Nursing Care of Clients with Neurologic Disorders

Nursing Care of Clients with Neurologic Disorders.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Nursing Care of Clients with Neurologic Disorders

Client with Alzheimer’s Disease
• Form of dementia characterized by progressive, irreversible deterioration of general intellectual functioning
• Begins with memory loss, initially subtle until progresses to being more noticeable; course includes deteriorating cognition and judgment with eventual physical decline and total inability to perform ADL
Risk factors
• older age
• female
• family history
• Exact cause is unknown; theories include loss of transmitter stimulation, genetic defects, viral and autoimmune cases

Warning signs include
• Memory loss affecting ability to function in job
• Difficulty with familiar tasks
• Problems with language, abstract thinking
• Disorientation, changes in mood and personality

Types and Changes in brain
• Familial (follows inheritance pattern) and sporadic
• Early-onset (<65)
• Older-onset (>65)
• Progressive brain atrophy

پاتولوژی فیزیو
های • لب در بویژه فراگیر و شدید بطور مغز قشر آتروفی. آهیانه – و پیشانی گیجگاهی
مغز • سوم بطن و طرفی های بطن شدن بزرگآن • های شیار شدن گشاد و مخ قشر های شکنج شدن باریک• - شکل تغییر و اندازه شدن کم و عصبی های کاهشسلول
مانده باقی ی ها نورونسلولی • برون پیری های پالکسلولی • درون فیبریلی نورو های کالفهعروقی • آمیلوئید رسوبات

• - و هیپوکامپ مخ قشر در بیشتر پیری های پالکبنام پپتید نوع یک از غالبا آیند می پدید ها آمیگدال
پروتئین بتا . A P ) آمیلوئید اند( شده تشکیلدر پروتئین این پیشساز سنتز مسئول ژن
. 21کروموزوم بر افزون ها پالک این دارد قراررسوبات مانند دیگر اجزای دارای فوق ماده
یافته شکل تغییر نوروگلی های سلول و آلومینیومزوائد و سلولی جسم تخریب در احتماال که هستند
. دارند. نقش ها نورون پالسمی سیتو

Manifestations : Stage I
• Appears healthy and alert
• Cognitive deficits are undetected
• Subtle memory lapses, personality changes
• Seems restless, forgetful, uncoordinated
Stage II • Memory deficits more apparent• Less able to behave spontaneously• Wandering behavior, deterioration in orientation to time
and place• Changes in sleeping patterns, agitation, stress• Trouble with simple decisions• Sundowning: increased agitation, wandering, disorientation
in afternoon and evening hours• Echolalia, scanning speech, total aphasia at times, apraxia,
astereognosis, inability to write• Becomes frustrated and depressed

Stage III
• Increasing dependence with inability to communicate, loss of continence
• Progressive loss of cognitive abilities, falls, delusion, paranoid reactions
• Average life expectancy is 7 years from diagnosis to death, often from pneumonia, secondary to aspiration



Collaborative Care
• No cure
• Supportive care for client and family

Diagnostic Tests
• Diagnosis by ruling out other conditions including depression, hypothyroidism, infection, stroke
• EEG shows slow pattern in later stages of disease• MRI and CT scan: shrinkage of hippocampus• Positron emission tomography (PET):visualizes
brain activity and interactions• Folstein Mini-Mental Status: instrument reflecting
loss of memory and cognitive skills
Medications Cholinesterase inhibitors used to treat mild to
moderate dementia• Tacrine hydrochloride (Cognex)• Donepezil hydrochloride (Aricept)• Rivastigmine (Exelon)• Medications to treat depressions• Tranquilizers for severe agitation• Thioridazine (Mellaril)• Haloperidol (Haldol)• Antioxidants: vitamin E, anti-inflammatory
agents, estrogen replacement therapy in women

The mechanism of action of acetylcholinesterase Cholinergic nerve transmission is terminated by the enzyme acetylcholinesterase (AchE). AchE is found
both on the post-synaptic membrane of cholinergic synapses and in other tissues eg red blood cells. Acetylcholine (Ach) binds to AchE and is hydrolysed to acetate and choline. This inactivates the Ach and
the nerve impulse is halted. AchE inhibitors (eg rivastigmine) prevent the hydrolysis of Ach, which increases the concentration of Ach in the synaptic cleft; AchE inhibitors are widely used in the treatment
of Alzheimer’s disease
• Rivastigmine

