NATURE REVIEWS | NEPHROLOGY VOLUME 8 | MARCH 2012 | 163 Division of Nephrology, Department of Internal Medicine, Yonsei University College of Medicine, 50 Yonsei-ro Seodaemun-gu, Seoul 120-752, Korea (S.‑H. Han, D.‑S. Han). Correspondence to: D.-S. Han [email protected] Nutrition in patients on peritoneal dialysis Seung-Hyeok Han and Dae-Suk Han Abstract | Protein–energy wasting (PEW) is prevalent among patients on dialysis and has emerged as an important risk factor for morbidity and mortality in these patients. Numerous factors, including inflammation, inadequate dialysis, insufficient nutrient intake, loss of protein during dialysis, chronic acidosis, hypercatabolic illness and comorbid conditions, are involved in the development of PEW. The causes and clinical features of PEW in patients on peritoneal dialysis and hemodialysis are comparable; assessment of the factors that lead to PEW in patients receiving peritoneal dialysis is important to ensure that PEW is managed correctly in these patients. For the past 20 years, much progress has been made in the prevention and treatment of PEW. However, the results of most nutritional intervention studies are inconclusive. In addition, the multifactorial and complicated pathogenesis of PEW makes it difficult to assess and treat. This Review summarizes the nutritional issues regarding the causes, assessment and treatment of PEW, with a focus on patients receiving peritoneal dialysis. In addition, an in-depth overview of the results of nutritional intervention studies is provided. Han, S.-H. & Han, D.-S. Nat. Rev. Nephrol. 8, 163–175 (2012); published online 7 February 2012; doi:10.1038/nrneph.2012.12 Introduction Dialysis is now established as a successful therapy for the management of patients with end-stage renal disease (ESRD). To further improve patient outcomes, much emphasis has focused on optimizing the adequacy of dialysis, managing blood pressure and anemia and maintaining biochemical parameters within the target range. When compared with these issues, however, the importance of protein–energy wasting (PEW) seems to be underestimated. Although much progress has been made in improving the nutritional status of patients, the prevalence of PEW in patients on dialysis remains high, ranging from 18% to 56%, depending on the assessment methods used. 1–5 Accumulating evidence indicates that PEW is an important predictor of morbidity and mortal- ity in patients on dialysis and impairs quality of life. 6–9 Constant monitoring of nutritional status and early detection, as well as therapeutic strategies for the preven- tion and treatment of PEW, are therefore crucial in the management of patients on dialysis. A number of tools are widely used in clinical practice for the assessment of PEW, yet no single method comprehensively reflects nutritional status, which should be cautiously assessed in combination with other clinical and biochemical para- meters. Of note, however, no data have convincingly demonstrated that improving PEW has a marked effect on morbidity or mortality of patients. The causes and features of PEW in patients on dialysis are similar between those on hemodialysis and perito- neal dialysis 10 and include inflammation, inadequate protein and calorie intake, loss of appetite, loss of resid- ual renal function (RRF), loss of protein during dialysis, psychosocial factors, physical inactivity and comorbid conditions. 11–14 Another important factor to note is that peritoneal dialysis itself could suppress appetite. 13,15 With these factors in mind, pertinent issues such as the causes, pathogenesis, assessment and treatment of PEW in patients on peritoneal dialysis are reviewed here. Nomenclature Malnutrition literally means ‘bad nutrition’ and is usually considered to entail undernutrition, which is character- ized by low food intake and a modest decrease in serum albumin levels; undernutrition can be corrected by increasing nutrient intake. In patients with ESRD, this form of malnutrition is sometimes termed ‘type 1 mal- nutrition’. 16 Another type of malnutrition also exists in which an inflammation-associated wasting process is involved. However, differentiating between these two types of malnutrition is difficult and the majority of patients on dialysis have both. To date, multiple terms have been used (often interchangeably and confusingly) to describe malnutrition in patients with ESRD, includ- ing uremic malnutrition, uremic cachexia, protein– energy malnutrition, malnutrition– inflammation atherosclerosis (MIA) syndrome and malnutrition– inflammation complex. Moreover, multiple conditions in patients with chronic kidney disease (CKD), such as inflammation, nutrient loss during dialysis, chronic acidosis, hypercatabolic illness, and endocrine dis- orders including resistance to insulin, growth hormone, and insulin-like growth factor (IGF)-I can cause loss of muscle mass despite adequate nutrient intake. 5,13 As the altered nutritional status associated with these condi- tions is not solely attributed to reduced nutrient intake, it cannot be corrected merely by increasing intake. To avoid confusion, the term PEW was proposed by a panel of experts from the International Society of Renal Competing interests The authors declare no competing interests. REVIEWS © 2012 Macmillan Publishers Limited. All rights reserved

Nutrition in patients on peritoneal dialysis.pdf
Nov 21, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
NATURE REVIEWS | NEPHROLOGY VOLUME 8 | MARCH 2012 | 163
Division of Nephrology, Department of Internal Medicine, Yonsei University College of Medicine, 50 Yonsei-ro Seodaemun-gu, Seoul 120-752, Korea (S.H.Han, D.S. Han).
Correspondence to: D.-S. Han [email protected]
Nutrition in patients on peritoneal dialysisSeung-Hyeok Han and Dae-Suk Han
Abstract | Proteinenergy wasting (PEW) is prevalent among patients on dialysis and has emerged as an important risk factor for morbidity and mortality in these patients. Numerous factors, including inflammation, inadequate dialysis, insufficient nutrient intake, loss of protein during dialysis, chronic acidosis, hypercatabolic illness and comorbid conditions, are involved in the development of PEW. The causes and clinical features of PEW in patients on peritoneal dialysis and hemodialysis are comparable; assessment of the factors that lead to PEW in patients receiving peritoneal dialysis is important to ensure that PEW is managed correctly in these patients. For the past 20years, much progress has been made in the prevention and treatment of PEW. However, the results of most nutritional intervention studies are inconclusive. In addition, the multifactorial and complicated pathogenesis of PEW makes it difficult to assess and treat. This Review summarizes the nutritional issues regarding the causes, assessment and treatment of PEW, with a focus on patients receiving peritoneal dialysis. In addition, an in-depth overview of the results of nutritional intervention studies is provided.
Han, S.-H. & Han, D.-S. Nat. Rev. Nephrol. 8, 163175 (2012); published online 7 February 2012; doi:10.1038/nrneph.2012.12
Introduction Dialysis is now established as a successful therapy for the management of patients with end-stage renal disease (ESRD). To further improve patient outcomes, much emphasis has focused on optimizing the adequacy of dialysis, managing blood pressure and anemia and maintaining biochemical parameters within the target range. When compared with these issues, however, the importance of proteinenergy wasting (PEW) seems to be underestimated. Although much progress has been made in improving the nutritional status of patients, the prevalence of PEW in patients on dialysis remains high, ranging from 18% to 56%, depending on the assessment methods used.15 Accumulating evidence indicates that PEW is an important predictor of morbidity and mortal-ity in patients on dialysis and impairs quality of life.69 Constant monitoring of nutritional status and early detection, as well as therapeutic strategies for the preven-tion and treatment of PEW, are therefore crucial in the management of patients on dialysis. A number of tools are widely used in clinical practice for the assessment of PEW, yet no single method comprehensively reflects nutritional status, which should be cautiously assessed in combination with other clinical and biochemical para-meters. Of note, however, no data have convincingly demonstrated that improving PEW has a marked effect on morbidity or mortality of patients.
The causes and features of PEW in patients on dialysis are similar between those on hemodialysis and perito-neal dialysis10 and include inflammation, inadequate protein and calorie intake, loss of appetite, loss of resid-ual renal function (RRF), loss of protein during dialysis, psychosocial factors, physical inactivity and comorbid
conditions.1114 Another important factor to note is that peritoneal dialysis itself could suppress appetite.13,15 With these factors in mind, pertinent issues such as the causes, pathogenesis, assessment and treatment of PEW in patients on peritoneal dialysis are reviewed here.
Nomenclature Malnutrition literally means bad nutrition and is usually considered to entail undernutrition, which is character-ized by low food intake and a modest decrease in serum albumin levels; undernutrition can be corrected by increasing nutrient intake. In patients with ESRD, this form of malnutrition is sometimes termed type1 mal-nutrition.16 Another type of malnutrition also exists in which an inflammation-associated wasting process is involved. However, differentiating between these two types of malnutrition is difficult and the majority of patients on dialysis have both. To date, multiple terms have been used (often interchangeably and confusingly) to describe malnutrition in patients with ESRD, includ-ing uremic malnutrition, uremic cachexia, proteinenergy malnutrition, malnutrition inflammation athero sclerosis (MIA) syndrome and malnutritioninflammation complex. Moreover, multiple conditions in patients with chronic kidney disease (CKD), such as inflammation, nutrient loss during dialysis, chronic acidosis, hypercatabolic illness, and endocrine dis-orders including resistance to insulin, growth hormone, and insulin-like growth factor (IGF)-I can cause loss of muscle mass despite adequate nutrient intake.5,13 As the altered nutritional status associated with these condi-tions is not solely attributed to reduced nutrient intake, it cannot be corrected merely by increasing intake.
To avoid confusion, the term PEW was proposed by a panel of experts from the International Society of Renal
Competing interestsThe authors declare no competing interests.
