NUTRITIONAL INTERVENTION IN DIABETES: BARAKATUN NISAK MOHD YUSOF Ph.D (UKMalaysia) Senior Lecturer and Dietitian Department of Nutrition & Dietetics Faculty of Medicine & Health Sciences Universiti Putra Malaysia 1 MJM-UPM 8 NOV 2012 Translating Scientific Evidence into Practice

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
NUTRITIONAL INTERVENTION IN DIABETES:
BARAKATUN NISAK MOHD YUSOF
Ph.D (UKMalaysia)
Senior Lecturer and Dietitian Department of Nutrition & Dietetics
Faculty of Medicine & Health Sciences Universiti Putra Malaysia
1 MJM-UPM 8 NOV 2012
Translating Scientific Evidence into Practice

SIZE of the PROBLEM
2
• The Size of the problem
• Patients’ common presentation
• Importance of nutritional intervention in diabetes management
• Translating the evidences into practices
• Summary

Where is Malaysia in the midst of Asian Epidemic of Diabetes?
3
Estimated prevalence of diabetes among adults aged 20-79
years old in 11 Asian countries
IDF Diabetes Atlas 2009

DIABETES: The SIZE of The PROBLEM
4
09
165%
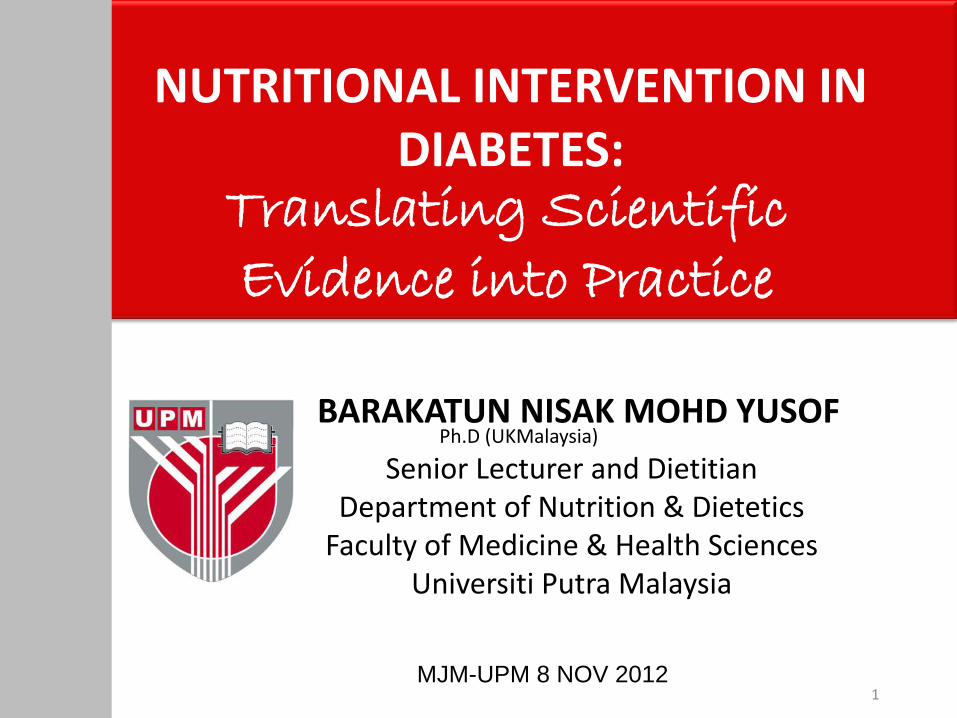
Common Presentations
1. Poor Glycemic Control
5
Proportion of patients achieving target HbA1c
Mafauzy et al. 2011 DiabCare 2008

