 fnu ckn vFkkZr~ Cycle ds 18th day ij Zygote Uterine Cavity esa izos’k djrk gS bls
Morula Stage dgrs gSaA (16 Cell Stage)
Morula ds pkjksa vksj ,d layer ह ह स Zona Pellucida dgrs gSaA Zona pellucida polyspermy ह A Fertilization ds 5 fnu ckn vFkkZr~ Cycle ds 20th day ij ;g Zona Pellucida lost gks tkrh gS bl izfØ;k dks
Zone Hatching dgrs gSaA
Morula - Mulberry Shaped
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 5
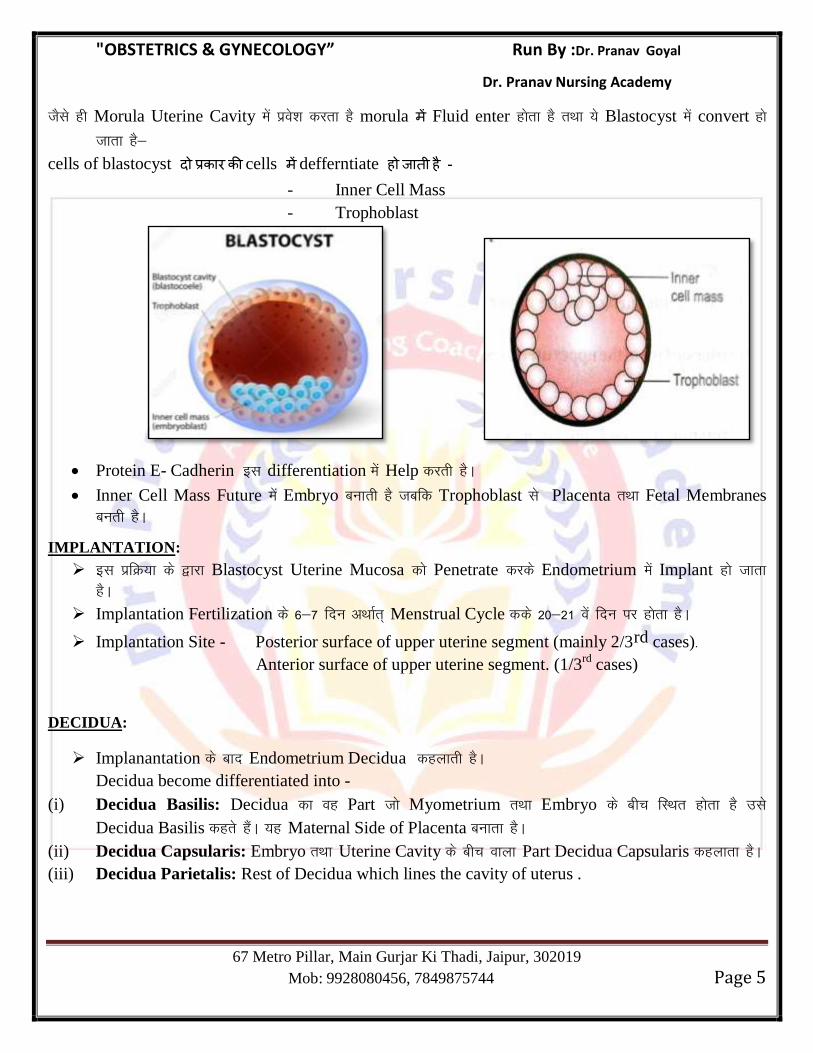
tSls gh Morula Uterine Cavity esa izos’k djrk gS morula Fluid enter gksrk gS rFkk ;s Blastocyst esa convert gks
tkrk gS&
cells of blastocyst cells defferntiate ह ह - - Inner Cell Mass
- Trophoblast
Protein E- Cadherin bl differentiation esa Help djrh gSA
Inner Cell Mass Future esa Embryo cukrh gS tcfd Trophoblast ls Placenta rFkk Fetal Membranes
curh gSA
IMPLANTATION:
bl izfØ;k ds }kjk Blastocyst Uterine Mucosa dks Penetrate djds Endometrium esa Implant gks tkrk
gSA
Implantation Fertilization ds 6&7 fnu vFkkZr~ Menstrual Cycle dds 20&21 osa fnu ij gksrk gSA
Implantation Site - Posterior surface of upper uterine segment (mainly 2/3rd cases)-
Anterior surface of upper uterine segment. (1/3rd
cases)
DECIDUA:
Implanantation ds ckn Endometrium Decidua dgykrh gSA
Decidua become differentiated into -
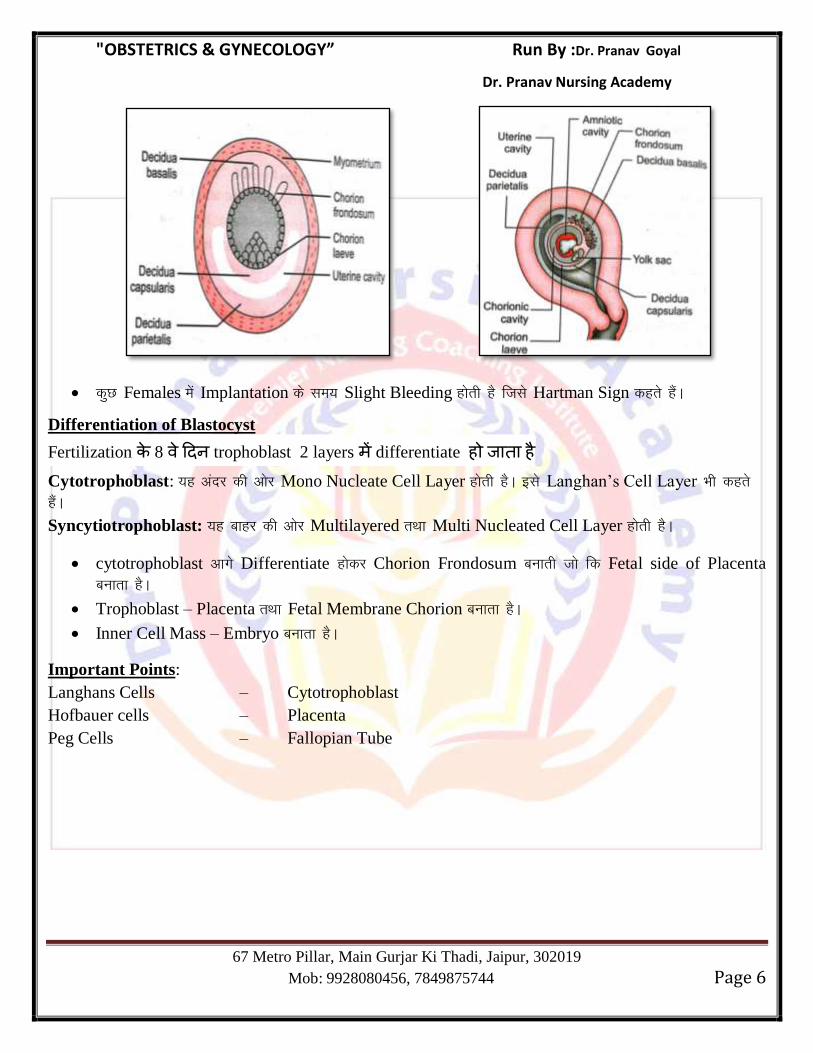
(i) Decidua Basilis: Decidua dk og Part tks Myometrium rFkk Embryo ds chp fLFkr gksrk gS mls
Decidua Basilis dgrs gSaA ;g Maternal Side of Placenta cukrk gSA
(ii) Decidua Capsularis: Embryo rFkk Uterine Cavity ds chp okyk Part Decidua Capsularis dgykrk gSA
(iii) Decidua Parietalis: Rest of Decidua which lines the cavity of uterus .
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 6
dqN Females esa Implantation ds le; Slight Bleeding gksrh gS ftls Hartman Sign dgrs gSaA
Differentiation of Blastocyst
Fertilization 8 trophoblast 2 layers differentiate ह ह Cytotrophoblast: ;g vanj dh vksj Mono Nucleate Cell Layer gksrh gSA bls Langhan‘s Cell Layer Hkh dgrs
gSaA
Syncytiotrophoblast: ;g ckgj dh vksj Multilayered rFkk Multi Nucleated Cell Layer gksrh gSA
cytotrophoblast vkxs Differentiate gksdj Chorion Frondosum cukrh tks fd Fetal side of Placenta
cukrk gSA
Trophoblast – Placenta rFkk Fetal Membrane Chorion cukrk gSA
Inner Cell Mass – Embryo cukrk gSA
Important Points:
Langhans Cells – Cytotrophoblast
Hofbauer cells – Placenta
Peg Cells – Fallopian Tube
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 7
Chapter 2
Placenta, Fetal Membranes, Umbilical Cord and Amniotic Fluid
PLACENTA:
Human Placenta Discoid, Haemochorial & Deciduate gksrk gSA
Discoid – Disc Shaped
Haemochorial – Direct contact of chorion with maternal blood.
Deciduate – Maternal tissue shed at Parturition.
DEVELOPMENT OF PLACENTA:
Placenta dk development nks source ls gksrk gSA
Fetal Part – Chorion Frundosum (Cytotrophoblast)
Maternal Part – Decidua Basilis
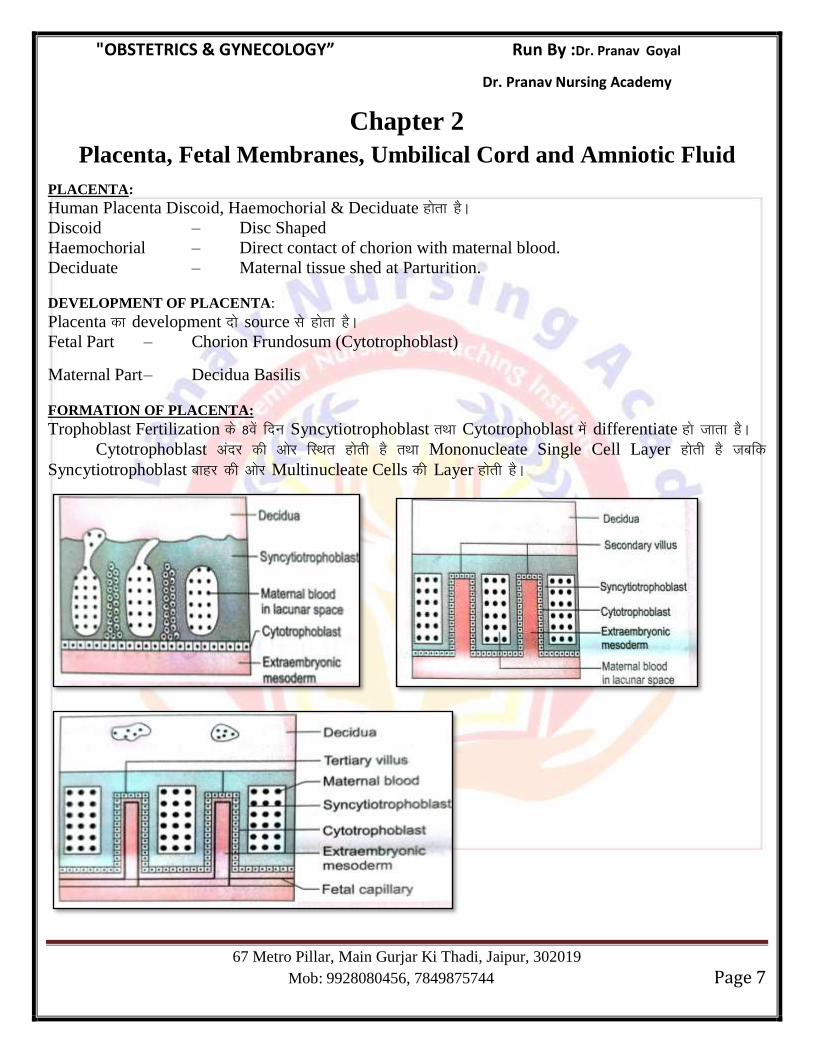
FORMATION OF PLACENTA:
Trophoblast Fertilization ds 8osa fnu Syncytiotrophoblast rFkk Cytotrophoblast esa differentiate gks tkrk gSA
Cytotrophoblast vanj dh vksj fLFkr gksrh gS rFkk Mononucleate Single Cell Layer gksrh gS tcfd
Syncytiotrophoblast ckgj dh vksj Multinucleate Cells dh Layer gksrh gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 8
Cytotrophoblast Mesoderm ds Åij dh vksj fLFkr gksrh gSA
Syncytiotrophoblast esa small cavities cu tkrh gS tks fd Lacunae ह agSA Syncytiotrophoblast Endometrium esa grow djrk gS tSls gh Endometrium eroded gksrh gS dqN
Maternal Blood Vessels Open gks tkrh gSa vkSj Blood Lacunar Space esa Hkj tkrk gSA
’kq:vkr esa izR;sd Trabeulae flQZ Syncytiotrophoblast dh cuh gksrh gS ckn esa Cytotrophoblast dh Cells
foHkkftr gksdj Trabeulae esa grow djrh gS ftls Primary Villi dgrs gSaA
izR;sd Primary Villi ds chp esa Extra Embryonic Mesoderm Invade djrh gS ftls Secondary Villi dgrs
gSaA
izR;sd Secondary Villi ds vanj dh vksj Fetal Blood Vessels grow djrh gS ftls Tertiary Villi dgrs gSaA
Lacunar Space esa Maternal Blood rFkk Fetal Blood vkil esa dHkh ,d nwljs ds Direct Contact esas ugha
gksrs ;s ,d nwljs ls Placental Barrier }kjk Seperate jgrs gSaA
Syncytiotrophoblast
Cytotrophoblast Placental Barrier
Extra Embryonic Mesoderm
Endothelium of Fetal Capillaries
Primary Villi – 13th day after Fertilization
Secondary Villi – 16th day after Fertilization
Tertiary Villi – 21st day after Fertilization
Fetoplacental Circulation Fertilization ds ckn D17 – D21 ij Establish gks tkrk gSA
Maternal Arterial Blood Fertilization ds ckn D15 ij Intervillous Space esa vkrk gSA
Functional Unit of Placenta – Cotyledon.
Term ij Placenta ,d Circular Disc dh rjg gksrk gS ftldk Diameter yxHkx 15–20 Cm rFkk
Thickness yxHkx 3 Cm gksrh gSA
Term ij Placenta dk Weight – 500 gm gksrk gSA
Term ij Ratio of Weight of Placenta & baby. is – 1: 6.
17th week of Gestation ij Placenta ,oa Fetus dk Weight yxHkx cjkcj gksrk gSA
Placenta Uterine wall dk yxHkx 30% Part Cover djrk gSA Mainly ;g yxHkx 2/3rd Cases esa Uterus
dh Posterior Wall ls Attach gksrk gS tcfd 1/3rd cases esa Uterus dh Anterior Wall ls Attach gksrk gSA
Term ij Placenta dk yxHkx 4/5 Part Fetal Origin dk gksrk gS tcfd Only 1/5 Part Maternal Origin
dk gksrk gSA
Nitabuch’s Membrane: ;g Outer Syncytiotrophoblast ds ckgj dh vksj Fibrinoid Material dh ,d Layer
gksrh gS tks fd Trophoblast dks vkxs Decidua esa Invasion ls jksdrh gSA
Nitabuch‘s Membrane ds Absence esa Placenta Accreta, Increta rFkk Percreta dh laHkkouk c<+ tkrh gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 9
Fetal Fibronectin (FFN):- bls Trophoblast glue Hkh dgrs gSaA ;g Protein mainly Trophoblast dss Maternal
Decidua esa Migration ds fy;s vko’;d gksrh gSA
Fetal Fibronectin (FFN) ds Cervical ;k Vaginal Fluid esa Preterm Labour ;k PROM dks Indicate
djrh gSA
Placenta dk fuekZ.k 6 week ls start gksrk gS tks fd yxHkx 14 – 15 week ij Complete gksrk gSA USG esa
Placenta dks yxHkx 10 weeks ij ns[kk tk ldrk gSA
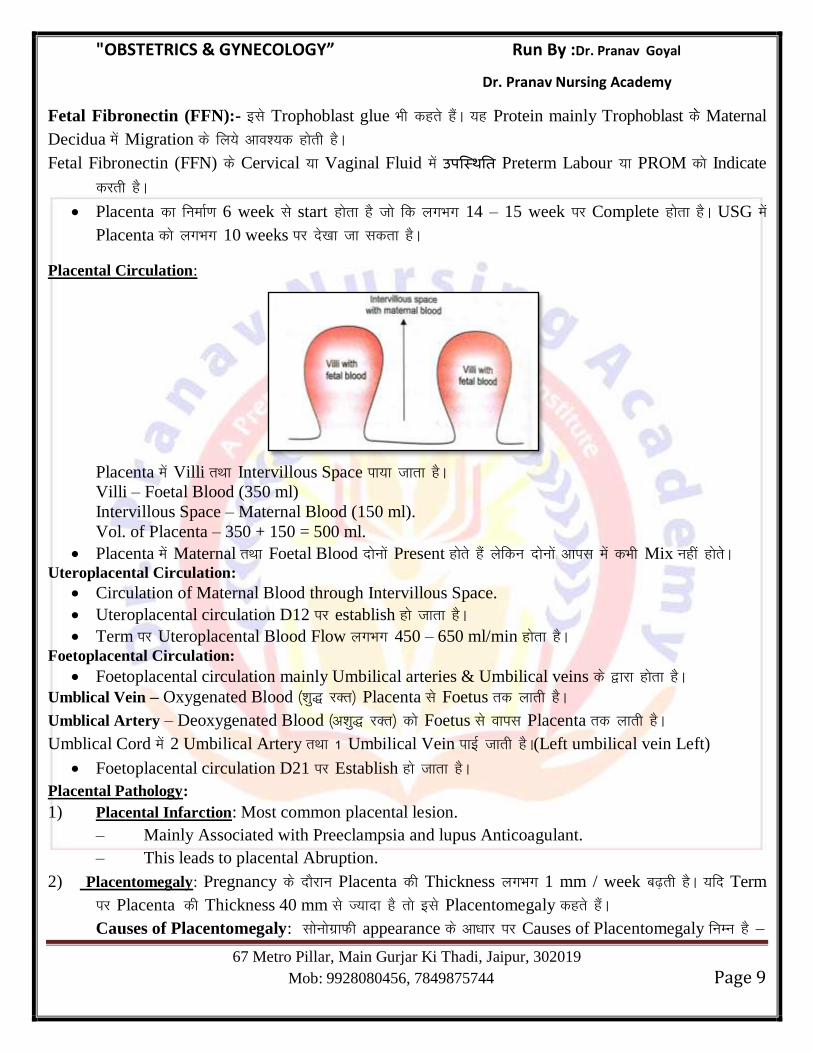
Placental Circulation:
Placenta esa Villi rFkk Intervillous Space ik;k tkrk gSA
Villi – Foetal Blood (350 ml)
Intervillous Space – Maternal Blood (150 ml).
Vol. of Placenta – 350 + 150 = 500 ml.
Placenta esa Maternal rFkk Foetal Blood nksuksa Present gksrs gSa ysfdu nksukas vkil esa dHkh Mix ugha gksrsA Uteroplacental Circulation:
Circulation of Maternal Blood through Intervillous Space.
Uteroplacental circulation D12 ij establish gks tkrk gSA
Term ij Uteroplacental Blood Flow yxHkx 450 – 650 ml/min gksrk gSA Foetoplacental Circulation:
Foetoplacental circulation mainly Umbilical arteries & Umbilical veins ds }kjk gksrk gSA
Umblical Vein – Oxygenated Blood ¼’kq) jDr½ Placenta ls Foetus rd ykrh gSA
Umblical Artery – Deoxygenated Blood ¼v’kq) jDr½ dks Foetus ls okil Placenta rd ykrh gSA
Umblical Cord esa 2 Umbilical Artery rFkk 1 Umbilical Vein ikbZ tkrh gSA(Left umbilical vein Left)
Foetoplacental circulation D21 ij Establish gks tkrk gSA
Placental Pathology:
1) Placental Infarction: Most common placental lesion.
– Mainly Associated with Preeclampsia and lupus Anticoagulant.
– This leads to placental Abruption.
2) Placentomegaly: Pregnancy ds nkSjku Placenta dh Thickness yxHkx 1 mm / week c<+rh gSA ;fn Term
ij Placenta dh Thickness 40 mm ls T;knk gS rks bls Placentomegaly dgrs gSaA
Causes of Placentomegaly: lksuksxzkQh appearance ds vk/kkj ij Causes of Placentomegaly fuEu gS &
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 10
Causes of Homogeneous Placental Thickening:
Diabetes Mallitus or Gestational Diabetes
Anemia
Hydrops Foetalis
TORCH Infection
Aneuploidy
Causes of Heterogeneous Placental Thickening:
Intraplacental Haemorrhage.
3) Small Placenta:
Postdatism
IUGR
Placental Infarction.
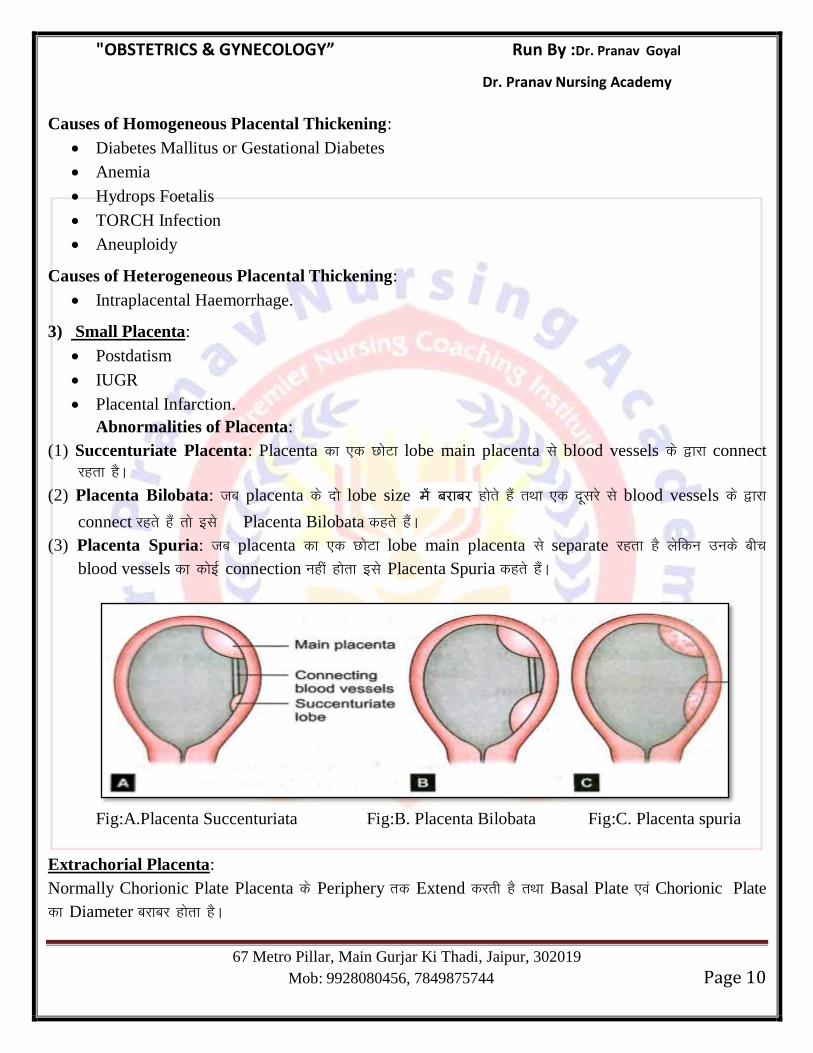
Abnormalities of Placenta:
(1) Succenturiate Placenta: Placenta dk ,d NksVk lobe main placenta ls blood vessels ds }kjk connect
jgrk gSA
(2) Placenta Bilobata: tc placenta ds nks lobe size gksrs gSa rFkk ,d nwljs ls blood vessels ds }kjk
connect jgrs gSa rks bls Placenta Bilobata dgrs gSaA
(3) Placenta Spuria: tc placenta dk ,d NksVk lobe main placenta ls separate jgrk gS ysfdu muds chp
blood vessels dk dksbZ connection ugha gksrk bls Placenta Spuria dgrs gSaA
Fig:A.Placenta Succenturiata Fig:B. Placenta Bilobata Fig:C. Placenta spuria
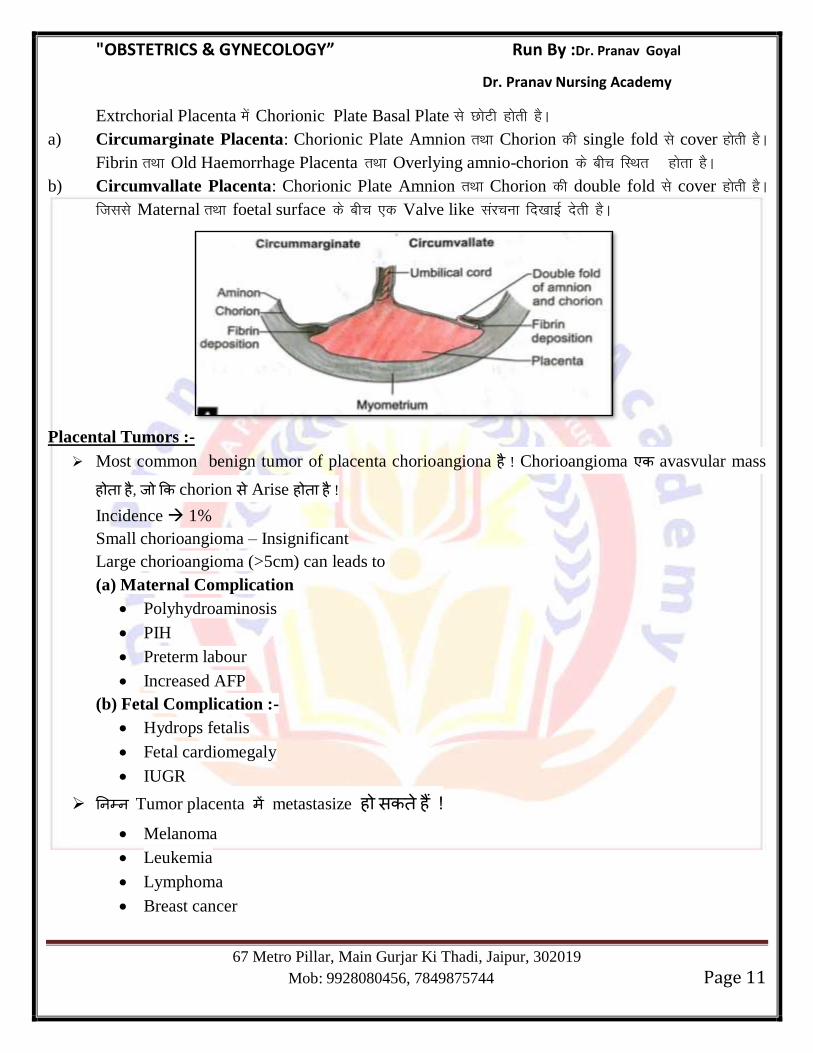
Extrachorial Placenta:
Normally Chorionic Plate Placenta ds Periphery rd Extend djrh gS rFkk Basal Plate ,oa Chorionic Plate
dk Diameter cjkcj gksrk gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 11
Extrchorial Placenta esa Chorionic Plate Basal Plate ls NksVh gksrh gSA
a) Circumarginate Placenta: Chorionic Plate Amnion rFkk Chorion dh single fold ls cover gksrh gSA
Fibrin rFkk Old Haemorrhage Placenta rFkk Overlying amnio-chorion ds chp fLFkr gksrk gSA
b) Circumvallate Placenta: Chorionic Plate Amnion rFkk Chorion dh double fold ls cover gksrh gSA
ftlls Maternal rFkk foetal surface ds chp ,d Valve like lajpuk fn[kkbZ nsrh gSA
Placental Tumors :-
Most common benign tumor of placenta chorioangiona ह ! Chorioangioma avasvular mass
ह ह , chorion स Arise ह ह ! Incidence 1%
Small chorioangioma – Insignificant
Large chorioangioma (>5cm) can leads to
(a) Maternal Complication
Polyhydroaminosis
PIH
Preterm labour
Increased AFP
(b) Fetal Complication :-
Hydrops fetalis
Fetal cardiomegaly
IUGR
Tumor placenta metastasize ह स ह ! Melanoma
Leukemia
Lymphoma
Breast cancer
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 12
Melanoma स Placental tumor ह , fetus metastasize ह स ह !
Function of Placenta :-
(i) Transfer of gases, nutrients & waste products
Example : Respiratory
Nutritive
Excretomy
Important Points :-
Fetus oxygen delivery गभग 8mL/kg of fetal wt/min हस स ह ह , placental
blood flow achieve ह !(Placental blood flow गभग 400 mL/min ह ह ) Fetus energy main sourse glucose ह ह ! Fetus maternal blood स glucose facilitated diffusion ह ! (Using GLUT-1
& GLUT-3).
Early pregnancy lipid mother स foetus direct transfer ह ह , late pregnancy fetus य lipid synthesis ग ह , स fetus lipid daul origon ह ह !
Water electrolytes simple diffusion transfer ह ह ! (i) Immunological function
(ii) Hormonal function/ Endocrine function
(iii) Enzymatic function
(iv) Barrier function
Hormonal function of placenta :-
Placenta Mainly hormones synthesis ह ह ! 1. Progesterone
2. Estrogen
3. Human placental lactogen (HPL)
4. Human chorionic gonadotropin (HCG)
5. Human chorionic thyrotropin
6. Pregnancy specefic β glycoprotein
7. Pregnancy associated plasma protein A (PAPP-A)
Placenta hormones mainly syncytiotrophoblast य ह ! Progestrone :-
Pregnancy 6-7 weeks progesterone mainly corpus luteum य ह !
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 13
8-10weeks progesterone placenta start ह ह ! Pregnancy maintain स स ह Hormone progesterone ह ह !
Abnormal level of progestrone :-
Low level Ectopic pregnancy
abortion
High level Molar pregnancy
Rh isoimmunization
Estrogen:- Estrogen placenta स भ ह ह य 17-α-hydroxylase enzyme ह स यह C21 steroid use ह ! Fetal adrenal gland DHEA-S ह , सस placenta estradiol estriol ह !
Important Points :-
Most common estrogen during pregnancy Estradiol (E2)
Most specefic estrogen during pregnancy Estriol (E3)
Hormone which can be used as a marker for fetal well being Estriol (E3)
Main product of fetal adrenal gland DHEA-S
Fetal Adrenal Gland :-
Morphologically, functionally and physiologically fetal adrenal gland remarkable
organ ह ! Term foetal adult adrenal gland weight ह ह ! Fetal adrenal gland mainly steroid hormone synthesis ह !
Human placental Lactogen(hPL) :-
स human chorionic somatotropin भ ह ह ! (hCS)
यह mainly syncytiotrophoblast synthesis ह ह ! Function :-
यह maternal lipolysis ह , सस produce ह free fatty acids mother source of
energy ह ! यह Hormone Breast lactation prepare ह ! Note :- hPL Lactation role !
Human chorionic gonadotropin (hCG) :-
यह Glycoprotein hormone ह !
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 14
Human सभ hormones स स य Carbohydrate content hCG य ह hCG 2 sub unit ह -
α-Submit :- Biologically यह FSH, LH TSH ह ह ह ! (Non specefic)
β- Submit :- Unique to hCG (Specefic)
Structurally यह FSH, LH TSH ह ह ह , Functionally यह LH ह ह ह (LH Leutotropic) Corpus luteum maintain help ह !
Half life of hCG 24-36 hrs.
Doubling time 2 days (1.4- 2 days)
यह hormone maternal serum fertilization 8 , menstrual cycle 22
appear ह ह ! Period missed ह ह स स य hCG level 100 IU/L ह ह ! 8-10 weeks गभग (70 days ) hCG level maximum 1,00,000 IU/L ह ह , स
यह ह start ह ह ! 16 weeks स level maximum ह ह , term स level minimum ह ह ! hCG delivery 48 urine स disappear ह ह ! hCG delivery 1-2 weeks maternal serum स disappear ह ह ! hCG abortion 4-6 weeks matrenal serum स disappear ह ह !
hCG ह titre gestational sac TVS (Transvaginal) sonography visible ह ह 1500 IU/L .
HCG ह titre gestational sac TAS (Transabdominal) sonography visible ह ह 6000-
6500 IU/L.
Clinical importance of the measurement of hCG
Increased hCG Decreased hCG
Multi fetal pregnancy Abortion
Gestational trophoblastic disease Trisomy other than down syndrome
Down syndrome Ectopic pregnancy
Underestimated gestational age
Erythroblastasis foetalis
Note :- Ectopic pregnancy hCG level Normal Pregnancy rise ह ह ! Function Of HCG :-
Corpus luteum maintain ह ! hCG, LH hormone stimulate ह , स ह स fetal testis स testosterone release ह ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 15
hCG immunosuppresive ह ह , fetus rejection ह ! hCG uterine muscles relaxation uterine vessels vasodilation ह ! hCG maternal thyroid gland stimulate ह !
Fetal membrane :-
AMNION :- यह Innermost fetal membrane ह ह , यह avascular ह ह ! Amnion smooth muscle cells,
nerves, lymphatic blood vessels ह ह ! यह membrane fertilization 10-11 ह ! CHORION :- यह outer membrane ह ह , easily break ह ह ! यह chorionic leave ह ! यह
memembrane fertilization 8 ह !
UMBILICAL CORD / FUNIS :-
Umblical cord स स ह ह , fetal umbilicus स ह placenta fetal surface
य chorionic plate स ह ह ! Umblical cord connecting stalk स develop ह ह ! Early fetal life umbilical cord 2 arteries 2 veins ह ह , right umbilical vein
disappear ह ह , स left umbilical vein ह ह ,(Left is left) umbilical cord 2
umbilical arteries 1 umbilical vein ह ह ! Umbilical arteries diameter, vein ह ह ! Umbilical cord स amnion cover ह ह , chorion absent ह ह ! Normal PH of umbilical cord 7.2
Structure & Function of umbilical cord :-
Umbilical cord whartons jelly ह ! (Connective tissue of umbilical cord).-mesoderm स derived ह ह !
Normal length of umbilical cord 55 cm
Range 30-100 cm
If < 30 cm Short cord
If > 100 cm Long cord
Umbilical cord arteries veins folded tortous ह ह , false knot ह ! Umbilical arteries lumen transverse fold ह , ह fold of hoboken ह ह !
Umbilical cord coils ह ! cm umbilical cord coils ह स umbilical coiling
index ह ह USG ह ! Normal coiling index 0.17 coils/cm
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 16
Hypocoiling < 0.07 coils/cm (causes IUD)
Hypercoiling causes IUGR & fetal acidosis
umbilical vein oxygenated blood carry ह umbilical artery deoxygenated blood carry ह !
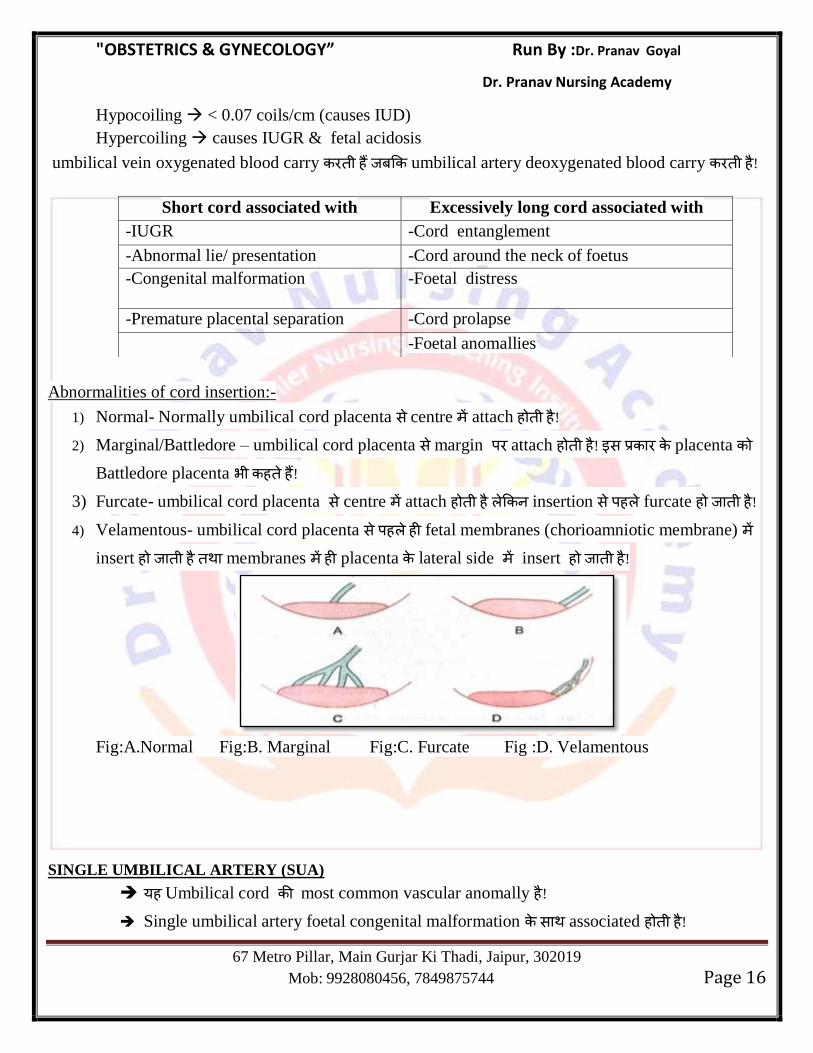
Abnormalities of cord insertion:-
1) Normal- Normally umbilical cord placenta स centre attach ह ह ! 2) Marginal/Battledore – umbilical cord placenta स margin attach ह ह ! स placenta
Battledore placenta भ ह ह ! 3) Furcate- umbilical cord placenta स centre attach ह ह insertion स ह furcate ह ह ! 4) Velamentous- umbilical cord placenta स ह ह fetal membranes (chorioamniotic membrane)
insert ह ह membranes ह placenta lateral side insert ह ह !
Fig:A.Normal Fig:B. Marginal Fig:C. Furcate Fig :D. Velamentous
SINGLE UMBILICAL ARTERY (SUA)
यह Umbilical cord most common vascular anomally ह ! Single umbilical artery foetal congenital malformation स associated ह ह !
Short cord associated with Excessively long cord associated with
-IUGR -Cord entanglement
-Abnormal lie/ presentation -Cord around the neck of foetus
-Congenital malformation -Foetal distress
-Premature placental separation -Cord prolapse
-Foetal anomallies
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 17
Mainly ----- Cardiovascular anomally
----- Renal anomally
Single umbilical artery य isolated finding ह , aneuploidy chances increase ह ह ! य single umbilical artery स other congenital malformation भ ह , aneuploidy
chances increase ह ह स situation amniocentasis य ह !
Most common aneuploidy associated with single umbilical artery- trisomy 18
Single umbilical artery स chances of Abortion,Prematurity ,IUGR Perinatal mortality
ह ! Amniotic Fluid :-
Specefic gravity of amniotic fluid 1-008-1.010.
Osmolality 250 mosm/L
Amniotic fluid completely replaced in 3 hrs.
Rate of amniotic fluid turn over 500 cc/hr.
Amniotic fluid volume maximum 36-38 weeks ह ह (approx 1 litre)
Composition of amniotic fluid :-
Water 98-99%
Solid 1-2%
Organic solid Protein, glucose, lipid, urea, creatinine,Hormone like
prolactin, Insulin &Renin
Inorganic solid Na, K, Cl
Origin of amniotic fluid :- Amniotic fluid mother fetus स ह ह ! In early pregnancy Forming by Ultra filtration of maternal plasma.
By beginning of the 2nd
trimester यह extracellular fluid स ह , fetal skin स secrete
ह ह ! After 20 weeks 20 week skin cornification ह ह , skin स secrete ह
extracellular fluid ह ! स स य amniotic fluid mainly fetal lung ह secretion
fetal urine स ह ! Major contributor Fetal urine
Colour of amniotic fluid:-
Early pregnancy colorless
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 18
Near term Pale straw colour (Due to presence of exfoliated lanugo hair and epidermal cell
from fetal skin)
Abnormal colour of amniotic fluid :-
1. Green (Meconium stained) Fetal distress/ listeria infection
2. Golden yellow Rh incompatibility (Because billirubin levels are increased in amniotic
fluid in case of Rh incompatibility).
3. Greenish yellow Saffron Postmaturity
4. Tobacco juice or Prue juice or Dark brown IUD
5. Dark Marron Concealed hemorrhage
2nd
trimester amniotic fluid fetal urine (approx 1000ml/day) fetal lung
secretion (Approx 350ml/day) ह ह ! Amniotic fluid balance process ह ह ! Fetal swallowing 750ml/day
Intramembranous flow across fetal vessels 400ml/day
Function of amniotic fluid :-
Protect the foetus
यह shock absorber ह ह य ह foetus trauma स ह ! Amniotic fluid temperature maintain ह ! Amniotic fluid amniotic cavity distend ह सस foetus Growth movement
space ह ! Amniotic fluid foetus body parts amniotic sac स adhesion ह स ह !
Important points :- Amniotic fluid foetus nutrition role ह ह !
Amniotic fluid index (AFI):-
Uterine cavity 4 quadrant divide य ह , य quadrant amniotic fluid largest vertical
measurement cm. य ह , quadrant largest vertical distance AFI ह AFI normal value 5-24 cm
AFI < 5 cm Oligohydramnios
AFI > 25 cm Polyhydramnios
Single deepest pocket (SDP) :- स quadrant largest amniotic fluid pocket स umbilical
cord ह ह cm. य ह ! Normal range 2-8 cm
>8cm Polyhydramnios
< 2 cm. Oligohydramnios
Abnormalities of amniotic fluid :-
Oligohydramnios :- amniotic fluid volume 200 ml स ह ! Sonographically oligohydramnios is defined as :-
Absence of amniotic fluid
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 19
Single quadrant maximum vertical diameter < 2cm. स ह ! Amniotic fluid index (AFI) < 5cm.
Causes of oligohydramnios :-
i. Drugs Prostaglandin synthatase inhibitor
ACE inhibitor
ii. IUGR
iii. Leaking of fluid (after amniocentesis/ chorionic villous sampling).
iv. Maternal hypertension/preeclampsia.
v. Post term pregnancy
vi. Premature rupture of membrane
vii. Amnion nodosum
viii. Chromosomal anomalies like triploidy
ix. Renal anomalies of foetus (decrease urine production)
Renal agenesis
Urethral obstruction (posterior urethral valve)
Prune belly syndrome
Bilateral multicystic dysplastic kidney
Important points :- Most common cause of mild oligohydramnios Idiopathic Most common cause of severe oligohydramnios Gross congenital anomaly (Renal anomalies).
Complication of oligohydramnios :-
Fetal complication:-
Amniotic sac amniotic fluid स foetus development space ह ह सस foetus anomaly ह स भ ह ह !
Pulmonary hypoplasia
limb deformities like talipes
Potter face
IUGR
य oligohydramnios late pregnancy ह ह ( organogenesis complete ह ह ) स ह
स cord compression meconium aspiration syndrome ह स ह !
Maternal complication :-
Prolonged labour
Increased chances of cesarean delivery due to malpresentation
Treatment :-
Third trimester य only oligohydramnios ह , foetus normal ह , conservatively manage
य ह !
Oral administration of water amniotic fluid volume increase ह !
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 20
Amnioinfusion (prophylactic and therapeutic) amnioinfusion normal saline amniotic cavity
infuse य ह , सस amniotic fluid volume ह ! Indication of amnioinfusion :-
Treatment of fetal distress
For dilute /Wash Out thick meconium
Renal agenesis
PROM
Note :-
Temperature at which saline is infused 370C.
250 ml Saline गभग 30 minutes infuse य ह ! Infusion स य intrauterine cavity resting pressure 25 mm of Hg स य ह ह ह
Polyhydramnios :- य Amniotic fluid volume 2000 ml (2 litre) स य ह AFI > 25 cm
Single pocket diameter > 8 cm
Grade of polyhydramnios :-
Mild single pocket diameter 8-11cm ह ! Moderate single pocket diameter 12-15 cm ह ! Severe single pocket diameter 16 cm स य ह !
Causes of polyhydramnios :-
Amniotic fluid main contributor fetal urine ह ह , य foetus य urine produce ह , polyhydramnios ह ग , स -
A. Twin/Multifetal pregnancy ( य Foetus ह , य urine produced ह ग ). B. Maternal hyperglycemia/Diabetes
Maternal hyperglycemia Fetal hyperglycemia Fetal polyurea Increased Amniotic fluid
C. Twin to twin transfusion syndrome
Foetus Amniotic fluid swallow ह , सस production of amniotic fluid absorption of
amniotic fluid balance ह ह ! य स भ स Amniotic fluid swallow impaired ह ह , polyhydramnios स भ
ह , स - Cleft lip & Cleft palate
Esophageal atresia/Stenosis
Dudoneal atresia/Stenosis
Bowel obstruction
Anencephaly (Swallowing is decreased + increased transudation of CSF into
Amniotic fluid due to absence of cranial vault )
Other important cause of polyhydramnios :-
Placental Cause:-
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 21
Chorioangioma of placenta
Circumvallate Placenta
Fetal Cause :-
-Hydrops Fetalis
-Rubella, syphilis, toxoplasma infection
-Sacrococcygeal teratoma
-Thalassemia of foetus
Important points :-
Most common cause of mild polyhydramnios Idiopathic
Most common cause of severe polyhydramnios Gross congenital anomaly (Cleft lip & cleft
palate)
Complication :-
Polyhydramnios ह ह स Membrane Overstretching ह ह , सस Premature rupture of
membrane Preterm labour स भ ह ! Abruptio Placenta
PPH
Subinvolution of uterus
Cord prolapse
Malpresentation
Unstable lie
Treatment:-
1. Serial amniocentesis :- 500 ml/lt. Fluid removed (Maximum 1500-2000ml).
2. Indomethacin therapy :- Indomethacin foetal urinary output decrease ह , lung fluid absorption ह !
Dose 1.5-3 mg/Kg/Day
Side effect of indomethacin therapy :-
Premature closure of fetal ductus arteriosus
स Indomethacin therapy 32 weeks stop य ह !
Chapter 3
FETAL PHYSIOLOGY & FETAL CIRCULATION
Landmarks in Fetal development :-
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 22
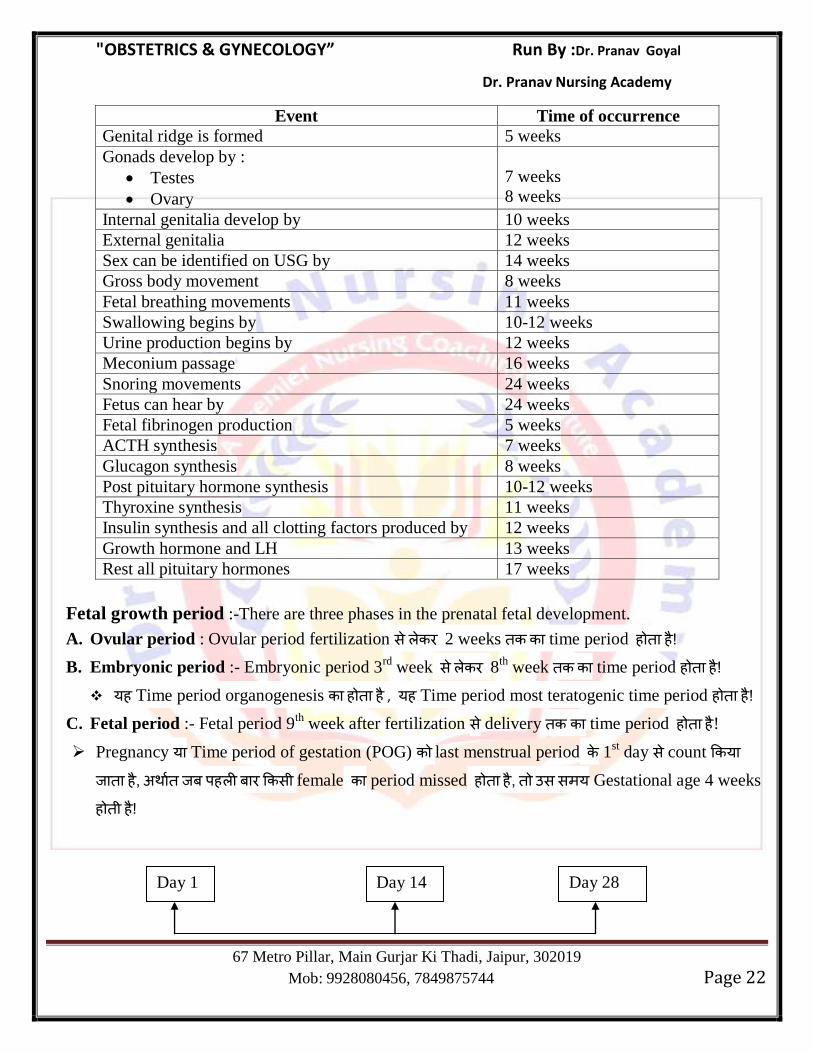
Event Time of occurrence
Genital ridge is formed 5 weeks
Gonads develop by :
Testes
Ovary
7 weeks
8 weeks
Internal genitalia develop by 10 weeks
External genitalia 12 weeks
Sex can be identified on USG by 14 weeks
Gross body movement 8 weeks
Fetal breathing movements 11 weeks
Swallowing begins by 10-12 weeks
Urine production begins by 12 weeks
Meconium passage 16 weeks
Snoring movements 24 weeks
Fetus can hear by 24 weeks
Fetal fibrinogen production 5 weeks
ACTH synthesis 7 weeks
Glucagon synthesis 8 weeks
Post pituitary hormone synthesis 10-12 weeks
Thyroxine synthesis 11 weeks
Insulin synthesis and all clotting factors produced by 12 weeks
Growth hormone and LH 13 weeks
Rest all pituitary hormones 17 weeks
Fetal growth period :-There are three phases in the prenatal fetal development.
A. Ovular period : Ovular period fertilization स 2 weeks time period ह ह ! B. Embryonic period :- Embryonic period 3
rd week स 8
th week time period ह ह !
यह Time period organogenesis ह ह , यह Time period most teratogenic time period ह ह ! C. Fetal period :- Fetal period 9
th week after fertilization स delivery time period ह ह !
Pregnancy य Time period of gestation (POG) last menstrual period 1st day स count य
ह , ह स female period missed ह ह , स स य Gestational age 4 weeks
ह ह !
Day 1 Day 14 Day 28
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 23
1st day of Ovulation Missed
menstrual period Fertilization Period
Pregnancy period यह स calculate य ह !
Pregnancy total duration 10 lunar months य 9 calander months + 7 days य 280 days य 40
weeks ह ह ! यह Time period 1st day of last menstrual period स count य ह , Actual
gestation time period 266 ह ह !
Calculation of EDD (Expected date of delivery) :
EDD calculation Naegele formula ह ! EDD=LMP (1
st day) + 9 month + 7 days
य Leap year ह , (Leap year=29 days in feb. month)
EDD=LMP (1st day) + 9 month + 6 days
Only 4-6% female ह Exact date delivery ह ह ! 50% Females EDD गभग 1 week ह य 1 week Delivery ह ह !
HAASE RULE :-(fetal length calculation)
Up to 5 month:-Fetal length is square of lunar months in centimeters.
From the 6th
month :- Fetal length is 5 times the No. of month.
Fetal Hemopoisis :-
Embryonic life स स ह Hemopoisis yolk sac ह ह ! 6 weeks Hemopoisis liver start ह ह [Mainly HbF (α2β2)].
24 weeks Hemopoisis bone marrow start ह ह , Adult haemoglobin start ह ह [HbA(α2β2)]
Fetal RBC size Adult RBC य ह ह life span ह ह Life span of fetal RBC Approx 80-90 days
At birth :-
Total Hb 16-18 g/dL
Fetal Hb 70-80%
Adult Hb (HbA) 20%
HbA2 5-10%
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 24
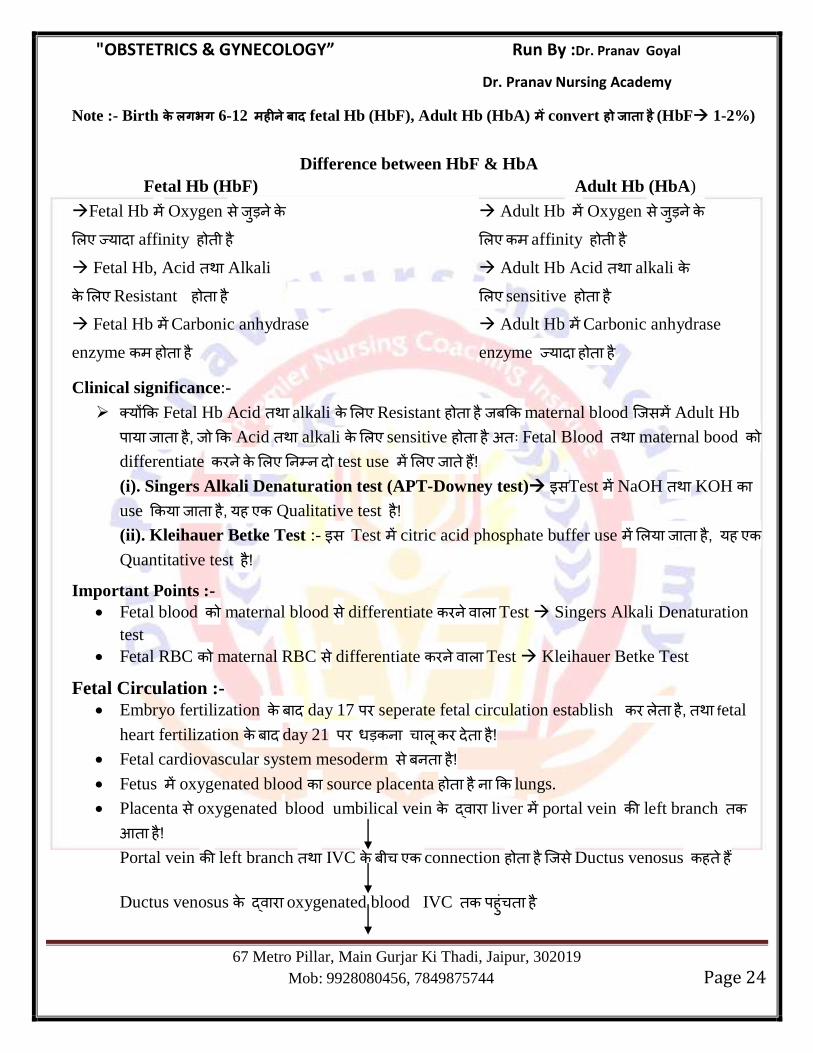
Note :- Birth लगभग 6-12 fetal Hb (HbF), Adult Hb (HbA) convert (HbF 1-2%)
Difference between HbF & HbA
Fetal Hb (HbF) Adult Hb (HbA)
Fetal Hb Oxygen स Adult Hb Oxygen स य affinity ह ह affinity ह ह
Fetal Hb, Acid Alkali Adult Hb Acid alkali Resistant ह ह sensitive ह ह Fetal Hb Carbonic anhydrase Adult Hb Carbonic anhydrase
enzyme ह ह enzyme य ह ह
Clinical significance:-
य Fetal Hb Acid alkali Resistant ह ह maternal blood स Adult Hb
य ह , Acid alkali sensitive ह ह Fetal Blood maternal bood differentiate test use ह ! (i). Singers Alkali Denaturation test (APT-Downey test) सTest NaOH KOH use य ह , यह Qualitative test ह ! (ii). Kleihauer Betke Test :- स Test citric acid phosphate buffer use य ह , यह
Quantitative test ह !
Important Points :-
Fetal blood maternal blood स differentiate Test Singers Alkali Denaturation
test
Fetal RBC maternal RBC स differentiate Test Kleihauer Betke Test
Fetal Circulation :-
Embryo fertilization day 17 seperate fetal circulation establish ह , fetal
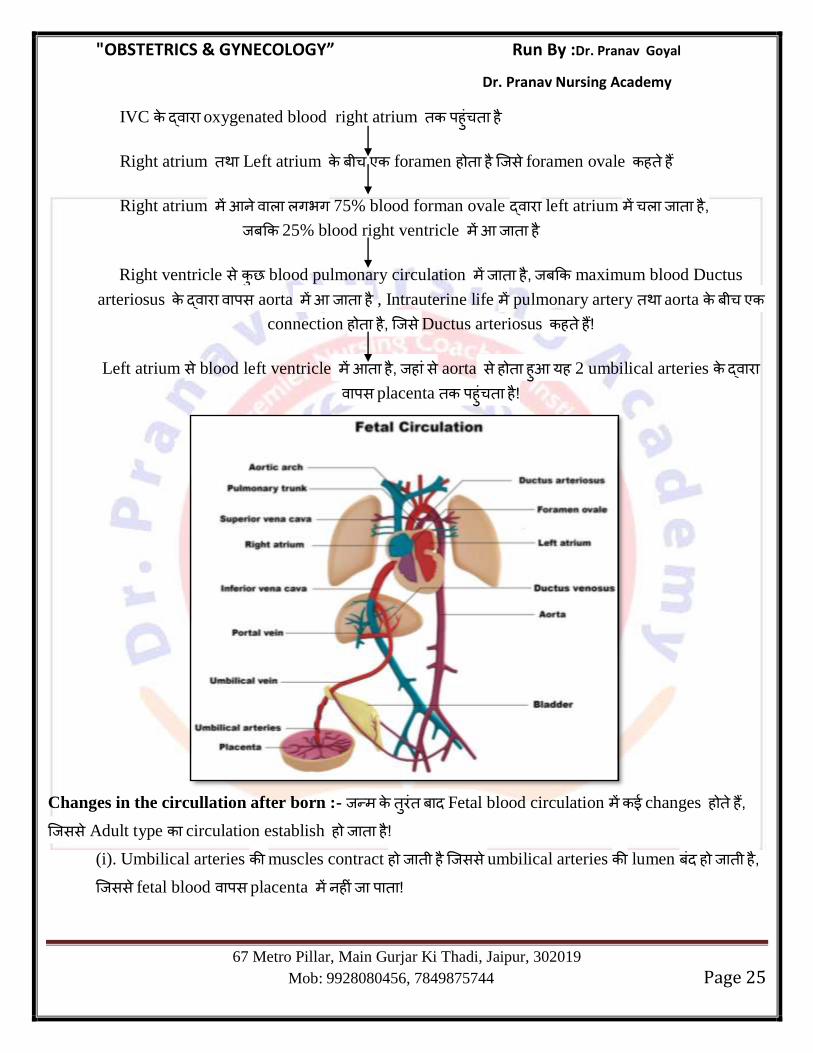
heart fertilization day 21 ह ! Fetal cardiovascular system mesoderm स ह ! Fetus oxygenated blood source placenta ह ह lungs.
Placenta स oxygenated blood umbilical vein liver portal vein left branch
ह ! Portal vein left branch IVC connection ह ह स Ductus venosus ह ह
Ductus venosus oxygenated blood IVC ह ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 25
IVC oxygenated blood right atrium ह ह
Right atrium Left atrium foramen ह ह स foramen ovale ह ह
Right atrium गभग 75% blood forman ovale left atrium ह , 25% blood right ventricle ह
Right ventricle स blood pulmonary circulation ह , maximum blood Ductus
arteriosus स aorta ह , Intrauterine life pulmonary artery aorta
connection ह ह , स Ductus arteriosus ह ह !
Left atrium स blood left ventricle ह , ह स aorta स ह ह यह 2 umbilical arteries स placenta ह ह !
Changes in the circullation after born :- Fetal blood circulation changes ह ह , सस Adult type circulation establish ह ह !
(i). Umbilical arteries muscles contract ह ह सस umbilical arteries lumen ह ह , सस fetal blood स placenta ह !
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 26
(ii). Umbilical vein ductus venosus lumen भ ह ह यह स य ह ह सस , maximum blood स placenta स fetus स ! (iii). Ductus arteriosus भ close ह ह , सस right ventricle blood lungs ह ह blood oxygenation ह ह ! (iv). Pulmonary vessels size increase ह ह सस स blood lung स oxygenation left atrium ह ह left atrium य blood ह ह , सस left atrium pressure
ह स स य right atrium pressure ह ह , य umbilical vein placenta स blood ह ह ! (v). Left atrium pressure right atrium य increase ह ह , सस foramen ovale
close ह ह ! Vessels ह ह , ह fibrous tissue replace ह , ligaments ह !
Vesseles Remnant
Umbilical Arteries Medial umbilical ligament
Left umbilical vein Ligamentum teres of liver
Ductus venosus Ligamentum venosum
Ductus arteriosus Ligamentum arteriosum
Important Points :-
Median umbilical ligaments, Urachus remnant ह ह ! Lateral umbilical ligament, inferior epigastric artery remnant ह ह
Maternal Adaptation in Pregnancy Maternal Adaption in Pregnancy :-
Pregnancy BMR 10-20% increase ह ह ! Pregnancy total retain water 6.5 ltr. ह ह ! Pregnancy Na
+ K+ retention increase ह ह , serum Na
+ K+ value
overall ह ह , य water retention य ह ह ! Pregnancy water retention ह स osmolality decrease ह ह ! Pregnancy Extra calories requirement 350kcal/day ह ह !
Weight Gain During pregnancy:-
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 27
Pregnancy total weight gain 11-12 kg ह ह ! 1
st trimester गभग 1 kg 2nd
& 3rd
trimester 5-5 kg weight increase ह ह ! Mother weight gain maximum 2
nd trimester fetus weight gain maximum 3
rd
trimester ह ह ! Pregnancy mother net weight gain गभग 6kg ह ह !
