Nonverbal expressive behaviour in schizophrenia and social phobia Jonathan Del-Monte a,b,c,n , Stéphane Raffard a,b , Robin N. Salesse c , Ludovic Marin c , Richard C. Schmidt d , Manuel Varlet c , Benoît G. Bardy c , Jean Philippe Boulenger b,e , Marie Christine Gély-Nargeot a , Delphine Capdevielle b,e a Epsylon, Laboratory Dynamic of Human Abilities & Health Behaviors, Department of Sport Sciences, Psychology and Medicine, University of Montpellier & St-Etienne, France b University Department of Adult Psychiatry, Hôpital de la Colombière, CHU Montpellier, Montpellier-1 University, Montpellier, France c Movement to Health Laboratory, EuroMov, Montpellier-1 University, Montpellier, France d Department of Psychology, College of the Holy Cross, Worcester, MA, USA e INSERM U-1061, Montpellier, France article info Article history: Received 4 December 2012 Received in revised form 24 May 2013 Accepted 27 May 2013 Keywords: Nonverbal expressive behaviours Schizophrenia Social phobia Negative symptoms Social functioning abstract Expressive behaviour plays a crucial role in the success of social interactions. Abnormality of expressive behaviour has been reported in interpersonal interactions of patients suffering from schizophrenia and social phobia, two debilitating mental disorders with important social deficits. However, no study has compared the expressive behaviour in these two disorders. Thirty schizophrenia patients, 21 social phobia patients and 30 healthy controls were evaluated and compared on expressive, cognitive and clinical dimensions. Expressive behaviour was assessed using the Motor Affective subscale of the Motor- Affective-Social-Scale (MASS). Covariables include the Positive and Negative Syndrome Scale (PANSS), the anxiety level Liebowitz-Social-Anxiety-Scale (LSAS) and cognitive tasks. After controlling for depression, schizophrenia and social phobia patients both exhibited significantly fewer expressive behaviours compared to healthy controls. Moreover, our results showed specific signatures: schizophrenia patients performed fewer spontaneous gestures (hand gestures and smiles) whereas social phobia patients had an impaired ability to produce voluntary smiles in comparison to healthy controls. Interestingly, poor social functioning was significantly correlated with a decrease of expressive behaviour for schizophrenia patients. Expressive behaviour is impaired in different ways in social phobia and schizophrenia and is associated in schizophrenia with poorer social functioning. The Motor Affective subscale of the MASS is an interesting tool for assessing the dysfunction of interpersonal expressive behaviour in mental disorders. & 2013 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Nonverbal expressive behaviour is a critical feature of success- ful social interaction and interpersonal rapport (Krauss et al., 1996). Expressive gestures that accompany speech play a funda- mental role in human communication, particularly to improve communication's quality, to modulate listener's actions and to convey information beyond that of the speakers' words (Ekman and Friesen, 1969; Goldin-Meadow, 1999; Schmidt and Richardson, 2008). Social deficits are a feature of many mental disorders, such as schizophrenia and social phobia (American Psychiatry Association, 2004), including many symptoms such as emotional (Phillips and Seidman, 2008; Bourke et al., 2012) or social functioning deficits (Sidlova et al., 2011; Panayiotou and Karekla, 2012). Past studies have attempted to explain social interaction disorders through social cognition deficits in both schizophrenia (Green et al., 2008) and social phobia (Tibi-Elhanany and Shamay- Tsoory, 2011). Brüne et al. (2009) have explored links between social cognition and nonverbal expressiveness in schizophrenia spectrum disorders. Patient's non-verbal behaviours were assessed using the Ethological Coding System for Interviews (ECSI). Results showed that schizophrenia patients had fewer prosocial beha- viours compared to healthy controls and a partial correlation existed between reduced prosocial behaviour and social compe- tence especially as indexed by the false-belief mentalising task for the schizophrenia group. Impairment in expressiveness thus seems to be a fundamental component of the social interaction disorder in schizophrenia. However, too few studies take into account the importance of the expressive behaviour in mental disorders with social interaction Contents lists available at ScienceDirect journal homepage: www.elsevier.com/locate/psychres Psychiatry Research 0165-1781/$ - see front matter & 2013 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.psychres.2013.05.034 n Correspondence to: Laboratory Epsylon EA 4556, Laboratory Dynamics of Human Abilities & Health Behaviors, Department of Medicine, Subject and Society Sciences, Sport Sciences, University of Montpellier and St-Etienne, 4 Boulevard Henri IV, 34000 Montpellier, France. Tel.: +33 411 757065. E-mail address: [email protected] (J. Del-Monte). Psychiatry Research 210 (2013) 29–35

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Psychiatry Research 210 (2013) 29–35
Contents lists available at ScienceDirect
Psychiatry Research
0165-17http://d
n CorrHumanScienceHenri IV
E-m
journal homepage: www.elsevier.com/locate/psychres
Nonverbal expressive behaviour in schizophrenia and social phobia
Jonathan Del-Monte a,b,c,n, Stéphane Raffard a,b, Robin N. Salesse c, Ludovic Marin c,Richard C. Schmidt d, Manuel Varlet c, Benoît G. Bardy c, Jean Philippe Boulenger b,e,Marie Christine Gély-Nargeot a, Delphine Capdevielle b,e
a Epsylon, Laboratory Dynamic of Human Abilities & Health Behaviors, Department of Sport Sciences, Psychology and Medicine,University of Montpellier & St-Etienne, Franceb University Department of Adult Psychiatry, Hôpital de la Colombière, CHU Montpellier, Montpellier-1 University, Montpellier, Francec Movement to Health Laboratory, EuroMov, Montpellier-1 University, Montpellier, Franced Department of Psychology, College of the Holy Cross, Worcester, MA, USAe INSERM U-1061, Montpellier, France
a r t i c l e i n f o
Article history:Received 4 December 2012Received in revised form24 May 2013Accepted 27 May 2013
Keywords:Nonverbal expressive behavioursSchizophreniaSocial phobiaNegative symptomsSocial functioning
81/$ - see front matter & 2013 Elsevier Irelandx.doi.org/10.1016/j.psychres.2013.05.034
espondence to: Laboratory Epsylon EA 455Abilities & Health Behaviors, Department of Ms, Sport Sciences, University of Montpellier, 34000 Montpellier, France. Tel.: +33 411 757ail address: [email protected] (J.