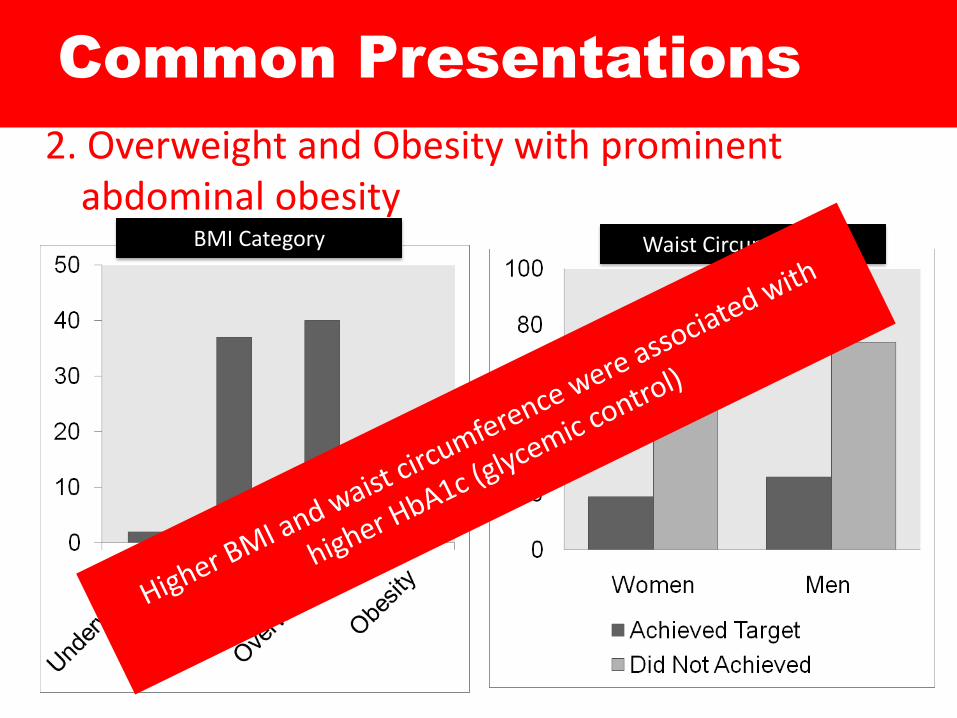
Common Presentations
2. Overweight and Obesity with prominent
abdominal obesity
6
BMI Category Waist Circumference
Barakatun Nisak et al 2009 - 2011

Collaborative Management
Diabetes Management
Nutrition Therapy
Physical Activity
Monitoring Blood Glucose
Medication – Insulin or oral
agents
7
+ Intensive
Education +
Self-
Management

Nutrition Intervention for the Management of Diabetes

DOES NUTRITION INTERVENTION REALLY HELP?
Ranging from 1-2% reduction in AIc 0.4% (p<0.05)
0.4kg (NS)
Barakatun Nisak et al. 2012

Patients’ Self Perception on
Treatment Adherence
10
Treatment Adherence +ve RESPONSES
Diet 85%
Exercise 57%
Taking medication as prescribed
96%
SMBG 52%
Come for appointments with HCP
97%
Mafauzy et al. 2011 DiabCare 2008

HOW MANY OF THEM WERE ACTUALLY
ADHERED TO THE TREATMENT?
11
55
39
27
87
3427
59
79
0
20
40
60
80
100
Diet Exercise SMBG Prescribed Mx (OAD)
2003 2008
Mafauzy et al. 2011 DiabCare 2008

Malaysian Diet
• We experience
more postprandial
hyperglycemia and
this could be due
to frequent
consumption of
high glycemic
index (GI) food (ie,
“glutinous”)
12
Country Fasting Postprandial
Indonesia 7.9 11.6
Bangladesh 8.4 8.6
Singapore 7.6 7.5
Malaysia 8 12.7
Taiwan 8 10.6
Thailand 7.9 11
Philippines 7.2 9.4
1. Mohamed M et al. Curr Med Res Opin 2008; 24: 507-514


Malaysian Style
75 – 90 g of CH0 (5-6 exch CHO)
1 exch = ½
cup of rice
OR 1pc
bread