Note :- smoking व mother weight gain पर अ र smoking mainly fetus weight gain पर अ र ल व IUGR !
Systemic changes in pregnancy
1. Hematological System
Blood volume (30-40%) Decrease hematocit
Plasma volume (40-50%) Decrease packed cell volume
RBC Volume (20-30%) Decrease viscosity of blood
(Plasma RBC
volume increase ह ह Pregnancy hemodilution ह ह ) Decrease platelet count
Hb mass (in gm‘s) य RBC Voume increased ह ह !
WBC count(Neutrophilic leucocytosis) Decrease clotting factor 11 &13
O2 carrying capacity of blood
All clotting factor (Except factor Decrease Hb count ( य plasma
11 & 13) --Pregnancy hyper volume य Increase ह ह !)
coagulable state ह ! S. Fibrinrogen (Clotting factor 1) -- Increases by 50%
ESR (Increase 4 times)
Note :- Pregnancy र Bleeding time and clotting time unaffected र ! 2. Cardiovascular system
Cardial output = Stroke volume X HR Peripheral vascular Resistance( य
Progesterone smooth muscle relaxant ह ह !) Diastolic & Systolic BP (Decrease
Parameter increases in Pregnancy Parameter decreases in Pregnancy
Parameter increases in Pregnancy Parameter decreases in Pregnancy
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 28
in DBP > SBP)
Parameter pregnancy affected ह ह - JVP or central venous pressure
Pulmonary capillary wedge pressure
Pregnancy maximum cardiac output 28-32 week ह ह term यह ह !
Maximum Cardiac output:
Immediate after delivery >2nd
stage of labour>Late 1st satge of labour> 28-32 week> Early 1
st
stage of labour
Pregnancy total plasma protein increase ह ह plasma protein concentration
decrease ह ह !
Respiratory system :
Increase Decrease Unaffected
Tidal Volume Functional residual capacity Respiratory rate
Minute ventilation Expiratory reserve volume Vital Capacity
Inspiratory capacity Residual volume Inspiratory reserve volume
Minute O2 up take Total lung capacity
PCO2 (mild respiratory alkalosis)
Renal System :-
Pregnancy right kideny ureter hydroureteronephrosis ह ह , य uterus dextro rotation स right ureter pressure ह सस right hydroureteronephrosis ह ह
1st & 3
rd trimester urine frequency increase ह ह !
Increase Decrease
Renal Blood flow (+50%) Plasma osmolality
GFR (+50%) S.creatinine
Creatinine clearance S.Uric acid
Glucosuria S. K+,
Na+
S.Cl-
Changes in Iron Metabolism during pregnancy :
Marker Change
Serum iron concentration Decreases
Serum ferritin (reflecting Iron stores) Decreases
Serum total iron binding capacity Increases
Percentage saturation (Serum ferritin/TIBC) Decreases
Serum transferrin Increases
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 29
GIT :-
Pregnancy hCG hormone ह स nausea vomitting ह ह ! Progesterone hormone ह स smooth muscles relax ह ह , सस peristaltic movement
ह ह (constipation) HCl production ह ह !
Changes in genital organ during pregnancy
Vagina :-
Pregnancy vagina, edematous य vascular ह ह ,vagina bluish
discloration ह ह स Jacquemier sign/Chadwick sign ह ह ! Pregnancy vagina doderlein bacteria growth ह ! Doderlein bacteria
glycogen lactic acid convert ह , सस vagina pH decrease ह ह (pH3.5-6)
Uterus :
Weight of non pregnant uterus 70 gm
Weight of pregnant uterus 1000gm
Length of non pregnant uterus 7.5 cm
Length of pregnant uterus 35 cm
Capacity of non pregnant uterus 10ml
Capacity of pregnant uterus 5000 ml
Shape of Uterus :
Non Pregnant Pyriform
6th
week Hen‘s egg
8th
week Cricket Ball
12th
week Globular
28th
week Pyriform
36th
week Spherical
Uteroplacental blood flow :
Non pregnant uterus blood flow 10 ml/min
Term uteroplacental blood flow 400-600 ml/min
Position of Uterus :- Non pregnant state uterus anteverted anteflexed ह ह ,pregnancy
uterus size increase ह ह abdominal cavity ह ! uterus mainly long axis rotate ह ह , dextrorotation ह ह ! Braxton Hicks -Contraction :- Mainly 2
nd trimester स uterus nonrhythmic, spordic, painless
contraction start ह ह स Braxton Hicks contraction ह ह Braxton Hicks contraction ह स cervix
dilatation ह ह ह !
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 30
Fergusons reflex :-Labour cervix pressure ग य ह cervix nerve supply
ह स uterus contraction ह ह स fergusons reflex ह ह Cervix :- Pregnancy गभग 6 weeks cervix soft ह ह स Goodell‘s sign भ ह ह !
Progesterone hormone ह स cervix स ग secretion ह स physiological
leucorrhoea of pregnancy भ ह ह labour स य यह thick cervical secretion, blood स
cervix स ह ह स show ह ह ! Ovary :-
Pregnancy ovulation ह ह ! Pregnancy corpus luteum 8 weeks progesterone release ह !8-10 weeks
corpus luteum सभ function mainly placenta ग ह ! Pregnancy corpus luteum life span गभग 10-12 weeks ह ह !
Breast :-
Pregnancy estrogen hormone ह स breast mammary ducts alveoli hypertrophy proliferation ह ह , सस breast size increase ह ह !
Nipple size increase ह ह स pigmentation ह ह ! Nipple ओ sebaceous gland hypertoophy ह ह स montgomery‘s
tubercle ह ह ! Colostrum : Pregnancy गभग 12
th week breast स thick,sticky,yellowish fluid ह
ग ह स colostrum ह ह ! Importants Point :-
Comparison between Breast milk & colostrum
Colostrum ग य ह ह , Alkaline ह ह ! Colostrum breast milk स य Immloglobulin स स स य ह ह , Except
K Pottasium
F Fat
C Carbohydrate (Sugar), Cesin
SKIN CHANGES IN PREGNANCY
(i) Chloasma Gravidarum or Pregnancy Mark : Pregnancy ds nkSjku Cheek, Forehead rFkk Eyes ds pkjksa
vksj Pigmentation gks tkrk gS] tks fd Delivery ds ckn vius vki lekIr gks tkrk gSA
(ii) Linea Nigra :Pregnancy ds nkSjku Abdomen ds Mid Line esa Xiphisternum ls ysdj Public Symphysis
rd ,d black Pigmented Line cu tkrh gS] ftls Linea Nigra dgrs gSaA ;g Changes Mainly Anterior Pitutory
Gland ds }kjk Secrete gksus okys Melanocyte Stimulating Hormone dh otg ls gksrs gSaA ;g Pigmentation Hkh
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 31
Delivery ds ckn Disappear gks tkrs gSaA Oral Contraceptive Pills ysus okyh Females esa Hkh blh rjg ds
Pigmentation fn[kkbZ nsrs gSaA
(iii) Striae Gravidarum : Pregnancy ds nkSjku Umbilicus ds uhps okys Part esa Abdominal Wall dh Stretching
dh otg ls Deep Skin Layer esa Scar Tissue Develop gks tkrk gSA Pregnancy ds nkSjku Excessive Stretching rFkk
Aldosterone Hormone dh otg ls ;s Stretch Marks curs gSaA
Supine Hypotension Syndrome (Mangert’s syndrome) : tc Female Supine Position esa ysVrh gS] rc
Pregnancy ds nkSjku 2nd rFkk 3rd
Trimester esa Female Gravid Uterus ds Inferior Vena Cava ij Pressure dh
otg ls Heart esa Venous Return de gks tkrk gSA
Venous Return de gksus dh otg ls Mother dk Cardiac Output de gks tkrk gSA Mother dk Cardiac Output
tc de gksrk gS] rks Foetus dks Blood Supply de gksrh gS] ftlls Fetel Distress iSnk gksrk gSA bls Supine
Hypotension Syndrome dgrs gSaA ;gh dkj.k gS fd Late 2nd
& 3rd
Trimester esa Pregnant Female dks Supine
Position esa ysVus dh lykg ugha nh tkrh gSA mls Left Lateral Position esa ysVuk pkfg,A
Carbodydrate Metabolism during Pregnancy : Pregnancy ds nkSjku Glucose Mother l s Fetus esa s
Facilitiated diffusion }kjk Transfer gksrk gSA
Mother esa Glucose rFkk Amino Acids dh otg ls Insulin dk Secretion c<+ tkrk gSA Pancreas ds beta-Cell
dh Hypertrophy rFkk Hyperplasia gks tkrk gSA
;|fi Pregnancy ds nkSjku Insulin dk Secretion c<+ tkrk gS] ysfdu Estrogen, Progesterone, Cortisol rFkk
Free Fatty Acid dh otg ls Insulin Resistance Develop gks tkrk gS] ftlls Mother esa Postprandial
Hyperglycemia ¼[kkus ds ckn Sugar dk c<+uk½ gks tkrk gSA Pregnancy ds le; 24-28 lIrkg esa Maximum Insulin
Resistance dh lEHkkouk gksrh gSA vr% Gestational Diabetes dk irk djus ds fy, ;g lcls vPNk le; gksrk gSA
Diagnosis of Pregnancy :
Important Terminology :
Early term pregnancy : 37 to 38 weeks + 6 days
Term pregnancy : 39 to 40 weeks + 6 days
Late term pregnancy : 40 to 41 weeks + 6 days
Post term pregnancy : > 42 weeks
Preterm pregnancy : < 37 weeks
The entire duration of pregnancy is divided in three trimester
First trimester : First 12 weeks
Second trimester : 13-28 weeks
Third trimester : 29-40 weeks
Ist Trimester :
Symptoms :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 32
1. Increased Urinary Frequency.
2. Amenorrhea.
3. Morning Sickness due to hCG.
4. Breast Discomfort.
5. Fatigue.
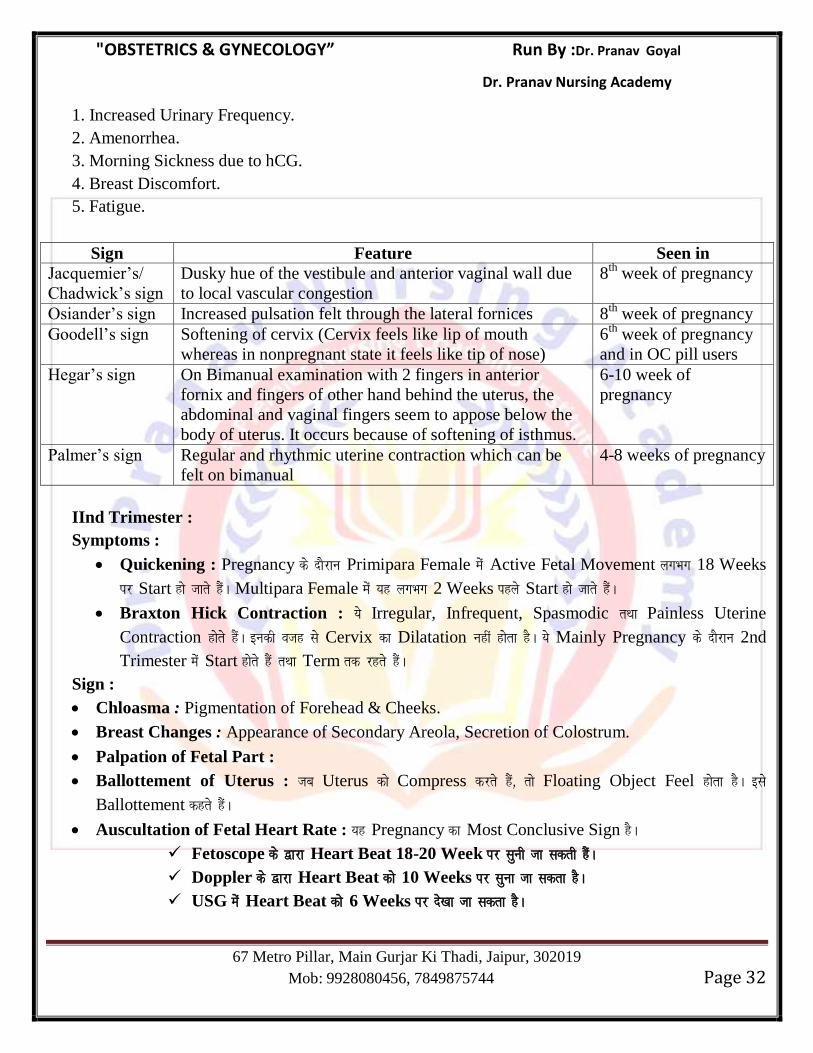
Sign Feature Seen in
Jacquemier‘s/
Chadwick‘s sign
Dusky hue of the vestibule and anterior vaginal wall due
to local vascular congestion
8th
week of pregnancy
Osiander‘s sign Increased pulsation felt through the lateral fornices 8th
week of pregnancy
Goodell‘s sign Softening of cervix (Cervix feels like lip of mouth
whereas in nonpregnant state it feels like tip of nose)
6th
week of pregnancy
and in OC pill users
Hegar‘s sign On Bimanual examination with 2 fingers in anterior
fornix and fingers of other hand behind the uterus, the
abdominal and vaginal fingers seem to appose below the
body of uterus. It occurs because of softening of isthmus.
6-10 week of
pregnancy
Palmer‘s sign Regular and rhythmic uterine contraction which can be
felt on bimanual
4-8 weeks of pregnancy
IInd Trimester :
Symptoms :
Quickening : Pregnancy ds nkSjku Primipara Female esa Active Fetal Movement yxHkx 18 Weeks
ij Start gks tkrs gSaA Multipara Female esa ;g yxHkx 2 Weeks igys Start gks tkrs gSaA
Braxton Hick Contraction : ;s Irregular, Infrequent, Spasmodic rFkk Painless Uterine
Contraction gksrs gSaA budh otg ls Cervix dk Dilatation ugha gksrk gSA ;s Mainly Pregnancy ds nkSjku 2nd
Trimester esa Start gksrs gSa rFkk Term rd jgrs gSaA
Sign :
Chloasma : Pigmentation of Forehead & Cheeks.
Breast Changes : Appearance of Secondary Areola, Secretion of Colostrum.
Palpation of Fetal Part :
Ballottement of Uterus : tc Uterus dks Compress djrs gSa] rks Floating Object Feel gksrk gSA bls
Ballottement dgrs gSaA
Auscultation of Fetal Heart Rate : ;g Pregnancy dk Most Conclusive Sign gSA
Fetoscope ds }kjk Heart Beat 18-20 Week ij lquh tk ldrh gSaA
Doppler ds }kjk Heart Beat dks 10 Weeks ij lquk tk ldrk gSA
USG esa Heart Beat dks 6 Weeks ij ns[kk tk ldrk gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 33
IIIrd Trimester :
Symptoms :
Amenorrhoea Persist.
Enlargment of Abdomen.
Lightening : Pregnancy ds nkSjku 36 Weeks ds ckn Head dk Engagement Pelvis esa gks tkrk gS] ftlls
Head uhps dh vksj f[kldrk gSA Head ds uhps dh vksj vkus dh otg ls Diaphragm ij Pressure de gks tkrk gS]
ftlls Mother dks Relax Feel gksrk gSA bls Lightening dgrs gSaA
Micutaration Frequency :
Presumptive Sign & Symptoms of Pregnancy : ¼,sls Sign rFkk Symptoms tks Pregnancy dh
Possibility dks crkrs gSa] ysfdu Pregnancy dks Confirm ugha djrsA½
1. Amenorrhoea.
2. Nausea/Vomitting.
3. Frequancy of Micturation.
4. Quickening.
5. Breast Discomfort.
6. Fatigue.
7. Skin Changes.
Positive or Absolute Sign of Pregnancy :
1. Palpation of Fetal Parts.
2. Auscultation of Fetal Heart Sound.
3. USG evidence of Embryo.
4. Radiological Demonstration of Fetal Skelton at 16 Weeks and onwards.
Pseudocyesis ((Phantom Pregnancy/Spurious Pregnancy/False Pregnancy) : ;g ,d Psychological
Disorder gSA blesa Female dks ,slk yxrk gS fd ह Pregnant gS tcfd okLrfodrk esa mlesa Pregnancy ds dksbZ Sign Present
ugha gksrsA ;s Female Infertile gksrh gSa] ftuesa cPps ds fy, izcy bPNk gksrh gSA Patient esa fuEufyf[kr Sign Present gksrs gSa %
1. Cessation of Menstruation.
2. Enlargement of Abdomen (Due to Fat deposition)
3. Secretion from Breast.
4. Fetal Movement (actually Intestinal Movement)
Antenatal Care : Ideally fuEu Schedule Antenatal Visit ds fy, gksuk pkfg, %
(i) 28th Week rd izR;sd ekg Visit gksuh pkfg,A
(ii) 28-36 Week rd izR;sd 15 fnu esa Visit gksuh pkfg,A
(iii) 36th Week rFkk mlds vkxs izR;sd 7 fnu esa Visit gksuh pkfg,A
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 34
vr% dqy 12-15 Visit gksuh pkfg,A
WHO Recommends atleast 4 Visit :
Ist Visit : 16 Weeks
2nd Visit : 24-28 Weeks
3rd Visit : 32 Weeks.
4th Visit : 36 Weeks
As per Indian scenario minimum 3 visits are essential
Ist Visit : 20 Weeks(or as soon as pregnancy is known)
2nd Visit : 32 Weeks
3rd Visit : 36 Weeks
tc igyh ckj Pregnant Female Health Care Facility ij vkrh gS] mls Booking Visit dgrs gSaA
Folic Acid Supplementation during Pregnancy : Pregnancy ds nkSjku Folic Acid Supplementation
Neural Tube Defect dks Prevent djrk gSA
When to Initiate Folic Acid : Folic Acid Conception ls rhu ekg igys ;k Atleast 1 Month igys Start
djuh pkfg, rFkk Pregnancy ds rhu ekg rd Continue j[kuh pkfg,A bl Dose dks Prophylactic Dose of Folic
Acid dgrs gSaA
Govt. of India, Iron rFkk Folic Acid dh Tablets Free of Cost Supply djrh gSA blesa 100 mg Elemental Fe
rFkk 500 mcg Folic Acid gksrk gSA
RDA of folic Acid during Pregnancy — 500 mcg
High Risk Patient tSls %
a) Females with H/o Previous NTD Babies.
b) Diabetic Females.
c) Female with sickle cell Anemia.
d) Female on Antiepileptic drugs like Valproic Acid.
bu High Risk Patient esa NTD dks Prevent djus ds fy, Folic Acid dh dose 4 mg gksrh gSA bls therepeutic
Dose of Folic Acid dgrs gSaA
Pregnancy ds nkSjku Megaloblastic Anemia dks Treat djus ds fy, Folic Acid dh Dose 1 mg/day gksrh gSA
Iron Supplementation during Pregnancy : Pregnancy ds nkSjku Total Iron dh Requirement yxHkx
1000 mg gksrh gSA (4-6 mg/daily)
Fetal & Placenta Require — 300 mg
Growing RBC of Mother Require — 500 mg
Lost through Sweat, Urine & Faeces — 200 mg
Lost at the time of delivery — 200 mg
Amount of Iron saved due to Amenorrhoea — 300 mg
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 35
So 1200 –300 = 900 – 1000 mg Iron Required gksrk gSA
Iron dks ftl Hkh form (Oral, IM) esa fy;k tk,] ;g Only 10% gh Absorbed gksrk gS] vr% Pregnancy ds nkSjku 4-
6 mg/daily requirement dks iwjk djus ds fy, 40-60 mg Iron daily diet esa gksuk t:Lh gS] tks fd Impossible gSA
blfy, Pregnancy ds nkSjku 6 Months rd Iron Absolutely Required gksrk gSA
National Anaemia Control Programme : lHkh Pregnant Females dks 100 mg Elemental Iron
(Ferrous Sulphate) + 500 mg Folic Acid atleast 100 days ds fy, nh tkrh gSA Iron Tablets 12-14 Weeks
ij Start dh tkuh pkfg,A
Important Points :
RDA of Calcim during Pregnancy — 1000 mg/day
RDA of Iodine during Pregnancy — 250 μg/day
Vaccination during Pregnancy :
Tetanus Vaccine : 0.5 ml Tetanus toxiod dh 2 dose IM 6 Weeks ds vUrjky ij nh tkuh pkfg,A
Ist Dose : 16-20 Weeks
IInd Dose : 20-24 Weeks
,slh Females ftuesa Vaccination igys ls gks j[kk gS] mues a Only Booster Dose 0.5 ml IM Delevery l s 4
Weeks igys nh tkuh pkfg,A
Other Vaccine in Pregnancy : Killed Vaccine Pregnancy esa Safe gksrs gSa tcfd Live Vaccine dks
Pregnancy esa Avoid fd;k tkrk gSA
Safe Only in
epidemics
To be given in case of travel to highly
endemic area or exposed to contacts
Contraindicated
H-Hepatitis
A/B
Tab-Typhoid
P-Pneumococcus
C-Cholera
Yellow fever
Japanese encephalitis
Polio (IPV)
Rubella
Measles
Mumps
I-Influenza
T-Tetanus
Rabies-Rabies
M-
Meningococcus
(Tab PCM)
BCG
Smallpox
Chickenpox
Grvida & Parity :
Gravida : ;g Pregnant State dks crkrk gSA ;g Frequency of Pregnancy dks crkrk gSA
Parity : ;g crkrk gS fd fdruh Previous Pregnancy Period of Viability rd igqaph gSA pkgs Period of
Viability ds ckn mudk dqN Hkh gqvk gksA (period of viability-20 weeks)
Example :
Eg.1. ,d 10 Weeks Pregnant Female gS] ftls ,d 4 lky dk cPpk gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 36
G2P1
;gka og nwljh ckj Pregnant gS vFkkZr Gravida 2 gS tcfd ,d Pregnancy Viability rd igqaph gS vFkkZr Parity 1 gSA
Eg.2. ,d 10 Weeks Pregnant Female gS] ftldk ,d Abortion 12 Weeks ij gks x;k FkkA
G2P0
;gka ij nwljh ckj Pregnant gS vFkkZr Gravida 2 gS] ysfdu vHkh dksbZ Hkh Pregnancy Viability rd ugha igqaph vFkkZr
Parity 0 gSA
Eg.3. ,d 12 Weeks Pregnant Female gS ftlesa igys 38 Weeks ij Twin Delivery dh History gSA
G2P1
;gka og nwljh ckj Pregnant gS vFkkZr Gravida 2 gS] ysfdu Last Pregnancy esa 38 Week ij Twin Delivery gS
vFkkZr ,d Pregnancy Period of Viability rd igqaph gS vFkkZr Parity 1 gSA ;gka cPpksa dh la[;k Count ugha dh tkrh]
Only Frequency Count dh tkrh gSA
Present pregnancy Parity include ह य ह ! GPT + P + A + L Method :
T : No. of Term Pregnancy (37-42 Weeks)
P : No. of Pretern Delivery (28-36 Weeks)
A : No. of Abortion (Death before 20 Weeks)
L : No. of Live children.
Still Birth : ;fn cPps dh Delivery 20 Weeks ds ckn gks rFkk cPpk Dead gks x;k gksA
Miscarriage : ;fn cPps dh Death 20 Weeks ls igys gks xbZ gks] rks bls Miscarriage dgrs gSaA
Primipara : ,slh Female tks igyh ckj Pregnant gqbZ gksA
Multipara : ,slh Female tks nks ;k nks ls T;knk ckj Pregnant gqbZ gSA
Elderly Primigravida : ,slh Female tks 30 Years dh Age ds ckn igyh ckj Pregnant gqbZ gSA
Grand Multipara : ,slh Pregnant Female tks igys ls 4 ;k 4 ls T;knk ckj Pregnant gks pqdh gSA
Nullipara : ,slh Female tks dHkh Hkh Pregnant ugha gqbZ gSA
Chapter 4
DIAGNOSIS IN OBSTETRICS & FETAL MONITORING
USG in Obstetrics :
Level I Examination (Routine/Basic Examination) : ;g Pregnancy ds nkSjku Routine Sonography
Examination gksrk gS] tks fd Dating ,No. of fetus, Amniotic Fluid rFkk Placenta ds Localization ds fy, fd;k tkrk gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 37
Level 2 (Tragated Examination/TIFFA : Targated imaging for Fetal Anomalies) : ;g Sonography Fetus
esa Congenital Anomally dks Detect djus ds fy, dh tkrh gSA
Important Points :
TIFFA Scan lHkh Pregnant Females esa 18-20 Weeks ij fd;k tkuk pkfg,A
Time for Routine Ultrasound Scan
-At the Booking Visit (Ist Trimester)
-18-22 Weeks.
-In 3rd Trimester
;fn iwjh Pregnancy ds nkSjku flQZ ,d gh Ultrasound djuh gks] rks lclss Best Time 18-20 Weeks gSA
Placenta dks Localize djus ds fy, USG dk Best Time 3rd Trimester gSA
Twins Pregnancy esa Chorionicity dks Detect djus ds fy, USG dk Best Time 11-14 weeks gSA
First Trimester Ultrasound Examination :
Pregnancy ds nkSjku lksuksxzkQh esa Pregnancy dk First Sign Gestation Sac dk fn[kkbZ nsuk gSA
Gestation Sac esa Yolk Sac dk fn[kkbZ nsuk 100% Intrauterine Pregnancy dks Confirm djrk gSA
USG esa Cardiac Activity 6 Weeks ij Appear gks tkrh gSA
For Determination of Gestational Age in Ist Trimester :
CROWN-RUMP LENGTH : Longest Straightline measurement of the embryo from the outer margin of
cephalic pole to rump.
Ist Trimester esa Fetal age Determine djus ds fy, lcls Best Parameter CRL
Second Trimester Ultrasound Examination :
BPD (Biparietal Diameter) : 14 Week ls 20 Week ds chp Fetal Age Determine djus ds fy, Best Parameter gksrk
gSA
HC : (Head Circumference) ;fn Fetus ds Head dh Shape esa dksbZ Changes gS] rks Head Circuference (HC) T;knk
Better Parameter gksrk gS] BPD dh rqyuk esaA
FL (Femur Length) : 3rd Trimester esa Fetal Age dks Determine djus ds fy, Best Parameter gksrk gSA
AC (Abdominal Circumference) : Fetal Growth dks Determine djus ds fy, Best Parameter gksrk gSA Eg. IUGR,
Macrosomia.
Fetal Congenital Anomallies :
Anencephaly
USG esa lcls igys Detect gksus okyh Anomally — Anencephaly
Anencephaly dks Earliest 10 Weeks ij USG esa Diagnose fd;k tk ldrk gSA
Sign of Anencephaly on USG :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 38
Fetal Head has an Irregular contour and No Bone.
No calcified Cranium.
Face Shows Mickey Mouse Sign.
Eye of Fetus are big- Frog eye sign.
Anencephaly ,d Neural Tube Defect gSA blesa Forebrain rFkk Midbrain Absent gksrk gSA
Diagnosis :
Screening Method :
(i) Increased level of Maternal serum alpha fetoprotein.
(ii) Most Specefic Marker of Anencephaly — Acetylcholinesterase.
(iii)Investigation of Choice — Ultrasound.
Spina Bifida : Spina Bifida dks 2nd Trimester esa Sonography }kjk Diagnose fd;k tk ldrk gSA
Sonographic Sign in Spina Bifida :
Small biparietal Diameter.
Ventriculomegaly.
Frontal Bone Scalloping (Lemon Sign)
Elongation & downward displacement of the cerebellum (Banana Sign)
Prenatal Diagnostic Techniques :
(i) Chorionic villi Sampling.
(ii) Amniocentesis.
(iii)Cordocentesis.
(iv) Fetal Tissue Biopsy (Not Done)
(i) Chorionic Villi Sampling (CVS) :
Study Material : Chorionic Villi from which Trophoblastic cells are used for study
Time --10-13 Weeks.
Indication :
To detect chromosomal Anomallies.
For DNA analysis-- in Haemoglobinopathies,sickle cell anemia.
To detect Inborn error of Metabolism like Phenylketonurea.
Ist Trimester diagnosis of Down Syndrome.
Risk :
Chances of Fetal loss/Abortion (1-2%)
;fn CVS 9 Weeks ls igys fd;k tkrk gS] rks Limb Reduction Defect dh lEHkkouk c<+ tkrh gSA
(ii) Amniocentesis : Amniotic Sac ls Amniotic Fluid dks fudkyuk Amniocentesis dgykrk gSA blds }kjk Fetal
Congenital Anomallies dks Detect fd;k tk ldrk gSA
Time : 15-20 Weeks
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 39
Early Amniocentesis : 11-14 weeks
(iii) Cordocentesis : (Perumbilical Blood Sampling) [PUBS]
Time >20 Weeks.
Cordocentesis esa Umbilical vein ls Blood Sample fy;k tkrk gSA ¼Site tgka Cord Placenta ls Attach gksrh gSA½
Chances of Fetal Loss = 3%
Most Common Indication of Cordocentesis is Evaluation & Treatment of Fetal Isoimmunization.
Biochemical Test :
a) Double Marker Test :
Beta-hCG
PAPP - A (Pregnancy associated Plasma Protein - A)
Down Syndrone esa Beta-hCG dk Level Increase gksrk gS rFkk PAPP-A dk Level Decrease gksrk gS tcfd ckdh lHkh
Aneuploidy esa Beta-hCG rFkk PAPP-A nksuksa dk Level Decrease gksrk gSA
Double Marker Test Ist Trimester esa 11-14 Week ds chp fd;k tkrk gSA
b) Tripple Marker Test :
;g Test 16-18 Week ds chp fd;k tkrk gSA
blesa 3 Hormones gksrs gSa-
1. Beta-hCG
2 AFP
3 Unconjugated Estriol (UE3)
HCG AFP UE3
Down Syndrome Increase Decrease Decrease
Edward syndrome Decrease Decrease Decrease
c) Quadruple Marker Test :
;g Test Mainly 18-22 Weeks ds chp fd;k tkrk gSA
blesa 4 Harmones gksrs gSa-
1. Beta-hCG
2. AFP
3. UE3
4. Inhibin-A
HCG AFP UE3 Inhibin A
Down Syndrome Increase Decrease Decrease Increase
Down Syndrome esa Inhibin-A dk Level Increase gks tkrk gSA
DOWN SYNDROME :
Mainly due to trisomy 21
Trisomy 21 — Nondisjunction of Chromosome
Non lethal trisomy.
Prevalance 1 : 1000 Pregnancies
;fn Mother dh Age Increase gksrh gS (At the time of Pregnancy) rks Down Syndrome ds Chances c<+ tkrs gSaA
Clinical Finding :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 40
Brachycephaly
Epicanthal Fold
Upslanting Palpebral Fissure
Brushfield Spot (Greyish spot on Iris)
Flat Nasal Bridge
Hypotonia
Single Palmar Crease
Hypoplasia of the middle Phalynx of 5th finger
Sandle Toe Gap
Cardiac Defeet — Endocardial cushion defect, VSD
GI Defect — Dudoneal Atresia, Esophageal Atresia, Hirschsprung Disease
Mental Retardation
Screening Test for Down Syndrone :
First Trimester Screening :
(i) Nuchal Translucency : ;g Down Syndrome ds fy, Sonographic Marker gSA ;g Mainly Ist Trimester esa ns[kk
tkrk gSA
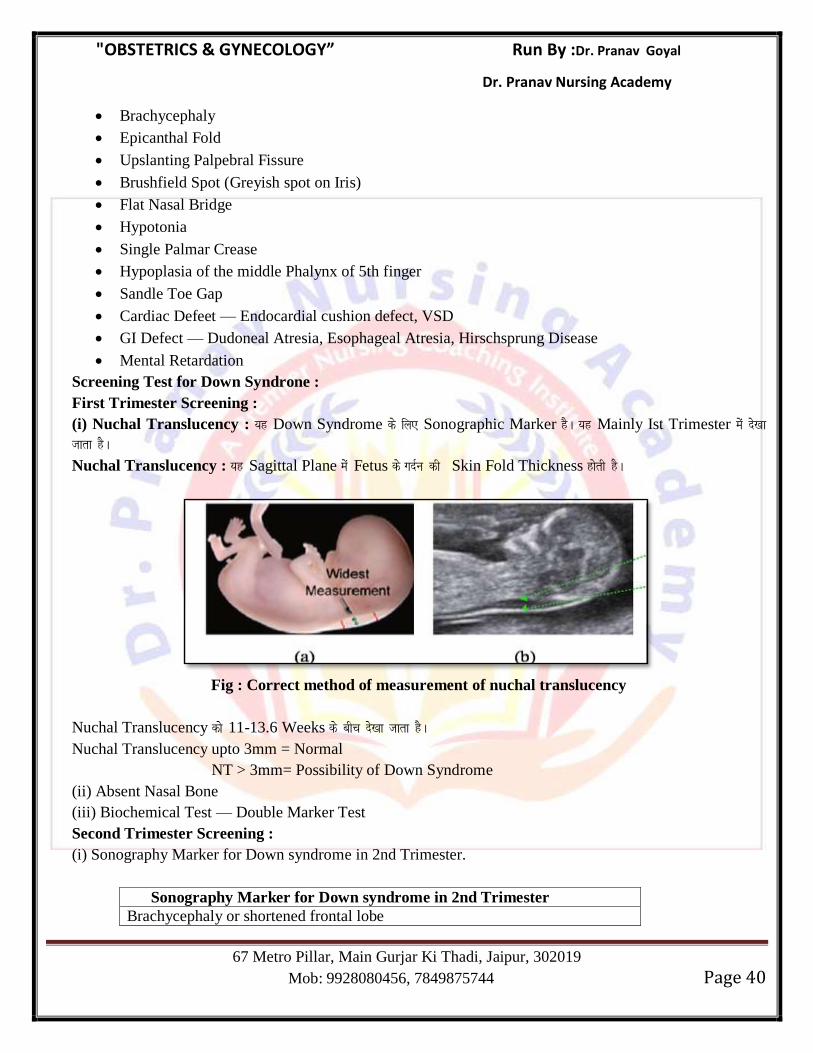
Nuchal Translucency : ;g Sagittal Plane esa Fetus ds xnZu dh Skin Fold Thickness gksrh gSA
Fig : Correct method of measurement of nuchal translucency
Nuchal Translucency dks 11-13.6 Weeks ds chp ns[kk tkrk gSA
Nuchal Translucency upto 3mm = Normal
NT > 3mm= Possibility of Down Syndrome
(ii) Absent Nasal Bone
(iii) Biochemical Test — Double Marker Test
Second Trimester Screening :
(i) Sonography Marker for Down syndrome in 2nd Trimester.
Sonography Marker for Down syndrome in 2nd Trimester
Brachycephaly or shortened frontal lobe
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 41
Clinodactyly (hypoplasia of the 5th
digit middle phalanx)
Hyperechogenic bowel
Echogenic intracardiac focus
Nasal bone absence or hypoplasia
Nuchal fold thickening
Aberrant right subclavian artery
‗Sandal gap‘ between first and second toes
Shortened ear length
Single umbilical artery
Short femur
Short humerus
Mild hydronephrosis ventriculomegaly
(ii) Biochemical Test :
a) Triple Marker Test
b) Quadruple Marker Test
Antepartum Fetal Monitoring :
Fetal Heart Rate : Base Line Fetal Heart Rate = 110-160 bpm
i)Bradycardia : FHR < 110 bpm
Causes :
2nd Stage of Labour esa Mild Head Compression dh otg ls Bradycardia gksrk gSA
Cogenital Heart Block
Fetal Bradycardia Serious Fetal Compromise dks iznf’kZr djrk gSA
ii)Tachycardia : FHR > 160 bpm
Causes :
Maternal Fever due to amnionitis.
Cardiac Arrythmias.
Maternal Parasympathomimetics (Atropine) or Sympathomimetics (Terbutaline)
May indicate Fetal compromite.
Beat to Beat Variability :
Baseline variability 5-25 bpm. Normal Fetal well being dk Sign gksrk gSA
Acceleration :
Acceleration vFkkZr Foetal Heart Rate dk 15 bpm ;k T;knk c<+uk de ls de 15 Sec. rdA (> 32 Weeks)
Acceleration ;g iznf’kZr djrk gS fd Fetal dk Neurohormonal rFkk Cardiovascular Activity intact gSA ;g iznf’kZr djrk
gS fd Fetus Healthy gSA
;fn Fetus 32 Weeks ls de gS] rks Fetal Heart Rate 10 bpm ;k blls T;knk c<+uh pkfg, de ls de 10 Sec. rdA
Deceleration :
Fetal Heart Rate dk Uterine contraction ds lkFk 15 Beat Per Minute, 15 Sec. rd de gksuk Deceleration dgykrk gSA
Deceleration esa 3 Pattern ik, tkrs gSa %
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 42
(i) Early Deceleration;
(ii) Late Deceleration
(iii) Variable Deceleration.
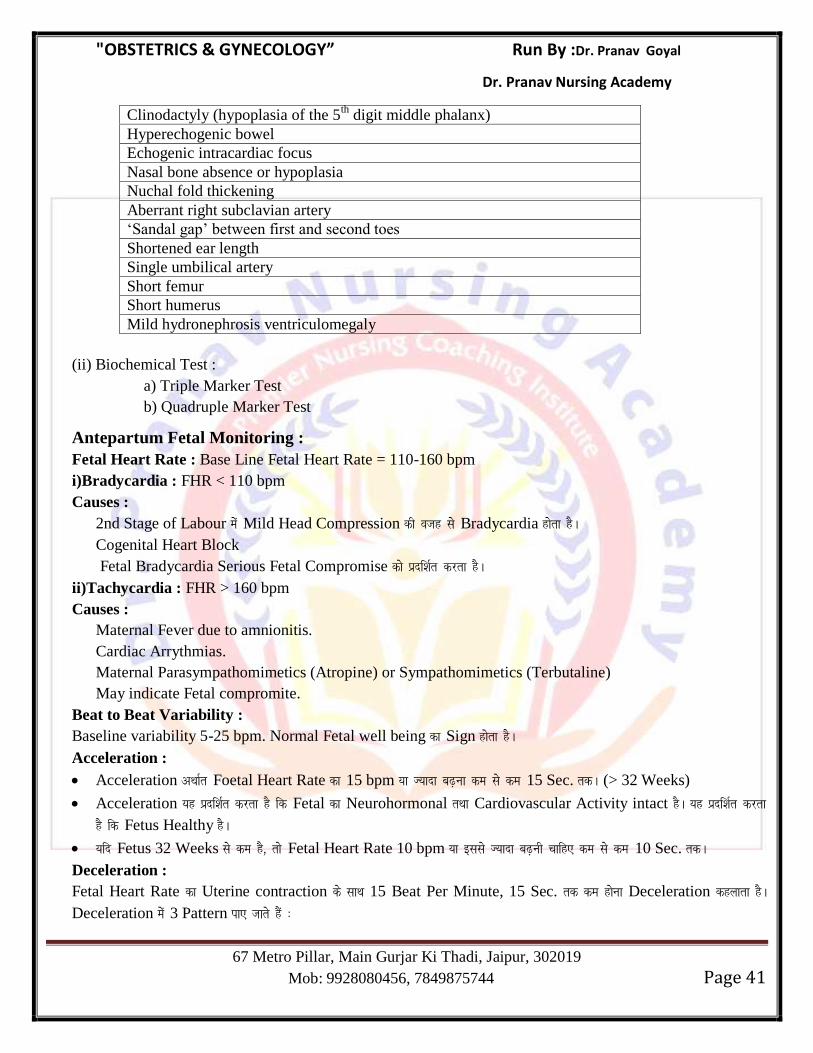
(i) Early Deceleration : Early Deceleration rFkk Uterine Contraction nksuksa ,d lkFk gksrs gSaA
Early Deceleration Head Compression esa fn[kkbZ nsrk gSA ;g ,d Physiological Process gSA blesa Fetal Hypoxia ugha gksrk
gSA
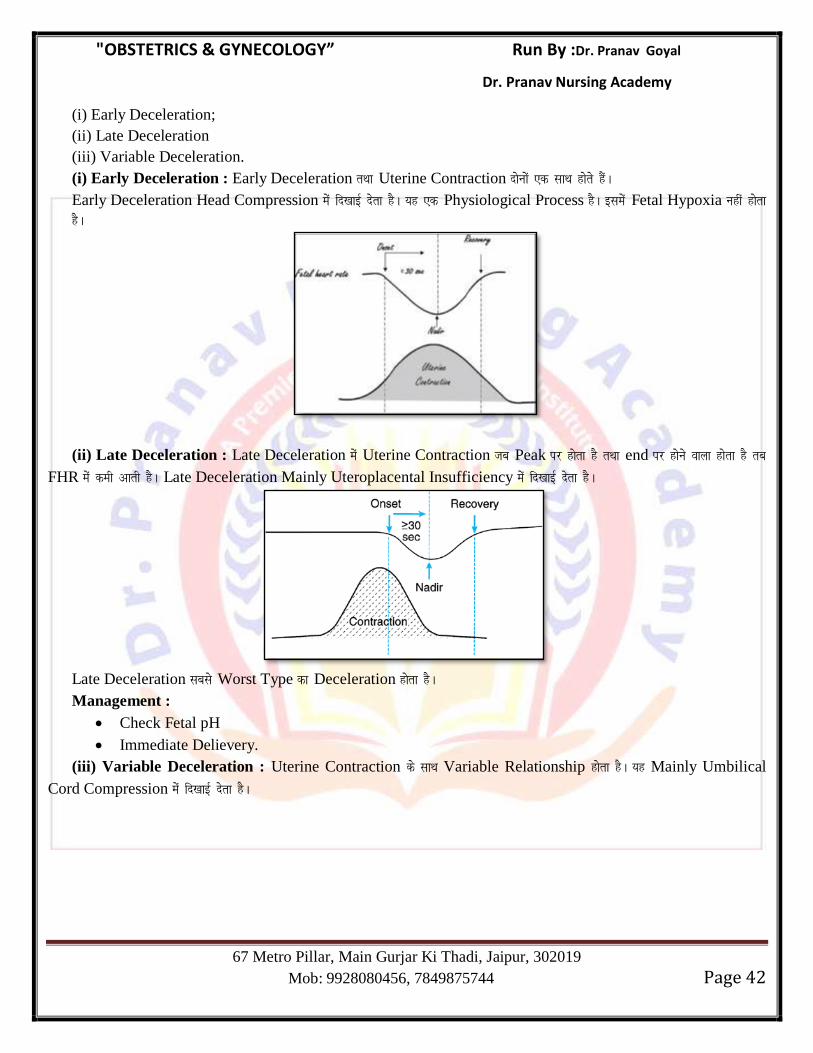
(ii) Late Deceleration : Late Deceleration esa Uterine Contraction tc Peak ij gksrk gS rFkk end ij gksus okyk gksrk gS rc
FHR esa deh vkrh gSA Late Deceleration Mainly Uteroplacental Insufficiency esa fn[kkbZ nsrk gSA
Late Deceleration lcls Worst Type dk Deceleration gksrk gSA
Management :
Check Fetal pH
Immediate Delievery.
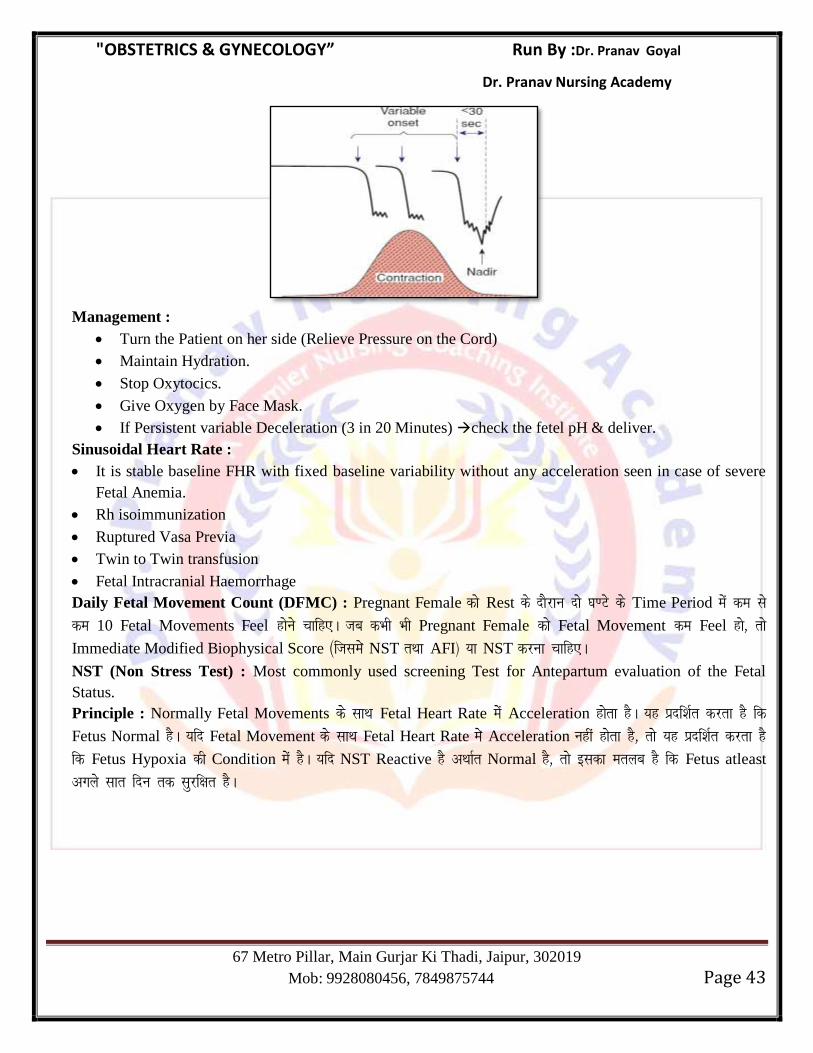
(iii) Variable Deceleration : Uterine Contraction ds lkFk Variable Relationship gksrk gSA ;g Mainly Umbilical
Cord Compression esa fn[kkbZ nsrk gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 43
Management :
Turn the Patient on her side (Relieve Pressure on the Cord)
Maintain Hydration.
Stop Oxytocics.
Give Oxygen by Face Mask.
If Persistent variable Deceleration (3 in 20 Minutes) check the fetel pH & deliver.
Sinusoidal Heart Rate :
It is stable baseline FHR with fixed baseline variability without any acceleration seen in case of severe
Fetal Anemia.
Rh isoimmunization
Ruptured Vasa Previa
Twin to Twin transfusion
Fetal Intracranial Haemorrhage
Daily Fetal Movement Count (DFMC) : Pregnant Female dks Rest ds nkSjku nks ?k.Vs ds Time Period esa de ls
de 10 Fetal Movements Feel gksus pkfg,A tc dHkh Hkh Pregnant Female dks Fetal Movement de Feel gks] rks
Immediate Modified Biophysical Score ¼ftlesa NST rFkk AFI½ ;k NST djuk pkfg,A
NST (Non Stress Test) : Most commonly used screening Test for Antepartum evaluation of the Fetal
Status.
Principle : Normally Fetal Movements ds lkFk Fetal Heart Rate esa Acceleration gksrk gSA ;g iznf’kZr djrk gS fd
Fetus Normal gSA ;fn Fetal Movement ds lkFk Fetal Heart Rate esa Acceleration ugha gksrk gS] rks ;g iznf’kZr djrk gS
fd Fetus Hypoxia dh Condition esa gSA ;fn NST Reactive gS vFkkZr Normal gS] rks bldk eryc gS fd Fetus atleast
vxys lkr fnu rd lqjf{kr gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 44
Biophysical Score/Manning Score : ;g Antepartumly Fetal Well Being dk Indicator gSA blesa 5 Parameter gksrs
gSaA
1. Fetal Tone,
2. Fetal Breathing Movement (Seen in 30 Minute)
3. Fetal gross body Movement (Seen in 30 Minute)
4. Amniotic Fluid Volume
5. Non Stress Test
Biophysical Profile (BPP) is a diagnostic test for Uteroplacental insufficiency.
Score 8-10 — Normal
Score 6 — Equivocal
Score <5 — Abnormal
Contraction Stress Test (CST) : bl Test esa Oxytocin }kjk Uterine Contraction dks Induce fd;k tkrk gS rFkk
Uterine Contraction ds nkSjku FHR esa Change dks Note fd;k tkrk gSA
No Change in FHR — Non Reactive — Normal
Change in FHR — Reactive — Abnormal
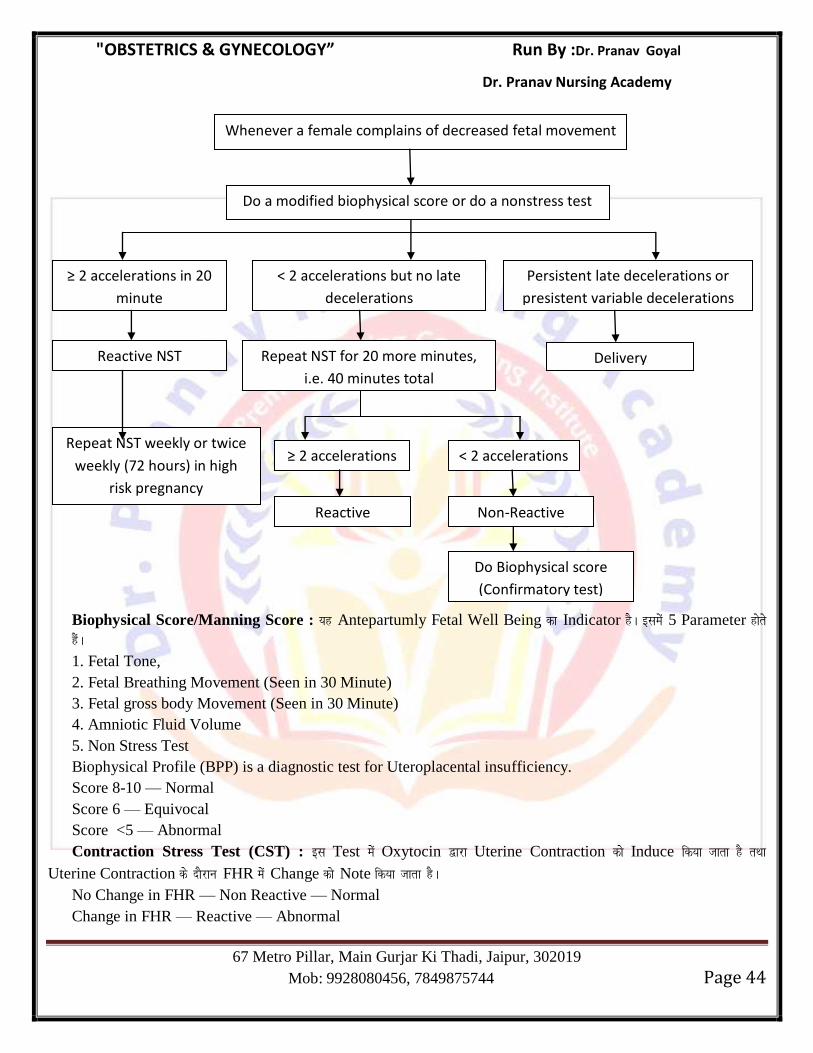
Whenever a female complains of decreased fetal movement
Do a modified biophysical score or do a nonstress test
≥ 2 accelerations in 20
minute
< 2 accelerations but no late
decelerations
Persistent late decelerations or
presistent variable decelerations
Reactive NST Delivery Repeat NST for 20 more minutes,
i.e. 40 minutes total
Repeat NST weekly or twice
weekly (72 hours) in high
risk pregnancy
Do Biophysical score
(Confirmatory test)
Non-Reactive Reactive
≥ 2 accelerations < 2 accelerations
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 45
Chapter 5
PELVIS & FETAL SKULL
Pelvis
Anatomy : Human Pelvis 4 Bones ls feydj cuh gksrh gSA
(1) Sacrum - 1
(2) Coccyx - 1
(3) Innominate Bone – 2
izR;sd Innominate Bone Ileum,ischium rFkk Pubis ls feydj curh gSA
Pelvic Joint : Pelvis esa Mainly 4 Joints gksrs gSa %
(1) Symphysis Pubis
(2) Sacroiliac Joint (Rt. & Lt.)
(3) Sacrococcygeal Joint.
Type of Joints :
Joints Type
Symphysis Pubis Fibrocartilagenous
Sacroiliac Joint Synovial Joint
Sacrococcygeal Joint Synovial Hinge Joint
Anatomically Pelvic Brim Pelvis dks nks Hkkxksa esa Devide djrh gSA
False Pelvis : ;g Pelvic Brim स ऊ part ह स obstetrical significance ह ह ! True Pelvis :-Pelvic Brim ds uhps okyk Part True Pelvis dgykrk gSA True Pelvis ,d Bony Canal cukrk gS] tgka ls
Labour ds le; Fetus dks xqtjuk iM+rk gSA
True Pelvis vkxs dh vksj Pubic Symphysis rFkk ihNs dh vksj Sacrum rFkk Coccyx ls curk gSA
True Pelvis dks rhu Hkkxksa esa Devide fd;k x;k gSA
(i) Pelvic Inlet
(2) Pelvic Cavity
(3) Pelvic Outlet
Pelvic Inlet : Most Common variety of Pelvis (Gynecoid Pelvis) esa Pelvic Inlet dk Shape Transverse Oval
gksrk gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 46
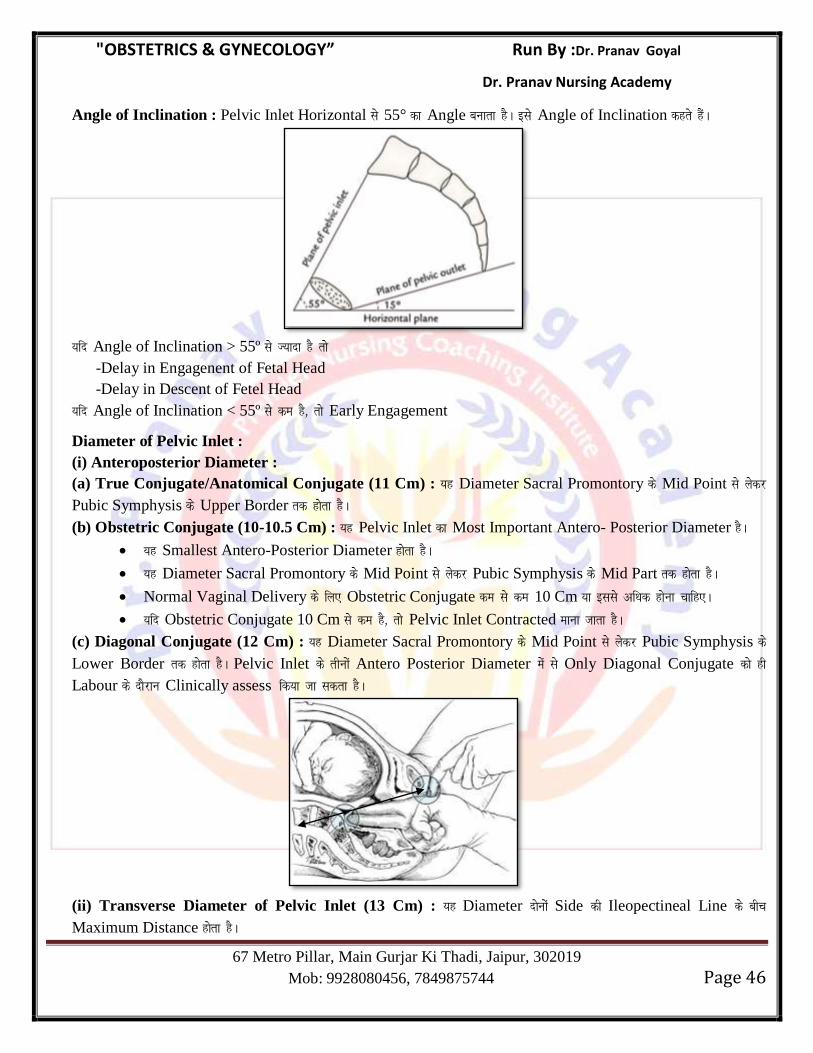
Angle of Inclination : Pelvic Inlet Horizontal ls 55° dk Angle cukrk gSA bls Angle of Inclination dgrs gSaA
;fn Angle of Inclination > 55º ls T;knk gS rks
-Delay in Engagenent of Fetal Head
-Delay in Descent of Fetel Head
;fn Angle of Inclination < 55º ls de gS] rks Early Engagement
Diameter of Pelvic Inlet :
(i) Anteroposterior Diameter :
(a) True Conjugate/Anatomical Conjugate (11 Cm) : ;g Diameter Sacral Promontory ds Mid Point ls ysdj
Pubic Symphysis ds Upper Border rd gksrk gSA
(b) Obstetric Conjugate (10-10.5 Cm) : ;g Pelvic Inlet dk Most Important Antero- Posterior Diameter gSA
;g Smallest Antero-Posterior Diameter gksrk gSA
;g Diameter Sacral Promontory ds Mid Point ls ysdj Pubic Symphysis ds Mid Part rd gksrk gSA
Normal Vaginal Delivery ds fy, Obstetric Conjugate de ls de 10 Cm ;k blls vf/kd gksuk pkfg,A
;fn Obstetric Conjugate 10 Cm ls de gS] rks Pelvic Inlet Contracted ekuk tkrk gSA
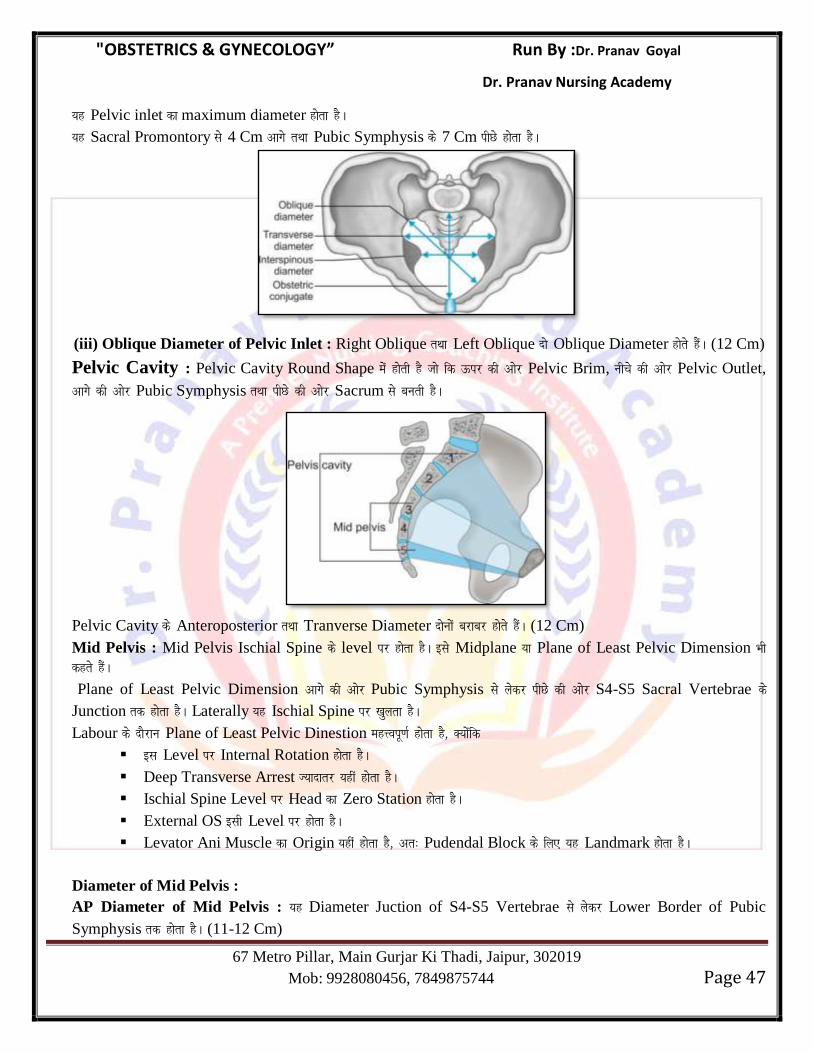
(c) Diagonal Conjugate (12 Cm) : ;g Diameter Sacral Promontory ds Mid Point ls ysdj Pubic Symphysis ds
Lower Border rd gksrk gSA Pelvic Inlet ds rhuksa Antero Posterior Diameter esa ls Only Diagonal Conjugate dks gh
Labour ds nkSjku Clinically assess fd;k tk ldrk gSA
(ii) Transverse Diameter of Pelvic Inlet (13 Cm) : ;g Diameter nksuksa Side dh Ileopectineal Line ds chp
Maximum Distance gksrk gSA
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 47
;g Pelvic inlet dk maximum diameter gksrk gSA
;g Sacral Promontory ls 4 Cm vkxs rFkk Pubic Symphysis ds 7 Cm ihNs gksrk gSA
(iii) Oblique Diameter of Pelvic Inlet : Right Oblique rFkk Left Oblique nks Oblique Diameter gksrs gSaA (12 Cm)
Pelvic Cavity : Pelvic Cavity Round Shape esa gksrh gS tks fd Åij dh vksj Pelvic Brim, uhps dh vksj Pelvic Outlet,
vkxs dh vksj Pubic Symphysis rFkk ihNs dh vksj Sacrum ls curh gSA
Pelvic Cavity ds Anteroposterior rFkk Tranverse Diameter nksuksa cjkcj gksrs gSaA (12 Cm)
Mid Pelvis : Mid Pelvis Ischial Spine ds level ij gksrk gSA bls Midplane ;k Plane of Least Pelvic Dimension Hkh
dgrs gSaA
Plane of Least Pelvic Dimension vkxs dh vksj Pubic Symphysis ls ysdj ihNs dh vksj S4-S5 Sacral Vertebrae ds
Junction rd gksrk gSA Laterally ;g Ischial Spine ij [kqyrk gSA
Labour ds nkSjku Plane of Least Pelvic Dinestion egÙoiw.kZ gksrk gS] D;ksafd
bl Level ij Internal Rotation gksrk gSA
Deep Transverse Arrest T;knkrj ;gha gksrk gSA
Ischial Spine Level ij Head dk Zero Station gksrk gSA
External OS blh Level ij gksrk gSA
Levator Ani Muscle dk Origin ;gha gksrk gS] vr% Pudendal Block ds fy, ;g Landmark gksrk gSA
Diameter of Mid Pelvis :
AP Diameter of Mid Pelvis : ;g Diameter Juction of S4-S5 Vertebrae ls ysdj Lower Border of Pubic
Symphysis rd gksrk gSA (11-12 Cm)
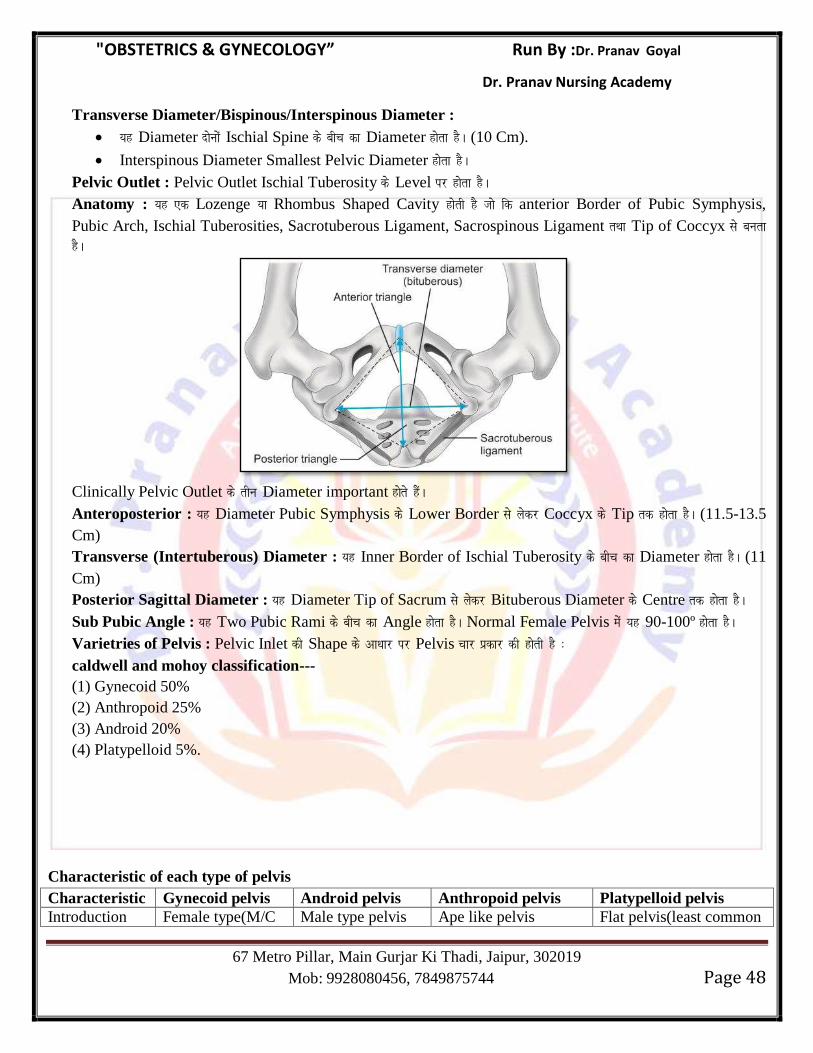
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 48
Transverse Diameter/Bispinous/Interspinous Diameter :
;g Diameter nksuksa Ischial Spine ds chp dk Diameter gksrk gSA (10 Cm).
