Intensive Care Med (2005) 31:1316–1326 DOI 10.1007/s00134-005-2790-2 REVIEW Alexandre Lima Jan Bakker Noninvasive monitoring of peripheral perfusion Received: 21 February 2005 Accepted: 4 August 2005 Published online: 17 September 2005 # Springer-Verlag 2005 This study was in part supported by mate- rials provided by Hutchinson Technology and a grant from Philips USA. Both authors received a grant US $12,000 from Philips USA and $10,000 from Hutchinson Tech- nology. A. Lima · J. Bakker ( ) ) Department of Intensive Care, Erasmus MC, University Medical Center Rotterdam, P.O. Box 2040, 3000 CA Rotterdam, The Netherlands e-mail: [email protected] Tel.: +31-10-4633629 Abstract Background: Early hemo- dynamic assessment of global pa- rameters in critically ill patients fails to provide adequate information on tissue perfusion. It requires invasive monitoring and may represent a late intervention initiated mainly in the intensive care unit. Noninvasive monitoring of peripheral perfusion can be a complementary approach that allows very early application throughout the hospital. In addition, as peripheral tissues are sensitive to alterations in perfusion, monitoring of the periphery could be an early marker of tissue hypoperfusion. This review discusses noninvasive meth- ods for monitoring perfusion in pe- ripheral tissues based on clinical signs, body temperature gradient, optical monitoring, transcutaneous oximetry, and sublingual capnometry. Discussion: Clinical signs of poor peripheral perfusion consist of a cold, pale, clammy, and mottled skin, as- sociated with an increase in capillary refill time. The temperature gradients peripheral-to-ambient, central-to-pe- ripheral and forearm-to-fingertip skin are validated methods to estimate dynamic variations in skin blood flow. Commonly used optical meth- ods for peripheral monitoring are perfusion index, near-infrared spec- troscopy, laser Doppler flowmetry and orthogonal polarization spec- troscopy. Continuous noninvasive transcutaneous measurement of oxy- gen and carbon dioxide tensions can be used to estimate cutaneous blood flow. Sublingual capnometry is a noninvasive alternative for gastric tonometry. Keywords Body temperature gradient · Hemodynamic assessment · Noninvasive monitoring · Peripheral tissue perfusion · Sublingual capnometry · Transcutaneous oximetry Introduction An important goal of hemodynamic monitoring is the early detection of inadequate tissue perfusion and oxy- genation to institute prompt therapy and guide resuscita- tion, avoiding organ damage. In clinical practice tissue oxygenation is frequently assessed by using conventional global measurements such as blood pressure, oxygen derived variables, and blood lactate levels. However, the assessment of global hemodynamic parameters fails to reflect increased blood lactate levels, the imbalance be- tween oxygen demand and oxygen supply, or the status of the microcirculation [1, 2, 3]. In addition, it often requires invasive monitoring techniques that usually limit early initiation, typically after the patient has been admitted to the intensive care unit (ICU). To address these limitations there have been many attempts to perform measurements of blood flow and oxygenation in peripheral tissues [4, 5]. In circulatory failure blood flow is diverted from the less important tissues (skin, subcutaneous, muscle, gastrointestinal tract) to vital organs (heart, brain, kidneys). Thus monitoring perfusion in these less vital tissues could be an early marker of vital tissue hypoperfusion. Second, the assess-

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Intensive Care Med (2005) 31:1316–1326DOI 10.1007/s00134-005-2790-2 R E V I E W
Alexandre LimaJan Bakker
Noninvasive monitoring of peripheral perfusion
Received: 21 February 2005Accepted: 4 August 2005Published online: 17 September 2005� Springer-Verlag 2005
This study was in part supported by mate-rials provided by Hutchinson Technologyand a grant from Philips USA. Both authorsreceived a grant US $12,000 from PhilipsUSA and $10,000 from Hutchinson Tech-nology.
A. Lima · J. Bakker ())Department of Intensive Care,Erasmus MC,University Medical Center Rotterdam,P.O. Box 2040, 3000 CA Rotterdam,The Netherlandse-mail: [email protected].: +31-10-4633629
Abstract Background: Early hemo-dynamic assessment of global pa-rameters in critically ill patients failsto provide adequate information ontissue perfusion. It requires invasivemonitoring and may represent a lateintervention initiated mainly in theintensive care unit. Noninvasivemonitoring of peripheral perfusioncan be a complementary approachthat allows very early applicationthroughout the hospital. In addition,as peripheral tissues are sensitive toalterations in perfusion, monitoringof the periphery could be an earlymarker of tissue hypoperfusion. Thisreview discusses noninvasive meth-ods for monitoring perfusion in pe-ripheral tissues based on clinicalsigns, body temperature gradient,optical monitoring, transcutaneousoximetry, and sublingual capnometry.Discussion: Clinical signs of poorperipheral perfusion consist of a cold,pale, clammy, and mottled skin, as-
sociated with an increase in capillaryrefill time. The temperature gradientsperipheral-to-ambient, central-to-pe-ripheral and forearm-to-fingertip skinare validated methods to estimatedynamic variations in skin bloodflow. Commonly used optical meth-ods for peripheral monitoring areperfusion index, near-infrared spec-troscopy, laser Doppler flowmetryand orthogonal polarization spec-troscopy. Continuous noninvasivetranscutaneous measurement of oxy-gen and carbon dioxide tensions canbe used to estimate cutaneous bloodflow. Sublingual capnometry is anoninvasive alternative for gastrictonometry.
Keywords Body temperaturegradient · Hemodynamic assessment ·Noninvasive monitoring · Peripheraltissue perfusion · Sublingualcapnometry · Transcutaneousoximetry
Introduction
An important goal of hemodynamic monitoring is theearly detection of inadequate tissue perfusion and oxy-genation to institute prompt therapy and guide resuscita-tion, avoiding organ damage. In clinical practice tissueoxygenation is frequently assessed by using conventionalglobal measurements such as blood pressure, oxygenderived variables, and blood lactate levels. However, theassessment of global hemodynamic parameters fails toreflect increased blood lactate levels, the imbalance be-tween oxygen demand and oxygen supply, or the status of
the microcirculation [1, 2, 3]. In addition, it often requiresinvasive monitoring techniques that usually limit earlyinitiation, typically after the patient has been admitted tothe intensive care unit (ICU).
To address these limitations there have been manyattempts to perform measurements of blood flow andoxygenation in peripheral tissues [4, 5]. In circulatoryfailure blood flow is diverted from the less importanttissues (skin, subcutaneous, muscle, gastrointestinal tract)to vital organs (heart, brain, kidneys). Thus monitoringperfusion in these less vital tissues could be an earlymarker of vital tissue hypoperfusion. Second, the assess-
1317
ment of perfusion in peripheral tissues is more easilyobtainable using noninvasive monitoring techniques, thusfacilitating earlier initiation.