Risk Reduction with 1% decline
in annual mean A1c
UKPDS 1998 15

Goals of Diabetes Management
16
• Achieve and maintain:
– Good Metabolic Control (Blood glucose, Lipid
profile, Blood pressure)
• Prevent or slow down complications of diabetes
• Individualized diets according to lifestyle and culture and willingness to change
• Limit food choices based on scientific evidence and maintain pleasure of eating
MNT MDA 2005
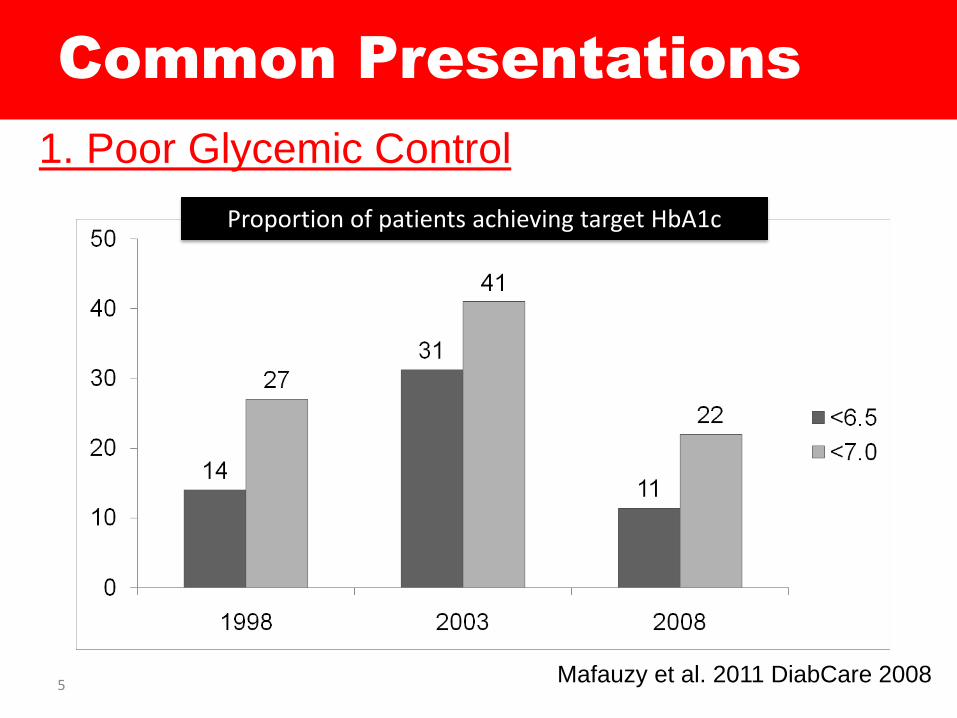
Diabetes and Cardiovascular Disease
• CVD: is a major cause of death in patient with DM1
• Independent risk factor –hyperglycemia2,3
(1) Node & Inoue 2009 Cardio Diab 8:23; (2) Nagakami et al.
2004 Diabetologia 47:385-394 (3) Huxley et al. 2006 BMJ 332:73-78
Cum
ula
tive I
ncid
ence o
f CVD
Mort
ality
0 2 6 4
CVD Mortality
DM
NGT
Barr EL, et al. Circulation. 2007;116:151–157
AusDiab = Australian Diabetes, Obesity, and Lifestyle Study
17

Achieving Good Metabolic Control thru Nutrition Intervention
• First Line Treatment-
Amount of carbohydrate (CHO exch or CHO counting) is the main option of treatment
18 MNT MDA 2005

CHO in Diabetes MNGT
• The component of diet that has the greatest influence on blood glucose
CARBOHYDRATE
*(85-94% variability of mean glc and insulin
responses)
• Carbohydrate has been the focus of management

First step of CHO recommendations
• Control the amount of carbohydrate

CHO prescription
• Carbohydrate should be consistently distributed throughout the day
• Avoid excessive intake at one
meal
• Distribute evenly through out
the day

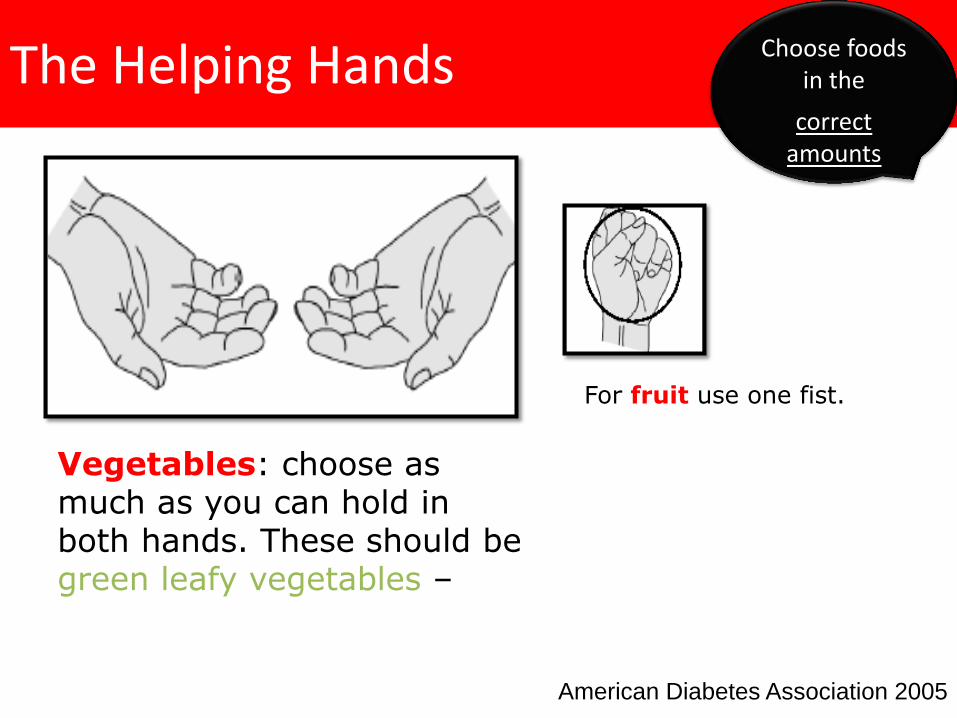
The Helping Hands
American Diabetes Association 2005
Choose foods in the
correct amounts
Starch Fat Protein
The Helping Hands
American Diabetes Association 2005
Choose foods in the
correct amounts
Vegetables: choose as much as you can hold in both hands. These should be green leafy vegetables –
For fruit use one fist.
Common Presentations
2. Overweight and Obesity with prominent abdominal obesity
24
BMI Category Waist Circumference

