© The C hildren's M ercy H ospital, 2015 Kim berly H artm an,M D A ssistantProfessorofPediatrics D epartm entofPediatric R ehabilitation M edicine C hildren’s M ercy H ospital K ansas C ity,M O Procedure-related Pain

Objective Recognize methods to manage procedural pain Pain + anxiety distress 2.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
© The Children's Mercy Hospital, 2015
Kimberly Hartman, MDAssistant Professor of Pediatrics
Department of Pediatric Rehabilitation MedicineChildren’s Mercy Hospital
Kansas City, MO
Procedure-related Pain

Objective
• Recognize methods to manage procedural pain
• Pain + anxiety distress
2

3
Common Procedures
• Chemodenervation
– Botulinum toxin
– Phenol
• Intrathecal Baclofen Pump refill
• EMG
• Trigger point injections

4
Why?
• Needle-based procedures induce high levels of distress:– 83% toddlers (2.5-6yo)– 51% children (7-12yo)– 28% adolescents (≥12yo)
• ED: IM injections reported in top 5 most painful and distressing procedures
• Inpatients: procedural pain reported as greater than disease-related and surgical pain
Humphrey 1992; Babl 2008; Shomaker 2015

5
Acute Implications
• Increased distress:– Patient– Parent– Providers
• Inability to perform procedure accurately or completely
• Increased time spent in procedure
Walco 2008; Smith 2007; Kennedy 2008
6
Memory
• Memory can shape future reactions to painful events
• Stressful experience recalled up to years later
• Adults report distress based on childhood experiences
Painful event
Remembered pain
Walco 2008; von Baeyer 2004; Noel 2002; Pate 1996
Remembered Pain
7von Baeyer 2004
•Decreased reaction over time
•Milder pain, more mature coping
Habituation
•Increased reaction over time ± reduced pain threshold
•More severe pain, younger kids, less mature coping
Sensitization
8
Long-term Implications
• Increased anticipatory anxiety
• Increased pain perception
• Diminished analgesic effectiveness
• Needle phobia (10% of adult population)
• Avoidance of medical care
Walco 2008; Taddio 1997; von Baeyer 2004; Weisman 1998; Hamilton 1995; Rocha 2003
Quality >> Quantity
9
Factors to Consider
• Patient temperament• Developmental age• Parental anxiety• Culture
• Prior patient experiences with procedure
• Type of procedure• Procedure duration
Bearden 2012; Kristjansdottir 2012
10
Management
• Procedural• Physical• Psychological• Pharmacological

11
Procedural
• Needle size
• Injection volume
• Simultaneous injections
No evidence higher Gauge is better
Patients need to be aware of sensation
Taddio 2009; Goodenough 2000; Beirne 2015; Price 2009; Hanson 2010
May have decreased pain behaviors

12
Procedural
• No aspiration and rapid injection speed
• Less painful formulation injected first
• Sitting up or holding (vs. supine)
Less pain and no negative effects (for IM imms)
Similar to less painful site first?
Safety concerns? Access to site?
Taddio 2009; Goodenough 2000; Beirne 2015; Price 2009; Howard 2012
13
Physical
• Stroking skin • Pressure• Cold• Vibration• Vibration + cold• Swaddling, tucking,
kangaroo care (infants)
Decreased pain with IM immunizations unknown if translates to Rehab procedures
Taddio 2009; Sahiner 2015; Howard 2012; Pillai Riddell 2012

14
Vapocoolant
• Mixed results• IM: in 4-6yo, can increase pain• IV: no significant pain reduction in children• EMG (adults): more effective than EMLA
cream or no treatment
Cohen 2009; Hogan 2014; Moon 2013; MacLaren 2007; Howard 2012
Fast and cheap
15
Physical
• Sucrose 24%
• Glucose 30%
• Breast-feeding
• Non-nutritive sucking
• Non-nutritive sucking (≤ 3 years)
• No benefit:
– Sweet gum
– Lollipop
– Sucrose
Infants ˂12 months Children ˃ 12 months
Harrison 2010; Kassab 2012; Harrison 2015
16
Psychological: Preparation
• What will happen• How it will feel• What will be done for pain• How child can help• Demonstration
Taddio 2014; Slifer 2011