a b s t r a c t
Expressive behaviour plays a crucial role in the success of social interactions. Abnormality of expressivebehaviour has been reported in interpersonal interactions of patients suffering from schizophrenia andsocial phobia, two debilitating mental disorders with important social deficits. However, no study hascompared the expressive behaviour in these two disorders. Thirty schizophrenia patients, 21 socialphobia patients and 30 healthy controls were evaluated and compared on expressive, cognitive andclinical dimensions. Expressive behaviour was assessed using the Motor Affective subscale of the Motor-Affective-Social-Scale (MASS). Covariables include the Positive and Negative Syndrome Scale (PANSS), theanxiety level Liebowitz-Social-Anxiety-Scale (LSAS) and cognitive tasks. After controlling for depression,schizophrenia and social phobia patients both exhibited significantly fewer expressive behaviourscompared to healthy controls. Moreover, our results showed specific signatures: schizophrenia patientsperformed fewer spontaneous gestures (hand gestures and smiles) whereas social phobia patients had animpaired ability to produce voluntary smiles in comparison to healthy controls. Interestingly, poor socialfunctioning was significantly correlated with a decrease of expressive behaviour for schizophreniapatients. Expressive behaviour is impaired in different ways in social phobia and schizophrenia and isassociated in schizophrenia with poorer social functioning. The Motor Affective subscale of the MASS isan interesting tool for assessing the dysfunction of interpersonal expressive behaviour in mentaldisorders.
& 2013 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Nonverbal expressive behaviour is a critical feature of success-ful social interaction and interpersonal rapport (Krauss et al.,1996). Expressive gestures that accompany speech play a funda-mental role in human communication, particularly to improvecommunication's quality, to modulate listener's actions and toconvey information beyond that of the speakers' words (Ekmanand Friesen, 1969; Goldin-Meadow, 1999; Schmidt and Richardson,2008). Social deficits are a feature of many mental disorders, suchas schizophrenia and social phobia (American PsychiatryAssociation, 2004), including many symptoms such as emotional
Ltd. All rights reserved.
6, Laboratory Dynamics ofedicine, Subject and Society
and St-Etienne, 4 Boulevard065.Del-Monte).
(Phillips and Seidman, 2008; Bourke et al., 2012) or socialfunctioning deficits (Sidlova et al., 2011; Panayiotou and Karekla,2012). Past studies have attempted to explain social interactiondisorders through social cognition deficits in both schizophrenia(Green et al., 2008) and social phobia (Tibi-Elhanany and Shamay-Tsoory, 2011). Brüne et al. (2009) have explored links betweensocial cognition and nonverbal expressiveness in schizophreniaspectrum disorders. Patient's non-verbal behaviours were assessedusing the Ethological Coding System for Interviews (ECSI). Resultsshowed that schizophrenia patients had fewer prosocial beha-viours compared to healthy controls and a partial correlationexisted between reduced prosocial behaviour and social compe-tence especially as indexed by the false-belief mentalising task forthe schizophrenia group.
Impairment in expressiveness thus seems to be a fundamentalcomponent of the social interaction disorder in schizophrenia.However, too few studies take into account the importance of theexpressive behaviour in mental disorders with social interaction

J. Del-Monte et al. / Psychiatry Research 210 (2013) 29–3530
deficits. Yet, reductions in expressive behaviour have beenreported in patients suffering from schizophrenia, in the expres-sions of facial affect or in body movements (Trémeau et al., 2005;Brüne et al., 2009), and from social phobia, in facial expressions oreye gaze (Melfsen et al., 2000; Schneier et al., 2011). Despite thesebehavioural similarities, no study has explicitly compared expres-sive behaviour deficits and how they appear in these two dis-orders. Knowing whether expressive behaviour deficits representthe behavioural signature of similar symptoms and clinical causes,or not, seems to be particularly relevant in understanding andtreating schizophrenia and social phobia. Consequently, it isfundamental to assess and to compare the expressive behaviourdimension of social interactions in both schizophrenia and socialphobia.
Concerning schizophrenia, several studies have demonstrated areduction in expressive behaviour (Trémeau et al., 2005; Brüneet al., 2009). Past research has shown that schizophrenia patientsshow a decrease in spontaneous facial expression (SFE) (Steimer-Krause et al., 1990) and more particularly have fewer spontaneoussmiles in funny situations compared to healthy controls (Henryet al., 2007). SFE was also found to be negatively correlated withnegative symptoms. Other studies have compared SFE in schizo-phrenia patients with SFE in other mental disorders. Bersani et al.(2012) compared facial expressions in schizophrenia and inobsessive-compulsive disorder (OCD). All patients watchedemotion-eliciting video clips while facial activity was videotaped.Results demonstrated that facial expressions were reduced inschizophrenia and OCD compared to healthy controls but notsignificantly different from each other. Earlier, Trémeau et al.(2005) assessed facial expressive behaviours (FEB), includingspontaneous and voluntary facial expressions (VFE) and facialcoverbal gestures, and speech flow in schizophrenia patients,depressed patients and healthy controls. They used a narrativetask in which an emotion was described. Results demonstratedthat schizophrenia patients and depressed patients were impairedin all FEB compared to healthy controls. Schizophrenia patientsand depressed patients were equally impaired in voluntary andspontaneous facial expressions and facial coverbal gestures.However, Trémeau et al. (2005) found that schizophrenia patientsspoke less than the depressed patients; and moreover, in schizo-phrenia, all FEB correlated with an index of negative symptoms.
Other studies have examined body movements, including handand head gestures, during social interactions in schizophrenia.Recently, Lavelle et al. (2012) showed that schizophrenia patientsspeak less and make less use of hand gestures when speakingcompared to healthy controls in a social interaction. Further,results exhibited that reductions in expressiveness in schizophre-nia, seem modulated by the type and the intensity of symptoma-tology. Patients with more positive symptoms used morenonverbal behaviours to demonstrate understanding and providefeedback to their speaking partner. Their partners appeared tocompensate for this by providing fewer of these cues when theywere listening. Patients with more negative symptoms displayedless nodding when listening, thus providing fewer indicators oftheir understanding to their speaking partner. Their partnerappears to respond to this by gesturing more while speaking.However, patients with more negative symptoms also gesturedmore when speaking. The patients may be increasing their use ofgestures while speaking in response to the reduced nonverbalfeedback being displayed by the listening partners. According toauthors, patients' gestures could be used as a possible indicator ofthe interpersonal relationship quality within the interaction. Thisindicator has been also proposed by Mittal et al. (2011), suggestingthat an increased amount of abnormal movement predicts poorersocial functioning in individuals with a high risk for developingschizophrenia.