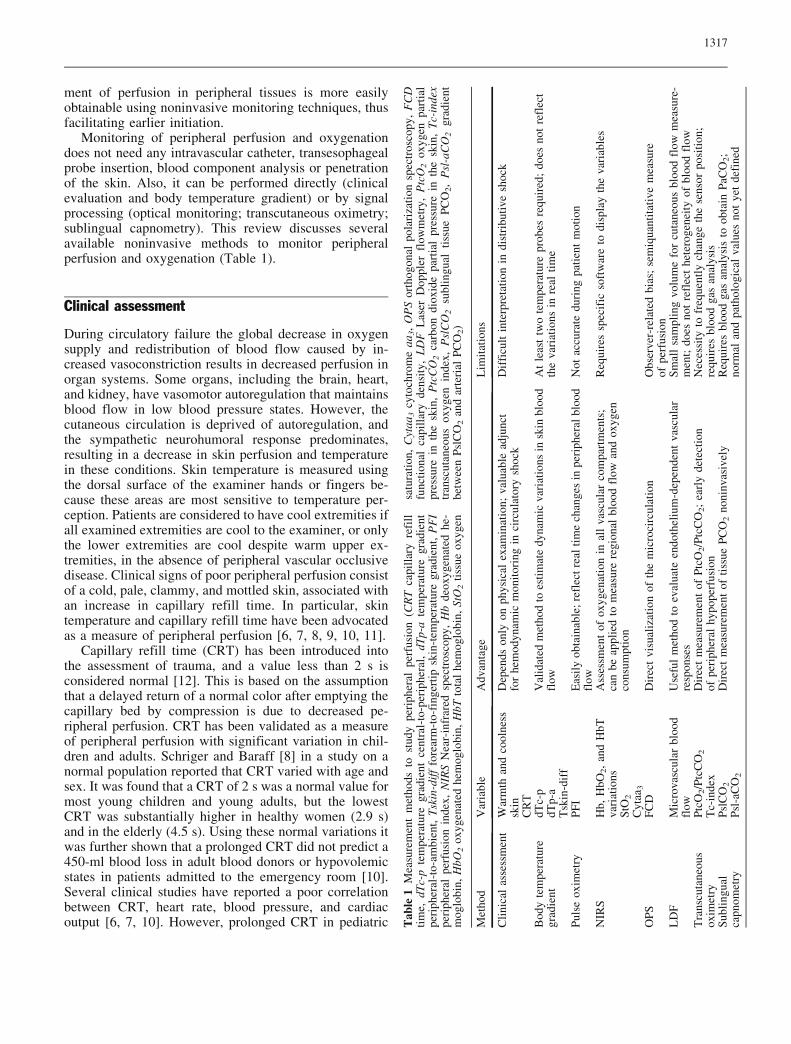
Monitoring of peripheral perfusion and oxygenationdoes not need any intravascular catheter, transesophagealprobe insertion, blood component analysis or penetrationof the skin. Also, it can be performed directly (clinicalevaluation and body temperature gradient) or by signalprocessing (optical monitoring; transcutaneous oximetry;sublingual capnometry). This review discusses severalavailable noninvasive methods to monitor peripheralperfusion and oxygenation (Table 1).
Clinical assessment
During circulatory failure the global decrease in oxygensupply and redistribution of blood flow caused by in-creased vasoconstriction results in decreased perfusion inorgan systems. Some organs, including the brain, heart,and kidney, have vasomotor autoregulation that maintainsblood flow in low blood pressure states. However, thecutaneous circulation is deprived of autoregulation, andthe sympathetic neurohumoral response predominates,resulting in a decrease in skin perfusion and temperaturein these conditions. Skin temperature is measured usingthe dorsal surface of the examiner hands or fingers be-cause these areas are most sensitive to temperature per-ception. Patients are considered to have cool extremities ifall examined extremities are cool to the examiner, or onlythe lower extremities are cool despite warm upper ex-tremities, in the absence of peripheral vascular occlusivedisease. Clinical signs of poor peripheral perfusion consistof a cold, pale, clammy, and mottled skin, associated withan increase in capillary refill time. In particular, skintemperature and capillary refill time have been advocatedas a measure of peripheral perfusion [6, 7, 8, 9, 10, 11].
Capillary refill time (CRT) has been introduced intothe assessment of trauma, and a value less than 2 s isconsidered normal [12]. This is based on the assumptionthat a delayed return of a normal color after emptying thecapillary bed by compression is due to decreased pe-ripheral perfusion. CRT has been validated as a measureof peripheral perfusion with significant variation in chil-dren and adults. Schriger and Baraff [8] in a study on anormal population reported that CRT varied with age andsex. It was found that a CRT of 2 s was a normal value formost young children and young adults, but the lowestCRT was substantially higher in healthy women (2.9 s)and in the elderly (4.5 s). Using these normal variations itwas further shown that a prolonged CRT did not predict a450-ml blood loss in adult blood donors or hypovolemicstates in patients admitted to the emergency room [10].Several clinical studies have reported a poor correlationbetween CRT, heart rate, blood pressure, and cardiacoutput [6, 7, 10]. However, prolonged CRT in pediatric T
able
1M
easu
rem
ent
met
hods
tost
udy
peri
pher
alpe
rfus
ion
(CR
Tca
pill
ary
refi
llti
me,
dTc-
pte
mpe
ratu
regr
adie
ntce
ntra
l-to
-per
iphe
ral,
dTp-
ate
mpe
ratu
regr
adie
ntpe
riph
eral
-to-
ambi
ent,
Tsk
in-d
iff
fore
arm
-to-
fing
erti
psk
in-t
empe
ratu
regr
adie
nt,
PF
Ipe
riph
eral
perf
usio
nin
dex,
NIR
SN
ear-
infr
ared
spec
tros
copy
,H
bde
oxyg
enat
edhe
-m
oglo
bin,
HbO
2ox
ygen
ated
hem
oglo
bin,
HbT
tota
lhe
mog
lobi
n,St
O2
tiss
ueox
ygen
satu
rati
on,
Cyt
aa3
cyto
chro
me
aa3,
OP
Sor
thog
onal
pola
riza
tion
spec
tros
copy
,F
CD
func
tion
alca
pill
ary
dens
ity,
LD
FL
aser
Dop
pler
flow
met
ry,
Ptc
O2
oxyg
enpa
rtia
lpr
essu
rein
the
skin
,P
tcC
O2
carb
ondi
oxid
epa
rtia
lpr
essu
rein
the
skin
,T
c-in
dex
tran
scut
aneo
usox
ygen
inde
x,P
slC
O2
subl
ingu
alti
ssue
PC
O2,
Psl
-aC
O2
grad
ient
betw
een
Psl
CO
2an
dar
teri
alP
CO
2)
Met
hod
Var
iabl
eA
dvan
tage
Lim
itat
ions
Cli
nica
las
sess
men
tW
arm
than
dco
olne
sssk
inD
epen
dson
lyon
phys
ical
exam
inat
ion;
valu
able
adju
nct
for
hem
odyn
amic
mon
itor
ing
inci
rcul
ator
ysh
ock
Dif
ficu
ltin
terp
reta
tion
indi
stri
buti
vesh
ock
CR
TB
ody
tem
pera
ture
grad
ient
dTc-
pV
alid
ated
met
hod
toes
tim
ate
dyna
mic
vari
atio
nsin
skin
bloo
dfl
owA
tle
ast
two
tem
pera
ture
prob
esre
quir
ed;
does
not
refl
ect
the
vari
atio
nsin
real
tim
edT
p-a
Tsk
in-d
iff
Pul
seox
imet
ryP
FI
Eas
ily
obta
inab
le;
refl
ectr
eal
tim
ech
ange
sin
peri
pher
albl
ood
flow
Not
accu
rate
duri
ngpa
tien
tm
otio
n
NIR
SH
b,H
bO2,
and
HbT
vari
atio
nsA
sses
smen
tof
oxyg
enat
ion
inal
lva
scul
arco
mpa
rtm
ents
;ca
nbe
appl
ied
tom
easu
rere
gion
albl
ood
flow
and
oxyg
enco
nsum
ptio
n
Req
uire
ssp
ecif
icso
ftw
are
todi
spla
yth
eva
riab
les
StO
2C
ytaa
3O
PS
FC
DD
irec
tvi
sual
izat
ion
ofth
em
icro
circ
ulat
ion
Obs
erve
r-re
late
dbi
as;
sem
iqua
ntit
ativ
em
easu
reof
perf
usio
nL
DF
Mic
rova
scul
arbl
ood
flow
Use
ful
met
hod
toev
alua
teen
doth
eliu
m-d
epen
dent
vasc
ular
resp
onse
sS
mal
lsa
mpl
ing
volu
me
for
cuta
neou
sbl
ood
flow
mea
sure
-m
ent;
does
not
refl
ect
hete
roge
neit
yof
bloo
dfl
owT
rans
cuta
neou
sox
imet
ryP
tcO
2/P
tcC
O2
Dir
ect
mea
sure
men
tof
Ptc
O2/P
tcC
O2;
earl
yde
tect
ion
ofpe
riph
eral
hypo
perf
usio
nN
eces
sity
tofr
eque
ntly
chan
geth
ese
nsor
posi
tion
;re
quir
esbl
ood
gas
anal
ysis
Tc-
inde
xS
ubli
ngua
lca
pnom
etry
Psl
CO
2D
irec
tm
easu
rem
ent
ofti
ssue
PC
O2
noni
nvas
ivel
yR
equi
res
bloo
dga
san
alys
isto
obta
inP
aCO
2;
norm
alan
dpa
thol
ogic
alva
lues
not
yet
defi
ned
Psl
-aC
O2

1318
patients has been found to be a good predictor of dehy-dration, reduced stroke volume, and increased bloodlactate levels [6, 11]. In adult patients following cardiacsurgery no significant relationship between cardiac indexand CRT was found during the first 8 h following ICUadmission [7].
