Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019 34 ISSN 2704-3568 Nursing Care Modalities Employed in Selected Hospitals in Batangas Province, Philippines Karen Shiela Ann D. Quesea, Bella P. Magnaye College of Nursing, Lyceum of the Philippines University, Batangas City, Philippines Abstract –A care modality is a method of organizing and delivering nursing care in a hospital setting in order to achieve desired patient outcomes. The study intended to identify nursing care modalities employed in selected hospitals in Batangas to assess the functional and primary nursing care in terms of effectiveness and efficiency; competency based on eleven key areas of nursing responsibilities; and management in the delivery of care in order to improve and or redesign the workloads and management in hospitals so that the tasks can be accomplished with fewer nurses yet still more effectively and efficiently. This study used the descriptive research design to compare Primary and Functional Nursing Care in general ward. The population for this study consisted of 100% total respondents, 59 registered nurses who were employed in Hospital A (functional nursing modality) and 45 registered nurses in Hospital B (primary nursing care modality) working particularly in ward unit within the institution. In addition to that, in order to validate the result, triangulation of the respondents were used. Additional respondents who volunteered to participate in the study involved 25 patients/relatives and 5 physicians/ nursing supervisor, for each institution. The study revealed that primary nursing excels more than functional nursing in all three aspects of care delivery. Furthermore, primary nursing care, when it comes to management of delivery of care has a substantial variance with functional nursing. Meanwhile, both modalities have no difference when it comes to competency, efficiency and effectiveness in care delivery. Also, profile variables which included age, gender, and marital status, length of service, and monthly income, and functional nursing had no substantial variance with effectiveness and efficiency, competency, and management in the delivery of functional care. This was almost the same in primary nursing modality except

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
34 ISSN 2704-3568
Nursing Care Modalities Employed in Selected
Hospitals in Batangas Province, Philippines
Karen Shiela Ann D. Quesea, Bella P. Magnaye
College of Nursing, Lyceum of the Philippines University,
Batangas City, Philippines
Abstract –A care modality is a method of organizing and
delivering nursing care in a hospital setting in order to achieve
desired patient outcomes. The study intended to identify nursing
care modalities employed in selected hospitals in Batangas to
assess the functional and primary nursing care in terms of
effectiveness and efficiency; competency based on eleven key
areas of nursing responsibilities; and management in the
delivery of care in order to improve and or redesign the
workloads and management in hospitals so that the tasks can be
accomplished with fewer nurses yet still more effectively and
efficiently. This study used the descriptive research design to
compare Primary and Functional Nursing Care in general ward.
The population for this study consisted of 100% total
respondents, 59 registered nurses who were employed in
Hospital A (functional nursing modality) and 45 registered
nurses in Hospital B (primary nursing care modality) working
particularly in ward unit within the institution. In addition to
that, in order to validate the result, triangulation of the
respondents were used. Additional respondents who volunteered
to participate in the study involved 25 patients/relatives and 5
physicians/ nursing supervisor, for each institution. The study
revealed that primary nursing excels more than functional
nursing in all three aspects of care delivery. Furthermore,
primary nursing care, when it comes to management of delivery
of care has a substantial variance with functional nursing.
Meanwhile, both modalities have no difference when it comes to
competency, efficiency and effectiveness in care delivery. Also,
profile variables which included age, gender, and marital status,
length of service, and monthly income, and functional nursing
had no substantial variance with effectiveness and efficiency,
competency, and management in the delivery of functional care.
This was almost the same in primary nursing modality except

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
35 ISSN 2704-3568
that there is difference between length of service and
management, requiring practice and training to execute the
primary nursing properly. In addition, action plan in enhancing
primary and functional nursing care models was developed for
future implementation.
Keywords – functional care, primary nursing care
INTRODUCTION
Nurses or healthcare providers who are working in a hospital
make sure to put their heart, mind and soul in giving quality care
to people who need their attention. However, in order to attain
excellence in organizing and in providing care, nurses must work
in a system or structured approach guided by values and beliefs
called nursing care modalities.
There are different care modalities used in different hospital
settings worldwide permissible to establish and deliver nursing
care to achieve optimum patient outcome. The study of Harris
and McGillis (2012) found that current research has extended the
field of knowledge regarding nursing care delivery models,
providing evidence of the need to capture other aspects of care in
studies linking nurse staffing to patient outcomes. Also,
traditional care delivery models, such as primary nursing and
functional nursing, appear to have mixed effects on patient and
nurse outcomes, highlighting the importance of considering
specific populations and care settings.
In the Philippines, two modalities of care have been practiced
in different hospitals, the primary and functional nursing care.
Because there was undeniably shortage of nurses and limited
funding to hire more nurses, hospitals were forced to compress
available staff in order to give care to patients. Despite that some
hospitals focus on giving care to patients without considering the
quality and risks among the nurses or healthcare providers. It is
only proper that some hospitals should value the persons
involved in giving nursing care in order to lessen the workload
of nurses or job exhaustion, and at the same time to give
appropriate care to admitted patients.
Subsequently, primary and functional nursing care varies in
some other ways, therefore, they need to be evaluated and
assessed. They have different advantages and disadvantages.

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
36 ISSN 2704-3568
Since there is a gap or negative effect, it is appropriate to asses
each modality in order to improve or resolve this gap. Also,
nurse managers need a concrete basis to apply appropriate
nursing care model in their hospitals. For this reason, there is a
need for an in depth study on the methods of nursing
management is necessary. Consequently, there is no generic
system used by the hospitals in the country, specifically in
Batangas province. Thus, research must be conducted to figure
out which is the best method that the hospital institution can
adopt to give more quality patient care. Furthermore, this study
can be a reference of Department of Health in order to give more
credit to nurses considering nurse patient ratio in their
deployment in hospital settings.
OBJECTIVES OF THE STUDY
This study aimed to identify nursing care modalities
employed in selected hospitals in Batangas to assess functional
and primary nursing care model in clinical setting. Specifically,
it intended to determine the profile of the nurse respondents in
terms of gender, age, marital status, length of service, monthly
income; to assess the functional and primary nursing care in
terms of effectiveness and efficiency; competency based on
eleven key areas of nursing responsibilities; and management in
the delivery of care; to test the significant differences between
functional and primary nursing care modalities; to determine the
significant differences between the profile variable and
functional nursing care modality; and the profile variable and
primary nursing care modality; to propose an action plan to
enhance primary and functional nursing care modalities.
METHODS
Research Design
For the researcher to come up with the solutions necessary to
solve the identified research problems, this study used the
descriptive research design to assess Primary and Functional
Nursing Care in hospital ward. Descriptive research, also known
as statistical research, describes data and characteristics about
the population or phenomenon being studied.
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
37 ISSN 2704-3568
This method ascertains the condition that prevails in the
group and obtains the facts regarding existing conditions, the
purpose of which is to find new truth [2]. It utilizes the
questionnaire with the aid of study guide as means of obtaining
the needed information.
Participants of the Study
The population for this study consisted of 100% total
respondents, 59 registered nurses who have been employed in
Hospital A, have practiced functional nursing care and 45
registered nurses in Hospital B, who have practiced primary
nursing care, in clinical settings particularly in ward unit within
the institution. Also, to verify the results given by nurses,
additional respondents included doctors, nurse supervisors,
patients and relatives presently available and affiliated in the said
hospitals during the conveyance of the questionnaires. For that
instance, 25 patients or relatives volunteered and 5 doctors or
nurse supervisors available for each hospital answered the
questionnaires.
Instrument
In the development of the questionnaire, the researcher made
a thorough reading and analyzed the variables involved in the
study through books, journals and other references related to the
study. These data and information helped the researcher to
formulate a self-made questionnaire that was used as a tool to
gather facts and essential data to answer the research problems.
The questionnaire consisted of two parts: the first part was
about the profile of the respondents in terms of gender, age,
marital status, length of service and, monthly income; the second
part tackled effectiveness and efficiency; competency based on
eleven key areas of nursing responsibilities; and management in
the delivery of care which have been applied in primary and
functional nursing care modalities.
The researcher used Likert Scale in the questionnaire to
obtain participants’ preferences or degree of agreement with a
statement or set of statements. Likert scales are a non-
comparative scaling technique and are unidimensional (only
measure a single trait) in nature (―Likert scale‖, 2014).

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
38 ISSN 2704-3568
In describing the effectiveness and efficiency in the delivery
of care that were applied in primary and functional nursing care
modalities, the following numerical scales below were used: 3.50
– 4.00: Highly effective; 2.50 – 3.49: Effective; 1.50 – 2.49: Less
effective; 1.00 - 1.49: Not effective.