Despite the fact that expressive behaviours play a fundamentalrole in social interactions (Goldin-Meadow, 1999), few studieshave assessed this dimension in social phobia. Past researchsuggests that adults with social phobia exhibit expressive beha-viour deficits (Schneier et al., 2011). Moukheiber et al. (2010) hasobserved gaze avoidance during social interaction. Also Melfsenet al. (2000) assessed spontaneous and voluntary facial expres-sions in socially anxious children. Children's SFE were covertlyrecorded when they were trying to solve a puzzle and whilewatching a funny movie. Additionally, they were asked to producevoluntary facial expressions (VFE). Results showed that childrenwith social anxiety exhibited fewer SFE and showed poorerperformance in voluntary expression of happiness, surprise andfear. Hence, research suggests that facial and body movementsmight be considered as behavioural indicators of the level ofanxiety.
However, the lack of studies documenting expressive beha-viours in social phobia suggests a need for further investigation ofthis domain. Moreover, often in previous research on expressivebehaviours in schizophrenia and social phobia methodologicalissues have made it difficult to draw valid conclusions. The useof numerous different tools to assess, in laboratory, expressivebehaviours does not allow a reliable comparison between studies.In order to propose a more ecological and more clinical assess-ment of expressive behaviours deficits, Trémeau et al. (2008)developed the Motor-Affective-Social-Scale (MASS) for schizo-phrenia. The first part of this scale, the Motor Affective subscaleof the MASS, is used to assess fundamental expressive deficitsthrough evaluating spontaneous smiles, hand gestures, voluntarysmiles and speech flow. The second part of the MASS assesses thelack of initiation (avolition) through motor retardation, personalhygiene, attendance at groups and verbal interaction. Trémeauet al. (2008) found that the MASS score correlated highly with thePANSS negative symptomatology score. Unfortunately, researchershave not investigated how the MASS relates to measures of socialfunctioning. Investigating such relationships will reveal whether alink exists between problems of social functioning in patients andtheir prosocial expressive behaviour deficits.
The aims of the current study were thus (i) to investigate andcompare expressive behaviours in schizophrenia and social phobiausing the Motor Affective subscale of the MASS. In addition, asnumerous studies have shown a link between cognition function-ing and intrapersonal motor behaviours (Smits-Engelsman andHill, 2012; Mohan et al., 2001), we investigated the relationshipbetween nonverbal expressive behaviours and cognitive andclinical variables in schizophrenia and social phobia. We hypothe-sized that cognitive functioning deficits would be positivelycorrelated with expressive behaviour impairments and that clin-ical variables, such as anxiety level, would be negatively correlatedwith expressive behaviour impairments.
2. Material and method
2.1. Recruitment
Fifty-one patients diagnosed with schizophrenia (n¼30) and social phobia(n¼21), according to DSM-IV-TR, participated in the study. The control groupconsisted of 30 healthy participants. All control participants were community-dwelling adults living in Montpellier, France, and were recruited from localassociative networks. They had no personal history of psychosis nor did any first-degree relative. Exclusion criteria for the controls were a positive history ofneurological or psychiatric disease or the presence of medication intake knownto influence cognition. Controls meeting clinical criteria for major depressiveepisode or anxiety disorder as confirmed using the mini-international neuropsy-chiatric interview (Sheehan et al., 1998) were also excluded. According to thecurrent treating psychiatrist, patients were in the stable phase of the illness definedas having no hospitalizations or changes in housing in the month prior to entering

J. Del-Monte et al. / Psychiatry Research 210 (2013) 29–35 31
the study. All patients were receiving outpatient treatment in the urban commu-nity of Montpellier. Individuals with schizophrenia were receiving antipsychoticmedication at the time of participation in this study. Exclusion criteria for bothgroups were (a) known neurological disease, (b) developmental disability, or(c) substance abuse in the past month. Participants were recruited from theUniversity Department of Adult Psychiatry in Montpellier. The Ethics Committeeof the University Hospital of Montpellier approved the study (CPP Sud Méditér-année III, Montpellier, France, AFSSAPS 2009-A00513-54 24, 07/22/2009).
2.2. Instruments
Subjects were asked to participate in nonverbal expressive behaviour tasks andto complete questionnaires. In the first session, for schizophrenia patients,symptom ratings were obtained using the Positive and Negative Syndrome Scale(PANSS) (Kay et al., 1987) and social functioning was assessed by the modifiedprosocial subscale of the PANSS (Baran and Docherty, 2008) by a first experimenter.The prosocial subscale is composed of four items: G16: Active social avoidance, N2:Emotional withdrawal, N4: Passive/apathetic social withdrawal and N5: Difficultyin abstract thinking items. A high score on the prosocial subscale reflects emotionalwithdrawal and a lack of social interaction. Finally, for schizophrenia patients, extrapyramidal symptoms were assessed using the Simpson–Angus-Scale (SAS)(Simpson and Angus, 1970). In the second session, expressive behaviours, cognitivefunctions and clinical variables were evaluated for all participants.
2.2.1. Nonverbal expressive behaviours taskThe Motor Affective subscale of the MASS (Trémeau et al., 2008) was used to
measure expressiveness in social interactions. During a structured interview,participants were asked three questions in the same order. First, participants wereasked to report everything they did the day before (for 2 min). Second, they wereasked to describe a movie from memory (for 1 min). Third, they were asked toimagine what they would do if given one million Euros (for 30 s). Interviewerswere instructed to ask predefined questions each time the participant's speech flowstopped for 3 s. Four behaviours were recorded and rated: spontaneous smiles,spontaneous hand gestures, speech flow and voluntary facial expression. Eachoccurrence of these behaviours was recorded on a pre-defined rating sheet. Afterthe interview, participants were asked to make their “most beautiful smile”, andpre-defined behavioural anchors were used to rate the posed smiling. A high scoreon the Motor Affective subscale means less impairment of expressiveness. Clinicalratings were obtained after these tasks during the same interview.