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
-
164 | MARCH 2012 | VOLUME 8 www.nature.com/nrneph
Nutrition and Metabolism (ISRNM),4 and is steadily gaining acceptance. According to the ISRNM, PEW is the state of decreased body stores of protein and energy fuels (that is, body protein and fat masses). PEW is character ized by markedly decreased serum albumin levels, the presence of inflammation and oxidative stress and greater levels of protein breakdown than synthesis. A reduced muscle mass seems to be the most valid cri-terion for the presence of PEW. In addition, the ISRNM panel recommends that cachexia is differentiated from PEW and used to denote a severe form of PEW, often associated with profound physiological, metabolic, psycho logical and immunological disorders.4 Based on the suggestion by the ISRNM panel, in this Review we use the term PEW instead of malnutrition to avoid prob-lems in interpretation when nutritional problems occur in patients with CKD.
Causes and pathogenesis of PEW Inflammation In patients with ESRD, inflammation is common and leads to atherosclerosis and arteriosclerosis, which eventually results in increased cardiovascular morbid ity and mortality. Moreover, elevated levels of C-reactive protein (a serum inflammatory marker) predicts mortal ity independently of other comorbidi-ties in patients on peritoneal dialysis.17 Inflammation, alone or in combination with other factors, also has a key role in the pathogenesis of PEW. Indeed, malnutri-tion (that is, PEW), inflammation and atherosclerosis coordinate together in a vicious cycle of so called MIA syndrome16 and have been associated with high rates of morbidity and mortality. In particular, the 2-year mortal ity rate increased up to 70% in patients who had all three components of MIA syndrome compared with approximately 10% or less in patients who had none of these components.18,19
Several mechanisms have been proposed to explain how inflammation is involved in PEW. First, pro-inflammatory cytokines could cause muscle wasting by
Key points
Proteinenergy wasting (PEW) is common and is an important risk factor for morbidity and mortality in patients on dialysis
Inflammation, inadequate dialysis, insufficient nutrient intake, loss of protein during dialysis, chronic acidosis, hypercatabolic illness, comorbid conditions, psychosocial factors and physical inactivity are involved in the development of PEW
Peritoneal dialysis itself might lead to PEW as continuous glucose absorption from peritoneal dialysis solutions, abdominal fullness induced by the dialysate and peritonitis can suppress appetite
No single test is precisely indicative of PEW; comprehensive diagnostic criteria for PEW proposed by the International Society of Renal Nutrition and Metabolism could be useful
A number of treatment options for PEW are available but improving nutritional status is difficult and no data have convincingly shown that nutritional intervention improves patient survival
A multidisciplinary approach to PEW management should be provided by providing nutritional assessment and support, dietary counseling, management of comorbid conditions, and by maintaining an adequate dialysis dose and preserving residual renal function
increasing protein hydrolysis and muscle-protein break-down through activation of the ubiquitinproteasome proteolytic pathway or nuclear factor B signaling.20 In addition, inflammation can suppress appetite and induce anorexia. In fact, elevated plasma levels of tumor necrosis factor were found in patients with anorexia on peritoneal dialysis compared with levels in patients without anorexia.21 Inflammation-associated anorexia was reported to be mediated by leptina hormone that suppresses appetite. Indeed, blocking leptin signal-ing through the hypothalamic melanocortin 4 recep-tor improved uremic cachexia in a mouse model.22 Furthermore, visfatin, a newly identified adipocyte-derived factor that is sensitive to inflammation, might also contribute to uremic anorexia.23
A second mechanism involves insulin resistance. Insulin is an anabolic hormone that exerts anticatabolic effects on skeletal muscle.24 Inflammatory cytokines disturb insulin signaling pathways, which results in decreased insulin sensitivity.25 This effect, in turn, might dampen the anabolic effect of insulin on skeletal muscle and cause loss of muscle mass. Indeed, insulin resistance correlated with muscle wasting in 21 patients on perito-neal dialysis,26 which suggests that insulin resistance is closely linked with PEW.
Other peritoneal dialysis-related factors that might cause inflammation include poor oral health, volume overload, peritonitis, and bioincompatible solutions;2729 of note, these factors (unlike those discussed above) are potentially reversible. In fact, when the uid status of 25 patients on peritoneal dialysis was well-controlled, nutri-tional status and inflammation were improved, whereas fluid overload resulted in worse nutritional status and promoted inflammation.28
Inadequate nutritional intake The Kidney Dialysis Outcomes Quality Initiative (KDOQI) guidelines recommend a daily energy intake of 35 kcal/kg for patients on peritoneal dialysis 60years and daily protein intake of 1.21.3 g/kg.30 However, a large proportion of patients on peritoneal dialysis ingest a considerably lower amount of calories and protein than the recommended amounts.31,32 Moreover, inadequate dietary protein intake (DPI) is associated with increased all-cause and cardiovascular mortality in these patients.9 Despite inadequate protein or energy intake, one study showed that glucose absorption from the dialysate can provide some energy33 and another study demonstrated that the nitrogen balance in the majority of patients on peritoneal dialysis is positive.34
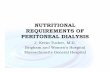
Nutrient intake by patients on dialysis can be influ-enced by many factors: inflammation, taste abnormali-ties, gastrointestinal problems, medications, physical inactivity, dietary restrictions, emotional and psycho-logical disorders and social constraints such as poverty (Figure1).3537 Factors that are specific to peritoneal dialysis might also be associated with poor oral intake as continuous absorption of glucose from peritoneal dialy-sis solutions15,38 and abdominal fullness induced by the
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
-
NATURE REVIEWS | NEPHROLOGY VOLUME 8 | MARCH 2012 | 165
dialysate13 can cause loss of appetite. Interestingly, gastric emptying was delayed in patients receiving peritoneal dialysis.39 However, whether this delay is attributed to dialysate dwell perse or to the absorption of substrate substances with caloric and metabolic activity such as glucose is uncertain.40
Ghrelin, a gut peptide that regulates hunger by stimu-lating neuropeptide Y and agouti-related peptide in the hypothalamus, has been identified as an appetite enhancer.41 Paradoxically, circulating ghrelin levels were increased in patients on dialysis when compared with levels in healthy controls,42 which suggests that these patients are resistant to ghrelin. Nevertheless, plasma ghrelin levels were markedly lower in anorexic patients on peritoneal dialysis than in those with normal appe-tite.43 Interestingly, as exchange with peritoneal dialysis solution lowers ghrelin levels,44 a reduced level of ghrelin might mediate this anorexic effect.
Bioincompatibility of peritoneal dialysis solu-tion might also influence appetite: in a rat model, a bicarbonate lactate solution suppressed appetite to a lesser extent than a lactate solution.45 No clinical evidence, however, exists to support this finding.
Loss of nutrients into dialysate Although waste products are cleared during dialy-sis treatment, nutrients are also lost into the dialysate. Patients on peritoneal dialysis lose approximately 912 g of total protein and 68 g of albumin daily.5,46 Loss of protein is much greater during an episode of perito-nitis.46 In particular, the type of peritoneal membrane transport might influence the amount of protein loss. In patients with a fast peritoneal solute transport rate (that is, high transporters), protein losses are consider-ably greater than in patients with a low solute transport rate.47 Relevant to this finding is our observation that a fast peritoneal solute transport rate is independently associated with poor nutritional status in patients on peritoneal dialysis.48 Fast peritoneal solute transport rates have also been associated with inflammation49 and mortality in some studies;50,51 however, other studies have found no association between peritoneal transport rate and nutritional status.52,53 Of note, high risk of adverse outcomes in high transporters was only observed in those on continuous ambulatory peritoneal dialysis; no relationship between peritoneal transport rate and either mortality or transfer to hemodialysis has been reported for patients receiving automated peritoneal dialysis.54,55 In addition, inherent fast transport (that is, when the patient has a fast solute transport rate from the start of peritoneal dialysis) and acquired fast transport (that is, when the transport rate increases with time on peritoneal dialysis) might have different clinical implications; inher-ent fast transport is associated with increased mortality because it is linked with greater levels of comorbidity and inflammation than acquired fast transport.56 Such discrepancy between findings regarding the relationship between peritoneal transport types and nutritional status can be explained by differences in study design, number of enrolled patients, patient characteristics, the
timing of evaluation of peritoneal transport type and nutritional assessments. Further investigations using more detailed methods such as the diagnostic criteria proposed by the ISRNM panel are required to delineate the association between peritoneal transport types and nutritional status.
Loss of residual renal function Over the past 20years, the importance of preserving RRF has been highlighted in many aspects of the management of patients on dialysis and low RRF is an independent risk factor for adverse outcomes in these patients.12,57 From a nutritional viewpoint, numerous reports have indicated that RRF is also important in determining nutritional status. In one study, preserved RRF was independently associated with a greater intake of dietary protein, calories and other nutrients, whereas peritoneal dialysis solute clearance was not.11 In addition, resting energy expenditure was found to be inversely correlated with RRF, which suggests that patients with decreased RRF have an altered protein metabolism.58 Furthermore, a number of studies have shown that patients with pre-served RRF have a better nutritional status, as deter-mined using different assessment methods such as lean body mass (LBM), normalized protein catabolic rate (nPCR), subjective global assessment (SGA) score, DPI, serum albumin level, and handgrip strength than patients who have low or no RRF.11,5961 Moreover, loss of RRF is associated with increased systemic inflam-mation.62 Given the importance of inflammation as a key mediator of muscle wasting and anorexia, loss of RRF can be presumed to contribute to PEW through exacerbated inflammation.