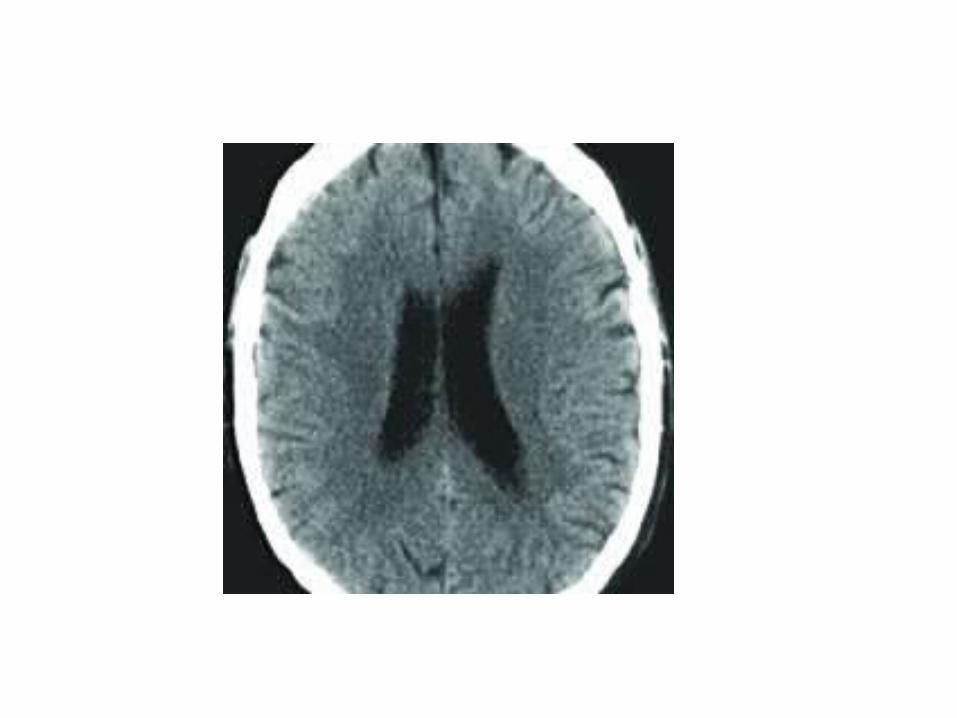
Case 1 - Normal CT Scan:Normal CT scan
The scan below is a slice through the human brain and you should imagine that you are viewing it as if looking up from the patient's feet. Therefore, the patient's left is to the right of
the screen. The shape of the ventricles is quite distinctive and they are shown outlined in green and orange. The presence of the third ventricle in the midline is one of the first things to look for. If the third ventricle is either not visible, or shows signs of shift away from the
midline, this suggests that there is an abnormality. The basal cisterns is the fluid filled space around the back of the midbrain outlined here in purple. Blood clots, or swelling of the brain
may cause this to become narrowed, or not visible altogether. Note in this scan, that the frontal horns of the lateral ventricles are symmetrical, with the septum between them in the
midline.

Acute Subdural Haematoma This CT scan shows a right sided acute haematoma, as well as an associated cerebral contusion (bruising). The true midline has been outlined by yellow dots and you can see that the frontal horns of the lateral ventricles have been pushed over to the left. In addition, the third ventricle is now not visible and it is also extremely difficult to make out the basal cisterns. This scan demonstrates four of the features which are included on the Early Outcome Form, namely midline shift greater than 5mm, intracranial haematoma - non evacuated, cortical contusion greater than 1cm in diameter and obliteration of the third ventricle. This haematoma requires surgical evacuation, otherwise deterioration of the patient's condition is inevitable.