Interspinous Diameter Smallest Pelvic Diameter gksrk gSA
Pelvic Outlet : Pelvic Outlet Ischial Tuberosity ds Level ij gksrk gSA
Anatomy : ;g ,d Lozenge ;k Rhombus Shaped Cavity gksrh gS tks fd anterior Border of Pubic Symphysis,
Pubic Arch, Ischial Tuberosities, Sacrotuberous Ligament, Sacrospinous Ligament rFkk Tip of Coccyx ls curk
gSA
Clinically Pelvic Outlet ds rhu Diameter important gksrs gSaA
Anteroposterior : ;g Diameter Pubic Symphysis ds Lower Border ls ysdj Coccyx ds Tip rd gksrk gSA (11.5-13.5
Cm)
Transverse (Intertuberous) Diameter : ;g Inner Border of Ischial Tuberosity ds chp dk Diameter gksrk gSA (11
Cm)
Posterior Sagittal Diameter : ;g Diameter Tip of Sacrum ls ysdj Bituberous Diameter ds Centre rd gksrk gSA
Sub Pubic Angle : ;g Two Pubic Rami ds chp dk Angle gksrk gSA Normal Female Pelvis esa ;g 90-100º gksrk gSA
Varietries of Pelvis : Pelvic Inlet dh Shape ds vk/kkj ij Pelvis pkj izdkj dh gksrh gS %
caldwell and mohoy classification---
(1) Gynecoid 50%
(2) Anthropoid 25%
(3) Android 20%
(4) Platypelloid 5%.
Characteristic of each type of pelvis
Characteristic Gynecoid pelvis Android pelvis Anthropoid pelvis Platypelloid pelvis
Introduction Female type(M/C Male type pelvis Ape like pelvis Flat pelvis(least common
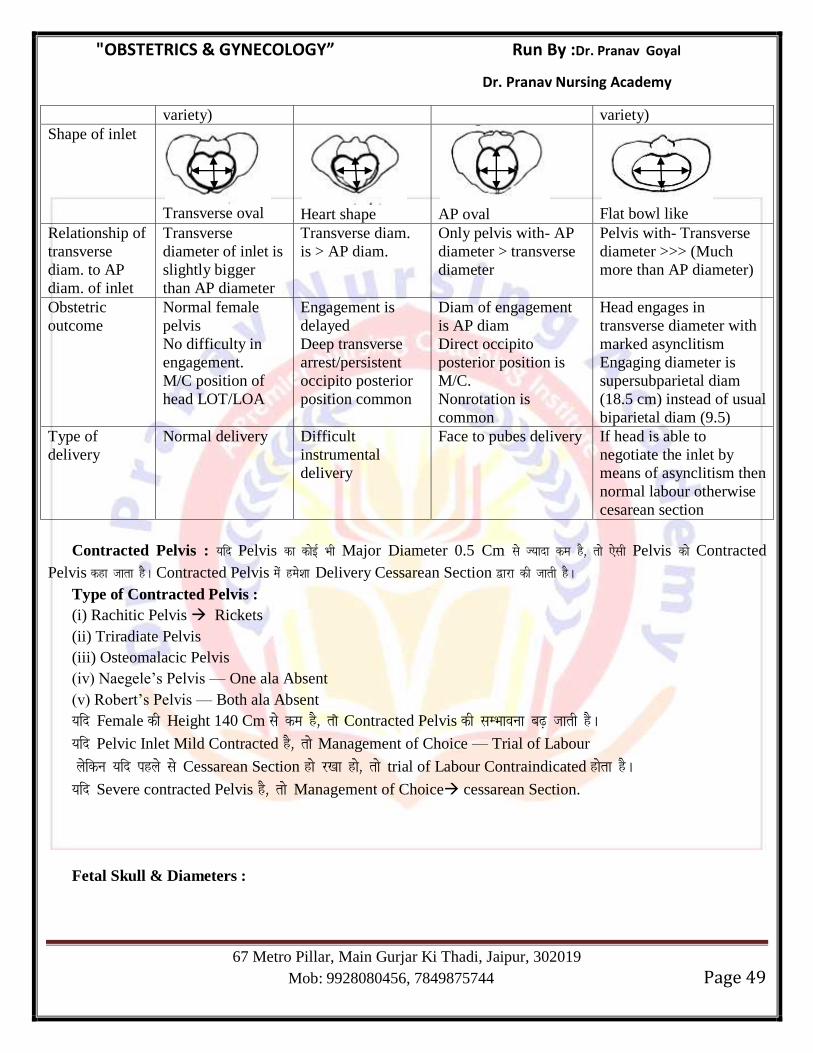
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 49
variety) variety)
Shape of inlet
Transverse oval
Heart shape
AP oval
Flat bowl like
Relationship of
transverse
diam. to AP
diam. of inlet
Transverse
diameter of inlet is
slightly bigger
than AP diameter
Transverse diam.
is > AP diam.
Only pelvis with- AP
diameter > transverse
diameter
Pelvis with- Transverse
diameter >>> (Much
more than AP diameter)
Obstetric
outcome
Normal female
pelvis
No difficulty in
engagement.
M/C position of
head LOT/LOA
Engagement is
delayed
Deep transverse
arrest/persistent
occipito posterior
position common
Diam of engagement
is AP diam
Direct occipito
posterior position is
M/C.
Nonrotation is
common
Head engages in
transverse diameter with
marked asynclitism
Engaging diameter is
supersubparietal diam
(18.5 cm) instead of usual
biparietal diam (9.5)
Type of
delivery
Normal delivery Difficult
instrumental
delivery
Face to pubes delivery If head is able to
negotiate the inlet by
means of asynclitism then
normal labour otherwise
cesarean section
Contracted Pelvis : ;fn Pelvis dk dksbZ Hkh Major Diameter 0.5 Cm ls T;knk de gS] rks ,slh Pelvis dks Contracted
Pelvis dgk tkrk gSA Contracted Pelvis esa ges’kk Delivery Cessarean Section }kjk dh tkrh gSA
Type of Contracted Pelvis :
(i) Rachitic Pelvis Rickets
(ii) Triradiate Pelvis
(iii) Osteomalacic Pelvis
(iv) Naegele‘s Pelvis — One ala Absent
(v) Robert‘s Pelvis — Both ala Absent
;fn Female dh Height 140 Cm ls de gS] rk s Contracted Pelvis dh lEHkkouk c<+ tkrh gSA
;fn Pelvic Inlet Mild Contracted gS] rks Management of Choice — Trial of Labour
ysfdu ;fn igys ls Cessarean Section gks j[kk gks] rks trial of Labour Contraindicated gksrk gSA
;fn Severe contracted Pelvis gS] rks Management of Choice cessarean Section.
Fetal Skull & Diameters :
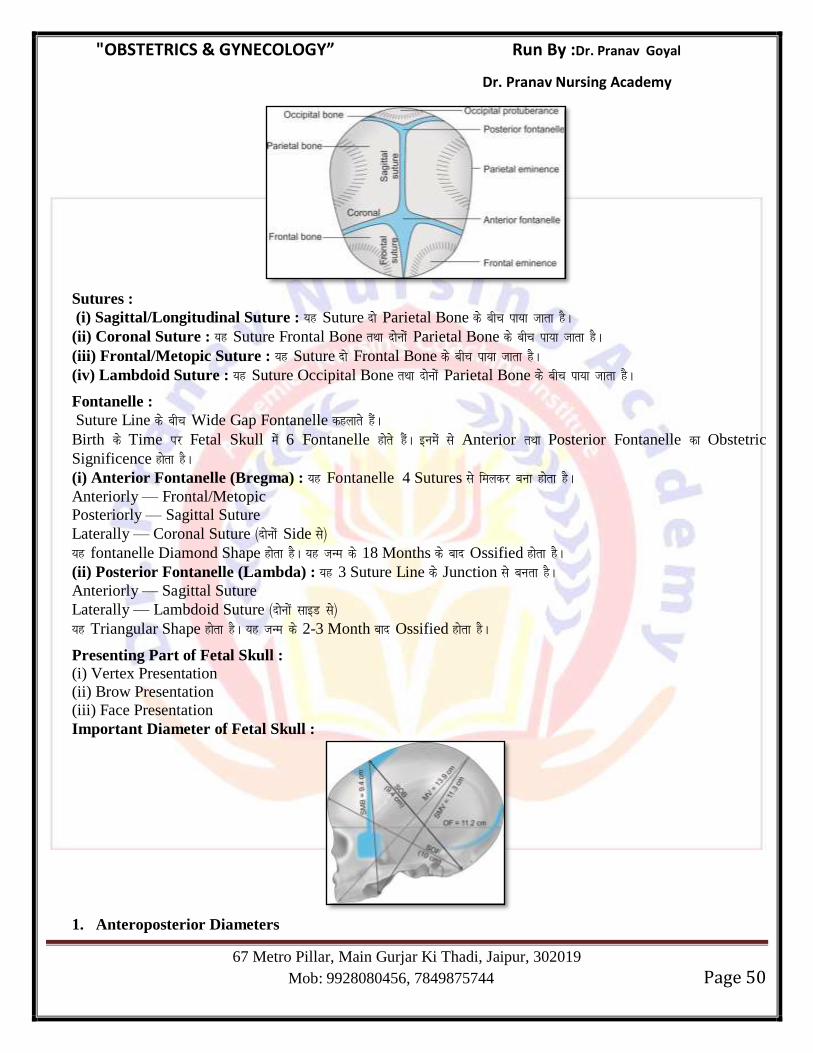
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 50
Sutures :
(i) Sagittal/Longitudinal Suture : ;g Suture nks Parietal Bone ds chp ik;k tkrk gSA
(ii) Coronal Suture : ;g Suture Frontal Bone rFkk nksuksa Parietal Bone ds chp ik;k tkrk gSA
(iii) Frontal/Metopic Suture : ;g Suture nks Frontal Bone ds chp ik;k tkrk gSA
(iv) Lambdoid Suture : ;g Suture Occipital Bone rFkk nksuksa Parietal Bone ds chp ik;k tkrk gSA
Fontanelle :
Suture Line ds chp Wide Gap Fontanelle dgykrs gSaA
Birth ds Time ij Fetal Skull esa 6 Fontanelle gksrs gSaA buesa ls Anterior rFkk Posterior Fontanelle dk Obstetric
Significence gksrk gSA
(i) Anterior Fontanelle (Bregma) : ;g Fontanelle 4 Sutures ls feydj cuk gksrk gSA
Anteriorly — Frontal/Metopic
Posteriorly — Sagittal Suture
Laterally — Coronal Suture ¼nksuksa Side ls½
;g fontanelle Diamond Shape gksrk gSA ;g tUe ds 18 Months ds ckn Ossified gksrk gSA
(ii) Posterior Fontanelle (Lambda) : ;g 3 Suture Line ds Junction ls curk gSA
Anteriorly — Sagittal Suture
Laterally — Lambdoid Suture ¼nksuksa lkbM ls½
;g Triangular Shape gksrk gSA ;g tUe ds 2-3 Month ckn Ossified gksrk gSA
Presenting Part of Fetal Skull :
(i) Vertex Presentation
(ii) Brow Presentation
(iii) Face Presentation
Important Diameter of Fetal Skull :
1. Anteroposterior Diameters
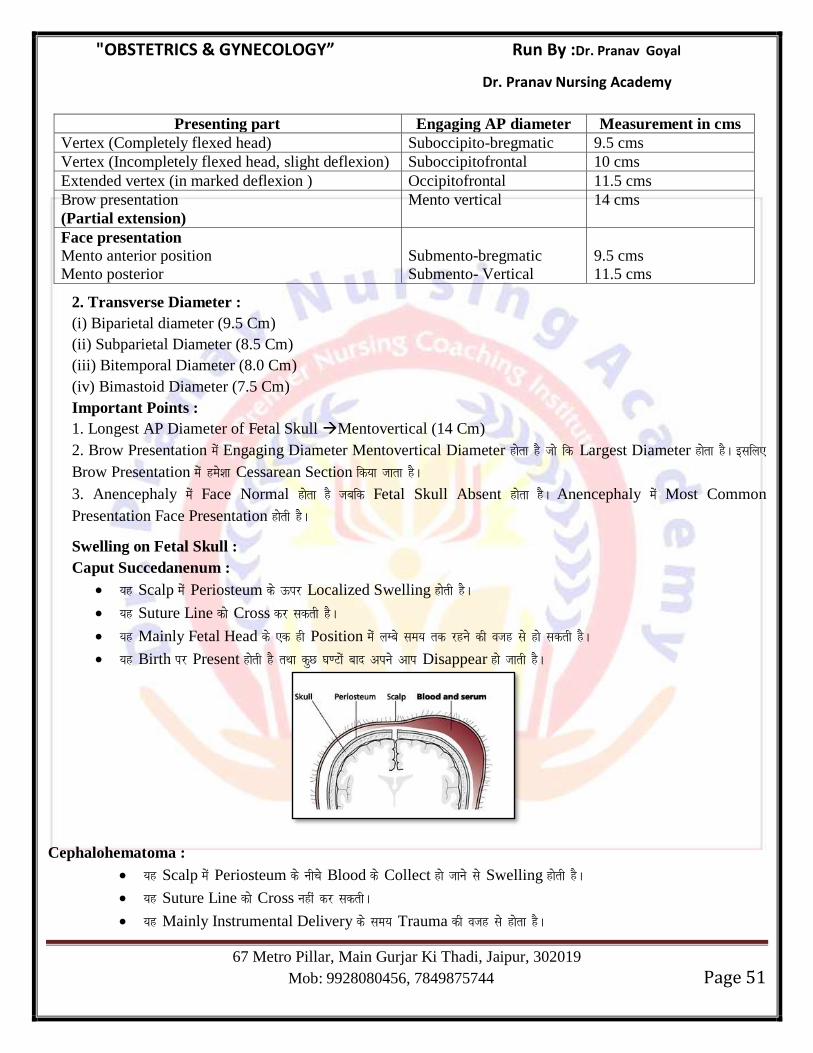
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 51
Presenting part Engaging AP diameter Measurement in cms
Vertex (Completely flexed head) Suboccipito-bregmatic 9.5 cms
Vertex (Incompletely flexed head, slight deflexion) Suboccipitofrontal 10 cms
Extended vertex (in marked deflexion ) Occipitofrontal 11.5 cms
Brow presentation
(Partial extension)
Mento vertical 14 cms
Face presentation
Mento anterior position
Mento posterior
Submento-bregmatic
Submento- Vertical
9.5 cms
11.5 cms
2. Transverse Diameter :
(i) Biparietal diameter (9.5 Cm)
(ii) Subparietal Diameter (8.5 Cm)
(iii) Bitemporal Diameter (8.0 Cm)
(iv) Bimastoid Diameter (7.5 Cm)
Important Points :
1. Longest AP Diameter of Fetal Skull Mentovertical (14 Cm)
2. Brow Presentation esa Engaging Diameter Mentovertical Diameter gksrk gS tks fd Largest Diameter gksrk gSA blfy,
Brow Presentation esa ges’kk Cessarean Section fd;k tkrk gSA
3. Anencephaly esa Face Normal gksrk gS tcfd Fetal Skull Absent gksrk gSA Anencephaly esa Most Common
Presentation Face Presentation gksrh gSA
Swelling on Fetal Skull :
Caput Succedanenum :
;g Scalp esa Periosteum ds Åij Localized Swelling gksrh gSA
;g Suture Line dks Cross dj ldrh gSA
;g Mainly Fetal Head ds ,d gh Position esa yEcs le; rd jgus dh otg ls gks ldrh gSA
;g Birth ij Present gksrh gS rFkk dqN ?k.Vksa ckn vius vki Disappear gks tkrh gSA
Cephalohematoma :
;g Scalp esa Periosteum ds uhps Blood ds Collect gks tkus ls Swelling gksrh gSA
;g Suture Line dks Cross ugha dj ldrhA
;g Mainly Instrumental Delivery ds le; Trauma dh otg ls gksrk gSA
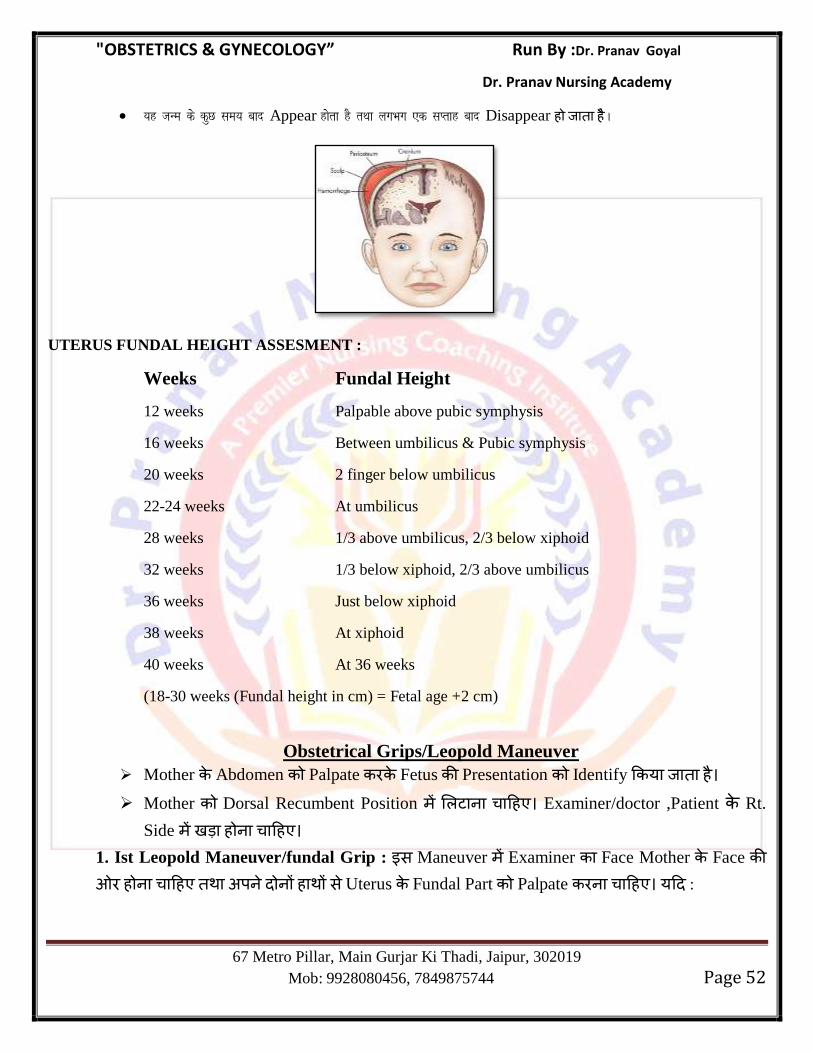
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 52
;g tUe ds dqN le; ckn Appear gksrk gS rFkk yxHkx ,d lIrkg ckn Disappear ह ह SA
UTERUS FUNDAL HEIGHT ASSESMENT :
Weeks Fundal Height
12 weeks Palpable above pubic symphysis
16 weeks Between umbilicus & Pubic symphysis
20 weeks 2 finger below umbilicus
22-24 weeks At umbilicus
28 weeks 1/3 above umbilicus, 2/3 below xiphoid
32 weeks 1/3 below xiphoid, 2/3 above umbilicus
36 weeks Just below xiphoid
38 weeks At xiphoid
40 weeks At 36 weeks
(18-30 weeks (Fundal height in cm) = Fetal age +2 cm)
Obstetrical Grips/Leopold Maneuver
Mother Abdomen Palpate Fetus Presentation Identify य ह
Mother Dorsal Recumbent Position ह Examiner/doctor ,Patient Rt.
Side ह ह
1. Ist Leopold Maneuver/fundal Grip : स Maneuver Examiner Face Mother Face ओ ह ह ह स Uterus Fundal Part Palpate ह य :
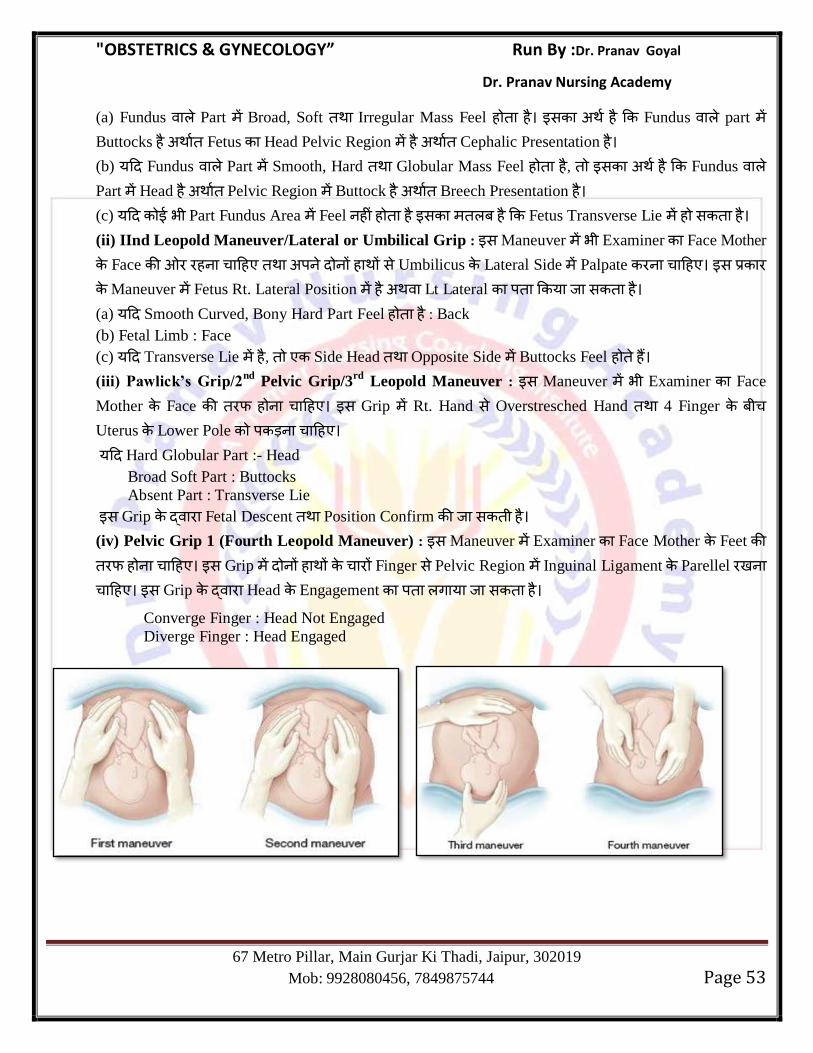
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 53
(a) Fundus Part Broad, Soft Irregular Mass Feel ह ह स ह Fundus part Buttocks ह Fetus Head Pelvic Region ह Cephalic Presentation ह
(b) य Fundus Part Smooth, Hard Globular Mass Feel ह ह , स ह Fundus Part Head ह Pelvic Region Buttock ह Breech Presentation ह
(c) य भ Part Fundus Area Feel ह ह ह स ह Fetus Transverse Lie ह स ह
(ii) IInd Leopold Maneuver/Lateral or Umbilical Grip : स Maneuver भ Examiner Face Mother
Face ओ ह ह ह स Umbilicus Lateral Side Palpate ह स
Maneuver Fetus Rt. Lateral Position ह Lt Lateral य स ह
(a) य Smooth Curved, Bony Hard Part Feel ह ह : Back
(b) Fetal Limb : Face
(c) य Transverse Lie ह , Side Head Opposite Side Buttocks Feel ह ह (iii) Pawlick’s Grip/2
nd Pelvic Grip/3
rd Leopold Maneuver : स Maneuver भ Examiner Face
Mother Face ह ह स Grip Rt. Hand स Overstresched Hand 4 Finger
Uterus Lower Pole ह
य Hard Globular Part :- Head
Broad Soft Part : Buttocks
Absent Part : Transverse Lie
स Grip Fetal Descent Position Confirm स ह (iv) Pelvic Grip 1 (Fourth Leopold Maneuver) : स Maneuver Examiner Face Mother Feet ह ह स Grip ह Finger स Pelvic Region Inguinal Ligament Parellel ह स Grip Head Engagement ग य स ह
Converge Finger : Head Not Engaged
Diverge Finger : Head Engaged
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 54
Chapter 6
Normal & Abnormal Labor Labor :Labor ह य ह , स Conception Viable Product गभ स Vagina ह य ह
Parturient : A patient in Labor.
Parturition : Process of giving Birth.
Normal Labor (EUTOCIA) : Labor is called Normal if it fulfills the following criteria.
i) Spontaneons in onset and at term
ii) With Vertex Presentation
iii) Without Prolongation.
iv) Natural termination with Minimal aids.
v) Without having any complication affecting the health of Mother & Baby.
Abnormal Labor (DYSTOCIA) : Any deviation from the definition of Normal Labor is called
abnormal Labor.
Pre Labor :
» It is premonitory stage of Labor and begins 2-3 weeks before the onset of true Labor in
Primigravida and few days before in Multigravida.
» It is associated with Increase oxytocin receptors in myometrium.
Following changes seen in Prelabor :
a) Lightening : Term Fetus Presenting Part Maternal Pelvis Descent ह स Fundal height Decrease ह ह , सस Mother Diaphragm Pressure ह ह औ
Mother Relax Feel ह ह स Lightening ह ह
b) Cervical Ripening : Softening of Cervix
Difference b/w True Labor Pain & False Labor Pain
Features True Labor pain False Labor pain
Cevical changes (Dilatation and
effacement)
Present Absent
Frequency and duration of contractions Regular and gradually increase Irregular
Pain Lower abdomen and back,
radiating to thighs
Lower abdomen only
Bag of water Formed Absent
Show Present Absent
Relief with enema/Sedation No Yes
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 55
True Labor : Onset of True Labor Pain characterized by :
» Appearance of True Labor Pain.
» Appearance of Show.
True Labor is divided in four functional Stages-
Stages of True Labor :
1. First Stage : यह Stage True Labor Pain स Start ह ह Cervix Full Dilatation स
ह ह (Full Dilatation of Cervix = 10 cm)
2. Second Stage : यह Stage full Dilation of Cervix स Start ह ह स Stage Fetus Mother
स ह ह Primipara यह Stage 1 hr. Multipara 30 Min. ह ह
3. Third Stage : यह Stage Fetus Delivery Start ह ह स Stage Placenta Fetal
Membrane Uterus स ह ह Primipara Multipara यह Stage गभग 15-25 Min.
ह ह
4. Fourth Stage : यह Stage Placenta Delivery गभग Observation Period ह ह
Physiological chills are experienced by the Mother in this Stage.
Uterine Contraction :
» Braxton Hicks Contraction : यह Painless, Irregular, Involuntary, Spasmodic Uterine
Contraction ह ह Mainly 2nd
Trimester Start ह ह Contraction ह स Cervix Dilatation ह ह ह
» True Labor Pain : यह Contraction Painful ह ह स ह स Cervix Dilatation ह ह
» Pacemaker of Uterine Contraction Cornu ह ह (Rt Pacemaker Predominant over
the left)
» Contraction mainly fundus Part स Start ह ओ ह
Intrauterine Pressure
Event Intrauterine pressure
Contractions are palpable 10 mm of Hg
Contractions are painful 15 mm of Hg
Cervix dilates 15 mm of Hg
Fundus cannot be indented 40 mm of Hg
1st stage of Labor 40-50 mm of Hg
2nd
and 3rd
stage of Labor 100-120 mm of Hg
Adequate Uterine Contraction :3 Contraction in 10 Min. each lasting for 45 Sec. & causing Intra
Uterine Pressure of 65-75 mm of Hg or 220 montevideo Unit.
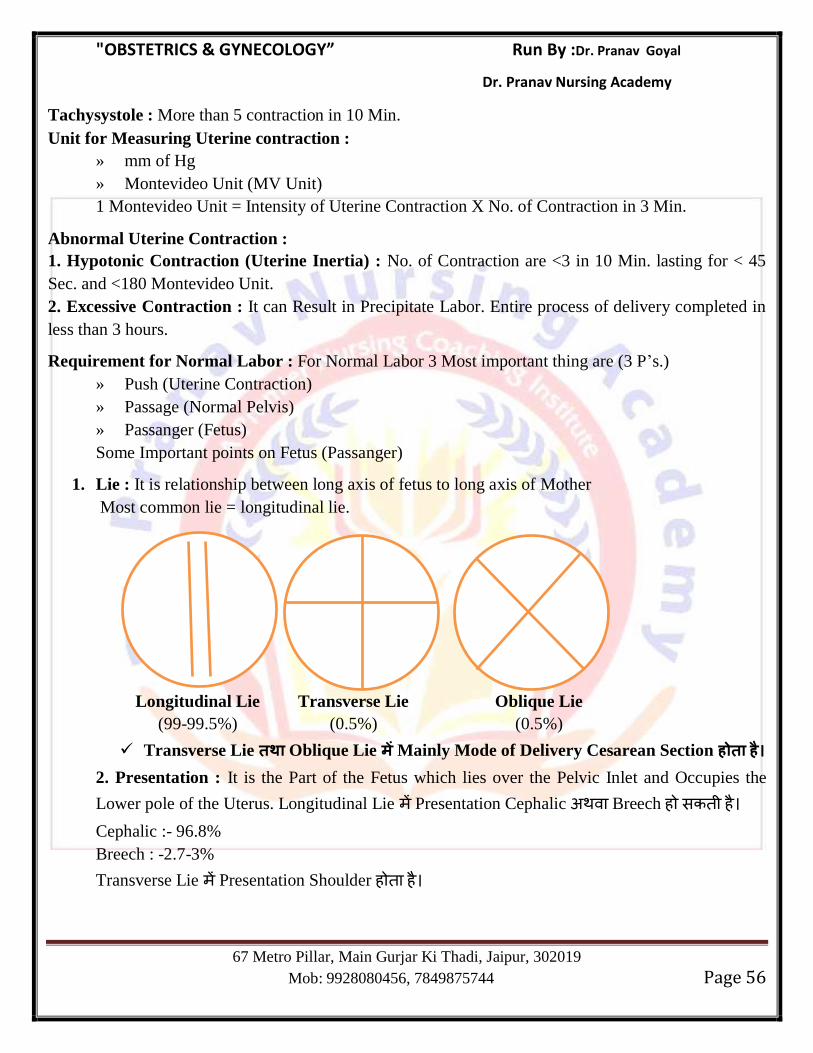
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 56
Tachysystole : More than 5 contraction in 10 Min.
Unit for Measuring Uterine contraction :
» mm of Hg
» Montevideo Unit (MV Unit)
1 Montevideo Unit = Intensity of Uterine Contraction X No. of Contraction in 3 Min.
Abnormal Uterine Contraction :
1. Hypotonic Contraction (Uterine Inertia) : No. of Contraction are <3 in 10 Min. lasting for < 45
Sec. and <180 Montevideo Unit.
2. Excessive Contraction : It can Result in Precipitate Labor. Entire process of delivery completed in
less than 3 hours.
Requirement for Normal Labor : For Normal Labor 3 Most important thing are (3 P‘s.)
» Push (Uterine Contraction)
» Passage (Normal Pelvis)
» Passanger (Fetus)
Some Important points on Fetus (Passanger)
1. Lie : It is relationship between long axis of fetus to long axis of Mother
Most common lie = longitudinal lie.
Longitudinal Lie Transverse Lie Oblique Lie
(99-99.5%) (0.5%) (0.5%)
Transverse Lie Oblique Lie Mainly Mode of Delivery Cesarean Section
2. Presentation : It is the Part of the Fetus which lies over the Pelvic Inlet and Occupies the
Lower pole of the Uterus. Longitudinal Lie Presentation Cephalic Breech ह स ह
Cephalic :- 96.8%
Breech : -2.7-3%
Transverse Lie Presentation Shoulder ह ह
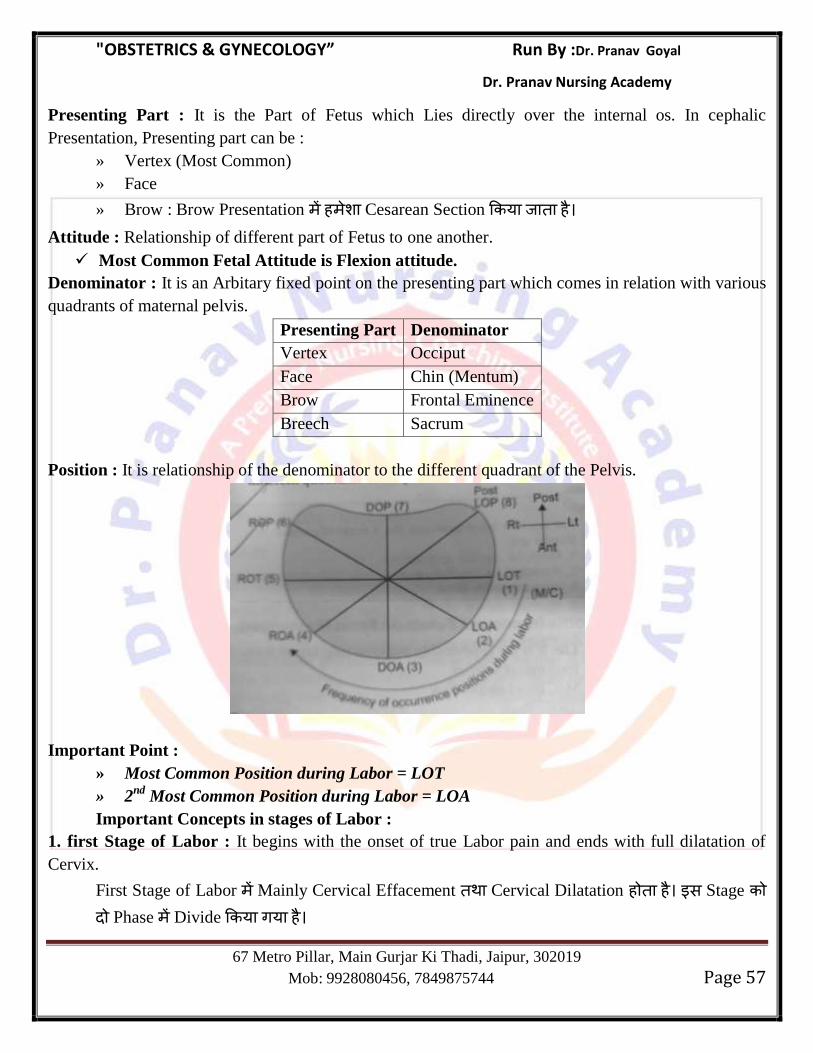
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 57
Presenting Part : It is the Part of Fetus which Lies directly over the internal os. In cephalic
Presentation, Presenting part can be :
» Vertex (Most Common)
» Face
» Brow : Brow Presentation ह Cesarean Section य ह
Attitude : Relationship of different part of Fetus to one another.
Most Common Fetal Attitude is Flexion attitude.
Denominator : It is an Arbitary fixed point on the presenting part which comes in relation with various
quadrants of maternal pelvis.
Presenting Part Denominator
Vertex Occiput
Face Chin (Mentum)
Brow Frontal Eminence
Breech Sacrum
Position : It is relationship of the denominator to the different quadrant of the Pelvis.
Important Point :
» Most Common Position during Labor = LOT
» 2nd
Most Common Position during Labor = LOA
Important Concepts in stages of Labor :
1. first Stage of Labor : It begins with the onset of true Labor pain and ends with full dilatation of
Cervix.
First Stage of Labor Mainly Cervical Effacement Cervical Dilatation ह ह स Stage Phase Divide य गय ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 58
a) Latent Phase
b) Active Phase
Difference B/W Latent Phase & Active Phase
Latent Phase Active Phase
It starts at the point at which the
mother percieves true about pains and
ends when cervix is 5 cm dilated.
It begins with cervical dilation of ≥ 6 with regular uterine
contractions
Its duration in primiparous is 12 hours
and 8 hour in multiparous females
Normal minimum cervical dialation rate of 1.2 cm/hr for
primiiparous and 1.5 cm/hr for multiparous women.According
to WHO Minimum dialation should be 1 cm/hr
Mainly concerned with cervical
effacement and dilatation
Mainly concerned with cervical dilatation and descent of
fetal head
Descent of fetal head
Primiparous = 1cm/hr
Multiparous = 2cm/hr
Abnormalities of Latent Phase :
Prolonged Latent Phase :latent Phase Prolonged ह ह य -
i) Greater than 20 hrs. in primipara.
ii) Greater than 14 hrs. in Multipara.
Causes of Prolonged latent Phase :
(i) Excessive sedation/Epidural analgesia
(ii) Poor Cervical Condition (Thick Uneffaced or Undilated)
(iii) False Labor (Most Common Cause in Multipara)
Management :
Therepeutic Rest : 15 mg Morphine is given Intramuscularly. Most of the patient are asleep
with in 1 hrs. & awake 4-5 hr. later.
Abnormalities of Active Phase : Cervix 6 cm य सस य Dilate ह ह , Active Phase Start
ह ह Active Phase Mainly 2 event ह ह
a) Dilatation of Cervix
b) Descent of Fetal Head
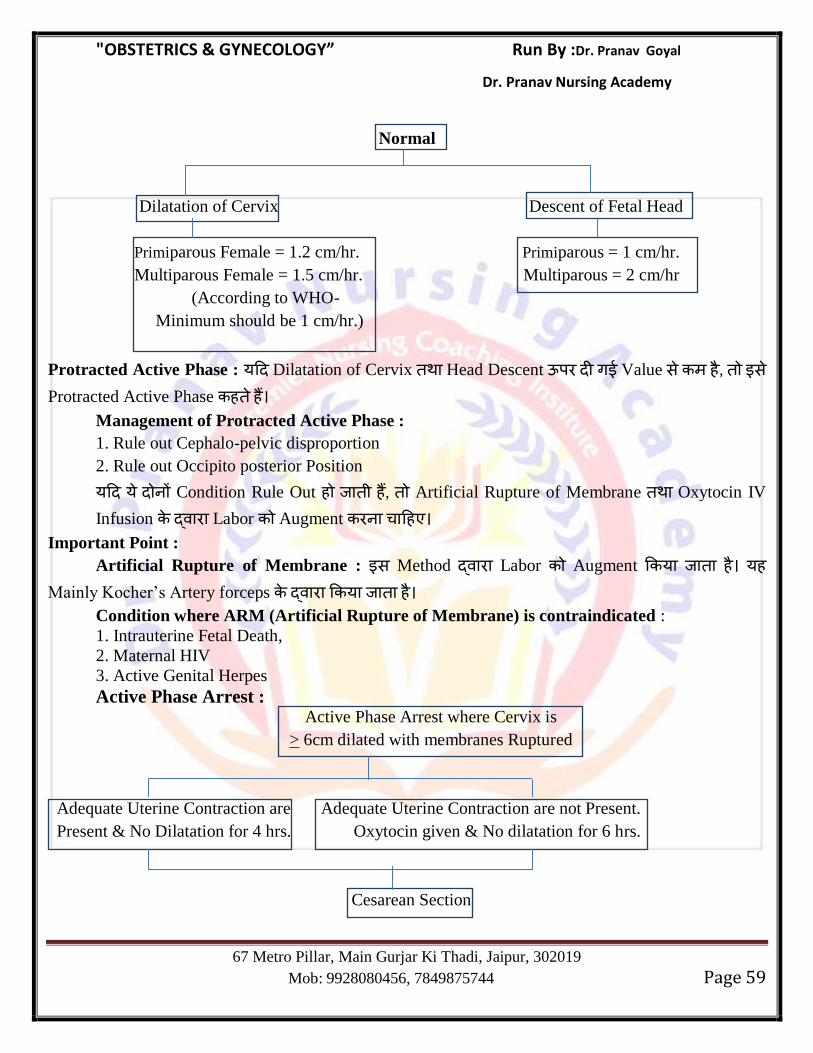
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 59
Normal
Dilatation of Cervix Descent of Fetal Head
Primiparous Female = 1.2 cm/hr. Primiparous = 1 cm/hr.
Multiparous Female = 1.5 cm/hr. Multiparous = 2 cm/hr
(According to WHO-
Minimum should be 1 cm/hr.)
Protracted Active Phase : य Dilatation of Cervix Head Descent ऊ ग Value स ह , स Protracted Active Phase ह ह
Management of Protracted Active Phase :
1. Rule out Cephalo-pelvic disproportion
2. Rule out Occipito posterior Position
य य Condition Rule Out ह ह , Artificial Rupture of Membrane Oxytocin IV
Infusion Labor Augment ह
Important Point :
Artificial Rupture of Membrane : स Method Labor Augment य ह यह
Mainly Kocher‘s Artery forceps य ह
Condition where ARM (Artificial Rupture of Membrane) is contraindicated :
1. Intrauterine Fetal Death,
2. Maternal HIV
3. Active Genital Herpes
Active Phase Arrest : Active Phase Arrest where Cervix is
> 6cm dilated with membranes Ruptured
Adequate Uterine Contraction are Adequate Uterine Contraction are not Present.
Present & No Dilatation for 4 hrs. Oxytocin given & No dilatation for 6 hrs.
Cesarean Section
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 60
Concept Box
1st Situation
A G2P1 is admitted in Labor at 8 AM on Monday.
P/V findings = Cervix 2 cms dilated, 20% effaced
At 10 PM findings are: Cervix=3cms dilated,60% effaced.
FHR=Regular, 140-146 bpm,
Membranes = intact.
What is next step of management
Solution
-This female is multiparous
-Stage of Labor = Latent phase (as cervix is < 6 cms dilated)
-Total duration = 8AM to 10 PM = 14 hours
-Latent phase is said to be prolonged if it is 14 hours in multiparous female
-Hence diagnosis is :- Prolonged latent phase
-Management :- Sedation/Therapeutic Rest
2nd
Situation
A G2P1 is admitted in Labor at 8 AM on Monday.
P/V findings = Cervix 2 cms dilated, 20% effaced
At 12 PM(midnoon):Cervix 6 cms dilated,80% effaced.
At 3 PM = Cervix 8 cms dilated, membranes intact
FHR is 140, Regular uterine contractions are present.
What is next step of management
Solution
Here again
female is multiparous
When she was admitted, she was in latent phase (cervix 2 cms dilated) but it ended in 4 hours
(at 12 PM = cervix is 6 cms dilated). Hence latent phase was normal. Now she came in active
phase at 12 PM. Since she is a multigravida, dilation of cervix should be 1.5 cm/hr (In 3 hours =
4.5 cms, already at 12 pm she is 6 cms dilated therefore by 3 pm she should be 6+4.5 = 10 cms,
i.e. fully dilated ). But here she is only 8 cms dilated, i.e. it is a case of protracted active phase.
Management should be ARM followed by Oxytocin.
3rd
Situation
A G2P1 female is admitted in Labor at 8 AM on Monday.
P/V findings = Cervix 6 cms dilated, 100% effaced
Membranes ruptured, No meconium
FHR = 140-148, Regular uterine contractions = Adequate
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 61
At 12 PM(midnoon): Same finding
Next step of management
Solution
Now here patient is :
-Multiparous
-She is admitted in active phase (cervix 6 cms dilated) at 8 am and 12 pm inspite of good uterine
contractions and membranes ruptured, there is no dilatation for 4 hours, hence diagnosis is
arrest of active phase
Management is cesarean section.
Second Stage of Labor : It begins from full dilatation of Cervix and end with expulsion of
Fetus. Second Stage of Labor Mother Bearing Down Effort Role Uterine contraction स य Important ह ह
Prolonged Second Stage
Normal Prolonged
Primiparous 1 hrs. 2 hrs.
Multiparous 30 Min. 1 hrs.
Management of Prolonged Second Stage of Labor : It depends on station of Fetal Head.
If Station of Fetal Head
At or Below +2 Station Above + 2 Station
Delivery by Forceps Vaccum Delivery by Cesarean section
Second Stage Arrest :
Primiparous : 3 hrs.
Multiparous : 2 hrs.
Second Stage Arrest Obstructed Labor भ ह ह Obstructed Labor Management of
Choice = Cesarean Section.
Mechanism of Labor : Mechanism of Labor is defined as the manner in which the fetus adjust
itself to pass through the parturient canal with minimal difficulty.
There are 8 cardinal movements of the Head in Normal Labor.
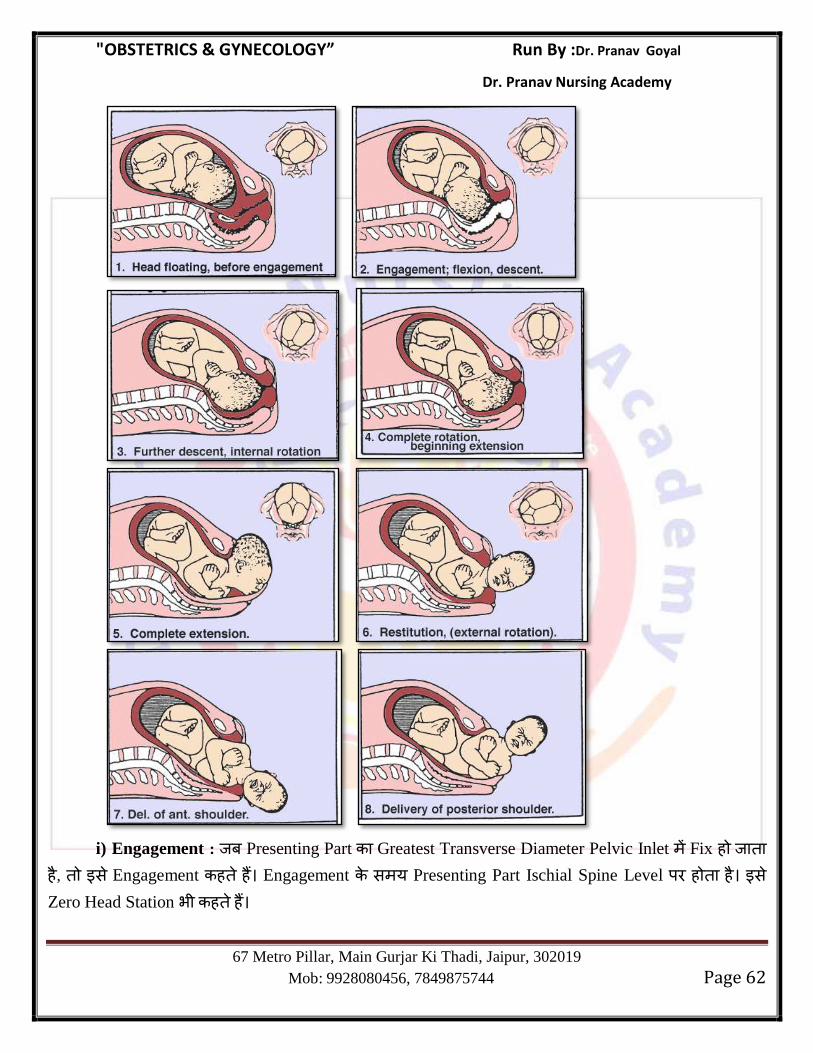
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 62
i) Engagement : Presenting Part Greatest Transverse Diameter Pelvic Inlet Fix ह ह , स Engagement ह ह Engagement स य Presenting Part Ischial Spine Level ह ह स Zero Head Station भ ह ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 63
Head Station 0 (+4 to –4) य Head Ischial Spine स ऊ ह , स –ve स Denote ह य
Ischial Spine स ह , स +ve स Denote ह
य Head –ve Station ह Ischial Spine स ऊ ह , स ह Delivery भ य स य ह औ य Head +ve Station ह Ischial Spine स ह स ह ह स य Delivery ह ह
Multipara Female Engagement, Labor स य ह Late Ist Stage य at the time of
Rupture of Membrane ह ह
Nullipara Female Engagement गभग 38 Weeks ह ह
Causes of Nonengagement of Head in nullipara female : -
a) Malpresentation/Occipitoposterior Position /deflexed Head.
b) Cephalopelvic Disproportion
c) Placenta Previa/Tumor in Lower Uterine segment.
d) Tumor of Fetal neck, cord around neck
e) Hydrocephalus
f) Polyhydroamnios
g) Distended Bladder & Rectum
ii) Descent : यह Natural Process ह स Fetus Downward Movement ह ह Labor Pain
Mother Bearing Down effort ह Descent Promote ह स Universal Step भ ह ह य Descent Continuous Process ह Fetus Delivery Continous सभ Stage ह ह
iii)Flexion : स Stage Pelvis Soft Tissues Resistance ह स Fetal Head Flexion ह ह सस Fetal Chin, Chest ह
iv) Internal Rotation :
Internal Rotation Ischial Spine (Zero station) ह ह
Upper Side Uterine Contraction Lower Side Pelvic Tissues Resistance ह
स Rotation ह ह
यह Fetal Head Rotation Clockwise direction ह ह Distance 1/8 ह ह
य Head Neck स ह ह स Head Rotation स Neck भ Clockwise Direction Twist/ Torsion ह ह
v) Crowning : Internal Rotation Fetal Head just Pubic Symphysis ह ह यह स Fetal Head Ist Time Visualize ह ह
vi) Extension : यह Most important Movement ह स Fetal Head Delivery ह ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 64
vii) Restitution :
Head Internal Rotation स य Neck Twisting ह , Restitution Movement Relieve ह ह
Direction Internal Rotation Opposite ह ह anti Clockwise Distance 1/8 ह ह
viii) External Rotation : Head Restitution Shoulder Externally rotate ह ह Expulsion : Head Shoulder Delivery Rest of the Body स स ह ह
Second Stage management Approach :
1. Provide Lithotomy Position with Perineal care.
2. Encourage Bearing Down efforts by Mother.
3. Monitor Uterine Contraction with Base line FHR monitoring.
4. Promote Flexion by putting force on Perineum.
5. Episiotomy if required.
6. Umbilical cord clamping & cutting.
Partogram : Partogram is the best method to access progress of Labor.
Partogram is a graphical recording of stages of Labor including cervical dilatation, descent &
rotation of the Head.
Various Partograph have been made.
1. Friedman Curve : Friedman Ist Stage of Labor Stage Divide य ह :- (a) latent Phase
(b) Active Phase.
Friedman स >3 cm Cervix Dilatation Active Phase Start ह ह Normal Labor Cervical dilatation Pattern Latent Active Phase Sigmoid Curve ह ह
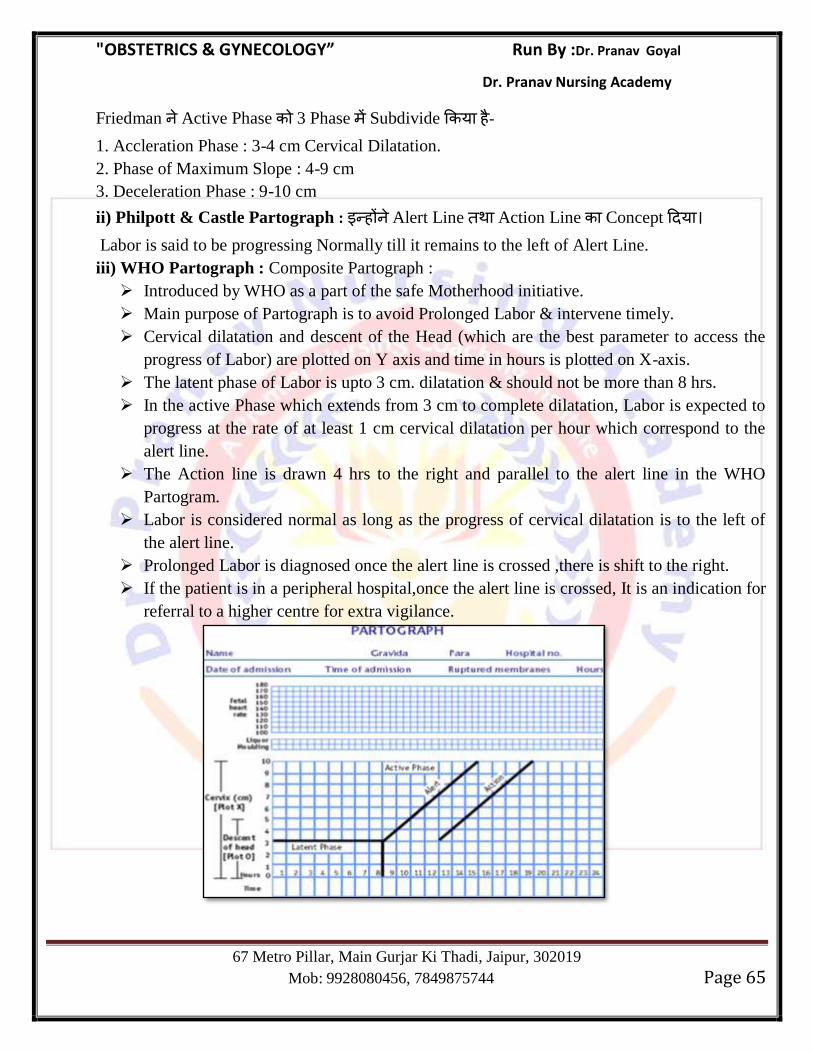
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 65
Friedman Active Phase 3 Phase Subdivide य ह - 1. Accleration Phase : 3-4 cm Cervical Dilatation.
2. Phase of Maximum Slope : 4-9 cm
3. Deceleration Phase : 9-10 cm
ii) Philpott & Castle Partograph : ह Alert Line Action Line Concept य
Labor is said to be progressing Normally till it remains to the left of Alert Line.
iii) WHO Partograph : Composite Partograph :
Introduced by WHO as a part of the safe Motherhood initiative.
Main purpose of Partograph is to avoid Prolonged Labor & intervene timely.
Cervical dilatation and descent of the Head (which are the best parameter to access the
progress of Labor) are plotted on Y axis and time in hours is plotted on X-axis.
The latent phase of Labor is upto 3 cm. dilatation & should not be more than 8 hrs.
In the active Phase which extends from 3 cm to complete dilatation, Labor is expected to
progress at the rate of at least 1 cm cervical dilatation per hour which correspond to the
alert line.
The Action line is drawn 4 hrs to the right and parallel to the alert line in the WHO
Partogram.
Labor is considered normal as long as the progress of cervical dilatation is to the left of
the alert line.
Prolonged Labor is diagnosed once the alert line is crossed ,there is shift to the right.
If the patient is in a peripheral hospital,once the alert line is crossed, It is an indication for
referral to a higher centre for extra vigilance.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 66
Induction of Labor :
Induction : Stimulation of contraction before the spontaneous onset of Labor.
Normally cervix closed Uneffaced ह ह स Induction of Labor स ह Cervix Soft
य ह स Process Cervical Ripening ह ह Before Labor is induced, Bishop scoring is done to access whether induction will be successful
or not.
BISHOP Score : Bishop score is a quantitative method for prediction of successful induction of Labor.
Bishop score includes the following Parameter.
Cervical Dilatation
Cervical Position
Cervical Effacement
Cervical Consistency
Head Station
Modified Bishop Score :
स Scoring Cervical Effacement गह Cervical Length ह य
Category Maximum Score 2 ह ह Maximum Score 10 ह ह
90% of patient Bishop Score 6-8 ह ह , 6 hrs. Delivery ह ह
Score य <6 ह ह , Delivery Unpredictable ह ह
Score Dilatation
(cm)
Length of
cervix
Station Cervical
consistency
Cervical position
0 0 2 cm -2 Firm Posterior
1 1cm 1 cm -1 Soft Midposition
2 2 cm < 0.5 cm 0 Soft and Stretchable Anterior
Cervical Ripening : Ripening of Cervix is changing the cervical matrix from sol to gel state by
dissolving the collagen bundles, ultimately the cervix becomes soft.
Technique for Cervical Ripening
Pharmacological method Non pharmacological method
Prostaglandin
-Dinoprostone gel (PGE2)
-It is the gold standard for cervical ripening
-Misoprostol (PGE1) tablet
(Vaginal or oral)
Stripping the membrane
Steroid receptor antagonist
-Mifepristone
Mechanical dilators
-Osmotic dilators
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 67
-Onapristone -Ballon catheter/ Transcervical catheter placed
through internal os
Relaxin Extra amniotic saline infusion
Glyceryl trinitrate,isosorbide mononitrate
Absolute Contraindication of Induction of Labor
Absolute contraindication of induction of Labor
Severe degree of contracted pelvis
Cancer cervix
Cord prolapse in early Labor
Major malpresentations like transverse lie, brow, mentoposterior face
Previous uterine scar of hysterotomy, classical cesarean section, repair of uterine rupture
Active genital herpes
Grade II posterior, Grade III and Grade IV placenta previa
Relative contraindication
Fetal distress
Cervical fibroid
Impacted ovarian cyst in pouch of doughlas
Third Stage of Labor:Third Stage of Labor Fetus Expulsion Start ह ह स Stage Placenta Fetal Membrance Expulsion ह ह
Average Time taken = 15-20 Minute
With Active Management of Third Stage of Labor (AMTSL) = 5 Min.
If time taken more than 30 Minute Prolonged 3rd
Stage
Key Concepts
In AMTSL, placental separation is actively facilitated and uterine contraction are initiated to
reduce the incidence of third stage complications (like PPH)
In AMTSL- Duration of third stage reduced (to 5 minutes)
Less bleeding
Less changes of PPH
Less maternal mortality
Hence active management of third stage of Labor is preferred these days.