2.2.2. Cognitive and clinical tasksFor all subjects, verbal working memory span was measured using the Letter
Number Sequencing task (Wechsler, 1999). Subjects were verbally presented with aseries of letters and numbers and asked to report back the numbers in numericalorder, followed by the letters in alphabetical order. Visual sustained attentionalfunction was assessed using the Concentration–Endurance Test (d2 test)(Brickenkamp, 1994). In this test, the items are composed of the letters “d” and“p” with one, two, three or four dashes arranged either individually or in pairsabove and below the letter. Participants are given 20 s to scan each line and markall “d's” with two dashes. Finally, Premorbid IQ was assessed using the FrenchNational Adult Reading Test (fNART) (Mackinnon and Mulligan, 2005), depressionwas assessed using the Beck Depression Inventory-II (BDI-II) (Beck et al., 1996) andsocial anxiety was measured by a self-rating version of the Liebowitz-Social-Anxiety-Scale (LSAS) (Liebowitz, 1987).
2.3. Statistical analysis
Clinical ratings and Motor Affective subscale scores were separately comparedfor the three groups with a non-parametric Kruskal–Wallis test. In order tocompare the scores of schizophrenia, social phobia patients and healthy controlgroup, non-parametric U-Mann–Whitney tests were computed. The level ofsignificance was set to po0.05. Spearman non-parametric correlations were usedto explore the relationships between expressive behaviour scores, cognitive dataand clinical data. We did not use a Bonferroni's correction, usually employed tocorrect type I errors, as it is considered to be particularly conservative and todramatically increase the risk of rejection of true correlations (Vialatte and Cichoki,2008). Taking the multiple correlations into account, we decided to use po0.01 toreduce type I errors due to multiple tests.
3. Results
3.1. Mean ratings and group comparisons
Mean ratings and group comparisons on the demographicaldata, fNART (premorbid IQ) and BDI-II are reported in Table 1. The
results revealed significant group differences on the premorbid IQand level of education. Social phobia group has significantly higherscores than schizophrenia and healthy control groups, which werestatistically equivalent.
Mean ratings and group comparisons on the d2 test, LetterNumber Sequencing and the LSAS are reported in Table 2. Schizo-phrenia patients were impaired in d2 test relative to the healthycontrol and social phobia groups. We found no significant differ-ence between social phobia patients and healthy controls on thed2 test. The LSAS score showed that social phobia patients had asignificantly higher score compared to the schizophrenia andhealthy control groups. No significant difference was foundbetween the schizophrenia patients and the healthy controls.
Mean ratings and group comparisons on the expressive beha-viours assessed by the Motor Affective subscale are presented inFig. 1. Schizophrenia and social phobia groups were significantlyimpaired on expressiveness compared to the healthy control group(Mean: 10.66, S.D.: 2.08/ Mean: 10.76, S.D.: 2.16/ Mean: 12.3, S.D.:1.68, respectively, H¼11.267, po0.05). Results showed that schi-zophrenia patients exhibited fewer expressive behaviours com-pared to the healthy controls (z¼−3.094, po0.05). Additonally,social phobia patients produced fewer expressive behaviourscompared to the healthy controls (z¼−2.445, po0.05). Finally,the analysis failed to reveal significant differences between theschizophrenia and social phobia groups. The item scores of theMotor Affective subscale, presented in Fig. 2 reveal significantdifferences between patient groups and healthy controls as well.
Schizophrenia patients were impaired in the number of spon-taneous smiles (Mean: 2.66, S.D.: 0.95) and hand gestures (Mean:2, S.D.: 0.90) in comparison to the healthy controls (Smiles: Mean:3.5, S.D.: 0.68, Hand gestures: Mean: 2.66, S.D.: 0.71, Smiles: z¼−3.343, po0.05, Hand gestures: z¼−2.787, po0.05), but not incomparison with the social phobia patients (Smiles: Mean: 2.95, S.D.: 1.20; Hand gestures: Mean: 2.23, S.D.: 0.94, Smiles: z¼−0.973,p40.05; Hand gestures: z¼−0.919, p40.05). Moreover, socialphobia patient's scores were equivalent to healthy controls. Thus,schizophrenia patients exhibited a spontaneous gesture deficitwhereas social phobia patients failed to reveal this deficit.
Concerning the speech flow dimension, social phobia patientsexhibited significantly higher scores compared to healthy controls(Mean: 3.52; S.D.: 0.75, Mean: 3.33, S.D.: 0.68, respectively, z¼−2.141, po0.05) and schizophrenia patients (Mean: 3.21, S.D.: 0.61,z¼−2.739, po0.05). No difference was found between schizo-phrenia patients and healthy controls.
Finally, social phobia patients were qualitatively impaired onthe voluntary facial expressions (VFE) relative to the healthycontrols (Mean: 2.04, S.D.: 1.12, Mean: 2.83, S.D.: 1.06, respectively,z¼−2.346, po0.05) and the schizophrenia patients (Mean: 2.80,S.D.: 1.09, z¼−2.256, po0.05). Healthy control and schizophreniagroups were equivalent. Thus, social phobia patients exhibiteda VFE deficit whereas schizophrenia patients have normal scores.
3.2. Correlations analyses
All confounding variables such as depression, education leveland premorbid IQ have been controlled in correlation analyses forthe schizophrenia and the social phobia groups. In schizophreniagroup, Spearman's correlations revealed a negative correlationbetween the expressive behaviour scores and negative sympto-matology as assessed by the PANSS (r¼−0.460, p¼0.016). Finally, anegative correlation was also observed between the prosocialfunctioning score evaluated by the modified prosocial and theexpressive behaviour scores (r¼−0.441, po0.02). There is a linkbetween the social difficulties exhibited by schizophrenia patientsand their expressive behaviour deficits. Analyses failed to revealany other correlations between clinical variables and the Motor
Table 1Demographic characteristics of patients and healthy controls.
Schizophrenia (SZ) (n¼30) Social phobia (SP) (n¼21) Control (CT) (n¼30) d.f. Statisticsa p Contrasts
Means S.D. Means S.D. Means S.D.