How to achieve reduce energy diet of 1200-
1500kcal/d?
1. Conventional reduced energy diet (Self-selected Diet)
2. Meal Replacements
25
Weight loss strategy
Overweight/Obesity
1.Physical activity consistent
with guidelines
2.Weight loss consistent with
guidelines
3.MNT consistent with
guidelines
4.Formula/Caloric
replacement consistent
with options and
strategies
5.Consider bariatric surgery

26
Malaysia – food heaven!

NUTRITION INTERVENTION AND WEIGHT LOSS?
0.4% (p<0.05)
0.4kg (NS)
Barakatun Nisak et al. 2012
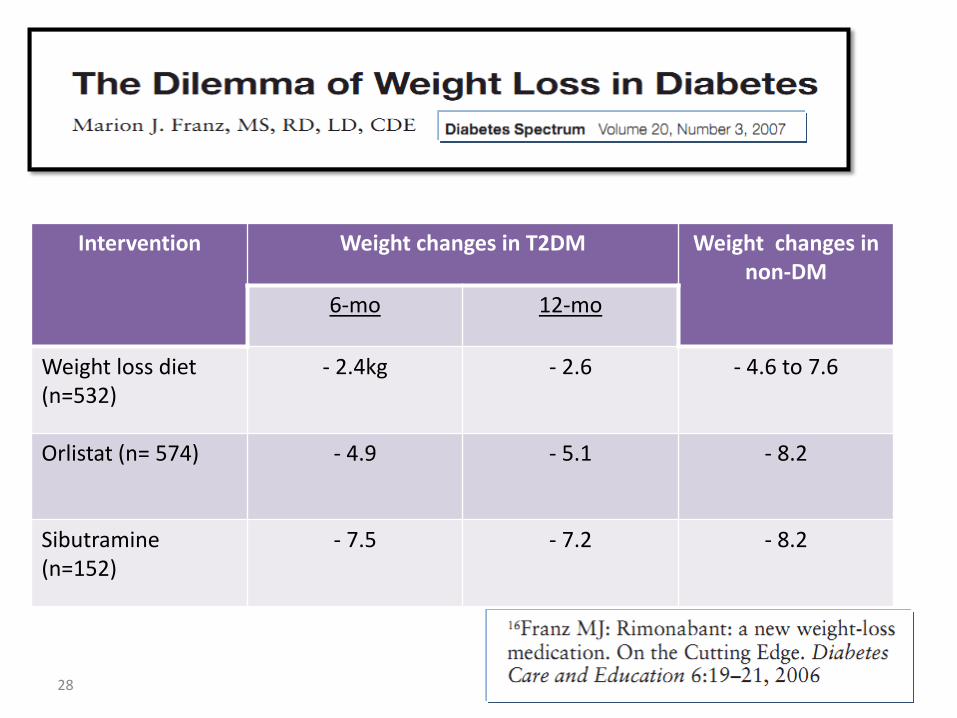
Intervention Weight changes in T2DM Weight changes in non-DM
6-mo 12-mo
Weight loss diet (n=532)
- 2.4kg - 2.6 - 4.6 to 7.6
Orlistat (n= 574) - 4.9 - 5.1 - 8.2
Sibutramine (n=152)
- 7.5 - 7.2 - 8.2
28