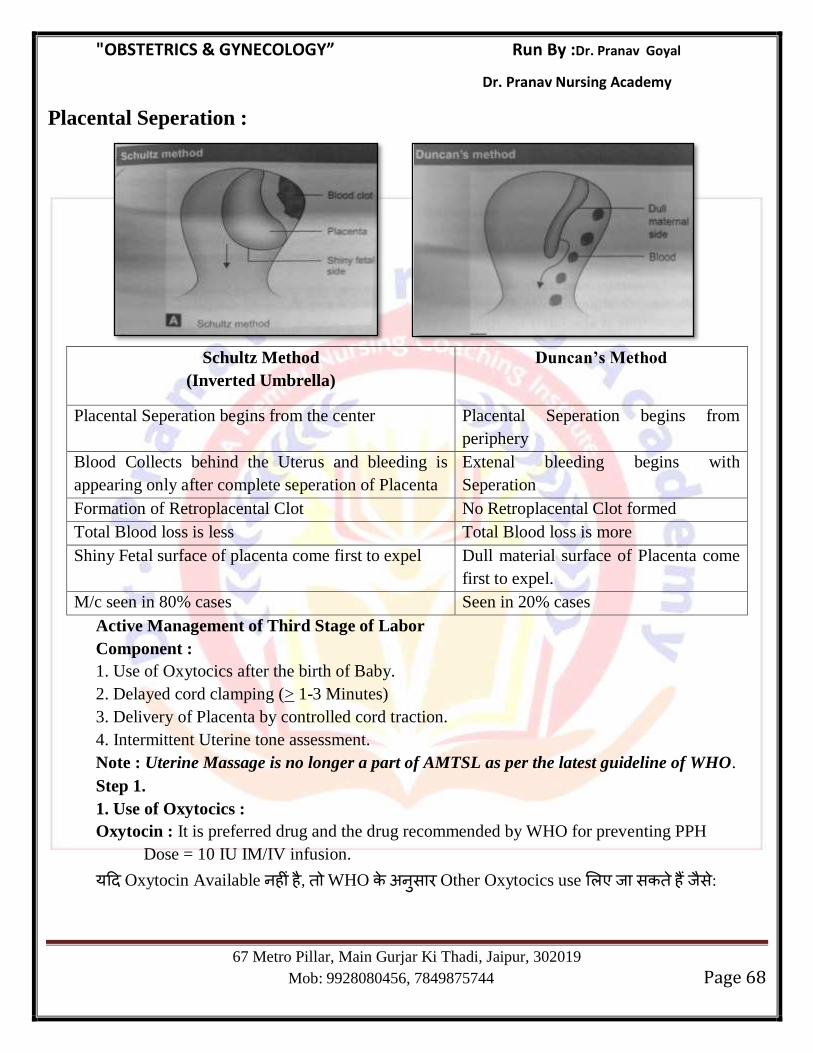
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 68
Placental Seperation :
Schultz Method
(Inverted Umbrella)
Duncan’s Method
Placental Seperation begins from the center Placental Seperation begins from
periphery
Blood Collects behind the Uterus and bleeding is
appearing only after complete seperation of Placenta
Extenal bleeding begins with
Seperation
Formation of Retroplacental Clot No Retroplacental Clot formed
Total Blood loss is less Total Blood loss is more
Shiny Fetal surface of placenta come first to expel Dull material surface of Placenta come
first to expel.
M/c seen in 80% cases Seen in 20% cases
Active Management of Third Stage of Labor
Component :
1. Use of Oxytocics after the birth of Baby.
2. Delayed cord clamping (> 1-3 Minutes)
3. Delivery of Placenta by controlled cord traction.
4. Intermittent Uterine tone assessment.
Note : Uterine Massage is no longer a part of AMTSL as per the latest guideline of WHO.
Step 1.
1. Use of Oxytocics :
Oxytocin : It is preferred drug and the drug recommended by WHO for preventing PPH
Dose = 10 IU IM/IV infusion.
य Oxytocin Available ह ह , WHO स Other Oxytocics use स ह स :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 69
a) Ergometrine (0.25 mg) or methylergometrine (0.20 mg) : यह Tetanic Contraction ह
स स Labor Induction Use ह ह
Side Effect : Transient Increase in BP
Contraindication :
1. Twin Pregnancy
2. Organic Health Disease
3. Preeclampsia
4. Eclampsia
5. Rh Negative Female.
b) Inj PGF-2α (Carboprost) : Dose 250 μg I/M
contraindicated in Bronchial Asthma.
यह Mainly Myometrium act ह स स Active Management of third stage of Labor
(AMTSL) PPH Use ह
c) PGE1 (Misoprostol) : Available as Tablet (600 mcg)
PGE1 Cervix Uterus Act ह स स Condition Use ह - 1. Ripening of Cervix
2. Induction of Labor
3. AMTSL
4. for Treating PPH
Side Effect : Nausea, vomitting, Abdominal Pain, Hyperpyrexia, Hypotension
य Previous Cesarean Section ह ह , Misoprostol contraindicated ह ह
d) Syntometrine : यह 5 Unit of Oxytocin 0.5 mg methargin combination ह ह
e) Carbetocin : Dose 100 mg I/V over 1 Minute.
यह Oxytocin Analogue ह ह स Function Oxytocin ह ह ह ह
Use : -Treatment of PPH,
-AMTSL
स Half Life Oxytocin य ह ह (85-100 min.)
f) Tranexamic Acid:यह Antifibrinolytic Drug ह , PPH Prevent Use ह
Step 2 : Delayed cord Clamping :
Delayed Cord Clamping ह Cord Fetus Delivery गभग 1-3 Min.
Clamp Early Cord Clamping ह Cord Fetus Delivery 1 Min. Clamp
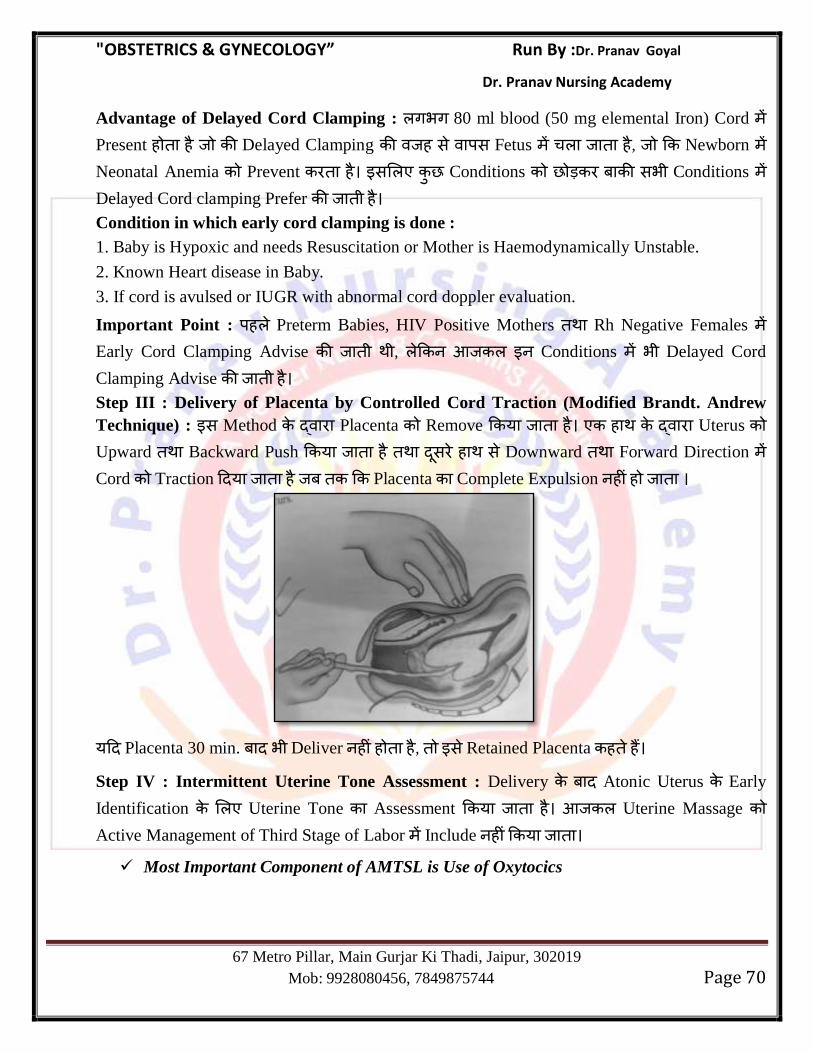
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 70
Advantage of Delayed Cord Clamping : गभग 80 ml blood (50 mg elemental Iron) Cord Present ह ह Delayed Clamping ह स स Fetus ह , Newborn Neonatal Anemia Prevent ह स Conditions सभ Conditions Delayed Cord clamping Prefer ह
Condition in which early cord clamping is done :
1. Baby is Hypoxic and needs Resuscitation or Mother is Haemodynamically Unstable.
2. Known Heart disease in Baby.
3. If cord is avulsed or IUGR with abnormal cord doppler evaluation.
Important Point : ह Preterm Babies, HIV Positive Mothers Rh Negative Females Early Cord Clamping Advise , Conditions भ Delayed Cord
Clamping Advise ह
Step III : Delivery of Placenta by Controlled Cord Traction (Modified Brandt. Andrew
Technique) : स Method Placenta Remove य ह ह Uterus Upward Backward Push य ह स ह स Downward Forward Direction Cord Traction य ह Placenta Complete Expulsion ह ह
य Placenta 30 min. भ Deliver ह ह ह , स Retained Placenta ह ह
Step IV : Intermittent Uterine Tone Assessment : Delivery Atonic Uterus Early
Identification Uterine Tone Assessment य ह Uterine Massage Active Management of Third Stage of Labor Include ह य
Most Important Component of AMTSL is Use of Oxytocics
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 71
4th
Stage of Labor :Fetus Placenta Delivery यह गभग 2-4 Observation
Time Period ह ह स Stage Newborn Airway Care, APGAR, Cord Care, Newborn
Assessment, weight, Tag य ह
Vital Monitoring
Fluid & Diet
Intake & Output Recording
COMPLICATION OF 3rd
STAGE OF LABOR :
Post Partum Haemorrhage (PPH) : Vaginal Delivery Genital Tract स 500 ml स य Blood Loss Cesarean Delivery 1000 ml स य Blood loss Postpartum Haemorrhage
(PPH) ह ह
Mild PPH if Blood loss 500-1000 ml
Moderate PPH > 1000 ml
Severe PPH > 2000 ml
Types of PPH :
Primary PPH Secondary PPH
य Haemorrhage Delivery 24
hrs. ह ह
य Haemorrhage Delivery 24 स 12 Weeks ह ह
Most Common Cause- Atonic PPH Most Common Cause- Retained Placenta
Causes of PPH : Cause of PPH = 4 T‘s
1. Atonic PPH (Tone) : यह Primary PPH Most Common Cause ह (90%)
Uterine Muscles Tone ह ह स Uterine Muscles Contraction Retraction ह ह ह सस Uterine Blood Vessels स ग Bleeding ह ह ह
2. Traumatic PPH (Trauma) :यह Mainly Delivery Genital Tract Injury ह स ह ह
3. Coagulopathy (Thrombosis) : Disseminated Intravascular Coagulation (DIC) Hypo-
fibrinogenemia Rare Cause ह
4. Other Cause (Tissue) : Retained Product of Conception (RPOC). Retained Placenta ह
स Mainly Secondary PPH ह ह
Predisposing Factor of PPH :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 72
Atonic PPH : Grand Multipara
Malnutrition/anemia
Previous H/o Atonic PPH
Overdistended Uterus due to
o Multiple Pregnancy
o Polyhydroamnios
o Macrosomia
Precipitate Labor (Labor < 3 hrs.)
Prolonged Labor (Labor > 12 hrs.)
Inadvertant use of Oxytocin
Use of General/Epidural Anaesthesia especially Halothane
Fibroid Uterus
Traumatic PPH :
Instrumental Delivery
Vaginal Birth after Cesarean(VBAC)
Face to Pubis delivery
Blood Coagulopathy :
Abruption
Sepsis
IUD
Severe preeclampsia
HELLP syndrome
Important Point :
Most Common Cause of PPH = Atonic Uterus
Most Common Cause of Primary PPH = Atonic Uterus
Most Common Cause of Secondary PPH = Retained Placenta
Structural Placental Abnormalities which can lead to PPH = Succenteuriate Placenta/Placenta
Bilobata.
Diagnosis of PPH :
Shock Index =
Normal Value = 0.5 – 0.7
य shock Index 0.9 – 1.1 Increase ह ह , Intensive Resuscitation य ह ह
Obstetric Shock Index (OSI) : During Pregnancy Normal Value = 0.7 – 0.8
OSI > 1 Indicate Massive Haemorrhage & need for Blood Transfusion.
Management of PPH :
First & Basic step in Management of PPH is resuscitation of Pt. which includes-
Securing I/V Lines
Volume Restroration by crystalloids (Normal saline/Ringer lactate)
Oxygen Inhalation
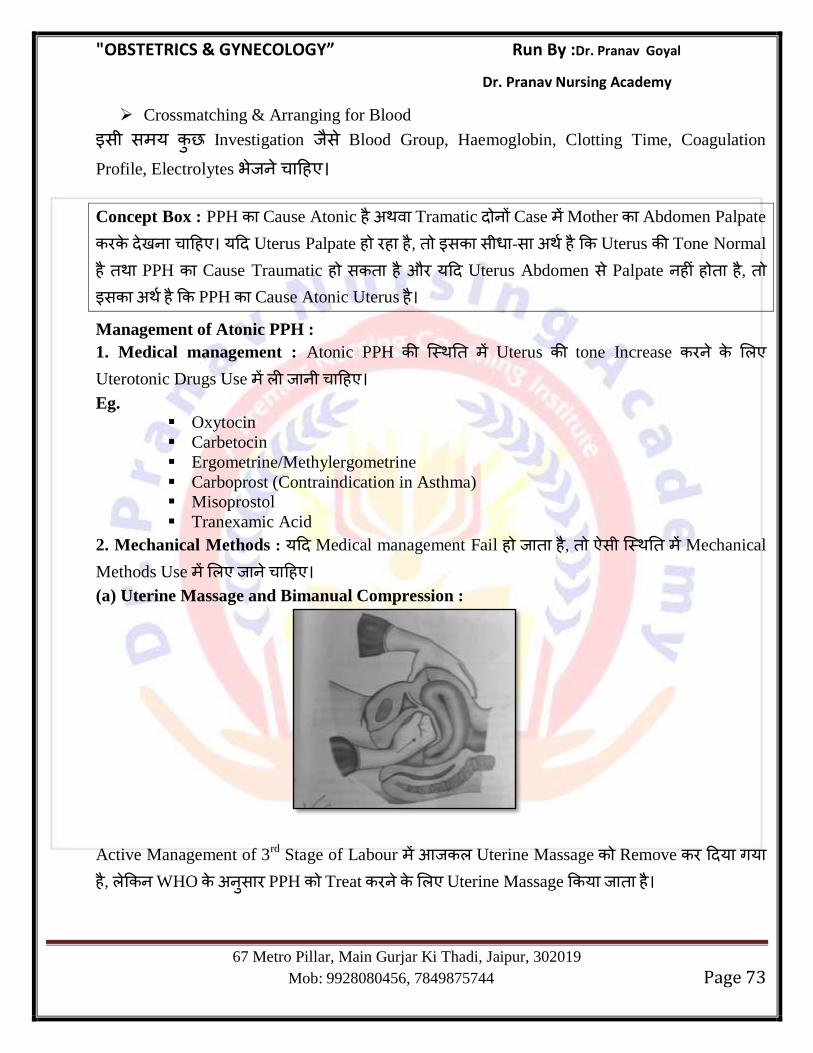
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 73
Crossmatching & Arranging for Blood
स स य Investigation स Blood Group, Haemoglobin, Clotting Time, Coagulation
Profile, Electrolytes भ ह
Concept Box : PPH Cause Atonic ह Tramatic Case Mother Abdomen Palpate
ह य Uterus Palpate ह ह ह , स स -स ह Uterus Tone Normal
ह PPH Cause Traumatic ह स ह औ य Uterus Abdomen स Palpate ह ह ह , स ह PPH Cause Atonic Uterus ह
Management of Atonic PPH :
1. Medical management : Atonic PPH Uterus tone Increase
Uterotonic Drugs Use ह
Eg. Oxytocin
Carbetocin
Ergometrine/Methylergometrine
Carboprost (Contraindication in Asthma)
Misoprostol
Tranexamic Acid
2. Mechanical Methods : य Medical management Fail ह ह , स Mechanical
Methods Use ह
(a) Uterine Massage and Bimanual Compression :
Active Management of 3rd
Stage of Labour Uterine Massage Remove य गय ह , WHO स PPH Treat Uterine Massage य ह
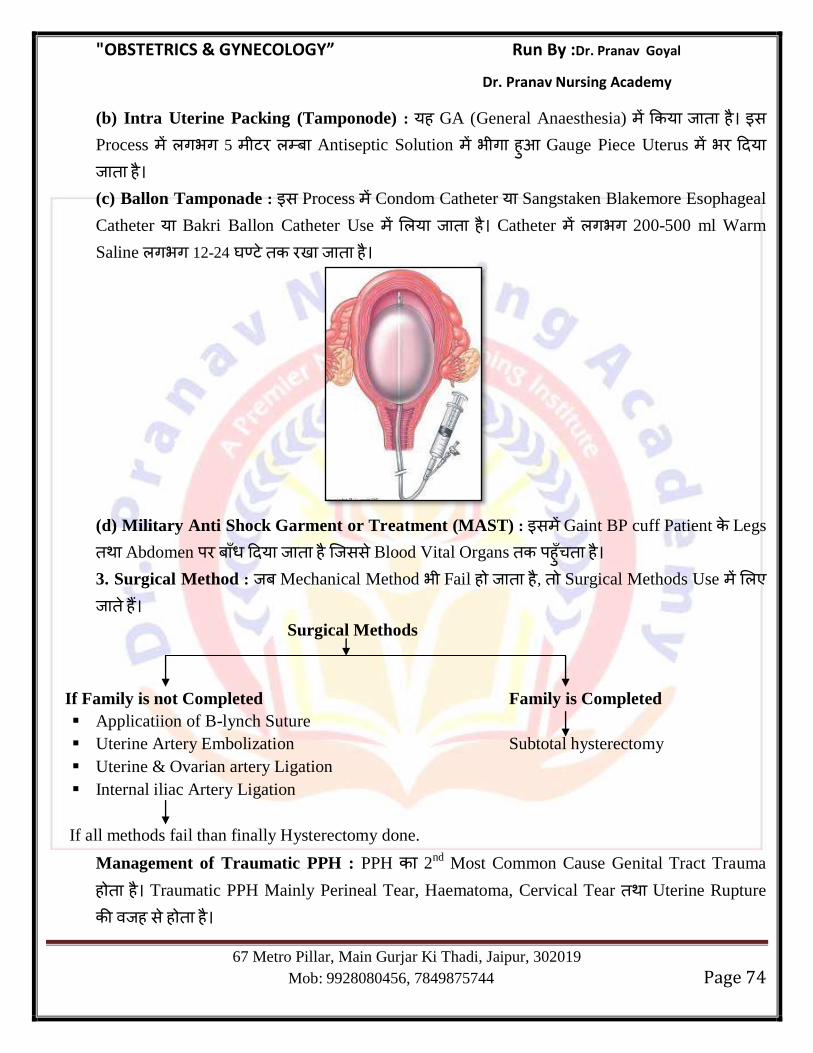
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 74
(b) Intra Uterine Packing (Tamponode) : यह GA (General Anaesthesia) य ह स
Process गभग 5 Antiseptic Solution भ ग ह Gauge Piece Uterus भ य ह
(c) Ballon Tamponade : स Process Condom Catheter य Sangstaken Blakemore Esophageal
Catheter य Bakri Ballon Catheter Use य ह Catheter गभग 200-500 ml Warm
Saline गभग 12-24 ह
(d) Military Anti Shock Garment or Treatment (MAST) : स Gaint BP cuff Patient Legs
Abdomen य ह सस Blood Vital Organs ह ह
3. Surgical Method : Mechanical Method भ Fail ह ह , Surgical Methods Use
ह
Surgical Methods
If Family is not Completed Family is Completed
Applicatiion of B-lynch Suture
Uterine Artery Embolization Subtotal hysterectomy
Uterine & Ovarian artery Ligation
Internal iliac Artery Ligation
If all methods fail than finally Hysterectomy done.
Management of Traumatic PPH : PPH 2nd Most Common Cause Genital Tract Trauma
ह ह Traumatic PPH Mainly Perineal Tear, Haematoma, Cervical Tear Uterine Rupture
ह स ह ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 75
Pelvic Haematoma :
Most Common Site for Pelvic Haematoma – Vulva
Most Common Artery to form Vulval Haematoma – Pudendal Artery
Most Common artery to form Vaginal Haematoma – Uterine Artery & its branches
Most Common Symptom of Pelvic Haematoma – Pain, Inability to Pass Urine.
Local Examination : Bluish Tender Swelling.
Management : य Samll Haematoma ह (< 3 cm) Cold Compression Analgesics Conservatively Manage य ह य Large Haematoma ह (>3 cm) Surgical
Management य ह Clot Drain ह य Bleeder Present ह , Figure of
8 Suture ग ह
Perineal Tear : Vagina स Anus Skin Soft Tissue Normal Vaginal
Delivery laceration/Tear ह ह , स Perineal Tear ह ह
Grade Description
1st degree Tear involving vaginal epithelium or skin only
2nd
degree Tear involving both vaginal skin and muscles (mediolateral episiotomy
corresponds to 2nd
degree perineal tear)
3rd
degree
Grade 3a
Grade 3b
Grade 3c
Involvement of anal sphincter
Tear of < 50% of external anal sphincter
Tear of ≥ 50% of external anal sphincter
Tear of external and internal anal sphincter
4th
degree Third degree tear along with involvement of anal epithelium
Note : Instrumental Delivery ह स Perineal Tear स भ ह Forceps Delivery
Ventouse Delivery Perineal Trauma स भ ह ह
Management of Perineal Tear :
First & Second Degree Tear :
Repaired in Labor Room.
Using Mainly Epidural Analgesia.
Technique : Vaginal Mucosa Repaired
Muscles Repaired
Vaginal Skin Repaired
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 76
Third & Fourth Degree Tear :
Anal Epithelium Repair
Internal Anal Sphinctor Repaired
External Anal Sphinctor Repaired
Vaginal Mucosa Repaired
Vaginal Muscle Repaired
Skin Repaired
3rd
& 4th
Degree Perineal Tear Repair स स 6 ह
Pregnancy Avoid ह
Cervical Tear : Most Common Site 3 ‗O‘ Clock Position followed by 9 ‗O‘ Clock Position.
Retained Placenta : य Placenta Delivery 30 Min. भ Uterine cavity स Expell ह ह ह , स Retained Placenta ह ह
Types
Category 1
Seperated Yet Retained Placenta Adherent to Uterus
Category 2
Simple Adherent Placenta Morbidly adherant Placenta
It is most Common cause of PlacentaAccreta
Retention. It can be due to Placenta Increta ,
Atonic Uterus Placenta Percreta
Management of Retained Placenta : (Category 1 & 2) as Recommended by WHO
Initial Step : य Placenta Expell ह ह ह , WHO स Oxytocin (10 IU I/M
or I/V) Controlled Cord Traction 30 Min. ह WHO स Drug
Retained Placenta Management Use ह ह :
(1) Ergometrine
(2) Denoprost.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 77
Most of the Cases Category 1 Category 2 Placenta Deliver ह ह , य Placenta
भ भ Deliver ह ह ह Manual Removal ह
Manual Removal of Placenta (MRP) :
Done in OT.
Under General Anaesthesia
Single Dose of Antibiotic (Ampicillin)
After the Procedure – I/V Oxytocin Infusion.
Placenta Accreta/Morbidly adherant Placenta : Placenta Accreta Morbidly Adherant
Placenta Type ह , Decidua Basilis Fibrinoid Layer Nitabuch‘s Membrane Absent ह ह स Develop ह ह स Placenta Uterine Wall Firmly Adherant ह ह
Classification :
Placenta Accreta : Chorionic villi attached to superficial Myometrium.
Placenta Increta : Chorionic villi Invade deep in the Myometrium.
Placenta Percreta : Choronic villi Penetrate the full thickness Myometrium and reach upto the
serosal layer.
Complication :
Excessive Bleeding
Shock
Sepsis
Uerine Inversion
Management :
Placenta Accreta
If Female has Complete her Family If Female has not Complete her Family
Cesarean followed by Hysterectomy Conservative Approach
Uterine Inversion : Uterine Inversion is a condition in which there is inside out turning of the
Uterus.
It is Rare cause of postpartum collapse but collapse occurs suddenly after labor.
Etiology :
Most Common Cause is Mismanagement of Third stage of Labor य Placenta Separate
ह ह ह औ सस ह ह Cord Traction Method Placenta Delivery ग ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 78
Spontaneous Inversion Atonic Uterus Condition ह स ह Placenta Accreta is rare Cause.
Clinical Feature :
Patient Present with shock immediately after delivery.
Uterine Inversion condition Haemorrhagic Shock ह स Patient Death ह स ह
Important Points :
Important Points
A patient after delivery goes into shock- Most probable cause is - : PPH
A patient after delivery goes immediately, into shock- Most probable cause is – :
Uterine inversion
A patient after delivery goes into unexpected shock- Most probable cause is – :
Amniotic fluid embolism
Management :
Manual Replacement
Hydrostatic O Sullivan Method
Surgery
Amniotic Fluid Embolism : Inevitable cause of Maternal Mortality.
Clinical Feature : Breathlessness
Cyanosis
Collapse
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 79
Chapter 7
MALPRESENTATION
Malposition : Flexed Occipito Anterior Occipito Transverse Position य औ
Position ह , स Malposition ह ह
Most Common Malposition = Occipito Posterior Position
Malpresentation:Vertex Presentation सभ Presentation Malpresentation ह ह
Most Common Malpresentation Breech Presentation ह ह
Face Presentation :
Presenting Part is Face.
Abnormal Attitude : Normal Delivery Head Attitude Flexion ह ह य Head Attitude Extension ह ह , स Face Presentation ह ह
Denominator = Mentum
Most Common seen in Multiparous Female.
Most Common Pelvis in which face Presentation seen platypelloid Pelvis.
Engaging Diameter = submentobregmatic (9.5 cm) and submentovertical (11.5 cm)
Brow Presentation :
यह Rarest Presentation ह यह Mainly Head Partial Extension ह स ह ह
Engaging Diameter = Mentovertical (14 cm)
Delivery = by cesarean section.
Breech Presentation :
Breech Presentatron Longitudinal lie ह ह Podalic Pole Pelvic Brim ह ह Fetus Buttock Part Maternal Pelvis ह ह
यह स स Common Malpresentation ह ह
Causes of Breech :
Prematurity – Most Common Cause
Twins
Oligohydroamnios
Congenital Malformation of Uterus Like Septate/Bicornuate Uterus
Short Cord
IUD
Hydrocephalus
Placenta Previa
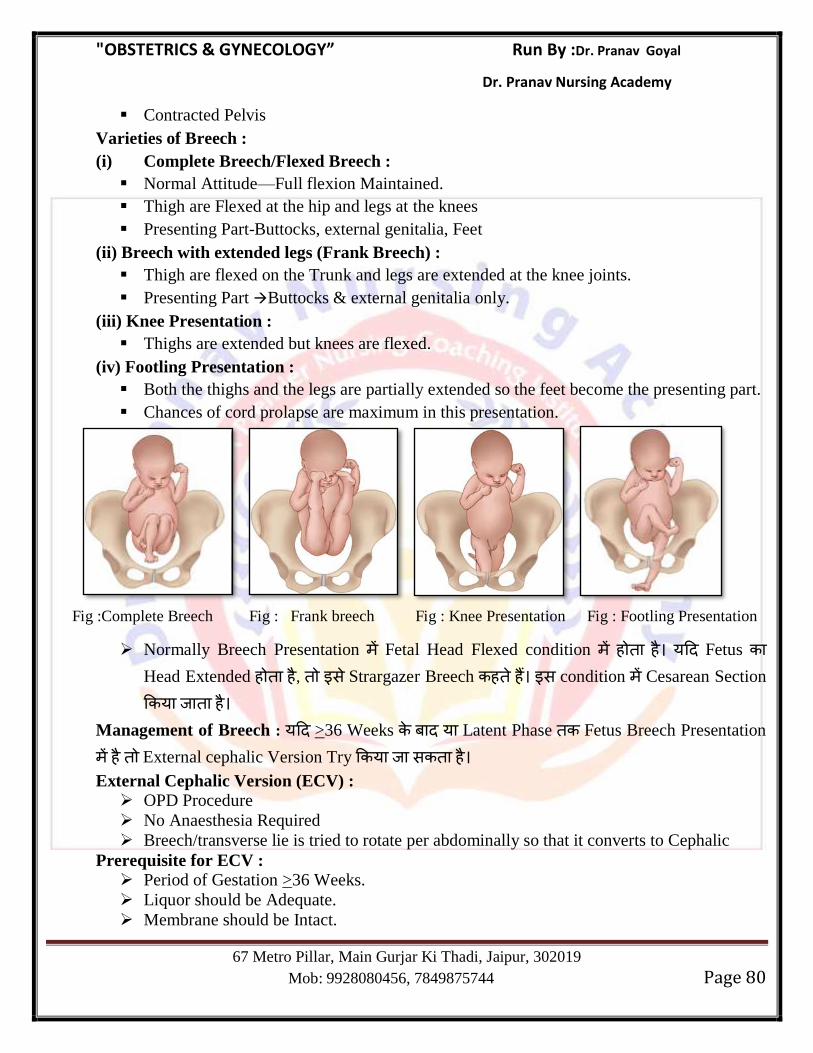
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 80
Contracted Pelvis
Varieties of Breech :
(i) Complete Breech/Flexed Breech :
Normal Attitude—Full flexion Maintained.
Thigh are Flexed at the hip and legs at the knees
Presenting Part-Buttocks, external genitalia, Feet
(ii) Breech with extended legs (Frank Breech) :
Thigh are flexed on the Trunk and legs are extended at the knee joints.
Presenting Part Buttocks & external genitalia only.
(iii) Knee Presentation :
Thighs are extended but knees are flexed.
(iv) Footling Presentation :
Both the thighs and the legs are partially extended so the feet become the presenting part.
Chances of cord prolapse are maximum in this presentation.
Fig :Complete Breech Fig : Frank breech Fig : Knee Presentation Fig : Footling Presentation
Normally Breech Presentation Fetal Head Flexed condition ह ह य Fetus Head Extended ह ह , स Strargazer Breech ह ह स condition Cesarean Section
य ह
Management of Breech : य >36 Weeks य Latent Phase Fetus Breech Presentation
ह External cephalic Version Try य स ह
External Cephalic Version (ECV) :
OPD Procedure
No Anaesthesia Required
Breech/transverse lie is tried to rotate per abdominally so that it converts to Cephalic
Prerequisite for ECV :
Period of Gestation >36 Weeks.
Liquor should be Adequate.
Membrane should be Intact.
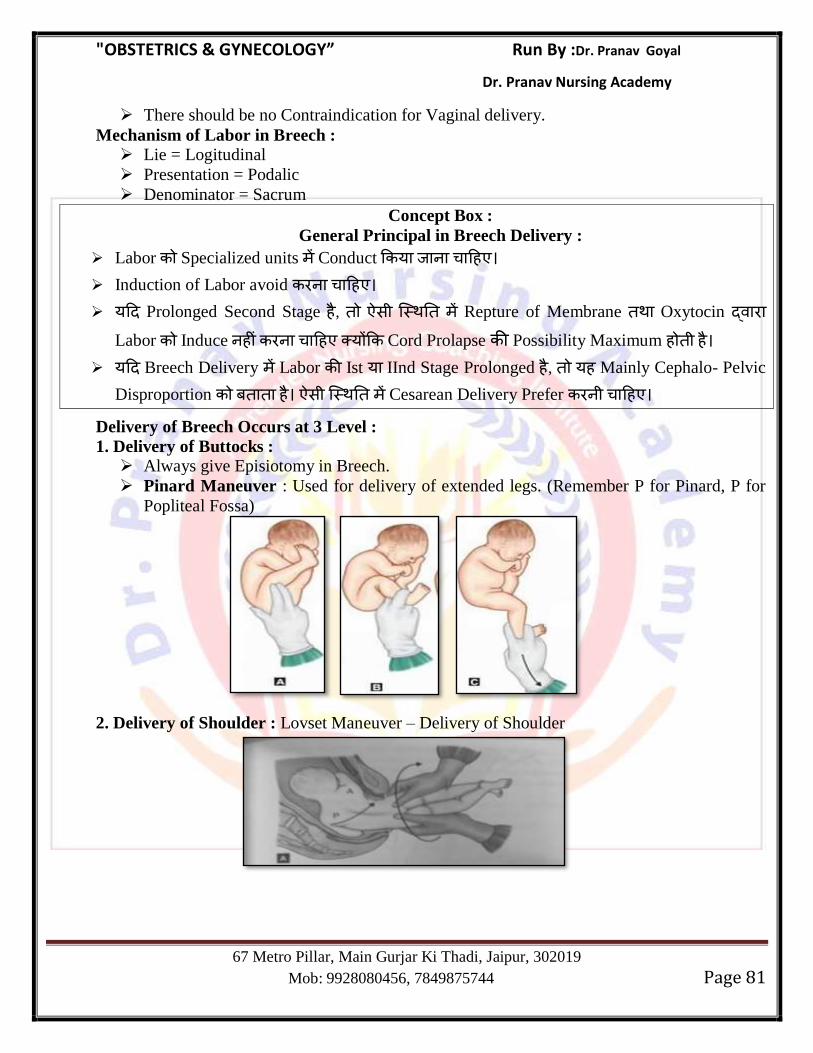
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 81
There should be no Contraindication for Vaginal delivery.
Mechanism of Labor in Breech : Lie = Logitudinal
Presentation = Podalic
Denominator = Sacrum
Concept Box :
General Principal in Breech Delivery :
Labor Specialized units Conduct य ह
Induction of Labor avoid ह
य Prolonged Second Stage ह , स Repture of Membrane Oxytocin Labor Induce ह ह य Cord Prolapse Possibility Maximum ह ह
य Breech Delivery Labor Ist य IInd Stage Prolonged ह , यह Mainly Cephalo- Pelvic
Disproportion ह स Cesarean Delivery Prefer ह
Delivery of Breech Occurs at 3 Level :
1. Delivery of Buttocks : Always give Episiotomy in Breech.
Pinard Maneuver : Used for delivery of extended legs. (Remember P for Pinard, P for
Popliteal Fossa)
2. Delivery of Shoulder : Lovset Maneuver – Delivery of Shoulder
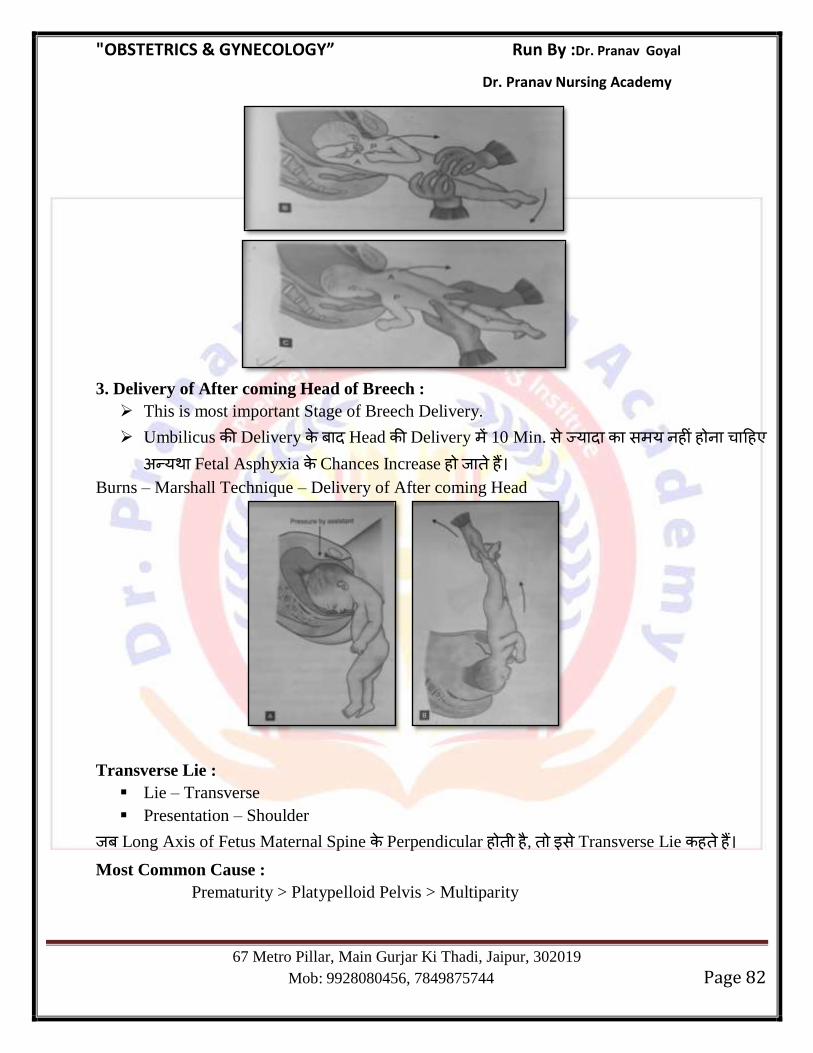
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 82
3. Delivery of After coming Head of Breech :
This is most important Stage of Breech Delivery.
Umbilicus Delivery Head Delivery 10 Min. स य स य ह ह ह
य Fetal Asphyxia Chances Increase ह ह Burns – Marshall Technique – Delivery of After coming Head
Transverse Lie :
Lie – Transverse
Presentation – Shoulder
Long Axis of Fetus Maternal Spine Perpendicular ह ह , स Transverse Lie ह ह Most Common Cause :
Prematurity > Platypelloid Pelvis > Multiparity
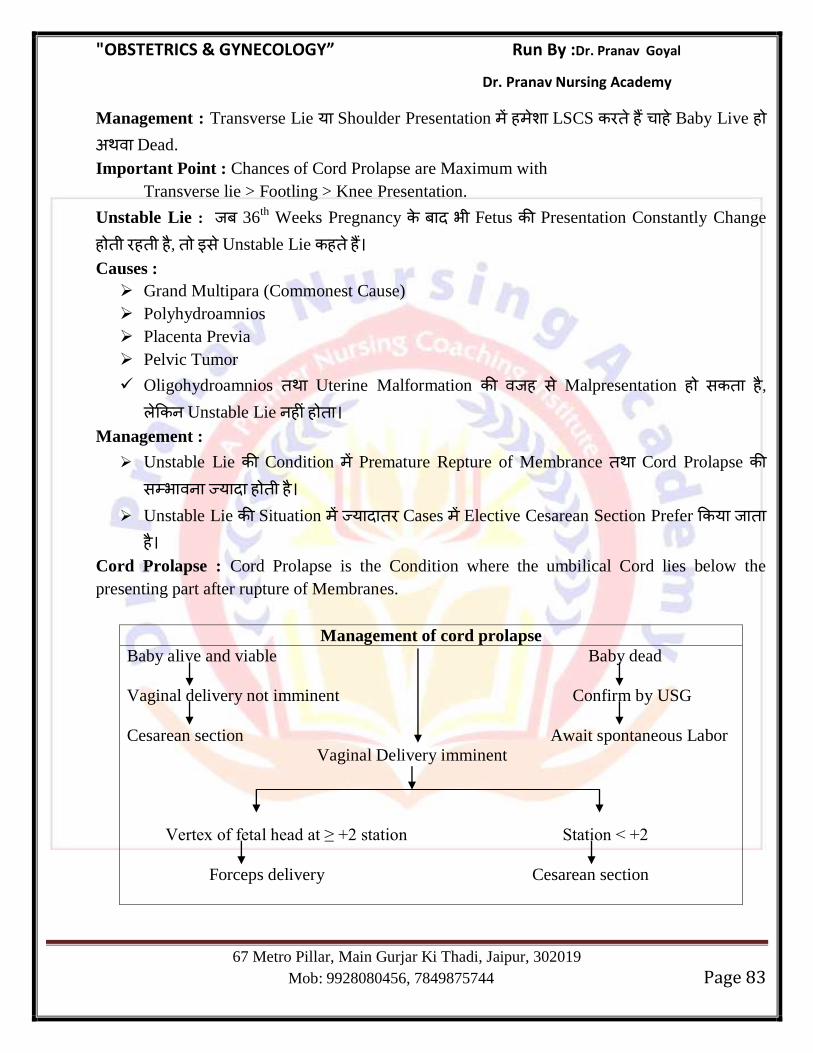
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 83
Management : Transverse Lie य Shoulder Presentation ह LSCS ह ह Baby Live ह Dead.
Important Point : Chances of Cord Prolapse are Maximum with
Transverse lie > Footling > Knee Presentation.
Unstable Lie : 36th
Weeks Pregnancy भ Fetus Presentation Constantly Change
ह ह ह , स Unstable Lie ह ह
Causes :
Grand Multipara (Commonest Cause)
Polyhydroamnios
Placenta Previa
Pelvic Tumor
Oligohydroamnios Uterine Malformation ह स Malpresentation ह स ह , Unstable Lie ह ह
Management :
Unstable Lie Condition Premature Repture of Membrance Cord Prolapse स भ य ह ह
Unstable Lie Situation य Cases Elective Cesarean Section Prefer य ह
Cord Prolapse : Cord Prolapse is the Condition where the umbilical Cord lies below the
presenting part after rupture of Membranes.
Management of cord prolapse
Baby alive and viable Baby dead
Vaginal delivery not imminent Confirm by USG
Cesarean section Await spontaneous Labor
Vaginal Delivery imminent
Vertex of fetal head at ≥ +2 station Station < +2
Forceps delivery Cesarean section
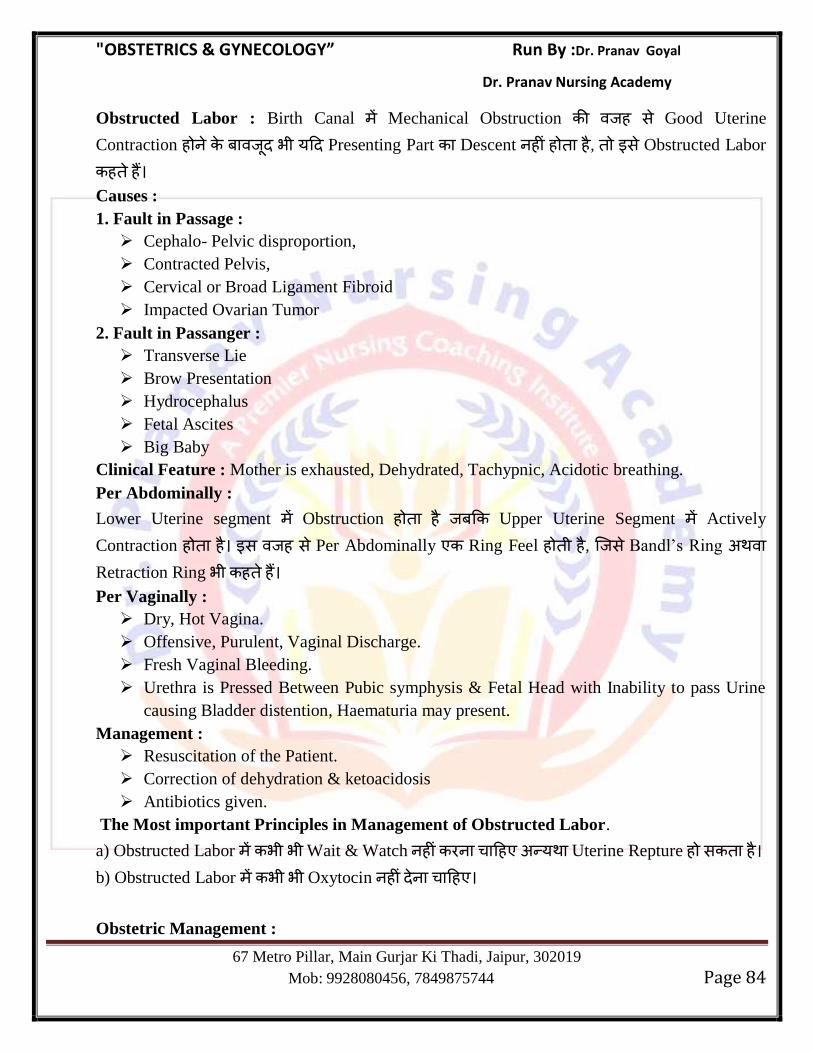
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 84
Obstructed Labor : Birth Canal Mechanical Obstruction ह स Good Uterine
Contraction ह भ य Presenting Part Descent ह ह ह , स Obstructed Labor
ह ह
Causes :
1. Fault in Passage :
Cephalo- Pelvic disproportion,
Contracted Pelvis,
Cervical or Broad Ligament Fibroid
Impacted Ovarian Tumor
2. Fault in Passanger :
Transverse Lie
Brow Presentation
Hydrocephalus
Fetal Ascites
Big Baby
Clinical Feature : Mother is exhausted, Dehydrated, Tachypnic, Acidotic breathing.
Per Abdominally :
Lower Uterine segment Obstruction ह ह Upper Uterine Segment Actively
Contraction ह ह स ह स Per Abdominally Ring Feel ह ह , स Bandl‘s Ring Retraction Ring भ ह ह Per Vaginally :
Dry, Hot Vagina.
Offensive, Purulent, Vaginal Discharge.
Fresh Vaginal Bleeding.
Urethra is Pressed Between Pubic symphysis & Fetal Head with Inability to pass Urine
causing Bladder distention, Haematuria may present.
Management :
Resuscitation of the Patient.
Correction of dehydration & ketoacidosis
Antibiotics given.
The Most important Principles in Management of Obstructed Labor.
a) Obstructed Labor भ भ Wait & Watch ह ह य Uterine Repture ह स ह
b) Obstructed Labor भ भ Oxytocin ह ह
Obstetric Management :
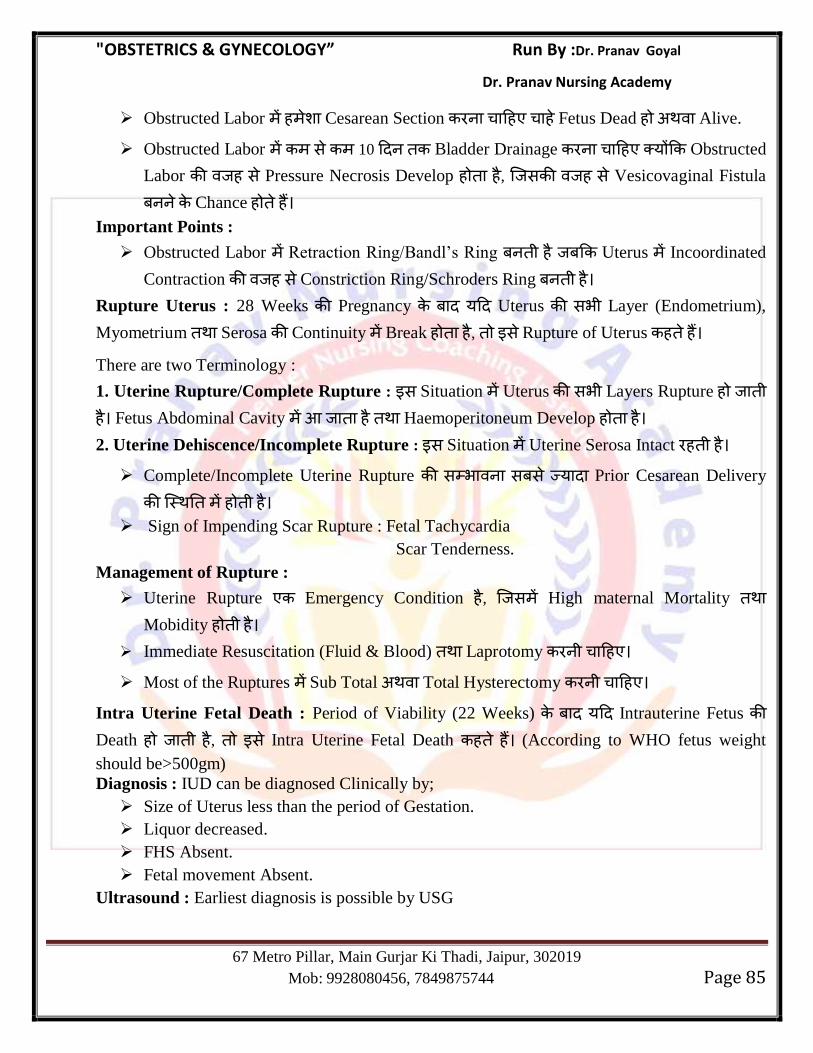
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 85
Obstructed Labor ह Cesarean Section ह ह Fetus Dead ह Alive.
Obstructed Labor स 10 Bladder Drainage ह य Obstructed
Labor ह स Pressure Necrosis Develop ह ह , स ह स Vesicovaginal Fistula
Chance ह ह
Important Points :
Obstructed Labor Retraction Ring/Bandl‘s Ring ह Uterus Incoordinated
Contraction ह स Constriction Ring/Schroders Ring ह
Rupture Uterus : 28 Weeks Pregnancy य Uterus सभ Layer (Endometrium),
Myometrium Serosa Continuity Break ह ह , स Rupture of Uterus ह ह
There are two Terminology :
1. Uterine Rupture/Complete Rupture : स Situation Uterus सभ Layers Rupture ह ह Fetus Abdominal Cavity ह Haemoperitoneum Develop ह ह
2. Uterine Dehiscence/Incomplete Rupture : स Situation Uterine Serosa Intact ह ह Complete/Incomplete Uterine Rupture स भ स स य Prior Cesarean Delivery
ह ह
Sign of Impending Scar Rupture : Fetal Tachycardia
Scar Tenderness.
Management of Rupture :
Uterine Rupture Emergency Condition ह , स High maternal Mortality Mobidity ह ह
Immediate Resuscitation (Fluid & Blood) Laprotomy ह
Most of the Ruptures Sub Total Total Hysterectomy ह
Intra Uterine Fetal Death : Period of Viability (22 Weeks) य Intrauterine Fetus Death ह ह , स Intra Uterine Fetal Death ह ह (According to WHO fetus weight
should be>500gm)
Diagnosis : IUD can be diagnosed Clinically by;
Size of Uterus less than the period of Gestation.
Liquor decreased.
FHS Absent.
Fetal movement Absent.
Ultrasound : Earliest diagnosis is possible by USG
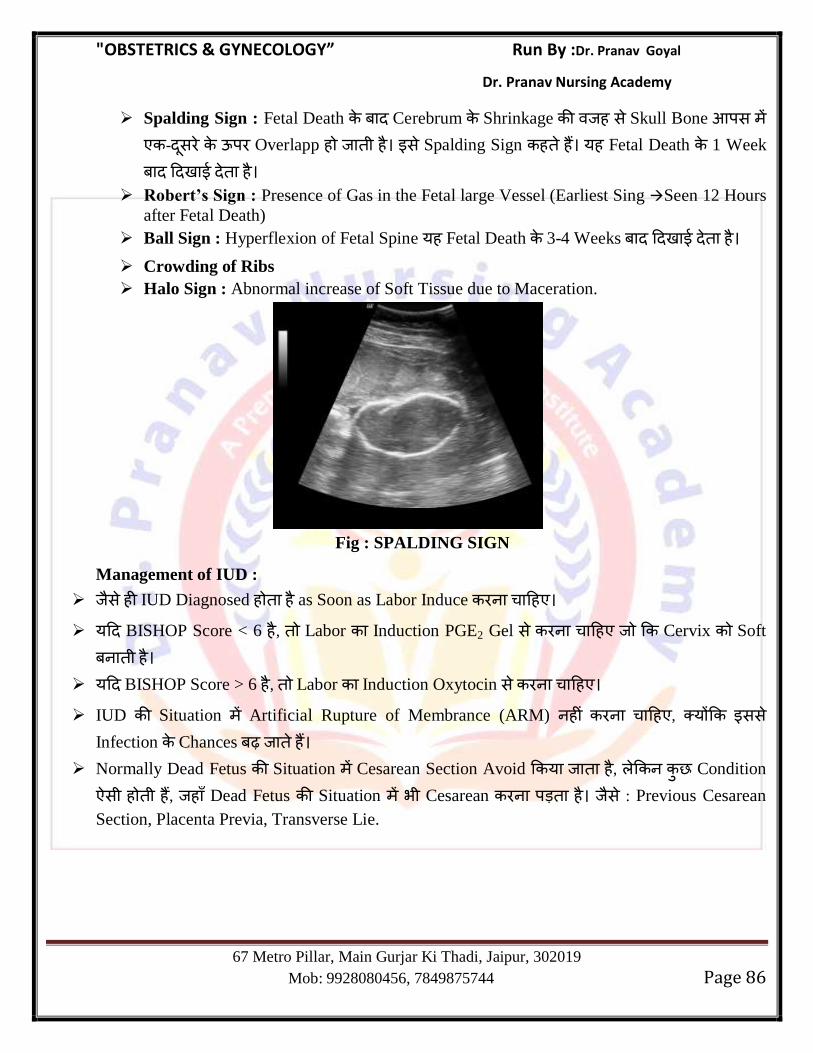
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 86
Spalding Sign : Fetal Death Cerebrum Shrinkage ह स Skull Bone स - स ऊ Overlapp ह ह स Spalding Sign ह ह यह Fetal Death 1 Week
ह
Robert’s Sign : Presence of Gas in the Fetal large Vessel (Earliest Sing Seen 12 Hours
after Fetal Death)
Ball Sign : Hyperflexion of Fetal Spine यह Fetal Death 3-4 Weeks ह Crowding of Ribs
Halo Sign : Abnormal increase of Soft Tissue due to Maceration.
Fig : SPALDING SIGN
Management of IUD :
स ह IUD Diagnosed ह ह as Soon as Labor Induce ह
य BISHOP Score < 6 ह , Labor Induction PGE2 Gel स ह Cervix Soft
ह
य BISHOP Score > 6 ह , Labor Induction Oxytocin स ह
IUD Situation Artificial Rupture of Membrance (ARM) ह ह , य सस Infection Chances ह
Normally Dead Fetus Situation Cesarean Section Avoid य ह , Condition
स ह ह , ह Dead Fetus Situation भ Cesarean ह स : Previous Cesarean
Section, Placenta Previa, Transverse Lie.
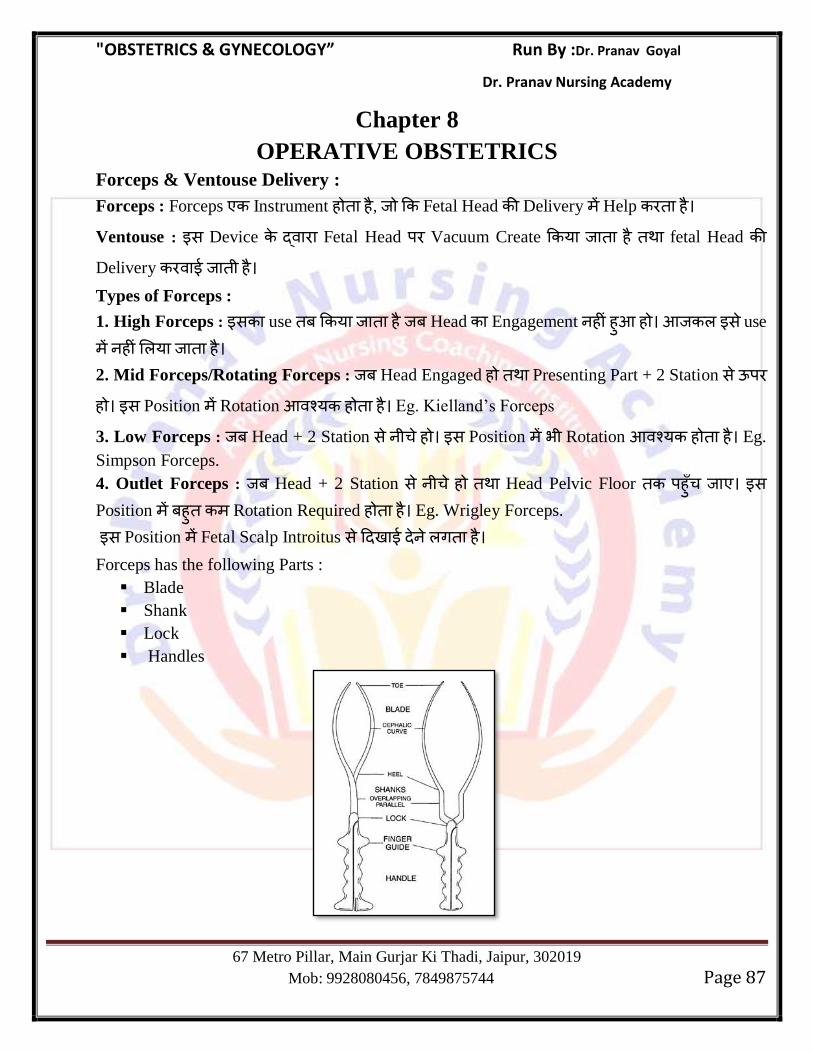
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 87
Chapter 8
OPERATIVE OBSTETRICS Forceps & Ventouse Delivery :
Forceps : Forceps Instrument ह ह , Fetal Head Delivery Help ह
Ventouse : स Device Fetal Head Vacuum Create य ह fetal Head Delivery ह
Types of Forceps :
1. High Forceps : स use य ह Head Engagement ह ह ह स use
ह य ह
2. Mid Forceps/Rotating Forceps : Head Engaged ह Presenting Part + 2 Station स ऊ
ह स Position Rotation य ह ह Eg. Kielland‘s Forceps
3. Low Forceps : Head + 2 Station स ह स Position भ Rotation य ह ह Eg.
Simpson Forceps.
4. Outlet Forceps : Head + 2 Station स ह Head Pelvic Floor ह स
Position ह Rotation Required ह ह Eg. Wrigley Forceps.
स Position Fetal Scalp Introitus स ग ह
Forceps has the following Parts :
Blade
Shank
Lock
Handles
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 88
Vacuum : Vacuum or Ventouse Consist 2 parts :
Suction Machine
Suction Cups.
Suction Cup Metallic/Sialistic ह ह
Vacuum Cup Flexion Point apply य ह Posterior fontanelle स 3 cm ग Anterior Fontanelle 6 Cm ह ह
Fetal Distress Situation Vacuum Use ह ह
Vacuum Vertex Presentation य स Presentation Use ह य स ह
Prerequisite For Forceps & Vacuum Delivery :
F : Favourable Position/Station
O : Os should be fully dilated
R : Membranes should be Ruptured
C : Uterus should be contracting
E : Episiotomy should be given, Bladder should be empty, Head should be engaged.
P : No CPD
Forceps : Pressure/Traction Primi = 20 Kg
Multi = 13 Kg.
Forceps applied along Occipitomental direction.
Indication :
Maternal Distress,
Fetal Distress (Head Station >+2)
Prolonged 2nd
Stage of Labor.
Advantage of Forceps over Vacuum :
यह Vertex Presentation Other Position भ Use य स ह
यह Preterm Babies Use य स ह Fetal Distress Condition Use य स ह
Contraindication :
CPD/Contracted Pelvis
HIV Positive Female
Osteogenesis Imperfecta
Known Coagulopathy in Fetus
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 89
Complication :
स ह स Maternal Injury Chances य ह ह Complete Perineal Tear is Most
Common.
Fetus Facial Nerve Palsy Brachial Plexus Injury ह स ह Maximum 3 Attempts स ह य 3 Attempts भ Fetal Head Delivery
ह ह ह , स Failed Forceps ह ह स Condition Cesarean य ह
Vacuum : य Cervix Full Dilated ह ह , भ Vacuum Use य स ह
Initial Pressure = 0.2 kg/cm3
Maximum Pressure = 0.8 kg/cm3
Fetal Distress Condition Vacuum Use ह ह
Preterm Babies भ Vacuum Use ह ह Vacuum स Fetal Injury Chances य ह ह
Complication :
Cephalohematoma
Retinal Nerve Injury
Sixth Nerve Palsy
Artificial Caput Succedaneum (Chignon)
Maximum 3 Attempts स ह य 3 Attempts भ Fetal Head Delivery ह ह ह , स Failed Vacuum ह ह स Condition Cesarean य ह
Episiotomy : Vaginal Delivery Vulval outlet Diameter Increase
Perineum Vulva Incision ग य ह सस Perineal Tear Develop ह स Episiotomy
ह ह
Episiotomy Second Degree Type Perineal Tear ह Vulval Outlet Diameter Increase य ह यह Routine Procedure ह ह यह Only Selective
Cases य ह Indication of Episiotomy :
1. In Rigid Perineum : Elderly Primigravida
2. Anticipating Perineal Tear : Big baby, Face to Pubis delivery, Breech Delivery shoulder
dystocia
3. Operative Delivery : Forceps Delivery, Ventouse Delivery.
4. Previous Perineal Surgery : Pelvic Floor Repair
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 90
Timing of Episiotomy : Crowning Just ह Head 3-4 cm Visible ह ह यह Time Episiotomy
Best ह ह
Types of Episiotomy :
1. Median : यह Incision Midline Fourchette स Start ह Anus ओ ह ह , Anal
sphinctor Involve ह ह स Cut य Extension ह ह , 3rd
4th
Degree Perineal Tear ह Chances ह ह 2. Mediolateral : यह Cut Centre Midline स Start ह Outward ह ह स Cut Safe
ह ह य Extension ह स Rectal Involvement ह ह
3. Lateral : यह Cut Midline स गभग 1 cm Lateral ह ह Outward ह ह स Cut Mainly Bartholin Duct Injury ह Chances ह ह 4. J-Shaped : स Cut Midline गभग 1.5 cm Outward Cut ग य ह सस Rectal Involvement ह ह
Mediolateral Median Episiotomy Most Common Type Episiotomy ह ह
Commonly Rt. Mediolateral Episiotomy is Performed.