Acute Subdural Haematoma The left lateral ventricle has been compressed and the midline is deviating to the right. The right lateral ventricle is actually slightly larger than normal and this is because the increased pressure is preventing escape of the cerebrospinal fluid from that ventricle. Dilatation of the contralateral ventricle like this indicates that there is very significant pressure on the brain.
This scan would be classified as "Intracranial haematoma”.
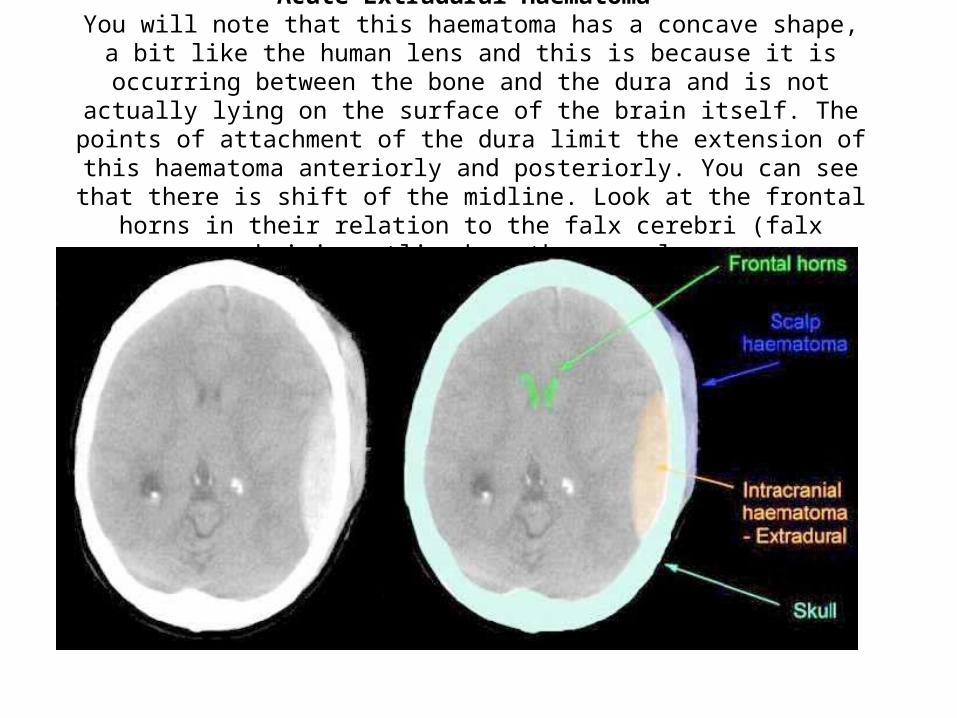
Acute Extradural Haematoma You will note that this haematoma has a concave shape, a bit like the human lens
and this is because it is occurring between the bone and the dura and is not actually lying on the surface of the brain itself. The points of attachment of the
dura limit the extension of this haematoma anteriorly and posteriorly. You can see that there is shift of the midline. Look at the frontal horns in their relation to the
falx cerebri (falx cerebri is outlined on the normal scan

Diffuse Axonal Injury The presence of petechial haemorrhages is usually an indication of a very severe primary
brain injury. Petechial haemorrhages tend to occur at the interface of grey and white matter. It can also occur in the dorsolateral quadrant of the midbrain at the middle orange arrow, as
well as elsewhere within the brain substance. Note on this scan, that the lateral ventricles and the third ventricle are visible and there is no midline shift. It is often a characteristic of
diffuse axonal injury, in which there are numerous petechial haemorrhages that there is no evidence of brain swelling, or midline shift. This scan would be classified as showing one, or
more, petechial haemorrhages within the brain.

Cerebral Contusion:Cortical contusion >1cm in diameter
This is a scan of a patient who has sustained a severe head injury. There is extensive bruising of the right side of the brain, showing up as a large, diffuse grey area. You can also see that there are patches of white
within the grey area. This represents bleeding. The grey area represents swelling (oedema). The area of the cortical contusion is outlined in purple. You will normally find a centimetre scale at the right hand side of a CT scan. This scan would be classified on the Early Outcome Form as "Cortical contusion -
greater than 1cm in diameter.