17
Parent Preparation
• Calm
• Coaching to cope
• Distraction
• Anxious
• Apologizing
• Criticizing
• Reassuring
• Empathizing
Positive strategies Negative strategies
Jones 2005; Taddio 2014
18
Distraction
• Distraction more beneficial than reassurance
• Parent involvement• Specialist involvement
(i.e., Child Life, Music)• No/low tech vs. high
tech• Interactive vs. passive• Child choice vs. no child
choice
McMutry 2010; Birnie 2014; Uman 2013

19
Reframing Memory
• Recall of positives:
– Portions of procedure (“You held really still”)
– Positive coping strategies (“You did a great job taking deep breaths”)
• May be able to create more adaptive memories
Chen
20
Pharmacological
• Topical• Enteral• Sedation• Anesthesia

21
Topical
Anesthetic Dosage forms
Application time (minutes)
Lidocaine 2.5% - prilocaine 2.5%
CreamGelPatch
60-90
Liposomal lidocaine 4%
Cream 30
Lidocaine 7% - tetracaine 7%
Heat patch
20-30
• Occlusive dressing helps lido/prilo permeate
• May not need occlusive dressing with liposomal lido
• Main side effects are local
• Methemoglobinemia at high doses
Things to consider
Taddio 2014; Zempsky 2014

22
Enteral
• Few studies with decreased local reaction (acetaminophen)
• No studies for acute pain during procedure• ? Benefit for soreness after procedure
Taddio 2014
23
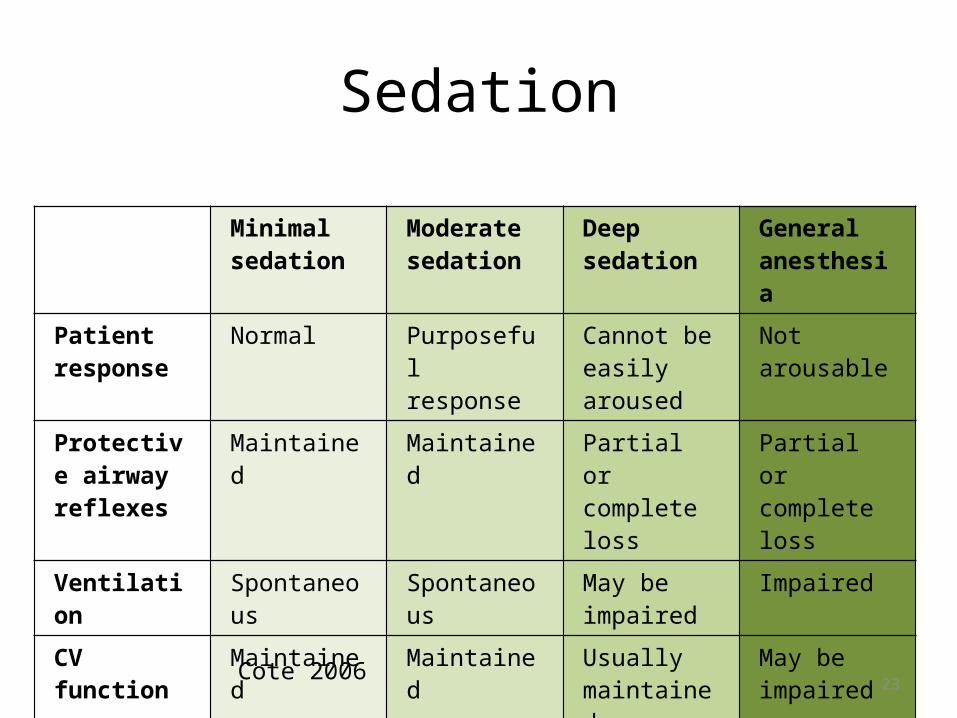
Sedation
Minimal sedation
Moderate sedation
Deep sedation
General anesthesia
Patient response
Normal Purposeful response
Cannot be easily aroused
Not arousable
Protective airway reflexes
Maintained Maintained Partial or complete loss
Partial or complete loss
Ventilation Spontaneous Spontaneous May be impaired
Impaired
CV function Maintained Maintained Usually maintained
May be impaired
Cote 2006

