North West Podiatric Foundation Summer Surgical Seminar – CLONTARF CASTLE, Dublin – 15 th August 2008 David R Tollafield, Consultant Podiatric Surgeon Podiatric Surgical Services Walsall NHS Community Trust, West Midlands, U.K. Adapted for the Consultant and clinical governance Group Midlands Region. Solihull 27 th November 2008

North West Podiatric Foundation Summer Surgical Seminar – CLONTARF CASTLE, Dublin – 15 th August 2008 David R Tollafield, Consultant Podiatric Surgeon.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
North West Podiatric Foundation Summer Surgical Seminar
– CLONTARF CASTLE, Dublin – 15th August 2008
David R Tollafield, Consultant Podiatric SurgeonPodiatric Surgical Services Walsall NHS Community Trust, West Midlands, U.K.
Adapted for the Consultant and clinical governance GroupMidlands Region. Solihull 27th November 2008

“I dressed the wound. God healed it.”
Illustrated: Primary wound healing with subcuticular PDS 4/0 [author]
What do you do when you What do you do when you have a problem...have a problem...Then you have another?Then you have another?

Case history management
• Mechanical• Nutritional• Age and health• Compliance• Social• Physical• Surgeon technique• Factors outside surgeon control
Factors disrupting normal surgical wounds
Negative effects of delayed wound healing
Economic factors patient loss of work
Drug supplyDressingsEscalate
laboratory testsImagingAdmission Theatre
Pyscho-social drug side effectssocial morbidityDepression &
suicideComplex regional
pain
36 sequelae?
Wound problems
Podiatric audit in surgery and clinical outcome measurementSociety of Chiropodists & Podiatrists(c)

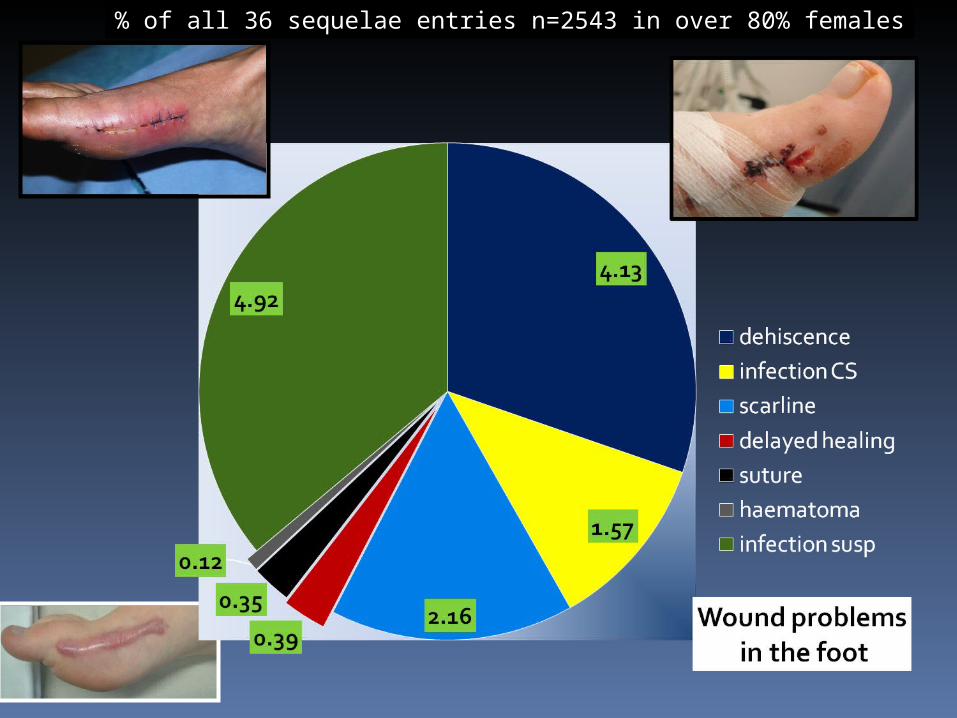
% of all 36 sequelae entries n=2543 in over 80% females

Sutures and materials
FREQUENCY OF REPAIR TECHNIQUES
Simple interrupted 38-50% Simple running 37-42% Subcuticular 28% Vertical mattress 3-8%
Nylon 51% Polypropylene44% Polyglactin 910 73%
Abdullah-Tawfik et al 2007
Adams et al 2006
Frederick J et al 1996Poly-p-dioxanon
Multinucleated foreign giant cells without infection

Sutures technique and Sequela
Sequela N=1000
% One layersuture
% TwoLayersutures
%
Tissue reactivity
335 33.5 177 31.6 158 35.9
Dehiscence 65 6.4 30 5.4 34 7.7
Infection 17 1.7 9 1.6 8 1.8
Gabrielli, et al 2001 No antibiotics were used in this trial
0.35
1.2
4.1

Comparing different operations: healing versus infection Proven.Source PASCOM Four centres same surgeon
Known's: haematoma causes problems!Known's: haematoma causes problems!