Age (years) 37.50 10.50 33.19 12.67 31.66 13.22 2 H¼4.151 0.125 –
Sex ratio 18M/12F 12M/9F 11M/19F 1 X2¼3.750 0.153 –
Education level 11.43 2.36 13.85 2.30 12.13 2.28 2 H¼11.428 0.003* SP4CT¼SZfNART (Premorbid IQ ) 104.13 7.84 111.19 4.87 106.70 7.96 2 H¼11.428 0.004* SP4CT¼SZBDI-II 14 8.59 20.52 11.07 7.53 5.63 2 H¼21.008 0.000* SP4SZ4CTPANSS positive 14.63 5.46 – – – – – – – –
PANSS negative 19.50 5.29 – – – – – – – –
PANSS psychopathology 35.16 7.71 – – – – – – – –
PANSS Total 69.36 14.14 – – – – – – – –
Prosocial PANSS items 14.65 3.90 – – – – – – – –
Simpson–Angus scale 6.10 3.23 – – – – – – – –
First generation antipsychotic 11 – – – – – – – –
Second generation antipsychotic 19 – – – – – – – –
BDI-II: Beck Depression Inventory II and PANSS: Positive and Negative Syndrome Scale.a Kruskal–Wallis test or analysis of variance.n po0.05.
Table 2Cognitive and clinical variables of patients and healthy controls.
Schizophrenia (SZ) (n¼30) Social phobia (SP) (n¼21) Control (CT) (n¼30) d.f. Statisticsa p Contrasts
Means S.D. Means S.D. Means S.D.
Concentration–Endurance Test (d2) 118.16 37.26 185.90 46.05 180.53 41.53 2 H¼33.315 o0.0001 SP¼CT4SZLetter Number Sequencing task 8.93 2.94 11.95 3.44 11.36 3.12 2 H¼12.342 o0.002 SP¼CT4SZLSAS anxiety 25.26 13.13 40.52 14.31 25.20 13.36 2 H¼15.794 o0.0001 SP4CT¼SZLSAS avoidance 21.84 12.85 32.76 17.72 19.53 9.87 2 H¼9.092 0.011 SP4CT¼SZLSAS anxiety in social interaction 11.48 7.55 18.19 8.34 9.20 4.97 2 H¼14.984 o0.001 SP4CT¼SZLSAS avoidance in social interaction 9.75 6.30 15.23 8.94 8.26 4.82 2 H¼8.296 0.016 SP4CT¼SZLSAS performance anxiety 14.00 7.31 22.66 6.54 15.96 9.04 2 H¼17.255 o0.0001 SP4CT¼SZLSAS performance avoidance 11.82 7.42 17.52 9.51 10.92 5.57 2 H¼8.347 0.015 SP4CT¼SZ
LSAS: Liebowitz-Social-Anxiety-Scale. Significant: po0.05.a Kruskal–Wallis test or analysis of variance.
Fig. 1. Patient groups were impaired on expressivity behaviours compared tohealthy control group. Social phobia and schizophrenia patients were equivalent.*po0.05, **po0.01, and error bars represent standard error of means.
J. Del-Monte et al. / Psychiatry Research 210 (2013) 29–3532
Affective subscale. In the absence of a direct measure of social lifethat could explain expressive behaviour impairments in schizo-phrenia patient, we have compared the number of prompts torevive the speech for the first and third response questions for theschizophrenia patients and control participants. Results show thatthe groups were equivalent for both questions (Q1: Schizophrenia,Mean: 1.56, S.D.: 1.40 and Control, Mean: 0.93, S.D.: 1.11, (F(1,58)¼3.743, p40.05) and Q3: Schizophrenia, Mean: 0.43, S.D.: 0.81 andControl, Mean: 0.26, S.D.: 0.58, (F(1,58)¼−0.860, p40.05).Although they had fewer expressive gestures during the taskcompared to control participants, the patients were not promptedmore for either question 1 or 3. In addition, to assess “retrievalfluency” and verbal output impairments at a clinical level inindividuals with schizophrenia, we used items P2 (disorganizationof thought and language) and N6 (lack of spontaneity and flow ofconversation) from the PANSS. We found no significant correlationbetween P2 and N6 subscales of the PANSS and the number ofstimulus to revive the speech to third question.
For the social phobia group, Spearman's correlations revealedno significant relations between cognitive and clinical variablesand the Motor Affective subscale scores.
4. Discussion
The main goal of this study was to investigate and comparenonverbal expressiveness in schizophrenia and social phobia. We
used the Motor Affective subscale of the MASS to assess sponta-neous smile expressions, spontaneous hand gestures, voluntaryfacial expression and the speech flow in these two disorders, and avariety of measures such as the LSAS as well as modified prosocialsubscale from the PANSS scale to measure social functioning.
In line with our hypothesis that nonverbal expressiveness willbe reduced in both disorders, results showed that schizophreniapatients and social phobia patients have significantly fewerexpressive behaviours compared to the healthy controls. Theseresults are consistent with the past literature (Melfsen et al., 2000;
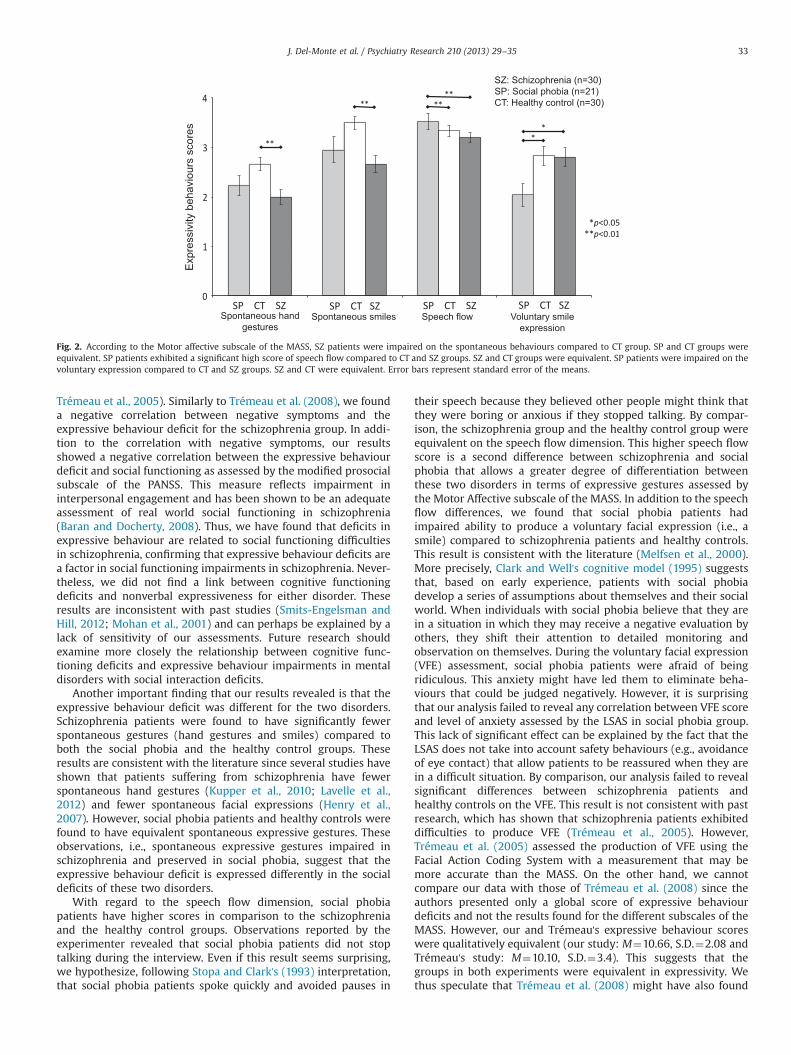
Fig. 2. According to the Motor affective subscale of the MASS, SZ patients were impaired on the spontaneous behaviours compared to CT group. SP and CT groups wereequivalent. SP patients exhibited a significant high score of speech flow compared to CT and SZ groups. SZ and CT groups were equivalent. SP patients were impaired on thevoluntary expression compared to CT and SZ groups. SZ and CT were equivalent. Error bars represent standard error of the means.