A decrease in middle molecule clearance is also clearly evident as RRF declines63 and this effect might adversely affect nutritional status. Whether increasing the removal of middle molecules improves nutritional status, however, remains to be further explored as their increased removal by high-flux dialysis failed to improve nPCR in patients on hemodialysis.64
Factors related to uremia Factors related to peritoneal dialysis
Inammation
Anorexia
Hypercatabolism
Chronic acidosis
Comorbid conditions:diabetes mellitus,
cardiovascular disease,infection
Inadequatenutrient intake
Inadequate dialysis
Loss of nutrientsinto dialysate
Appetite loss due toglucose absorption
from dialysate
Peritonitis
Bioincompatiblesolution?
Abdominal discomfortinduced by dialysate
Loss of residualrenal function
Proteinenergywasting
Figure 1 | The causes of proteinenergy wasting in patients on peritoneal dialysis.
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
-
166 | MARCH 2012 | VOLUME 8 www.nature.com/nrneph
Hypercatabolic statePatients with PEW on dialysis are characterized by a hypercatabolic state that is promoted by numerous factors including inflammation, negative protein and energy balance during dialysis, diabetic complications, concurrent infection or sepsis, comorbid conditions such as cardiovascular disease, acidosis and resistance to IGF-I and growth hormone.37
Possible mechanisms of acidosis-induced PEW are protein degradation, protein breakdown from skel-etal muscle and oxidation of branched-chain amino acids,65 a decrease in albumin synthesis,66 and reduced expression of IGF-I and growth hormone.67 Many cross-sectional studies have shown a direct relationship between the severity of metabolic acidosis and nutri-tional status in patients with CKD.68 We observed that patients on peritoneal dialysis with serum bicarbonate levels of 1820 mmol/l (associated with mild to mod-erate acidosis) had a favorable nutritional status.69,70 However, detailed analysis revealed that patients with severe metabolic acidosis (that is, serum bicarbonate levels
-
NATURE REVIEWS | NEPHROLOGY VOLUME 8 | MARCH 2012 | 167
sensitive marker of nutritional status than albumin. However, prealbumin can also be lost into dialysates and its levels in serum are higher in patients on peritoneal dialysis than in those on hemodialysispossibly owing to the increased hepatic synthesis in response to its peritoneal loss.76
Body mass Epidemiological studies indicate the presence of an obesity paradox (that is, a high BMI is associated with survival) in patients on maintenance dialysis.77 Indeed, in patients on hemodialysis and peritoneal dialysis, a low BMI is associated with an increased risk of mor-tality.78,79 However, BMI can be affected by fat mass or hydration status. In particular, peritoneal dialysis often leads to greater volume expansion than hemodialysis,80 which suggests that BMI might not be a useful parameter of nutritional status in patients on peritoneal dialysis. Interestingly, the survival advantage associated with a higher BMI is less apparent in patients on peritoneal dialysis than in those on hemodialysis.79,81 Furthermore, the majority of studies that show this obesity paradox in patients on dialysis were conducted in the USA. In fact, obesity was associated with worse outcomes in a study of patients on peritoneal dialysis in Australia and New Zealand;82 an analysis that pools patients on hemo dialysis and peritoneal dialysis might not, therefore, be appro-priate. Defining BMI as indicative of PEW in patients on peritoneal dialysis might need to be individualized depending on the patient population.
Muscle mass Muscle wasting is a key feature of PEW. In fact, a reduced muscle mass with high BMI (so-called sarcopenic obesity) was associated with inflammation and increased mortality in patients with ESRD, although the patients with these characteristics were indeed obese as assessed by BMI.83,84 Anthropometric assessment of mid-arm muscle circumference is commonly used to measure muscle mass. However, this method can be insensitive as it is associated with a substantial interobserver error and is affected by hydration status.13 As for BMI, interpreta-tion of parameters of muscle mass in patients on perito-neal dialysis should be made after a careful considera tion of fluid status.
Dietary intake Dietary intake as assessed by dietary diaries and inter-views, even when a dietitian is involved, can be subjec-tive and inaccurate. The accuracy of determining dietary intake depends on the reliability of patients to properly quantify the amount of food eaten.85 In fact, in a study of 40 patients on peritoneal dialysis, a significant number of patients (particularly those who were overweight) were found to under-report energy intake as evaluated by 3-day food diaries.86 In addition, estimation of DPI using a urea kinetic model can be unreliable in patients who are in anabolic or catabolic states and can be confounded by the concomitant loss of protein into, or energy intake from, the dialysate.85
The ISRNM panel recommended other potential tools for assessment of PEW that include scoring systems such as the SGA score and malnutritioninflammation scoreboth of which are widely used in clinical practice. However, the accuracy of these scoring systems depends on the examiner and considerable training is required to ensure consistent and steady results. In addition, no consensus has been reached on the relationship of these subjective assessments in the diagnosis of PEW.4
Prevention and treatment of PEW As PEW is multifactorial in origin, a single therapeutic strategy is unlikely to be successful. Although a number of treatment options are available, restoring normal nutritional status in patients with PEW on dialysis is difficult and no data exist that convincingly show that nutritional intervention improves patient survival. Here, we provide an overview of the management of PEW in patients on peritoneal dialysis.
Dialysis dose Accumulation of uremic toxin with CKD progression is associated with anorexia.87 In clinical practice, patients with anorexia commonly regain appetite after dialysis is initiated; however, whether increasing dialysis dose leads to better clinical outcomes is still debated. Observational studies have suggested a link between dialysis adequacy and nutritional status;8,11,88 however, although several prospective longitudinal studies have investigated whether increasing dialysis dose improves nutritional status in patients on peritoneal dialysis,8993 the results of these have been inconclusive and limited by short follow- up duration and small sample size. In one of these studies, an increase in dialysis-derived calories and cre-atinine appearance, as well as stabilization of weight and mid-arm circumference, was observed in malnourished patients after dialysis dose was increased.93 Objective measures of improvement, such as increased serum albumin level, were marked in patients without comorbid disease. By contrast, other studies found no improvement in either serum albumin level or normalized protein nitrogen appearance (nPNA) despite an increase in Kt/V.89,92 Moreover, secondary analyses of the Adequacy of Peritoneal Dialysis in Mexico (ADEMEX) trial94 and of an interventional study conducted in six centers in Hong Kong95 found no association between higher dialy-sis dose and improved nutritional status. To date, only one prospective, randomized study has investigated the link between dialysis dose and nutritional status; increas-ing Kt/V from 1.82 to 2.02 over 12months resulted in an increase in nPNA from 1.10 g/kg to 1.24 g/kg, whereas no improvement was observed in serum albumin level, SGA score, LBM or DPI.96 Interestingly, reports have suggested that the relationship between Kt/V and nPNA is not linear but reaches a plateau at a weekly Kt/V of approximately 1.8.9799 This finding is in line with the secondary analyses of the ADEMEX trial and Hong Kong study. Depending on the baseline dialy-sis dose, therefore, increasing the dialysis dose could improve nutritional status in some patients. However,
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
-
168 | MARCH 2012 | VOLUME 8 www.nature.com/nrneph
the effects of increments beyond a certain point seem to be attenuated.
If underdialysis is suspected in patients with anorexia and declining nutritional status on peritoneal dialysis, the dialysis dose should be increased to optimize dialy-sis adequacy. Alternatively, combined peritoneal dialysis and hemodialysis therapy might be helpful in improv-ing nutritional status. Indeed, nPNA, creatinine genera-tion rate and LBM significantly increased after adding a once weekly hemodialysis session to 56days per week of peritoneal dialysis regimen in patients affected by underdialysis or fluid overload.100
Preservation of RRFAs loss of RRF is associated with deterioration in nutri-tional status, preservation of RRF could be assumed to maintain nutritional status. Prospective, random-ized intervention studies are not feasible, however, as RRF declines over time. Moreover, RRF is influenced by many factors and cannot be easily manipulated. One study showed a marked decline in the nutritional status of patients on peritoneal dialysis who lost RRF.93 Furthermore, RRF had a considerable effect on nutri-tional status as nutritional intake was affected to a greater extent by RRF than by peritoneal dialysis solute clear-ance,11 which supports the findings from a previous study.101 Given the large contribution of RRF to nutri-tional status and patient outcome, various efforts to pre-serve RRF in patients on dialysis should be an essential part of PEW prevention strategies.