For the level of competency based on eleven key areas of
nursing responsibilities in the delivery of care that were used in
primary and functional nursing care modalities, the subsequent
likert scale were followed: 3.50 – 4.00: Highly competent; 2.50 –
3.49: Competent; 1.50 – 2.49: Less competent; 1.00 - 1.49: Not
competent.
The extent of management in the delivery of care which
pertains in primary and functional nursing care modalities were
measured using the following range: 3.50 – 4.00: (Always) All
the time; 2.50 – 3.49: Often; 1.50 – 2.49: Rarely; 1.00 - 1.49:
Never.
Procedure
In conducting this research study, the researcher made use of
a self-structured questionnaire based from books, internet-related
studies and previous theses. The questionnaires were tested and
validated by the experts which included the adviser, dean of
nursing and statistician. Pre-test, also known as pilot test of
questionnaire, was done within a small sample of participants to
check respondents’ understanding and ability to answer the
questions before use. After the approval of the questionnaire, the
researcher submitted a letter of request, which had been signed
by the Dean of Graduate School, research adviser and the
researcher. The researcher distributed the questionnaires to the
participants assuring confidentiality and protected information
through utilization of informed consent within the institution.
Same set of questionnaire were used for both primary and
functional nursing care participants.
However, additional respondents were needed to validate the
results of the first participant (nurses). For this, second
distribution of questionnaires was done to different respondents
in the same institutions to confirm the previous gathered data,
the data triangulation method. Clear directions were given in the
questionnaire to guide the participants in answering the items,
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
39 ISSN 2704-3568
ensuring a favorable response from the participants. Data
retrieved were tabulated, interpreted and analyzed.
Data Analysis
All data needed were encoded, tabulated and interpreted
using different statistical tools. Frequency distribution was used
to describe the profile of the respondents. Also, weighted mean
was used to assess the functional and primary nursing care. In
addition, t-test and eta2
were used to test the significant
difference and relationship on the variables tested. The obtained
data were also supported using PASW version 18 to further
analyze the result using 0.05 alpha level.
RESULTS AND DISCUSSIONS
Table 1. Percentage Distribution of the Respondents’ Profile
Profile
Variables F % Profile Variables F %
Age
Length of service in Primary of
Functional nursing care setting
20-25 55 52.88 1 month- 6mos. 8 7.69
26-30 30 28.85 7mos- 1 year 15 14.42
30-35 6 5.77 1year- 2 years 23 22.12
36-40 4 3.85 3years-5years 24 23.08
41-50 9 8.65
Gender
5years-10years 27 25.86
Male 23 22.12 10years and above 7 6.73
Female 81 77.88 Monthly Income
Marital
Status Php 3,000-6,000 30 28.85
Single 77 74.04 Php 6,000-10,000 43 41.35
Married 25 24.04 Php 10,000-15,000 27 25.96
Divorced 2 1.92 Php 15,000- 20,000 4 3.85
Widower 0 0 Php 20,000-30,000 0 0
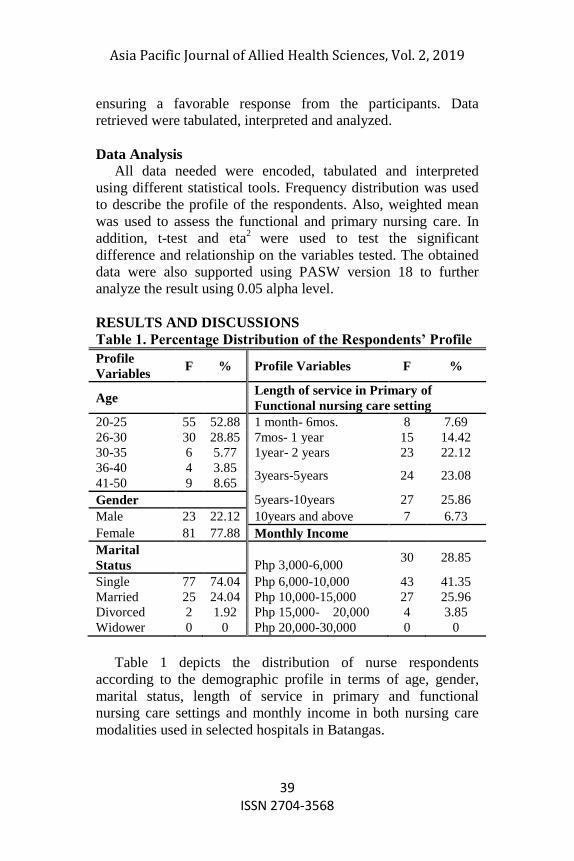
Table 1 depicts the distribution of nurse respondents
according to the demographic profile in terms of age, gender,
marital status, length of service in primary and functional
nursing care settings and monthly income in both nursing care
modalities used in selected hospitals in Batangas.
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
40 ISSN 2704-3568
In the breakdown of the nurse respondents, most of them
were single as accounted by 74.0 percent, which reflects to the
age of the nurse respondents that almost half of the total
population were in their early 20’sin both institutions using
primary and functional modalities. The age bracket of 36-49 had
the smallest portion of 3.58 percent as recorded.
Furthermore, the distribution of nurse participants regarding
gender was dominated by female (77.88%), while male
composed almost a quarter of the entire population of nurses
respectively. Most nurses are female as observed in the world
history of nursing. This conforms to Thompson and Vertein
(2008) statement that Nightingale transformed nursing into an
acceptable and respectable occupation for women. Both believed
that women were naturally better at nurturing the sick, more
affectionate and more caring than men despite the fact that men
had shown compassion and caring as nurses throughout history.
With regards to the length of service in primary and
functional nursing care settings, over three-fifths of the nurse
respondent were up to 5 years in their respective organization got
the greater portion. Meanwhile, few of the nurse respondents
(6.73%) were in the service for more than 10 years respectively.
This point towards that a very large majority (70%) of the nurse
respondents acquired the monthly income of PHp 3,000-10,000
only, which is the basic salary for nurses with 5 years experience
as seen in the result.
This findings contradict to the Health Human Resources
Production, Utilization and Development, Article VII, Sec. 32
that in order to enhance the general welfare, commitment to
service and professionalism of nurses the minimum base pay of
nurses working in the public health institutions shall not be lower
than salary grade 15 ( approximately PHp 24,000-26,000)
prescribes under Republic Act No. 6758, otherwise known as the
―Compensation and Classification Act of 1989.″ However,
Republic Act No. 6758 is self-contained in government
institutions alone and private sectors are not required to follow.
This verdict that nurses in the Philippines regardless of
employment in primary or functional modality were underpaid.
In fact, this is one of the reasons why most of the Philippine
nurses chooses to work overseas after gaining definite years of

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
41 ISSN 2704-3568
experience which is also reflected in the outcome of this study.
This implies that most nurses acquire low compensation
throughout their hard work that reflects poor general welfare.
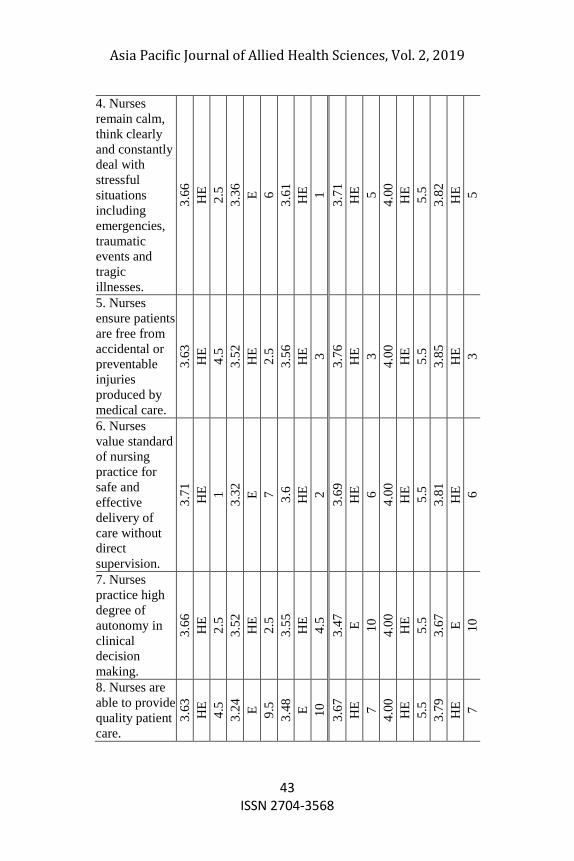
As illustrated in table 2.1 on page 25, functional nurses have
little confusion regarding responsibilities which reflected in the
results because functional nursing is tasked-oriented in which a
particular nursing function is assigned to each worker (Venzon
& Nagtalan, 2010).