Distal extremity skin temperature has also been relatedto the adequacy of the circulation. Kaplan et al. [9]compared distal extremity skin temperature (evaluated bysubjective physical examination) with biochemical andhemodynamic markers of hypoperfusion in adult ICUpatients. This study found that patients with cold pe-riphery (including septic patients) had lower cardiacoutput and higher blood lactate levels as a marker of moresevere tissue hypoxia. In another study Hasdai et al. [13]showed the importance of the physical examination indetermining the prognosis of patients with cardiogenicshock. This study reported the presence of a cold andclammy skin to be an independent predictor of 30-daymortality in patients with cardiogenic shock complicatingacute myocardial infarction.
The findings of these studies show that skin tempera-ture together with CRT are a valuable adjunct in hemo-dynamic monitoring during circulatory shock, and shouldbe the first approach to assess critically ill patient. Notmuch is known about the clinical applicability of thesevariables after the patient has been admitted to the in-tensive care unit [14].
Temperature gradients
Since Joly and Weil [15] and Ibsen [16] studied the toetemperature as an indicator of the circulatory shock, bodytemperature gradients have been used as a parameter ofperipheral perfusion. In the presence of a constant envi-ronmental temperature a change in the skin temperature isthe result of a change in skin blood flow [17]. The tem-perature gradients peripheral-to-ambient (dTp-a) andcentral-to-peripheral (dTc-p) can better reflect cutaneousblood flow than the skin temperature itself. Considering aconstant environment condition, dTp-a decreases anddTc-p increases during vasoconstriction. The peripheralskin temperature is measured using a regular temperatureprobe attached to the ventral face of the great toe. Thissite is more convenient for peripheral temperature mea-surement because of the negligible local heat productionand the distal location from other monitoring devices[18]. The concept of the dTc-p is based on the transfer ofheat from the body core to the skin. The heat conductionto the skin by the blood is also controlled by the degree ofvasoconstriction of the arterioles and arteriovenousanastomoses. High blood flow causes heat to be con-ducted from the core to the skin, whereas reduction inblood flow decreases the heat conduction from the core.During vasoconstriction the temperature of the skin falls
and the heat conduction from the core decreases, andtherefore the central temperature rises and the dTc-p in-creases. A gradient of 3–7�C occurs in patients with stablehemodynamics [19]. Hypothermia, cold ambient temper-ature (<20�C) [20], and vasodilatory shock limits the useof dTc-p as an estimate of peripheral perfusion. Forearm-to-fingertip skin-temperature gradient (Tskin-diff) hasalso been used as an index of peripheral circulation toidentify the initiation of thermoregulatory vasoconstric-tion in patients following surgery [21]. Fingertip tem-perature is measured with the temperature probe attachedto the ventral face of the finger. The use of Tskin-diff isbased on assumption that the reference temperature is askin site exposed to the same ambient temperature as thefingertip. It has been applied in conditions where anambient temperature is not stable, such as in patientsundergoing surgery [21, 22, 23]. A change in ambienttemperature therefore affects similarly forearm and fin-gertip temperature, producing little influence in the gra-dient. Basically, when vasoconstriction decreases finger-tip blood flow, finger skin temperature decreases, andTskin-diff increases. Experimental studies have suggesteda Tskin-diff threshold of 0�C for the initiation of vaso-constriction, and a threshold of 4�C for severe vasocon-striction in anesthetized patients [22, 23].
The body temperature gradient was first applied toassess patients with circulatory shock and to differentiatecentral heat retention caused by fever from peripheralvasoconstriction [15, 16, 24]. A number of studies haveexamined the correlation between body temperature gra-dient and global hemodynamic variables in hypovolemic,septic and cardiogenic shock, but these have producedconflicting results [15, 25, 26, 27, 28, 29, 30, 31]. Hen-ning et al. [28] studied dTp-a in patients with circulatoryfailure associated with hypovolemia and low cardiacoutput. An increase in dTp-a to more than 4–6�C over12 h was observed in survivors, and a good relationshipbetween the lowest dTp-a and the highest blood lactatelevels was found in hypovolemic patients at time of ad-mission. In assessing the potential value of dopamine as atherapeutic agent to treat circulatory shock Ruiz et al. [25]showed that survival is associated with an increase indTp-a of more than 2�C, and that dTp-a is correlated toincreases in cardiac output and a reduction in blood lac-tate levels. In examining the value of dTp-a for assessingperipheral perfusion in cardiogenic shock Vincent et al.[27] found that a cardiac index below 1.8 l/min�1 m�2 isassociated with a decrease in dTp-a below 5�C, and thatthe increase in dTp-a occurs earlier than the increase inskin oxygen partial pressure during recovery; this corre-lation was not found in septic shock. No relationship hasbeen observed between dTc-p and cardiac output in adultswith diverse causes of shock [31] or in children after openheart surgery [26, 29, 30]. One reason for the inaccuraterelationship between body temperature gradient andglobal hemodynamic parameters could be related to an
1319
unstable environment, as skin temperature depends alsoon ambient temperature, and the thermoregulatory re-sponse is suppressed in anesthetized patients [32]. Inaddition, global hemodynamic parameters may not besensitive enough to reflect changes in peripheral bloodflow in critically ill patients [33, 34]. Tskin-diff may bean alternative, but its use in these conditions has not yetbeen defined.
Optical monitoring
Optical methods apply light with different wave lengthsdirectly to tissue components using the scattering char-acteristics of tissue to assess various states of these tissues[35]. At physiological concentrations the molecules thatabsorb most light are hemoglobin, myoglobin, cyto-chrome, melanins, carotenes, and bilirrubin. These sub-stances can be quantified and measured in intact tissuesusing simple optical methods. The assessment of tissueoxygenation is based on the specific absorption spectrumof oxygenated hemoglobin (HbO2), deoxygenated hemo-globin (Hb) and cytochrome aa3 (cytaa3). Commonlyused optical methods for peripheral monitoring are per-fusion index, near-infrared spectroscopy, laser-Dopplerflowmetry, and orthogonal polarization spectral.