Dietary counselingIn patients on peritoneal dialysis, regular and compre-hensive assessments to identify factors that cause PEW are mandatory. Of note, only 39% of 266 patients on peri-toneal dialysis complied with a DPI of 1.2 g/kg per day as recommended by the KDOQI guidelines.102 Therefore, dietary counseling might be useful if inadequate nutri-tional intake is a problem. Indeed, a marked improve-ment in nutrient intake and in grades of malnutrition was observed in 283 patients on peritoneal dialysis after repeated dietary counseling.103 However, the results of two prospective studies were inconsistent with each other.104,105 In particular, a randomized, controlled trial that included 54 patients on peritoneal dialysis demon-strated that a substantial proportion of these patients were unable to increase protein and energy intake over 4 months, even though dietary advice was provided.105
Although DPI 1.21.3 g/kg per day is generally recom-mended for patients on peritoneal dialysis, the optimal target has not yet been determined. In fact, the European guidelines suggest a protein intake 1.0 g/kg per day106 and a study of Chinese patients on peritoneal dialysis showed that DPI >0.94 g/kg per day was associated with favorable nutritional status and long-term outcomes.9 Interestingly, both this study and the European guide-lines warned against lower DPIs of
-
NATURE REVIEWS | NEPHROLOGY VOLUME 8 | MARCH 2012 | 169
proteins into the dialysate.5,46 One exchange with a 1.1% amino acid solution can compensate for these losses and meet the nutritional requirements in patients on peri-toneal dialysis. A 6 h dwell time with a 1.1% amino acid solution enables approximately 16 g (7278%) of amino acids to be absorbed, which is greater than the peri-toneal loss of amino acids using conventional glucose solutions.123 Anabolic effects are also induced as muscle protein synthesis and IGF-I levels are increased, which reduces muscle protein breakdown.124 The results from some studies support the use of an amino acid-based dialysis solution in patients with PEW, as they have demonstrated improvement in several biochemical and anthropometric nutritional parameters and a positive nitrogen balance (Table2).125134 However, these find-ings are not consistent with those from other studies (Table3).135139 Our long-term observations, however, support the use of amino acid-based dialysis solutions, as daily use of an amino-acid based solution for 12 months resulted in significant increases in nutritional para-meters, including LBM, hand grip strength and nPNA in patients with PEW on peritoneal dialysis.134
Metabolic acidosis is a potential adverse effect of amino acid-based dialysis solutions.127 However, in agreement with previous studies,140 we observed that although bicarbonate levels decreased, levels of bicar-bonate remained within the normal range.134 To date, only two randomized clinical trials examined the effects of amino acid-based solutions on clinical outcomes or nutritional status in patients on peritoneal dialysis.130,133
Of these two studies, only one examined the mortality rate and showed that patient survival and incidence of peritonitis did not differ between patients receiv-ing amino acid-based solutions and those receiv-ing glucose-based solutions over a 3-year follow-up, although some nutritional parameters such as nPNA and DPI improved in the former group. The second study only examined changes in nutritional status.133 Interpretation of published data on the effects of amino acid-based solutions should therefore be made with caution because most studies that have demon-strated positive effects of amino acid-based solutions on outcomes have been small and observational, and it is therefore uncertain whether an amino acid-based solution confers a clinical benefit.
Hormonal treatmentsAs patients on dialysis are frequently hypercatabolic, stimulation of muscle protein anabolism is therefore an attractive therapeutic option to avoid muscle wasting. Anabolic hormones that have been tested include growth hormone, IGF-I and androgenic anabolic ste-roids (Table4). As mentioned earlier, altered growth hormoneIGF-I axis and growth hormone resistance are potential mechanisms for PEW in patients on dialysis; nearly all of the studies that have evaluated the nutri-tional effects of recombinant human growth hormone (rhGH) have demonstrated the anabolic effects of decreases in blood urea nitrogen levels and nPNA.141 These effects have been consistently observed in patients
Table 1 | Effects of oral supplements on nutritional status in patients on peritoneal dialysis
Study Study type Population Interventions Followup Results
Shimomura etal. (1993)109
Nonrandomized controlled
36 Supplement of 0.10.3 g protein per kg per day (n = 18); controls had no supplement (n = 18)
6months serum albumin, prealbumin, transferrin, plasma total amino acids, and the ratio of essential amino acids to nonessential amino acids
Heaf etal. (1999)110
No control group 14 Commercial supplement with 40 g protein per day
10weeks No change in serum albumin, DPI, calorie intake and nPNA
Eustace etal. (2000)111
Randomized double blind placebo-controlled
47 (18 on PD and 29 on HD)
Oral essential amino acid tablets vs placebo
3months No change in serum albumin level or grip strength; skinfold thickness
Aguirre Galindo etal. (2003)112
Randomized 100 High protein diet (1.4 g/kg per day) (n = 50) vs calcium caseinate diet (n = 50)
4months serum albumin level and total protein in both groups
Boudville etal. (2003)113
Single blind crossover 13 on PD Commercial supplement with 475 kcal and 16.6 g protein
ND serum albumin level, total calorie and protein intake
Teixid-Planas etal. (2005)114
Randomized controlled 75 Commercial supplement with 20 g of protein per day
12months No change in serum albumin level; high rate of noncompliance and intolerance to commercial protein supplement
Gonzlez-Espinoza etal. (2005)115
Randomized controlled 30 Egg albumin supplement with 30 g protein per day (n = 13); control (n = 15)
6months serum albumin, total calorie and protein intake, and nPNA
Poole and Hamad (2008)116
No control group 190 (157 on HD and 33 on PD)
2030 g protein and 500 kcal per day for nondiabetics; 13.8 g protein and 250 kcal per day for diabetics
3months serum albumin (HD only); no significant improvement in PD
Moretti etal. (2009)117
Randomized crossover 49 (6 on PD and 43 on HD)
PD: 105 g protein per week; HD: 45 g protein per week
12months No change nPCR and serum albumin level in protein supplemented group; nPCR and serum albumin level in controls
Abbreviations: DPI, dietary protein intake; HD, hemodialysis; ND, not determined; nPNA, normalized protein nitrogen appearance; nPCR, normalized protein catabolic rate; PD, peritoneal dialysis.
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
-
170 | MARCH 2012 | VOLUME 8 www.nature.com/nrneph
on peritoneal dialysis.142145 Our work has also shown that rhGH treatment improves nitrogen balance and increases LBM in malnourished patients on peritoneal dialysis.143 Another possible anabolic treatment is IGF-I, which differs from growth hormone in that it is antilipo-lytic and reduces serum glucose levels. However, clinical trials using recombinant IGF-I (rIGF-I) are scarce. Only one pilot study in six patients with PEW on peritoneal dialysis has shown that rIGF-I treatment resulted in a positive nitrogen balance.146
Similar to growth hormone and IGF-1, androgenic anabolic steroids also induce net muscle protein synthe-sis and inhibit protein catabolic processes.141 Although most studies on androgen treatment for PEW have been conducted in patients on hemodialysis, positive effects on nutritional parameters have been reported in those on peritoneal dialysis.147149 In a double-blind, random-ized controlled trial, treatment of patients on perito-neal dialysis with oxymetholone for 6months resulted in a significant increase in serum albumin levels and
Table 3 | Studies showing neutral effects of 1.1% amino acid-based solution in patients on peritoneal dialysis
Study Study type Population Interventions Followup (months)
Results
Young etal. (1989)135
Case series 8 One exchange of 1.1% amino acid-based solution
3 No change in serum albumin or prealbumin; no change in serum bicarbonate; transferrin
Dombros etal. (1990)136
Case series 5 One exchange of 1.1% amino acid-based solution
6 No change in serum albumin, transferrin, DPI, DEI and skinfold thickness; no change in serum bicarbonate
Dibble etal. (1990)137
Case series 8 One exchange of 1.1% amino acid-based solution
3 No change in total energy intake, MAMC and skinfold thickness
Maurer et al. (1996)138
Randomized controlled
18 One or two exchanges of a 1.1% amino acid-based solution (n = 9); control (n = 9)
6 No change in serum albumin, transferrin, and LBM; no change in serum bicarbonate
Grzegorzewska etal. (1999)139
Case series 16 One exchange of 1.1% amino acid-based solution with antacid (n = 8); control (n = 8)
6 No change in serum albumin, LBM, skinfold thickness, DPI and DEI; no change in serum bicarbonate
Abbreviations: DEI, dietary energy intake; DPI, dietary protein intake; LBM, lean body mass; MAMC, mid-arm muscle circumference.
Table 2 | Studies showing positive effects of 1.1% amino acid-based solution in patients on peritoneal dialysis
Study Study type Population Interventions Followup Result
Bruno etal. (1989)125
Crossover 6 One exchange of a 1.1% amino acid-based solution
6months nitrogen balance and MAMC; serum bicarbonate
Arfeen etal. (1990)126
Case series 7 Two exchanges of a 1.1% amino acid-based solution
2months serum albumin; serum bicarbonate
Kopple etal. (1995)127
Case series 19 12 exchanges of a 1.1% amino acid-based solution
20days nitrogen balance, BUN and transferrin; serum bicarbonate
Faller etal. (1995)128
Case series 15 One exchange of a 1.1% amino acid-based solution
3months serum albumin, BUN and transferrin; no change in serum bicarbonate
Chertow etal. (1995)129
Observational 183 One exchange of a 1.1% amino acid-based solution
Mean 6.6months serum albumin; no change in serum bicarbonate
Misra etal. (1996)130
Randomized crossover
18 One exchange of a 1.1% amino acid-based solution
6months Improved nutrition score; no change in serum albumin and transferrin; serum albumin in patients with baseline albumin
-
NATURE REVIEWS | NEPHROLOGY VOLUME 8 | MARCH 2012 | 171
LBM.150 However, the long-term efficacy and risk of adverse effects have not yet been determined in patients with ESRD.