That is why ―nurses remain calm, think clearly and constantly
deal with stressful situations including emergencies, traumatic
events and tragic illnesses‖ and ―nurses values standard of
nursing practice for safe and effective delivery of care without
direct supervision‖. This clearly implies that defined policies and
procedures are used to complete the physical aspects of care in
an efficient and economical manner (Dadich, 2007).
This conforms to Paulino (2007) statement that the health
care delivered by a nurse to a patient must be harmonious
integration of knowledge and skill, maintained and nurtured to
ensure each efficiency and effectiveness.
Certainly, to achieve positive outcome and wellness of the
patient, nurses must guarantee accurate and effective
implementation of nursing practice which according to Paulino
(2007) could be reflected in the nonexistence of patient’s
incidents and in the absence of avoidable adverse patient
outcome during nursing.
However, the outcomes of the study which is highly effective
contradicts to what Williams and Wilkins (2009) presumed that
employees in functional nursing modality often focus only on
their own efforts, with less interest in overall results.
Also, the findings refutes that nurses’ accountability and
responsibility are diminished; evaluation of nursing care is poor
and outcomes are rarely documented (Venzon & Nagtalan,
2010). Indeed, the result likely to oppose the disadvantages of
functional nursing which includes fragmentation of nursing care
and therefore holistic care is not achieved (Venzon & Nagtalan,
2010), and there is no overall plan for assuring that all the
patient’s needs are met (Hayne & Baily, 2004). Anticipating
patient’s needs and providing patient care were both efficient
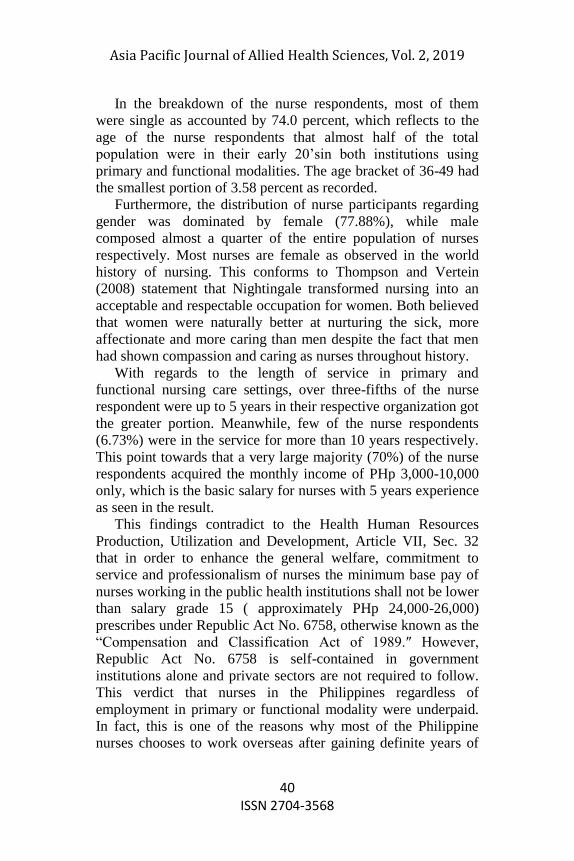
although not highly efficient based on the results. Overall, the
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
42 ISSN 2704-3568
functional nursing care in terms of effectiveness and efficiency
in the delivery of care was highly effective since the computed
mean values of each indicator were all greater than 3.50
respectively with the composite mean of 3.54.
Table 2.1. Effectiveness and Efficiency in the Delivery of
Care
Functional Nursing Care Primary Nursing Care
Nu
rse
Pa
tien
t/
Rel
ati
ve
Ov
er-a
ll
Nu
rse
Pa
tien
t/
Rel
ati
ve
Ov
er-a
ll
Indicators
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
1. Nurses
identify
patient needs
in a holistic
manner.
3.5
8
HE
7
3.2
8
E
8
3.5
5
HE
4.5
3.7
8
HE
2
4.0
0
HE
5.5
3.8
6
HE
2
2. Nurses
advocate for
their patients
and anticipates
their needs.
3.5
8
HE
7
3.5
2
HE
2.5
3.4
9
E
9
3.8
2
HE
1
4.0
0
HE
5.5
3.8
9
HE
1
3. Nurses keep
track of and
record minor
changes in a
patient’s
health or
behavior.
3.5
6
HE
9.5
3.2
4
E
9.5
3.5
4
HE
6
3.7
3
HE
4
4.0
0
HE
5.5
3.8
3
HE
4
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
43 ISSN 2704-3568
4. Nurses
remain calm,
think clearly
and constantly
deal with
stressful
situations
including
emergencies,
traumatic
events and
tragic
illnesses.
3.6
6
HE
2.5
3.3
6
E
6
3.6
1
HE
1
3.7
1
HE
5
4.0
0
HE
5.5
3.8
2
HE
5
5. Nurses
ensure patients
are free from
accidental or
preventable
injuries
produced by
medical care.
3.6
3
HE
4.5
3.5
2
HE
2.5
3.5
6
HE
3
3.7
6
HE
3
4.0
0
HE
5.5
3.8
5
HE
3
6. Nurses
value standard
of nursing
practice for
safe and
effective
delivery of
care without
direct
supervision.
3.7
1
HE
1
3.3
2
E
7
3.6
HE
2
3.6
9
HE
6
4.0
0
HE
5.5
3.8
1
HE
6
7. Nurses
practice high
degree of
autonomy in
clinical
decision
making.
3.6
6
HE
2.5
3.5
2
HE
2.5
3.5
5
HE
4.5
3.4
7
E
10
4.0
0
HE
5.5
3.6
7
E
10
8. Nurses are
able to provide
quality patient
care.
3.6
3
HE
4.5
3.2
4
E
9.5
3.4
8
E
10
3.6
7
HE
7
4.0
0
HE
5.5
3.7
9
HE
7
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
44 ISSN 2704-3568
9. Nurses
attain
maximum
patient
outcomes
across the
continuum of
care.
3.5
6
HE
9.5
3.4
8
E
5
3.5
2
HE
7
3.6
2
HE
8
4.0
0
HE
5.5
3.7
6
HE
8
10. Nurses
gain the
patient's
satisfaction
after nursing
care has been
performed.
3.5
8
HE
7
3.5
2
HE
2.5
3.5
1
HE
8
3.6
HE
9
4.0
0
HE
5.5
3.7
5
HE
9
Composite
Mean 3.6
1
HE
3.4
0
E
3.5
4
HE
3.6
8
HE
4.0
0
HE
3.8
HE
Legend: HE= highly effective; E=effective; LE=less effective; NE= not
effective
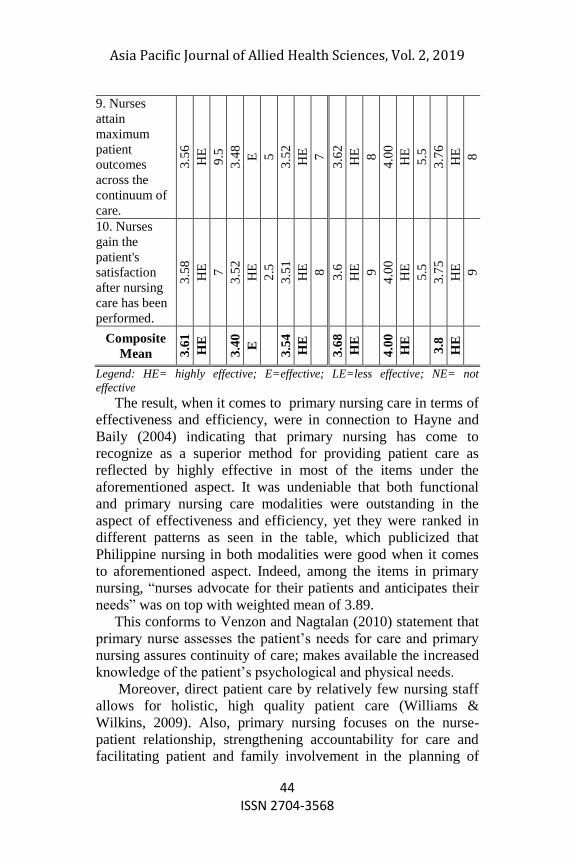
The result, when it comes to primary nursing care in terms of
effectiveness and efficiency, were in connection to Hayne and
Baily (2004) indicating that primary nursing has come to
recognize as a superior method for providing patient care as
reflected by highly effective in most of the items under the
aforementioned aspect. It was undeniable that both functional
and primary nursing care modalities were outstanding in the
aspect of effectiveness and efficiency, yet they were ranked in
different patterns as seen in the table, which publicized that
Philippine nursing in both modalities were good when it comes
to aforementioned aspect. Indeed, among the items in primary
nursing, ―nurses advocate for their patients and anticipates their
needs‖ was on top with weighted mean of 3.89.