Median Episiotomy Extension ह स 3rd 4th
Degree Perineal Tear स भ ह ह
स Median Episiotomy Routine Use ह य
Cesarean Section : यह Operative Procedure ह स 28 Weeks Abdomen Uterus
Wall Incision ग Fetus Delivery ह
Indication :
Absolute Indication :
Central Placenta Previa
Contracted Pelvis or Cephalopelvic Disproportion
Pelvic Mass (Cervical or Broad Ligament Fibroid)
Advanced Carcinoma Cervix
Vaginal Obstruction (Atresia, Stenosis)
Relative Indication :
Cephalopelvic Disproportion
Previous Cesarean Delivery
Non Reassuring FHR (Fetal Distress)
Dystocia due to 3 ‗P‘ :
(1) Large Fetus (Passanger)
(2) Small Pelvis (Passage)
(3) Ineffective Uterine Contraction (Power)
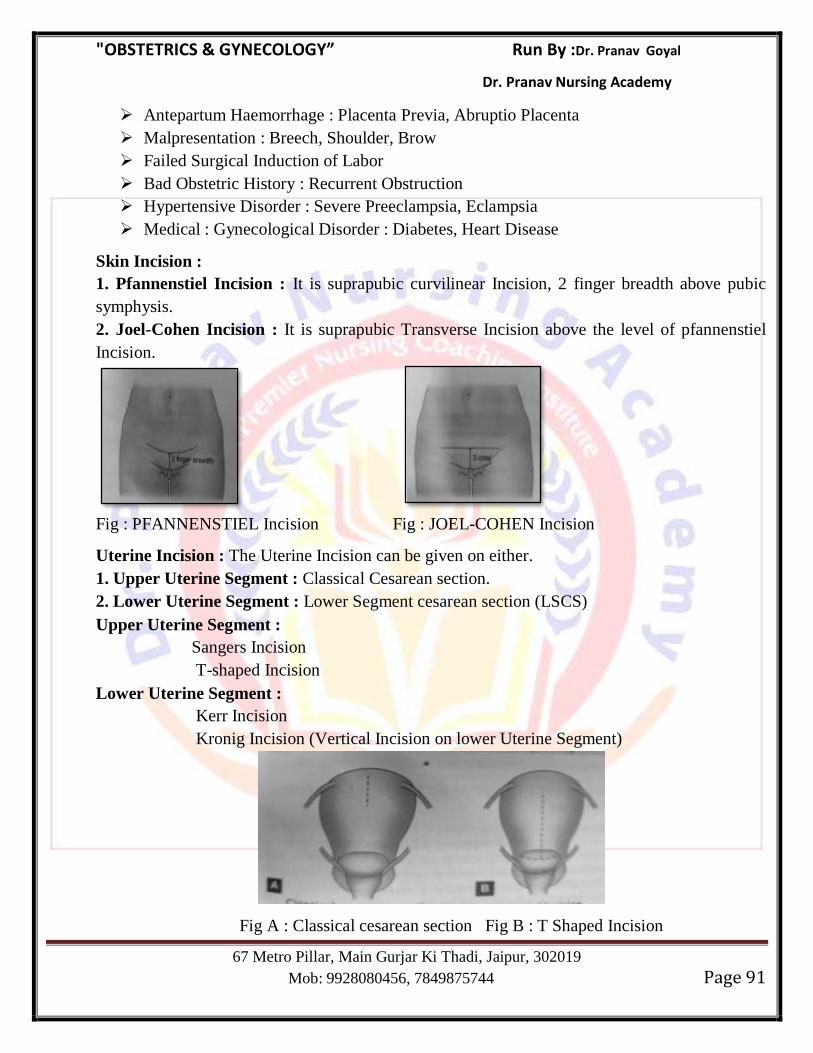
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 91
Antepartum Haemorrhage : Placenta Previa, Abruptio Placenta
Malpresentation : Breech, Shoulder, Brow
Failed Surgical Induction of Labor
Bad Obstetric History : Recurrent Obstruction
Hypertensive Disorder : Severe Preeclampsia, Eclampsia
Medical : Gynecological Disorder : Diabetes, Heart Disease
Skin Incision :
1. Pfannenstiel Incision : It is suprapubic curvilinear Incision, 2 finger breadth above pubic
symphysis.
2. Joel-Cohen Incision : It is suprapubic Transverse Incision above the level of pfannenstiel
Incision.
Fig : PFANNENSTIEL Incision Fig : JOEL-COHEN Incision
Uterine Incision : The Uterine Incision can be given on either.
1. Upper Uterine Segment : Classical Cesarean section.
2. Lower Uterine Segment : Lower Segment cesarean section (LSCS)
Upper Uterine Segment :
Sangers Incision
T-shaped Incision
Lower Uterine Segment :
Kerr Incision
Kronig Incision (Vertical Incision on lower Uterine Segment)
Fig A : Classical cesarean section Fig B : T Shaped Incision
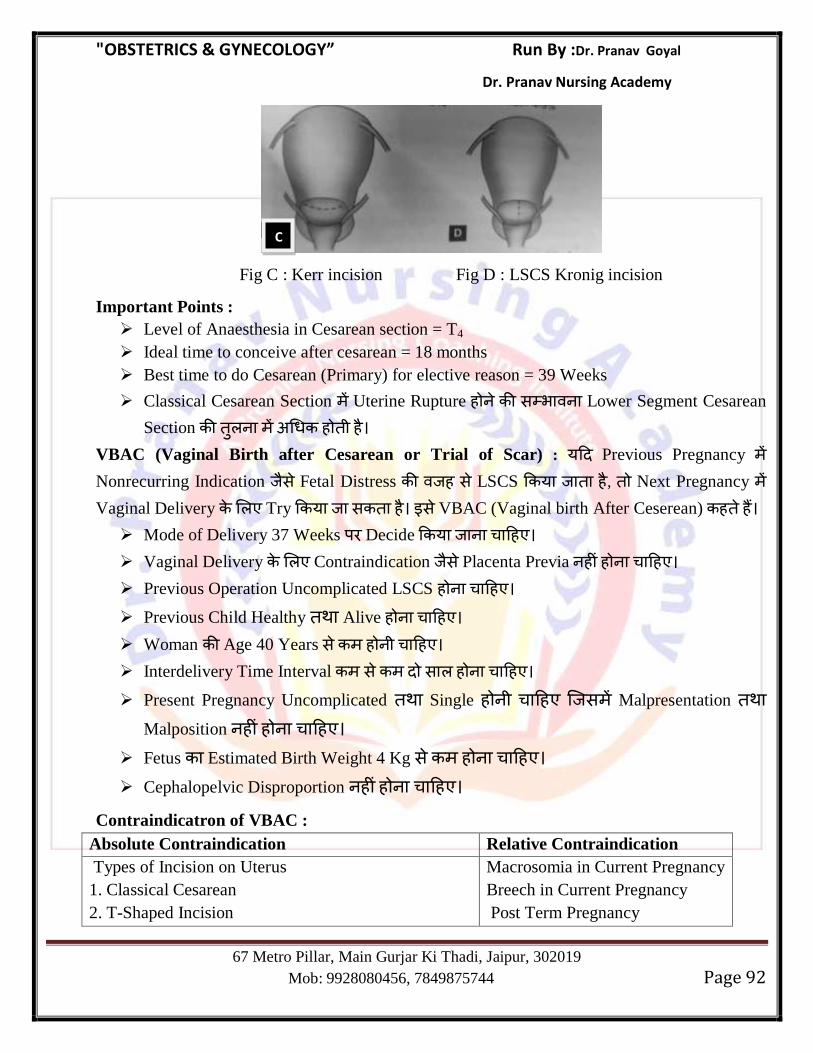
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 92
Fig C : Kerr incision Fig D : LSCS Kronig incision
Important Points :
Level of Anaesthesia in Cesarean section = T4
Ideal time to conceive after cesarean = 18 months
Best time to do Cesarean (Primary) for elective reason = 39 Weeks
Classical Cesarean Section Uterine Rupture ह स भ Lower Segment Cesarean
Section ह ह
VBAC (Vaginal Birth after Cesarean or Trial of Scar) : य Previous Pregnancy Nonrecurring Indication स Fetal Distress ह स LSCS य ह , Next Pregnancy Vaginal Delivery Try य स ह स VBAC (Vaginal birth After Ceserean) ह ह Mode of Delivery 37 Weeks Decide य ह Vaginal Delivery Contraindication स Placenta Previa ह ह ह
Previous Operation Uncomplicated LSCS ह ह Previous Child Healthy Alive ह ह
Woman Age 40 Years स ह ह
Interdelivery Time Interval स स ह ह
Present Pregnancy Uncomplicated Single ह ह स Malpresentation Malposition ह ह ह
Fetus Estimated Birth Weight 4 Kg स ह ह
Cephalopelvic Disproportion ह ह ह
Contraindicatron of VBAC :
Absolute Contraindication Relative Contraindication
Types of Incision on Uterus
1. Classical Cesarean
2. T-Shaped Incision
Macrosomia in Current Pregnancy
Breech in Current Pregnancy
Post Term Pregnancy
C
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 93
3. Kronig Incision
H/o Previous Uterine Rupture
If any Contraindication to Vaginal Delivery is Present.
Management of VBAC :
VBAC (Vaginal Brith after Cesarean) well equiped Hospital य ह ह Continuous Intrapartum Care Monitoring Emergency Immediate Cesarean
Section, Blood Transfusion Neonatal Resuscitation स ह ह Labour Augment स Amniotomy ह
VBAC Induction of Labor भ भ Oxytocin Use ह ह , य Oxytocin
Strong Uterine Contraction Produce ह सस Uterine Rupture स भ ह ह
Vaginal Prostaglandin E2 Tablet (Dinoprostone) भ Cervix Ripening Use ह ह (Due to High Risk of Rupture)
Epidural Anaesthesia not Contraindicated.
Misoprost is Contraindicated in Previous Cesarean Section.
Labor Procedure Fetal Heart Rate Monitoring ह Fetal distress
is one of the Earliest Sign of Scar Dehiscence.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 94
Chapter 9
Preterm Labor, Premature Rupture of Membrance & Post Dated Pregnancy
Preterm Labor :
> य Onset of Labor (Regular Painful Uterine Contraction associated with effacement and
dilatation of the Cervix) 37 Weeks स ह ह , स Preterm Labor ह ह Risk Factor of Preterm Labor (PTL)
Previous H/O Pre Term Labor
Most Common Cause of Preterm Labor is Idiopathic followed by Infection.
Low Socioeconomic Status
Smoking
Congenital Anomallies of Uterus
Pregnancy complication like Antepartum Haemorrhage, PROM, Polyhydroamnios,
Twins
Genital tract Infection
Bacterial Vaginosis
Gardnerella Vaginalis
Ureaplasma Urealyticum
Mycoplasma Hominis
Fusobacterium
Incompetent OS
Prophylactic Measures to decrease Preterm Labor :
Stop Smoking
Progesterone : Progesterone decrease Uterine Contraction by suppressing cytokine
Activity.
Diagnosis of Preterm Labor :
1. Symptoms & sign of PTL :
Uterine Contraction Frequency 4 in 20 min. or 8 in 60 minutes.
Lower Back Pain
Passage of Blood Stained Vaginal discharge (Show)
Sensation of Pelvic Pressure
Bulging/Rupture of Membrane.
2. On TVS :
Length of Cervix : < 2.5 cm (2.5 cm is cut off value for length of cervix to predict PTL)
Dilatation of Cervix : > 2 cm
Effacement of Cervix : U-shaped (80%)
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 95
3.Level of Fibronectin Protein :
Presence of fibronectin Glycoprotein produced by Fetal Amnion in the cervico- vaginal
discharge between 24-34 weeks is a predictor of pretern Labor. When the test is Negative it
Reassure that delivery will not occur with in next 7 days.
Management of Preterm Labor :
General Principles : Preterm Labor स स Important Risk ह Fetus Lung Mature ह ह ह सस Fetus Respiratory Distress Syndrone ह Possibility ह ह Fetus Lung Maturity
Enhance Corticosteroid य ह
Dose of Corticosteroid :
1. Two dose of Betamethasone (12 mg) IM 24 hourly.
2. Four Dose of Dexamethasone (6 mg) IM 12 hourly.
Use of Corticosteroids :
Decrease chances of Respiratory distress Syndrome.
Decrease chances of Intraventricular Haemorrhage
Decrease chances of Necrotising enterocolitis.
Weekly repeat courses are not recommended as it can lead to cerebral palsy in fetus.
Contraindication for corticosteroid : Chorioamnionitis
Tocolytic Therapy : Corticosteroid गभग 24-48 स Best Effect ह
स स 24-48 Uterine Contraction Stop य ह स Short
Term Tocolytic Drug Use ह
Tocolytic Drugs :
Prostaglandin Synthatase Inhibitor : Indomethacin
Calcium Channel Blockers : Nifedipine
Oxytocin Antagonist : Atosiban
Mangnesium Sulfate
Nitric Oxide Donor : Glyceryl Trinitrate
β-Agonist : Ritodrine, Terbutaline, Isoxsuprine, Salbutamol.
Important Points :
Tocolytic of Choice Nifedipine
Tocolytic of Choice in Heart Patient Atosiban
Tocolytic with Maximum Maternal side effect β-Agonist
side effect of β-Agonist
Tremor,
Hyperglycemia
Hypokalemia
Pulmonary edema
Tocolytic with Maximum fetal side effect Indomethacin
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 96
Side Effect of Indomethacin
premature Closure of Ductus Arteriosus
Oligohydroamnios
Neonatal Pulmonary Hypertension
Tocolytic Contraindicated in Diabetes β-Agonist
Long Term MgSo4 Tocolytic ह Use स Neonatal Osteopenia स भ ह
MgSo4 Preterm Labor 24-32 Weeks Use स Cerebral Palsy स भ
ह ह
Preterm Labor Antibiotics Role ह ह Membrane Rupture ह ह ग ह Progesterone Uterine contraction Suppress ह स Preterm Labor Tocolytic
ह Use ह य
Contraindicatron of Tocolytics : chorioamnionitis
Advanced Labor
Preeclampsia/Eclampsia
Abruptio Placenta
congenital Anomally of Fetus not Compatible with life.
Management of Pre term Labor
If corticosteroid was not given earlier it has to be given
Tocolytics
MgSo4 (For neuroprotection)
Send Rectal & vaginal swab for group B Streptcoccal infection (Causes neonatal meningitis)
PROM (Premature Rupture of Membrane) : Premature Rupture of Membrane is defined as
spontaneous rupture of membrane before the onset of Labor.
PROM
Term PROM Preterm PROM
य Membrane Rupture य Membrane Rupture 37
37 Week ह Week स ह ह
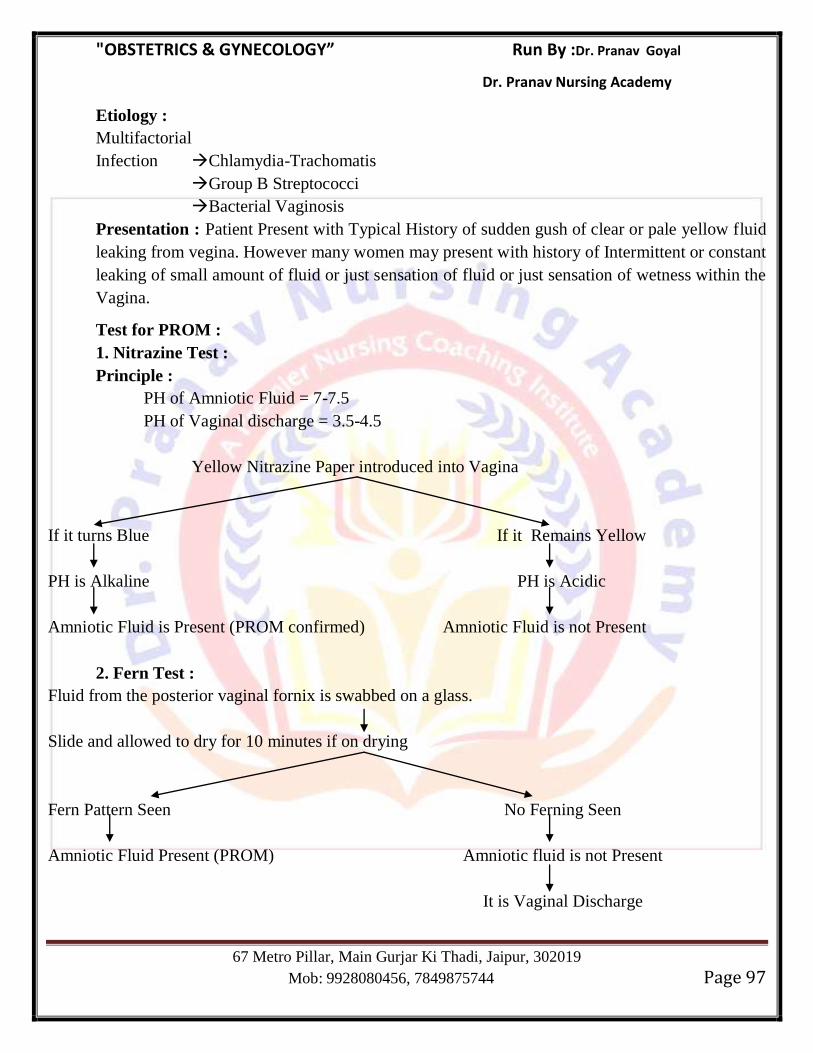
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 97
Etiology :
Multifactorial
Infection Chlamydia-Trachomatis
Group B Streptococci
Bacterial Vaginosis
Presentation : Patient Present with Typical History of sudden gush of clear or pale yellow fluid
leaking from vegina. However many women may present with history of Intermittent or constant
leaking of small amount of fluid or just sensation of fluid or just sensation of wetness within the
Vagina.
Test for PROM :
1. Nitrazine Test :
Principle :
PH of Amniotic Fluid = 7-7.5
PH of Vaginal discharge = 3.5-4.5
Yellow Nitrazine Paper introduced into Vagina
If it turns Blue If it Remains Yellow
PH is Alkaline PH is Acidic
Amniotic Fluid is Present (PROM confirmed) Amniotic Fluid is not Present
2. Fern Test :
Fluid from the posterior vaginal fornix is swabbed on a glass.
Slide and allowed to dry for 10 minutes if on drying
Fern Pattern Seen No Ferning Seen
Amniotic Fluid Present (PROM) Amniotic fluid is not Present
It is Vaginal Discharge
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 98
3. USG : In case of PROM in USG decrease amount of Amniotic Fluid or Anhydroamnios.
4. Fetal Fibronectin Protein : If present in Vaginal cervix dischage it shows PROM.
Diagnosis :
Per Speculum Examination : PROM Diagnosis Sterile per Speculum
Examination य ह
PROM Per Vaginal Examination ह ह य सस intrauterine Infection Preterm Labor स भ ह
Effect of Preterm Premature Rupture of Membrane :
Preterm Labor & Birth
Pulmonary Hypoplasia due to severe oligohydroamnios
Skeltal & Joint deformities of the Fetus due to compression.
Chorioamnionitis
General Principle for management of PROM :
1. Bed Rest.
2. Sterile Pads for inspection & Monitor Sign of Infection
3. Observed sign of clinical chorioamnionitis
Maintain temperature chart 4-8 hourly.
Auscultate Fetal heart rate 4-8 hourly
Observe for offensive vaginal discharge.
4. High Vaginal swab examination
5. Maternal CBC & C-Reactive Protein
6. Cardiotocography: Useful for monitor Fetal tachycardia due to Chorioamnionitis
7. Use of Prophylactic Antibiotics Erythromycin can be given for 10 days.
8. Antenatal corticosteroid
9. Tocolysis
9. Delivery at 34 Weeks.
Post Term Pregnancy : य Preganancy 42 Weeks भ Continue ह ह , स Postmaturity य Post Term Pregnancy ह ह
Cause :
1. Wrong Dates : Due to wrong LMP date (Most common)
2. Hereditory
3. Maternal Factor : Primipara, Elderly Multipara, Sedentary Habit
4. Fetal Factors : Congenital Anomallies like Anencephaly, Adrenal Hypoplasia
5. Placental Factor : Sulphatase Deficiency (Low estrogen)
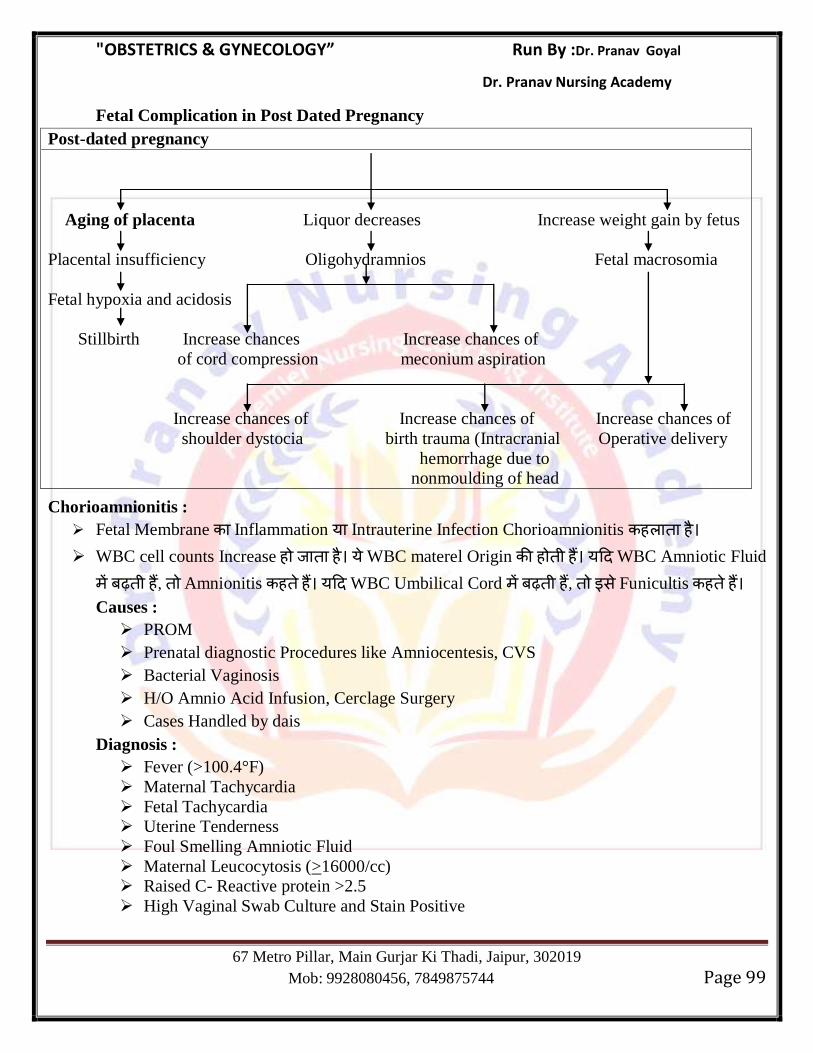
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 99
Fetal Complication in Post Dated Pregnancy
Post-dated pregnancy
Aging of placenta Liquor decreases Increase weight gain by fetus
Placental insufficiency Oligohydramnios Fetal macrosomia
Fetal hypoxia and acidosis
Stillbirth Increase chances Increase chances of
of cord compression meconium aspiration
Increase chances of Increase chances of Increase chances of
shoulder dystocia birth trauma (Intracranial Operative delivery
hemorrhage due to
nonmoulding of head
Chorioamnionitis :
Fetal Membrane Inflammation य Intrauterine Infection Chorioamnionitis ह ह
WBC cell counts Increase ह ह य WBC materel Origin ह ह य WBC Amniotic Fluid
ह , Amnionitis ह ह य WBC Umbilical Cord ह , स Funicultis ह ह Causes :
PROM
Prenatal diagnostic Procedures like Amniocentesis, CVS
Bacterial Vaginosis
H/O Amnio Acid Infusion, Cerclage Surgery
Cases Handled by dais
Diagnosis :
Fever (>100.4°F)
Maternal Tachycardia
Fetal Tachycardia
Uterine Tenderness
Foul Smelling Amniotic Fluid
Maternal Leucocytosis (>16000/cc)
Raised C- Reactive protein >2.5
High Vaginal Swab Culture and Stain Positive
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 100
Management :
Antibiotic : Ampicillin 500 gram 6 hours
Removal of Cerclage
Delivery as soon as possible regardless of Gestational age.
Abortion & MTP
Abortion/Misscarriage : Abortion य Misscarriage ह Process ह Fetus/Embryo 20 Weeks स ह (Wt < 500 gm) Terminate ह
Period of Viability depends on Medical Facilities of a country.
Period of Viability ह Time Period ह Fetus Independent Survive स ह WHO स
Period of Viability is 22 weeks
In India Period of Viability is 28 Weeks.
Incidence of Abortion : गभग 10-20% Pregnancies Misscarriage ह ह 75% Abortion
16 Weeks स ह ह ह औ स Abortions स 75% Abortion 8th
Weeks स ह ह ह Blighted Ovum : Early Pregnancy Uterus Gestation Sac ह ह ,
Fetal Part Development ह ह (Yolk Sac May or may not be present)
Recurrent Abortion : 3 य 3 स य 20 Weeks स ह Spontaneous Abortion ह ह , स Recurrent Abortion ह ह
Causes of Abortion :
Fetal Causes :
Chromosomal Abnormalities (Most Common)
Hydropic Degeneration of villi
Multiple Pregnancy.
Maternal Causes :
Trauma
Infection/Immunological Causes
Maternal Medical Disease
Environmental Factor/Endocrine Problem
Developmental/Anatomical Problem
Most Common Cause of Ist Trimester Abortion : Chromosomal Abnormalities.
Most Common cause of 2nd
Trimester Recurrent Abortion : Cervical Incompetence.
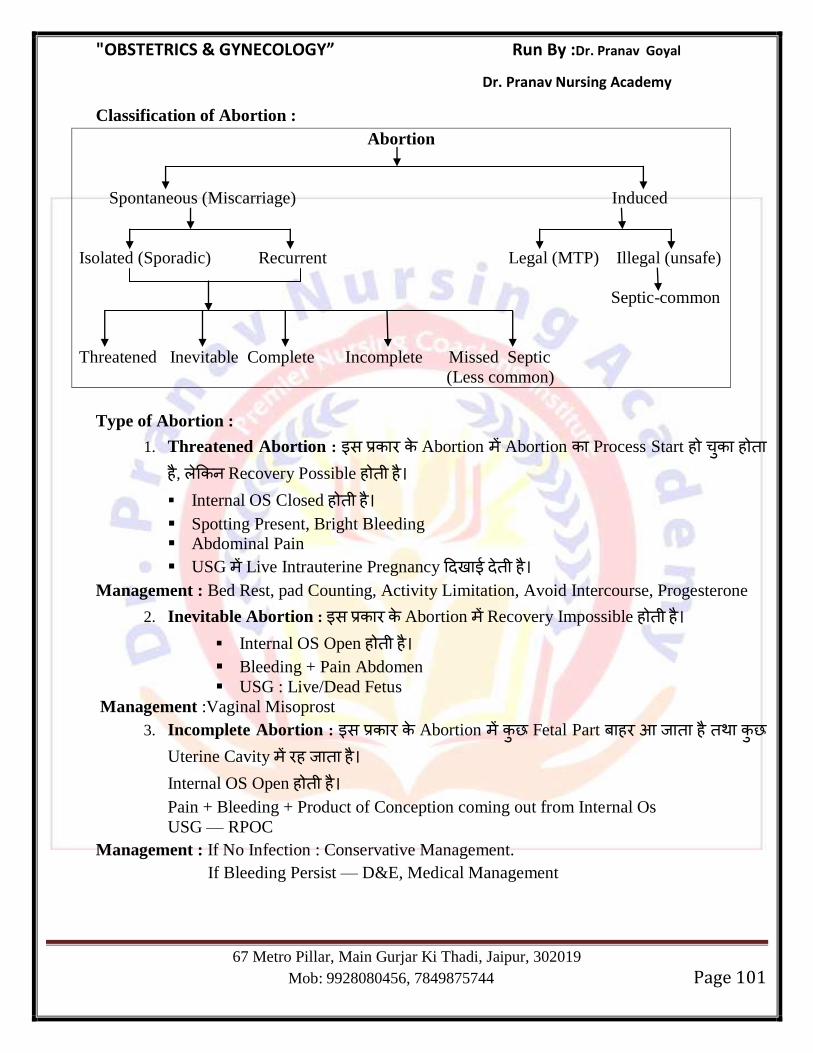
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 101
Classification of Abortion :
Abortion
Spontaneous (Miscarriage) Induced
Isolated (Sporadic) Recurrent Legal (MTP) Illegal (unsafe)
Septic-common
Threatened Inevitable Complete Incomplete Missed Septic
(Less common)
Type of Abortion :
1. Threatened Abortion : स Abortion Abortion Process Start ह ह ह , Recovery Possible ह ह
Internal OS Closed ह ह
Spotting Present, Bright Bleeding
Abdominal Pain
USG Live Intrauterine Pregnancy ह Management : Bed Rest, pad Counting, Activity Limitation, Avoid Intercourse, Progesterone
2. Inevitable Abortion : स Abortion Recovery Impossible ह ह
Internal OS Open ह ह
Bleeding + Pain Abdomen
USG : Live/Dead Fetus
Management :Vaginal Misoprost
3. Incomplete Abortion : स Abortion Fetal Part ह ह
Uterine Cavity ह ह
Internal OS Open ह ह
Pain + Bleeding + Product of Conception coming out from Internal Os
USG — RPOC
Management : If No Infection : Conservative Management.
If Bleeding Persist — D&E, Medical Management
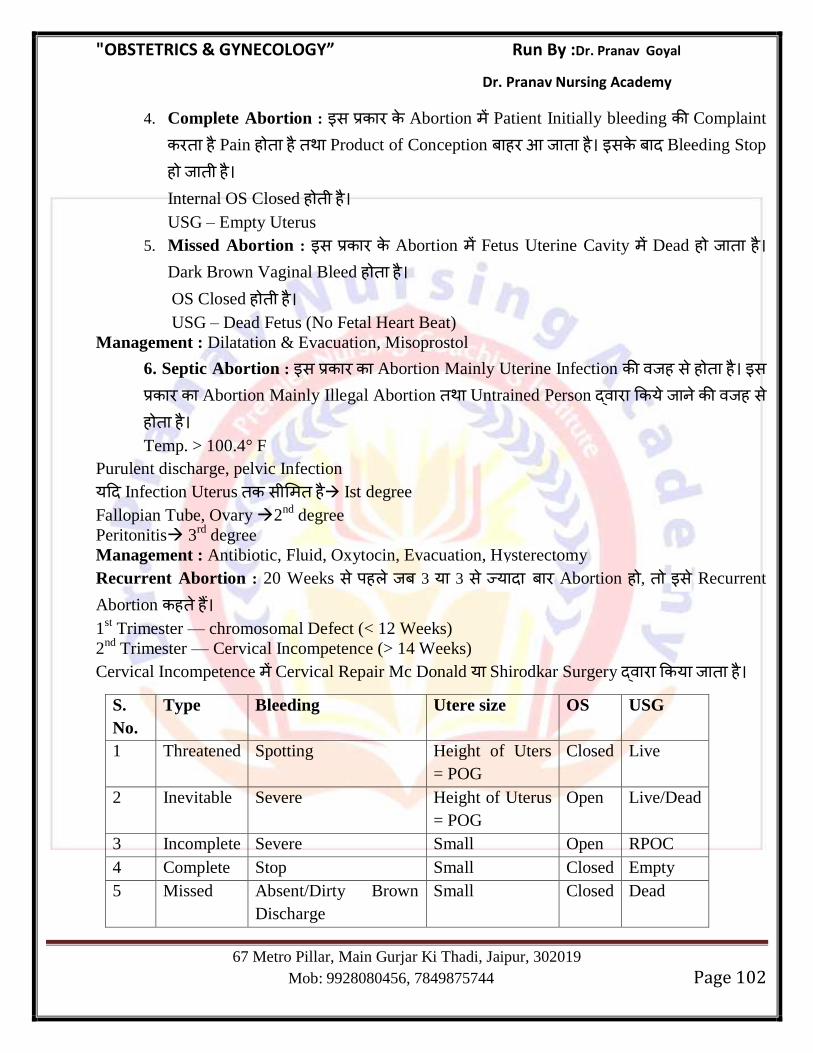
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 102
4. Complete Abortion : स Abortion Patient Initially bleeding Complaint
ह Pain ह ह Product of Conception ह ह स Bleeding Stop
ह ह
Internal OS Closed ह ह
USG – Empty Uterus
5. Missed Abortion : स Abortion Fetus Uterine Cavity Dead ह ह
Dark Brown Vaginal Bleed ह ह
OS Closed ह ह
USG – Dead Fetus (No Fetal Heart Beat)
Management : Dilatation & Evacuation, Misoprostol
6. Septic Abortion : स Abortion Mainly Uterine Infection ह स ह ह स
Abortion Mainly Illegal Abortion Untrained Person य ह स ह ह
Temp. > 100.4° F
Purulent discharge, pelvic Infection
य Infection Uterus स ह Ist degree
Fallopian Tube, Ovary 2nd
degree
Peritonitis 3rd
degree
Management : Antibiotic, Fluid, Oxytocin, Evacuation, Hysterectomy
Recurrent Abortion : 20 Weeks स ह 3 य 3 स य Abortion ह , स Recurrent
Abortion ह ह
1st Trimester — chromosomal Defect (< 12 Weeks)
2nd
Trimester — Cervical Incompetence (> 14 Weeks)
Cervical Incompetence Cervical Repair Mc Donald य Shirodkar Surgery य ह
S.
No.
Type Bleeding Utere size OS USG
1 Threatened Spotting Height of Uters
= POG
Closed Live
2 Inevitable Severe Height of Uterus
= POG
Open Live/Dead
3 Incomplete Severe Small Open RPOC
4 Complete Stop Small Closed Empty
5 Missed Absent/Dirty Brown
Discharge
Small Closed Dead
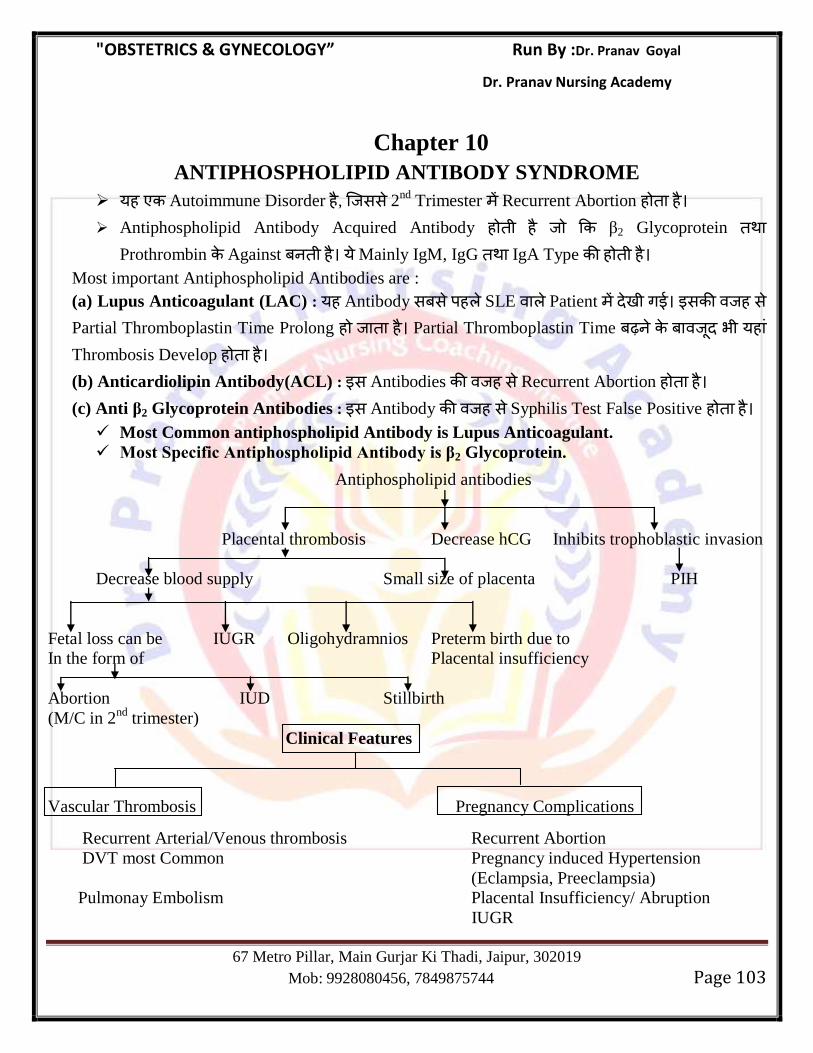
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 103
Chapter 10
ANTIPHOSPHOLIPID ANTIBODY SYNDROME
यह Autoimmune Disorder ह , सस 2nd Trimester Recurrent Abortion ह ह
Antiphospholipid Antibody Acquired Antibody ह ह β2 Glycoprotein Prothrombin Against ह य Mainly IgM, IgG IgA Type ह ह
Most important Antiphospholipid Antibodies are :
(a) Lupus Anticoagulant (LAC) : यह Antibody स स ह SLE Patient ग स ह स Partial Thromboplastin Time Prolong ह ह Partial Thromboplastin Time भ यह Thrombosis Develop ह ह
(b) Anticardiolipin Antibody(ACL) : स Antibodies ह स Recurrent Abortion ह ह
(c) Anti β2 Glycoprotein Antibodies : स Antibody ह स Syphilis Test False Positive ह ह
Most Common antiphospholipid Antibody is Lupus Anticoagulant.
Most Specific Antiphospholipid Antibody is β2 Glycoprotein.
Antiphospholipid antibodies
Placental thrombosis Decrease hCG Inhibits trophoblastic invasion
Decrease blood supply Small size of placenta PIH
Fetal loss can be IUGR Oligohydramnios Preterm birth due to
In the form of Placental insufficiency
Abortion IUD Stillbirth
(M/C in 2nd
trimester)
Clinical Features
Vascular Thrombosis Pregnancy Complications
Recurrent Arterial/Venous thrombosis Recurrent Abortion
DVT most Common Pregnancy induced Hypertension
(Eclampsia, Preeclampsia)
Pulmonay Embolism Placental Insufficiency/ Abruption
IUGR
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 104
DIAGNOSIS :
Clinical Criteria :
Unexplained one or more clinical episode of arterial,venous or small vessel thrombosis.
One or more Unexplained death of Morphologically normal fetus beyond 10th
week of
Gestation.
One or more premature birth before 34th
week of Gestation due to Eclampsia or preeclampsia
and placental Insufficiency.
Three or more unexplained consecutive spontaneous abortion before the 10th
week of
Gestation.
Laboratory Criteria :
Lupus Anticoagulant present in plasma on two or more occasion at least 12 week apart.
Anticardiolipin antibodiy of IgG/IgM isotype present in plasma on two or more occasion at
least 12 weeks apart.
Anti β2 Glycoprotein-1 antibodies present in plasma twice at least 12 weeks apart.
Management : 2 durgs are used.
1. Heparin : Regular or low molecular weight Heparin can be used. It should be started as soon
as Intrauterine pregnancy is diagnosed on USG. The drug has to be continued throughout
pregnancy and stopped at the onset of labor.
2. Aspirin : Should be started as soon as UPT become positive. It should be continued
throughout pregnancy and stopped 7 days before labor.
3. 2nd
Line therapy : Immunoglobulin therapy.
MTP (MEDICAL TERMINATION OF PREGNANCY ACT, 1971) :
India MTP Act स स ह ग , 1971 स ह 1972 स यह ग ह 1975 यह
ह
Indication :
(a) Therapeutic : Pregnancy Continue स Mother Physical Mental Health ह (b) Eugenic : ह Serious Physical Mental Abnormalities ह स भ ह
(c) Humanitarian : Pregnancy Rape ह ह
(d) Social : Married Woman Pregnancy Contraceptive Failure ह स ह ह Rules :
Who can do MTP : (i) Who has degree or diploma in OBS & Gynae.
(ii) Who has done 6 months house job in OBS & Gynae.
(iii) Who has assisted in 25 MTP‘s in an authorized center.
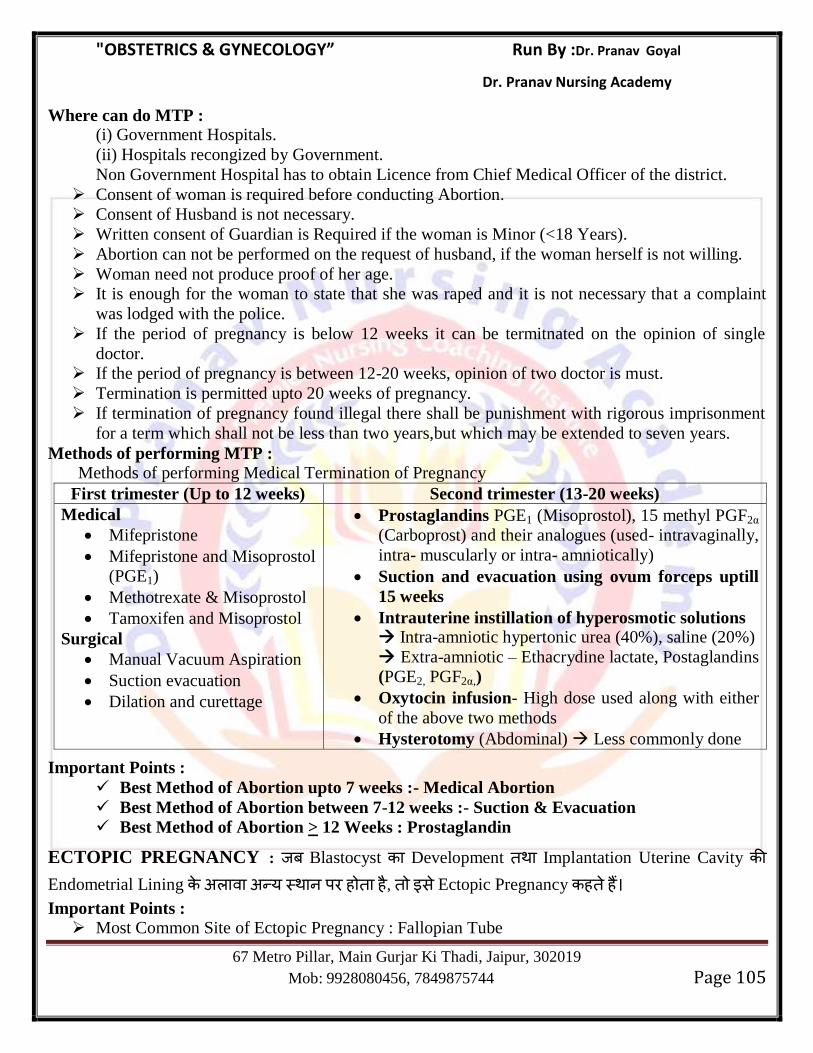
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 105
Where can do MTP : (i) Government Hospitals.
(ii) Hospitals recongized by Government.
Non Government Hospital has to obtain Licence from Chief Medical Officer of the district.
Consent of woman is required before conducting Abortion.
Consent of Husband is not necessary.
Written consent of Guardian is Required if the woman is Minor (<18 Years).
Abortion can not be performed on the request of husband, if the woman herself is not willing.
Woman need not produce proof of her age.
It is enough for the woman to state that she was raped and it is not necessary that a complaint
was lodged with the police.
If the period of pregnancy is below 12 weeks it can be termitnated on the opinion of single
doctor.
If the period of pregnancy is between 12-20 weeks, opinion of two doctor is must.
Termination is permitted upto 20 weeks of pregnancy.
If termination of pregnancy found illegal there shall be punishment with rigorous imprisonment
for a term which shall not be less than two years,but which may be extended to seven years.
Methods of performing MTP :
Methods of performing Medical Termination of Pregnancy
First trimester (Up to 12 weeks) Second trimester (13-20 weeks)
Medical
Mifepristone
Mifepristone and Misoprostol
(PGE1)
Methotrexate & Misoprostol
Tamoxifen and Misoprostol
Surgical
Manual Vacuum Aspiration
Suction evacuation
Dilation and curettage
Prostaglandins PGE1 (Misoprostol), 15 methyl PGF2α
(Carboprost) and their analogues (used- intravaginally,
intra- muscularly or intra- amniotically)
Suction and evacuation using ovum forceps uptill
15 weeks
Intrauterine instillation of hyperosmotic solutions Intra-amniotic hypertonic urea (40%), saline (20%)
Extra-amniotic – Ethacrydine lactate, Postaglandins
(PGE2, PGF2α,)
Oxytocin infusion- High dose used along with either
of the above two methods
Hysterotomy (Abdominal) Less commonly done
Important Points :
Best Method of Abortion upto 7 weeks :- Medical Abortion
Best Method of Abortion between 7-12 weeks :- Suction & Evacuation
Best Method of Abortion > 12 Weeks : Prostaglandin
ECTOPIC PREGNANCY : Blastocyst Development Implantation Uterine Cavity Endometrial Lining य ह ह , स Ectopic Pregnancy ह ह Important Points :
Most Common Site of Ectopic Pregnancy : Fallopian Tube
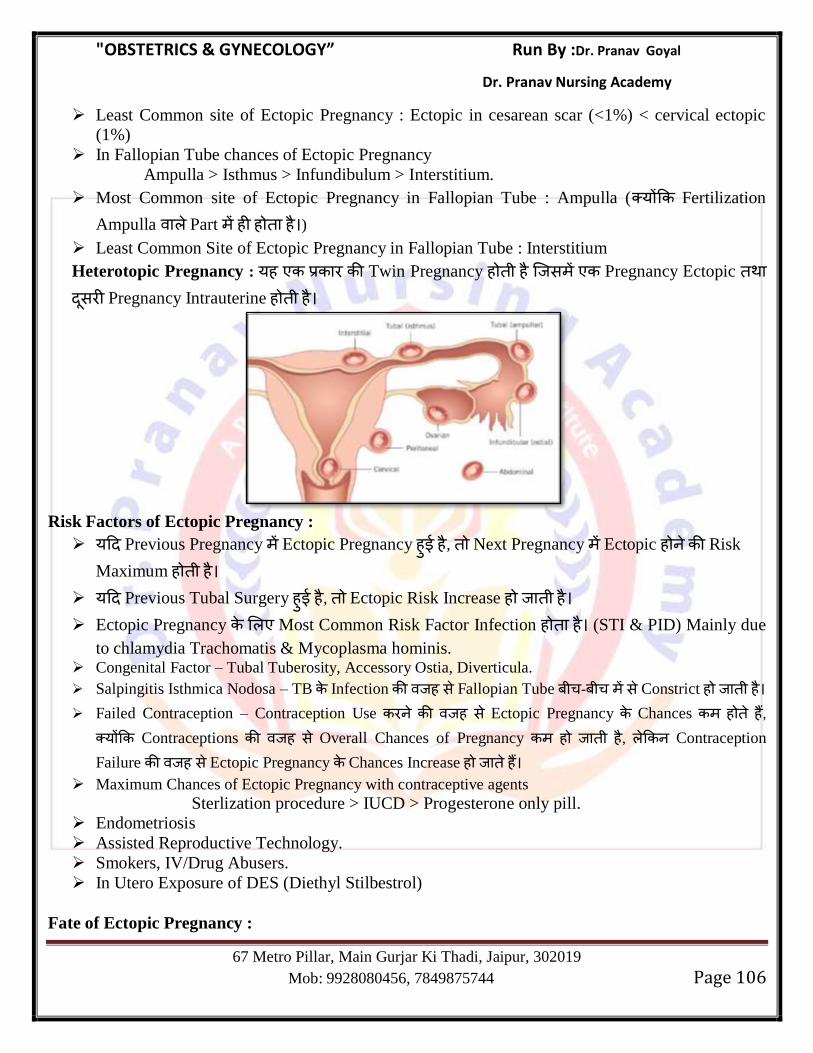
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 106
Least Common site of Ectopic Pregnancy : Ectopic in cesarean scar (<1%) < cervical ectopic
(1%)
In Fallopian Tube chances of Ectopic Pregnancy
Ampulla > Isthmus > Infundibulum > Interstitium.
Most Common site of Ectopic Pregnancy in Fallopian Tube : Ampulla ( य Fertilization
Ampulla Part ह ह ह )
Least Common Site of Ectopic Pregnancy in Fallopian Tube : Interstitium
Heterotopic Pregnancy : यह Twin Pregnancy ह ह स Pregnancy Ectopic स Pregnancy Intrauterine ह ह
Risk Factors of Ectopic Pregnancy :
य Previous Pregnancy Ectopic Pregnancy ह ह , Next Pregnancy Ectopic ह Risk
Maximum ह ह
य Previous Tubal Surgery ह ह , Ectopic Risk Increase ह ह
Ectopic Pregnancy Most Common Risk Factor Infection ह ह (STI & PID) Mainly due
to chlamydia Trachomatis & Mycoplasma hominis. Congenital Factor – Tubal Tuberosity, Accessory Ostia, Diverticula.
Salpingitis Isthmica Nodosa – TB Infection ह स Fallopian Tube - स Constrict ह ह
Failed Contraception – Contraception Use ह स Ectopic Pregnancy Chances ह ह , य Contraceptions ह स Overall Chances of Pregnancy ह ह , Contraception
Failure ह स Ectopic Pregnancy Chances Increase ह ह
Maximum Chances of Ectopic Pregnancy with contraceptive agents
Sterlization procedure > IUCD > Progesterone only pill.
Endometriosis
Assisted Reproductive Technology.
Smokers, IV/Drug Abusers.
In Utero Exposure of DES (Diethyl Stilbestrol)
Fate of Ectopic Pregnancy :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 107
(i) Tubal Abortion : Ectopic Pregnancy Fallopian Tube Ampulla Infundibulum Part ह ह , Tube ह Abortion ह ह
(ii) Rupture of the Tube : Ectopic Pregnancy Fallopian tube Isthmus Interstitial Part ह ह , Tube Rupture ह स भ स स य ह ह
Most Common site of Tubal Abortion - Ampulla
Most Common Site of Tubal Rupture - Isthmus
Fallopian tube Ectopic Pregnancy end स स ह Isthmus Part ह ह (6 Week)
Fallopian Tube Ectopic Pregnancy Maximum Survival Interstitum Part ह ह , य यह स Uterine Myometrium स Support ह ह स Ectopic Pregnancy Most Dangerous site
Interstitium ह
Overall Ectopic Pregnancy Longest Survival Abdomen ह ह यह Ectopic pregnancy Term
Continue ह स ह
Symptoms and Sign :
Classical Triad : Amenorrhoea, Abdominal Pain, Vaginal Bleeding.
Ruptured Ectopic Pregnancy Pain Mainly Hemoperitoneum ह स ह ह blood Diaphragmatic Irritation ह ह स Pain Shoulder Referred ह स ह स Danforth Sign
ह ह
Unruptured Ectopic Pregnancy Pain Fallopian Tube Stretching ह स ह ह
Sign :
Ruptured Ectopic Pregnancy Patient Shock ह ग (BP-Decrease, HR-Increase)
P/A examination-Tenderness, Rigidity, Guarding in Lower Abdomen
Hemoperitoneum ह स Periumbilical Region Bluish Discoloration ह ह स Cullen Sign
ह ह
P/V Examination : Cervical Movement Tender,
Bulging of Post Vaginal Fornix due to Blood Collection in POD
Tender Boggy Mass may be felt on one side of uterus.
Ruptured Ectopic : भ Female 6-10 Weeks Amenorrhoea, Lower Abdominal Pain स य
Urine Pregnancy Test Positive ह , Patient Shock ह , ह Ectopic Pregnancy Possibility स स ह स ह
Management of Ruptured Ectopic Pregnancy :
Simultaneous Resuscitation & Laparotomy.
Ruptured Ectopic Pregnancy ह Salpingectomy ह ह Female Primiparous ह Multiparous.
Salpingectomy Ruptured Ectopic Gold Standard Treatment ह ह
Ruptured Ectopic Expectant/Medical management ह य
Unruptured Ectopic Pregnancy :
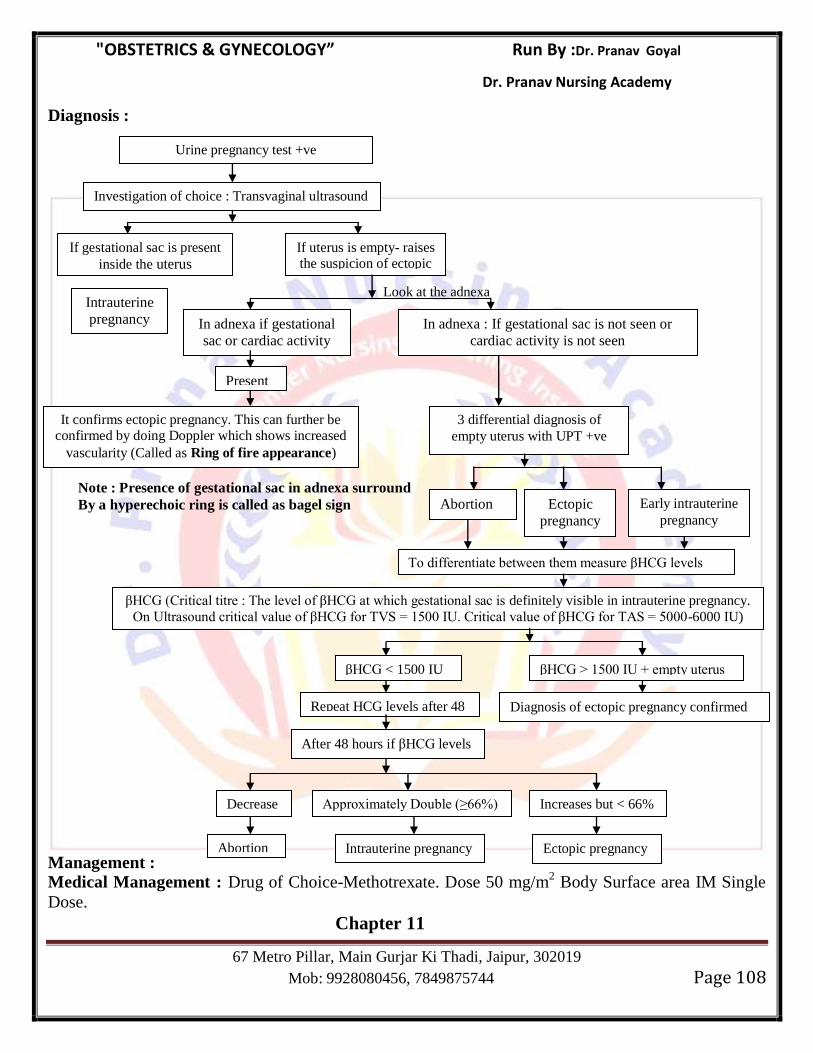
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 108
Diagnosis :
Look at the adnexa
Note : Presence of gestational sac in adnexa surround
By a hyperechoic ring is called as bagel sign
Management :
Medical Management : Drug of Choice-Methotrexate. Dose 50 mg/m2 Body Surface area IM Single
Dose.
Chapter 11
Urine pregnancy test +ve
Investigation of choice : Transvaginal ultrasound
(TVS)
βHCG (Critical titre : The level of βHCG at which gestational sac is definitely visible in intrauterine pregnancy.
On Ultrasound critical value of βHCG for TVS = 1500 IU. Critical value of βHCG for TAS = 5000-6000 IU)
βHCG > 1500 IU + empty uterus βHCG < 1500 IU
Repeat HCG levels after 48 hours
If gestational sac is present
inside the uterus
If uterus is empty- raises the suspicion of ectopic
pregnancy
Intrauterine
pregnancy In adnexa : If gestational sac is not seen or
cardiac activity is not seen
In adnexa if gestational
sac or cardiac activity
Present
It confirms ectopic pregnancy. This can further be confirmed by doing Doppler which shows increased
vascularity (Called as Ring of fire appearance)
3 differential diagnosis of
empty uterus with UPT +ve
To differentiate between them measure βHCG levels
Early intrauterine
pregnancy Ectopic
pregnancy
Abortion
After 48 hours if βHCG levels
Diagnosis of ectopic pregnancy confirmed
Decrease Approximately Double (≥66%) Increases but < 66%
Ectopic pregnancy Intrauterine pregnancy Abortion
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 109
TROPHOBLASTIC DISEASE
Hydatiform Mole :
यह Most Common Gestational Trophoblastic Disease ह
यह Placenta Abnormal Condition ह , स Chorionic villi partly Degenerative Partly Proliferative Changes ह ह
Hydatiform Mole Benign Neoplasm of Chorion ह स Malignant Potential ह ह
ह Choriocarcinoma Convert ह स ह
Uterine Cavity Multiple Grapes Like Vesicles ह Fetus Normally Absent ह ह
Vesicles Interstitial Fluid ह ह स hCG ह ह
Microscopically :
(a) Marked Proliferation of Syncytio & Cytotrophoblastic epithelium.
(b) Thinning of Stromal tissue due to hydropic degeneration.
(c) Avascular Vill
Risk Factor :
Maximum Incidence Asia South America & Least in USA.
Maximum Incidence in Philippines (1 in 80), in India (1 in 400 Pregnancies)
य Woman Age > 35 Year स य ह < 18 Year स ह , Risk य ह ह
Low Socioeconomic Status
History of Molar Pregnancy
Diet Deficient in Protein, Folic Acid and Vitamin A
Blood Group A woman married to group O Man.
Pathophysiology of H.Mole :
H. Mole Blastocyts Trophoblast Excessive Proliferation ह स Develop ह ह
Proliferating Trophoblast Fluid Secret ह Chorionic Villi ह ह औ Grapes
Like Vesicles ह Hydropic Degeneration ह ह
Uterus Grapes Like Vesicles भ ह सस Blastocyst Inner Cell Mass Grow Space
ह
य Fetal Part Develop ह ह , य Fetal Part Develop ह ह ह Partial Mole ह Complete Mole ह
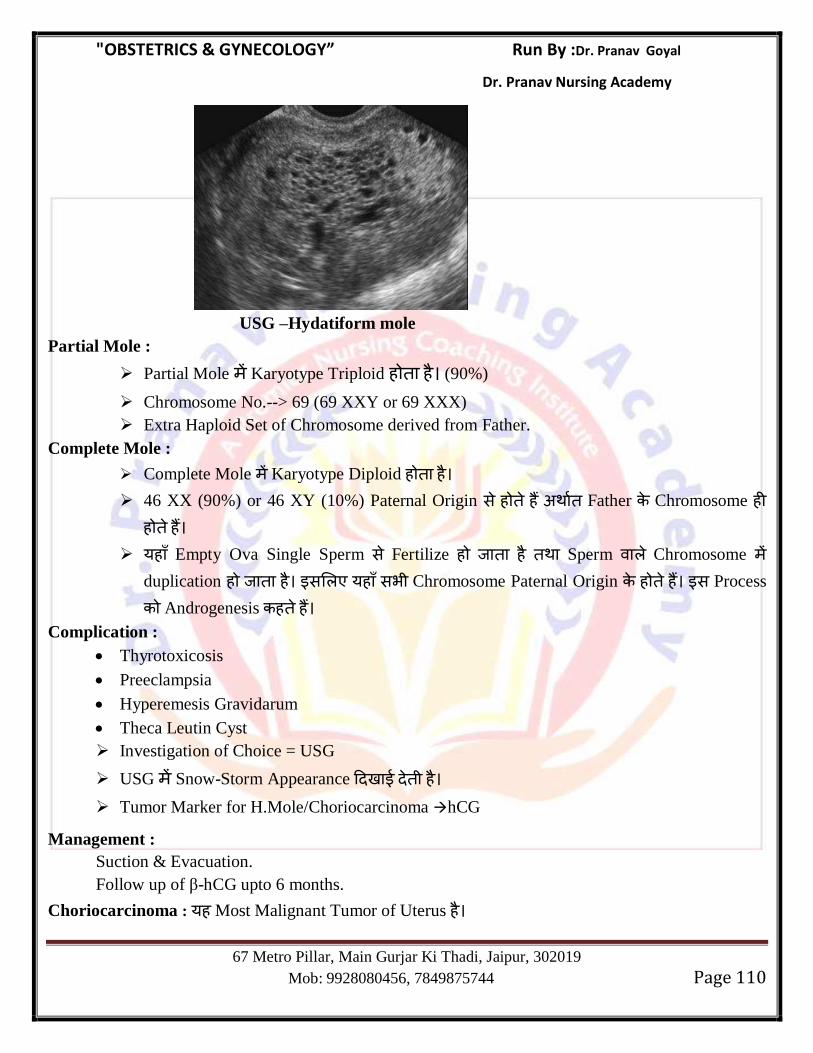
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 110
USG –Hydatiform mole
Partial Mole :
Partial Mole Karyotype Triploid ह ह (90%)
Chromosome No.--> 69 (69 XXY or 69 XXX)
Extra Haploid Set of Chromosome derived from Father.
Complete Mole :
Complete Mole Karyotype Diploid ह ह
46 XX (90%) or 46 XY (10%) Paternal Origin स ह ह Father Chromosome ह ह ह
यह Empty Ova Single Sperm स Fertilize ह ह Sperm Chromosome duplication ह ह स यह सभ Chromosome Paternal Origin ह ह स Process
Androgenesis ह ह
Complication :
Thyrotoxicosis
Preeclampsia
Hyperemesis Gravidarum
Theca Leutin Cyst
Investigation of Choice = USG
USG Snow-Storm Appearance ह
Tumor Marker for H.Mole/Choriocarcinoma hCG
Management :
Suction & Evacuation.