24
ASA Physical Status ClassificationClass I A normally healthy patient
Class II A patient with mild systemic disease (eg, controlled reactive airway disease)
Class III A patient with severe systemic disease (eg, a child who is actively wheezing)
Class IV A patient with severe systemic disease that is a constant threat to life (eg, a child with status asthmaticus)
Class V A moribund patient who is not expected to survive without the operation (eg, a patient with severe cardiomyopathy requiring heart transplantation)
Cote 2006
25
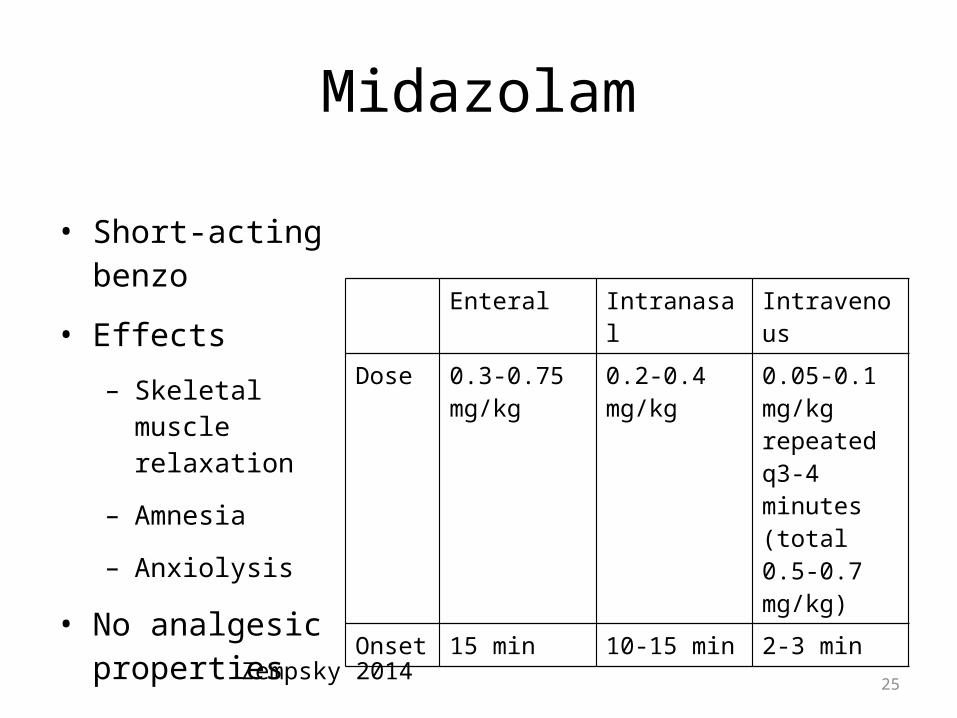
Midazolam
• Short-acting benzo
• Effects
– Skeletal muscle relaxation
– Amnesia
– Anxiolysis
• No analgesic properties
Enteral Intranasal IntravenousDose 0.3-0.75
mg/kg0.2-0.4 mg/kg 0.05-0.1
mg/kg repeated q3-4 minutes (total 0.5-0.7 mg/kg)
Onset 15 min 10-15 min 2-3 min
Zempsky 2014

26
Nitrous Oxide
• Analgesic
• Anesthetic
• Weak sedative
• Onset: minutes
• Offset: rapid when gas discontinued
• Minimal CV or respiratory effects
Zempsky 2014; Pedersen 2013; Brochard 2009
27
Other Medications
• Pentobarbital
• IV Propofol
• IV Dexmedetomidine
• Fentanyl
• Ketamine
Sedatives Analgesics
Zempsky 2014
28
Anesthesia Risks
• Anesthetic-induced neuro-toxicity• Exposure < 3 years old:
– Deficits in language– Deficits in reasoning
Ing 2012; Sanders 2013