Peripheral perfusion index
The peripheral perfusion index (PFI) is derived from thephotoeletric plesthysmographic signal of pulse oximetryand has been used as a noninvasive measure of peripheralperfusion in critically ill patients [36]. Pulse oximetry is amonitoring technique used in probably every trauma,critically ill and surgical patient. The principle of pulseoximetry is based on two light sources with differentwavelengths (660 nm and 940 nm) emitted through thecutaneous vascular bed of a finger or earlobe. The Hbabsorbs more light at 660 nm and HbO2 absorbs morelight at 940 nm. A detector at the far side measures theintensity of the transmitted light at each wavelength, andthe oxygen saturation is derived by the ratio between thered light (660 nm) and the infrared light (940 nm) ab-sorbed. As other tissues also absorb light, such as con-nective tissue, bone, and venous blood, the pulse oximetrydistinguishes the pulsatile component of arterial bloodfrom the nonpulsatile component of other tissues. Using atwo-wavelength system the nonpulsatile component isthen discarded, and the pulsatile component is used tocalculate the arterial oxygen saturation. The overall he-moglobin concentration can be determined by a thirdwavelength at 800 nm, with a spectrum that resemblesthat of both Hb and HbO2. The resulting variation in in-tensity of this light can be used to determine the variationin arterial blood volume (pulsatile component). The PFI is
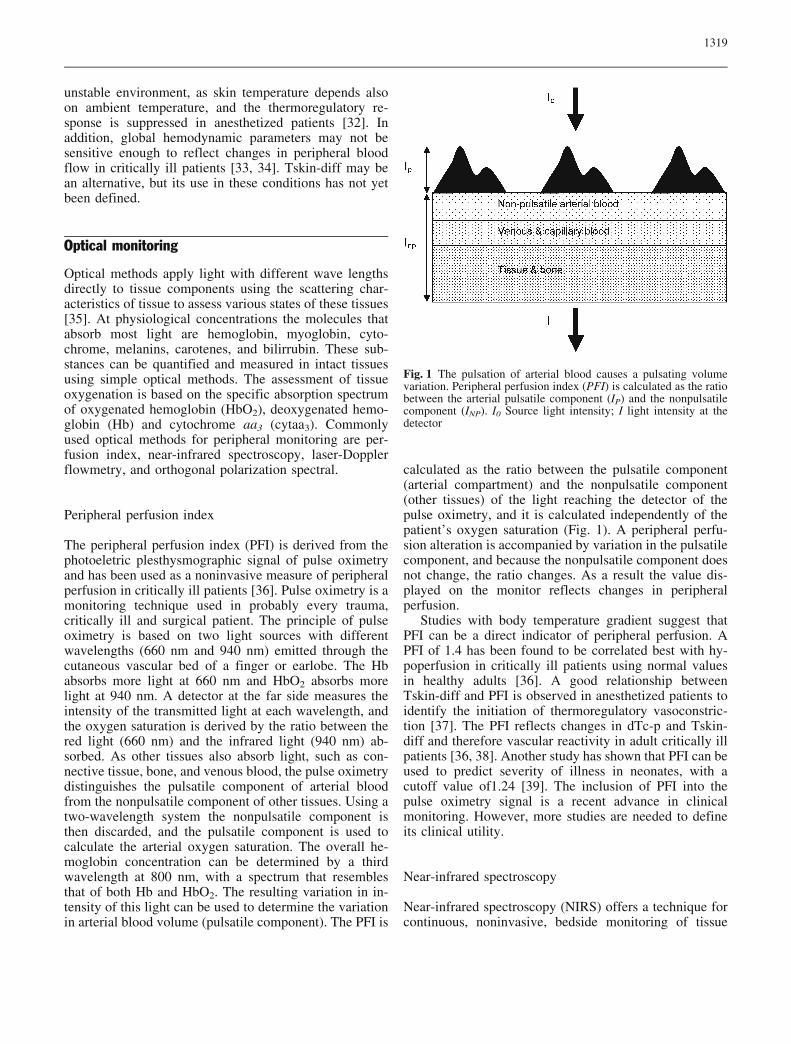
calculated as the ratio between the pulsatile component(arterial compartment) and the nonpulsatile component(other tissues) of the light reaching the detector of thepulse oximetry, and it is calculated independently of thepatient’s oxygen saturation (Fig. 1). A peripheral perfu-sion alteration is accompanied by variation in the pulsatilecomponent, and because the nonpulsatile component doesnot change, the ratio changes. As a result the value dis-played on the monitor reflects changes in peripheralperfusion.
Studies with body temperature gradient suggest thatPFI can be a direct indicator of peripheral perfusion. APFI of 1.4 has been found to be correlated best with hy-poperfusion in critically ill patients using normal valuesin healthy adults [36]. A good relationship betweenTskin-diff and PFI is observed in anesthetized patients toidentify the initiation of thermoregulatory vasoconstric-tion [37]. The PFI reflects changes in dTc-p and Tskin-diff and therefore vascular reactivity in adult critically illpatients [36, 38]. Another study has shown that PFI can beused to predict severity of illness in neonates, with acutoff value of1.24 [39]. The inclusion of PFI into thepulse oximetry signal is a recent advance in clinicalmonitoring. However, more studies are needed to defineits clinical utility.
Near-infrared spectroscopy
Near-infrared spectroscopy (NIRS) offers a technique forcontinuous, noninvasive, bedside monitoring of tissue
Fig. 1 The pulsation of arterial blood causes a pulsating volumevariation. Peripheral perfusion index (PFI) is calculated as the ratiobetween the arterial pulsatile component (IP) and the nonpulsatilecomponent (INP). I0 Source light intensity; I light intensity at thedetector

1320
oxygenation. As with pulse oximetry, NIRS uses theprinciples of light transmission and absorption to measurethe concentrations of hemoglobin, oxygen saturation(StO2), and cytaa3 noninvasively in tissues. NIRS has agreater tissue penetration than pulse oximetry and pro-vides a global assessment of oxygenation in all vascularcompartments (arterial, venous, and capillary). Tissuepenetration is directly related to the spacing between il-lumination and detection fibers. At 25 mm spacing ap-prox. 95% of the detected optical signal is from a depth of0 to 23 mm (Fig. 2). NIRS has been used to assessforearm skeletal muscle oxygenation during induced re-active hyperemia in healthy adults and produces repro-ducible measurements of tissue oxygenation during botharterial and venous occlusive events [40]. Using the ve-nous and arterial occlusion methods NIRS can be appliedto measure regional blood flow and oxygen consumptionby following the rate of HbO2 and Hb changes [40, 41,42]. In the venous occlusion method a pneumatic cuff isinflated to a pressure of approx. 50 mmHg. Such a pres-sure blocks venous occlusion but does not impede arterialinflow. As a result venous blood volume and pressureincrease. NIRS can reflect this change by an increase inHbO2, Hb, and total hemoglobin. In arterial occlusionmethod, the pneumatic cuff is inflated to a pressure ofapprox. 30 mmHg greater than systolic pressure. Such apressure blocks both venous outflow and arterial inflow.Depletion of local available O2 is monitored by NIRS as adecrease in HbO2 and a simultaneous increase in Hb,whereas total Hb remains constant. After release of theoccluding cuff a hyperemic response is observed (Fig. 3).Blood volume increases rapidly, resulting in an increasein HbO2 and a quick washout of Hb. In addition to bloodflow and evaluation of HbO2 and Hb changes, NIRS canassess cytaa3 redox state. Cytaa3 is the final receptor inthe oxygen transport chain that reacts with oxygen toform water, and approx. 90% of cellular energy is derivedfrom this reaction. Cytaa3 remains in a reduced state
during hypoxemia. The absorption spectrum of cytaa3 inits reduced state shows a weak peak at 70 nm, whereas theoxygenated form does not. Therefore monitoring changesin its redox state can provide a measure of the adequacyof oxidative metabolism. Despite the potential clinicalapplications of NIRS, some limitations still exist. Thecontribution of the cytaa3 signal is small, and its inter-pretation remains controversial, requiring more rigorousdevelopment [43]. There is no a gold standard to whichNIRS data can be directly compared, and one of thereasons is that a variety of NIRS equipment is commer-cially available with different working systems.
In both small- and large-animal models of hemorrhagicshock and resuscitation NIRS has demonstrated sensitiv-ity in detecting skeletal muscle and visceral ischemia [44,45, 46, 47]. As a noninvasive measure of peripheralperfusion NIRS has been applied in superficial muscles(brachioradialis muscle, deltoid muscle, tibialis anterior)of trauma ICU patients to monitor the adequacy of tissue
Fig. 2 A Diagram of a distal tip of the NIRS optical cable. B With 25 mm spacing (d) between emission and detection probes, approx.95% of the detected optical signal is from 23 mm of tissue penetration
Fig. 3 Quantitative NIRS measurements during arterial occlusion.After release of the occluding cuff blood volume increases rapidly,resulting in an increase in HbO2 and a quick washout of Hb, fol-lowed by a hyperemic response. Oxygen consumption is calculatedas the rate of decrease in HbO2 (dotted line)
1321
oxygenation and detect a compartment syndrome [48, 49,50, 51, 52]. The use of NIRS in deltoid muscle duringresuscitation of severe trauma patients has recently beenreported [48, 49]. Cairns et al. [49] studied trauma ICUpatients and reported a strong association between ele-vated serum lactate levels and elevated cytaa3 redox stateduring 12 h of shock resuscitation and development ofmultiple organ failure. More recently Mckinley et al. [48]showed a good relationship between StO2, systemicoxygen delivery and lactate in severely trauma patientsduring and after resuscitation over a period of 24 h. Arecent study with septic and nonseptic patients used NIRSto measure both regional blood flow and oxygen con-sumption after venous occlusion [53]. In this study septicpatients had muscular oxygen consumption twice that ofnonseptic patients, but oxygen extraction was similar inboth groups, emphasizing oxygen extraction dysfunctionin sepsis. Another study observed no relationship betweenforearm blood flow, measured by NIRS, and systemicvascular resistance in septic shock patients [41]. Thesefindings demonstrate the ability of NIRS to reflect mi-crocirculatory dysfunction in skeletal muscle in septicshock. The potential to monitor regional perfusion andoxygenation noninvasively at the bedside makes clinicalapplication of NIRS technology of particular interest inintensive care.