Follow up of β-hCG upto 6 months.
Choriocarcinoma : यह Most Malignant Tumor of Uterus ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 111
Causes :
50% develop following H.Mole.
25% develop following on Abortion.
20% develop following full term pregnancy.
5% develop following Ectopic Pregnancy.
Most common mode of spread : Hematogenous.
Most Common site of Metastasis of Choriocarcinoma
Lung 80% > Vagina (30%) > Pelvis (20%) Liver & Brain (10%)
Symptoms : Irregular Bleeding
Snow Storm appearance in Uterus (USG) : H.Mole
Snow Storm apperance in Lungs (X-Ray) : Choriocarcinoma
Tumor Marker for Choriocarcinoma : β hCG
Tumor Marker for placental site trophoblastic tumor : hPL (Human Placental Lactogen)
Management : Chemotherapy
Methotrexate is drug of choice
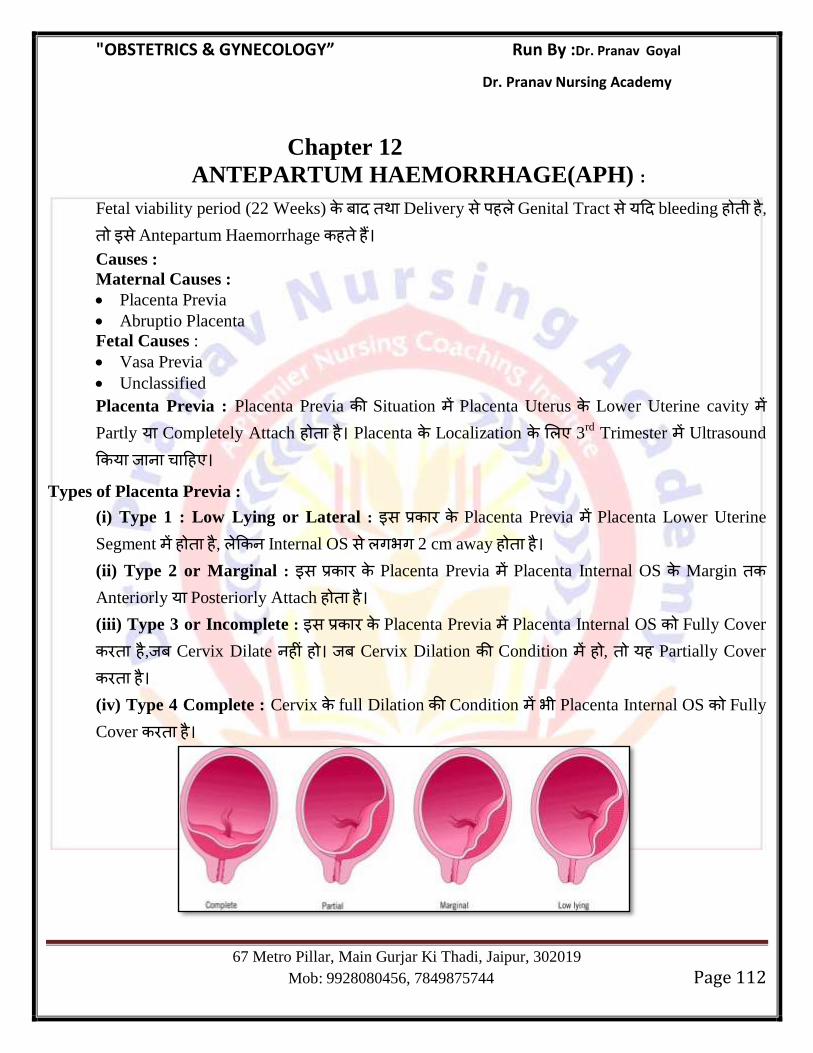
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 112
Chapter 12
ANTEPARTUM HAEMORRHAGE(APH) :
Fetal viability period (22 Weeks) Delivery स ह Genital Tract स य bleeding ह ह , स Antepartum Haemorrhage ह ह
Causes :
Maternal Causes :
Placenta Previa
Abruptio Placenta
Fetal Causes :
Vasa Previa
Unclassified
Placenta Previa : Placenta Previa Situation Placenta Uterus Lower Uterine cavity Partly य Completely Attach ह ह Placenta Localization 3
rd Trimester Ultrasound
य ह
Types of Placenta Previa :
(i) Type 1 : Low Lying or Lateral : स Placenta Previa Placenta Lower Uterine
Segment ह ह , Internal OS स गभग 2 cm away ह ह
(ii) Type 2 or Marginal : स Placenta Previa Placenta Internal OS Margin
Anteriorly य Posteriorly Attach ह ह
(iii) Type 3 or Incomplete : स Placenta Previa Placenta Internal OS Fully Cover
ह , Cervix Dilate ह ह Cervix Dilation Condition ह , यह Partially Cover
ह
(iv) Type 4 Complete : Cervix full Dilation Condition भ Placenta Internal OS Fully
Cover ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 113
Placenta Previa Condition Placenta Fetus OS Compress ह ह सस Bleeding स भ ह ह
Type 1 Type 2 Placenta OS ह Cover ह स Bleeding ह ह
Type 3 Type 4 Placenta OS Cover ह स Bleeding य ह ह
Minor Degree : Type 1, Type 2 Anterior.
Major Degree : Type 2 Posterior, Type 3 & Type 4
Type 2 Posterior Placenta Previa Dangerous Type ह ह , य यह Pelvis Ischial Spine Level Attach ह ह सस Fetal Head Engagement ह ह ह स Cord
Compression स भ स स य ह ह सस Fetal Asphyxia भ - भ Fetal Death भ ह स ह
Stallworthy Sign : Fetal Head Pelvis Push ह ह , स स य Fetal Heart Rate Decrease
ह ह स Stallworthy sign ह ह Mainly Posterior Placenta Previa Stallworthy Sign Present
ह ह
Risk Factor :
Previous H/O Placenta Previa.
Multiparity & Increased Maternal Age.
H/O any Previous Uterine Surgery : Like Cesarean section (Risk Increase as No. of cesarean
Increases), Myomectomy.
Previous Uterine Curettage.
Increased placental size seen in Multifetal pregnancy.
Succenturiate Lobe.
Smoking
Increased Maternal serum AFP
Clincial Features :
Symptoms : In Placenta Previa Bleeding is :
Painless
Recurrent
Revealed
Sign :
Pallor :Proportionate to the amount of Bleeding.
Size of Uterus corresponds to the period of Amenorrhoea.
Uterus is soft and Nontender.
Malpresentations are common and if it is in cephalic presentation, head is usually floating.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 114
Fetal Heart sound Heard.
Note : Suspected Placenta Previa Vaginal Examination ह य ह
Management :
Placenta Previa Vaginal Examination ह ह
Investigation of Choice : TVS Ultrasound
Double set up examination : Placenta Previa Situation Per vaginal Examination
Operation Theatre य ह ह Cesarean Facility availabe ह ह
(i) Expectant Management (Macafee Regime)
Indication :
No Active Bleeding Present.
Hemodynamically Stable.
Gestation age < 37 Weeks.
CTG – should be Reactive
No Fetal Anomally incompatible with life.
Steps :
Hospitalize the Patient.
Arrange for Blood.
If patient is Rh (–), give her Anti D.
Give Injection corticosteroid to hasten lung maturity of Fetus.
If contraction present give short term tocolytic (Nifedipine)
Expectant Management 37 Week ह य Expectant Management
patient स भ स य Rebleed ह , Pregnancy Immediate Terminate ह (ii) Active Management : Active Management Pregnancy Immediate Terminate य ह ह Fetus Gestational Age भ ह
Indication :
If active Bleeding Present.
Haemodynamically Unstable/Shock.
Gestational Age > 37 Weeks.
Fetal Distress Present.
FHS absent.
USG Shows fetal anomally incompatible with life.
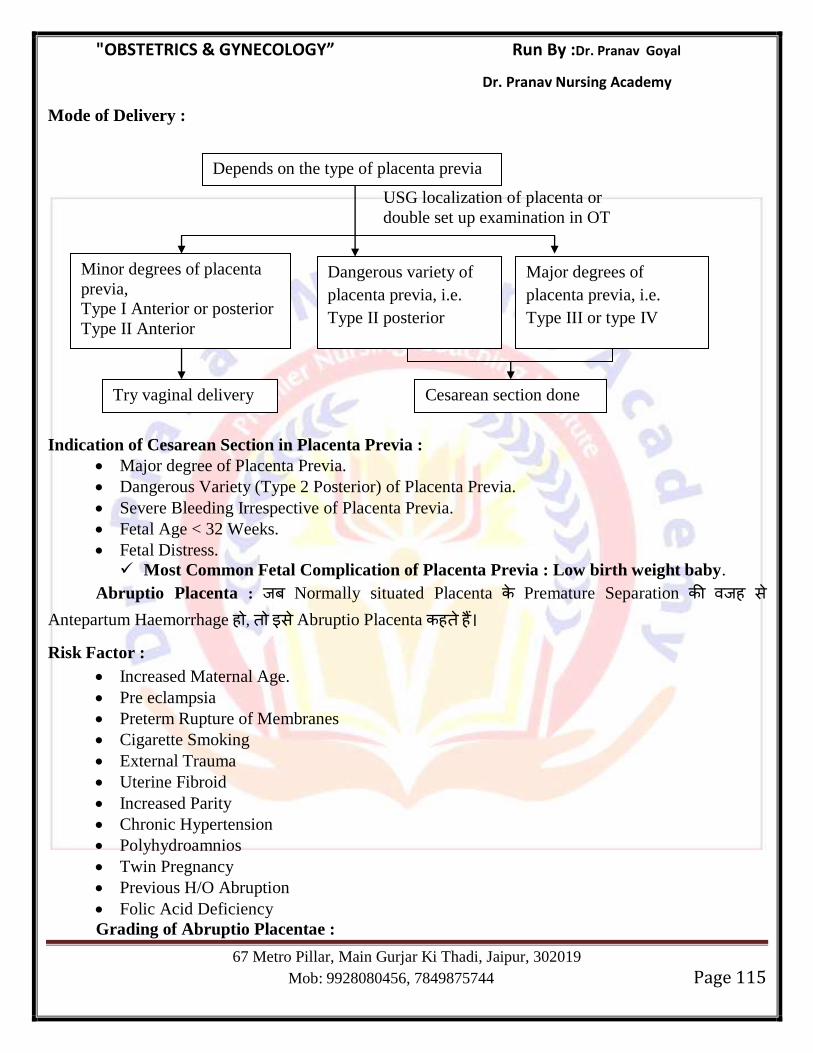
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 115
Mode of Delivery :
USG localization of placenta or
double set up examination in OT
Indication of Cesarean Section in Placenta Previa :
Major degree of Placenta Previa.
Dangerous Variety (Type 2 Posterior) of Placenta Previa.
Severe Bleeding Irrespective of Placenta Previa.
Fetal Age < 32 Weeks.
Fetal Distress.
Most Common Fetal Complication of Placenta Previa : Low birth weight baby.
Abruptio Placenta : Normally situated Placenta Premature Separation ह स Antepartum Haemorrhage ह , स Abruptio Placenta ह ह
Risk Factor :
Increased Maternal Age.
Pre eclampsia
Preterm Rupture of Membranes
Cigarette Smoking
External Trauma
Uterine Fibroid
Increased Parity
Chronic Hypertension
Polyhydroamnios
Twin Pregnancy
Previous H/O Abruption
Folic Acid Deficiency
Grading of Abruptio Placentae :
Depends on the type of placenta previa
Dangerous variety of
placenta previa, i.e.
Type II posterior
Try vaginal delivery
Minor degrees of placenta
previa,
Type I Anterior or posterior
Type II Anterior
Major degrees of
placenta previa, i.e.
Type III or type IV
Cesarean section done
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 116
Grade Bleeding Uterus B.P. or Pulse Heart rate Separation
0 No No change No change No change <10%
1 Mild No change No change No change 10-20%
2 Moderate Tender Altered Distress 20-30%
3 Severe Titanic contraction Shock Death >50%
Types of Abruptio Placenta :
(i) Concealed : स Variety Placenta स Separate ह ह Blood Placenta ह ह ह Vagina ह ह ह Collected Blood Uterus Wall Middle Outer Muscle Layer Intravasate ह ह सस Muscle Layer Separate ह ह
स Couvelaire Uterus (Uteroplacental Apoplexy) ह ह couvelaire Uterus Hysterectomy ह ह
(ii) Revealed : स Variety Placenta स Separate ह ह Blood Vagina ह ह
(iii) Mixed : Blood Placenta ह ह , Vagina ह ह (Most Common Variety)
Clincical Features :
Symptoms :
Severe and constant Abdominal pain (More in concealed and less in Revealed)
Bleeding : Absent in concealed type present in revealed & Mixed type.
Abruptio Placenta Bleeding Placenta Previa Different ह ह
Associated with pain in Abdomen.
Non-Recurrent in same pregnancy.
No warning Haemorrhage.
Never without any reason.
Sign :
General condition of patient is usually out of proportion to the extent of Bleeding.
Hypertension may present (Preeclampsia)
Uterus will be larger than period of amenorrhoea (In concealed variety)
Uterus may be tender, tense, rigid (woddy hard)
Difficulty in palpating the underlying fetal part.
Fetal distress absent FHS.
Management :
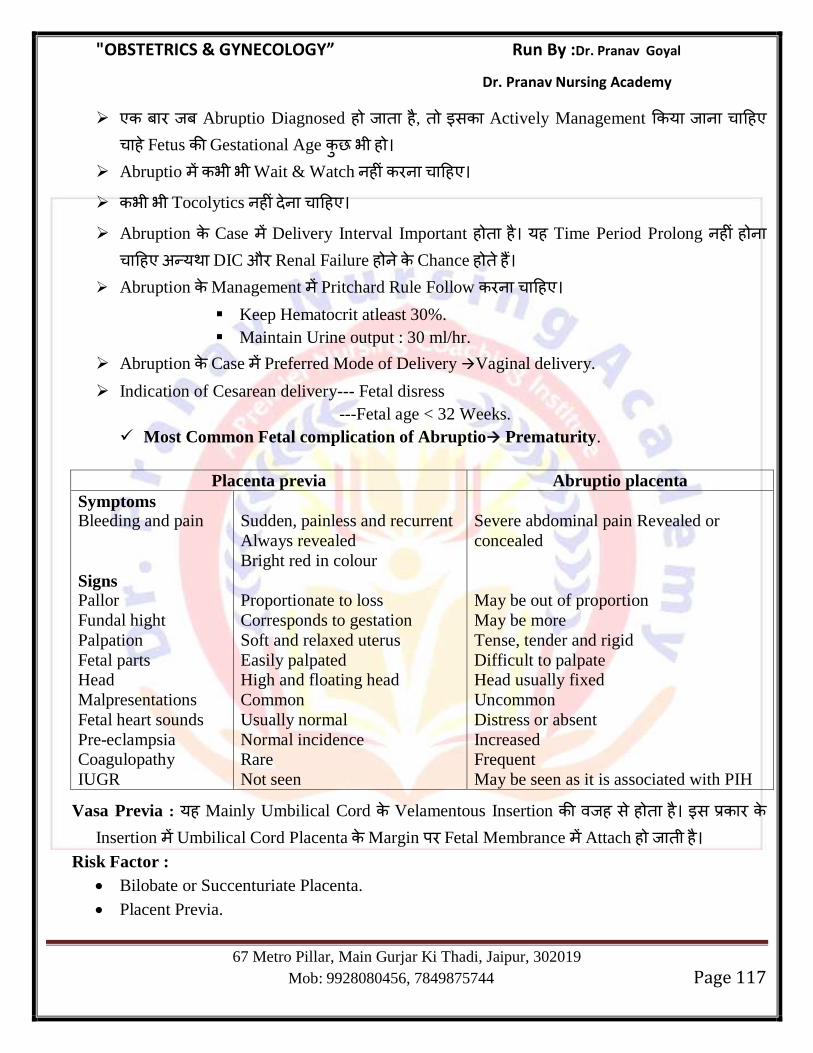
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 117
Abruptio Diagnosed ह ह , स Actively Management य ह
ह Fetus Gestational Age भ ह
Abruptio भ भ Wait & Watch ह ह
भ भ Tocolytics ह ह
Abruption Case Delivery Interval Important ह ह यह Time Period Prolong ह ह ह य DIC औ Renal Failure ह Chance ह ह
Abruption Management Pritchard Rule Follow ह
Keep Hematocrit atleast 30%.
Maintain Urine output : 30 ml/hr.
Abruption Case Preferred Mode of Delivery Vaginal delivery.
Indication of Cesarean delivery--- Fetal disress
---Fetal age < 32 Weeks.
Most Common Fetal complication of Abruptio Prematurity.
Placenta previa Abruptio placenta
Symptoms Bleeding and pain
Signs Pallor
Fundal hight
Palpation
Fetal parts
Head
Malpresentations
Fetal heart sounds
Pre-eclampsia
Coagulopathy
IUGR
Sudden, painless and recurrent
Always revealed
Bright red in colour
Proportionate to loss
Corresponds to gestation
Soft and relaxed uterus
Easily palpated
High and floating head
Common
Usually normal
Normal incidence
Rare
Not seen
Severe abdominal pain Revealed or
concealed
May be out of proportion
May be more
Tense, tender and rigid
Difficult to palpate
Head usually fixed
Uncommon
Distress or absent
Increased
Frequent
May be seen as it is associated with PIH
Vasa Previa : यह Mainly Umbilical Cord Velamentous Insertion ह स ह ह स Insertion Umbilical Cord Placenta Margin Fetal Membrance Attach ह ह
Risk Factor :
Bilobate or Succenturiate Placenta.
Placent Previa.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 118
Blood Loss mainly fetal Origin ह ह स Fetal Mortality Chances Increase ह ह Maternal Mortality Chance ह ह ह
Bleeding ह ह , Fetal Anaemia ह स FHS Sinusoidal Pattern ह Diagnosis ,Bleeding स य Singers Alkali Denaturation/Apt Test स य ह
Management : Emergency Cesarean Section
Chapter 13
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 119
MULTIFETAL PREGNANCY
Zygosity : Twins Monozygotic य Dizygotic ह स ह
Zygosity : Refers to the type of conception.
Dizygotic (75%) dizygotic Twins Ova ग- ग Spermatozoa Fertilization स ह
Monozygotic (25%) : Monozygotic Twin Single Zygote Divide ह स ह स Sex Same ह ह स ह
Dizygotic Twins :
More Common (70%)
Incidence of Dizygotic Twins Increases with.
Increased Maternal Age.
Increased parity.
Maternal Family H/O Twining.
Ovulution Induction drugs like clomiphine or gonadotropin.
Dizygotic Twin ग- ग Zygote ह स स Twins Baby Sex
Same Different ह स ह
Dizygotic Twins ह 2 Chorion 2 Amnion ह ह (Dichorionic & Diamniotic)
Dizygotic Twins Genetic Feature, Finger Prints भ ग- ग ह ह Skin Graft भ स Reject ह ह
Monozygotic Twins :
Less Common (30%)
स Twins य ह Zygote Split ह स ह स Fetus Sex ह स ह ह
Chorion Amnion स य Zygote Split ह Time Depend ह
स Twins Genetic Feature, DNA imprints Same ह ह Skin Grafts स Accept ह ह
Fingerprints स Different ह ह Important Points :
Incidence of Twins Highest in Nigeria (1 in 20)
Incidence of Twins lowest in Japan.
Incidence of Twins in India : 1 in 80
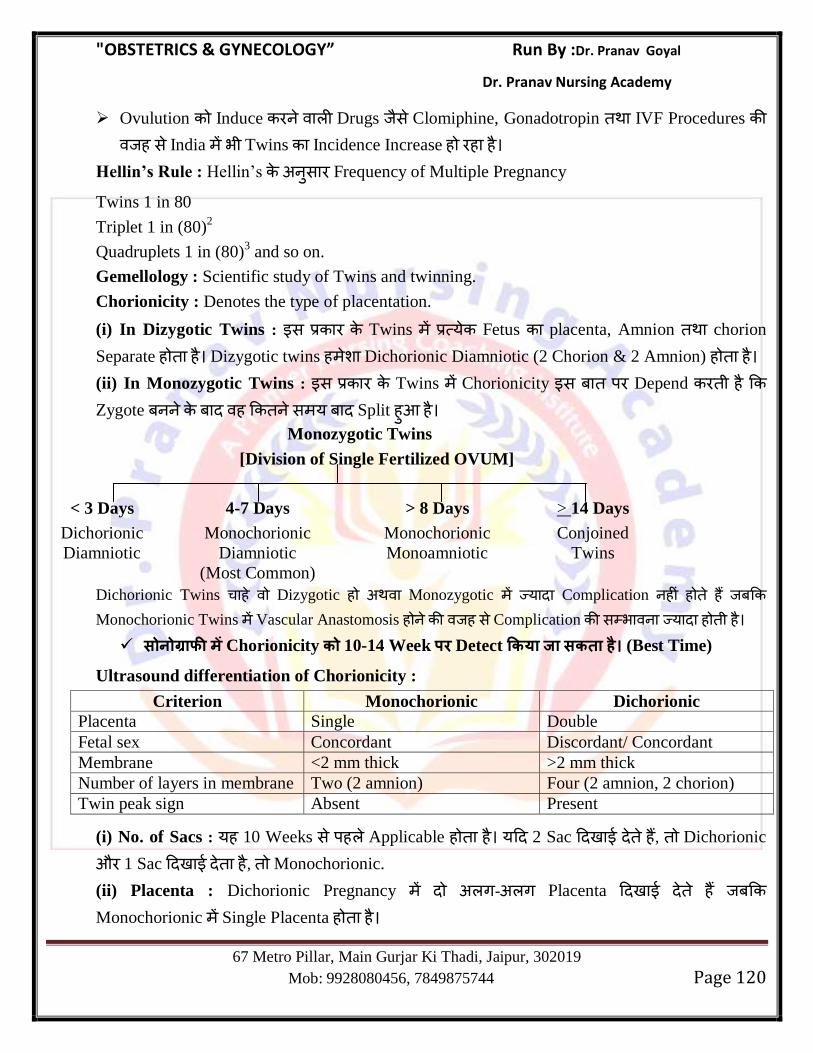
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 120
Ovulution Induce Drugs स Clomiphine, Gonadotropin IVF Procedures ह स India भ Twins Incidence Increase ह ह ह
Hellin’s Rule : Hellin‘s स Frequency of Multiple Pregnancy
Twins 1 in 80
Triplet 1 in (80)2
Quadruplets 1 in (80)3 and so on.
Gemellology : Scientific study of Twins and twinning.
Chorionicity : Denotes the type of placentation.
(i) In Dizygotic Twins : स Twins य Fetus placenta, Amnion chorion
Separate ह ह Dizygotic twins ह Dichorionic Diamniotic (2 Chorion & 2 Amnion) ह ह (ii) In Monozygotic Twins : स Twins Chorionicity स Depend ह
Zygote ह स य Split ह ह
Monozygotic Twins
[Division of Single Fertilized OVUM]
< 3 Days 4-7 Days > 8 Days > 14 Days
Dichorionic Monochorionic Monochorionic Conjoined
Diamniotic Diamniotic Monoamniotic Twins
(Most Common)
Dichorionic Twins ह Dizygotic ह Monozygotic य Complication ह ह ह
Monochorionic Twins Vascular Anastomosis ह ह स Complication स भ य ह ह
Chorionicity 10-14 Week पर Detect (Best Time)
Ultrasound differentiation of Chorionicity :
Criterion Monochorionic Dichorionic
Placenta Single Double
Fetal sex Concordant Discordant/ Concordant
Membrane <2 mm thick >2 mm thick
Number of layers in membrane Two (2 amnion) Four (2 amnion, 2 chorion)
Twin peak sign Absent Present
(i) No. of Sacs : यह 10 Weeks स ह Applicable ह ह य 2 Sac ह , Dichorionic
औ 1 Sac ह , Monochorionic.
(ii) Placenta : Dichorionic Pregnancy ग- ग Placenta ह
Monochorionic Single Placenta ह ह
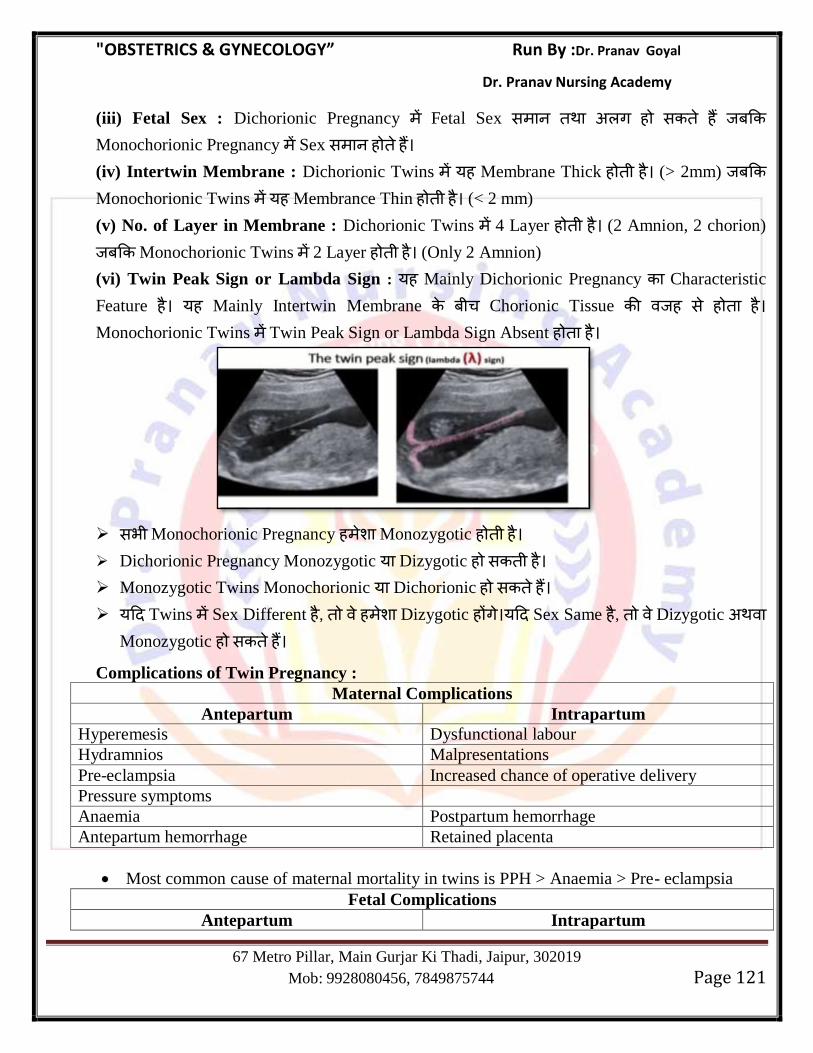
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 121
(iii) Fetal Sex : Dichorionic Pregnancy Fetal Sex स ग ह स ह
Monochorionic Pregnancy Sex स ह ह
(iv) Intertwin Membrane : Dichorionic Twins यह Membrane Thick ह ह (> 2mm)
Monochorionic Twins यह Membrance Thin ह ह (< 2 mm)
(v) No. of Layer in Membrane : Dichorionic Twins 4 Layer ह ह (2 Amnion, 2 chorion)
Monochorionic Twins 2 Layer ह ह (Only 2 Amnion)
(vi) Twin Peak Sign or Lambda Sign : यह Mainly Dichorionic Pregnancy Characteristic
Feature ह यह Mainly Intertwin Membrane Chorionic Tissue ह स ह ह
Monochorionic Twins Twin Peak Sign or Lambda Sign Absent ह ह
सभ Monochorionic Pregnancy ह Monozygotic ह ह
Dichorionic Pregnancy Monozygotic य Dizygotic ह स ह
Monozygotic Twins Monochorionic य Dichorionic ह स ह
य Twins Sex Different ह , ह Dizygotic ह ग य Sex Same ह , Dizygotic Monozygotic ह स ह
Complications of Twin Pregnancy :
Maternal Complications
Antepartum Intrapartum
Hyperemesis Dysfunctional labour
Hydramnios Malpresentations
Pre-eclampsia Increased chance of operative delivery
Pressure symptoms
Anaemia Postpartum hemorrhage
Antepartum hemorrhage Retained placenta
Most common cause of maternal mortality in twins is PPH > Anaemia > Pre- eclampsia
Fetal Complications
Antepartum Intrapartum
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 122
Prematurity PROM and cord prolapse
IUGR
Single fetal demise Abruption in the second twin
Monochorionic monoamniotic twins
Twin-twin transfusion syndrome Interlocking of twins (extremely rare)
Vanishing twin and abortion
Congenital anomalies including acardiac fetus
and conjoined twins
Most Commmon cause of perinatal death in twins is pre-maturity > IUGR > Infection
Complications specific to monochorionic twins
Twin-twin transfusion syndrome
Conjoined twining
Acardiac fetus
Selective IUGR
Single fetus demise
Complications specific to monoamniotic twins
Cord entanglement
Conjoint Twins Siamese Twins भ ह ह Different type of conjoined twins.
(a) Thoracopagus : Fusion at Chest. Most Common (40%)
(b) Omphalopagus (Xiphopagus) : Fuision at Anterior Abdominal wall (33%)
(c) Pyopagus : Fusion at buttocks (18%)
(d) Ischiopagus : Fusion at Ischium (6%)
(e) Craniopagus : Fusion at Head (2%) Least Common.
Mode of delivery of Conjoint twins : Cesarean section.
Monoamniotic Twin Pregnancies :
Monoamniotic twin pregnancies Rare ह ह (Only 1% of Monozygotic Twins).
Main Complication : Umbilical Cord entanglement
Congenital Malformation
Preterm Delivery.
Sonographic Diagnosis : Single Amniotic Membrane
Twins of Same Sex
Presence of Single Placenta
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 123
Best Criteria to Diagnose Monochorionic Monoamniotic twins is single Amniotic Cavity.
Color Doppler Examination : Variable Deceleration seen in cord entanglement.
Mode of Delivery : Cesarean section after 2 dose of betamethasone between 32-34 weeks.
Twin to twin transfusion syndrone (TTTS) :
यह ह Monochorionic Twins ह
यह Deep Arteriovenous Malformation ह ह स Donor Twin Umbilical Artery Recipient Twin Umbilical Vein स Abnormal Communication ह ह
Donor Twin : IUGR, Hypovolemia, Oligohydroamnios, Anaemia.
Recipient Twin : Macrosomia, Hypervolemia, Polycythemia, Polyhydroamnios, Plethoric
Twin to twin transfusion female fetus य Common ह ह
Fetus Heart Failure ह स ह Recipient Fetus Cardiac complication ह स Death य Chance ह ह
Important Points :
Twin Pregnancy Fetus Most Common lie Longitudinal ह ह
Twin Pregnancy Most Common Presentation Fetus Vertex Presentation ह ह
Both Vertex (Most Common) : 60%
Vertex (Ist) Breech (IInd) : 20%
Breech (Ist) Vertex (IInd) : 10%
Both Breech : 8-10%
Management of Labor
Time of Delivery :
Monochorionic Monoamniotic Twins: Cesarean section at 32-34 weeks after giving
corticosteroid.
Monochorionic Diamniotic : elective delivery at 36-37 weeks.
Dichorionic Twins : elective cesarean 37-38 weeks.
Triplet Pregnancy : elective cesarean at 35 weeks after giving corticosteroid.
Mode of Delivery :
If Ist twin is Cephalic than Vaginal delivery is possible.
If Ist twin is Breech/Transverse than cesarean section should be done.
Condition 1 :
If Ist twin is cephalic Vaginal delivery
If 2nd
Twin is cephalic Vaginal delivery.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 124
Condition 2 :
If 1st Twin is cephalic Normal vaginal delivery.
2nd
Twin breech Assisted breech delivery.
Condition 3 :
If 1st twin cephalic Normal vaginal delivery.
2nd
twin transverse lie. Internal podalic version
under GA in OT
Make it breech
Do breech extraction.
Condition 4 :
If 1st twin breech/Transverse lie always do cesarean section.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 125
Chapter 14
PREGNANCY IN Rh- NEGATIVE WOMEN
Rh-Antigen
Rh-System स स ह Carl Landsteiner 1940 Rhesus Blood Group Antigen ह Antigens ह ह Eg. C, c, D, E, e य antigens
Chromosome 1 Short Arm Present ह ह
सभ Antigens स D Antigen स स य Immunogenic ह ह Rh (D) स Antigen Presence य Absence स Person ह Denote ह ह Rh Positive ह Rh Negative
Fetal Rh Antigen Fertilization 38 Appear ह ह
New Born Babies ABO (Major Blood Group Antigen A and B) Incompatibility
Haemolytic Disease Main Cause ह ह , स ह स ह Anaemia Mild
Anaemia ह ह
Anti A Anti B Antibodies IgM Type Immunoglobulin ह ह Placenta Cross
ह स
Rh-Negative Pregnancy :
Mother Rh Negative ह ह , Fetus Blood Group Rh Positive ह ह Delivery Time Placental Seperation ह ह स स य Maternal Blood Fetal Blood Contact ह सस Rh Antigen Mother Blood Enter ह Rh Isoimmunization ह ह
Condition Predisposing to Isoimmunization in Rh Negative Female/Fetomaternal/
Hemorrhage/Indication of giving Anti D
Abortion, Ectopic Pregnancy, Molar Pregnancy
Cordocentesis
Amniocentesis
Chorionic Villous Sampling
Attempted Version
Manual Removal of Placenta
Trauma
Antepartum Hemorrhage
Vaginal Delivery
Cesarean Section
Forceps Delivery
Placental Abruption
Blood Transfusion
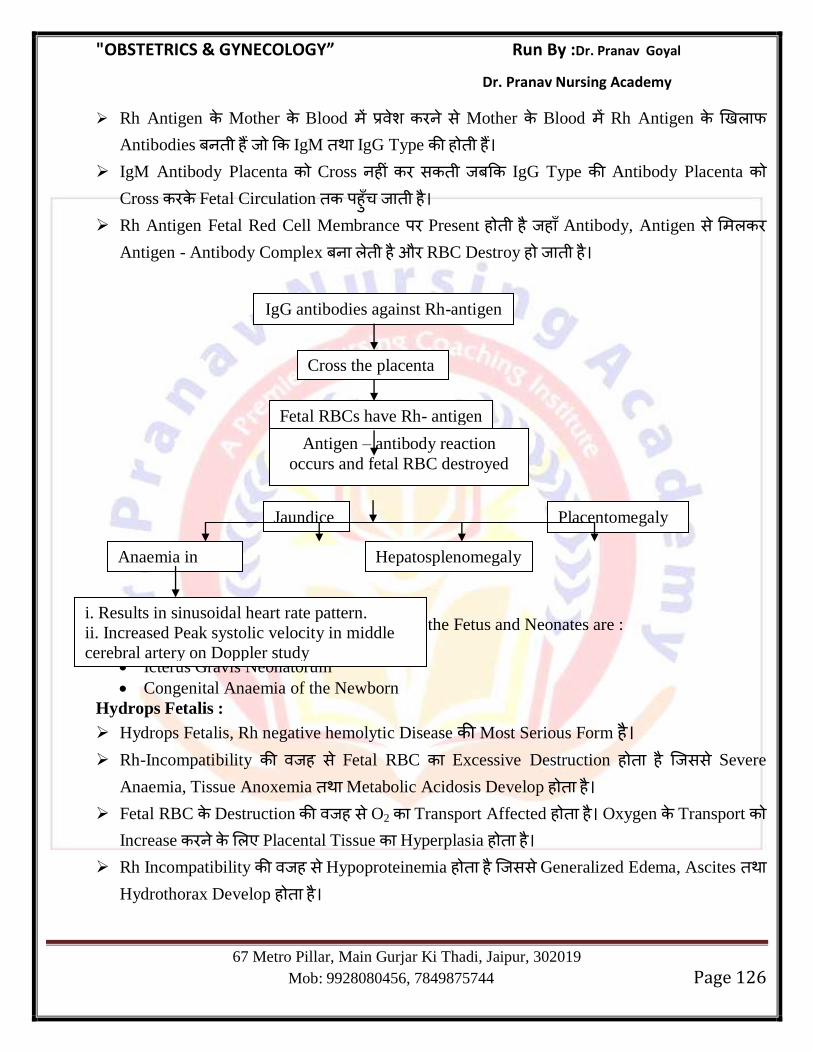
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 126
Rh Antigen Mother Blood स Mother Blood Rh Antigen
Antibodies ह IgM IgG Type ह ह
IgM Antibody Placenta Cross ह स IgG Type Antibody Placenta Cross Fetal Circulation ह ह
Rh Antigen Fetal Red Cell Membrance Present ह ह ह Antibody, Antigen स
Antigen - Antibody Complex ह औ RBC Destroy ह ह
Clinical Manifestation of Hemolytic Disease of the Fetus and Neonates are :
Hydrops Fetalis
Icterus Gravis Neonatorum
Congenital Anaemia of the Newborn
Hydrops Fetalis :
Hydrops Fetalis, Rh negative hemolytic Disease Most Serious Form ह
Rh-Incompatibility ह स Fetal RBC Excessive Destruction ह ह सस Severe
Anaemia, Tissue Anoxemia Metabolic Acidosis Develop ह ह
Fetal RBC Destruction ह स O2 Transport Affected ह ह Oxygen Transport Increase Placental Tissue Hyperplasia ह ह
Rh Incompatibility ह स Hypoproteinemia ह ह सस Generalized Edema, Ascites Hydrothorax Develop ह ह
IgG antibodies against Rh-antigen
Cross the placenta
Fetal RBCs have Rh- antigen
Antigen – antibody reaction
occurs and fetal RBC destroyed
Placentomegaly
Hepatosplenomegaly
Jaundice
e
Anaemia in
fetus
i. Results in sinusoidal heart rate pattern.
ii. Increased Peak systolic velocity in middle
cerebral artery on Doppler study
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 127
Hydrops Fetalis ह Situation ह स स Two Fetal Compartment Fluid
Accumulation Edema ह ह Hydrops Fetalis Situation Cardiac Failure ह स Fetal Death ह ह
Antenatal Investigation Protocol of Rh-Negative Mothers :
य Woman Rh Negative ह , Husband भ Rh-Grouping ह य Husband भ Rh-Negative ह ह Problem ह ह ह , य Husband Rh-Positive ह , Further
Investigation ह
Methods of know whether Antibodies have been formed or not.
Indirect Coombs Test : यह Test Maternal Blood स य ह
य Test Positive ह , स ह Mother Rh Antigen Antibodies ह ह
य Test Negative ह , स ह Mother भ Antibodies ह ह ह
Primigravida Case य 12th
Week ICT Negative ह 20 28 week Test Repeat
य ह
Multigravida Case 24 Weeks य ह Test Repeat य ह
Pregnant Rh Negative Mother Anti D Injection ह य य स भ
ह स य Fetal Blood स Rh Antigen Present ह , Mother Blood ह , Anti D Antibodies, Rh Antigen स Reaction Antigen -Antibody complex ह औ
स Antigen ह य Antigen ह ह ग Mother Immune System Antibodies
Produce ह ग
य Mother ह स ह Antibodies ग ह , Anti D य ह ह य
Indirect Coomb‘s Test Negative ह , ह Anti D Injection ह य Indirect Coombs
Test Positive ह , Anti D Injection ह ह
ICT Test Antibodies Concentration Dilution Method स Check स ह : Antibody Titre > 1 : 4 : Isoimmunization
Antibody Titre > 1 : 16 : Severe Hemolysis (Critical Titre)
Direct Coomb’s Test : यह Test Delivery Newborn Baby Blood Rh Antibody Titre Check य ह
Middle Crebral Artery Doppler : Antenatally Fetal Anaemia Detect Middle
Crebral Artery Doppler Test य ह यह Noninvasive Test ह
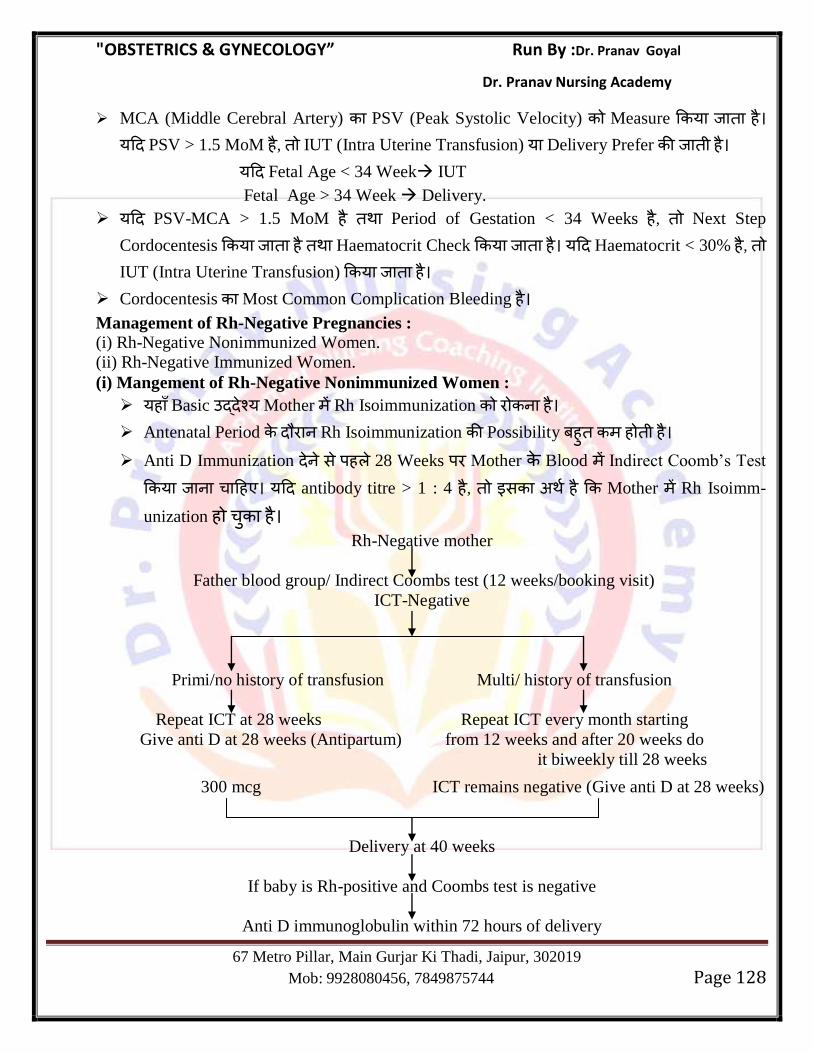
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 128
MCA (Middle Cerebral Artery) PSV (Peak Systolic Velocity) Measure य ह
य PSV > 1.5 MoM ह , IUT (Intra Uterine Transfusion) य Delivery Prefer ह
य Fetal Age < 34 Week IUT
Fetal Age > 34 Week Delivery.
य PSV-MCA > 1.5 MoM ह Period of Gestation < 34 Weeks ह , Next Step
Cordocentesis य ह Haematocrit Check य ह य Haematocrit < 30% ह , IUT (Intra Uterine Transfusion) य ह
Cordocentesis Most Common Complication Bleeding ह
Management of Rh-Negative Pregnancies :
(i) Rh-Negative Nonimmunized Women.
(ii) Rh-Negative Immunized Women.
(i) Mangement of Rh-Negative Nonimmunized Women :
यह Basic य Mother Rh Isoimmunization ह
Antenatal Period Rh Isoimmunization Possibility ह ह ह
Anti D Immunization स ह 28 Weeks Mother Blood Indirect Coomb‘s Test
य ह य antibody titre > 1 : 4 ह , स ह Mother Rh Isoimm-
unization ह ह
Rh-Negative mother
Father blood group/ Indirect Coombs test (12 weeks/booking visit)
ICT-Negative
Primi/no history of transfusion Multi/ history of transfusion
Repeat ICT at 28 weeks Repeat ICT every month starting
Give anti D at 28 weeks (Antipartum) from 12 weeks and after 20 weeks do
it biweekly till 28 weeks
300 mcg ICT remains negative (Give anti D at 28 weeks)
Delivery at 40 weeks
If baby is Rh-positive and Coombs test is negative
Anti D immunoglobulin within 72 hours of delivery
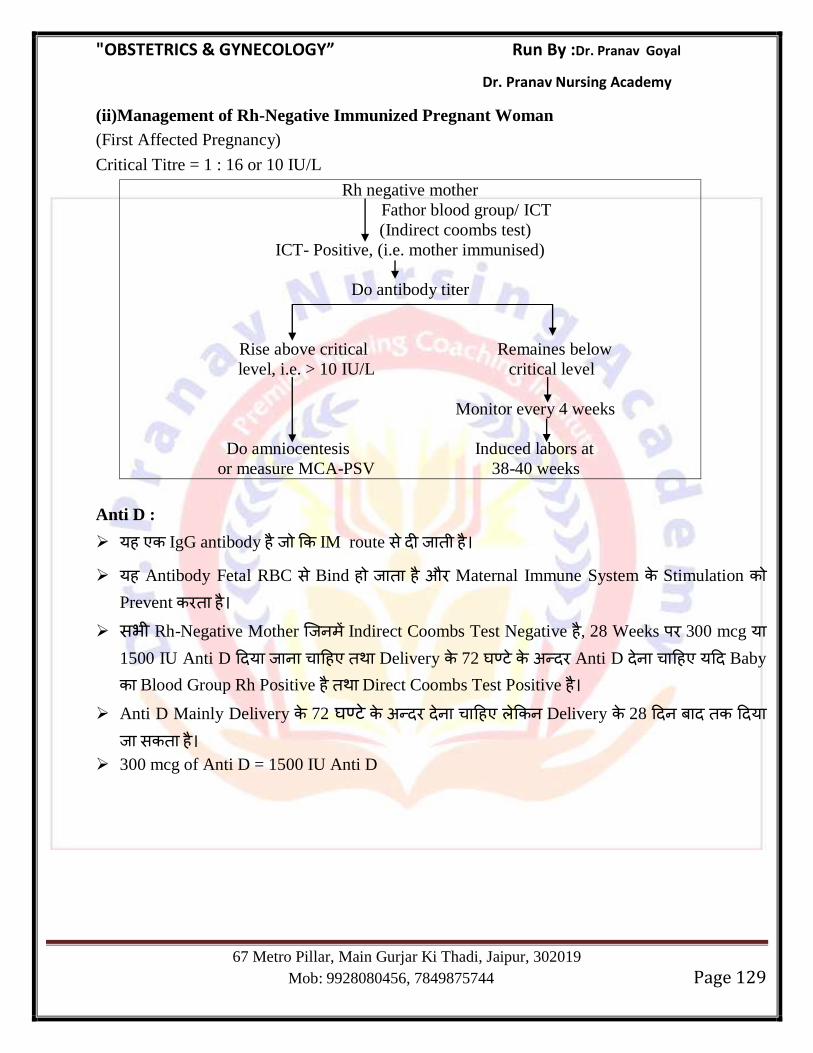
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 129
(ii)Management of Rh-Negative Immunized Pregnant Woman
(First Affected Pregnancy)
Critical Titre = 1 : 16 or 10 IU/L
Rh negative mother
Fathor blood group/ ICT
(Indirect coombs test)
ICT- Positive, (i.e. mother immunised)
Do antibody titer
Rise above critical Remaines below
level, i.e. > 10 IU/L critical level
Monitor every 4 weeks
Do amniocentesis Induced labors at
or measure MCA-PSV 38-40 weeks
Anti D :
यह IgG antibody ह IM route स ह
यह Antibody Fetal RBC स Bind ह ह औ Maternal Immune System Stimulation Prevent ह
सभ Rh-Negative Mother Indirect Coombs Test Negative ह , 28 Weeks 300 mcg य 1500 IU Anti D य ह Delivery 72 Anti D ह य Baby
Blood Group Rh Positive ह Direct Coombs Test Positive ह Anti D Mainly Delivery 72 ह Delivery 28 य
स ह
300 mcg of Anti D = 1500 IU Anti D
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 130
Chapter 15
MEDICAL COMPLICATIONS IN PREGNANCY
Heart disease in Pregnancy
Normal finding in CVS During Pregnancy
(i) Pulse Rate Increases.
(ii) Diastolic BP Decreases (Peripheral Vascular Resistance Decrease)
(iii) First Heart Sound is Prominent & split.
(iv) Second Heart Sound : Normal
(v) Third Heart Sound : Normally not heard but in Pregnancy it is prominent.
(vi) Slight Cardiomegaly on X-Ray.
(vii) ECG-Left Axis deviation.
Most Common Heart Disease :
Acquired Valvular disease : Mitral Stenosis
Congenital Heart Disease : Atrial Septal Defect
Cyanotic Congenital Heart Disease : Fallot‘s Tetralogy.
Heart Disease in which termination of Pregnancy is advised/pregnancy is contraindicated.
(i) Marfan Syndrome with Aorta involvement (> 45 mm)
(ii) Coarctation of Aorta
(iii) Eisenmenger Syndrome
(iv) Severe Mitral Stenosis/severe Symptomatic/ Aortic Stenosis.
(v) Any Heart Disease which belongs to NYHA Class 4 or Class 3
(vi) Ejection Fraction < 45%
(vii) Pulmonary arterial Hypertension due to any cause.
Predictors of cardiac event during pregnancy :
N : New York Heart Associatron (NYHA) Class > 2
O : Obstructive lesion of left heart (Mitral valve area < 2 cm2 or Aortic valve area < 1.5 cm
2,
Peak LV outflow tract gradient > 30 mm of Hg.
P : Prior Cardiac event before pregnancy eg. Heart Failure, Arrythmia, Transient Ischemic
attack, stroke.
E : Ejection Fraction < 40%
NYHA Classification (Revised 1979)
Class I : No limitation of Physical Activity.
Class II : Slight limitation of Physical Activity.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 131
Class III : Marked limitation of Physical Activity.
Class IV : Severely compromised -inability to perform any physical activity without discomfort.
Important Points :
Heart disease with maximum risk of maternal mortality : Eisenmenger‘s Syndrome.
Most Common time of Heart failure during pregnancy-
Immediate Postpartum > 2nd
stage of labor > late 1st stage of labor > 28-32 Weeks of pregnancy
> early 1st stage of labor.
Management of Heart Disease in Pregnancy : Antepartum Management time of
Hospitalization
Class I : 36 Weeks
Class II : 28 Week
Class III & IV : If seen in 1st trimester MTP should be advised ideally. if patient want to
continue pregnancy than the woman are hospitalized for the remainder of pregnancy.
India MTP Legally 20 Weeks य स ह Heart Disease Patient MTP 12
Weeks ह ह य 12 Weeks Delivery Abortion Same Risk
ह ह
MTP Suction & Evacuation ह
Heart Diseased Patient Pregnancy ह स Heart Work Load Patient
Activity Restricted ह
Sodium Water Retention Moderetely Sodium Dietry Restriction
ह
य sodium Restriction भ Intra vascular volume Increase ह ह , diuretics
(Furoseuide) Use ह
Intrapartum Management :
Patient Spontaneous Labor ह
य Labor Induction य ह , Vaginal PGE2 Use ह
Note : Induction is safe in case of Heart Desease.
Heart diseased Patient Trial of Labor Contraindicated ह ह
Patient Propped up Position ह
I/V Fluid Restrict ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 132
Vaginal Delivery Preferred ह य 2nd
Stage of Labor 30 Minute स य ह , Head
Delivery Outlet Forceps Vaccum Use ह (Vacuum is more better
than Forceps)
Labor pain Relief Epidural Analgesia Use ह
Heart Disease Patient LSCS Anaesthesia Epidural Anaesthesia
Post Partum Management :
Immediately Delivery Heart Failure Chances ह ह , : स Stage Pulmonary
Edema Prevent Placenta delivery I/V furosemide य ह
Heart Diseased Patient Delivery Bleeding Ergometrine Methylergo-
metrine Contraindicated ह ह Bleeding Oxytocin य स ह
Condition where Methylergometrine is Contraindicated-
Twin Pregnancy
Organic Cardiac Disease
Severe Preeclampsia & Eclampsia
Rh Negative Mother
Contraception in Heart Disease :
Heart Diseased Patient OCP Use ह ह य OCP Use ह स Thromboembolism स भ ह
Contraception may be used Temporary IUCD, Progesterone only Pills, Implants, Barrier
Contraceptives (condoms)
Contraception of Choice Permanent Sterlization.
य Female Heart Compensated ह ह , Male Vasectomy Advise ह
य Female Heart compensated ह , Tubal Sterlization Delivery गभग 1 Week
Under Local anaesthesia ह (Procedure preferred –Minilap technique by Abdominal
route)
Prognosis of Heart Disease in Pregnancy
General Concpet :
Highest mortality associated with Eisenmengar syndrome
Stenotic lesions have a higher mortality than regurgitant lesions
Aortic stenosis > Mitral > Pulmonary (in alphabetical order)
Congenital heart disease and mitral valve prolapse have least mortality
Most Common Fetal complication in Heart Disease : IUGR
Best Tocolytic in Heart Disease : Atosiban
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 133
Cardiovasculer drug safety profile in Pregnancy :
Safe Drug :
Adenosine
Lidocaine
Procainamide
Quinidine
Digoxin
Drug which should be used Judiciously :
Diuretics
Calcium antagonist
Unsafe Drugs :
ACE Inhibitor
Amiodarone.
Chapter 16
Hypertensive Disorders in Pregnancy
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 134
PIH (Pregnancy Induced Hypertension)
Definition : Hypertension in pregnancy is defined as systolic BP >140mm of Hg or diastolic BP
> 90mm of Hg on two occasions atleast 4 hours apart.
Pregnancy induced Hypertension chronic Hypertension in Pregnancy
य Normal Female Conceive BP
Increase ह
य Female Conceive स ह ह Hypertensive ह
No Past H/O Hypertension Past H/O Hypertension present.
Increase in BP is seen after 20 weeks of
Pregnancy.
Increase in BP seen before 20 weeks of
Pregnancy.
BP comes back to normal within 12 weeks of
delivery.
BP does not come back normal with in 12
weeks of delivery.
No Proteinurea
Types of PIH :
S. No. Pre Eclampsia S. No. Gestational Hypertension
1 Proteinurea & sign of end organ
damage are present.
1. Proteinurea & sign of end organ
damage are absent.
Proteinurea :
Excreation of Protein > 300 mg/24 hours urine.
Proteinurea of preeclampsia is non selective.
Sign of End organ damage :
Platelet count < 1 lacs.
Raised serum creatinine > 1.1 mg/dl
Elevated liver enzymes more than 2 times.
Evidence of pulmonary edema.
Onset of visual/cerebral symptoms.
Risk factor for preeclampsia :
Previous H/O Pre-eclampsia.
Primigravida
Obesity BMI > 35 kg/m2
Diabetes
Chronic Renal Failure
Extreme of Maternal age
Molar Pregnancy
Twin Pregnancy
Rh Negative Pregnancy
Antiphospholipid antibody syndrome
Pathophysiology of PIH
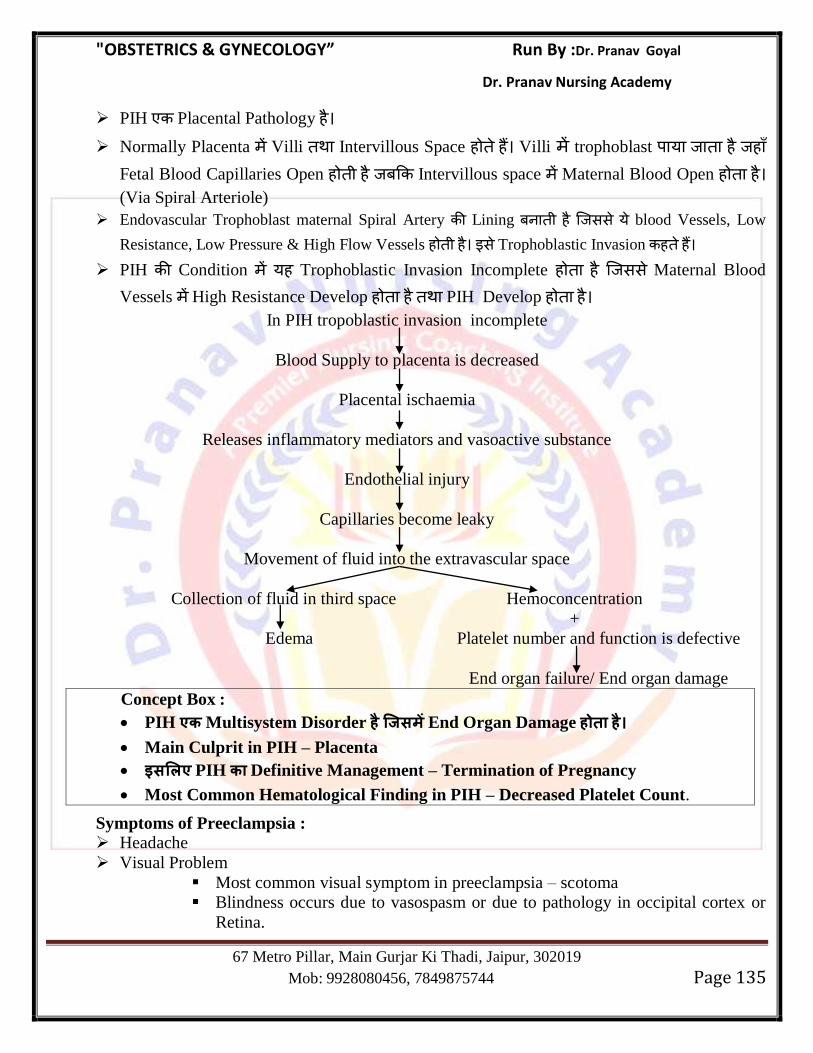
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 135
PIH Placental Pathology ह
Normally Placenta Villi Intervillous Space ह ह Villi trophoblast य ह ह Fetal Blood Capillaries Open ह ह Intervillous space Maternal Blood Open ह ह (Via Spiral Arteriole)
Endovascular Trophoblast maternal Spiral Artery Lining ह सस य blood Vessels, Low
Resistance, Low Pressure & High Flow Vessels ह ह स Trophoblastic Invasion ह ह
PIH Condition यह Trophoblastic Invasion Incomplete ह ह सस Maternal Blood
Vessels High Resistance Develop ह ह PIH Develop ह ह
In PIH tropoblastic invasion incomplete
Blood Supply to placenta is decreased
Placental ischaemia
Releases inflammatory mediators and vasoactive substance
Endothelial injury
Capillaries become leaky
Movement of fluid into the extravascular space
Collection of fluid in third space Hemoconcentration
+
Edema Platelet number and function is defective
End organ failure/ End organ damage
Concept Box :
PIH ए Multisystem Disorder End Organ Damage
Main Culprit in PIH – Placenta
लए PIH Definitive Management – Termination of Pregnancy
Most Common Hematological Finding in PIH – Decreased Platelet Count.
Symptoms of Preeclampsia :
Headache
Visual Problem
Most common visual symptom in preeclampsia – scotoma
Blindness occurs due to vasospasm or due to pathology in occipital cortex or
Retina.
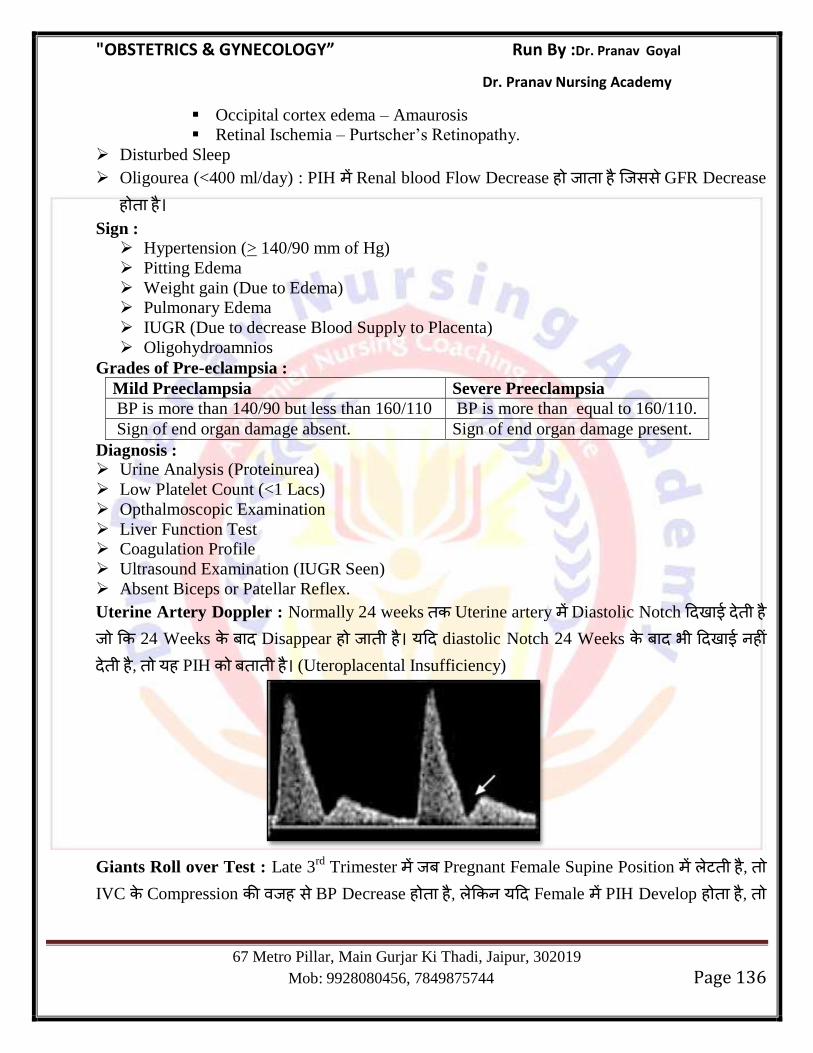
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 136
Occipital cortex edema – Amaurosis
Retinal Ischemia – Purtscher‘s Retinopathy.