J. Del-Monte et al. / Psychiatry Research 210 (2013) 29–35 33
Trémeau et al., 2005). Similarly to Trémeau et al. (2008), we founda negative correlation between negative symptoms and theexpressive behaviour deficit for the schizophrenia group. In addi-tion to the correlation with negative symptoms, our resultsshowed a negative correlation between the expressive behaviourdeficit and social functioning as assessed by the modified prosocialsubscale of the PANSS. This measure reflects impairment ininterpersonal engagement and has been shown to be an adequateassessment of real world social functioning in schizophrenia(Baran and Docherty, 2008). Thus, we have found that deficits inexpressive behaviour are related to social functioning difficultiesin schizophrenia, confirming that expressive behaviour deficits area factor in social functioning impairments in schizophrenia. Never-theless, we did not find a link between cognitive functioningdeficits and nonverbal expressiveness for either disorder. Theseresults are inconsistent with past studies (Smits-Engelsman andHill, 2012; Mohan et al., 2001) and can perhaps be explained by alack of sensitivity of our assessments. Future research shouldexamine more closely the relationship between cognitive func-tioning deficits and expressive behaviour impairments in mentaldisorders with social interaction deficits.
Another important finding that our results revealed is that theexpressive behaviour deficit was different for the two disorders.Schizophrenia patients were found to have significantly fewerspontaneous gestures (hand gestures and smiles) compared toboth the social phobia and the healthy control groups. Theseresults are consistent with the literature since several studies haveshown that patients suffering from schizophrenia have fewerspontaneous hand gestures (Kupper et al., 2010; Lavelle et al.,2012) and fewer spontaneous facial expressions (Henry et al.,2007). However, social phobia patients and healthy controls werefound to have equivalent spontaneous expressive gestures. Theseobservations, i.e., spontaneous expressive gestures impaired inschizophrenia and preserved in social phobia, suggest that theexpressive behaviour deficit is expressed differently in the socialdeficits of these two disorders.
With regard to the speech flow dimension, social phobiapatients have higher scores in comparison to the schizophreniaand the healthy control groups. Observations reported by theexperimenter revealed that social phobia patients did not stoptalking during the interview. Even if this result seems surprising,we hypothesize, following Stopa and Clark's (1993) interpretation,that social phobia patients spoke quickly and avoided pauses in
their speech because they believed other people might think thatthey were boring or anxious if they stopped talking. By compar-ison, the schizophrenia group and the healthy control group wereequivalent on the speech flow dimension. This higher speech flowscore is a second difference between schizophrenia and socialphobia that allows a greater degree of differentiation betweenthese two disorders in terms of expressive gestures assessed bythe Motor Affective subscale of the MASS. In addition to the speechflow differences, we found that social phobia patients hadimpaired ability to produce a voluntary facial expression (i.e., asmile) compared to schizophrenia patients and healthy controls.This result is consistent with the literature (Melfsen et al., 2000).More precisely, Clark and Well's cognitive model (1995) suggeststhat, based on early experience, patients with social phobiadevelop a series of assumptions about themselves and their socialworld. When individuals with social phobia believe that they arein a situation in which they may receive a negative evaluation byothers, they shift their attention to detailed monitoring andobservation on themselves. During the voluntary facial expression(VFE) assessment, social phobia patients were afraid of beingridiculous. This anxiety might have led them to eliminate beha-viours that could be judged negatively. However, it is surprisingthat our analysis failed to reveal any correlation between VFE scoreand level of anxiety assessed by the LSAS in social phobia group.This lack of significant effect can be explained by the fact that theLSAS does not take into account safety behaviours (e.g., avoidanceof eye contact) that allow patients to be reassured when they arein a difficult situation. By comparison, our analysis failed to revealsignificant differences between schizophrenia patients andhealthy controls on the VFE. This result is not consistent with pastresearch, which has shown that schizophrenia patients exhibiteddifficulties to produce VFE (Trémeau et al., 2005). However,Trémeau et al. (2005) assessed the production of VFE using theFacial Action Coding System with a measurement that may bemore accurate than the MASS. On the other hand, we cannotcompare our data with those of Trémeau et al. (2008) since theauthors presented only a global score of expressive behaviourdeficits and not the results found for the different subscales of theMASS. However, our and Trémeau's expressive behaviour scoreswere qualitatively equivalent (our study: M¼10.66, S.D.¼2.08 andTrémeau's study: M¼10.10, S.D.¼3.4). This suggests that thegroups in both experiments were equivalent in expressivity. Wethus speculate that Trémeau et al. (2008) might have also found

J. Del-Monte et al. / Psychiatry Research 210 (2013) 29–3534
that schizophrenia patients had a normal score in voluntary facialexpression. This result, i.e., that VFE is preserved in schizophreniaand impaired in social phobia, corresponds to the third maindifference in expressive behaviour between the two disorders.