Wk 0
Wk 12
Wk 24
Schedule
Tatti P and Di Mauro P, 2010
Tatti P and Di Mauro P. Mediterr J Nutr Metab. 2010. In press.
Baseline
Weight, blood glucose, A1C, lipids and blood pressure
Weight, blood glucose, A1C, lipids and blood pressure
> 5% wt loss < 5% wt loss
Weight, blood glucose, A1C, lipids and blood pressure
Diabetes Meal
Replacement
Subjects Enrolled (n=96) and informed
consent obtained

30

31

Look AHEAD Trial
(Action for Health in Diabetes)
The Look AHEAD Research Group. Diabetes Care 2007. 30;6:1374-1383.
Objective To determine the effectiveness of intentional weight loss in reducing cardiovascular disease events in type 2 diabetes. 13.5 year follow up
Methods 5,145 men and women with type 2 diabetes who were 45 – 74 years of age and had a BMI ≥25kg/m²
Randomly assigned to Intensive Lifestyle Intervention (ILI) or a control condition, Diabetes Support and Education (DSE)
Weight loss goal of 10% (study goal = 7%)
Physical activity goal of 175 minutes per wk
Ongoing group and individual sessions
Portion-controlled diet including liquid meal replacements
Invited to three group sessions each year
Information on behavioral strategies presented but not implemented in sessions
Information focused on diet, physical activity, or social support
ILI Group included: DSE Group included:

33

34

35

What is Meal Replacement Program
(MRP)
• To help achieve reduced energy diet by controlling energy
and portion size.
• For people who have difficulty with self selection and/or
portion control, meal replacements (e.g., liquid meals,
meal bars, calorie-controlled packaged meals) may be
used as part of the diet component for a comprehensive
weight management program.
• Substituting one or two daily meals or snacks with meal
replacements is a successful weight loss and weight
maintenance strategy (Level A)
36
Ref : ADA Evidence Based Library 2011

WHAT FORMULA/
PRODUCTS TO USE IN
MRP?

Quick Guide of Selecting The Right MRP
38
Meal-Replacement Products for People with Diabetes
Quick Guide for Selecting the Right MRPs
Calories 190 to 250
For MRPs fewer than 200 calories, add an extra 15 to 20 grams of carbohydrates (about 100 calories) by including fat-free light yogurt,
low-fat whole-grain crackers, fresh fruit or fat-free milk. Raw or
cooked non-starchy vegetables (which are low in calories but contribute extra fiber, vitamins and minerals) may be eaten with any
of the MRPs.
Protein 10 to 15 grams Adequate protein promotes health and mealtime fullness.
Carbohydrate 14 to 34 grams
To slow the rate blood glucose (sugar) rises after a meal, look for the first carbohydrate listed in the ingredients to be maltodextrin or
tapioca dextrin rather than refined sugars, such as sucrose, corn
syrup, high-fructose corn syrup or brown rice syrup.
Dietary Fiber 3 to 6 grams
Total Fat 5 to 8 grams The primary fat source should be unsaturated fat from vegetable oils rather than saturated fat, such as partially hydrogenated oil, palm oil
or coconut oil. All MRPs should be trans-fat free.
Cholesterol 0 to 20 milligrams
Sodium 100 to 300 milligrams
Vitamins and Minerals
Look for 50 to 100 percent of the Dietary Reference Intake.
Avoid products containing stimulants, such as caffeine, ginseng, guarana and ephedra.
MRPs are effective for weight loss for a variety of reasons other than reducing calories. MRPs:
· Offer a structured calorie-controlled plan without having to count calories or choose what to eat for one or two meals and/ or one to two snacks a day
· Help establish a routine for eating meals and snacks at regular times · Help satisfy a craving for sweets (and help reduce the amount eaten), as many MRPs
have a sweet taste · Save time and require no preparation or refrigeration if unopened (Most fit easily into a
purse or briefcase for times when you cannot eat a regular meal.) · Save money when compared to many other commercial diet plans
"Use of meal replacements once or twice daily to replace a usual meal
can result in significant weight loss, but meal-replacement therapy must be continued if weight loss is
to be maintained."
- The American Diabetes Association
Meal-replacement products (MRPs) provide a meal or snack alternative for people with diabetes. MRPs may help:
· Stabilize blood glucose (sugar) levels · Assist with weight loss
MRPs include multi-flavored and ready-to-go drinks, powdered shakes, soups, bars, and puddings. Most are lactose and gluten-free and many offer non-nutritive sweeteners as replacements for some sugars. Adding regular aerobic exercise most days of the week will not only help with weight loss, but also help maintain a healthy weight long term. Ask your registered dietitian, diabetes educator or health care provider about using MRPs to optimize your health goals.
Eat Move Live A nutrition resource for living well with diabetes
Meal replacement products should provide at least 50-100% of the RNI for vitamins and minerals and low in fat and sodium. MNT 2012
Unpublished