Disturbed Sleep
Oligourea (<400 ml/day) : PIH Renal blood Flow Decrease ह ह सस GFR Decrease
ह ह
Sign :
Hypertension (> 140/90 mm of Hg)
Pitting Edema
Weight gain (Due to Edema)
Pulmonary Edema
IUGR (Due to decrease Blood Supply to Placenta)
Oligohydroamnios
Grades of Pre-eclampsia :
Mild Preeclampsia Severe Preeclampsia
BP is more than 140/90 but less than 160/110 BP is more than equal to 160/110.
Sign of end organ damage absent. Sign of end organ damage present.
Diagnosis : Urine Analysis (Proteinurea)
Low Platelet Count (<1 Lacs)
Opthalmoscopic Examination
Liver Function Test
Coagulation Profile
Ultrasound Examination (IUGR Seen)
Absent Biceps or Patellar Reflex.
Uterine Artery Doppler : Normally 24 weeks Uterine artery Diastolic Notch ह 24 Weeks Disappear ह ह य diastolic Notch 24 Weeks भ ह ह , यह PIH ह (Uteroplacental Insufficiency)
Giants Roll over Test : Late 3rd
Trimester Pregnant Female Supine Position ह , IVC Compression ह स BP Decrease ह ह , य Female PIH Develop ह ह ,
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 137
ह BP decrease ह य गभग 20 mm of Hg Increase ह ह यह Test 28-32 Week य ह
Management :
Drugs to Prevent Pre-eclampsia :
(i) Aspirin : (75 mg/day)--To be given after 1st trimester & continued throughout pregnancy
and stopped 7 days before delivery.
(ii) calcium Supplementation : स Female Calcium ह , Pre-eclampsia Prevent Calcium supplementation ह य Female ह स Calcium Normal ह , Pre Eclampsia Prevent Calcium Role ह ह ह
Measures proven to have no role in pregnancy Pre eclampsia :
Salt Restriction
Supplementation of Antioxidants
Supplementation of fish oil
Supplementation of Vit C, D, E
Progesterone
Low dose Heparin
Management Principles :
Pregnancy Induced Hypertension (Pre-eclampsia/Gestational Hypertension) Placental
Pathology ह स BP Increase ह ह , : स Condition ह Definitive Treatment
Termination of Pregnancy ह ह
Chronic Hypertension ह Antihypertensive Drug of Choice Methyldopa ह ,
Labetalol Use ह
Pregnancy Induced Hypertension (Preeclampsia/Gestational Hypertension) Drug of
Choice Labetalol > Alpha-Methyldopa
Antihypertensive of choice for hypertensive crisis – Labetalol > Hydralazine
Antihypertensive in Pregnancy
Safe Contraindicated
Labetalol ACE Inhibitor
Calcium Channel Blockers—Nifedipine Diuretics
Hydralazine Diazoxide
Alpha Methyl dopa Losartan
Nitroglycerine
Sodium Nitropruside
Preeclampsia Antihypertensive भ Use ह BP > 160/110 mm of Hg ह
Target BP in Preeclampsia is
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 138
Systolic : 130-140 mm of Hg
Diastolic : 80-90 mm of Hg
Target BP in chronic Hypertension is Systolic : 140-150 mm of Hg
Diastolic : 90-100 mm of Hg
Management of Mild Preeclampsia :
Role of Antihypertensive is +/–
Definitive Management – Termination of Pregnancy at 37 Weeks.
Mode of Delivery – Vaginal Delivery
Eclampsia : Severe Preeclampsia Condition Tonic Clonic Convulsion Coma ह , स Eclampsia ह ह यह Convulsion Coma Definitive (Metabolic,
Neurological) Cause ह ह Eclampsia Severe Pre eclampsia Advance Stage ह
Sign/Symptoms of Impending Eclampsia :
Epigastric Pain (Due to Stretching of Glisson Capsule of Liver), Nausea, Vomitting.
Headache, Dizziness (Due to Cerebral Hypoxia)
Visual Symptoms – Blurring/diplopia/scotoma/Blindness
Oligurea.
Severe Pre eclampsia Eclampsia Condition BP ह य Increase ह ह
Pressure ह य Increase ह ह स Brain Blood ह ह सस Cerebral
Hypoxia ह ह औ Convulsion Develop ह ह Important Points :
Most Common Type of Eclampsia : Antepartum Eclampsia
Eclampsia with worst prognosis : Antepartum Eclampsia
Most Common MRI Finding in Eclampsia : subcortical white matter edema
Most Common cause of death in Eclampsia & Preeclampsia : Intracranial Bleeding
There are four stage of convulsion in Eclampsia.
Pre-monitory TONIC CLONIC COMA
30 sec 15-20 sec 1 to 4 min Brief
Invasion stage Contraction stage Sizure stage Short period
Unconsciousness Respiration ceases Muscle contraction Sleepy
Muscle twisting Body spasm Tounge biting
Eye ball turn & fix Opisthotonus position Frothy secretion
Management of Eclampsia :
First line Management in eclampsia : Airway Management
Drug of choice to control convulsion : MgSO4
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 139
Antihypertensive should be given to control BP.
Drug of choice in Hypertensive crisis :- I/V Labetalol.
Definitive Management : Termination of Pregnancy Irrespective of Gestational age.
Mode of Delivery : Try vaginal delivery.
य Last convulsion 24 भ Spontaneous Labor Start ह ह ह , Cesarean ह
Indication for Cesarean in Eclampsia :
Prolonged Fetal Bradycardia
Unripe Cervix
Gestational Age < 32 Weeks
Poor Progress in Labor
IUGR
Uncontrolled BP
Prevention & Treatment of Convulsion with MgSO4 :
Eclampsia condition Convulsion Treat Drug of Choice : MgSO4
Mechanism of Action :
It Blocks NMDA Receptors in Brain.
It causes Cerebral Vasodilatation.
Block Calcium Channel and decrease intracranial edema.
Therapeutic range of MgSO4 : 4-7 mEq/L
Mg Therepeutic Range ह Short ह ह , : MgSO4 Maintenence Dose स य
Magnesium Toxicity Monitoring य ह
Urine output should be atleast : 30 ml/hr
Deep Tendon Reflex (Patellar Reflex) should be present.
Respiration Rate should be more than 14/min
Pulse Oximetry should be > 96%
Absolute Contraindication of MgSO4 :
Myasthenia Gravis
Deranged Renal Function.
Important Points :
1st sign of impending toxicity of MgSO4 : Disappearance of pateller Reflex.
Mg++ concentratron 10 mEq/L स य ह ह pateller reflex lost ह ह य Mg++ concentration
> 12 mEq/L : Respiratory Depression
> 15 mEq/L : Respiratory Arrest
> 30 mEq/L : Cardiac Arrest
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 140
Mg Toxicity Best Marker Pulse Oximetry ह ह य Mg Toxicity ह स respiratory
Depression Start ह स ह O2 Saturation ह ग ह
MgSO4 Calcium Channel Blocker स Cautiously य ह य य ह Drug
Neuro Muscular Blockage ह Antidote of MgSO4 Toxicity : 10 ml injection of 10% Calcium gluconate
Uses of MgSO4 : Prophylactic use in Severe Preeclampsia.
Prophylactic use in Severe HELLP syndrome.
Prophylactic use in Severe impending eclampsia.
Therepeutic use in Eclampsia.
Use as a short term tocolytic.
Neuroprotective Action :- It protect cerebral palsy in Neonate.
HELLP Syndrome :
Weinstein 1985 स स ह HELLP Syndrome य
यह Severe Pre-eclampsia Most Severe Hematological Complication ह
The acronym HELLP Stands for :
H = Evidence of Hemolysis
EL = Elevated Liver Enzyme
LP = Low Platelet Count.
Haemolysis Mainfested by :
1) LDH > 600 IU/L
2) Elevated Billirubin > 1.3 mg/dL
3) Low Serum Haptoglobin (Most Specefic Marker)
4) Abnormal peipheral Blood smear : Showing Schistocytes, Burr cell and helmet cells.
Elevated liver enzymes : AST and ALT > 70 IU/L
Low Platelet Count (< 1 Lac/mm3)
HELLP syndrome सभ Coagulation Parameter ( स PT, aPTT, Fibrinogen) Normal ह ह
Management :
If Pregnancy is > 34 Weeks = give prophylactically MgSO4 and Immediate deliver.
If Pregnancy is between 24 and 34 weeks give MgSO4 and corticosteroid (Betamethasone 12
mg I/M 2 dose 24 hrs. apart) & deliver.
Mode of Delivery :
If Cervix is Ripe, Gestational age > 32 weeks & FHR Reactive : Vaginal Delivery.
Otherwise Cesarean Section.
Chapter 17
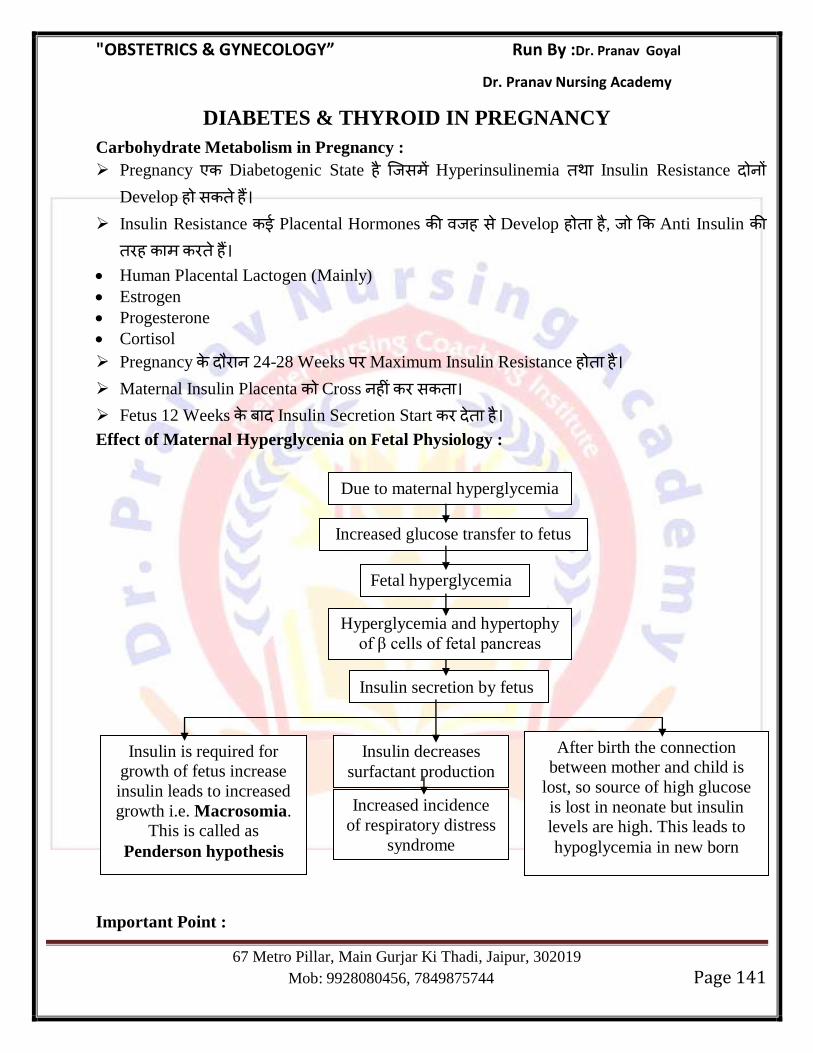
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 141
DIABETES & THYROID IN PREGNANCY
Carbohydrate Metabolism in Pregnancy :
Pregnancy Diabetogenic State ह स Hyperinsulinemia Insulin Resistance Develop ह स ह
Insulin Resistance Placental Hormones ह स Develop ह ह , Anti Insulin ह ह
Human Placental Lactogen (Mainly)
Estrogen
Progesterone
Cortisol
Pregnancy 24-28 Weeks Maximum Insulin Resistance ह ह
Maternal Insulin Placenta Cross ह स
Fetus 12 Weeks Insulin Secretion Start ह
Effect of Maternal Hyperglycenia on Fetal Physiology :
Important Point :
Due to maternal hyperglycemia
Insulin decreases
surfactant production
Increased glucose transfer to fetus
Fetal hyperglycemia
Hyperglycemia and hypertophy
of β cells of fetal pancreas
Insulin secretion by fetus
After birth the connection
between mother and child is
lost, so source of high glucose
is lost in neonate but insulin
levels are high. This leads to
hypoglycemia in new born
Increased incidence
of respiratory distress
syndrome
Insulin is required for
growth of fetus increase
insulin leads to increased
growth i.e. Macrosomia.
This is called as
Penderson hypothesis
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 142
Maternal Hyperglycemia ह स Placenta Hydropic Degeneration ह ह सस Placenta - स Non Functional ह ह Fetus Size Increase ह ह स O2
Demand ह Supply Decrease ह ह (due to Hydropic Degeneration
of Placenta) स ह स Hypoxia Develop ह ह सस Sudden Fetus Death ह स ह
स ह स Diabetic Mother Fetus Hypertrophic Cardiomyopathy Develop ह स ह
Diabetes in Pregnancy :
Gestational Diabetes :
स Female ह Normal , स Pregnancy Insulin Resistance Develop ह ह स Diabetes ह ह स Gestational Diabetes ह ह
Pregnancy Insulin Resistance Maximum 24-28 Weeks Develop ह ह
(Mainly due to human placental Lactogen Hormone)
Diabetic patient High Blood Sugar Level ह ह स Free Redicals ग ह ह स Fetus Congenital Malformation Develop ह ग ह , Gestational Diabetes 24 Weeks Free Radicals ह स स य Fetus Organogenesis ह ह ह , : Gestational Diabetes Congenital Malformation ह ह ह
Overt Diabetes : Overt Diabetes ह स Female स ह स ह Type-I य Type-II
diabetes ह औ ह Pregnant ह ह
Pregnancy Overt Diabetes Female Oral Hypoglycemic Drugs Insulin
य ह य Oral Hypoglycemic Drugs Placenta Cross स ह
Overt Diabetes Condition ह स ह Sugar Level य ह ह , : Pregnancy Day-1 स ह Free Redicals ह ह स Fetus Congenital Malformation ह ह
Diagnostic Criteria for Diabetes during Pregnancy :
1) Random Plasma Glucose > 200 mg/dL
2) Fasting blood Glucose > 126 mg/dL
3) HbA1c > 6.5%
4) Two or More Abnormal Values on 100 gram oral Glucose tolerance test during pregnancy
5) Classical Symptoms of Diabetes
Gestational Diabetes Congenital Malformation ह ह ह Overt Diabetes congenital Malformation ह ह
Congenital malformation in Infant of Diabetic Mother
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 143
Overt Diabetic Female Fetus Congenital Malformation Risk Predict स स Best Parameter : Estimation of HbA1c Level
HbA1c Level < 6.5% --No Increased Risk
6.5-8.5% -- 5% Risk
> 10% -- 22 % Risk
Diabetic Female Fetus Antenatally congenital Malformation Detect Best
Test = Level II /TIFFA Scan at 18-20 Weeks
Most Common System involved in Congenital malformation = CVS > CNS
Most Common Congenital Anomally = Ventricular Septal defect (VSD > Neural Tube
Defect)
Most Specefic Anomally = Caudal Regression Syndrome (Sacral Agenesis) यह
Anomally ह Rare ह ह
Most Common Cardiac Anomally in Infant of Diabetic Mother = VSD
Most Common CVS Finding in Infant of Diabetic Mother = HOCM (Hypertrophic
Cardiomyopathy)
Most Specific Cardiac Anomally : Transposition of Great Aorta (TGA)
Meausures to Decrease the risk of congenital Malformation in Overt diabetic Females :
Periconceptional Period Early Pregnancy स य Strict Blood Sugar Control Insulin ह
स ह Diabetic Female Pregnancy Diagnose ह ह , Oral Hypoglycemic Agent
Rapid/Intermediate Acting Insulin Start ह
Prepregnancy HbA1c Level < 6.0% ह ह
Folic Acid Supplementation Dose = 4 mg स Therepeutic Dose of Folic Acid भ ह ह यह
Conception स ह Start ह conception ह Continue ह
Protocol for Diagnosis of Congenital Malformation :
HbA1c level estimation before 14 Weeks of Pregnancy
TVS in 1st Trimester to detect Anencephaly (11-14 Weeks)
β-hCG & PAPP-A to Detect Down Syndrome
Targated Anomally Scan at 18-20 Weeks
Fetal Echocardiography done between 22-24 Weeks.
Diagnosis of Gestational Diabetes :
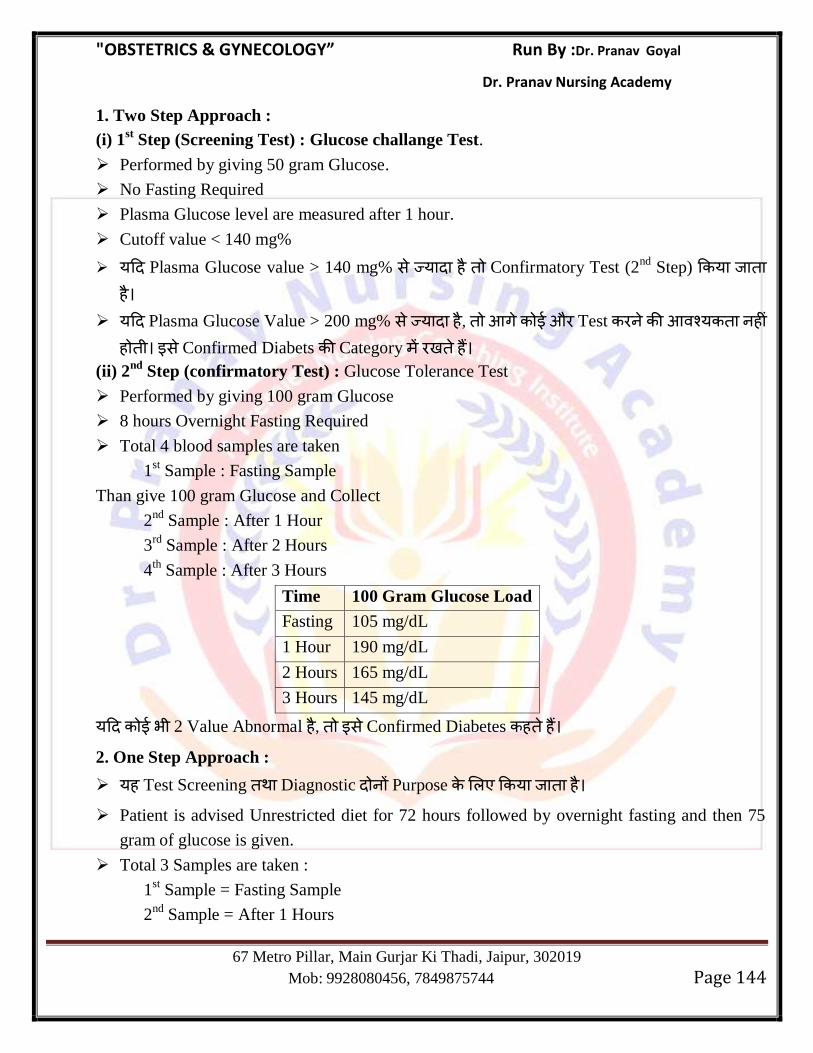
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 144
1. Two Step Approach :
(i) 1st Step (Screening Test) : Glucose challange Test.
Performed by giving 50 gram Glucose.
No Fasting Required
Plasma Glucose level are measured after 1 hour.
Cutoff value < 140 mg%
य Plasma Glucose value > 140 mg% स य ह Confirmatory Test (2nd
Step) य ह
य Plasma Glucose Value > 200 mg% स य ह , ग औ Test य ह ह स Confirmed Diabets Category ह
(ii) 2nd
Step (confirmatory Test) : Glucose Tolerance Test
Performed by giving 100 gram Glucose
8 hours Overnight Fasting Required
Total 4 blood samples are taken
1st Sample : Fasting Sample
Than give 100 gram Glucose and Collect
2nd
Sample : After 1 Hour
3rd
Sample : After 2 Hours
4th
Sample : After 3 Hours
Time 100 Gram Glucose Load
Fasting 105 mg/dL
1 Hour 190 mg/dL
2 Hours 165 mg/dL
3 Hours 145 mg/dL
य भ 2 Value Abnormal ह , स Confirmed Diabetes ह ह 2. One Step Approach :
यह Test Screening Diagnostic Purpose य ह
Patient is advised Unrestricted diet for 72 hours followed by overnight fasting and then 75
gram of glucose is given.
Total 3 Samples are taken :
1st Sample = Fasting Sample
2nd
Sample = After 1 Hours
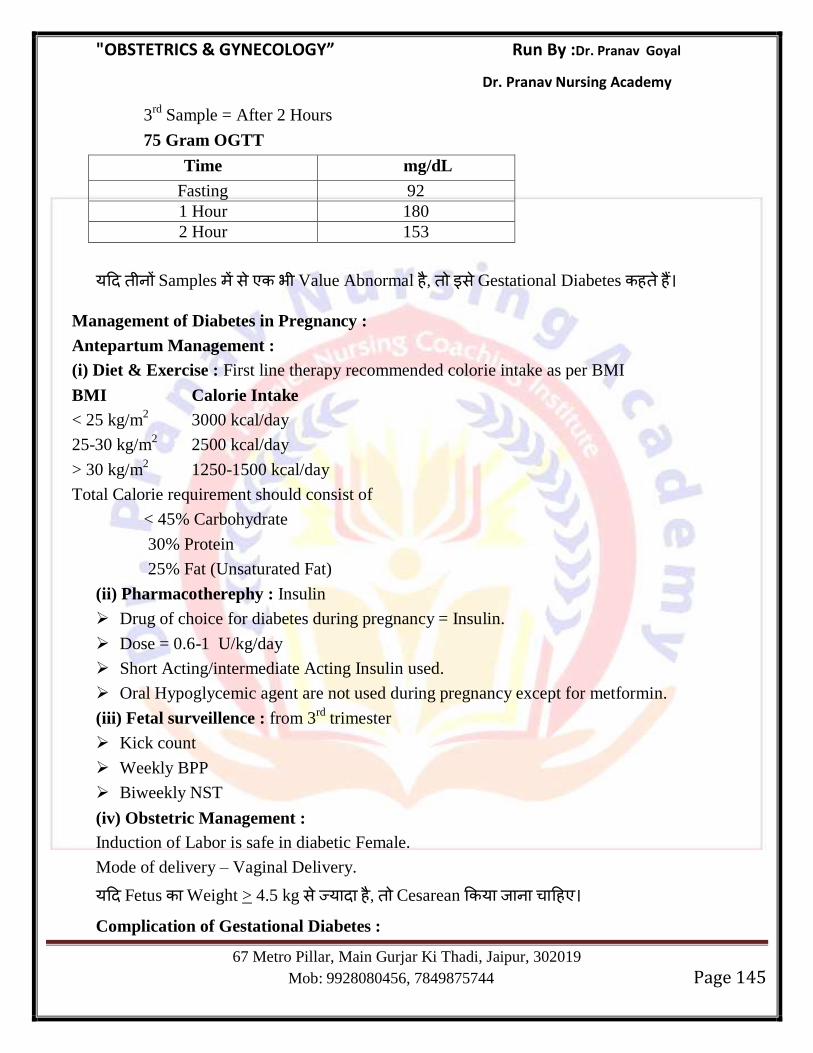
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 145
3rd
Sample = After 2 Hours
75 Gram OGTT
Time mg/dL
Fasting 92
1 Hour 180
2 Hour 153
य Samples स भ Value Abnormal ह , स Gestational Diabetes ह ह
Management of Diabetes in Pregnancy :
Antepartum Management :
(i) Diet & Exercise : First line therapy recommended colorie intake as per BMI
BMI Calorie Intake
< 25 kg/m2 3000 kcal/day
25-30 kg/m2 2500 kcal/day
> 30 kg/m2 1250-1500 kcal/day
Total Calorie requirement should consist of
< 45% Carbohydrate
30% Protein
25% Fat (Unsaturated Fat)
(ii) Pharmacotherephy : Insulin
Drug of choice for diabetes during pregnancy = Insulin.
Dose = 0.6-1 U/kg/day
Short Acting/intermediate Acting Insulin used.
Oral Hypoglycemic agent are not used during pregnancy except for metformin.
(iii) Fetal surveillence : from 3rd
trimester
Kick count
Weekly BPP
Biweekly NST
(iv) Obstetric Management :
Induction of Labor is safe in diabetic Female.
Mode of delivery – Vaginal Delivery.
य Fetus Weight > 4.5 kg स य ह , Cesarean य ह
Complication of Gestational Diabetes :
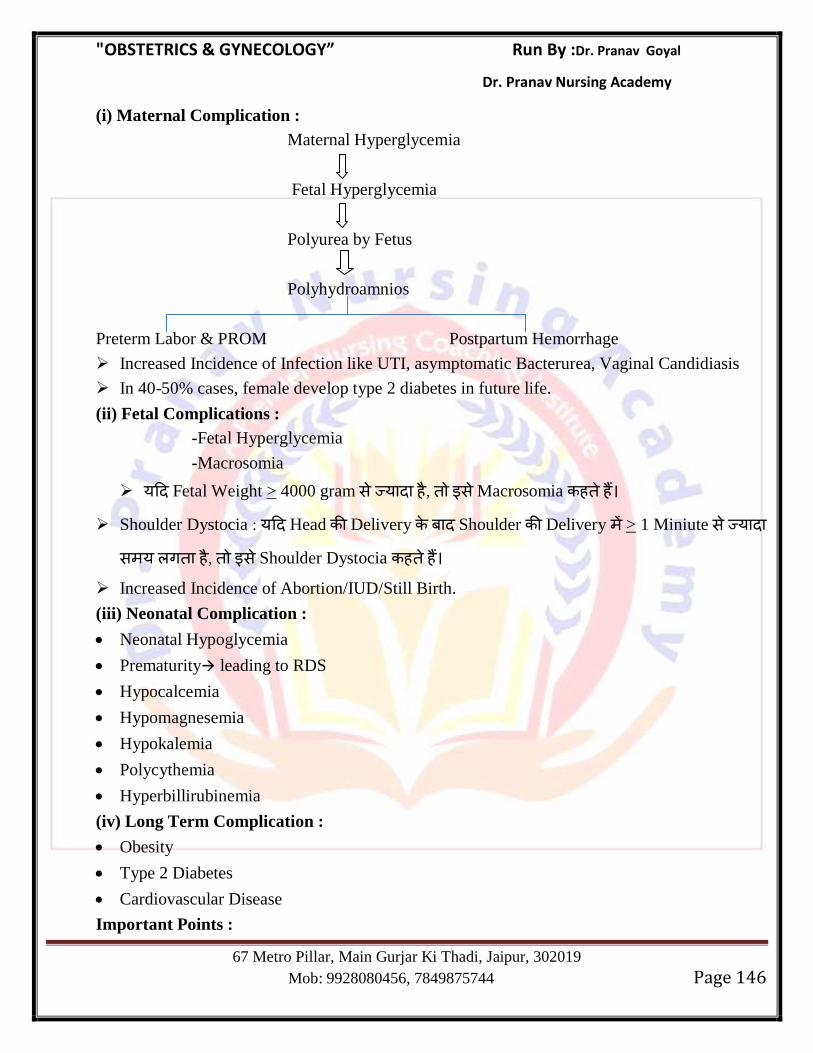
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 146
(i) Maternal Complication :
Maternal Hyperglycemia
Fetal Hyperglycemia
Polyurea by Fetus
Polyhydroamnios
Preterm Labor & PROM Postpartum Hemorrhage
Increased Incidence of Infection like UTI, asymptomatic Bacterurea, Vaginal Candidiasis
In 40-50% cases, female develop type 2 diabetes in future life.
(ii) Fetal Complications :
-Fetal Hyperglycemia
-Macrosomia
य Fetal Weight > 4000 gram स य ह , स Macrosomia ह ह
Shoulder Dystocia : य Head Delivery Shoulder Delivery > 1 Miniute स य
स य ग ह , स Shoulder Dystocia ह ह Increased Incidence of Abortion/IUD/Still Birth.
(iii) Neonatal Complication :
Neonatal Hypoglycemia
Prematurity leading to RDS
Hypocalcemia
Hypomagnesemia
Hypokalemia
Polycythemia
Hyperbillirubinemia
(iv) Long Term Complication :
Obesity
Type 2 Diabetes
Cardiovascular Disease
Important Points :
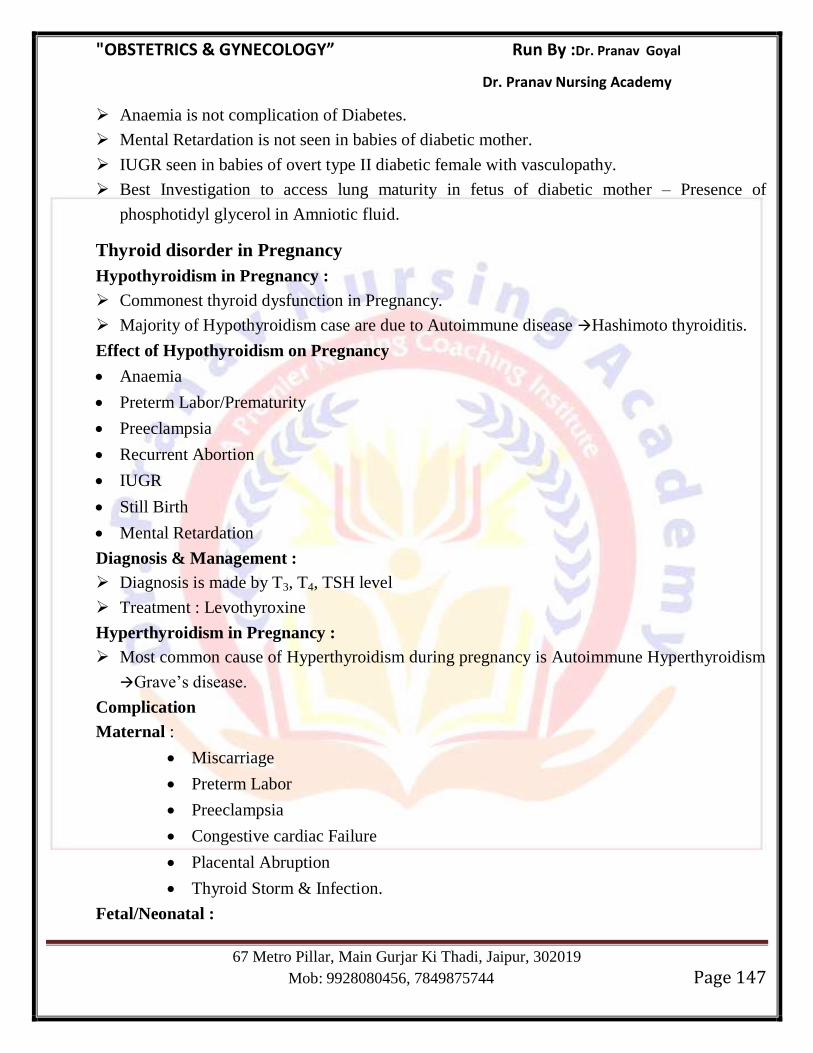
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 147
Anaemia is not complication of Diabetes.
Mental Retardation is not seen in babies of diabetic mother.
IUGR seen in babies of overt type II diabetic female with vasculopathy.
Best Investigation to access lung maturity in fetus of diabetic mother – Presence of
phosphotidyl glycerol in Amniotic fluid.
Thyroid disorder in Pregnancy
Hypothyroidism in Pregnancy :
Commonest thyroid dysfunction in Pregnancy.
Majority of Hypothyroidism case are due to Autoimmune disease Hashimoto thyroiditis.
Effect of Hypothyroidism on Pregnancy
Anaemia
Preterm Labor/Prematurity
Preeclampsia
Recurrent Abortion
IUGR
Still Birth
Mental Retardation
Diagnosis & Management :
Diagnosis is made by T3, T4, TSH level
Treatment : Levothyroxine
Hyperthyroidism in Pregnancy :
Most common cause of Hyperthyroidism during pregnancy is Autoimmune Hyperthyroidism
Grave‘s disease.
Complication
Maternal :
Miscarriage
Preterm Labor
Preeclampsia
Congestive cardiac Failure
Placental Abruption
Thyroid Storm & Infection.
Fetal/Neonatal :
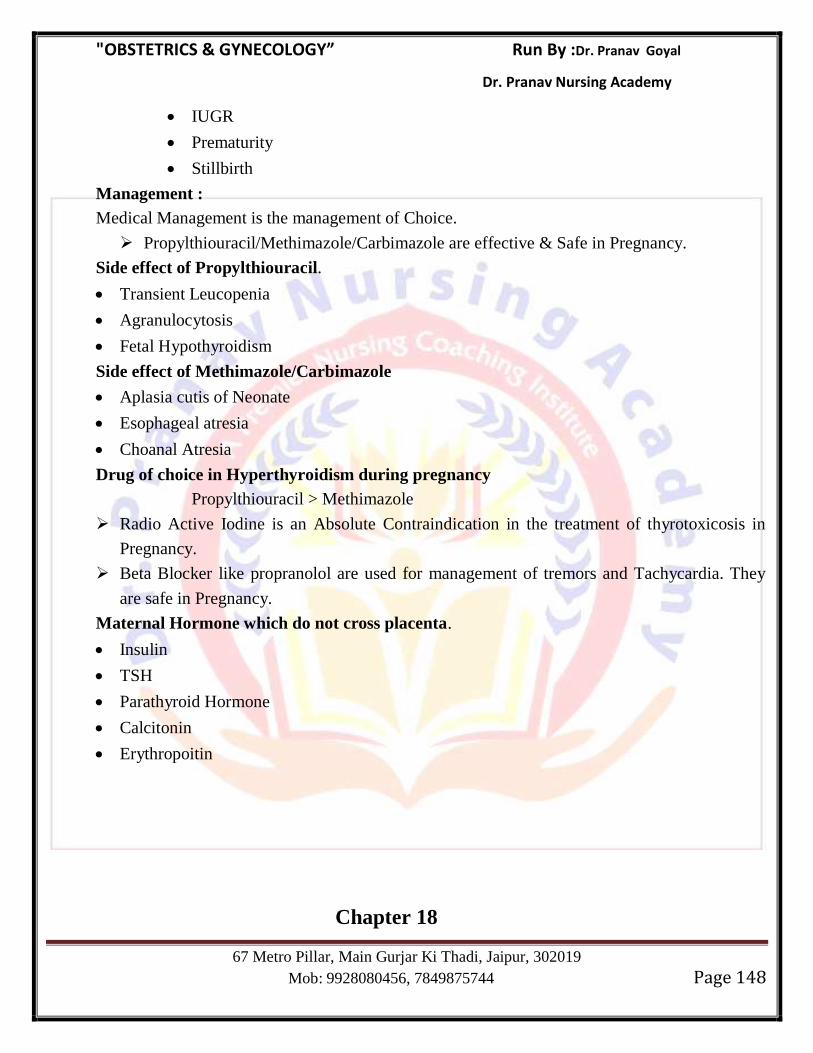
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 148
IUGR
Prematurity
Stillbirth
Management :
Medical Management is the management of Choice.
Propylthiouracil/Methimazole/Carbimazole are effective & Safe in Pregnancy.
Side effect of Propylthiouracil.
Transient Leucopenia
Agranulocytosis
Fetal Hypothyroidism
Side effect of Methimazole/Carbimazole
Aplasia cutis of Neonate
Esophageal atresia
Choanal Atresia
Drug of choice in Hyperthyroidism during pregnancy
Propylthiouracil > Methimazole
Radio Active Iodine is an Absolute Contraindication in the treatment of thyrotoxicosis in
Pregnancy.
Beta Blocker like propranolol are used for management of tremors and Tachycardia. They
are safe in Pregnancy.
Maternal Hormone which do not cross placenta.
Insulin
TSH
Parathyroid Hormone
Calcitonin
Erythropoitin
Chapter 18
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 149
ANAEMIA IN PREGNANCY
Anaemia in Pregnancy : WHO स Pregnancy Hb Concentration 11 gm % स
ह Hematocrit Value 33% स ह , स Anaemia ह ह Severity of Anaemia :
Mild : 10-10.9 gm%
Moderate : 7-10 gm%
Severe : Less than 7 gm%
Very Severe : Less than 4 gm%
Physiological Anaemia during Pregnancy : Pregnancy Red Cell Mass (10-15%) Plasma Volume (30-40%) य Increase ह ह सस Hemodilution ह ह औ Hb
concentration Decrease ह ह स Physiological Anaemia of Pregnancy ह ह
Cause of Anaemia during Pregnancy :
Acquired Hereditary
Iron Deficiency anaemia
Dimorphic anaemia- Anaemia due to iron and folic acid
deficiency
Anaemia caused by acute blood loss
Anaemia of inflammation or malignancy
Megaloblastic anaemia
Acquired hemolytic anaemia
Aplastic or hypoplastic anaemia
Thalassemias
Sickle-cell hemoglobinopathies
Other hemoglobinopathies
Hereditary hemolytic anaemia
Complication of Anaemia :
Maternal :
Preeclampsia
Infection
Heart Failure
PPH
Shock
Subinvolution
Pulmonary embolism during Puerperium
Fetal :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 150
Low Birth Weight
Intra Uterine Death
Iron deficiency Anaemia :
यह Pregnancy Most Common Anaemia ह
Pregnancy Total Iron Requirement गभग 1000mg ह ह 4-6 mg Iron
Daily Required ह ह
Pregnancy Iron Deficiency Anaemia Serum Iron, Serum ferritin ह ह TIBC Serum Transferrin Increase ह ह
Iron स भ Form य ह Only 10% ह Absorb ह ह , : 4-6 mg/daily
requirement 40-60 mg Daily Iron य ह Diet स भ ह ह स Pegnancy गभग ह ह Iron Supplementation
य ह
Ministry of Health & Family National Anaemia Control Programme ह सभ Pregnant Females Iron Folic Acid Tablet ह
100 mg elemental Iron + 500 mcg Folic Acid Tablets 100 Days ह
Earliest Indicator of Iron deficiency Anaemia decrease serum ferritin.
Normal S. Ferritin 50-300 μg/L
S. Ferritin < 30 μg/L Iron deficiency Anaemia
Most Sensitive Blood Index of Iron deficiency MCHC
Diagnosis of Iron deficiency Anaemia :
(i) PBF : Microcytic Hypochromic anaemia, Reticulocyte count slightly raised.
(ii) Decrease MCV, MCH, MCHC, Seme Ferritin
(iii) TIBC & Serum Transferrin increased.
(iv) Most Accurate method of measuring Hb : Cyanomethemoglobin method.
Management of Iron deficiency Anaemia :
(i) Prophylactic Therapy :
Avoid Frequent child Birth.
Supplementory Iron Tablets.
Early detection of Anaemia
(ii) Curative Therapy (Oral Iron Therapy)
180-200 mg elemental Iron orally + 1 mg Folic Acid
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 151
Oral Iron Therapy Parameter स स ह ह Reticulocyte Count (With in 7-
10 Days)
Parenteral Iron Therapy :
स Patient Hemo/Peritoneal Dialysis, Malabsorption Syndrome य Pregnant Female
with severe Anaemia ह , स Parenteral Iron य ह
Parenteral Oral Iron Therapy स गभग 0.7-1.0 gram% per week Haemoglobin
Concentration Increase ह ह Parenteral Iron स स Iron Increase ह ह ह
Types of Parenteral Iron :
Iron Dextran
Iron Sucrose
Iron Sorbitol
Iron Carboxymaltose
Dose of parenteral Iron :
Total iron requirement is calculated by the following formulae
a. 4.4 x body weight (kg) x Hb deficit (g/dL) – This formula includes iron needed for
replenishment of stores
b. 0.3 x weight (lb) x (Hb deficit) = iron req in mg. add 500 mg for stores
c. 250 mg of elemental iron for each gm% of Hb deficit
d. 2.21 x body weight (kg) x Hb deficit (g/dL) + 1000 mg (replenishment of stores)
Note : Weight in kg = wt in lb x 2.2
Normal Hb is taken as 14 g/dl
(iii) Blood Transfusion :
1 unit Blood 0.8-1 gram% Hb level ह (Within 24 Hours)
Delivery Time Hb Level स 7 Gram% ह ह
Dimorphic Anaemia :
स Anaemia Iron Folic Acid य Vit B12 स ह ह
PBF Shows : Macrocytic or Normocytic
Hypochromic or Normochromic
Treatment : Iron & Folic Acid (Therapeutic Dose)
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 152
Sickle Cell Anaemia :
Pregnancy Haemolytic Anaemia Most Common Cause Intravascular Microangi-
opathic Hemolysis ह HELLP Syndrome Part ह
Sickle Cell Disease Pregnancy ह Most Common Hemoglobinopathy ह
Sickle Cell Anaemia Hereditory Disorder ह स Chromosome 11 β-Globin chain Point Mutation ह ह
β -chain Point Mutation ह स 6th Position Glutamic Acid Valine amino
acid ह ह
Gene Mutation Homozygous Condition ह ह , Sickle Cell Anaemia disease ह ह
(HB-SS) (Small Quantity of HbF but No HbA)
य यह Heterozygons State ह ह , स Sickle Cell Trait (HbAS) ह ह स Person 55-60% HbA ह ह 35-40% HbS ह ह
Normal RBC Life Span 90-120 Days ह ह Sickle Cell Life Span only 5-10
Days ह ह
Sickle Cell Crisis :
Characterized by intense bone pain due to sequestration of sickled erythrocyte & Infarction
in various organ.
Management :
IV Fluid
O2
Epidural Analgesia
Antibiotic
Thromboprophylaxis
Red Cell Transfusion
Complication during Pregnancy :
Preterm Labor
IUGR
Fetal Death
Abortion
Increased Incidence of
(i) Preeclampsia
(ii) PPH
(iii) Infection
Management during Pregnancy :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 153
Folic Acid supplementation 4-5 mg daily (Folic Acid increase blood cell Turnover)
Prophylactic Penicillin (Penicillin V 250 mg BD Daily)
Prophylactic Blood Transfusion during pregnancy to maintain Hematocrit above 25% and
HbS below 60%
Hydroxyurea not recommended in Pregnancy.
य Antenatal visit Hb, hematocrit, Platelet Count, Billirubin, Transaminase Lactate dehydrogenase (LDH) Level Check ह (Fortnightly)
Vaginal Delivery is Preferred
Epidural Analgesia is given during labor to Relieve pain.
Postnatal thromboprophylaxis upto 6 weeks.
Contraception :
Low Dose Oral Progestins or DMPA or Progesterone implant are Ideal Contraceptive
choice in sickle cell female.
Thalassemia :
Thalassemia Group of Inherited blood Disorder ह स Severe Microcytic Hypochromic
Anaemia ह स ह यह स ह स ह
α- Thalassemia
β- Thalassemia
Thalassemia Hemoglobin α β Chain Structurally Normal ह ह , स Production ह ह
Thalassemia : Autosomal Recessive Trait
Alpha Thalassemia :
यह Disease Southeast Asia, Africa,Carribbean Mediterranean Region ह ह
यह Disease Chromosome 16p Deletion ह स ह ह
यह α-Chain Absent ह ह excess β chain ह सस β -Globin Tetramer ह
स HbH ह ह
स Disease Fetus भ Affected ह ह य Fetal Hb (HbF) भ α -Chain
Required ह ह
β -Thalassemia :
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 154
यह Disease Mainly Mediterranean, Asia ,Middle East, Caribbean Region ह ह
यह Disease Chromosome 11 Point Mutation ह स ह ह सस β –Globin Chain Synthesis य ह ह ह
स Condition α -Chain य ह ह Red Cell Membrance स bind ह ह औ स Damage ह
Haematological Finding in Thalassemia :
Low MCV, Low MCH but normal MCHC
Serm Iron & TIBC : Normal or Elevated
Hemoglobin electrophoresis Shows
Increase HbA2 (α2 + δ2) > 3.5%
Increase or normal HbF (α2 + γ2)
Serm Billirubin Raised 2-3 mg%
NESTROFT Test : Naked eye single tube Red cell osmotic Fragility test. यह Thalassemia Screening Test ह ह
Chapter 19
INFECTION IN PREGNANCY
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 155
Fetal Cell Mediated Humoral Immunity Intrauterine Life 9-15 Weeks of Gestation
Start ह ह
स भ Infection Against स स ह Immunoglobulin IgM Type ह ह
Passive Immunity Mother स Fetus Placenta Transfer ह ह , IgG Type Immunoglobulin ह ह
Vertical Transmission : Infectious agent Placenta, Labor, Delivery Breast Feeding
Mother स Fetus Transmission ह Vertical Transmission ह ह
Chickenpox (Vericella Zoster)
Chickenpox vericella zoster virus ह
Route of Transmission : Respiratory Route
यह Infection Placenta Mother स Fetus Transmit ह स ह
Incubation Period = 11 Days
Most Common cause of Maternal Mortality in chickenpoxPneumonia
Drug of choice for vericella in pregnant woman Acyclovir
Acyclovir 20 Weeks स ह (Due to Organogenesis) Avoid ह
य Pregnancy 20 Week स य ह , Rash Start ह 24 Hours Acyclovir Start
ह
Pregnant Female य स Chickenpox Patient contact ह Exposure 96
Hours Varicella Immunoglobulins Prophylaxis ह यह contact स भ य स ह
Varicella Zoster Vaccine Pregnancy Contraindicated ह ह य यह Live Attenuated
Vaccine ह ह
Varicella Zoster Vaccine Breast Feeding Contraindicated ह ह ह
य Varicella Infection Pregnancy 1st Trimester ह ह (Time of Organogenesis)
Fetus congenital Varicella Syndrome ह स ह
Congenital Varicella Syndrome
Chorioretinitis
Micro-opthalmia
Cerebral Cortical Atrophy
IUGR
Hydronephrosis
Skin/Bone Defect
य Congenital Varicella Syndrome Antenatally Diagnose ह ह , MTP ह
Neonatal Varicella : Pneumonitis
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 156
Hepatitis
DIC
Influenza :
Influenza Virus RNA Virus ह
Hemagglutinin (H) Neuraminidase (N) Antigen Surface ह Influenza Virus Strain Genus, Species H N Subtype ह
ह
Effects on Pregnancy due to H1-N1 infection (Swine Flu)
Miscarriage
Preterm Labor
PROM
Pneumonia
ARDS
Renal Failure
DIC
Pregnancy Influenza Infection स Teratogenic Effect ह ह ह Infection 1st
Trimester (Time of Organogenesis) ह ह ह
Influenza (Inactivated) Vaccine Pregnancy Breast Feeding Safe ह ह Diagnosis – Immunoassay, RT-PCR
Management – Supportive Care
Measles :
o Measles Virus Paramyxovirus Family Belong ह यह RNA Virus ह
o Measles infection Teratogenic ह ह ह
o Measles Infection High Fever ह स Miscarriage, IUGR, Microcephaly,
Oligohydramnios, Still Birth Premature Delivery ह स ह
o Incubation Period = 10 Days from Exposure to onset of Fever
14 days to appearance of Rashes (Avg. 7-21 days)
o Diagnosis – assay of IgM – Detection of Viral RNA (RT-PCR)
o Management – Supportive Care
o Ribavirin may be given for viral pneumonia
o Measles vaccine live attenuated vaccine ह ह स यह Pregnancy Containdicated ह ह
Rubella (German Measles)
Rubella Vaccine RNA Virus ह Togavirus Family Belong ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 157
Incubation Period 2-3 Weeks (18 Days Avg.)
Route of Transmission – Droplet Infection
यह Infection Pregnancy Fetus Most Severe Congenital Malformation Produce
ह
Mother Rubella Infection ह स Rash, Malaise, Fever, Lymphadenopathy Polyarthritis ह ह
य Mother Rubella Infection 2nd
Trimester ह ह Fetus Transmission Possibility Negligible ह ह
Congenital Rubella Syndrome : (i) Mental Retardation (Most Common)
(ii) Sensorineural Deafness
(iii) Cataract /Glaucoma
(iv) Congenital Heart Disease – PDA, PS
(v) CNS Defect-Microcephaly, MR
(vi) Thrombocytopenia
(vii) Hepatosplenomegaly
य Infection Late 2nd
Trimester 3rd Trimester ह ह , Fetal Malformation ह ह ह ,
Mental Retardation Hearing Loss ह स ह
Maternal Diagnosis :
Maternal IgM and IgG should be done within 7-10 days of exposure and repeated after 3
week.
IgM & IgG Negative – No Infection
IgM – Negative, IgG – Rise [Infection may Occur but reduced Risk]
IgM – Positive in any sample – Acute Infection Do MTP
Fetal Diagnosis : PCR by CVS, Amniocentesis, Cordocentesis
Management : य Pregnant Female Ist Trinmester य Early 2nd
Trimester Infection ह ह , MTP ह
Prevention : Vaccine – MMR Vaccine/Rubella Vaccine
MMR Vaccine live attenuated Vaccine ह ह स स Pregnancy ह ह Cytomegalo Virus (CMV)
यह Herpesvirales Family Virus ह यह ds DNA Virus ह
Maternal Infection usually Asymptomatic ह ह
Patient Mononucleosis स Symptons ह ह :Like : Malaise, Fever, Generalized
Lymphadenopathy, Hepatosplenomegaly
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 158
Menifestation of Congenital CMV Infection :
Still Birth
Mental Retardation
Microcephaly
IUGR
Chorioretinitis
Hepatosplenomegaly
Deafness
Haemolytic Anaemia
Intracranial calcification seen in periventricular zone while in toxoplasma, calcification is
scattered throughout brain.
CMV ह स Fetus भ भ Heart Defect ह ह ह , Most Commonly Brain Defect ह ह
Childhood Age CMV, Sensorineural Hearing Loss Most Common Cause ह
Diagnosis : CMV – IgM antibody
CMV – PCR of Amniotic Fluid
Management :
Symptomatic Treatment
Passive Immunization
No Vaccine Available till Date
Herpes Infection :
Maternal HSV : U/L or B/L vesicular lesion along the dermatome.
Management : Acyclovir 200 mg 5 times a day for 5 days.
Mode of Delivery : Cesarean Section
Toxoplasmosis :
यह Toxoplasma Gondii ह Obligate Intracellular Parasite ह
Cat is Definitive Host
Mother Infection undercooked Meat स ह
Toxoplasma Infection Maximum 3rd
Trimester ह ह
य Toxoplasma Infection 1st Trimester ह ह , य Severe Infection ह ह
Symptoms – Posterior Cervical Lymphadenopathy, Fever, Fatigue, Rash
Drug of choice for toxoplasma during pregnancy – spiramycin (1 g every 8 hourly)
Triad of congenital Toxoplasma
Intracranial calcification
Hydrocephalus
Chorioretinitis
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 159
य Non Pregnant Woman Toxoplasma diagnosed ह ह , 6 Months Pregnancy
Avoid ह
HIV in Pregnancy :
Pregnancy Least Teratogenic Infection - HIV
Most Common Time Period of Vertical Transmission
Peripartum Period
During Delivery
Risk depends on following factors.
Maternal Viral Loads
CD4+ Cell count
Vit A deficiency
Chorioamnionitis
Screening Test – ELISA
Confirmatory Test : Western Blot Test
CD4 + Cell Count < 200 cells/mm3 स ह , Pneumocystic Jiroveci य
Opportunistic Infection Prevent Prophylaxis ह
Anti Retroviral Therapy is highly effective in Reducing Viral Load & Perinatal
Transmission.
HAART (Highly Active Anti Retro Viral Therapy) : यह Perinatal Transmission Best Regimen ह ह , यह Expensive Treatment ह ह
य Female HIV Positive ह , Tripple Drug Therapy as soon as Start ह औ
Throughout Pregnancy, Labor & Post Partum Period Contiune ह
Care during Labor :
य Female HIV Positive ह , 38 Weeks Elective Cesarean ह Elective Cesarean Delivery Vertical Transmission Reduce ह
HIV Positive Females ARM (Artificial Rupture of Membrane) ह ह
Post Exposure Prophylaxis :
Zidovudine 200 mg TDS
Lamivudine 150 mg BD x (4 Weeks)
Nelfinavir 750 mg TDS
य Mother HIV Positive ह , Breast Feeding Avoid ह Navirapine Therapy : Mother स Fetus HIV Vertical Transmission Prevent
Navirapive ह यह Cost Effective ह ह 200 mg orally 4 hours before cesarean section
& Single dose to baby (2 mg/kg) with in 72 hours of birth.
Key Concept
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 160
Most common infection CMV
Most teratogenic infection Rubella
In rubella –Most common single defect which occurs is –Sensorineural hearing loss.
Heart defects seen in rubella Patent ductus arteriosus and pulmonary artery stenosis.
After rubella vaccine, pregnancy is contraindicated for 1 month.
CMV –Transmission can occur in any trimester
CMV never leads to heart defects in fetus
Most common time for toxoplasma infection—3rd
Trimester
Triad of toxoplasma infection –Intracerebral calcification, chorioretinitis and hydrocephalus.
Treatment—Spiramycin (Prevents fetal transmission but it cannot treat fetal infection if it is
present).
Spiramycin + Pyrimethamine and sulfonamide combination is given to treat fetal infection
and prevent further transmission.
Infection DOC in pregnancy
Bacterial vaginosis Metronidazole to patient only 1st trimester-clindamycin
Pneumocystis carinii Sulphamethozole –trimethoprim
Typhoid Third gen. cephalosporins/ azithromycin
Syphilis < 1 year > 1
year
Benzathine penicillin 2.4 million U IM single dose Benzathine penicillin
2.4 million U IM weekly x 3 doses
Gonorrhoea Inj. Ceftriaxone 125 mg IM single dose or Tab cefixime 400 mg single
dose or inj. Spectinomycin 2 g i.m. single dose
Chlamydia Azithromycin single dose or Amoxicillin 500 mg TDS * 7 days, 2nd
choice- Erythromycin
Group B streptococci Pencillin, 2nd
best –Ampicillin. In patients who are pencillin-resistant-
Cefazolin
Malaria-Prophylaxis Chloroquine
Malaria -Treatment Chloroquine. For radical cure primaquine is advised after delivery. In
resistant cases (Mostly d/t P. falciparum) – Quinine + Clindamycin or
mefloquine
Appendicits Immediate appendicectomy
Red degeneration Conservative management (no termination of pregnancy and no
myomectomy)
Viral Hepatitis in Pregnancy :
Tropical Countries Pregnancy Jaundice Most Common Cause Viral hepatitis ह
Hepatitis A (HAV) : Picorna Virus (RNA Virus)
Hepatitis A Feco oral Route स ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 161
Diagnosis Anti HAV IgM antibody
Perinatal Transmission is Rare.
Chronic carrier stage not exist.
Pregnant women HAV Infection ह ह Immunoglobulin 0.02 ml/kg exposure 2
Weeks ह
Hepatitis B (HBV) :
यह DNA Virus ह ह
Route of Transmission : Parenteral
Sexual Contact
Vertical Transmission
Hepatitis B Transmission Risk 1st Trimester 10% 3rd
Trimester 90%
ह ह
HBV is not Teratogenic
Clinicial Feature : Malaise, Anorexia, Nausea, Vomitting, Cirrhosis, HCC
Chronic Carrier stage present
Diagnosis :
Serological detection of HBSAg, HBCAg (Denote high Infectivity) Antibody to hepatitis
B core Antigen (HBcAg) & Viral load HBV DNA titre.
Management:
HBsAg Positive mother स fetus Hepatitis Transmission Active
Passive ह Immunization ह
Hepatitis Immunoglobulin (0.5 ml IM) within 12 hours after birth
+
1st Dose of Hepatitis B recombinant vaccine followed by Hepatitis B vaccine at 1 & 6
Month.
Hepatitis B is not a contraindication for breast feeding.
Hepatitis C (HCV) : RNA Virus
Major cause of Non-A, Non-B Hepatitis worldwide & leading cause of Transfusion
associated Hepatitis.
Route of Transmission Blood Borne.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 162
Perinatal Transmission is high if coinfected with HIV & HBV
Chronic Carrier stage Present.
Breast Feeding is not Contraindicated.
Hepatitis D (HDV) : RNA Virus
यह Infection ह Hepatitis B infection स ह
Hepatitis E (HEV) : RNA Virus
Most important cause of Non A, Non-B Hepatitis in developing country like India.
Chronic Carrier stage present.
Maternal Mortality is very High.
Important Points :
Maximum Risk of Maternal Mortality : Hepatitis E
Maimum Risk of Hepatic Encephalopathy :Hepatitis E
Maximum Risk of Perinatal transmission: Hepatitis B
Maximum Risk of Transmission of Hepatitis: at the time of delivery.
Breast Feeding is not contraindicated in case of Hepatitis.
Tuberculosis in pregnancy :
Caused by : Mycobactrium Tuberculosis.
Effect of Pregnancy on TB : TB Relapse Maximum Puerperium Period ह स ह TB
Flare up भ Puerperium Period ह स ह
Effect of TB on pregnancy :
Decrease Fertility
Abortion
IUD
Preterm Delivery
IUGR
Low Birth Weight
Mode of Infection in Fetus :
Hematogenous : Through umbilical vein
Ingestion of infected Amniotic Fluid during delivery
Post partum Infection
TB is not an Indication for termination of Pregnancy.
ATT Pregnancy स भ Trimester स ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 163
First Line Drug for TB
Isoniazid
Rifampicin
Pyrazinamide
Ethambutol
Pregnancy Streptomycin contraindicated ह ह यह Drug Fetus Oto-toxicity
Develop ह
Breast Feeding is not contraindicated if the woman is on treatment but contraindicated if
active lesion is present.
Delivery Baby ह INH (Isoniazid) Prophylaxis ह य ह
Montoux Test Negative ह Prophylaxis ह BCG Vaccination ह
Antitubercular Drugs contraindicated in Pregnancy :
K = Kanamycin
F = Fluro-quinolones
C = Capreomycin
A = Amikacin
S = Streptomycin
Mnenonic = KFC always surprising
TB is not a Indication for Termination of Pregnancy.
Epilepsy in Pregnancy :
Pregnancy Most Common Neurological Disorder Epilepsy ह
Pregnancy Epilepsy Most Common Cause Idiopathic ह
Pregnancy सभ Anticonvulsant Drug Congenital Anomally ह (Due to
defective folic Acid Metabolism)
Malformation due to Anticonvulsant drugs :
Cleft Lip/Palate
Mental Retardation
Limb Defect
Hypoplasia of Terminal Phalanges
Sodium valproate is associated with neual tube defect.
Chances of Neonatal Hemorrhage Increased due to Anticonvulsant induced vitamin K
dependent coagulopathy.
Antepartum Management :
Mono drug therapy preferred.
Lowest possible dose should be given.
Therapeutic dose Monitoring
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 164
सभ Females Anticonvulsant Drug ह , ह Conception स ह ह 4 mg/day
Folic Acid Start ह Pregnancy ह
Prenatal Screening :
MSAFP (Maternal Serum Alpha Fetoprotein) at 16 weeks + Level IInd USG
Vitamin K 10 mg/day orally from 36 weeks onward to prevent Hemorrhagic disease of
New born.
Post partum management : Newborn is given Vitamin K (1mg IM)
Breast Feeding is not contraindicated.
Drugs in pregnancy :
Food and drug administration (FDA) charted out categories for drugs, taking into account the possible
fetal adverse effects.
Category A Drugs which have no fetal risks as demonstrated by well-controlled studies in
humans, e.g. pencillin.
Category B Drugs which have shown no risk in animal studies but human studies do not
exist, or also if any adverse effects have been seen in animal studies with no
such effect in well-controlled human trails, e.g., paracetamol, ranitidine
Category C Drugs for which there are no studies either animal or human, or drugs in which
there are adverse fetal effects in animal studies but no such data exists in
human trials, e.g. chloroquine, acyclovir, zidovudine.
Category D Drugs which have proven risks but their use in essential and the benefits
outweigh the risks, e.g. phenytoin, warfarin, propylthiouracil.
Category X Drugs which are clearly teratogenic and the risks outweigh the benefits and
hence should be avoided.
CNS anomaly (NTD) + CVS anomaly + facial defects are seen with the use of isotretinoin
Drug Teratogenicity
Alcohol Fetal alcohol syndrome (dose related) Pre and postnatal growth restriction
Facial abnormalities like shortened palpebral fissure, low set ears, smooth philtrum,
thinned upper lip and midfacial hypoplasia.
CNS defects like microcephaly, mental retardation and behavioral disorders
Warfarin Fetal warfarin syndrome
Chondrodysplasia punctata, epiphyseal stippling, nasal hypoplasia, optic atrophy
and microcephaly
Phenytoin Fetal hydantoin syndrome Hypertelorism, broad nasal bridge, low set ears, hypoplastic nails and digits.
Sodium
valproate
Fetal valporate syndrome Brachycephaly with a high forehead, hypertelorism, small nose and mouth, shallow
orbits, overlapping long fingers and toes and hyperconvex nails.