This conforms to Venzon and Nagtalan (2010) statement that
primary nurse assesses the patient’s needs for care and primary
nursing assures continuity of care; makes available the increased
knowledge of the patient’s psychological and physical needs.
Moreover, direct patient care by relatively few nursing staff
allows for holistic, high quality patient care (Williams &
Wilkins, 2009). Also, primary nursing focuses on the nurse-
patient relationship, strengthening accountability for care and
facilitating patient and family involvement in the planning of

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
45 ISSN 2704-3568
care (Manthey, 2013). As concluded by Maratning (2004), the
presence of nurses along with their patients as regarded to
contribute significantly to the attainment of a better feeling of
satisfaction among patients. Nurses in primary nursing regarding
patient safety in accordance to standard nursing practice were
also greatly observed in the outcome.
On the other hand, ―nurses practice high degree of autonomy
in clinical decision making‖ was only effective in primary
nursing and got the smallest in number by 3.47 among the items.
This is due to the fact that the primary method required high
degree of responsibility and autonomy that the implementation
became challenging.
Likewise, Cherry and Joven (2014) pointed out that an
inadequate prepared primary nurse may not be able to make the
necessary clinical decisions or communicate effectively with the
health care team which needs proper training.In this same
reason, once nurses develop skill in primary nursing care
delivery, they feel challenged and rewarded (Williams &
Wilkins, 2009) by gaining patient’s satisfaction which revealed
in the output of this study as proven by the result.
To sum up, although there were items that were verbally
interpreted in both functional and primary nursing, still, after
getting the composite mean of each modalities, they were both
verbally interpreted as highly effective. However, it is obvious
that primary nursing care (3.80) was greater than functional
nursing care (3.54) with the difference of 0.26 in number.
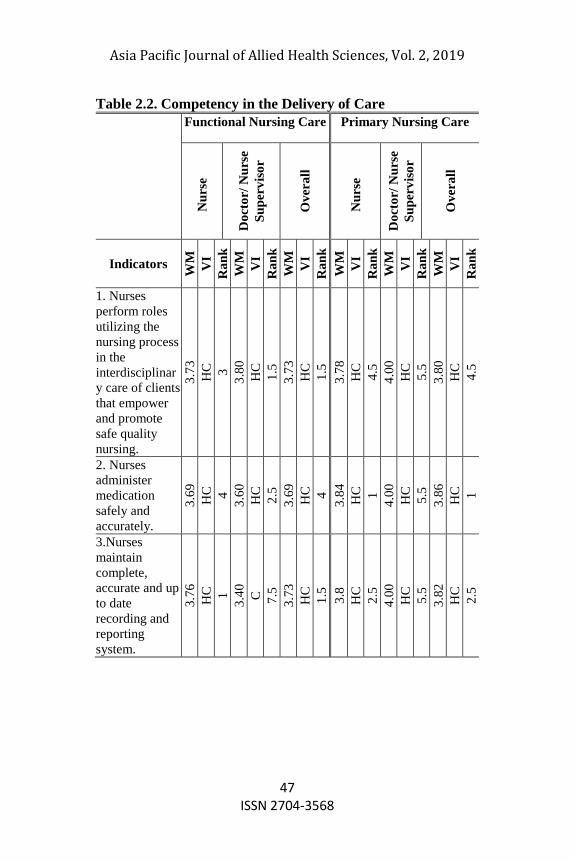
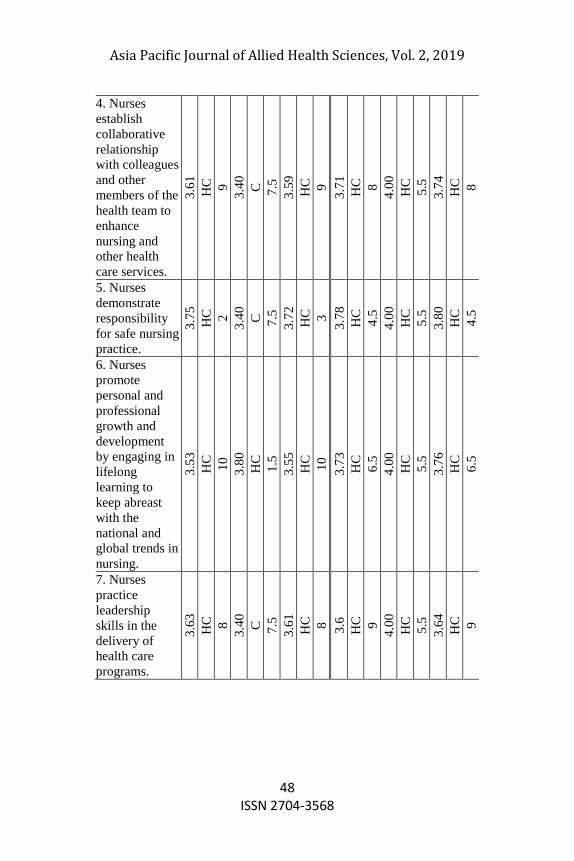
As shown in table 2.2, functional nursing, as well as, primary
nursing competency in delivery of care were both rated ―highly
competent‖. It seemed to collaborate with the statement made by
Llanes (2011), in which the existing competencies are
considered to be very comprehensive, and that even after five
years from the time of promulgation are still found to be very
relevant and frequently used based on the perspectives of the
nursing experts. In point of fact, the first in rank in functional
delivery of care was shared by ―nurses perform roles utilizing the
nursing process in the interdisciplinary care of clients that
empower and promote safe quality nursing,‖ and ―nurses
maintain complete, accurate and up to date recording and
reporting system,‖ garnered the weighted mean of 3.73, followed
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
46 ISSN 2704-3568
by demonstrating responsibility for safe nursing practice with
3.72 respectively. On the other hand, in primary delivery of care,
nurses administer medication safely and accurately obtained the
highest score as reflected by the weighted mean of 3.86. Nurses
maintain complete, accurate and up to date recording and
reporting system; communicate effectively in the level of health
in various cultural setting both secured weighted mean of 3.82.
As clearly seen from the table, different weighted mean and
ranking of functional and primary method did not affect the
overall result. This implies that Philippine nurses excel when it
comes to competency that is guided by the standard of nursing
practice together with nursing process that adheres to the nurses'
national and international code of ethics. Certainly, this nursing
process assists the nurse to manage each patient’s nursing care
intelligently, scientifically and judiciously (Paulino, 2007).
In fact, according to Article IV of Competency Standards,
Section 5, graduates of Bachelor of Science in Nursing program
must be able to apply analytical and critical thinking in the
nursing practice. The nurse must be competent in Key Areas of
Responsibility with their respective core competency standards
and indicators. This includes providing nursing care that is safe
and of high quality. Moreover, Philippine nurses must be aware
of their duties and responsibilities in the practice of their
profession as defined in the ―Philippine Nursing Act of 2002‖. In
addition, the respondents made sure that the nursing practice of
safe and quality nursing care meet the optimum standard as
presented by the findings.
However, the fact that the Philippines is facing shortage in
nurses due to decrease general welfare coming from the
government and the presence of gap or disadvantages of
functional and primary care in the delivery of quality care. Still,
this is not a hindrance to Filipino nurses to give optimum care,
and provide value in their work to the extent that they push their
limits. This was proven, as seen on the above table, that the
second set of respondents, doctors and nurse supervisor, give an
average scores to the nurses in primary and functional nursing
care. Still, Philippine nurses were able to be competitive when it
comes in caring despite of obstacles.
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
47 ISSN 2704-3568
Table 2.2. Competency in the Delivery of Care
Functional Nursing Care Primary Nursing Care
Nu
rse
Do
cto
r/ N
urs
e
Su
per
vis
or
Ov
era
ll
Nu
rse
Do
cto
r/ N
urs
e
Su
per
vis
or
Ov
era
ll
Indicators
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
1. Nurses
perform roles
utilizing the
nursing process
in the
interdisciplinar
y care of clients
that empower
and promote
safe quality
nursing.
3.7
3
HC
3
3.8
0
HC
1.5
3.7
3
HC
1.5
3.7
8
HC
4.5
4.0
0
HC
5.5
3.8
0
HC
4.5
2. Nurses
administer
medication
safely and
accurately.
3.6
9
HC
4
3.6
0
HC
2.5
3.6
9
HC
4
3.8
4
HC
1
4.0
0
HC
5.5
3.8
6
HC
1
3.Nurses
maintain
complete,
accurate and up
to date
recording and
reporting
system.