Complementary Therapy
• Massage, herbs, ginko biloba, Coenzyme Q10
• Art therapy, music, dance

معبد درخت

Nursing Care &Health Promotion
• Intensive, supportive nursing interventions directed at physical and psychosocial responses to illness
• Maintain functional abilities
• Maintain safety of client and caregiver

Nursing Diagnoses • Impaired Memory
• Include written or verbal reminders
• Use cues to deal with memory loss
• Chronic Confusion
• Anxiety
• Hopelessness
• Caregiver Role Strain

Home Care
• Education regarding disease, anticipation of needs, use of memory cues, support groups and peer counseling
• Refer to home health agencies, family support, group support

Client with Multiple Sclerosis • Description• Chronic demyelinating disease of CNS associated with
abnormal immune response to environmental factor• Initial onset followed by total remission making diagnosis
difficult• Most persons have disease with periods of exacerbations
and remissions• Progression of disease with increasing loss of function• Incidence is highest in young adults (20 – 40); onset
between 20 – 50• Affects females more than males• More common in temperate climates
• Occurs mainly in Caucasians

Pathophysiology • Autoimmune response to prior viral infection
• Inflammation destroys myelin leading to axon dysfunction
• Myelin sheaths of white matter of spinal cord, brain, optic nerve destroyed in patches called plaques
• Demyelination slows and distorts nerve conduction resulting in absence of impulse transmission
• Neurons in spinal cord, brain stem, cerebrum, cerebellum, and optic nerve affected
• Recurrent demyelination and plaque formation result in scarring of glia and degeneration of axons
• Disease follows different courses, most common is the relapsing-remitting type
• Stressors trigger MS: febrile states, pregnancy, physical exertion and fatigue; and these also can trigger relapses
Manifestations • Fatigue• Optic nerve involvement: blurred vision, haziness• Brain stem involvement: nystagmus, dysarthria
(scanning speech), cognitive dysfunctions, vertigo, deafness
• Weakness, numbness in leg(s), spastic paresis, bladder and bowel dysfunction
• Cerebellar: nystagmus, ataxia, hyptonia• Blindness

Collaborative Care
Focus is on retaining optimum functioning, limiting disability

Diagnostic Tests • Neurological exam, careful history
• Lumbar puncture with CSF analysis: increased number of T lymphocytes; elevated level of immunoglobulin G (IgG)
• Cerebral, spinal optic nerve MRI: shows multifocal lesions
• CT scan of brain: changes
• PET: measures brain activity
• Evoked response testing of visual, auditory, somatosensory impulses show delayed conduction

Medications
• ACTH
• Glucocorticosteroids
• Immunosuppressants: azathioprine (Imuran), cyclophosphamide (Cytoxan)
• Cychophosphamide
• Antispasmodics to treat muscle spasms
• Medications to deal with bladder problems: anticholinergics or cholinergics depending on problem experienced by client
Rehabilitation
• Physical therapy to maintain abilities and deal with spasticity

Nursing Care
• Education and support of client dealing with chronic disease with unpredictable course
Health Promotion
• Client needs to develop strategies to deal with fatigue, exacerbations
• Prevention of respiratory and urinary tract infections

Nursing Diagnoses
• Fatigue
• Self care deficits

Home Care
• Education
• Referral to support group and resources
• Referral to home health agencies when condition requires
Client with Parkinson’s Disease

Progressive, degenerative neurological disease
• characterized by tremor at rest, muscle rigidity and akinesia (poor movement); cause unknown
• Affects older adults mostly, mean age 60 with males more often than females
• Parkinson-like syndrome can occur with some medications, encephalitis, toxins; these are usually reversible

Pathophysiology
• Neurons in cerebral cortex atrophy and dopamine receptors in basal ganglia decrease
• Decrease in dopamine, which is neurotransmitter involved with motor function
• Disturbance between balance of dopamine and acetylcholine
• Balance needed for smooth coordinated movement

Manifestations
Tremor at rest with pill rolling motion of thumb and fingers
• Lessens with purposeful movement• Worsens with stress and anxiety• Progressive impairment affecting ability to write
and eatRigidity• Involuntary contraction of skeletal muscles• Cogwheel rigidity: jerky motion

Manifestations
Akinesia• Slowed or delayed movement that affects chewing,
speaking, eating• May freeze: loss of voluntary movement• Bradykinesia: slowed movementAbnormal posture• Involuntary flexion of head and shoulders, stooped
leaning forward position• Equilibrium problems causing falls, and short,
accelerated steps

Manifestations
Autonomic nervous system• Constipation and urinary hesitation or frequency• Orthostatic hypotension, dizziness with position
change• Eczema, seborrheaDepression and dementia; confusion, disorientation,
memory loss, slowed thinkingInability to change position while sleeping, sleep
disturbance