Signs of poor healing are obvious, The decision to undertake surgical intervention may not be.
Type 1 SADWound
Management of wounds with directional
advancement flaps
Vaughan et al 2006Steristrips n=60

24 days
Dystrophiccalcification
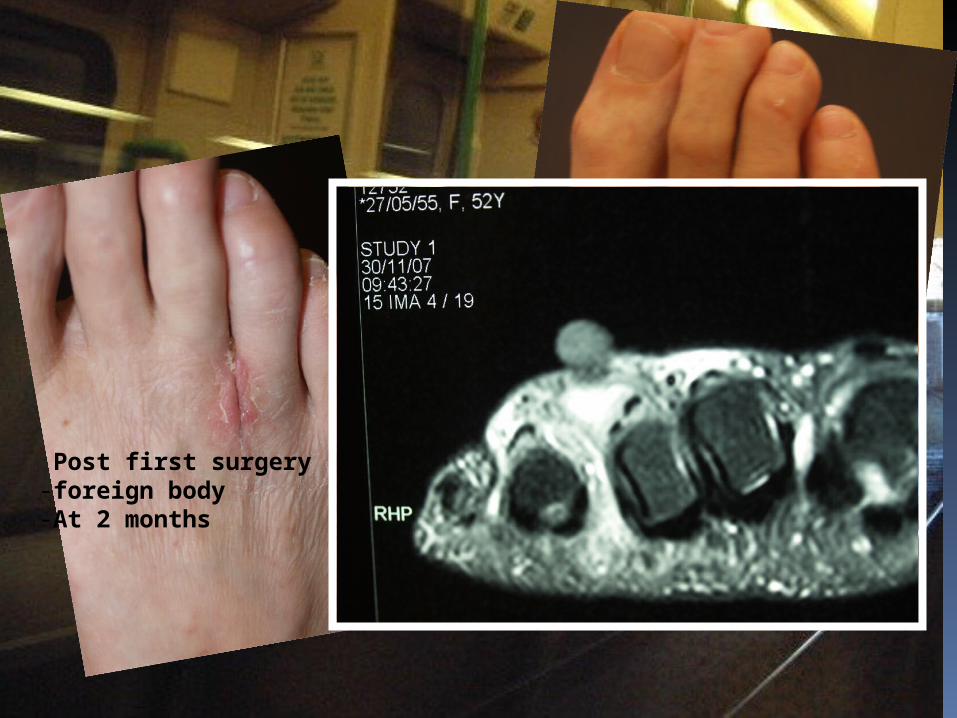
Post first surgery-foreign body-At 2 months

SecondRevisionarySurgery
Zonal hist0logyZonal hist0logy
necrosis
Org. haem
FBGC

39 days
48 days
31 days
2 days
5days
21 days
Secondary intention healing 48 days following management of wound