3.7
6
HC
1
3.4
0
C
7.5
3.7
3
HC
1.5
3.8
HC
2.5
4.0
0
HC
5.5
3.8
2
HC
2.5
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
48 ISSN 2704-3568
4. Nurses
establish
collaborative
relationship
with colleagues
and other
members of the
health team to
enhance
nursing and
other health
care services.
3.6
1
HC
9
3.4
0
C
7.5
3.5
9
HC
9
3.7
1
HC
8
4.0
0
HC
5.5
3.7
4
HC
8
5. Nurses
demonstrate
responsibility
for safe nursing
practice.
3.7
5
HC
2
3.4
0
C
7.5
3.7
2
HC
3
3.7
8
HC
4.5
4.0
0
HC
5.5
3.8
0
HC
4.5
6. Nurses
promote
personal and
professional
growth and
development
by engaging in
lifelong
learning to
keep abreast
with the
national and
global trends in
nursing.
3.5
3
HC
10
3.8
0
HC
1.5
3.5
5
HC
10
3.7
3
HC
6.5
4.0
0
HC
5.5
3.7
6
HC
6.5
7. Nurses
practice
leadership
skills in the
delivery of
health care
programs.
3.6
3
HC
8
3.4
0
C
7.5
3.6
1
HC
8
3.6
HC
9
4.0
0
HC
5.5
3.6
4
HC
9
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
49 ISSN 2704-3568
8. Nurses
demonstrate
capacity to lead
and supervise
nursing support
staff. 3
.68
HC
5.5
3.4
0
C
7.5
3.6
6
HC
6
3.5
3
HC
10
4.0
0
HC
5.5
3.5
8
HC
10
9. Nurses
collaborate for
referral to other
medical health
team.
3.6
6
HC
7
3.6
0
HC
2.5
3.6
6
HC
6
3.7
3
HC
6.5
4.0
0
HC
5.5
3.7
6
HC
6.5
10. Nurses
communicate
effectively in
the level of
health in
various cultural
setting.
3.6
8
HC
5.5
3.4
0
C
7.5
3.6
6
HC
6
3.8
HC
2.5
4.0
0
HC
5.5
3.8
2
HC
2.5
Composite
Mean 3.6
7
HC
3
.52
HC
3
.66
HC
3
.73
HC
4
.00
HC
3
.76
HC
Legend: HC= highly competent; C=competent; LE=less competent; NE= not
competent
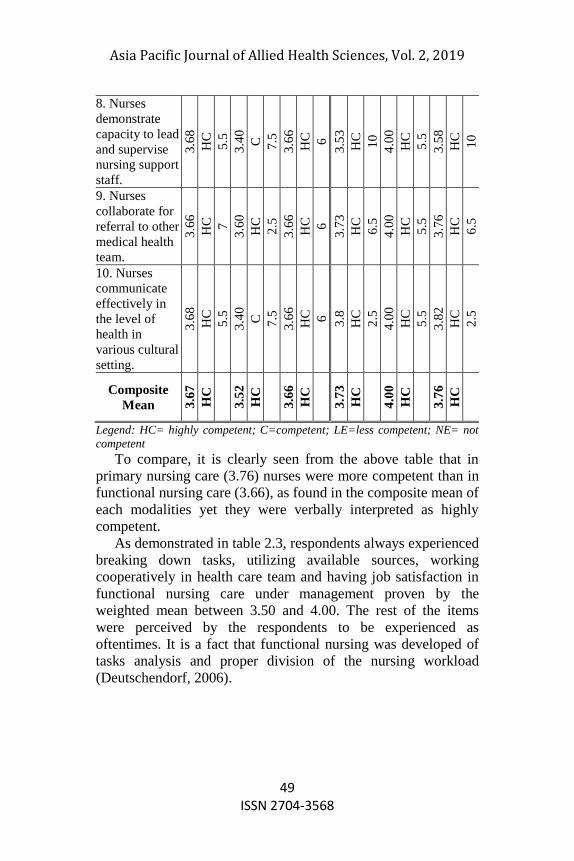
To compare, it is clearly seen from the above table that in
primary nursing care (3.76) nurses were more competent than in
functional nursing care (3.66), as found in the composite mean of
each modalities yet they were verbally interpreted as highly
competent.
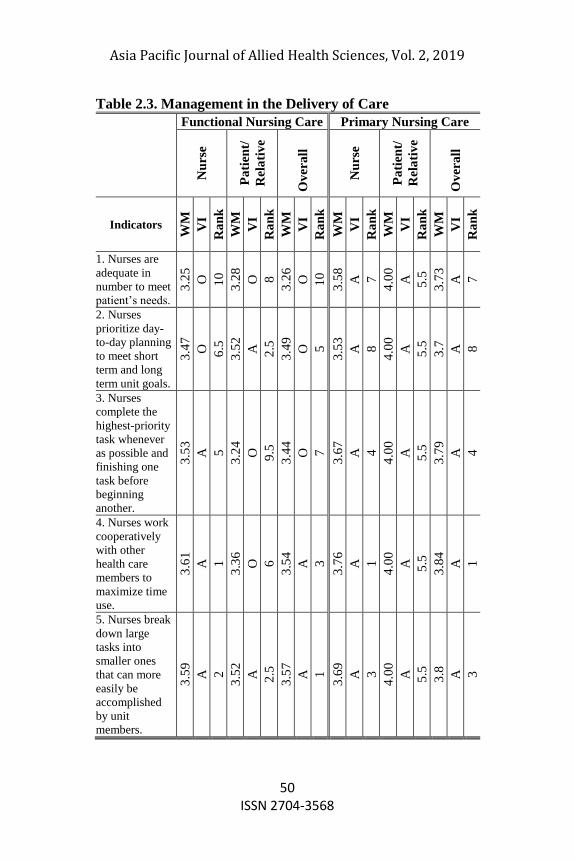
As demonstrated in table 2.3, respondents always experienced
breaking down tasks, utilizing available sources, working
cooperatively in health care team and having job satisfaction in
functional nursing care under management proven by the
weighted mean between 3.50 and 4.00. The rest of the items
were perceived by the respondents to be experienced as
oftentimes. It is a fact that functional nursing was developed of
tasks analysis and proper division of the nursing workload
(Deutschendorf, 2006).
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
50 ISSN 2704-3568
Table 2.3. Management in the Delivery of Care
Functional Nursing Care Primary Nursing Care
Nu
rse
Pa
tien
t/
Rel
ati
ve
Ov
era
ll
Nu
rse
Pa
tien
t/
Rel
ati
ve
Ov
era
ll
Indicators
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
WM
VI
Ra
nk
1. Nurses are
adequate in
number to meet
patient’s needs.
3.2
5
O
10
3.2
8
O
8
3.2
6
O
10
3.5
8
A
7
4.0
0
A
5.5
3.7
3
A
7
2. Nurses
prioritize day-
to-day planning
to meet short
term and long
term unit goals.
3.4
7
O
6.5
3.5
2
A
2.5
3.4
9
O
5
3.5
3
A
8
4.0
0
A
5.5
3.7
A
8
3. Nurses
complete the
highest-priority
task whenever
as possible and
finishing one
task before
beginning
another.
3.5
3
A
5
3.2
4
O
9.5
3.4
4
O
7
3.6
7
A
4
4.0
0
A
5.5
3.7
9
A
4
4. Nurses work
cooperatively
with other
health care
members to
maximize time
use.
3.6
1
A
1
3.3
6
O
6
3.5
4
A
3
3.7
6
A
1
4.0
0
A
5.5
3.8
4
A
1
5. Nurses break
down large
tasks into
smaller ones
that can more
easily be
accomplished
by unit
members.
3.5
9
A
2
3.5
2
A
2.5
3.5
7
A
1
3.6
9
A
3
4.0
0
A
5.5
3.8
A
3
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
51 ISSN 2704-3568
6. Nurses
organize work
load to facilitate
client care.
3.4
6
O
8
3.3
2
O
7
3.4
2
O
8
3.7
1
A
2
4.0
0
A
5.5
3.8
1
A
2
7. Nurses utilize
all available
resources to
support client
care.
3.5
6
A
3
3.5
2
A
2.5
3.5
5
A
2
3.6
2
A
6
4.0
0
A
5.5
3.7
6
A
6
8. Nurses work
a number of
successive days
with a client to
ensure that there
is time to
formulate and
evaluate a plan
of care.
3.4
4
O
9
3.2
4
O
9.5
3.3
8
O
9
3.4
9
O
9
4.0
0
A
5.5
3.6
7
O
9
9. Nurses are
able to finish
work
assignment on
time.