Orthogonal polarization spectral
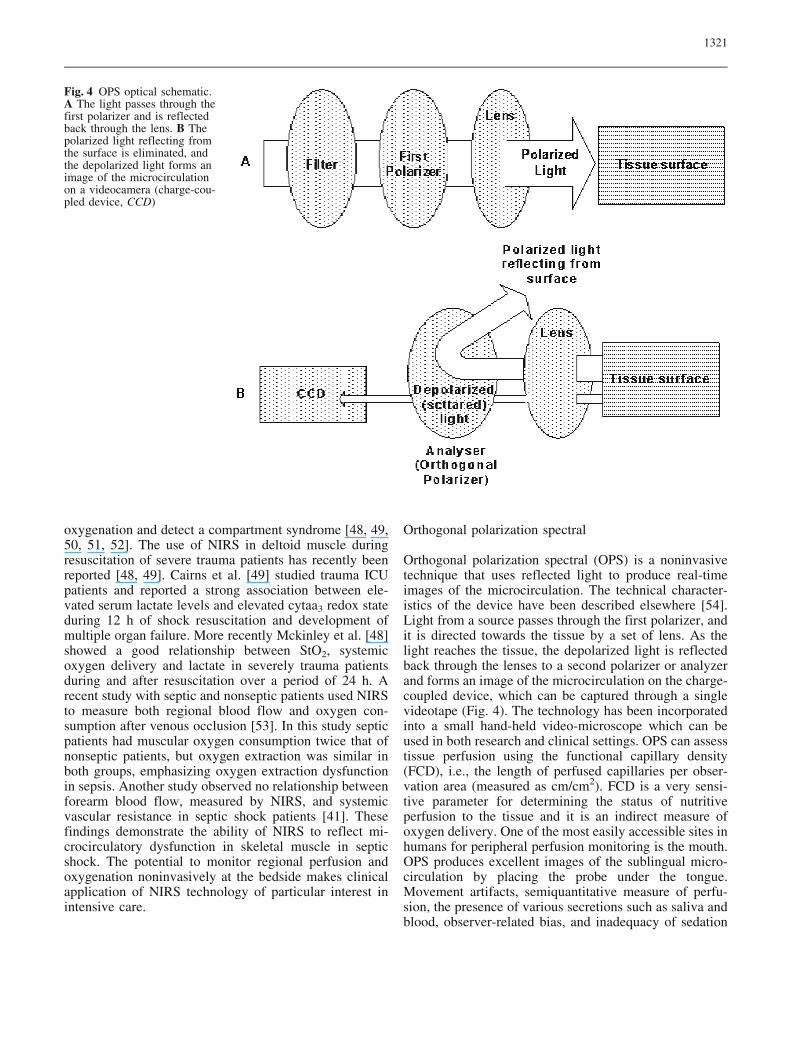
Orthogonal polarization spectral (OPS) is a noninvasivetechnique that uses reflected light to produce real-timeimages of the microcirculation. The technical character-istics of the device have been described elsewhere [54].Light from a source passes through the first polarizer, andit is directed towards the tissue by a set of lens. As thelight reaches the tissue, the depolarized light is reflectedback through the lenses to a second polarizer or analyzerand forms an image of the microcirculation on the charge-coupled device, which can be captured through a singlevideotape (Fig. 4). The technology has been incorporatedinto a small hand-held video-microscope which can beused in both research and clinical settings. OPS can assesstissue perfusion using the functional capillary density(FCD), i.e., the length of perfused capillaries per obser-vation area (measured as cm/cm2). FCD is a very sensi-tive parameter for determining the status of nutritiveperfusion to the tissue and it is an indirect measure ofoxygen delivery. One of the most easily accessible sites inhumans for peripheral perfusion monitoring is the mouth.OPS produces excellent images of the sublingual micro-circulation by placing the probe under the tongue.Movement artifacts, semiquantitative measure of perfu-sion, the presence of various secretions such as saliva andblood, observer-related bias, and inadequacy of sedation
Fig. 4 OPS optical schematic.A The light passes through thefirst polarizer and is reflectedback through the lens. B Thepolarized light reflecting fromthe surface is eliminated, andthe depolarized light forms animage of the microcirculationon a videocamera (charge-cou-pled device, CCD)
1322
to prevent patients from damaging the device are some ofthe limitations of the technique.
The use of sublingual tissues with OPS provides in-formation about the dynamics of microcirculatory bloodflow, and therefore it can monitor the perfusion duringclinical treatment of circulatory shock. It has been used tomonitor the effects of improvements in microcirculatoryblood flow with dobutamine and nitroglycerin in volumeresuscitated septic patients [55, 56]. OPS has been appliedin the ICU to study the properties of sublingual micro-circulation in both septic shock and cardiogenic shock [2,56, 57, 58]. In septic patients it has been shown with OPSthat microvascular alterations are more severe in patientswith a worse outcome, and that these microvascular al-terations can be reversed using vasodilators [2]. In pa-tients with cardiac failure and cardiogenic shock thenumber of small vessels and the density of perfusedvessels are lower than in controls, and the proportion ofperfused vessels is higher in patients who survived than inpatients who did not survive [57]. Using OPS during thetime course of treatment of patients with septic shock,Sakr et al. [58] demonstrated that the behavior of thesublingual microcirculation differs between survivors andnonsurvivors. Although alterations in the sublingual mi-crocirculation may not be representative of other micro-vascular beds, changes in the sublingual circulationevaluated by capnometry during hemorrhagic shock havebeen related to changes in perfusion of internal organssuch as the liver and intestine [59]. Thus OPS could be ofuse in the monitoring of tissue perfusion.
Laser Doppler flowmetry
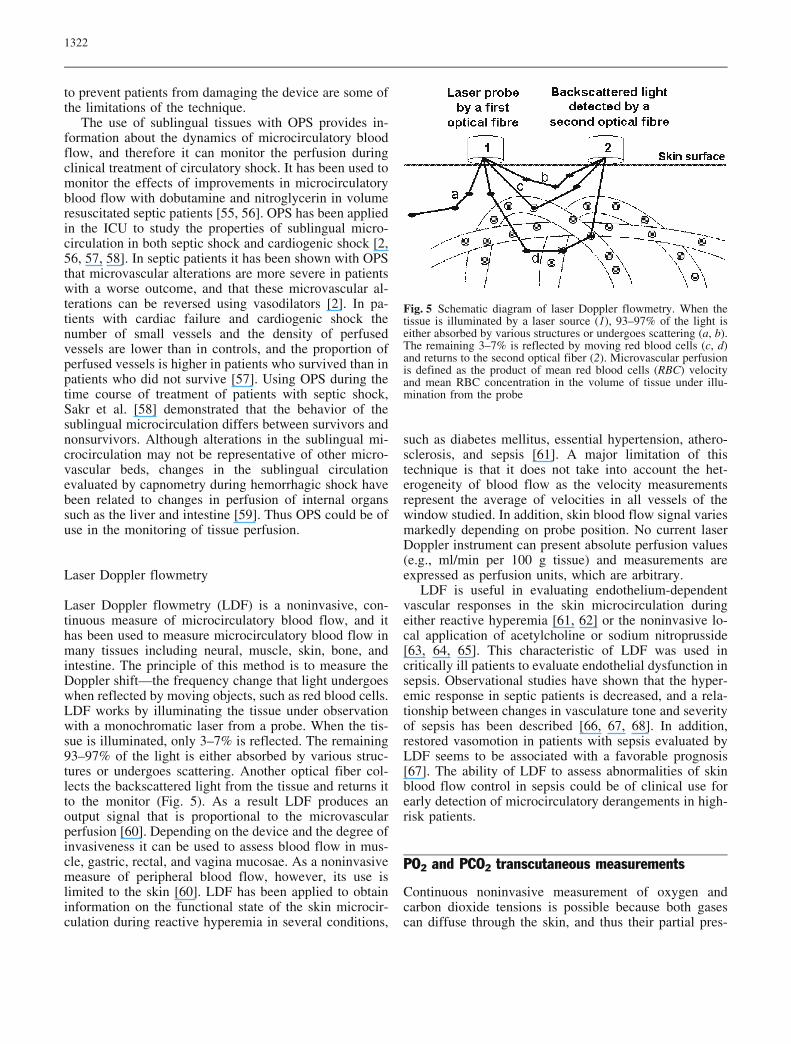
Laser Doppler flowmetry (LDF) is a noninvasive, con-tinuous measure of microcirculatory blood flow, and ithas been used to measure microcirculatory blood flow inmany tissues including neural, muscle, skin, bone, andintestine. The principle of this method is to measure theDoppler shift—the frequency change that light undergoeswhen reflected by moving objects, such as red blood cells.LDF works by illuminating the tissue under observationwith a monochromatic laser from a probe. When the tis-sue is illuminated, only 3–7% is reflected. The remaining93–97% of the light is either absorbed by various struc-tures or undergoes scattering. Another optical fiber col-lects the backscattered light from the tissue and returns itto the monitor (Fig. 5). As a result LDF produces anoutput signal that is proportional to the microvascularperfusion [60]. Depending on the device and the degree ofinvasiveness it can be used to assess blood flow in mus-cle, gastric, rectal, and vagina mucosae. As a noninvasivemeasure of peripheral blood flow, however, its use islimited to the skin [60]. LDF has been applied to obtaininformation on the functional state of the skin microcir-culation during reactive hyperemia in several conditions,
such as diabetes mellitus, essential hypertension, athero-sclerosis, and sepsis [61]. A major limitation of thistechnique is that it does not take into account the het-erogeneity of blood flow as the velocity measurementsrepresent the average of velocities in all vessels of thewindow studied. In addition, skin blood flow signal variesmarkedly depending on probe position. No current laserDoppler instrument can present absolute perfusion values(e.g., ml/min per 100 g tissue) and measurements areexpressed as perfusion units, which are arbitrary.