MEAL REPLACEMENT
Characteristics Glycemic Targeted Products
Commercialized Low Calorie Diet
Energy /Serving 200-300 kcal/serving 80-160 kcal/serving
Protein 15-25% 25-40%
Carbohydrate 45-55% 50%
Fat 25-35% (MUFA) 15-20%
Fibre Added fibre (15g/serv) Nil - 3g
Vit/Mineral 50-100% Dietary Reference Intake
Products Liquid form and snack bar Liquid, milk shake, snack bar, soup
Glycemic Index LOW NA

Meal Replacement using Glycemia
Targeted Specialized Nutrition (GTSN)
• GTSN – diabetes specific formula
• Role of GTSN
– To provide proper nutrition (Complete Balance Meal)
(vs. Complete But Not Balance) – improve overall nutritional status
– To promote effective weight management suitably to patients with diabetes
– Maintained better glycemic control than standard formulas
40

LUNCH
TEA TIME BREAKFAST
DINNER
1200 kcal/day

Considerations before
starting MRP
• Patients should undergo at least 3 to 6 months of individualized conventional low calorie diet
42

Meal Replacement vs. Reduced Energy
Diet on Calories Intake/day
% c
han
ges i
n c
alo
ries i
nta
ke
Ditschuneit and Marion 2001; Obesity Research

Life examples..
• Without prior knowledge on self-selected diet of low caloric diet, may
– Promotion of eating disorder (Binge eating)
– Fostering poor eating habit
44

Considerations before
starting MRP
• Patients should undergo at least 3 to 6 months of individualized conventional low calorie diet
• MRPs as weight loss strategy are not recommended for persons with complications such as chronic kidney disease Stage 3 onwards, recent myocardial infarction and other severe complications.
• Risk of hypoglycemia should be assessed and monitored
45
Disadvantages of using MRP as part
of weight loss strategy
• Boredom with use of MRP over time
• Limitation of outcomes and evidence for ‘off the shelf’
– Research in MRP often involve provision of MRP products free of charge and ongoing support to develop their skills which are likely to increase their compliance
– There is a need to evaluate the real life outcomes of using MRP within our healthcare setting with limited resources and time that are usually evident
• Cost implication – May not be considered a viable option for lower SES groups
• Satiety Issues
46

INTENSIVE LIFESTLE DIABETES MANAGEMENT
Look AHEAD Trial
Intervention format Individual + Group
Frequency of Follow up for
the first 6 mo
4 /mo
Refresher Group/ campaigns 2-3 times/year after 2 years
Supervised activity Periodically in campaigns

P<0.001
Lifestyle Intervention Can Produce Long Term
Benefits: Results After 4 Year
Arch Intern Med. 2010;170(17):1566-1575
Some factors for success:
Ongoing intensive contact
Meal replacements
Diet and physical activity

MONITORING AND EVALUATION
• Individuals on meal replacements for weight loss should be followed-up by a dietitian within 1-3 mo.
• Dietitian should help to progress to low calorie diets for weight maintenance where appropriate. However, continued use of meal replacements may be needed to maintain weight (Grade A).
• Risk of hypoglycemia should be assessed and monitored.
49

Summary
• Nutrition Intervention is important in managing diabetes and delaying diabetes complications
• Nutrition Intervention: – Focus on the total amount of carbohydrate
– Avoid excessive portion size (dietary CHO)
– Consider Meal Replacement Program using Glycemic Targeted Specialized Nutrition
• Add exercise most days of the week
• Self-monitoring and frequent follow-ups 50

Summary
• More information is needed about
– Which patients do best with MRP approaches?
– How to integrate MRP within Malaysia health care and community setting?
• Individuals on MRP should be followed-up by a dietitian
51

Red vs green apple
15 g CHO 58 g CHO
Related Documents