Complications
• Oculogyric crisis (fixed lateral and upward gaze)• Impaired communication• Falls• Infection related to immobility and pneumonia• Malnutrition related to dysphagia• Skin breakdown• Depression and isolation

Prognosis
• Slow progressive degeneration
• Eventual debilitation

Diagnostic Tests: No specific test for disease
• Drug screens to determine medications or toxins causing parkinsonism
• EEG: slowed and disorganized pattern

Medications
• Initially selegiline (Carbex), amantadine (Symmetrel), anticholinergics
• Combination carbidopa-levodopa (Sinemet)
• Bromocriptine (Parlodel) pergolide (Permax) inhibit dopamine breakdown
• Medications may lose their efficacy; response to drugs fluctuates: “on-off” effect

Treatments
Electrical stimulation for tremor suppression
Surgery has sometimes been done
• Pallidotomy: destruction of involved tissue
• Stereotaxic thalamotomy: destroys specific tissue involved in tremor
• Autologous adenal medullary transplant
Rehabilitation
• Physical therapy
• Occupational therapy
• Speech therapy

Nursing Care
• Education and support to client and family
• Maintain functioning
• Referral to home care, community resources
Health Promotion
• Fall, malnutrition, aspiration prevention

Nursing Diagnoses
• Impaired Physical Mobility
• Impaired Verbal Communication
• Impaired Nutrition: Less than body requirements
• Disturbed Sleep Patterns

Home Care
• Medication education
• Adaptation of home environment
• Gait training and exercises
• Nutritional teaching

Client with Huntington’s Disease (chorea)

Progressive, degenerative inherited neurologic disease
• characterized by increasing dementia and chorea (rapid, jerky involuntary movements)
• Cause unknown
• No cure
• Usually asymptomatic until age of 30 – 40

Pathophysiology
• involves destruction of cells in basal ganglia and other brain areas, decrease in acetylcholine

Manifestations • Abnormal movement and progressive dementia• Early signs are personality change with severe
depression, memory loss; mood swings, signs of dementia
• Increasing restlessness, worsened by environmental stimuli and emotional stress; arms and face and entire body develops choreiform movements, lurching gait; difficulty swallowing, chewing, speaking
• Slow progressive debilitation and total dependence• Death usually results from aspiration pneumonia or
another infectious process

Collaborative Care
• almost always requires long-term care

Diagnostic Tests
• genetic testing of blood
Medications
• Antipsychotic (phenothiazines and butyrophenones) to restore neurotransmitters
• Antidepressants
Nursing Care
• Very challenging: physiological, psychosocial and ethical problems
• Genetic counseling

Nursing Diagnoses
• Risk for Aspiration
• Imbalanced Nutrition: Less than body requirements
• Impaired Skin Integrity
• Impaired Verbal Communication
Home Care
• Referral to agencies to assist client and family, support group and organization

Client with Amyotrophic Lateral Sclerosis (ALS)
Description • Progressive, degenerative neurologic disease
characterized by weakness and wasting of muscles without sensory or cognitive changes
• Several types of disease including a familial type; onset is usually between age of 40 – 60; higher incidence in males at earlier ages but equally post menopause
• Physiologic problems involve swallowing, managing secretions, communication, respiratory muscle dysfunction
• Death usually occurs in 2 – 5 years due to respiratory failure

Pathophysiology
• Degeneration and demyelination of motor neurons in anterior horn of spinal cord, brain stem and cerebral cortex
• Involves upper and lower motor neurons
• Reinnervation occurs in the early course of disease, but fails as disease progresses

Manifestations • Initial: spastic, weak muscles with increased DTRs
(UMN involvement); muscle flaccidity, paresis, paralysis, atrophy (LMN involvement); clients note muscle weakness and fasciculations (twitching of involved muscles); muscles weaken, atrophy; client complains of progressive fatigue; usually involves hands, shoulders, upper arms, and then legs
• Atrophy of tongue and facial muscles result in dysphagia and dysarthria; emotional lability and loss of control occur
• 50% of clients die within 2 – 5 years of diagnosis, often from respiratory failure or aspiration pneumonia