LDF is useful in evaluating endothelium-dependentvascular responses in the skin microcirculation duringeither reactive hyperemia [61, 62] or the noninvasive lo-cal application of acetylcholine or sodium nitroprusside[63, 64, 65]. This characteristic of LDF was used incritically ill patients to evaluate endothelial dysfunction insepsis. Observational studies have shown that the hyper-emic response in septic patients is decreased, and a rela-tionship between changes in vasculature tone and severityof sepsis has been described [66, 67, 68]. In addition,restored vasomotion in patients with sepsis evaluated byLDF seems to be associated with a favorable prognosis[67]. The ability of LDF to assess abnormalities of skinblood flow control in sepsis could be of clinical use forearly detection of microcirculatory derangements in high-risk patients.
PO2 and PCO2 transcutaneous measurements
Continuous noninvasive measurement of oxygen andcarbon dioxide tensions is possible because both gasescan diffuse through the skin, and thus their partial pres-
Fig. 5 Schematic diagram of laser Doppler flowmetry. When thetissue is illuminated by a laser source (1), 93–97% of the light iseither absorbed by various structures or undergoes scattering (a, b).The remaining 3–7% is reflected by moving red blood cells (c, d)and returns to the second optical fiber (2). Microvascular perfusionis defined as the product of mean red blood cells (RBC) velocityand mean RBC concentration in the volume of tissue under illu-mination from the probe

1323
sures can be measured in transcutaneous tissue. Normallythe skin is not very permeable to gases, but at highertemperatures the ability of the skin to transport gases isimproved. Oxygen sensors for transcutaneous electro-chemical measurements are based on polarography: atypical amperometric transducer in which the rate of achemical reaction is detected by the current drainedthrough an electrode. The sensor heats the skin to 43–45�C. The skin surface oxygen tension is increased as aresult of three effects: (a) heating the stratum corneumbeyond 40�C changes its structure, which allows oxygento diffuse faster; (b) the local oxygen tension is increasedby shifting the oxygen dissociation curve in the heateddermal capillary blood; and (c) by dermal capillary hy-peremia. These transcutaneous sensors enable us directlyto estimate arterial oxygen pressure (PaO2) and arterialcarbon dioxide pressure (PaCO2), and it has been suc-cessfully used for monitoring PaO2 and PaCO2 in bothneonates and in adults [69, 70, 71]. Newborn infant issuitable because of its thin epidermal layer. However, inadults the skin is thicker, and differences in the skin causethe transcutaneous oxygen partial pressure (PtcO2) to belower than PaO2. The correlation between PtcO2 andPaO2 also depends on the adequacy of blood flow. Thelow blood flow caused by vasoconstriction during shockovercomes the vasodilatory effect of PtcO2 sensor. Thiscauses a mild tissue hypoxia beneath the PtcO2 sensor.The lack of the PtcO2 ability to accurately reflect thePaO2 in low flow shock enables us to estimate cutaneousblood flow through the relationship between the twovariables. Some studies have suggested the use of atranscutaneous oxygen index (tc-index), i.e., the changesin PtcO2 relative to changes in PaO2 [69, 72, 73, 74, 75].When blood flow is adequate, PtcO2 and PaO2 values arealmost equal, and the tc-index is close to 1. During lowflow shock the PtcO2 drops and becomes dependent onthe PaO2 value, and tc-index decreases. A tc-index greaterthan 0.7 has been reported to be associated with hemo-dynamic stability [69, 72, 74, 75]. Transcutaneous carbondioxide partial pressure (PtcCO2) has been also used as anindex of cutaneous blood flow. Differences betweenPaCO2 and PtcCO2 have been explained by local accu-mulation of CO2 in the skin due to hypoperfusion. Be-cause of the diffusion constant of CO2 is about 20 timesgreater than O2, PtcCO2 has been showed to be lesssensitive to changes in hemodynamics than PtcO2 [76].One of the main limitations of this technique is the ne-cessity of blood gas analysis to obtain the tc-index andPaCO2. In addition, the sensor position must be changedevery 1–2 h to avoid burns. After each repositioning aperiod of 15–20 min is required for the next readings,which limits its use in emergency situations.
The ability of PtcO2 to reflect tissue perfusion incritically ill adult patients has been applied using the tc-index. Tremper and Shoemaker [72] found a good cor-relation (r=0.86) between tc-index and cardiac index in
patients with shock. These authors reported that at cardiacindex values higher than 2.2 l min�1 m�2 the tc-indexaverages 0.79, at 1.5–2.2 l min�1 m�2 it is 0.48, and atvalues lower than 1.5 l min�1 m�2 it is 0.12. However, therelationship between tc-index and cardiac index may notexist in hyperdynamic shock. Reed et al. [75] studiedPtcO2 at different cardiac indices. In this study 71 mea-surements were made in 19 patients, and a low tc-indexwas seen in 71% of the patients with a cardiac indexhigher than 4.2l min�1 m�2. PtcO2 and PtcCO2 monitoringhas been used as an early indicator of tissue hypoxia andsubclinical hypovolemia in acutely ill patients [77, 78].Tatevossian et al. [78] studied 48 severely injured patientsduring early resuscitation in the emergency departmentand operating room. The sequential patterns of PtcO2 andPtcCO2 were described throughout initial resuscitation.Nonsurvivors had lower PtcO2 values and higher PtcCO2values than survivors. These differences were evidenteven early after the patient’s arrival. The authors reporteda critical tissue perfusion threshold of PtcO2 50 mmHg formore than 60 min and PtcCO2 60 mmHg for more than30 min. Patients who failed to avoid these criticalthresholds had 89% to 100% mortality. This technologyhas not gained widespread acceptance in clinical practiceas the time needed for calibration limits its early use inthe emergency department, and critical PtcO2 and PtcCO2values have not been established.