The role of ghrelin as an appetite enhancer is currently being investigated.151 To date, only two studiesboth of randomized, double-blind, crossover design and per-formed by the same grouphave explored the effects of ghrelin in patients on dialysis. A single subcutane-ous injection of ghrelin resulted in a substantial increase in energy intake when compared with a placebo in nine patients with PEW on peritoneal dialysis.152 These find-ings were subsequently confirmed using daily ghrelin administration for an extended period of 7days in 12 patients on dialysis.153 Ghrelin therefore seems to directly target appetite regulation, and is a potential treatment for patients with PEW on peritoneal dialysis.
Correction of acidosisA small study of seven patients on peritoneal dialysis showed a decrease in protein degradation with correc-tion of acidosis.154 In a randomized, single-blind study, correction of metabolic acidosis led to increases in body weight and mid-arm circumference in the first year of
continuous ambulatory peritoneal dialysis.155 Using a similar protocol, another study also showed that the bene ficial effects of acidosis correction on nutri-tional status were mediated by the downregulation of branched-chain amino acid degradation and muscle proteo lysis via the ubiquitinproteasome system.156 In addition, another randomized controlled trial showed that treatment with oral sodium bicarbonate for 12months resulted in increases in SGA score and nPNA in patients on peritoneal dialysis with acidosis and Kt/V
-
172 | MARCH 2012 | VOLUME 8 www.nature.com/nrneph
ConclusionsImproving the poor nutritional status of patients with PEW on peritoneal dialysis is difficult owing to the multi factorial and complicated pathogenesis of this disease. Early identification is key to rehabilitating these malnourished patients and avoiding poor outcomes. Thus, a multidisciplinary approach should be provided through careful nutritional assessment, dietary counsel-ing and proper nutritional support (Box2). In addition, management of psychological illnesses and comorbid conditions should not be ignored. Accurate monitoring and evaluation of inflammation is of paramount impor-tance given the fact that inflammation is a key mediator of PEW. However, a paucity of data are available con-cerning the effect of anti-inflammatory therapies on nutritional status.
In patients on peritoneal dialysis, factors specific to peritoneal dialysis should also be considered. In particular, preservation of RRF should be empha-sized because reduced RRF adversely affects not only morbidity and mortality but also nutritional status. Prevention of peritonitis is also important as recur-rent peritonitis impairs appetite and nutritional status. Adequate nutritional support should be provided that considers the inadequate calorie and protein intake in patients on peritoneal dialysis as well as the substan-tial protein loss into the dialysate. In this regard, it is tempting to use amino acid-based dialysis solutions to compensate for protein loss although no data has con-vincingly shown that these solutions improve patient survival. Unfortunately, most nutritional intervention trials that have evaluated the efficacy of oral supple-ments or hormonal treatments are inconclusive. These studies have not been well controlled and are limited by short follow-up duration and small sample sizes. In addition, some crucial safety issues have not been resolved. Given the paucity of data demonstrating that nutritional intervention improves clinical outcomes, long-term prospective, randomized, controlled trials are required to clarify the beneficial effects of nutri-tional therapies in patients with PEW. In the meantime, maintenance of good nutritional status and treatment of PEW with currently available therapies should be an essential strategy in the management of patients on peritoneal dialysis.
Box 2 | Management of PEW in peritoneal dialysis
General management Maintain adequate dialysis dose Correct acidosis Manage comorbid or catabolic conditions Dietary counseling Encourage adequate food intake:
Daily energy intake 35 kcal/kg of body weight for patients 60yearsProtein intake 1.21.3 g/kg body weight per day* Oral nutritional supplements
Peritoneal dialysisrelated therapies Preserve residual renal function Prevent and treat peritonitis Maintain optimal fluid balance Utilize amino acid-based solutions Use biocompatible solutions
Potential therapies Appetite stimulants Hormonal treatments (growth hormone; insulin-like
growth factor I; anabolic steroids; ghrelin) Anti-inflammatory treatment
*1.0 g/kg body weight per day can be acceptable unless there is evidence of declining nutritional status. Abbreviation: PEW, proteinenergy wasting.
Review criteria
The PubMed database was searched for English-language articles published up to 31st August 2011, with no set earliest date of publication. The majority were full-text papers. The search terms used were malnutrition, proteinenergy wasting, peritoneal dialysis, inflammation, residual renal function, appetite, peritoneal membrane transport, dialysis dose, inadequate dialysis dietary intake, dietary counseling, oral supplement, acidosis, amino acid peritoneal dialysis solution, growth hormone, androgen and megesterol acetate.
1. Kang, D.H., Kang, E.W., Choi, S.R., Yoon, S.Y. & Han, D.S. Nutritional problems of Asian peritoneal dialysis patients. Perit. Dial. Int. 23(Suppl. 2), S58S64 (2003).
2. Cianciaruso, B. etal. Cross-sectional comparison of malnutrition in continuous ambulatory peritoneal dialysis and hemodialysis patients. Am. J. Kidney Dis. 26, 475486 (1995).
3. Young, G.A. etal. Nutritional assessment of continuous ambulatory peritoneal dialysis patients: an international study. Am. J. Kidney Dis. 17, 462471 (1991).
4. Fouque, D. etal. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 73, 391398 (2008).
5. Dukkipati, R. & Kopple, J.D. Causes and prevention of protein-energy wasting in chronic kidney failure. Semin. Nephrol. 29, 3949 (2009).
6. Kopple, J.D. Effect of nutrition on morbidity and mortality in maintenance dialysis patients. Am. J. Kidney Dis. 24, 10021009 (1994).
7. Bergstrom, J. Nutrition and mortality in hemodialysis. J. Am. Soc. Nephrol. 6, 13291341 (1995).
8. Adequacy of dialysis and nutrition in continuous peritoneal dialysis: association with clinical outcomes. Canada-USA (CANUSA) Peritoneal Dialysis Study Group. J. Am. Soc. Nephrol. 7, 198207 (1996).
9. Dong, J., Li, Y., Xu, Y. & Xu, R. Daily protein intake and survival in patients on peritoneal dialysis. Nephrol. Dial. Transplant. 26, 37153721 (2011).
10. Bergstrom, J. Why are dialysis patients malnourished? Am. J. Kidney Dis. 26, 229241 (1995).
11. Wang, A.Y. etal. Independent effects of residual renal function and dialysis adequacy on actual dietary protein, calorie, and other nutrient intake
in patients on continuous ambulatory peritoneal dialysis. J. Am. Soc. Nephrol. 12, 24502457 (2001).
12. Wang, A.Y. & Lai, K.N. The importance of residual renal function in dialysis patients. Kidney Int. 69, 17261732 (2006).
13. Chung, S.H., Stenvinkel, P., Lindholm, B. & Avesani, C.M. Identifying and managing malnutrition stemming from different causes. Perit. Dial. Int. 27 (Suppl. 2), S239S244 (2007).
14. Bossola, M. etal. Malnutrition in hemodialysis patients: what therapy? Am. J. Kidney Dis. 46, 371386 (2005).
15. Chung, S.H., Carrero, J.J. & Lindholm, B. Causes of poor appetite in patients on peritoneal dialysis. J. Ren. Nutr. 21, 1215 (2011).
16. Stenvinkel, P., Heimburger, O., Lindholm, B., Kaysen, G.A. & Bergstrom, J. Are there two types of malnutrition in chronic renal failure?
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
-
NATURE REVIEWS | NEPHROLOGY VOLUME 8 | MARCH 2012 | 173
Evidence for relationships between malnutrition, inflammation and atherosclerosis (MIA syndrome). Nephrol. Dial. Transplant. 15, 953960 (2000).
17. Noh, H. etal. Serum C-reactive protein: a predictor of mortality in continuous ambulatory peritoneal dialysis patients. Perit. Dial. Int. 18, 387394 (1998).
18. Stenvinkel, P., Chung, S.H., Heimburger, O. & Lindholm, B. Malnutrition, inflammation, and atherosclerosis in peritoneal dialysis patients. Perit. Dial. Int. 21 (Suppl. 3), S157S162 (2001).
19. de Mutsert, R. etal. Excess mortality due to interaction between protein-energy wasting, inflammation and cardiovascular disease in chronic dialysis patients. Nephrol. Dial. Transplant. 23, 29572964 (2008).
20. Mitch, W.E., Du, J., Bailey, J.L. & Price, S.R. Mechanisms causing muscle proteolysis in uremia: the influence of insulin and cytokines. Miner. Electrolyte Metab. 25, 216219 (1999).
21. Aguilera, A. etal. Anorexigen (TNF-alpha, cholecystokinin) and orexigen (neuropeptide Y) plasma levels in peritoneal dialysis (PD) patients: their relationship with nutritional parameters. Nephrol. Dial. Transplant. 13, 14761483 (1998).
22. Mak, R.H., Cheung, W., Cone, R.D. & Marks,D.L. Leptin and inflammation-associated cachexia in chronic kidney disease. Kidney Int. 69, 794797 (2006).
23. Carrero, J.J. etal. Visfatin is increased in chronic kidney disease patients with poor appetite and correlates negatively with fasting serum amino acids and triglyceride levels. Nephrol. Dial. Transplant. 25, 901906 (2010).
24. Price, S.R. etal. Muscle wasting in insulinopenic rats results from activation of the ATP-dependent, ubiquitin-proteasome proteolytic pathway by a mechanism including gene transcription. J. Clin. Invest. 98, 17031708 (1996).