Collaborative Care
• Evaluation to make the diagnosis
• Referrals for home health support;
• Client needs to make decisions regarding gastrostomy tube, ventilator support
Diagnostic Test
• Testing rules out other conditions that may mimic early ALS such as hyperthyroidism, compression of spinal cord, infections, neoplasms
• EMG to differentiate neuropathy from myopathy• Muscle biopsy shows atrophy and loss of muscle
fiber• Serum creatine kinase if elevated (non-specific)• Pulmonary function tests: to determine degree of
respiratory involvement

Medications
• Rilutek (Riluzole) antiglutamate
• Prescribed to slow muscle degeneration
• Requires monitoring of liver function, blood count, chemistries, alkaline phosphatase

Nursing Care
• Help client and family deal with current health problems
• Plan for future needs including inability to communicate

Nursing Diagnoses
• Risk for Disuse Syndrome
• Ineffective Breathing Pattern: may require mechanical ventilation and tracheostomy

Home Care
• Education regarding disease, community resources for health care assistance and dealing with disabilities

Client with Creutzfeldt-Jakob disease
(CJD, spongiform encephalopathy)

Description • Rapid progressive degenerative neurologic disease
causing brain degeneration without inflammation• Transmissible and progressively fatal• Caused by prion protein: transmission of prion is
through direct contamination with infected neural tissue• Rare in USA affecting persons 55 - 74• Variant form of CJD is “mad cow disease”: believed
transmitted by consumption of beef contaminated with bovine form of disease; none identified in USA as of yet
• Pathophysiology: spongiform degeneration of gray matter of brain
Manifestations
• Onset: memory changes, exaggerated startle reflex, sleep disturbances
• Rapid deterioration in motor, sensory, language function
• Confusion progresses to dementia
• Terminal states: clients are comatose with decorticate and decerebrate posturing

Diagnostic Tests
• Clinical pictures, suggestive changes on EEG and CT scan
• Similar to Alzheimers in early stages
• Final diagnosis made on postmortem exam

Nursing Care
• Use of standard precautions with blood and body fluids
• Support and assistance to client and family
Client with Myasthenia gravis (MG)
Description
• Chronic neuromuscular disorder characterized by fatigue and severe weakness of skeletal muscles
• Occurs with remissions and exacerbations
• Believed to be autoimmune in origin
• Occurs more frequently in females, with onset between ages 20 – 30
Pathophysiology
• Antibodies destroy or block neuromuscular junction receptor sites, resulting in decreased number of acetylcholine receptors
• Causes decrease in muscle’s ability to contract, despite sufficient acetylcholine
• Majority of clients have hyperplasia of thymus gland which is usually inactive after puberty; believed that thymus is source of autoantigen causing MG
• Associated in some clients with other autoimmune conditions

Manifestations
Seen in the muscles that are affected• Ptosis (drooping of eyelids), diplopia (double vision)• Weakness in mouth muscles resulting in dysarthria
and dysplagia• Weak voice, smile appears as snarl• Head juts forwardMuscles are weak but DTRs are normalWeakness and fatigue exacerbated by stress, fever,
overexertion, exposure to heat; improved with rest

Complications
Pneumonia
Myasthenic Crisis
• Sudden exacerbation of motor weakness putting client at risk for respiratory failure and aspiration
• Manifestations: tachycardia, tachypnea, respiratory distress, dysphasia

Complications
Cholinergic Crisis• Occurs with overdosage of medications
(anticholinesterase drugs) used to treat MG• Develops GI symptoms, severe muscle weakness,
vertigo and respiratory distressBoth crises often require ventilation assistanceDifferentiation is by administration of (edrophonium
chloride) Tensilon, which will improve the muscle weakness in myasthenic crisis and be ineffective with cholinergic crisis

Diagnostic Tests
• Physical examination and history• Tensilon Test: edrophonium chloride (Tensilon)
administered and client with myasthenia will show significant improvement lasting 5 minutes
• EMG: reduced action potential• Antiacetylcholine receptor antibody serum levels:
increased in 80% MG clients; used to follow course of treatment
• Serum assay of circulating acetylcholine receptor antibodies: if increased is diagnostic of MG
Medications
• Anticholinesterase medications, which act at neuromuscular junction, allowing acetylcholine to concentrate at receptor sites and promote muscle contraction; most commonly used medication is pyridostigmine (Mestinon)
• Immunsuppression medications including glucocorticoids
• Cyclosporineor azathioprine (Imuran)