Sublingual capnometry
Measurement of the tissue-arterial CO2 tension gradienthas been used to reflect the adequacy of tissue perfusion.The gastric and ileal mucosal CO2 clearance is been theprimary reference for measurements of regional PCO2gradient during circulatory shock [79]. The regional PCO2gradient represents the balance between regional CO2production and clearance. During tissue hypoxia CO2 isproduced by hydrogen anions buffered by tissue bicar-bonate, which adds to the amount of CO2 produced bynormal oxidative metabolism. The amount of CO2 pro-duced, either aerobically or because of tissue hypoxia,will be cleared if blood flow is maintained. In low flowstates CO2 increases as a result of stagnation phenomenon[80]. Gastric tonometry is a technique that can be used toassess the adequacy of gut mucosal blood flow to me-tabolism. The methodological limitations of gastric to-nometry required a search for a tissue in which PCO2 canbe measured easily in a noninvasive approach. Compa-rable decreases in blood flow during circulatory shockhave been also demonstrated in the sublingual tissuePCO2 (PslCO2) [81, 82]. The currently available systemfor measuring PslCO2 consists of a disposable PCO2sensor and a battery powered handheld instrument. Theinstrument uses fiberoptic technology to transmit lightthrough the sensor placed between the tongue and the

1324
References
1. Bakker J, Coffernils M, Leon M, Gris P,Vincent J-L (1991) Blood lactate levelsare superior to oxygen-derived vari-ables in predicting outcome in humanseptic shock. Chest 99:956–962
2. De Backer D, Creteur J, Preiser JC,Dubois MJ, Vincent JL (2002) Micro-vascular blood flow is altered in pa-tients with sepsis. Am J Respir CritCare Med 166:98–104
3. Rady MY, Rivers EP, Nowak RM(1996) Resuscitation of the critically illin the ED: responses of blood pressure,heart rate, shock index, central venousoxygen saturation, and lactate. Am JEmerg Med 14:218–225
4. Shoemaker WC, Appel PL, Kram HB,Nathan RC, Thompson JL (1988) Mul-ticomponent noninvasive physiologicmonitoring of circulatory function. CritCare Med 16:482–490
5. Siegemund M, van Bommel J, Ince C(1999) Assessment of regional tissueoxygenation. Intensive Care Med25:1044–1060
6. Tibby SM, Hatherill M, Murdoch IA(1999) Capillary refill and core-periph-eral temperature gap as indicators ofhaemodynamic status in paediatric in-tensive care patients. Arch Dis Child80:163–166
7. Bailey JM, Levy JH, Kopel MA, TobiaV, Grabenkort WR (1990) Relationshipbetween clinical evaluation of periph-eral perfusion and global hemodynam-ics in adults after cardiac surgery. CritCare Med 18:1353–1356
8. Schriger DL, Baraff L (1988) Definingnormal capillary refill: variation withage, sex, and temperature. Ann EmergMed 17:932–935
9. Kaplan LJ, McPartland K, Santora TA,Trooskin SZ (2001) Start with a sub-jective assessment of skin temperatureto identify hypoperfusion in intensivecare unit patients. J Trauma 50:620–627
10. Schriger DL, Baraff L (1991) Capillaryrefill: is it a useful predictor of hypo-volemic states? Ann Emerg Med20:601–605
11. Steiner MJ, DeWalt DA, Byerley JS(2004) Is this child dehydrated? JAMA291:2746–2754
12. Champion HR, Sacco WJ, Carnazzo AJ,Copes W, Fouty WJ (1981) Traumascore. Crit Care Med 9:672–676
13. Hasdai D, Holmes DR Jr, Califf RM,Thompson TD, Hochman JS, PfistererM, Topol EJ (1999) Cardiogenic shockcomplicating acute myocardial infarc-tion: predictors of death. GUSTO In-vestigators. Global Utilization ofStreptokinase and Tissue-PlasminogenActivator for Occluded Coronary Arte-ries. Am Heart J 138:21–31
14. McGee S, Abernethy WB, III, SimelDL (1999) Is this patient hypovolemic?JAMA 281:1022–1029
15. Joly HR, Weil MH (1969) Temperatureof the great toe as an indication of theseverity of shock. Circulation 39:131–138
16. Ibsen B (1967) Treatment of shock withvasodilators measuring temperature ofthe great toe: ten years experience in150 cases. Dis Chest 52:425
17. Guyton AC (1996) Body temperature,temperature regulation, and fever. In:Guyton AC, Hall JE (eds) Textbook ofmedical physiology. Saunders,Philadelphia, pp 911–922
18. Ross BA, Brock L, Aynsley-Green A(1969) Observations on central and pe-ripheral temperatures in the under-standing and management of shock. BrJ Surg 56:877–882
sublingual mucosa. Carbon dioxide diffuses across asemipermeable membrane of the sensor and into a fluo-rescent dye solution. The dye emits light that is propor-tional to the amount of CO2 present. This light intensity isanalyzed by the instrument and displayed as a numericPslCO2 value.
Clinical studies have suggested that PslCO2 is a reli-able marker of tissue hypoperfusion [83, 84, 85, 86]. Weilet al. [86] applied PslCO2 in 46 patients with acutely lifethreatening illness or injuries admitted to the emergencydepartment or ICU. In this study 26 patients with physicalsigns of circulatory shock and high blood lactate levelshad higher PslCO2 values, and a PslCO2 threshold valueof 70 mmHg was predictive for the severity of the cir-culatory failure. Similarly as PCO2 in the gut mucosal,PslCO2 is also influenced by PaCO2 [87]. Hence thegradient between PslCO2 and PaCO2 (Psl-aCO2) is morespecific for tissue hypoperfusion. This was shown in thestudy by Marik and Bankov [85] who determined theprognostic value of sublingual capnometry in 54 hemo-dynamic unstable critically ill patients. In this study Psl-aCO2 was a sensitive marker for tissue perfusion and auseful endpoint for the titration of goal-directed therapy.Psl-aCO2 differentiated better than PslCO2 alone betweensurvivors and nonsurvivors, and a difference of more than25 mmHg indicated a poor prognosis. One limitation of
this technique includes the necessity of blood gas analysisto obtain PaCO2. In addition, normal vs. pathological Psl-aCO2 values are not well defined.
Conclusion
The conventional systemic hemodynamic and oxygen-ation parameters are neither specific nor sensitive enoughto detect regional hypoperfusion. In clinical practice amore complete evaluation of tissue oxygenation can beachieved by adding noninvasive assessment of perfusionin peripheral tissues to global parameters. Noninvasivemonitoring of peripheral perfusion could be a comple-mentary approach that allows very early applicationthroughout the hospital, including the emergency depart-ment, operating room, and hospital wards. Such approachcan be applied using both simple physical examinationand new current technologies, as discussed above. Al-though these methods may reflect variations in peripheralperfusion with certain accuracy, more studies are neededto define the precise role of such methods in the man-agement of the critically ill patients. Finally, evidence forclinical and cost effectiveness of these methods is animportant aspect that needs a formal technology assess-ment.