3.4
7
O
6.5
3.4
8
O
5
3.4
8
O
6
3.3
8
O
10
4.0
0
A
5.5
3.6
O
10
10. Nurses have
job satisfaction
and fulfilment
in giving quality
patient care.
3.5
4
A
4
3.5
2
A
2.5
3.5
4
A
4
3.6
4
A
5
4.0
0
A
5.5
3.7
7
A
5
Composite
Mean 3.4
9
Oft
en
3
.40
Oft
en
3
.47
Oft
en
3
.60
7
Alw
ay
s
4
.00
Alw
ay
s
3
.75
Alw
ay
s
Legend: A=always; O=often; R=rarely; Never
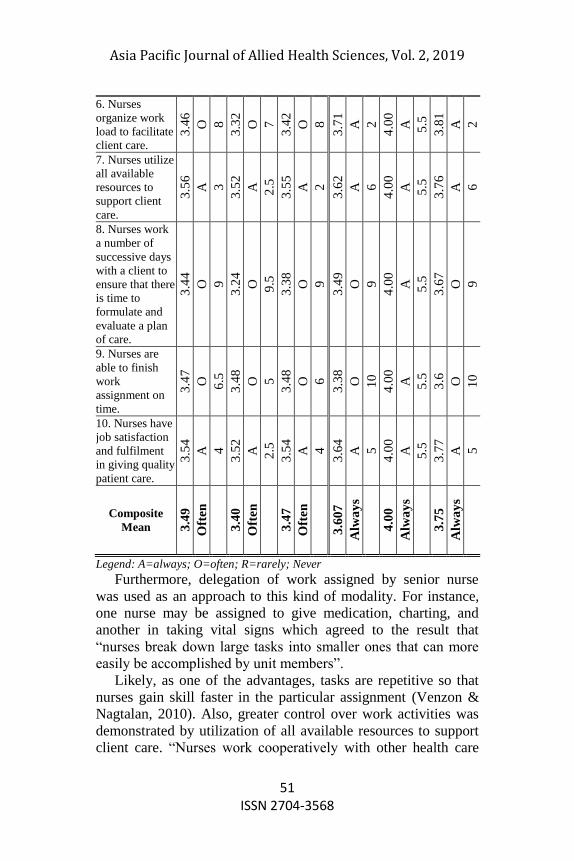
Furthermore, delegation of work assigned by senior nurse
was used as an approach to this kind of modality. For instance,
one nurse may be assigned to give medication, charting, and
another in taking vital signs which agreed to the result that
―nurses break down large tasks into smaller ones that can more
easily be accomplished by unit members‖.
Likely, as one of the advantages, tasks are repetitive so that
nurses gain skill faster in the particular assignment (Venzon &
Nagtalan, 2010). Also, greater control over work activities was
demonstrated by utilization of all available resources to support
client care. ―Nurses work cooperatively with other health care

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
52 ISSN 2704-3568
members to maximize time use‖ since, in functional nursing,
nurses could be able to learn to work fast which could possibly
accomplished work in shortest time as possible, therefore they
can have spare time to help others in medical team. Williams and
Wilkins (2009) cited that due to the fact that because some
workers feel unchallenged and under stimulated in their roles,
functional nursing also may result in own job satisfaction was
similar to what respondents perceived, because according to
them, nurses always gain job satisfaction and fulfilment in giving
quality patient care. At the last spot, ―nurses are adequate in
number to meet patient’s needs‖ in which most of the
respondents experienced it frequently (often) as evidenced by
weighted mean of 3.26 respectively. This implies what Venzon
and Nagtalan (2010) mentioned that functional method is best
system that can be used when there are many patients and
professional nurses are few. Overall, in functional nursing care,
nurses often experienced quality management with the
composite mean of 3.47.
Meanwhile, the respondents in primary nursing practiced
quality management in delivery of care at all times or
always(3.75).To dissect the findings, the respondents in primary
nursing derived that ―nurses work cooperatively with other
health care members to maximize time use‖ as the top item with
weighted mean of 3.73 among statements under management of
care. The result agreed to Carter and colleagues (2012) report
that delivery of collaborative services by an inter professional
team will assist to better meet patients’ needs and has potential
to improve patient outcomes. The clear communication among
all members of the health team is the fundamental responsibility
of the nurses in the primary nursing care model. Since, there is
high in authority, accountability an autonomy of nurses in this
method, nurses communicates directly to health care team to
facilitate coordination in patient care management. Hence,
primary care nurses directs patient plan of care within the hours
of duty, ―nurses can organize work load to facilitate client care‖
to be fulfilled within the working hours. This is supported by
Venzon and Nagtalan (2010), in which the primary nurse
assesses the patient’s needs for care, sets care goals, writes a
nursing care plan, evaluates the outcomes of care, and makes the

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
53 ISSN 2704-3568
necessary changes or adjustments as necessary. However, as
experienced by the respondents, the shortage of nurses in the
institution could affect the nurse’s number of successive days
with a client to ensure that there is time to formulate and
evaluate a plan of care. In addition, the heavy nursing workload
due to scarcity of nurses collaborates to what Gurses (2011)
identified, in which, it affects the time that a nurse can allot to
various tasks. Therefore, nurses may not have sufficient time to
perform tasks within the span of duty. That is the reason why
nurses often finish work assignment on time as perceived by the
respondents.
In general, there were differences in approach when it comes
to the administration of both functional and primary nursing care
modalities. Also, as what obtained from the findings, primary
nursing is greater than functional nursing care modality. In terms
of quality management of delivery of care, primary nursing was
always experienced by the respondents while functional nursing,
often experienced by the respondents.
Table 2.4. Summary of Aspects in Delivery of Care in
Functional and Primary Nursing Care Modalities
Functional
Nursing Care
Primary Nursing
Care Overall
W
M VI R
W
M VI R
W
M VI R
Compete
ncy in the
Delivery
of Care
3.6
6
Highly
Compet
ent
1 3.7
6
Highly
Compet
ent
1
3.7
1
Highly
Compet
ent
1
Effective
ness and
Efficienc
y in the
Delivery
of Care
3.5
4
Highly
Effecti
ve
2 3.8
Highly
Effectiv
e
2
3.6
7
Highly
Effectiv
e
2
Managem
ent in the
Delivery
of Care
3.4
7 Often 3
3.7
5 Always 3
3.6
1
Always
(All the
time)
3
Composit
e Mean
3.5
6
3.7
7
3.6
6
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
54 ISSN 2704-3568
Table 2.4 shows the summary of aspects in delivery of care in
functional and primary nursing care modality as perceived by the
respondents within their respective institutions. It revealed that
both functional and primary nursing care in terms of competency
in the delivery of care was highly competent (3.71) which
outranked the two other aspects, since, both of the respondents
under the two modalities of care perceived the abovementioned
aspect as highly competent. Philippine nurses were guided by
nursing laws, both functional and primary nursing proves that
Philippine nurses were highly competent when it comes to the
delivery of care, despite that there were differences in the
methodology. This demonstrates that there is excellence in the
competitiveness of Philippine nurses with the help of nursing
process which adheres to the nurses' national and international
code of ethics. Certainly, this nursing process assists the nurse to
manage each patient’s nursing care intelligently, scientifically
and judiciously (Paulino, 2007).
Furthermore, as supported by Carter [15], includes that a
clear understanding of each healthcare provider’s unique
knowledge, skills or competencies as well as commonalities will
improve understanding of scope of practice, assist with role
delineation, promote the optimal utilization of providers, and
ultimately result in positive outcomes for patients. As a matter of
fact, there are eleven key areas of nursing responsibilities
recognized by the Philippine Regulatory Commission in order to
produce a more competent nurses and establish a standard
nursing practice which were highly competent regardless of
modalities of care that ensure accurate and effective nursing
action for the recovery and wellness of the patients as proven in
the study.
However, primary nursing care(3.76) was greater than
functional nursing care(3.66) in the aspect of competency.
Unlike in functional nursing, primary nursing care registered
nurses were responsible for the total care of a small group of
patients from admission to discharge. Also, the primary nurse
assesses the patient’s needs for care, sets care goals, writes a
nursing care plan, evaluates the outcomes of care, and makes the
necessary changes or adjustments as necessary (Venzon &
Nagtalan, 2010).

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
55 ISSN 2704-3568
Additionally, according to Manthey (2013), the registered
nurse in partnership with the patient, identifies the patient’s
unique health needs and priorities, establishes an individualized
plan of care, provides direct care as appropriate, and
communicates the plan to other members of the team.
Second in ranking was effectiveness and efficiency in the
delivery of care in which both modalities were highly effective.