29
Summary
• Untreated procedure-related pain & anxiety has short- and long-term consequences
• Treatment needs to be based on individual characteristics and developmental age
• Procedural and physical adaptations can help but may not be feasible
• Distraction helps• Topical anesthetic helps• Sedation: weigh risks &
benefits• Need more research!
Questions: [email protected]
30
References• Babl FE, Mandrawa C, O’Sullivan R, Crellin D. Procedural pain and distress in young children as perceived by
medical and nursing staff. Pediatric Anesth. 2008;18:412-419.• Baxter AL, Cohen LL, McElvery HL, Lawson ML, von Baeyer CL. An integration of vibration and cold relieves
venipuncture pain in a pediatric emergency department. Ped Emer Care. 2011;27(12):1151-1156.• Bearden DJ, Feinstein A, Cohen LL. The influence of parent preprocedural anxiety on child procedural pain:
mediation by child procedural anxiety. J Pediatr Psychol. 2012;37(6):680-686.• Beirne PV, Hennessy S, Cadogan SL, Shiely F, Fitzgerald T, MacLeod F. Needle size for vaccination
procedures in children and adolescents. Cochrane Database of Systematic Reviews. 2015;6(Art. No: CD010720:1-118.
• Birnie KA, Noel M, Parker JA et al. Systematic review and meta-analysis of distraction and hypnosis for needle-related pain and distress in children and adolescents. J Pediatric Psychol. 2014;39(8)783-808.
• Brochard S, Blajan V, Lempereur M et al. Effectiveness of nitrous oxide and analgesic cream (lidocaine and prilocaine) for prevention of pain during intramuscular botulinum toxin injections in children. Ann Phys Rehab Med. 2009:52(10):704-716.
• Cote CJ, Wilson S. Guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures: an update. Pediatrics. 2006;118(6):2587-2602.
• Cravero JP. Procedural sedation. In: McGrath PJ et al., ed. Oxford Textbook of Paediatric Pain. Oxford, UK: Oxford University Press; 2014:194-204.
• Cummings EA, Reid GJ, Finley GA, McGrath P, Ritchie JA. Prevalence and source of pain in pediatric inpatients. Pain. 1996;68:25-31.
• Hanson D, Hall W, Mills LL et al. Comparison of distress and pain in infants randomized to groups receiving standard versus multiple immunizations. Inf Beh Dev. 2010;33:289-296.