25. Wellen, K.E. & Hotamisligil, G.S. Inflammation, stress, and diabetes. J. Clin. Invest. 115, 11111119 (2005).
26. Lee, S.W., Park, G.H., Song, J.H., Hong, K.C. & Kim, M.J. Insulin resistance and muscle wasting in non-diabetic end-stage renal disease patients. Nephrol. Dial. Transplant. 22, 25542562 (2007).
27. Bayraktar, G. etal. Oral health and inflammation in patients with end-stage renal failure. Perit. Dial. Int. 29, 472479 (2009).
28. Cheng, L.T., Tang, W. & Wang, T. Strong association between volume status and nutritional status in peritoneal dialysis patients. Am. J. Kidney Dis. 45, 891902 (2005).
29. Lai, K.N. & Leung, J.C. Inflammation in peritoneal dialysis. Nephron Clin. Pract. 116, c11c18 (2010).
30. Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am. J. Kidney Dis. 35 (Suppl. 2), S1140 (2000).
31. Wang, A.Y. etal. Nutrient intake during peritoneal dialysis at the Prince of Wales Hospital in Hong Kong. Am. J. Kidney Dis. 49, 682692 (2007).
32. Lindholm, B., Wang, T., Heimburger, O. & Bergstrom, J. Influence of different treatments and schedules on the factors conditioning the nutritional status in dialysis patients. Nephrol. Dial. Transplant. 13 (Suppl. 6), 6673 (1998).
33. Bazanelli, A.P. etal. Resting energy expenditure in peritoneal dialysis patients. Perit. Dial. Int. 26, 697704 (2006).
34. Bergstrom, J., Furst, P., Alvestrand, A. & Lindholm, B. Protein and energy intake, nitrogen balance and nitrogen losses in patients treated with continuous ambulatory peritoneal dialysis. Kidney Int. 44, 10481057 (1993).
35. Carrero, J.J. etal. Appetite disorders in uremia. J. Ren. Nutr. 18, 107113 (2008).
36. Aguilera, A. etal. Gastrointestinal and pancreatic function in peritoneal dialysis patients: their relationship with malnutrition and peritoneal membrane abnormalities. Am. J. Kidney Dis. 42, 787796 (2003).
37. Kalantar-Zadeh, K., Ikizler, T.A., Block, G., Avram,M.M. & Kopple, J.D. Malnutrition-inflammation complex syndrome in dialysis patients: causes and consequences. Am. J. Kidney Dis. 42, 864881 (2003).
38. Zheng, Z.H. etal. Acute effects of peritoneal dialysis solutions on appetite in non-uremic rats. Kidney Int. 60, 23922398 (2001).
39. Stompor, T. etal. Association between gastric emptying rate and nutritional status in patients treated with continuous ambulatory peritoneal dialysis. Perit. Dial. Int. 22, 500505 (2002).
40. Van, V. etal. Influence of dialysate on gastric emptying time in peritoneal dialysis patients. Perit. Dial. Int. 22, 3238 (2002).
41. Cummings, D.E. etal. A preprandial rise in plasma ghrelin levels suggests a role in meal initiation in humans. Diabetes 50, 17141719 (2001).
42. Perez-Fontan, M. etal. Plasma ghrelin levels in patients undergoing haemodialysis and peritoneal dialysis. Nephrol. Dial. Transplant. 19, 20952100 (2004).
43. Aguilera, A. etal. Ghrelin plasma levels and appetite in peritoneal dialysis patients. Adv. Perit. Dial. 20, 194199 (2004).
44. Perez-Fontan, M. etal. Acute plasma ghrelin and leptin responses to oral feeding or intraperitoneal hypertonic glucose-based dialysate in patients with chronic renal failure. Kidney Int. 68, 28772885 (2005).
45. Zheng, Z.H. etal. Bicarbonate-based peritoneal dialysis solution has less effect on ingestive behavior than lactate-based peritoneal dialysis solution. Perit. Dial. Int. 29, 656663 (2009).
46. Blumenkrantz, M.J. etal. Protein losses during peritoneal dialysis. Kidney Int. 19, 593602 (1981).
47. Kathuria, P. etal. Effect of dialysis modality and membrane transport characteristics on dialysate protein losses of patients on peritoneal dialysis. Perit. Dial. Int. 17, 449454 (1997).
48. Kang, D.H. etal. Relationship of peritoneal membrane transport characteristics to the nutritional status in CAPD patients. Nephrol. Dial. Transplant. 14, 17151722 (1999).
49. Pecoits-Filho, R. etal. Plasma and dialysate IL-6 and VEGF concentrations are associated with high peritoneal solute transport rate. Nephrol. Dial. Transplant. 17, 14801486 (2002).
50. Churchill, D.N. etal. Increased peritoneal membrane transport is associated with decreased patient and technique survival for continuous peritoneal dialysis patients. The Canada-USA (CANUSA) Peritoneal Dialysis Study Group. J. Am. Soc. Nephrol. 9, 12851292 (1998).
51. Rumpsfeld, M., McDonald, S.P. & Johnson, D.W. Higher peritoneal transport status is associated with higher mortality and technique failure in the Australian and New Zealand peritoneal dialysis patient populations. J. Am. Soc. Nephrol. 17, 271278 (2006).
52. Cueto-Manzano, A.M., Espinosa, A., Hernandez,A. & Correa-Rotter, R. Peritoneal transport kinetics correlate with serum albumin
but not with the overall nutritional status in CAPD patients. Am. J. Kidney Dis. 30, 229236 (1997).
53. Szeto, C.C., Law, M.C., Wong, T.Y., Leung, C.B. & Li, P.K. Peritoneal transport status correlates with morbidity but not longitudinal change of nutritional status of continuous ambulatory peritoneal dialysis patients: a 2-year prospective study. Am. J. Kidney Dis. 37, 329336 (2001).
54. Brimble, K.S., Walker, M., Margetts, P.J., Kundhal, K.K. & Rabbat, C.G. Meta-analysis: peritoneal membrane transport, mortality, and technique failure in peritoneal dialysis. J. Am. Soc. Nephrol. 17, 25912598 (2006).
55. Johnson, D.W. etal. Superior survival of high transporters treated with automated versus continuous ambulatory peritoneal dialysis. Nephrol. Dial. Transplant. 25, 19731979 (2010).
56. Chung, S.H., Heimburger, O. & Lindholm, B. Poor outcomes for fast transporters on PD: the rise and fall of a clinical concern. Semin. Dial. 21, 710 (2008).
57. Shemin, D., Bostom, A.G., Laliberty, P. & Dworkin, L.D. Residual renal function and mortality risk in hemodialysis patients. Am. J. Kidney Dis. 38, 8590 (2001).
58. Wang, A.Y. etal. Resting energy expenditure and subsequent mortality risk in peritoneal dialysis patients. J. Am. Soc. Nephrol. 15, 31343143 (2004).
59. Szeto, C.C. etal. Independent effects of residual renal function and dialysis adequacy on nutritional status and patient outcome in continuous ambulatory peritoneal dialysis. Am. J. Kidney Dis. 34, 10561064 (1999).
60. Suda, T. etal. The contribution of residual renal function to overall nutritional status in chronic haemodialysis patients. Nephrol. Dial. Transplant. 15, 396401 (2000).
61. Wang, A.Y. etal. Evaluation of handgrip strength as a nutritional marker and prognostic indicator in peritoneal dialysis patients. Am. J. Clin. Nutr. 81, 7986 (2005).
62. Pecoits-Filho, R. etal. Associations between circulating inflammatory markers and residual renal function in CRF patients. Am. J. Kidney Dis. 41, 12121218 (2003).
63. Bammens, B., Evenepoel, P., Verbeke, K. & Vanrenterghem, Y. Time profiles of peritoneal and renal clearances of different uremic solutes in incident peritoneal dialysis patients. Am. J. Kidney Dis. 46, 512519 (2005).
64. Marcus, R.G., Cohl, E. & Uribarri, J. Middle molecule clearance does not influence protein intake in hemodialysis patients. Am. J. Kidney Dis. 31, 491494 (1998).
65. Bailey, J.L. etal. The acidosis of chronic renal failure activates muscle proteolysis in rats by augmenting transcription of genes encoding proteins of the ATP-dependent ubiquitin-proteasome pathway. J. Clin. Invest. 97, 14471453 (1996).
66. Ballmer, P.E. etal. Chronic metabolic acidosis decreases albumin synthesis and induces negative nitrogen balance in humans. J. Clin. Invest. 95, 3945 (1995).
67. Brungger, M., Hulter, H.N. & Krapf, R. Effect of chronic metabolic acidosis on the growth hormone/IGF-1 endocrine axis: new cause of growth hormone insensitivity in humans. Kidney Int. 51, 216221 (1997).
68. Chiu, Y.W., Kopple, J.D. & Mehrotra, R. Correction of metabolic acidosis to ameliorate wasting in chronic kidney disease: goals and strategies. Semin. Nephrol. 29, 6774 (2009).
69. Kang, S.W. etal. Impact of metabolic acidosis on serum albumin and other nutritional
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
-
174 | MARCH 2012 | VOLUME 8 www.nature.com/nrneph
parameters in long-term CAPD patients. Adv. Perit. Dial. 13, 249252 (1997).
70. Kang, D.H. etal. Metabolic acidosis and composite nutritional index (CNI) in CAPD patients. Clin. Nephrol. 53, 124131 (2000).