However, it is clearly seen that primary nursing care (3.80) was
higher than functional nursing care (3.54). Indeed, primary
nursing has come to recognize as a superior method for
providing patient care as reflected by highly effective in most of
the items under the aforementioned aspect (Hayne & Baily,
2004). Henceforth, there is also a need in functional nursing to
apply harmonious integration of knowledge and skill, maintained
and nurtured to ensure each efficiency and effectiveness in
health care by nurses to a patient (Paulino, 2007). The value of
safe nursing practice was greatly implemented in both functional
and primary nursing care modalities. Undeniably, both
functional and primary nursing care modalities were outstanding
in the aspect of effectiveness and efficiency, yet they were
ranked in different patterns, which publicized that Philippine
nursing in both modalities were excellent when it comes to
aforementioned aspect.
Moreover, primary nursing was greater than 0.26 points than
functional nursing in terms of effectiveness and efficiency.
Unlike primary nursing, functional nursing was not fully
maximized since anticipating patient’s needs and providing
patient care were both efficient and not highly efficient based on
the results that reflect to the disadvantages. This same goes to
primary nursing that, on the other hand, was only effective in the
implementation of high degree of autonomy in clinical decision
making as perceived by the respondents. However, it does not
greatly affect the composite mean due to the fact that the primary
method required high degree of responsibility and autonomy that
the implementation became challenging.
Lastly, functional nursing care nurses oftentimes practiced
quality management (3.47), whereas, the respondents in primary
nursing care always experienced the aforementioned aspect as
accounted by the result of 3.75. Although as mentioned by Jost
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
56 ISSN 2704-3568
et al. (2010 that nursing care delivery model, informed by values
and beliefs, has been described as a structured approach for
organizing and providing nursing care to clients. Even though
functional and primary were under nursing care delivery model,
there were differences in approach when it comes to the
management of both nursing care modalities. Functional
modality is task-oriented while primary modality directs care to
the patient.
Furthermore, according to Williams and Wilkins (2009),
primary nursing, also known as relationship-based nursing, uses
some of the concepts of total patient care, and this is one type of
patient care delivery that requires a one-to-one relationship
between a registered nurse and a patient, with responsibility for
planning and managing care clearly established. Meanwhile, in
functional nursing, breaking down tasks, utilizing available
sources, working cooperatively in health care team, and having
job satisfaction were only those perceived by the respondents to
be done always, proven by the weighted mean between 3.50-
4.00, while the rest are experienced oftentimes which also
reflected in the overall result. It is a fact that functional nursing
was developed of tasks analysis and proper division of the
nursing workload (Deutschendorf, 2006).
In the aspect of management, primary nursing administered
the system well than functional nursing as grounded by the
result. As deliberated from the result, primary nursing excels
most in all three aspects of delivery of care, known to be a
superior method in providing patient care.
Table 3 shows the differences between primary and
functional care modalities. Based from the result, there are no
significant differences between functional and primary nursing
care in terms of effectiveness and efficiency and competency in
the delivery of care since the computed p-values greater than
0.05 level of significance. However, there are differences
between functional and primary nursing care in terms of
management in the delivery care since the computed p-value is
less than 0.05 level of significance. Thus, the hypothesis that
there are no differences between functional and primary nursing
care in terms of Management in the Delivery of Functional Care
is rejected.

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
57 ISSN 2704-3568
It is clearly seen from the table that there were no substantial
variance in both models of care (functional and primary) in
relation to effectiveness and efficiency and; competency in the
delivery of care. As mentioned by Jost et al. (2010), nursing
care delivery model, informed by values and beliefs, has been
described as a structured approach for organizing and providing
nursing care to clients. Even though functional and primary were
under nursing care delivery model, there were differences in
approach when it comes to the management of both nursing care
modalities. As Koloroutis (2004) mentioned that in functional
care, nursing assignments are task-based, nurses are assigned to
tasks rather than patients, while, in primary care, nurse
assignments are patient-based to ensure continuity of care.
Therefore, nurse approach management in functional and
primary nursing models in different ways as proven by the result
of computed p-value is less than 0.05 level of significance. It
was noted that when it comes to management of delivery of care,
there was a substantial variance between the two models of care.
Table 3. Differences between the Primary and Functional
Nursing Care Modalities
Mean F-value p-value
Effectiveness and Efficiency
in the Delivery of Care
Functional 3.53 3.57* 0.06
Primary 3.80
Competency in the Delivery
of Care
Functional 3.66 2.52 0.12
Primary 3.76
Management in the Delivery
of Care
Functional 3.47 7.436* 0.01
Primary 3.75
Legend:* Significant at p-value < 0.05
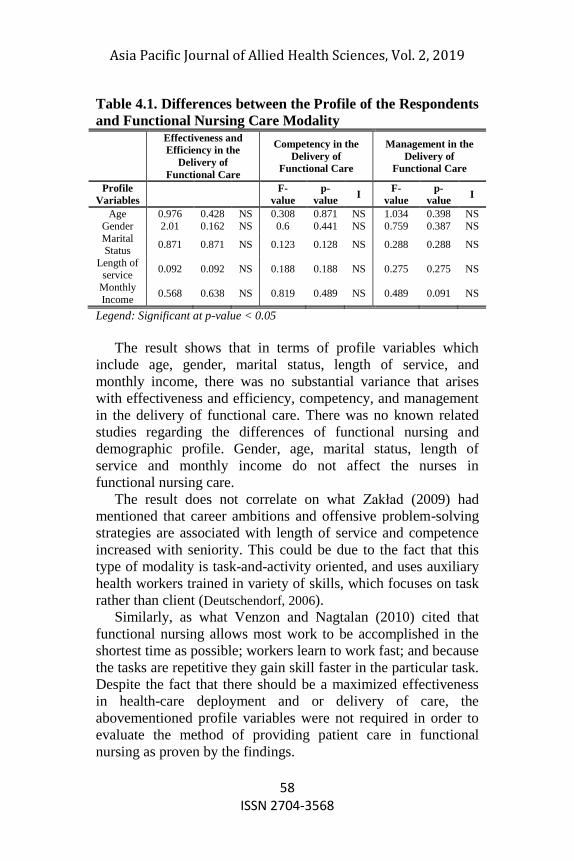
Table 4.1 presents the differences between the profile of the
respondents and functional nursing care modality. It can be
observed from the table that effectiveness and efficiency in the
delivery of functional care, competency in the delivery of
functional care and management in the delivery of functional
care have no significant difference with the profile variable since
the computed p-values greater than 0.05 level of significance.
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
58 ISSN 2704-3568
Table 4.1. Differences between the Profile of the Respondents
and Functional Nursing Care Modality
Effectiveness and
Efficiency in the
Delivery of
Functional Care
Competency in the
Delivery of
Functional Care
Management in the
Delivery of
Functional Care
Profile
Variables
F-
value
p-
value I
F-
value
p-
value I
Age 0.976 0.428 NS 0.308 0.871 NS 1.034 0.398 NS
Gender 2.01 0.162 NS 0.6 0.441 NS 0.759 0.387 NS
Marital Status
0.871 0.871 NS 0.123 0.128 NS 0.288 0.288 NS
Length of service
0.092 0.092 NS 0.188 0.188 NS 0.275 0.275 NS
Monthly
Income 0.568 0.638 NS 0.819 0.489 NS 0.489 0.091 NS
Legend: Significant at p-value < 0.05
The result shows that in terms of profile variables which
include age, gender, marital status, length of service, and
monthly income, there was no substantial variance that arises
with effectiveness and efficiency, competency, and management
in the delivery of functional care. There was no known related
studies regarding the differences of functional nursing and
demographic profile. Gender, age, marital status, length of
service and monthly income do not affect the nurses in
functional nursing care.
The result does not correlate on what Zakład (2009) had
mentioned that career ambitions and offensive problem-solving
strategies are associated with length of service and competence
increased with seniority. This could be due to the fact that this
type of modality is task-and-activity oriented, and uses auxiliary
health workers trained in variety of skills, which focuses on task
rather than client (Deutschendorf, 2006).
Similarly, as what Venzon and Nagtalan (2010) cited that
functional nursing allows most work to be accomplished in the
shortest time as possible; workers learn to work fast; and because
the tasks are repetitive they gain skill faster in the particular task.
Despite the fact that there should be a maximized effectiveness
in health-care deployment and or delivery of care, the
abovementioned profile variables were not required in order to
evaluate the method of providing patient care in functional
nursing as proven by the findings.