Surgery
• Thymectomy is recommended in clients <60
• Remission occurs in 40 % of clients, but may takes several years to occur

Plasmapheresis
• Used to remove antibodies
• Often done before planned surgery, or when respiratory involvement has occurred

Nursing Care
• Teaching interventions to deal with fatigue
• Importance of following medication therapy

Nursing Diagnoses
• Ineffective Airway Clearance
• Impaired Swallowing: plan to take medication to assist with chewing activity

Home Care
• Avoid fatigue and stress
• Plan for future with treatment options
• Keep medications available
• Carry medical identification
• Referral to support group, community resources
Client with Guillain-Barre Syndrome

Description • Acute inflammatory demyelinating disorder of
peripheral nervous system characterized by acute onset of motor paralysis (usually ascending)
• Cause is unknown but precipitating events include GI or respiratory infection prior, surgery, or viral immunizations
• 80 – 90% of clients have spontaneous recovery with little or no disabilities
• 4 – 6% mortality rate, and up to 10% have permanent disabling weakness
• Characterized by progressive ascending flaccid paralysis of extremities with paresthesia and numbness
• 20 % require mechanical ventilation due to respiratory involvement

Pathophysiology
• Destruction of myelin sheath covering peripheral nerves as result of immunologic response
• Demyelinization causes sudden muscle weakness and loss of reflex response

Manifestations • Most clients have symmetric weakness beginning in lower
extremities• Ascends body to include upper extremities, torso, and
cranial nerves • Sensory involvement causes severe pain, paresthesia and
numbness• Client cannot close eyes• Paralysis of intercostals and diaphragmatic muscle can
result in respiratory failure• Autonomic nervous system involvement: blood pressure
fluctuations, cardiac dysrhythmias, paralytic illness, SIADH, urinary retention
• Weakness usually plateaus or starts to improve in the fourth week with slow return of muscle strength

Collaborative Care
• Ensuring adequate respiration and oxygenation
• Preventing complications due to immobility

Diagnostic Tests
• diagnosis made thorough history and clinical examination; there is no specific test
• CSF analysis: increased protein
• EMG: decrease nerve conduction
• Pulmonary function test reflect degree of respiratory involvement

Medications
• supportive and prophylactic care
• Antibiotics
• Morphine for pain control
• Anticoagulation to prevent thromboembolic complications
• Vasopressors as needed

Surgery
• may need tracheostomy, if prolonged ventilator support

Plasmapheresis
• may be helpful, if used early in the course of disease

Dietary Management
• usually requires enteral feeding or total parenteral nutrition

Physical and Occupational Therapy
• usually require long-term rehabilitation to regain maximum muscle strength

Nursing Care
• involves acute neurological and critical care nursing and rehabilitation

Nursing Diagnoses
• Acute Pain
• Risk for Impaired Skin Integrity
• Impaired Communication
Home Care
• Clients will usually require hospitalization, rehabilitation, and eventually discharge to home
• Client and family will need support; support groups

Trigeminal neuralgia
(tic douloureux)
Description
• Chronic disease of trigeminal nerve (cranial nerve V) causing severe facial pain
• The maxillary and mandibular divisions of nerve are effected
• Occurs more often in middle and older adults, females more than males
• Cause is unknown

Manifestations • Severe facial pain occurring for brief seconds to minutes
hundreds of times a day, several times a year• Usually occurs unilaterally in area of mouth and rises
toward ear and eye• Wincing or grimacing in response to the pain • Trigger areas on the face may initiate the pain• Sensory contact or eating, swallowing, talking may set
off the pain• Often there is spontaneous remission after years, and
then condition recurs with dull ache in between pain episodes

Diagnosis
• by physical assessment

Medications
• Anticonvulsants
• carbamazepine (Tegretol)
• phenytoin (Dilantin)
• gabapentin (Neurotin)
Surgery
• Intractable pain may be treated by severing the nerve root: rhizotomy
• Client may have lost facial sensation and have loss of corneal reflex
Nursing Care
• Teaching client self-management of pain
• Maintaining nutrition
• Preventing injury