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 165
Diethyl
stilbesterol
Neural tube defects
Vaginal and cervical adenosis, clear cell adenocarcinoma, uterine anomalies,
cryptorchidism and testicular hypoplasia
Isotretinoin Cleft palate, neural tube defect, microcephaly, deafness, blindness, cardiac defects
like atrial septal defect and great vessel defects.(CNS +CVS + facial defect)
ACE
inhibitors
Renal tubular dysgenesis, anuria and oligohydramnios
Androgens
and danazol
Masculinisation of a female fetus
Antineoplastic
agents
IUGR, craniosynostosis, micrognathia, severe limb abnormalities
Tetracyclines Discoloration of deciduous teeth
Cocaine Microcephaly, limb reduction defects and genitourinary malformations due to
cerebral infraction
Chapter 20
PUERPERIUM & ITS ABNORMALITIES Puerperium Delivery 6 Weeks Time Period ह ह स Pelvic Organs Anatomically
Physiologically Pre-Pregnant State ह
Involution ह Process ह स Genital Organs स Pre-Pregnant Stage ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 166
Duration : Normal Puerperium expulsion of Placenta स Start ह 6 Weeks (42 days ) ह ह स य भ ग गय ह : 1. Immediate Puerperium : 1
st 24 Hours after delivery.
2. Early Puerperium : 1st
7 days after delivery.
3. Remote Puerperium : 2nd
Week to 6th
Week after delivery.
Physiological Changes :
Uterine Changes :
Involution of the Uterus :
Delivery Just Contracted Uterus Fundal Height Pubic symphysis स 13 cm ह ह , Umbilicus Just Feel ह ह
48 Uterus 1.25-1.5 cm per day हस स Shrink ह Start ह ह औ गभग स ह Uterus Intrapelvic Organ ह ह
Delivery गभग स ह Uterus Pre-Pregnant Stage ह
Uterus Weight
At the time of Delivery : 1000 Gram
After One Week : 500 Gram
After Three Week : 100 Gram
After Six Week : 60 Gram
Pregnancy Uterus स ह , स स य Uterine Muscles Hypertrophy Hyperplasia ह ह , Uterus Pre-Pregnant Stage ह , स स य No. of Cells Decrease ह ह ह , Only Cells Size Decrease ह ह
Delivery Puerperium period estrogen Progesterone hormone Withdrawl स Uterus Collagenase Proteolytic Enzyme Release ह ह सस Uterine Cell Size
Decrease ह ह
Uterus Delayed Involution Subinvolution ह ह
Cervix :
Labor Cervix 10 cm Dilate ह ह स Prepregnant Stage ह
Delivery Cervix 5 cm स Close ह ह 1 Week Complete
Close ह ह (Pre Pregnant Stage)
Delivery Internal os ह स Close ह ह , External os स भ ह ह
Endometrium :
Delivery Decidua Superficial Part Necrotic ह Lochia Shred ह ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 167
Endometrium Basal Layer Myometrium ह ह ह Intact ह ह औ स Regeneration Start ह ह
Endometrium Regeneration ह Fast Process ह ह Delivery स ह Endometrium Complete Regeneration ह ह
Placental Site Regeneration slowest ह ह (Approx-6 Weeks)
Vaginal Changes :
Vagina स Prepregnant Stage य स य ग ह यह Slow Process ह
Size & Elasticity never revert back.
Delivery Puerperium period 1st 15 days Vagina स fluid Discharge ह ह स
Lochia ह ह Lochia Uterine Body, Cervix Vagina स Originate ह ह स Fishy Smell ह ह
Initially Lochia Alkaline ह ह - Acidic ह ह
Lochia Colour स ग- ग य गय ह : (i) Lochia Rubra [1-4 Days] :(Red Colour). It consist Blood, shred of fetal membrane, decidua,
vernix caseosa, Lanugo and Meconium.
(ii) Lochia Serosa [5-9 Days] : (Yellow colour) serosa meansserum (yellowish discharge). It
consist of leucocyte, wound exudate ,Mucus from cervix and Micro- Organism.
(iii) Lochia Alba [10-15 Days] : (Pale White). It consist decidual cells, leucocytes, Mucus,
Fatty & granular epithelial cells & Micro -Organism.
5-6 Average Dischange गभग 250 ml ह ह
Post partum Period Average Blood Loss गभग 200 ml ह ह
Total 15 Complete Fluid Loss गभग 400 ml ह ह
Clinical Importance :
Discharge Premature Labor Infection Condition Scanty ह स ह Twin
Delivery, Polyhydroamnios, Subinvolution RPOC Condition Excessive ह स ह
य Discharge स Fishy Smell गह ग ग ह , यह Infection Show ह
य Lochia Red Color Normal time period भ Continue ह ह यह Subinvolution
य RPOC ह स ह स ह
Breast Changes :
Postpartum Period Breast Milk Secretion ह ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 168
(i) Mamogenesis : Growth of Alveolar Tissue.
(ii) Lactogenesis : Synthesis and Secretion of Milk from Alveoli.
(iii) Galactokinesis :Ejection of Milk from Breast.
Milk Ejection Oxytocin Hormone Responsible ह ह , Posterior Pitutory स Release
ह ह
(iv) Galactopoiesis : Maintenence of Lactation. यह Prolactin Dependent ह ह
Milk Synthesis Mainly Prolactin Hormone Responsible ह Anterior Pitutory स Release ह ह
Prolactin Level Increase ह ह , यह Hypothalamus Suppress ह सस Gonadotropin Releasing Hormone Release ह ह सस Pitutory स Gonadotropin FSH LH Release ह ह Ovulution ह ह स Lactational Amenorrhoea ह ह
Urinary Tract : Delivery Urinary Bladder Trauma ह स Nerve Plexus Injury ह स ह सस Intravesicle Pressure Increase ह भ Micturation Feeling ह ह ह औ Urinary Bladder overdistended ह ह Bladder Incomplete empty ह ह सस Puerperium Period UTI ह स भ य ह ह
Gestrointestinal Tract : Puerperium Period Intestinal Paresis ह स Constipation ह ह
Loss of Weight : Delivery of Fetus, Placenta, Amniotic Fluid Blood Loss ह स Puerperium Period Immediately 5 kg Weight Loss ह ह
6 Weeks Extra 4 kg Weight भ Loss ह ह (Due to excreation of Fluid & electrolytes)
Fluid Loss : Delivery First Week 2 Litre Fluid Loss ह ह ग 5 Weeks गभग 1.5 Litre Fluid Loss ह ह
Haematocrit Changes : Early puerperium period Platetlet Coagulation Factor Increase
ह ह स Hypercoagulable State ह ह सस Puerperium Period Thromboembolism ह स भ ह
Temperature :
Delivery Slight Reactionary Temperature (0.5°F) Increase ह ह गभग 12
Hours Normal ह ह
Temperature First 24 Hours 37.2° C स य ह ह ह
Delivery Breast Engorgement ह स 3rd Day slight Temperature Increase ह ह
24 Normal ह ह
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 169
Important Points :
Rule of 3 : Delivery Nonlactating Female 3 Weeks Lactating Female 3 Month Contraceptives Use ह
Abnormal Puerperium :
Puerperal sepsis : Delivery First 10 Days य Oral Temperature. 38°C स य ह , स Hyperpyrexia ह ह
Sepsis : Delivery स 42 Genital Tract Infection ह स य Pelvic Pain, >
38.5°C Temp, Subinvolution य Vaginal Discharge ह ह
Mode of Infection : Direct Spread (Endogenous/Exogeous)
Micro Organism : Streptococcus
Clinical Manifestation : Endometritis
Risk Factor :
(i) Patient Related : Unhygiene, Anaemia, Malnutrition.
(ii) Delivery Related : Frequent examination, Prolonged/Obstructed Labor, Instrument
Delivery.
(iii) Health Care Person Related : Untrained Staff, Use of unsterlized Instruments.
Prevention :
Antenatal : Hb > 11%, treat local infection.
Intranatal : Aseptic Method, Perineal Hygiene
Post Natal : Clean Pad, early detection & treatment of infection.
Chapter 21
Practice Questions
1. How many primary spermatocytes formed by one spermatogonia ?
(A). 4 (B). 16 (C). 64 (D). 8
2. Time taken in spermiogenesis is ?
(A). 14 days (B). 74 days (C). 61 days (D). 46 days
3. Capacitation occurs in ?
(A). Vas deferns (B). Seminal vesicle (C). Ejaculatory ducts (D). Female genital tract
4. SRY gene present at ?
(A). Short arm of ―Y‖ chromosome (B). Long arm of ―Y‖ chromosome
(C). Short arm of ―X‖ chromosome (D). Long arm of ―X‖ chromosome
5. Which of the following statement is wrong ?
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 170
(A). time taken in sperm capacitation is 7 hrs (B). Life span of sperms 48-72 hrs
(C). Main hormone responsible for spermatogenesis is testesterone(D). Testesterone is secreted by sertoli cell
6. At birth all oogonia present at which stage of development ?
(A). Primary oocyte (B). Secondary oocyte (C). Polar body (D). Ovum
7. The process of ovulation is known as ?
(A). Release of secondary oocyte from primary oocyte (B). Release of ovum from secondary oocyte
(C). Release of primary oocyte from oogonia (D). Release of 2nd
polar body from secondary oocyte
8. Which of the following statements is false ?
(A). Maximum no of oogonia during intra uterine life present at 5th
month of intrauterine life
(B). At birth secondary oocyte division arrested at diplotene stage of meiosis-I
(C). Size of mature ovum is 120-130 micron, which is largest cell of the body
(D). Life span of ovum is 12-24 hrs
9. Morula is 16 cell stage structure, sorrounded by a layer which prevent polyspermy known as ?
(A). Zona pellucida (B). Corona radiata (C). Amnion (D). Chorion
10. Zygote enters the uterine cavity after how many days of fertilization ?
(A). 3 days (B). 4 days (C). 5 days (D). 6 days
11. Which structure of the blastocyst developed into embryo proper ?
(A). Trophoblast (B). Inner cell mass (C). External cell mass (D). Zona pellucida
12. True statement is ?
(A). Fertilization occurs in isthmus part of fallopian tube (B). Implantation occurs 6-7 days after fertilization
(C). Zona hatching occurs 8th
day after fertilization (D). hCG hormone secreted mainly by cytotrophoblast
13. 1st meiotic division of oogenesis gets arrested at ?
(A). Pachytene stage of prophase (B). Diplotene stage of prophase
(C). Leptotene stage of prophase (D). Metaphase stage of prophase
14. Fertilisation is said to be complete if ?
(A). 1st polar body formed (B). 2
nd polar body formed
(C). Primary oocyte is formed (D). Secondary oocyte is formed
15. Match the following ?
Color of amniotic fluid Disease
P. Greenish yellow (Saffron) W.Rh incompatibility
Q. Golden yellow X. Postmaturity
R. Green Y. IUD
S. Tobacco juice Z. Fetal distress
(A). P (X) Q (W) R (Y) S (Z) (B). P (X) Q (Y) R (Z) S (W)
(C). P (X) Q (Y) R (W) S (Z) (D). P (X) Q (W) R (Z) S (Y)
16. Uteroplacental blood flow at term is ?
(A). 400-600 ml/min (B). 100-200 ml/min (C). 200-400 ml/min (D). 800-1000 ml/min
17. Which of the followig is /are charecteristic of human placenta ?
(A). Discoid (B). Hemochorial (C). Deciduate (D). All of the above
18. Placental barrier is formed by all, Except ?
(A). Syncytiotrophoblast(B). Cytotrophoblast (C). Endothelium of fetal capilleries (D). Decidua parietalis
19. Fetoplacental circulation is established after fertilization ?
(A). 10-12 days (B). 17-21 days (C). 7-10 days (D). 25-28 days
20. Identify the wrong statement ?
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 171
(A). At 17 week of gestation the weight of placenta & fetus are equal
(B). The ratio of weight of placenta to the weight of the baby at term is 1:6
(C). Hoffbauer cells are macrophage cells which are present in fallopian tube
(D). In placenta villi contain 350 ml fetal blood & intervillous space contain 150 ml maternal blood at term
21. Which of the folowing limits the invasion of decidua by trophoblast ?
(A). Nitabuch‘s membrane(B). Amnion (C). Chorion (D). Cytotrophoblast
22. Small placenta seen in all except ?
(A). Postdatism (B). IUGR (C). Placental infract (D). Gestational diabetes
23. Identify the anomally of placenta in given diagram ?
(A). Placenta succenturiata (B). Placenta Bilobata(C). Placenta Spuria (D). Battledore Placenta
24. After 8-10 weeks of pregnancy main source of progesterone is ?
(A). Syncytiotrophoblast(B). Cytotrophoblast (C). Corpus luteum (D). Ovary
25. Doubling time of hCG is ?
(A). 1.4-2 days (B). 3-4 days (C). 5-7 days (D). 8-10 days
26. A 30-year-old-female H/O Rt adnexal ectopic pregnancy 1 year back coming in OPD with pain in Lt
Adnexa with UPT-positive. Doctor advised her to test spot β-hCG test which value is 20 IU/L, For the
diagnosis of Ectopic pregnancy β-hCG value after 48 hrs should be ?
(A). 45 IU/L (B). 30 IU/L (C). 50 IU/L (D). 55 IU/L
27. Single umbilical artery (SUA) is a significant finding, it is associated with all complications, Except ?
(A). Congenital malformation (B). Prematurity(C). IUGR (D). Post partum haemorrhage
28. Which of the following statement is/are true regarding amniotic fluid ?
(i) Specific gravity of amniotic fluid is 1.008-1.010
(ii) Volume of amniotic fluid is maximum at 24-28 weeks
(iii) Fetal urine is main contributor of amniotic fluid
(iv) Normal color of amniotic fluid is green
(A). (i) & (iii) (B). (i), (ii) & (iii) (C). (i), (ii), (iii) & (iv) (D). (i), (iii) & (iv)
29. Function of amniotic fluid are all except ?
(A). Act as a shock absorber & protect fetus from trauma (B). Give nutrition to fetus
(C). Maintain temperature (D). Prevent adhesion of fetal parts
30. During fetal life maximum growth occurs due to ?
(A). GH (B). Cortisol (C). Thyroxin (D). insulin
31. Wrong statement is ?
(A). Amnion is inner most fetal membrane and it is highly vascular
(B). Chorion is outer most fetal membrane
(C). Amnion is derivative of fetal ectoderm (D). Formation of chorion occurs after 8 day of fertilization
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 172
32. Umbilical cord contains ?
(A). 2 arteries & 2 vein (B). 2 arteries & 1 vein (C). 1 artery & 2 vein (D). Only 2 arteries
33. When the umbilical cord attached to margin of the placenta is called ?
(A). Battledore placenta (B). Velamentons cord insertion
(C). Furcate cord insertion (D). None
34. Complication of placenta succenturita may all, Except ?
(A). Preterm delivery (B). PPH (C). Sepsis & subinvolution(D). Missing lobe
35. Wharton’s Jelly of umbilical cord is derived from ?
(A). Ectoderum (B). Mesoderm (C). Endoderm (D). Trophoblast
36. Oligohydroamnios is considerd when AFI is ?
(A). Below 5 (B). Below 10 (C). Beow 7 (D). Below 15
37. Cause of oligohydroamnios are all, Except ?
(A). Preeclampsia (B). B/L multicystic dysplastic kideny
(C). Maternal DM (D). Posterior urethral valve
38. Complication of oligohydroamnios are all except ?
(A). Malpresentation (B). IUGR (C). Limb deformilies (D). Unstable lie
39. A pregnant women is found to have excessive accumulation of amniotic fluid. Such polyhydroamnios is
likely to be associated with all of the following condition except ?
(A). Oesophageal atretia (B). Cleft lip (C). Anencephaly (D). B/L Renal agenesis
40. All are the indication of amnioinfusion, Except ?
(A). Oligohydroamnios (B). Suspected renal anommalies
(C). To facilitate labour (D). In case of fetal distress
41. A pregnant female goes to doctor and ask for expected date of delivery. Doctor tell her that EDD will be 25
July 2016. According to EDD the patient LMP was ?
(A). 19 Oct 2015 (B). 18 Oct 2015 (C). 02 May 2017 (D). 01 May 2017
42. Life span of fetal RBC is ?
(A). 60 days (B). 90 days (C). 100 days (D). 120 days
43. Ligamentum teres is formed after ?
(A). Obliteration of the umbilical vein (B). Obliteration of the ductus venosus
(C). Obliteration of the ductus arteriosus (D). Obliteration of the umbilical arteries
44. During fetal circulation arrange in descending order according to concentration of oxygen ?
(A). Umbilical vein > RA > IVC > LV> Umbilical artery
(B). Umbilical vein > IVC > RA > LV > Umbilical artery
(C). Umbilical artery > LV > IVC > RA > Umbilical vein
(D). Umbilical artery > IVC > LV > RA > Umbilical vein
45. HbA2 contains ?
(A). 2α + 2β chain (B). 2α + 2γ chain (C). 2α + 2δ chain (D). 2α + 2θ chain
46. Which of the following test differentiate maternal blood from fetal blood ?
(A). Kleihauer- batke test(B). Bubble test (C). Lily‘s test (D). Shake test
47. Fetal sex can be identified on USG by ?
(A). 14 weeks (B). 16 weeks (C). 9 weeks (D). 10 weeks
48. Fetal kidney’s start producing urine by ?
(A). 5 months (B). 3 months (C). 4 months (D). 6 months
49. Estrogen and progesterone is first two months of pregnancy are produced by ?
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 173
(A). Fetal ovaries (B). Fetal adrenal (C). Placenta (D). Corpus luteum
50. Primigravida with full term, complains of faintness on lying down and she feels well when turns to side or
sitting position. This is due to ?
(A). Increased abdominal pressure (B). IVC compression
(C). Increased intracranial pressure (D). After heavy lunch
51. Which of the following is the least likely physiological change in pregnancy ?
(A). Increase in intravascular volume (B). Increase in cardiac output
(C). Increase in stroke volume (D). Increase in peripheral vascular resistance
52. Which is not feature of pseudocyesis ?
(A). Amenorrhea (B). Abdominal distension
(C). Fetal heart sounds are audible (D). None of the above
53. Extra calories requirement during pregnancy & lactation is ?
(A). 350, 600 K. Cal. (B). 300, 550 K. Cal. (C). 600, 350 K. Cal. (D). 550, 300 K. Cal.
54. Total weight gain during pregnancy ?
(A). 6-8 kg (B). 11-12 kg (C). 15-16 kg (D). 18-20 kg
55. Which of the following parameter not decrease during pregnancy ?
(A). Platelet count (B). WBC count (C). Cotting factor 11 & 13 (D). Haematocrit level
56. Maximum cardiac output during pregnancy at ?
(A). Immediately after delivery (B). 2nd
stage of labour
(C). 1st stage of labour (D). 28-32 weeks
57. Which of the following parameter of respiratory system unaffected during pregnancy ?
(A). Tidal volume (B). Total lung capacity
(C). Vital capacity (D). Expiratory reserve volume
58. Which of the following statement is false regarding iron metabolism during pregnancy ?
(A). Decrease serum iron concentration (B). Decrease serum ferritin
(C). Increased total iron binding capacity (D). Decrease serum transferrin
59. NESTROFT test is used for detection of ?
(A). β-Thalassemia (B). Down syndrome (C). Cystic fibrosis (D). Sickle cell anemia
60. Match the following ?
Test Time
(i)Double marker test (P)16-18 week
(ii)Tripple marker test (Q)11-14 weeks
(iii)Quadruple marker test (R)18-22 weeks
(A). (i) Q (ii) P (iii) R (B). (i) P (ii) Q (iii) R (C). (i) Q (ii) R (iii) P (D). (i) R (ii) Q (iii) P
61. Match the following ?
(i)Early deceleration(P)Uteroplacental insufficiency
(ii)Late deceleration (Q)Umbilical cord compressor
(iii)Variable deceleration (R)Head compression
(A). (i) R (ii) Q (iii) P (B). (i) R (ii) P (iii) Q (C). (i) P (ii) Q (iii) R (D). (i) Q (ii) P (iii) R
62. Manning score is done for ?
(A). Fetal well being (B). Progression of labour(C). Induction of labour (D). Cervical dilation
63. Early CVS procedure (before 9 weeks) cause which of the following complication ?
(A). Rh isoimmunization (B). Oromandibular limb defects
(C). Rupture of membrane (D). Vaginal bleeding
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 174
64. Early amniocentesis can be done at ?
(A). 9-11 weeks (B). 11-14 weeks (C). 14-16 weeks (D). 7-9 weeks
65. All of the following test are used for detection of down syndrome except ?
(A). NT scan (B). Double marker test(C). Karyotyping (D). NESTROFT test
66. Triple test includes all except ?
(A). hCG (B). AFP (C). Unconjugated estriol(D). Inhibin-A
67. Which of the following is not seen in down syndrome ?
(A). Trisomy at 21 chromosome (B). Clinodactyly(C). Nasal bone hypoplasia (D). Cystic mass in neck
68. During 1st trimester best parameter to detect fetal age ?
(A). CRL (B). BPD (C). FL (D). AC
69. Targeted anomally scan by ultrasound should be done at ?
(A). 12 weeks (B). 20 weeks (C). 28 weeks (D). 32 weeks
70. Which of the following anomally can be detect earliest on USG ?
(A). Anencephaly (B). Omphalocele (C). Cystic hygroma (D). Diaphragmatic hernia
71. All of the following are included in neural tube defect except ?
(A). Anencephaly (B). Spina bifida (C). Encephalocele (D). Gastroschiasis
72. Match the following ?
Test Time
(i)Chorionic villi sampling (P)15-20 weeks
(ii)Amniocentesis (Q)10-13 weeks
(iii)Cordocentesis (R)20-22 weeks
(A). (i) P (ii) Q (iii) R (B). (i) Q (ii) R (iii) P (C). (i) Q (ii) P (iii) R (D). (i) R (ii) P (iii) Q
73. In india 1st dose of tetanus toxoid during pregnancy should be given at ?
(A). 2nd
trimester (B). As early pregnancy is diagnosed
(C). Before labour pain (D). 3rd
trimester
74. All of the following vaccine are contraindicated during pregnancy, Except ?
(A). BCG (B). MMR (C). Chickenpox (D). IPV
75. A 12 weeks pregnant female with previous history of twin delivery at 38 weeks denotes ?
(A). G2P1 (B). G3P1 (C). G2P2 (D). G2P3
76. At 16 weeks fundal height of uterus is ?
(A). At umbilicus (B). At pubic symphysis
(C). Midway between pubic symphysis & Umbilicus(D). Midway between Umbilicus & Xiphoid process
77. Calcium requirement during pregnancy ?
(A). 600 mg (B). 800 mg (C). 1200 mg (D). 1500 mg
78. Calculation of EDD is done by ?
(A). Naegele‘s formula (B). Shirodkar formula (C). Robin‘s formula (D). Chadwick formula
79. Absolute sign of pregnancy are all, Except ?
(A). Auscultation of fetal heart sound (B). USG evidence of embryo
(C). Radiological demonstration of fetal skelton (D). Amenorrhoea
80. WHO recommends how many antenatal visits ?
(A). 3 visits (B). 12-14 visits (C). 4 visits (D). 6 visits
81. Which of the following statement false regarding folic acid supplementation during pregnancy ?
(A). Folic acid supplementation prevents neural tube defects
(B). Prophylactic dose of folic acid should be start in 1st trimester of pregnancy
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 175
(C). Folic acid dose is 500 μg (D). All are true
82. Total amount of iron required during pregnancy is ?
(A). 500 mg (B). 1000 mg (C). 300 mg (D). 700 mg
83. Match the following ?
Sign Feature
(i)Chadwick sign (P)Softening of cervix
(ii)Osiander’s sign (Q)Bluish discoloration of vagina
(iii)Goodell’s sign (R)Increased pulsation in lateral fornix
(iv)Hegar sign (S)Softening of isthms
(A). (i) Q (ii) R (iii) S (iv) P (B). (i) Q (ii) P (iii) R (iv) S
(C). (i) Q (ii) R (iii) P (iv) S (D). (i) Q (ii) S (iii) P (iv) R
84. Which of the following statement are wrong ?
(A). Palmer‘s sign is regular & Rhythmic uterine contraction which seen at 4-8 weeks of pregnancy
(B). Braxton hicks contraction is nonrhythmic sporadic painless contraction which starts in 2nd
trimester
(C). Quickening is perception of active fetal movement felt by 24 weeks of GA
(D). Lightening seen at 36 weeks of GA
85. Which of the following is not a presumptive sign of pregnancy ?
(A). Amenorrhoea (B). Palpation of fetal part (C). Quickening (D). Breast discomfort
86. Most conclusive sign of pregnancy is ?
(A). Auscultation of fetal heart sound (B). Quickening
(C). Breast discomfort (D). Ballottement
87. During pregnancy PH of vagina is decreased due to ?
(A). Doderlein bacilli (B). Proteus bacilli (C). Klobs-loffler bacilli (D). Klebseilla bacilli
88. Braxton hick contraction starts at ?
(A). 1st trimester (B). 2
nd trimester (C). 3
rd trimester (D). At term
89. Montogomery’s tubercle seen at ?
(A). Vagina (B). Abdonem (C). Breast (D). Face
90. Skin changes during pregnancy are all, Except ?
(A). Chloasma (B). Linea nigra (C). Stria gravidarum (D). Necrobiosis lipodica
91. Colostrum has all component in high amount compared to breast milk except ?
(A). Immunoglobulin (B). Protein (C). Potassium (D). Sodium
92. Best time to test for gestational diabetes during pregnancy ?
(A). 24-28 weeks (B). 10-12 weeks (C). 32-34 weeks (D). 6-8 weeks
93. Supine hypotension syndrome (Mengerts syndrome) occur due to compression of ?
(A). Aorta (B). IVC (C). Carotid artery (D). Iliac vain
94. All of the following statements are true for parity Except ?
(A). Parity refers to number of pregnancies reaching viability (B). In twin pregnancy, parity remains same
(C). If a female has still birth her parity decreases (D). Parity is to affected by number of fetuses delivered
95. Kegels exercise should begin ?
(A). Immediately after delivery (B). 24 hours after delivery
(C). 3 weeks after delivery (D). 6 weeks after delivery
96. Which is most significant finding in cardiotocography for detection of fetal hypoxia ?
(A). Late deacceleration (B). Variable deacceleration
(C). Sinusoidal deacceleration (D). Early deacceleration
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 176
97. Consider the following
(i)Reactive NST
(ii)Absence of deacceleration
(iii)Sinusoidal pattern
Which of the above findings in an antepartum CTG indicate fetal well-being ?
(A). (i) and (ii) only (B). (ii) and (iii) only (C). (i) and (iii) only (D). (i),(ii),(iii)
98. Best confirmation for pregnancy at six weeks ?
(A). USG for cardiac activity (B). Doppler(C). Estimation of serum beta-hCG in urine(D). Bimanual palpation
99. Which of the following is the investigation of choice in a pregnant lady at 18 weeks of pregnancy with past
history of delivering a baby with Down’s syndrome ?
(A). Triple screen test (B). Amniocentesis (C). Chorionic villous biopsy (D). Ultrasonography
100. Most important diameter of pelvis during labour is ?
(A). Interspinous diameter (B). Oblique diameter of inlet
(C). AP diameter of outlet (D). Intertuberous diameter
101. The shortest diameter of fetal head is ?
(A). Biparietal diameter (B). Suboccipitofrontal diameter
(C). Occipitofrontal diameter (D). Bitemporal diameter
102. AP diameter is maximum in which type of pelvis ?
(A). Platypelloid (B). Android (C). Anthropoid (D). Gynecoid
103. The characteristics of caput succedaneum include all of the following except ?
(A). Crosses midline (B). Crosses the suture line
(C). It does not disappear within 2-3 days(D).It is diffuse edematous swelling of the soft tissues of the scalp
104. All of the following are included in first stage of labour except ?
(A). Effacement of Cervix (B). Dilatation of Cervix
(C). Crowning of fetal head (D). Descent of head
105. The perineal injury can be prevented in normal labour by all except ?
(A). Maintaining flexion of the head (B). Timely episiotomy as a routine
(C).Slow delivery of the head in between contractions (D). Effective perineal guard
106. Ritgen maneuver is done in ?
(A). Shoulder dystocia (B). For delivery of head in breech presentation
(C). For delivery of legs in breech (D). For delivery of head in normal labour
107. Cardinal movements of labour are ?
(A). Engagement descent flexion internal rotation extension restitution external rotation
expulsion
(B). Engagement flexion descent internal rotation extension expulsion
(C). Engagement flexion descent external rotation expulsion
(D). Engagement extension internal rotation external rotation expulsion
108. In bishop score all are included except ?
(A). Effacement of cervix(B). Dilatation of cervix(C). Station of head (D). Interspinal diameter
109. All are signs of placental separation except ?
(A). Lengthening of cord(B). Gushing of blood (C). Suprapubic bulge (D). Increase of BP
110. Most common cause of maternal death immediately after delivery ?
(A). Amniotic fluid embolism (B). PPH (C). Uterine inversion (D). Pulmonary embolism
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 177
111. A 24-year-old-female reports in the casualty with history of amenorrhoea for two and half months and
abdominal pain and bleeding per vaginum for one day. On examination, vital parameters and other
systems are normal. On speculum examination, bleeding is found to come from Os. On bimanual
examination, uterus is of 10 weeks size, soft and Os admits one finger. The most likely diagnosis is ?
(A). Threatened abortion(B). Missed abortion (C). Inevitable abortion (D). Incomplete abortion
112. Young lady presents with acute abdominal pain and history of 1.5 months amenorrhoea, on USG
examination there is collection of fluid in the pouch of doughlas and empty gestational sac. Diagnosis is ?
(A). Ectopic pregnancy (B). Pelvic hematocele (C). Threatened abortion (D). Twisted ovarian cyst
113. Match the following ?
(i) True conjugate (P) 10.5 cm
(ii)Obstetric conjugate (Q) 12 cm
(iii)Diagonal conjugate (R) 11 cm
(A). (i) R (ii) Q (iii) P (B). (i) P (ii) Q (iii) R (C). (i) R (ii) P (iii) Q (D). (i) Q (ii) P (iii) R
114. Which of the following statement ia/are true ?
(i) Gynecoid pelvis is most common pelvis
(ii)Anthropoid pelvis is heart shape pelvis
(iii)Face to pubic delivery is most common in anthropoid pelvis
(iv)Anthropoid pelvis AP diameter is more than transverse diameter
(A). (i), (ii), (iii) &(iv) (B). (i), (ii) & (iv) (C). (ii), (iii) & (iv) (D). (i), (iii) & (iv)
115. In which pelvis one Ala of sacral bone is absent ?
(A). Naegele‘s pelvis (B). Robert‘s pelvis (C). Triradiate pelvis (D). Osteomalacic pelvis
116. Most common position during labour is ?
(A). LOT (B). LOA (C). DOA (D). ROA
117. Which of the following statement is false ?
(A). Lambda fuses at 2-3 month (B). Coronal suture seen between frontal & parietal bone
(C). Bregma is triangular shaped & fuses at 18 months (D). Suture are helpful in moulding
118. Vertex presentation seen in which engaging diameter ?
(A). Mentovertical (B). Submentobregmatic(C). Submentovertical (D). Suboccipitobregmatic
119. All of the following statement are true regarding true labour pain except ?
(A). Cervical dilatation & effacement seen (B). Lower abdomen pain radiating to thigh
(C). Absent bag of water (D). Contraction are regular & frequency increases gradually
120. Partograph shows ?
(A). Progression of labour(B). Induction of labour(C). Fetal well being (D). Amount of amniotic fluid
121. Bishop score include all except ?
(A). Cervical dilatation & effacement (B). Cervical position & consistency
(C). Head station (D). Pelvic diameter
122. A primigravida at 37 week of gestation reported to labour room with central placenta previa with heavy
bleeding per vaginum. The fetal heart rate was normal at the time of examination. The best management
option for her is ?
(A). Expectant management (B). Cesarean section
(C). Induction and vaginal delivery (D). Induction and forceps delivery
123. Dose of anti D for antenatal prophylaxis in Rh-negative nonimmunized females ?
(A). Single dose of 1000 IU at 28 weeks (B). Single dose of 1500 IU at 28 weeks
(C). Single dose of 500 IU at 28 weeks (D). Single dose of 1500 IU at 32 weeks
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 178
124. All of the following are used in the treatment of postpartum hemorrhage except ?
(A). Misoprostol (B). Mifepristone (C). Carboprost (D). Methylergometrine
125. Most common type of breech presentation ?
(A). Frank breech (B). Complete breech (C). Footling (D). Knee
126. All of the following are features of obstructed labour except ?
(A). Hot dry vagina (B). Tonic contracted uterus
(C). Bandl‘s ring (D). Unruptured membranes
127. In transverse lie, the presentation is ?
(A). Vertex (B). Breech (C). Brow (D). Shoulder
128. Uterine rupture is least common with ?
(A). LSCS (B). Classical cesarean section (C). Inverted T-shaped incision (D). T-shaped incision
129. An elderly multigravida female presents in labour. She has multiple fibroids in lower uterine segment.
Managemet is ?
(A). Vaginal delivery (B). Trial of labour
(C). LSCS (D). Classical cesarean section followed by hysterectomy
130. A cesarean section was done in the previous pregnancy. All of the following would be indications for
elective cesarean section except ?
(A). Breech (B). Macrosomia (C). Polyhydroamnios (D). Post-term
131. A women at 32 weeks of pregnancy, presents with labour pain. On examination, her cervix is dilated and
uterine contractions are felt. The management is ?
(A). Isoxsuprine hydrochloride (B). Dilatation and evacuation
(C). Termination of pregnancy (D). Wait and watch
132. All of the following drugs have been used for medical abortion except ?
(A). Mifepristone (B). Misoprostol (C). Methotrexate (D). Atosiban
133. A 27-year-old female with a history of 8 weeks amenorrhoea complains of vaginal bleeding and lower
abdominal pain. On USG examination there is gestational sac with absent fetal parts. The diagnosis is ?
(A). Ectopic pregnancy (B). Incarcerated abortion
(C). Threatened abortion (D). Corpus luteum cyst
134. Most valuable diagnostic test in case of suspected ectopic pregnancy ?
(A). Serial β-hCG levels (B). Transvaginal USG
(C). Progesterone measurement (D). Culdocentesis
135. A hypertensive pregnant women at 34 weeks comes with history of pain in abdomen, bleeding per
vaginum and loss of fetal movements. On examination the uterus is contracted with increased uterine tone.
Fetal heart sounds are absent. The most likely diagnosis is ?
(A). Placenta previa (B). Hydramnios (C). Premature labour (D). Abruptio placenta
136. A lady with 38 weeks pregnancy and painless vaginal bleeding comes to casualty. On examination head is
engaged and uterus is non tender and relaxed. The next line of treatment is ?
(A). Perspeculum examination (B). Conservative management
(C). Termination of pregnancy (D). Ultrasonography
137. Best time to give Anti-D to a pregnant patient ?
(A). 12 weeks (B). 28 weeks (C). 36 weeks (D). After delivery
138. Which of the following tests is most sensitive for the detection of iron depletion in pregnancy ?
(A). Serum iron (B). Serum ferritin (C). Serum transferrin (D). Serum iron binding capacity
139. In pregnancy, which type of anemia is not common in India ?
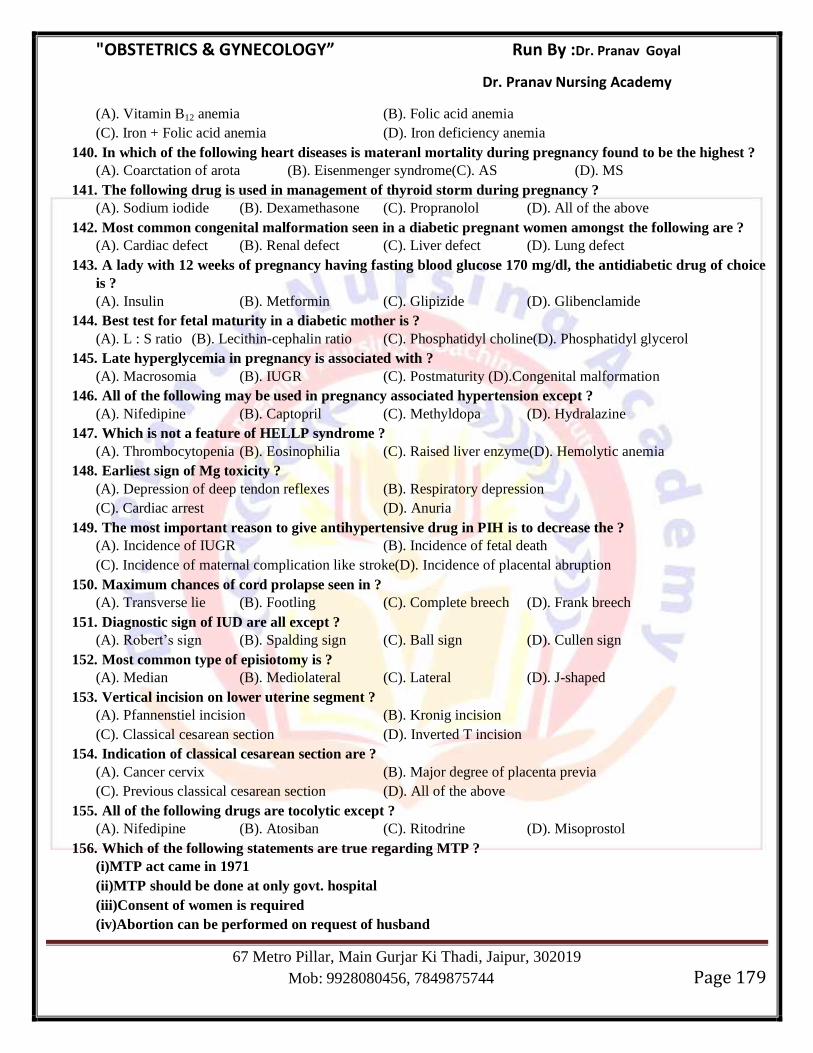
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 179
(A). Vitamin B12 anemia (B). Folic acid anemia
(C). Iron + Folic acid anemia (D). Iron deficiency anemia
140. In which of the following heart diseases is materanl mortality during pregnancy found to be the highest ?
(A). Coarctation of arota (B). Eisenmenger syndrome(C). AS (D). MS
141. The following drug is used in management of thyroid storm during pregnancy ?
(A). Sodium iodide (B). Dexamethasone (C). Propranolol (D). All of the above
142. Most common congenital malformation seen in a diabetic pregnant women amongst the following are ?
(A). Cardiac defect (B). Renal defect (C). Liver defect (D). Lung defect
143. A lady with 12 weeks of pregnancy having fasting blood glucose 170 mg/dl, the antidiabetic drug of choice
is ?
(A). Insulin (B). Metformin (C). Glipizide (D). Glibenclamide
144. Best test for fetal maturity in a diabetic mother is ?
(A). L : S ratio (B). Lecithin-cephalin ratio (C). Phosphatidyl choline(D). Phosphatidyl glycerol
145. Late hyperglycemia in pregnancy is associated with ?
(A). Macrosomia (B). IUGR (C). Postmaturity (D).Congenital malformation
146. All of the following may be used in pregnancy associated hypertension except ?
(A). Nifedipine (B). Captopril (C). Methyldopa (D). Hydralazine
147. Which is not a feature of HELLP syndrome ?
(A). Thrombocytopenia (B). Eosinophilia (C). Raised liver enzyme(D). Hemolytic anemia
148. Earliest sign of Mg toxicity ?
(A). Depression of deep tendon reflexes (B). Respiratory depression
(C). Cardiac arrest (D). Anuria
149. The most important reason to give antihypertensive drug in PIH is to decrease the ?
(A). Incidence of IUGR (B). Incidence of fetal death
(C). Incidence of maternal complication like stroke(D). Incidence of placental abruption
150. Maximum chances of cord prolapse seen in ?
(A). Transverse lie (B). Footling (C). Complete breech (D). Frank breech
151. Diagnostic sign of IUD are all except ?
(A). Robert‘s sign (B). Spalding sign (C). Ball sign (D). Cullen sign
152. Most common type of episiotomy is ?
(A). Median (B). Mediolateral (C). Lateral (D). J-shaped
153. Vertical incision on lower uterine segment ?
(A). Pfannenstiel incision (B). Kronig incision
(C). Classical cesarean section (D). Inverted T incision
154. Indication of classical cesarean section are ?
(A). Cancer cervix (B). Major degree of placenta previa
(C). Previous classical cesarean section (D). All of the above
155. All of the following drugs are tocolytic except ?
(A). Nifedipine (B). Atosiban (C). Ritodrine (D). Misoprostol
156. Which of the following statements are true regarding MTP ?
(i)MTP act came in 1971
(ii)MTP should be done at only govt. hospital
(iii)Consent of women is required
(iv)Abortion can be performed on request of husband
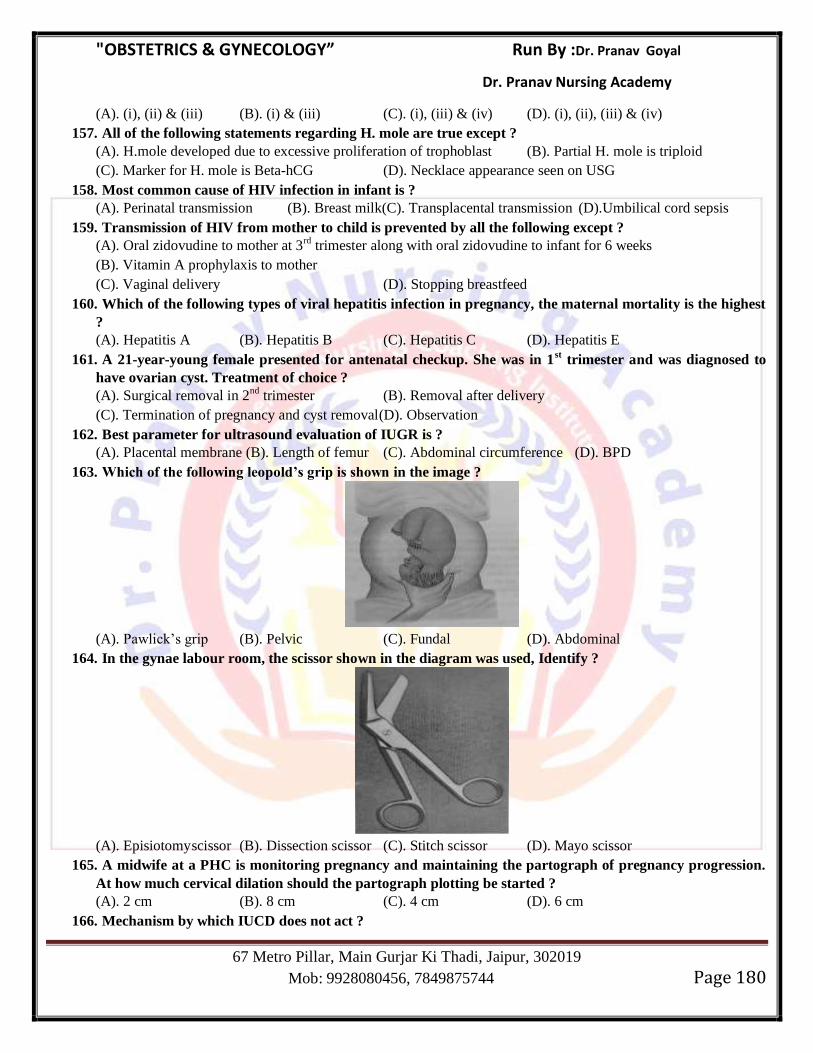
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 180
(A). (i), (ii) & (iii) (B). (i) & (iii) (C). (i), (iii) & (iv) (D). (i), (ii), (iii) & (iv)
157. All of the following statements regarding H. mole are true except ?
(A). H.mole developed due to excessive proliferation of trophoblast (B). Partial H. mole is triploid
(C). Marker for H. mole is Beta-hCG (D). Necklace appearance seen on USG
158. Most common cause of HIV infection in infant is ?
(A). Perinatal transmission (B). Breast milk(C). Transplacental transmission (D).Umbilical cord sepsis
159. Transmission of HIV from mother to child is prevented by all the following except ?
(A). Oral zidovudine to mother at 3rd
trimester along with oral zidovudine to infant for 6 weeks
(B). Vitamin A prophylaxis to mother
(C). Vaginal delivery (D). Stopping breastfeed
160. Which of the following types of viral hepatitis infection in pregnancy, the maternal mortality is the highest
?
(A). Hepatitis A (B). Hepatitis B (C). Hepatitis C (D). Hepatitis E
161. A 21-year-young female presented for antenatal checkup. She was in 1st trimester and was diagnosed to
have ovarian cyst. Treatment of choice ?
(A). Surgical removal in 2nd
trimester (B). Removal after delivery
(C). Termination of pregnancy and cyst removal(D). Observation
162. Best parameter for ultrasound evaluation of IUGR is ?
(A). Placental membrane (B). Length of femur (C). Abdominal circumference (D). BPD
163. Which of the following leopold’s grip is shown in the image ?
(A). Pawlick‘s grip (B). Pelvic (C). Fundal (D). Abdominal
164. In the gynae labour room, the scissor shown in the diagram was used, Identify ?
(A). Episiotomy scissor (B). Dissection scissor (C). Stitch scissor (D). Mayo scissor
165. A midwife at a PHC is monitoring pregnancy and maintaining the partograph of pregnancy progression.
At how much cervical dilation should the partograph plotting be started ?
(A). 2 cm (B). 8 cm (C). 4 cm (D). 6 cm
166. Mechanism by which IUCD does not act ?
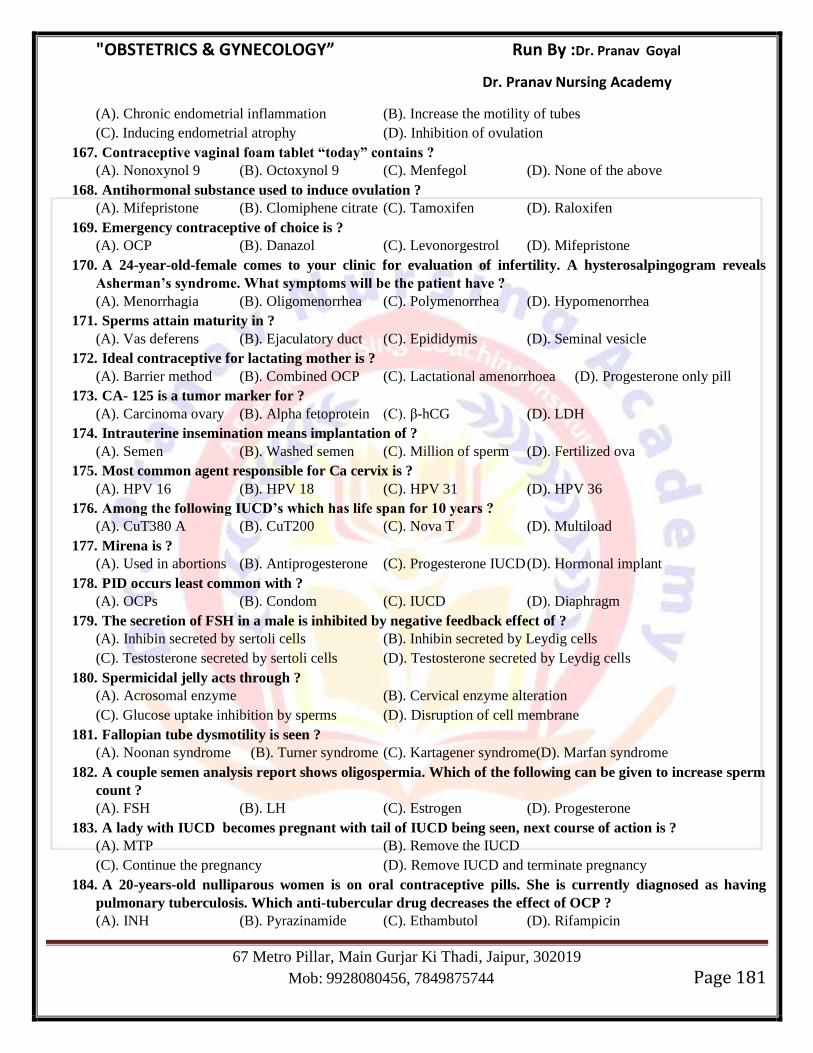
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 181
(A). Chronic endometrial inflammation (B). Increase the motility of tubes
(C). Inducing endometrial atrophy (D). Inhibition of ovulation
167. Contraceptive vaginal foam tablet “today” contains ?
(A). Nonoxynol 9 (B). Octoxynol 9 (C). Menfegol (D). None of the above
168. Antihormonal substance used to induce ovulation ?
(A). Mifepristone (B). Clomiphene citrate (C). Tamoxifen (D). Raloxifen
169. Emergency contraceptive of choice is ?
(A). OCP (B). Danazol (C). Levonorgestrol (D). Mifepristone
170. A 24-year-old-female comes to your clinic for evaluation of infertility. A hysterosalpingogram reveals
Asherman’s syndrome. What symptoms will be the patient have ?
(A). Menorrhagia (B). Oligomenorrhea (C). Polymenorrhea (D). Hypomenorrhea
171. Sperms attain maturity in ?
(A). Vas deferens (B). Ejaculatory duct (C). Epididymis (D). Seminal vesicle
172. Ideal contraceptive for lactating mother is ?
(A). Barrier method (B). Combined OCP (C). Lactational amenorrhoea (D). Progesterone only pill
173. CA- 125 is a tumor marker for ?
(A). Carcinoma ovary (B). Alpha fetoprotein (C). β-hCG (D). LDH
174. Intrauterine insemination means implantation of ?
(A). Semen (B). Washed semen (C). Million of sperm (D). Fertilized ova
175. Most common agent responsible for Ca cervix is ?
(A). HPV 16 (B). HPV 18 (C). HPV 31 (D). HPV 36
176. Among the following IUCD’s which has life span for 10 years ?
(A). CuT380 A (B). CuT200 (C). Nova T (D). Multiload
177. Mirena is ?
(A). Used in abortions (B). Antiprogesterone (C). Progesterone IUCD (D). Hormonal implant
178. PID occurs least common with ?
(A). OCPs (B). Condom (C). IUCD (D). Diaphragm
179. The secretion of FSH in a male is inhibited by negative feedback effect of ?
(A). Inhibin secreted by sertoli cells (B). Inhibin secreted by Leydig cells
(C). Testosterone secreted by sertoli cells (D). Testosterone secreted by Leydig cells
180. Spermicidal jelly acts through ?
(A). Acrosomal enzyme (B). Cervical enzyme alteration
(C). Glucose uptake inhibition by sperms (D). Disruption of cell membrane
181. Fallopian tube dysmotility is seen ?
(A). Noonan syndrome (B). Turner syndrome (C). Kartagener syndrome(D). Marfan syndrome
182. A couple semen analysis report shows oligospermia. Which of the following can be given to increase sperm
count ?
(A). FSH (B). LH (C). Estrogen (D). Progesterone
183. A lady with IUCD becomes pregnant with tail of IUCD being seen, next course of action is ?
(A). MTP (B). Remove the IUCD
(C). Continue the pregnancy (D). Remove IUCD and terminate pregnancy
184. A 20-years-old nulliparous women is on oral contraceptive pills. She is currently diagnosed as having
pulmonary tuberculosis. Which anti-tubercular drug decreases the effect of OCP ?
(A). INH (B). Pyrazinamide (C). Ethambutol (D). Rifampicin
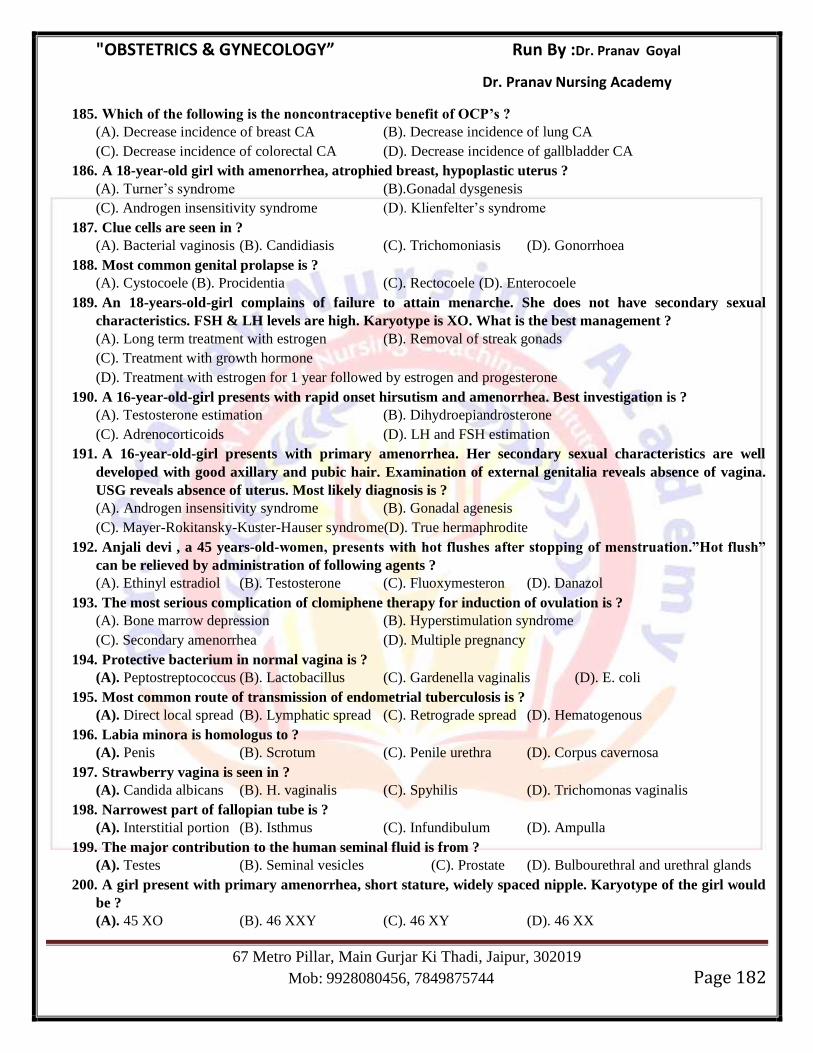
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 182
185. Which of the following is the noncontraceptive benefit of OCP’s ?
(A). Decrease incidence of breast CA (B). Decrease incidence of lung CA
(C). Decrease incidence of colorectal CA (D). Decrease incidence of gallbladder CA
186. A 18-year-old girl with amenorrhea, atrophied breast, hypoplastic uterus ?
(A). Turner‘s syndrome (B).Gonadal dysgenesis
(C). Androgen insensitivity syndrome (D). Klienfelter‘s syndrome
187. Clue cells are seen in ?
(A). Bacterial vaginosis (B). Candidiasis (C). Trichomoniasis (D). Gonorrhoea
188. Most common genital prolapse is ?
(A). Cystocoele (B). Procidentia (C). Rectocoele (D). Enterocoele
189. An 18-years-old-girl complains of failure to attain menarche. She does not have secondary sexual
characteristics. FSH & LH levels are high. Karyotype is XO. What is the best management ?
(A). Long term treatment with estrogen (B). Removal of streak gonads
(C). Treatment with growth hormone
(D). Treatment with estrogen for 1 year followed by estrogen and progesterone
190. A 16-year-old-girl presents with rapid onset hirsutism and amenorrhea. Best investigation is ?
(A). Testosterone estimation (B). Dihydroepiandrosterone
(C). Adrenocorticoids (D). LH and FSH estimation
191. A 16-year-old-girl presents with primary amenorrhea. Her secondary sexual characteristics are well
developed with good axillary and pubic hair. Examination of external genitalia reveals absence of vagina.
USG reveals absence of uterus. Most likely diagnosis is ?
(A). Androgen insensitivity syndrome (B). Gonadal agenesis
(C). Mayer-Rokitansky-Kuster-Hauser syndrome(D). True hermaphrodite
192. Anjali devi , a 45 years-old-women, presents with hot flushes after stopping of menstruation.”Hot flush”
can be relieved by administration of following agents ?
(A). Ethinyl estradiol (B). Testosterone (C). Fluoxymesteron (D). Danazol
193. The most serious complication of clomiphene therapy for induction of ovulation is ?
(A). Bone marrow depression (B). Hyperstimulation syndrome
(C). Secondary amenorrhea (D). Multiple pregnancy
194. Protective bacterium in normal vagina is ?
(A). Peptostreptococcus (B). Lactobacillus (C). Gardenella vaginalis (D). E. coli
195. Most common route of transmission of endometrial tuberculosis is ?
(A). Direct local spread (B). Lymphatic spread (C). Retrograde spread (D). Hematogenous
196. Labia minora is homologus to ?
(A). Penis (B). Scrotum (C). Penile urethra (D). Corpus cavernosa
197. Strawberry vagina is seen in ?
(A). Candida albicans (B). H. vaginalis (C). Spyhilis (D). Trichomonas vaginalis
198. Narrowest part of fallopian tube is ?
(A). Interstitial portion (B). Isthmus (C). Infundibulum (D). Ampulla
199. The major contribution to the human seminal fluid is from ?
(A). Testes (B). Seminal vesicles (C). Prostate (D). Bulbourethral and urethral glands
200. A girl present with primary amenorrhea, short stature, widely spaced nipple. Karyotype of the girl would
be ?
(A). 45 XO (B). 46 XXY (C). 46 XY (D). 46 XX
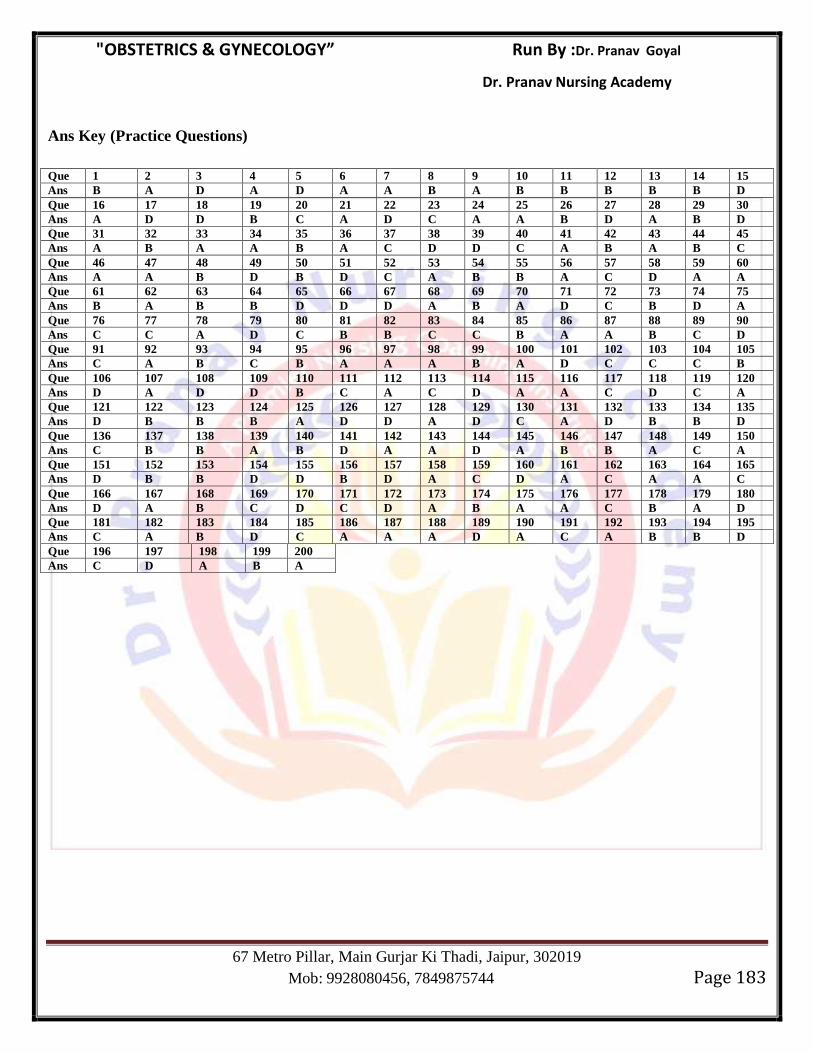
"OBSTETRICS & GYNECOLOGY” Run By :Dr. Pranav Goyal
Dr. Pranav Nursing Academy
67 Metro Pillar, Main Gurjar Ki Thadi, Jaipur, 302019
Mob: 9928080456, 7849875744 Page 183
Ans Key (Practice Questions)
Que 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Ans B A D A D A A B A B B B B B D
Que 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Ans A D D B C A D C A A B D A B D
Que 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45
Ans A B A A B A C D D C A B A B C
Que 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
Ans A A B D B D C A B B A C D A A
Que 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75
Ans B A B B D D D A B A D C B D A
Que 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90
Ans C C A D C B B C C B A A B C D
Que 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105
Ans C A B C B A A A B A D C C C B
Que 106 107 108 109 110 111 112 113 114 115 116 117 118 119 120
Ans D A D D B C A C D A A C D C A
Que 121 122 123 124 125 126 127 128 129 130 131 132 133 134 135
Ans D B B B A D D A D C A D B B D
Que 136 137 138 139 140 141 142 143 144 145 146 147 148 149 150
Ans C B B A B D A A D A B B A C A
Que 151 152 153 154 155 156 157 158 159 160 161 162 163 164 165
Ans D B B D D B D A C D A C A A C
Que 166 167 168 169 170 171 172 173 174 175 176 177 178 179 180
Ans D A B C D C D A B A A C B A D
Que 181 182 183 184 185 186 187 188 189 190 191 192 193 194 195
Ans C A B D C A A A D A C A B B D
Que 196 197 198 199 200
Ans C D A B A
Related Documents