71. Blake, P.G. Growth hormone and malnutrition in dialysis patients. Perit. Dial. Int. 15, 210216 (1995).
72. Fryburg, D.A., Gelfand, R.A. & Barrett, E.J. Growth hormone acutely stimulates forearm muscle protein synthesis in normal humans. Am. J. Physiol. 260, E499E504 (1991).
73. Spiegel, D.M. & Breyer, J.A. Serum albumin: a predictor of long-term outcome in peritoneal dialysis patients. Am. J. Kidney Dis. 23, 283285 (1994).
74. Han, S.H. etal. Improving outcome of CAPD: twenty-five years experience in a single Korean center. Perit. Dial. Int. 27, 432440 (2007).
75. Han, D.S. etal. Factors affecting low values of serum albumin in CAPD patients. Adv. Perit. Dial. 12, 288292 (1996).
76. Goldwasser, P., Feldman, J.G. & Barth, R.H. Serum prealbumin is higher in peritoneal dialysis than in hemodialysis: a meta-analysis. Kidney Int. 62, 276281 (2002).
77. Kalantar-Zadeh, K. & Kopple, J.D. Obesity paradox in patients on maintenance dialysis. Contrib. Nephrol. 151, 5769 (2006).
78. Snyder, J.J., Foley, R.N., Gilbertson, D.T., Vonesh,E.F. & Collins, A.J. Body size and outcomes on peritoneal dialysis in the United States. Kidney Int. 64, 18381844 (2003).
79. Stack, A.G., Murthy, B.V. & Molony, D.A. Survival differences between peritoneal dialysis and hemodialysis among large ESRD patients in the United States. Kidney Int. 65, 23982408 (2004).
80. Enia, G. etal. Long-term CAPD patients are volume expanded and display more severe left ventricular hypertrophy than haemodialysis patients. Nephrol. Dial. Transplant. 16, 14591464 (2001).
81. Abbott, K.C. etal. Body mass index and peritoneal dialysis: exceptions to the exception in reverse epidemiology? Semin. Dial. 20, 561565 (2007).
82. McDonald, S.P., Collins, J.F. & Johnson, D.W. Obesity is associated with worse peritoneal dialysis outcomes in the Australia and New Zealand patient populations. J. Am. Soc. Nephrol. 14, 28942901 (2003).
83. Honda, H. etal. Obese sarcopenia in patients with end-stage renal disease is associated with inflammation and increased mortality. Am. J. Clin. Nutr. 86, 633638 (2007).
84. Ramkumar, N., Pappas, L.M. & Beddhu, S. Effect of body size and body composition on survival in peritoneal dialysis patients. Perit. Dial. Int. 25, 461469 (2005).
85. Bargman, J.M. The rationale and ultimate limitations of urea kinetic modelling in the estimation of nutritional status. Perit. Dial. Int. 16, 347351 (1996).
86. Bazanelli, A.P., Kamimura, M.A., Vasselai, P., Draibe, S.A. & Cuppari, L. Underreporting of energy intake in peritoneal dialysis patients. J.Ren. Nutr. 20, 263269 (2010).
87. Bergstrom, J. Mechanisms of uremic suppression of appetite. J. Ren. Nutr. 9, 129132 (1999).
88. Fung, L. etal. Dialysis adequacy and nutrition determine prognosis in continuous ambulatory peritoneal dialysis patients. J. Am. Soc. Nephrol. 7, 737744 (1996).
89. Williams, P., Jones, J. & Marriott, J. Do increases in dialysis dose in CAPD patients lead to nutritional improvements? Nephrol. Dial. Transplant. 9, 18411842 (1994).
90. Lynn, R.I., Fishbane, S. & Ginsberg, N.S. The effect of KT/V(urea) on nitrogen appearance and appetite in peritoneal dialysis. Perit. Dial. Int. 15(Suppl. 5), S50S52 (1995).
91. Malhotra, D. etal. Serum albumin in continuous peritoneal dialysis: its predictors and relationship to urea clearance. Kidney Int. 50, 243249 (1996).
92. Harty, J., Boulton, H., Faragher, B., Venning, M. & Gokal, R. The influence of small solute clearance on dietary protein intake in continuous ambulatory peritoneal dialysis patients: a methodologic analysis based on cross-sectional and prospective studies. Am. J. Kidney Dis. 28, 553560 (1996).
93. Davies, S.J., Phillips, L., Griffiths, A.M., Naish,P.F. & Russell, G.I. Analysis of the effects of increasing delivered dialysis treatment to malnourished peritoneal dialysis patients. Kidney Int. 57, 17431754 (2000).
94. Paniagua, R. etal. Effects of increased peritoneal clearances on mortality rates in peritoneal dialysis: ADEMEX, a prospective, randomized, controlled trial. J. Am. Soc. Nephrol. 13, 13071320 (2002).
95. Lo, W.K. etal. Effect of Kt/V on survival and clinical outcome in CAPD patients in a randomized prospective study. Kidney Int. 64, 649656 (2003).
96. Mak, S.K. etal. Randomized prospective study of the effect of increased dialytic dose on nutritional and clinical outcome in continuous ambulatory peritoneal dialysis patients. Am. J. Kidney Dis. 36, 105114 (2000).
97. Nolph, K.D. etal. A new approach to optimizing urea clearances in hemodialysis and continuous ambulatory peritoneal dialysis. ASAIO J. 41, M446M451 (1995).
98. Ronco, C. Adequacy of peritoneal dialysis is more than Kt/V. Nephrol. Dial. Transplant. 12 (Suppl. 1), 6873 (1997).
99. Oreopoulos, D.G. The optimization of continuous ambulatory peritoneal dialysis. Kidney Int. 55, 11311149 (1999).
100. Kawanishi, H., Moriishi, M. & Tsuchiya, S. Evaluation of dialysis dose during combination therapy with peritoneal dialysis and hemodialysis. Adv. Perit. Dial. 23, 135139 (2007).
101. Bargman, J.M., Thorpe, K.E. & Churchill, D.N. Relative contribution of residual renal function and peritoneal clearance to adequacy of dialysis: a reanalysis of the CANUSA study. J. Am. Soc. Nephrol. 12, 21582162 (2001).
102. Wang, A.Y. etal. Important factors other than dialysis adequacy associated with inadequate dietary protein and energy intakes in patients receiving maintenance peritoneal dialysis. Am. J. Clin. Nutr. 77, 834841 (2003).
103. Prasad, N. etal. Changes in nutritional status on follow-up of an incident cohort of continuous ambulatory peritoneal dialysis patients. J. Ren. Nutr. 18, 195201 (2008).
104. Martin-Del-Campo, F. etal. Conventional nutritional counselling maintains nutritional status of patients on continuous ambulatory peritoneal dialysis in spite of systemic inflammation and decrease of residual renal function. Nephrology (Carlton) 14, 493498 (2009).
105. Sutton, D., Higgins, B. & Stevens, J.M. Continuous ambulatory peritoneal dialysis patients are unable to increase dietary intake to recommended levels. J. Ren. Nutr. 17, 329335 (2007).
106. Dombros, N. etal. European best practice guidelines for peritoneal dialysis. 8 Nutrition in peritoneal dialysis. Nephrol. Dial. Transplant. 20(Suppl. 9), ix28ix33 (2005).
107. Blumenkrantz, M.J., Kopple, J.D., Moran, J.K. & Coburn, J.W. Metabolic balance studies and dietary protein requirements in patients undergoing continuous ambulatory peritoneal dialysis. Kidney Int. 21, 849861 (1982).
108. Fouque, D., Pelletier, S., Mafra, D. & Chauveau, P. Nutrition and chronic kidney disease. Kidney Int. 80, 348357 (2011).
109. Shimomura, A., Tahara, D. & Azekura, H. Nutritional improvement in elderly CAPD patients with additional high protein foods. Adv. Perit. Dial. 9, 8086 (1993).
110. Heaf, J.G., Honore, K., Valeur, D. & Randlov, A. The effect of oral protein supplements on the nutritional status of malnourished CAPD patients. Perit. Dial. Int. 19, 7881 (1999).
111. Eustace, J.A. etal. Randomized double-blind trial of oral essential amino acids for dialysis-associated hypoalbuminemia. Kidney Int. 57, 25272538 (2000).
112. Aguirre Galindo, B.A. etal. Effect of polymeric diets in patients on continuous ambulatory peritoneal dialysis. Perit. Dial. Int. 23, 434439 (2003).
113. Boudville, N., Rangan, A. & Moody, H. Oral nutritional supplementation increases caloric and protein intake in peritoneal dialysis patients. Am. J. Kidney Dis. 41, 658663 (2003).
114. Teixido-Planas, J. etal. Oral protein-energy supplements in peritoneal dialysis: a multicenter study. Perit. Dial. Int. 25, 163172 (2005).
115. Gonzalez-Espinoza, L. etal. Randomized, open label, controlled clinical trial of oral administration of an egg albumin-based protein supplement to patients on continuous ambulatory peritoneal dialysis. Perit. Dial. Int. 25, 173180 (2005).
116. Poole, R. & Hamad, A. Nutrition supplements in dialysis patients: use in peritoneal dialysis patients and diabetic patients. Adv. Perit. Dial. 24, 118124 (2008).