In sum, both schizophrenia and social phobia patients exhib-ited expressive behaviour deficits compared to healthy controls.However, our results showed that social interaction deficits inthese disorders could be differentiated on the basis of specific sub-deficits. On the one hand, schizophrenia patients have a sponta-neous gestures deficit but preserved voluntary facial expressionwhile, social phobia patients have a voluntary facial expressiondeficit but preserved spontaneous gestures. It is important to notethat our study controlled for potential confounding variables suchas depression (Trémeau et al., 2005) that could have otherwiseexplained the nonverbal expressive behaviour abnormalities inschizophrenia patients. The lack of association between medica-tion, extrapyramidal symptoms and the expressive behaviourdeficit provides supplementary support to the hypothesis thatexpressive behaviour deficits are specific and directly related toschizophrenic disorder.
From a more methodological point of view, we have assessedsocial behaviours such as spontaneous hand gestures, spontaneoussmiles, speech flow and voluntary facial expressions as evaluatedwith the Motor Affective subscale of the MASS. The scale is anaccurate and easy to use clinical tool. The scale, however, is limitedby its item quantification on a Likert scale of 0–4 and does not takeinto account other nonverbal body movements such as sponta-neous head movements. Recently, Ramseyer and Tschacher (2006)developed a Motion Energy Analysis tool (MEA), which wasspecifically dedicated to quantify spontaneous movements duringa recorded interview. Kupper et al. (2010) have used the MEAmethod to assess body movements during social interactions ofthose with schizophrenia. Results showed that patients have adecrease in body movements compared to healthy controls. Theyalso showed that body movements were correlated with negativesymptoms assessed by the PANSS. On the other hand, spontaneoushead nods were correlated with positive symptoms such assymptoms of suspiciousness.
These studies showed that body movement deficits seem morereflected in social functioning dimensions rather than only in thenegative symptoms of schizophrenia. Body movement assessmentseems to open new perspectives in the understanding of mentalillness and future research should take into account research onexpressive behaviour deficits in mental disorders to emphasizespecific social motor markers in these disorders. The detection ofspecific markers will allow one to develop new group therapymethods with the aim of limiting the number of relapses andimprove the quality of life for patients.
The present study possesses several limitations. First, as men-tioned above, the Motor Affective subscale of the MASS is limitedby its item quantification on a Likert scale of 0–4, which limits thetool's sensibility, and by the assessment of voluntary facialexpression, which is quantified by only one item. A tool moresensitive, such as the Motion Energy Analysis tool (MEA), couldenable more accurate assessment of the global expressive beha-viours. A second limitation of the current study is that the MASShas not been validated for the social phobia. However, it isimportant to note that among the 21 social phobia participants,none refused to participate until the end of the experiment.A study exploring the validity and reliability of the MASS for socialphobics is needed. A third limitation is that raters were not blindto the diagnosis of the participants. Nevertheless it must be notedthat our study was exploratory without an inital hypothesis thatcould have biased our result. A fourth limitation is the possibilitythat social isolation and verbal fluency impairments may to someextent explain the results of the schizophrenia patients. In future
studies, we will take into account these two variables whenassessing social behaviour abilities in schizophrenia patients.Finally, the modified prosocial subscale of the PANSS includesitem such as “Difficulty in abstract thinking” which is not commonlyconsidered as reflecting social functioning. A scale more sensitiveand specific such as Personal and Social Performance Scale(Morosini et al., 2000) should be used instead.
In conclusion, our results have shown that the nonverbalexpressive is a complex phenomenon. Two disorders with socialinteraction deficits lead to different and sometimes oppositebehavioural sub-deficits. These results have several implicationssuch as the need to systematize the assessment of expressivebehaviour to facilitate the diagnosis in mental disorders withsocial interaction deficits. Our results also demonstrate the neces-sity of taking into account the motor dimensions of the DSM-Vdiagnostic categories. Moreover, we highlight the necessity tocreate a simple and easy to use clinical tool for more completeand accurate assessments of nonverbal expressiveness in mentaldisorders.
Role of funding source
This study was supported by an Agence Nationale de laRecherche grant (Project SCAD # ANR-09-BLAN-0405-03).
References
American Psychiatry Association. MINI DSM-IV-TR, 2004. Critères diagnostiques.Masson, Paris.
Baran, X., Docherty, J., May 3–8, 2008. The A-effect of aripiprazole. Presented at theAmerican Psychiatric Association meeting. Washington.
Beck, A.T., Steer, R.A., Ball, R., Ranieri, W., 1996. Comparaison of Beck DepressionInventory-IA and II in psychiatric outpatient. Journal of Personality Assessment67, 588–597.
Bersani, G., Bersani, F.S., Valeriani, G., Robiony, M., Anastasia, A., Colletti, C., Liberati, D.,Capra, E., Quartini, A., Polli, E., 2012. Comparison of social expression in patientswith obsessive-compulsive disorder and schizophrenia using the Facial ActionCoding System: a preliminary study. Neuropsychiatric Disease and Treatment 8,537–547.
Bourke, C., Porter, R.J., Carter, J.D., McIntosh, V.V., Jordan, J., Bell, C., Carter, F.,Colhoun, H., Joyce, P.R., 2012. Comparison of neuropsychological functioningand emotional processing in major depression and social anxiety disordersubjects, and matched healthy controls. The Australian and New ZealandJournal of Psychiatry 46 (10), 972–981.
Brickenkamp, R., 1994. Test d2 Aufmerksamkeits-Belastungs-Test. Handanweisung.8., erweiterte und neu gestaltete Auflage. Hogrefe.
Brüne, M., Abdel-Hamid, M., Sonntag, C., Lehmkämper, C., Langdon, R., 2009.Linking social cognition with social interaction: non-verbal expressivity, socialcompentence an “mentalising” in patients with schizophrenia spectrum dis-orders. Behavioral and Brain Fuctions 5, 6.
Clark, D.M., Wells, A., 1995. A Cognitive Model of Social Phobia: Diagnosis,Assessment, and Treatment. Guilford Press, New York.
Ekman, P., Friesen, W., 1969. The repertoire of nonverbal behavior. Categories,origins, usage, and coding. Semiotica 1, 49–98.
Goldin-Meadow, S., 1999. The role of gesture in communication and thinking.Trends in Cognitive Sciences 3, 419–429.
Green, M.F., Penn, D.L., Bentall, R., Carpenter, W.T., Gaebel, W., Gur, R.C., Kring, A.M.,Park, S., Silverstein, S.M., Heinssen, R., 2008. Social cognition in schizophrenia:an nimh workshop on definitions, assessment, and research opportunities.Schizophrenia Bulletin 34, 1211–1220.