-0.5
0
0.5
1
1.5
2
2.5
3
3.5
0 50 100 150 200
uncomplicated healing
0
0.5
1
1.5
2
2.5
3
3.5
0 50 100 150 200 250 300
complicated healing
Primary surgery
SAD system (based) wound classificationWithout infection
0 skin intact
1Skin and subcutaneous tissues
2Tendon exposed
3Joint space
Macfarlane & Jeffcoate 1999 modification of San Antonio/Texas system
Primary surgery
Case 1
Case 2
48 days
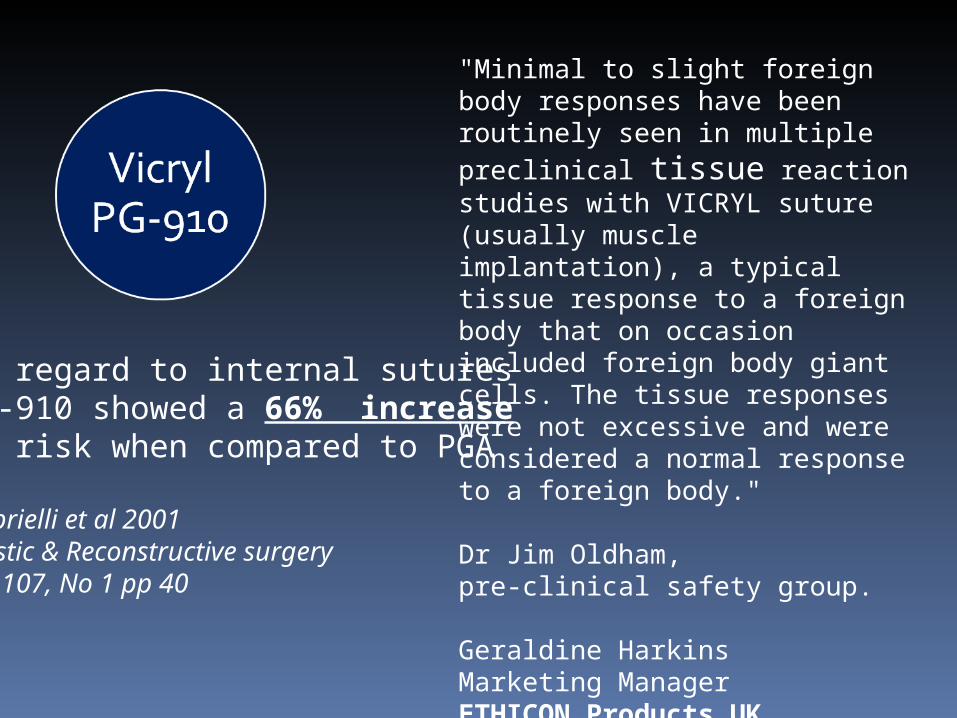
"Minimal to slight foreign body responses have been routinely seen in multiple preclinical tissue reaction studies with VICRYL suture (usually muscle implantation), a typical tissue response to a foreign body that on occasion included foreign body giant cells. The tissue responses were not excessive and were considered a normal response to a foreign body." Dr Jim Oldham, pre-clinical safety group. Geraldine Harkins Marketing Manager ETHICON Products UK August 2008
In regard to internal suturesPg-910 showed a 66% increaseIn risk when compared to PGA
Gabrielli et al 2001Plastic & Reconstructive surgeryVol.107, No 1 pp 40
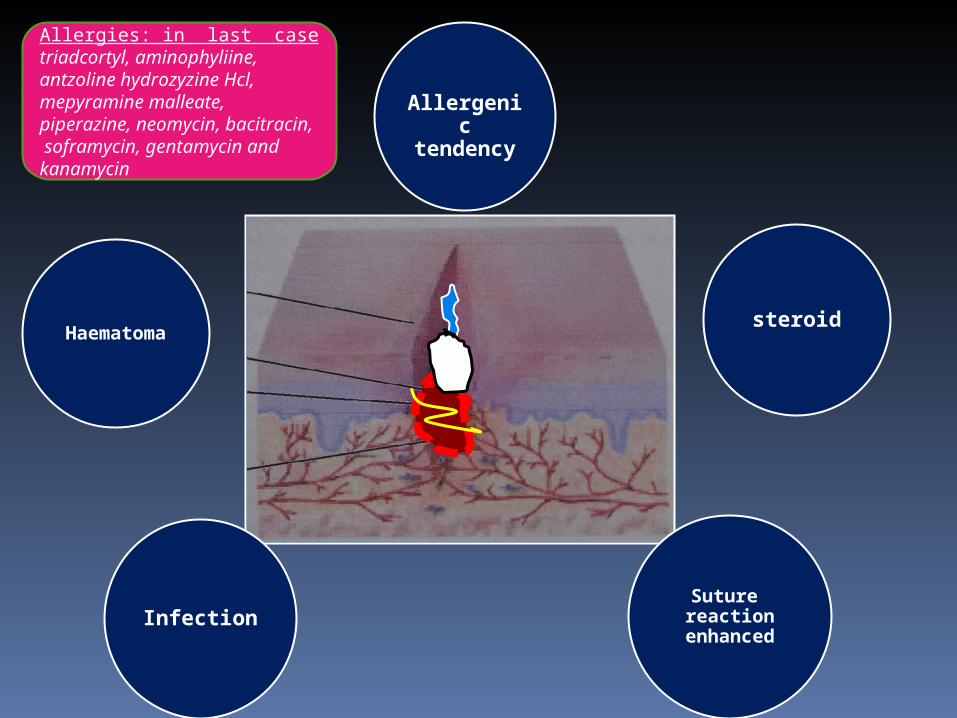
Allergenic tendency
steroidHaematoma
InfectionSuture reaction
enhanced
Allergies: in last case triadcortyl, aminophyliine, antzoline hydrozyzine Hcl, mepyramine malleate, piperazine, neomycin, bacitracin, soframycin, gentamycin and kanamycin

Conclusion
•We need to be clearer when describing wound problems
•Not all wounds lead to complications
•Haematomata may not be obvious for 21 days
•Steroids may compound haematoma effects
•PG-910 reaction is accelerated with haematoma
•Infection remains unproven
Thank you you
Murphy’s Law
“If all seems to be going well you probably don’t know what the hell is going on”.
Related Documents