117. Moretti, H.D., Johnson, A.M. & Keeling-Hathaway, T.J. Effects of protein supplementation in chronic hemodialysis and peritoneal dialysis patients. J. Ren. Nutr. 19, 298303 (2009).
118. Inui, A. Cancer anorexia-cachexia syndrome: current issues in research and management. CA Cancer J. Clin. 52, 7291 (2002).
119. Lien, Y.H. & Ruffenach, S.J. Low dose megestrol increases serum albumin in malnourished dialysis patients. Int. J. Artif. Organs 19, 147150 (1996).
120. Costero, O. etal. Treatment of anorexia and malnutrition in peritoneal dialysis patients with megestrol acetate. Adv. Perit. Dial. 20, 209212 (2004).
121. Golebiewska, J. etal. Influence of megestrol acetate on nutrition and inflammation in dialysis patients - preliminary results. Acta Biochim. Pol. 56, 733737 (2009).
122. Boccanfuso, J.A., Hutton, M. & McAllister, B. The effects of megestrol acetate on nutritional parameters in a dialysis population. J. Ren. Nutr. 10, 3643 (2000).
123. Park, M.S. etal. Peritoneal transport during dialysis with amino acid-based solutions. Perit. Dial. Int. 13, 280288 (1993).
124. Garibotto, G. etal. Acute effects of peritoneal dialysis with dialysates containing dextrose or dextrose and amino acids on muscle protein turnover in patients with chronic renal failure. J.Am. Soc. Nephrol. 12, 557567 (2001).
125. Bruno, M. etal. CAPD with an amino acid dialysis solution: a long-term, cross-over study. Kidney Int. 35, 11891194 (1989).
126. Arfeen, S., Goodship, T.H., Kirkwood, A. & Ward,M.K. The nutritional/metabolic and
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
-
NATURE REVIEWS | NEPHROLOGY VOLUME 8 | MARCH 2012 | 175
hormonal effects of 8weeks of continuous ambulatory peritoneal dialysis with a 1% amino acid solution. Clin. Nephrol. 33, 192199 (1990).
127. Kopple, J.D. etal. Treatment of malnourished CAPD patients with an amino acid based dialysate. Kidney Int. 47, 11481157 (1995).
128. Faller, B. etal. Clinical evaluation of an optimized 1.1% amino-acid solution for peritoneal dialysis. Nephrol. Dial. Transplant. 10, 14321437 (1995).
129. Chertow, G.M. etal. Laboratory surrogates of nutritional status after administration of intraperitoneal amino acid-based solutions in ambulatory peritoneal dialysis patients. J. Ren. Nutr. 3, 116123 (1995).
130. Misra, M., Ashworth, J., Reaveley, D.A., Muller,B. & Brown, E.A. Nutritional effects of amino acid dialysate (Nutrineal) in CAPD patients. Adv. Perit. Dial. 12, 311314 (1996).
131. Jones, M. etal. Treatment of malnutrition with 1.1% amino acid peritoneal dialysis solution: results of a multicenter outpatient study. Am. J. Kidney Dis. 32, 761769 (1998).
132. Taylor, G.S., Patel, V., Spencer, S., Fluck, R.J. & McIntyre, C.W. Long-term use of 1.1% amino acid dialysis solution in hypoalbuminemic continuous ambulatory peritoneal dialysis patients. Clin. Nephrol. 58, 445450 (2002).
133. Li, F.K. etal. A 3-year, prospective, randomized, controlled study on amino acid dialysate in patients on CAPD. Am. J. Kidney Dis. 42, 173183 (2003).
134. Park, M.S. etal. New insight of amino acid-based dialysis solutions. Kidney Int. Suppl. 103, S110S114 (2006).
135. Young, G.A. etal. The use of an amino-acid-based CAPD fluid over 12weeks. Nephrol. Dial. Transplant. 4, 285292 (1989).
136. Dombros, N.V. etal. Six-month overnight intraperitoneal amino-acid infusion in continuous ambulatory peritoneal dialysis (CAPD) patientsno effect on nutritional status. Perit. Dial. Int. 10, 7984 (1990).
137. Dibble, J.B., Young, G.A., Hobson, S.M. & Brownjohn, A.M. Amino-acid-based continuous ambulatory peritoneal dialysis (CAPD) fluid over twelve weeks: effects on carbohydrate and lipid metabolism. Perit. Dial. Int. 10, 7177 (1990).
138. Maurer, O. etal. Six-month overnight administration of intraperitoneal amino acids does not improve lean mass. Clin. Nephrol. 45, 303309 (1996).
139. Grzegorzewska, A.E., Mariak, I., Dobrowolska-Zachwieja, A. & Szajdak, L. Effects of amino acid dialysis solution on the nutrition of continuous ambulatory peritoneal dialysis patients. Perit. Dial. Int. 19, 462470 (1999).
140. Tjiong, H.L. etal. Dialysate as food: combined amino acid and glucose dialysate improves protein anabolism in renal failure patients on automated peritoneal dialysis. J. Am. Soc. Nephrol. 16, 14861493 (2005).
141. Fouque, D., Guebre-Egziabher, F. & Laville, M. Advances in anabolic interventions for malnourished dialysis patients. J. Ren. Nutr. 13, 161165 (2003).
142. Ikizler, T.A. etal. Short-term effects of recombinant human growth hormone in CAPD patients. Kidney Int. 46, 11781183 (1994).
143. Kang, D.H. etal. Recombinant human growth hormone improved nutritional status of undernourished adult CAPD patients. J. Am. Soc. Nephrol. 5, 494 (1994).
144. Ikizler, T.A. etal. Effects of recombinant human growth hormone on plasma and dialysate amino acid profiles in CAPD patients. Kidney Int. 50, 229234 (1996).
145. Iglesias, P. etal. Recombinant human growth hormone therapy in malnourished dialysis patients: a randomized controlled study. Am. J. Kidney Dis. 32, 454463 (1998).
146. Fouque, D., Peng, S.C., Shamir, E. & Kopple,J.D. Recombinant human insulin-like growth factor-1 induces an anabolic response in malnourished CAPD patients. Kidney Int. 57, 646654 (2000).
147. Dombros, N.V., Digenis, G.E., Soliman, G. & Oreopoulos, D.G. Anabolic steroids in the treatment of malnourished CAPD patients: a retrospective study. Perit. Dial. Int. 14, 344347 (1994).
148. Johansen, K.L., Mulligan, K. & Schambelan, M. Anabolic effects of nandrolone decanoate in patients receiving dialysis: a randomized controlled trial. JAMA 281, 12751281 (1999).
149. Navarro, J.F., Mora, C., Macia, M. & Garcia, J. Randomized prospective comparison between
erythropoietin and androgens in CAPD patients. Kidney Int. 61, 15371544 (2002).
150. Aramwit, P., Palapinyo, S., Wiwatniwong, S. & Supasyndh, O. The efficacy of oxymetholone in combination with erythropoietin on hematologic parameters and muscle mass in CAPD patients. Int. J. Clin. Pharmacol. Ther. 48, 803813 (2010).
151. Wren, A.M. etal. Ghrelin enhances appetite and increases food intake in humans. J. Clin. Endocrinol. Metab. 86, 5992 (2001).
152. Wynne, K. etal. Subcutaneous ghrelin enhances acute food intake in malnourished patients who receive maintenance peritoneal dialysis: a randomized, placebo-controlled trial. J. Am. Soc. Nephrol. 16, 21112118 (2005).
153. Ashby, D.R. etal. Sustained appetite improvement in malnourished dialysis patients by daily ghrelin treatment. Kidney Int. 76, 199206 (2009).
154. Graham, K.A. etal. Correction of acidosis in CAPD decreases whole body protein degradation. Kidney Int. 49, 13961400 (1996).
155. Stein, A. etal. Role of an improvement in acid-base status and nutrition in CAPD patients. Kidney Int. 52, 10891095 (1997).
156. Pickering, W.P. etal. Nutrition in CAPD: serum bicarbonate and the ubiquitin-proteasome system in muscle. Kidney Int. 61, 12861292 (2002).
157. Szeto, C.C., Wong, T.Y., Chow, K.M., Leung,C.B. & Li, P.K. Oral sodium bicarbonate for the treatment of metabolic acidosis in peritoneal dialysis patients: a randomized placebo-control trial. J. Am. Soc. Nephrol. 14, 21192126 (2003).
158. Montenegro, J. etal. Long-term clinical experience with pure bicarbonate peritoneal dialysis solutions. Perit. Dial. Int. 26, 8994 (2006).
159. Mehrotra, R. etal. Effect of high-normal compared with low-normal arterial pH on protein balances in automated peritoneal dialysis patients. Am. J. Clin. Nutr. 90, 15321540 (2009).
Author contributionsAll authors contributed equally to all aspects of the article.
REVIEWS
2012 Macmillan Publishers Limited. All rights reserved
Nutrition in patients on peritoneal dialysisSeung-Hyeok Han and Dae-Suk HanIntroduction Nomenclature Key pointsCauses and pathogenesis of PEW Figure 1 | The causes of proteinenergy wasting in patients on peritoneal dialysis.Box 1 | ISRNM criteria for diagnosis of PEW in patients with ESRDAssessment of nutritional status Prevention and treatment of PEW Box 2 | Management of PEW in peritoneal dialysis Review criteriaConclusionsAuthor contributions
Related Documents