Henry, J.D., Green, M.J., de Lucia, A., Restuccia, C., McDonald, S., O’Donnell, M., 2007.Emotion dysregulation in schizophrenia: reduced amplification of emotionalexpression is associated with emotional blunting. Schizophrenia Research 95,197–204.
Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The positive and negative syndrome scale(PANSS) for schizophrenia. Schizophrenia Bulletin 13, 261–276.
Krauss, R.M., Chen, Y., Chawla, P., 1996. Nonverbal behavior and nonverbalcommunication: what do conversational hand gestures tell us?. In: Zanna, M.(Ed.), Advances in Experimental Social Psychology. Academic Press, San Diego,CA, pp. 389–450.
Kupper, Z., Ramseyer, F., Hoffmann, H., Kalbermatten, S., Tschacher, W., 2010.Video-based quantification of bady movement during social interaction indi-cates the severity of negative symptoms in patients with schizophrenia.Schizophrenia Research 121, 90–100.
J. Del-Monte et al. / Psychiatry Research 210 (2013) 29–35 35
Lavelle, M., Healey, P.G., McCabe, R., 2012. Is nonverbal communication disrupted ininteraction involving patients with schizophrenia. Schizophrenia Bulletin,http://dx.doi.org/10.1093/schbul/sbs091.
Liebowitz, M.R., 1987. Social phobia. Modern Problems of Pharmacopsychiatry 22,141–173.
Mackinnon, A., Mulligan, R., 2005. [The estimation of premorbid intelligence levelsin French speakers]. Encephale 31, 31–43.
Melfsen, S., Osterlow, J., Florin, I., 2000. Deliberate emotional expressions of sociallyanxious children and their mothers. Journal of Anxiety Disorders 14, 249–261.
Mittal, V.A., Jalbrzikowski, M., Daley, M., Roman, C., Bearden, C.E., Cannon, T.D.,2011. Abnormal movements are associated with poor psychosocial functioningin adolescents at high risk for psychosis. Schizophrenia Research 130, 164–169.
Mohan, A., Singh, A.P., Mandal, M.K., 2001. Transfer and interference of motor skillsin people with intellectual disability. Journal of Intellectual Disability Research45 (Pt4), 361–369.
Morosini, P.L., Magliano, L., Brambilla, L., Ugolini, S., Pioli, R., 2000. Development,reliability and acceptability of a new version of the DSM-IV Social andOccupational Functioning Assessment Scale (SOFAS) to assess routine socialfunctioning. Acta Psychiatrica Scandinavica 1001, 323–329.
Moukheiber, A., Rautureau, G., Perez-Diaz, F., Soussignan, R., Dubal, S., Jouvent, R.,Pelissolo, A., 2010. Gaze avoidance in social phobia: objective measure andcorrelates. Behaviour Research and Therapy 48, 147–151.
Panayiotou, G., Karekla, M., 2012. Perceived social support helps, but does notbuffer the negative impact of anxiety disorders on quality of life and perceivedstress. Social Psychiatry and Psychiatric Epidemiology 48 (2), 283.
Phillips, L.K., Seidman, L.J., 2008. Emotion processing in persons at risk forschizophrenia. Schizophrenia Bulletin 34, 888–903.
Ramseyer, F., Tschacher, W., 2006. Synchrony: a core concept for a constructivismapproach to psychotherapy. Constructivism in the Human Sciences 11 (1–2),150–171.
Schneier, F.R., Rodebaugh, T.L., Blanco, C., Lewin, H., Liebowitz, M.R., 2011. Fear andavoidance of eye contact in social anxiety disorder. Comprehensive Psychiatry52, 81–87.
Schmidt, R.C., Richardson, M.J., 2008. Dynamics of interpersonal coordination. In:Fuchs, A, Jirsa, V (Eds.), Coordination: Neural, Behavioral and Social Dynamics.Springer-Verlag, Heidelberg, pp. 281–308.
Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E.,Hergueta, T., Baker, R., Dunbar, G.C., 1998. The Mini International Neuropsy-chiatric Intervie (M.I.N.I.): the development and validation of a structureddiagnostic psychiatric interview for DSM-IV and ICD-10. Journal of ClinicalPsychiatry 59 (Suppl. 20), 22–33, quiz 34–57. Review.
Sidlova, M., Prasko, J., Jelenova, D., Kovacsova, A., Latalova, K., Sigmundova, Z.,Vrbova, K., 2011. The quality of life of patients suffering from schizophrenia– acomparaison with healthy controls. Biomedical papers of the Medical Faculty ofthe University Palacký, Olomouc, Czechoslovakia 155, 173–180.
Simpson, G.M., Angus, J.W., 1970. A rating scale for extrapyramidal side effects. ActaPsychiatrica Scandinavica Supplementum 212, 11–19.
Smits-Engelsman, B., Hill, E.L., 2012. The relationship between motor coordinationand intelligence across the IQ range. Pediatrics 130 (4), e950–e956.
Steimer-Krause, E., Krause, R., Wagner, G., 1990. Interaction regulations used byschizophrenic and psychosomatic patients: studies facial behavior in dyadicinteractions. Psychiatry 53, 209–228.
Stopa, L., Clark, D.M., 1993. Cognitive processes in social phobia. Behaviour Researchand Therapy 31, 255–267.
Tibi-Elhanany, Y., Shamay-Tsoory, S.G., 2011. Social cognition in social anxiety: firstevidence for increased empathic abilities. The Israel Journal of Psychiatry andRelated Sciences 48, 98–106.
Trémeau, F., Goggin, M., Antonius, D., Czobor, P., Hill, V., Citrome, L., 2008. A newrating scale for negative symptoms: the Motor-Affective-Social Scale. PsychiatryResearch 160, 346–355.
Trémeau, F., Malaspina, D., Duval, F., Corrêa, H., Hager-Budny, M., Coin-Bariou, L.,Macher, J.P., Gorman, J.M., 2005. Facial expressiveness in patients with schizo-phrenia compared to depressed patients and nonpatient comparison subjects.The American Journal of Psychiatry 162, 92–101.
Vialatte, F.B., Cichoki, A., 2008. Slipt-test bonferroni correction for qeeg statisticalmaps. Biological Cybernetics 98, 295–303.
Wechsler, D., 1999. Wechsler Abbreviated Scale of Intelligence (WASI). TX: HarcourtAssessment, San Antonio.
Related Documents