31
• Harrison D, Stevens B, Bueno M et al. Efficacy of sweet solutions for analgesia in infants between 1 and 12 months of age: a systematic review. Arch Dis Child. 2010;95:406-413.
• Harrison D, Yamada J, Adams-Webber T, OhlssonA, Beyene J, Stevens B. Sweet tasting solutions for reduction of needle-related procedural pain in children aged one to 16 years (review). Cochrane Database of Systematic Reviews. 2015;5(Art No:CD008408).
• Hogan M, Smart S, Shah V, Taddio A. A systematic review of vapocoolants for reducing pain from venipuncture and venous cannulation in children and adults. J Emer Med. 2014;47(6):736-749.
• Horn MI, McCarthy AM. Children’s responses to sequential versus simultaneous immunization injections. J Pediatr Health Care. 1999;13:18-23.
• Howard R, Carter B, Curry J et al. Good practice in postoperative and procedural pain management, 2nd edition, 2012. Pediatric Anesthesia. 2012;22(Suppl. 1):1-79.
• Humphrey GB, Boon CMJ, van Linden van den Huevell GFEC, van de Wiel HBM. The occurrence of high levels of acute behavioral distress in children and adolescents undergoing routine venipunctures. Pediatrics. 1992;90:87-91.
• Ing C, DiMaggio C, Whitehouse A et al. Long-term differences in language and cognitive function after childhood exposure to anesthesia. Pediatrics. 2012;130(3):e476-e485.
• Jones M, Qazi M, Young KD. Ethnic differences in parent preference to be present for painful medical procedures. Pediatrics.2005;116(2):e191-e197.
• Kassab M, Foster JP, Foureur M, Fowler C. Sweet-tasting solutions for needle-related procedural pain in infants one month to one year of age (review). Cochrane Database of Systematic Reviews. 2012;12(Art No: CD008411). Kazak AE, Penati B, Brophy P, Himelstein B. Pharmacologic and psychologic interventions for procedural pain. Pediatrics. 1998;102(1):59-66.
• Kennedy RM, Luhmann J, Zempsky WT. Clinical implications of unmanaged needle-insertion pain and distress in children. Pediatrics. 2008;122(3):S130-S133.
• Kristjansdottir O, Unruh AM, McAlpine L, McGrath PJ. A systematic review of cross-cultural comparison studies of child, parent, and health professional outcomes associated with pediatric medical procedures. J Pain. 2012;13(3):207-219.
• Lee GY, Yamada J, Kyololo O, Shorkey A, Stevens B. Pediatric clinical practice guidelines for acute procedural pain: a systematic review. Pediatrics. 2014;133(3):500-515.
• MacLaren JE, Cohen LL. Interventions for paediatric procedure-related pain in primary care. Paediatr Child Health. 2007;12(2):111-116.
• McCarthy AM, Kleiber C, Hanrahan K, Zimmerman MB, Westhus N, Allen S. Factors explaining children’s responses to intravenous needle insertion. Nurs Res. 2010;59(6): 407-416.
• Noel M, Chamgers CT, McGrath PJ, Klein RM, Stewart SH. The influence of children’s pain memories on subsequent pain experience. Pain. 2012;153:1563-1572.
• Pillai Riddell RR, Racine NM, Turcotte K et al. Non-pharmacological management of infant and young child procedural pain (review). Cochrane Database of Systematic Reviews. 2012;10(Art No.: CD006275)
• Pedersen RS, Bayat A, Steen NP, Bouchy Jacobsson ML. Nitrous oxide provides safe and effective analgesia for minor paediatric procedures—a systematic review. Dan Med J. 2013;60(6):1-8.
• Price KM, Williams ZY, Woodward JA. Needle preference in patients receiving cosmetic botulinum toxin type A. Dermatol Surg. 2010;36:109-112.
• Rocha EM, Prkachin KM, Beaumont SL, Hardy CL, Zumbo BD. Pain reactivity and somatization in kindergarten-age children. J Pediatric Psychol. 2003;28(1):47-57.
• Sahiner NC, Inal S, Akbay AS. The effect of combined stimulation of external cold and vibration during immunizations on pain and anxiety levels in children. J PeriAnesth Nurs. 2015;30(3):228-235.
• Sanders RD, Hassell J, Davidson AJ, Roberston NJ, Ma D. Impact of anaesthetics and surgery on neurodevelopment: an update. Br J Anesth. 2013;110(S1);i53-i72.
• Shah V, Taddio A, Rieder MJ. Effectiveness and tolerability of pharmacologic combined interventions for reducing injection pain during routine childhood immunizations: systematic review and meta-analyses. Clin Thera. 2009;31(Supplement B):S104-151.
• Shomaker K, Dutton S, Mark M. Pain prevalence and treatment patterns in a US children’s hospital. Hosp Peds. 2015;5(7):363-370.
• Slater R, Cornelissen L, Fabrizi L et al. Oral sucrose as an analgesic drug for procedural pain in newborn infants: a randomized controlled trial. Lancet. 2010;376:1225-1232.
• Slifer KJ, Hankinson JC, Zettler MA et al. Distraction, exposure therapy, counterconditioning, and topical anesthetic for acute pain management during needle sticks in children with intellectual and developmental disabilities. Clin Pediatrics. 2011;50(8):688-697.
• Taddio A, Katz J, Ilersich AL, Koren G. Effect of neonatal circumcision on pain response during subsequent routine vaccination. Lancet. 1997;349:599-603.
• Taddio A, Manley J, Potash L, Ipp M, Sgro M, Shah V. Routine immunization practices: use of topical anesthetics and oral analgesics. Pediatrics. 2007;120(3):e637-e643
• Taddio A, Ilersich AL, Ipp M, Kikuta A, Shah V. Physical interventions and injection techniques for reducing injection pain during routine childhood immunizations: systematic review of randomized controlled trials and quasi-randomized controlled trials. Clin Therap. 2009;31(Suppl B):S48-S76.
• Taddio A, Appleton M, Bortolussi R et al. Reducing the pain of childhood vaccination: an evidence-based clinical practice guideline. CMAJ. 2010;182(18):E843-E855.
• Taddio A. Needle procedures. In: McGrath PJ et al., ed. Oxford Textbook of Paediatric Pain. Oxford, UK: Oxford University Press; 2014:184-193.
• Uman LS, Birnie KA, Noel M et al. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database of Systematic Reviews. 2013;10(Art. No. CD005179).
• Von Baeyer CL, Marche TA, Rocha EM, Salmon K. Children’s memory for pain: overview and implications for practice. J Pain. 2004;5(5):241-249.
• Walco GA. Needle pain in children: contextual factors. Pediatrics. 2008;122(Suppl 3):S125-S129.• Zepmsky WT. Topical anaesthetics and analgesics. In: McGrath PJ et al., ed. Oxford Textbook of Paediatric Pain.
Oxford, UK: Oxford University Press; 2014:486-494. • Zier JL, Rivard PF, Krach LE, Wendorf HR. Effectiveness of sedation using nitrous oxide compared with enteral
midazolam for botulinum toxin A injections in children. Dev Med Child Neuro. 2008;50:854-858.
Related Documents