Bell’s Palsy

Description
• Disorder of seventh cranial nerve and causes unilateral facial paralysis
• Occurs between age of 20 – 60 equally in males and females
• Cause unknown, but thought to be related to herpes virus

Manifestations
• Numbness, stiffness noticed first
• Later face appears asymmetric: side of face droops; unable to close eye, wrinkle forehead or pucker lips on one side
• Lower facial muscles are pulled to one side; appears as if a stroke
Prognosis
• Majority of person recover fully in few weeks to months
• Some persons have residual paralysis

Diagnosis
• based on physical examination

Collaborative Care
• Corticosteroids are prescribed in some cases but use has been questioned
• Treatment is supportive

Nursing Care
• Teaching client self-care: prevent injury and maintain nutrition
• Use of artificial tears, wearing eye patch or taping eye shut at night; wearing sunglasses
• Soft diet that can be chewed easily, small frequent meals

Neurologic Diseases that result from viral infections or
neurotoxins

Postpoliomyelitis Syndrome • Complication of previous poliomyelitis virus (epidemic
occurred in USA during 1940’s and 1950’s); persons who recovered are re-experiencing manifestation of acute illness in their advanced age
• Pathophysiology: Process is unknown• Manifestations: Fatigue, muscle and joint weakness, loss
of muscle mass, respiratory difficulties, and pain• Diagnosis: By history and physical examination• Treatment: Involves physical therapy and pulmonary
rehabilitation• Nursing Care: Involves emotional support and
interventions to deal with dysfunction; ADL, safety are including in interventions

Rabies
Rhabovirus infection of CNS transmitted by infected saliva that enters the body through bite or open wound
• Critical illness almost always fatal
• Source often is bite of infected domestic or wild animal
• Incubation is 10 days to years

Rabies
Manifestations occur in stages• Prodromal: wound is painful, various paresthesias,
general signs of infection; increased sensitivity to light, sound, and skin temperature changes
• Excitement stage: periods of excitement and quiet; develops laryngospasm and is afraid to drink (hydrophobia), convulsions, muscle spasms and death usually due to respiratory failure

Rabies
Collaborative Care
• Animal that bit person is held under observation for 7 – 10 days to detect rabies
• Sick animal are killed and their brains are tests for presence of rabies virus
• Blood of client may be tested for rabies antibodies

Rabies
Post-exposure treatment• Rabies immune globulin (RIG) is administered for passive
immunization• Client often has local and mild systemic reaction; treatment
is over 30 daysTreatment of client with rabies: involves intensive care
treatmentHealth Promotion• Vaccination of pets• Avoid wild animals, especially those appearing ill• Follow up care for any bites

Tetanus (lockjaw) Disorder of nervous system caused by neurotoxin from
Clostridium tetani, anaerobic bacillus present in the soil• Contract disease from open wound contaminated with
dirt, debris• Has high mortality rateIncubation is usually 8 – 12 daysManifestations • Stiffness of jaw and neck and dysphagia• Spasms of jaw and facial muscles• Develops generalized seizures and painful body muscle
spasms• Death occurs from respiratory and cardiac complications
Tetanus (lockjaw)
Diagnosis is made on clinical manifestationsClients with disease are treated in intensive care with
antibiotics, chlorpromazine (Thorazine) and diazepam (Valium ) for muscles spasms
Health Promotion• Active immunization with boosters given at time
of exposure• Passive immunization is given to persons who are
not adequately immunized

Botulism
Food poisoning caused by ingestion of food contaminated with toxin from Clostridium botulinum, anaerobic bacteria found in soil
• Contracted by eating contaminated foods usually improperly canned or cooked
• Untreated death rate is highPathophysiology: Bacteria produce a toxin, which
blocks release of acetylcholine from nerve endings causing respiratory failure by paralysis of muscles

BotulismManifestations• Visual disturbances• Gastrointestinal symptoms• Paralysis of all muscle groups• Effecting respirationDiagnosis • Based on clinical picture• Verified by laboratory analysis of client’s
serum and stool• Testing the suspected food
BotulismTreatment• Administration of antitoxin• Supportive treatment including mechanical
ventilation and systemic support in intensive care unit
Health Promotion• Teaching clients to process foods properly when
home canning• Boiling foods for 10 minutes which destroys the
toxin• Not eating spoiled foods
Related Documents