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
59 ISSN 2704-3568
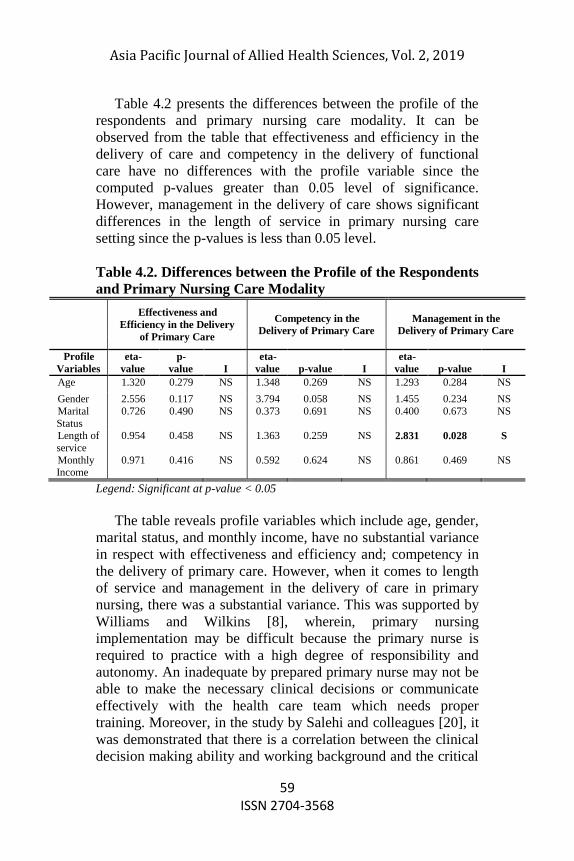
Table 4.2 presents the differences between the profile of the
respondents and primary nursing care modality. It can be
observed from the table that effectiveness and efficiency in the
delivery of care and competency in the delivery of functional
care have no differences with the profile variable since the
computed p-values greater than 0.05 level of significance.
However, management in the delivery of care shows significant
differences in the length of service in primary nursing care
setting since the p-values is less than 0.05 level.
Table 4.2. Differences between the Profile of the Respondents
and Primary Nursing Care Modality
Effectiveness and
Efficiency in the Delivery
of Primary Care
Competency in the
Delivery of Primary Care
Management in the
Delivery of Primary Care
Profile
Variables
eta-
value
p-
value I
eta-
value p-value I
eta-
value p-value I
Age 1.320 0.279 NS 1.348 0.269 NS 1.293 0.284 NS
Gender 2.556 0.117 NS 3.794 0.058 NS 1.455 0.234 NS
Marital
Status
0.726 0.490 NS 0.373 0.691 NS 0.400 0.673 NS
Length of
service
0.954 0.458 NS 1.363 0.259 NS 2.831 0.028 S
Monthly Income
0.971 0.416 NS 0.592 0.624 NS 0.861 0.469 NS
Legend: Significant at p-value < 0.05
The table reveals profile variables which include age, gender,
marital status, and monthly income, have no substantial variance
in respect with effectiveness and efficiency and; competency in
the delivery of primary care. However, when it comes to length
of service and management in the delivery of care in primary
nursing, there was a substantial variance. This was supported by
Williams and Wilkins [8], wherein, primary nursing
implementation may be difficult because the primary nurse is
required to practice with a high degree of responsibility and
autonomy. An inadequate by prepared primary nurse may not be
able to make the necessary clinical decisions or communicate
effectively with the health care team which needs proper
training. Moreover, in the study by Salehi and colleagues [20], it
was demonstrated that there is a correlation between the clinical
decision making ability and working background and the critical

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
60 ISSN 2704-3568
thinking and clinical decision making in nurse. Likely, it was
found that career ambitions and offensive problem-solving
strategies correlate with length of service.
Nurses with the shortest length of service were least active in
coping with problems revealing that competence increased with
seniority (Zakład, 2009). It seems that as the nurses have higher
work experience, their clinical decision making ability and
management of delivery of care improves. Thus, if there is an
increase in experience, the primary nurse will be likely to be
more autonomous in providing patient care.
Proposed Action Plan in Enhancing Primary and Functional
Nursing Care Modalities
The rationale for this proposed action plan is to improve safe,
competent, quality care that meets client needs and maximize
client outcomes across the continuum of care; to utilize health-
care providers effectively through maximizing the effectiveness
of health-care worker deployment and or delivery of care; to
reflect an understanding of nursing work processes while also
considering the evolving role of nurses in care delivery models;
thus, to promote quality work environments. This focuses more
on functional nursing care since this is the weakness of the study.
CONCLUSIONS AND RECOMMENDATION
The female dominates the respondents in primary and
functional care settings. Most of the respondents were single
which greatly reflects the age of the respondents which is in their
early 20’s. Moreover, the minimum salary for nurses was Php
3,000-10,000 for the length of service up to 5 years. Primary
nursing excel more than functional nursing in all three aspects of
care delivery. Primary nursing care, when it comes to
management of delivery of care has a substantial variance with
functional nursing. Both modalities had no difference when it
comes to competency, efficiency and effectiveness in delivery of
care. Profile variables which include age, gender, marital status,
length of service, and monthly income, and functional nursing
had no substantial variance with effectiveness and efficiency,
competency, and management in the delivery of functional care.
This was almost the same in primary nursing modality except
Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
61 ISSN 2704-3568
that there is difference between length of service and
management which requires practice and training to execute the
primary nursing properly. Action plan in enhancing primary and
functional nursing care models was developed for future
implementation.
It is recommended that the Department of Health may
consider primary nursing modality as the standard hospital
setting and serve basis to deploy nurses appropriately without
compromising both the nurse and patient. Hospitals may
implement the utilization of proposed action plan which may be
appropriate for the institution. Further research may be
conducted to measure the extent to which the benefits, or
potential benefits, of the model of care will be sustained in the
future.
REFERENCES Carter, R., Oelke, N., Wilhelm, A., Jackson, K., Suter, E. (2012).
―Optimizing Collaborative Practice of Nurses in Primary Care
Settings‖. 64
Cherry, B. and Jacob, S. (2014). Contemporary Nursing, Issues, Trends,
& Management, 6th Edition. 324-350
Dadich, K. (2007). Care Delivery Strategies. (12) 241-265
Descriptive method. (2014). Retrieved March 10, 2014 from
http://www.sagepub.com/
Deutschendorf, A. (2006). Models of Care Delivery.In Huber, D.
Leadership and Nursing Care Management, 3rd ed. 16 (315-
335)
Gurses, A. & Carayon, P. (2011). Nursing Workload and Patient
Safety—A Human Factors Engineering Perspective. 30.
Harris, A. and McGillis Hall, L. (2012) .Evidence to Inform Staff Mix
Decision-making: A Focused Literature Review, 5-23.
Hayne, A. & Baily, Z. (2004). Nursing Administration of Critical
Care.81-163.
Jost, S., Bonnell, M., Chacko, S., & Parkinson, D. (2010).Integrated
primary nursing: A care delivery model for the 21st-century
knowledge worker.Nursing Administration Quarterly, 34(3),
208-216.
Koloroutis, M. (2004).Relationship-Based Care: A Model for
Transforming Practic. 125-150
Likert scale. (2014). Retrieved May 25, 2014, from
http://www.academia.edu/

Asia Pacific Journal of Allied Health Sciences, Vol. 2, 2019
62 ISSN 2704-3568
Llanes, M. (2011). Thesis: Core Competency Standards for Nursing
Practice in the Philippines: Development and Validation.
University of Sto.Tomas.
Manthey, M. (2013).The Practice of Primary Nursing, 2nd Edition.
Maratning, A. (2004). Thesis: Nurses Spiritual Well-Being and Extent
of Patients’ Satisfaction in selected Hospitals of Kalimutan
Indonesia: Basis for development Spiritual Health Care-
Program. University of Sto.Tomas.
Paulino, A. (2007). Thesis: The nurses delivery of Quality Health Care
Services in a University Hospital: Basis For improving
Administrative Approaches. University of Santo Tomas.
Salehi, Sh., and colleagues (2007).Critical Thinking and Clinical
Decision Making in Nurse. Iranian Journal of Nursing and
Midwifery Research Winter, 12 (1), 13
Thompson, K., and Vertein, D. (2008).Rethinking Gender Stereotypes
in Nursing, Minority Nurse Journal.
Venzon, L. & Nagtalan, J. (2010). Nursing Management Towards
Quality Care. 4th ed. 82-93.
Williams and Wilkins (2009). Leadership Roles and Management:
Functions in Nursing, 6th ed. 9 (186-408)
Zakład, K. (2009). Length of Service as a Nurse: Continuing to Burnout.
PubMed. 55(2):83-9
Related Documents