1325
19. Curley FJ, Smyrnios NA (2003) Rou-tine monitoring of critically ill patients.In: Irwin RS, Cerra FB, Rippe JM (eds)Intensive care medicine. LippincottWilliams & Wilkins, New York, pp250–270
20. Ibsen B (1966) Further observations inthe use of air-conditioned rooms in thetreatment of hyperthermia and shock.Acta Anaesthesiol Scand Suppl 23:565–570
21. Rubinstein EH, Sessler DI (1990) Skin-surface temperature gradients correlatewith fingertip blood flow in humans.Anesthesiology 73:541–545
22. Sessler DI (2003) Skin-temperaturegradients are a validated measure offingertip perfusion. Eur J Appl Physiol89:401–402
23. House JR, Tipton MJ (2002) Using skintemperature gradients or skin heat fluxmeasurements to determine thresholdsof vasoconstriction and vasodilatation.Eur J Appl Physiol 88:141–145
24. Brock L, Skinner JM, Manders JT(1975) Observations on peripheral andcentral temperatures with particularreference to the occurrence of vaso-constriction. Br J Surg 62:589–595
25. Ruiz CE, Weil MH, Carlson RW (1979)Treatment of circulatory shock withdopamine. Studies on survival. JAMA242:165–168
26. Ryan CA, Soder CM (1989) Relation-ship between core/peripheral tempera-ture gradient and central hemodynamicsin children after open heart surgery. CritCare Med 17:638–640
27. Vincent JL, Moraine JJ, van der LP(1988) Toe temperature versus trans-cutaneous oxygen tension monitoringduring acute circulatory failure. Inten-sive Care Med 14:64–68
28. Henning RJ, Wiener F, Valdes S, WeilMH (1979) Measurement of toe tem-perature for assessing the severity ofacute circulatory failure. Surg GynecolObstet 149:1–7
29. Murdoch IA, Qureshi SA, Mitchell A,Huggon IC (1993) Core-peripheraltemperature gradient in children: does itreflect clinically important changes incirculatory haemodynamics? Acta Pae-diatr 82:773–776
30. Butt W, Shann F (1991) Core-periph-eral temperature gradient does not pre-dict cardiac output or systemic vascularresistance in children. Anaesth Inten-sive Care 19:84–87
31. Woods I, Wilkins RG, Edwards JD,Martin PD, Faragher EB (1987) Dangerof using core/peripheral temperaturegradient as a guide to therapy in shock.Crit Care Med 15:850–852
32. Sessler DI (2000) Perioperative heatbalance. Anesthesiology 92:578–596
33. Rivers E, Nguyen B, Havstad S, ResslerJ, Muzzin A, Knoblich B, Peterson E,Tomlanovich M (2001) Early goal-di-rected therapy in the treatment of severesepsis and septic shock. N Engl J Med345:1368–1377
34. Vincent JL (1996) End-points of resus-citation: arterial blood pressure, oxygendelivery, blood lactate, or..? IntensiveCare Med 22:3–5
35. Flewelling R (2000) Noninvasive opti-cal monitoring. In: Bronzino JD (ed)The biomedical engineering handbook.Springer, Berlin Heidelberg New York,pp 1–10
36. Lima AP, Beelen P, Bakker J (2002)Use of a peripheral perfusion indexderived from the pulse oximetry signalas a noninvasive indicator of perfusion.Crit Care Med 30:1210–1213
37. Kurz A, Xiong J, Sessler DI, DechertM, Noyes K, Belani K (1995) Desflu-rane reduces the gain of thermoregula-tory arteriovenous shunt vasoconstric-tion in humans. Anesthesiology83:1212–1219
38. Lima A, Bakker J (2004) The peripheralperfusion index in reactive hyperemiain critically ill patients. Crit Care8:S27–P53
39. De Felice C, Latini G, Vacca P, KopoticRJ (2002) The pulse oximeter perfusionindex as a predictor for high illnessseverity in neonates. Eur J Pediatr161:561–562
40. Van Beekvelt MC, Colier WN, WeversRA, Van Engelen BG (2001) Perfor-mance of near-infrared spectroscopy inmeasuring local O (2) consumption andblood flow in skeletal muscle. J ApplPhysiol 90:511–519
41. De Blasi RA, Ferrari M, Natali A, ContiG, Mega A, Gasparetto A (1994) Non-invasive measurement of forearm bloodflow and oxygen consumption by near-infrared spectroscopy. J Appl Physiol76:1388–1393
42. Edwards AD, Richardson C, van derZP, Elwell C, Wyatt JS, Cope M, DelpyDT, Reynolds EO (1993) Measurementof hemoglobin flow and blood flow bynear-infrared spectroscopy. J ApplPhysiol 75:1884–1889
43. Taylor DE, Simonson SG (1996) Use ofnear-infrared spectroscopy to monitortissue oxygenation. New Horiz 4:420–425
44. Rhee P, Langdale L, Mock C, Gen-tilello LM (1997) Near-infrared spec-troscopy: continuous measurement ofcytochrome oxidation during hemor-rhagic shock. Crit Care Med 25:166–170
45. Puyana JC, Soller BR, Zhang S, HeardSO (1999) Continuous measurement ofgut pH with near-infrared spectroscopyduring hemorrhagic shock. J Trauma46:9–15
46. Beilman GJ, Myers D, Cerra FB,Lazaron V, Dahms RA, Conroy MJ,Hammer BE (2001) Near-infrared andnuclear magnetic resonance spectro-scopic assessment of tissue energeticsin an isolated, perfused canine hindlimb model of dysoxia. Shock 15:392–397
47. Crookes BA, Cohn SM, Burton EA,Nelson J, Proctor KG (2004) Noninva-sive muscle oxygenation to guide fluidresuscitation after traumatic shock.Surgery 135:662–670
48. McKinley BA, Marvin RG, CocanourCS, Moore FA (2000) Tissue hemo-globin O2 saturation during resuscita-tion of traumatic shock monitored usingnear infrared spectrometry. J Trauma48:637–642
49. Cairns CB, Moore FA, Haenel JB,Gallea BL, Ortner JP, Rose SJ, MooreEE (1997) Evidence for early supplyindependent mitochondrial dysfunctionin patients developing multiple organfailure after trauma. J Trauma 42:532–536
50. Muellner T, Nikolic A, Schramm W,Vecsei V (1999) New instrument thatuses near-infrared spectroscopy for themonitoring of human muscle oxygen-ation. J Trauma 46:1082–1084
51. Arbabi S, Brundage SI, Gentilello LM(1999) Near-infrared spectroscopy: apotential method for continuous, trans-cutaneous monitoring for compartmen-tal syndrome in critically injured pa-tients. J Trauma 47:829–833
52. Giannotti G, Cohn SM, Brown M,Varela JE, McKenney MG, WisebergJA (2000) Utility of near-infraredspectroscopy in the diagnosis of lowerextremity compartment syndrome.J Trauma 48:396–399
53. Girardis M, Rinaldi L, Busani S, FloreI, Mauro S, Pasetto A (2003) Muscleperfusion and oxygen consumption bynear-infrared spectroscopy in septic-shock and non-septic-shock patients.Intensive Care Med 29:1173–1176
54. Groner W, Winkelman JW, Harris AG,Ince C, Bouma GJ, Messmer K, NadeauRG (1999) Orthogonal polarizationspectral imaging: a new method forstudy of the microcirculation. Nat Med5:1209–1212
55. De Backer D, Dubois MJ, Creteur J,Vincent J-L (2001) Effects of dobuta-mine on microcirculatory alterations inpatients with septic shock. IntensiveCare Med 27:S237
56. Spronk PE, Ince C, Gardien MJ,Mathura KR, Oudemans-van StraatenHM, Zandstra DF (2002) Nitroglycerinin septic shock after intravascular vol-ume resuscitation. Lancet 360:1395–1396
1326
57. De Backer D, Creteur J, Dubois MJ,Sakr Y, Vincent JL (2004) Microvas-cular alterations in patients with acutesevere heart failure and cardiogenicshock. Am Heart J 147:91–99
58. Sakr Y, Dubois MJ, De Backer D,Creteur J, Vincent JL (2004) Persistentmicrocirculatory alterations are associ-ated with organ failure and death inpatients with septic shock. Crit CareMed 32:1825–1831
59. Jin X, Weil MH, Sun S, Tang W, BiseraJ, Mason EJ (1998) Decreases in organblood flows associated with increases insublingual PCO2 during hemorrhagicshock. J Appl Physiol 85:2360–2364
60. Schabauer AM, Rooke TW (1994) Cu-taneous laser Doppler flowmetry: ap-plications and findings. Mayo Clin Proc69:564–574
61. Farkas K, Fabian E, Kolossvary E, JaraiZ, Farsang C (2003) Noninvasive as-sessment of endothelial dysfunction inessential hypertension: comparison ofthe forearm microvascular reactivitywith flow-mediated dilatation of thebrachial artery. Int J Angiol 12:224–228
62. Koller A, Kaley G (1990) Role of en-dothelium in reactive dilation of skele-tal muscle arterioles. Am J Physiol259:H1313–H1316
63. Morris SJ, Shore AC, Tooke JE (1995)Responses of the skin microcirculationto acetylcholine and sodium nitroprus-side in patients with NIDDM. Dia-betologia 38:1337–1344
64. Warren JB (1994) Nitric oxide and hu-man skin blood flow responses to ace-tylcholine and ultraviolet light. FASEBJ 8:247–251
65. Blaauw J, Graaff R, van Pampus MG,van Doormaal JJ, Smit AJ, Rakhorst G,Aarnoudse JG (2005) Abnormal endo-thelium-dependent microvascular reac-tivity in recently preeclamptic women.Obstet Gynecol 105:626–632
66. Hartl WH, Gunther B, Inthorn D,Heberer G (1988) Reactive hyperemiain patients with septic conditions. Sur-gery 103:440–444
67. Young JD, Cameron EM (1995) Dy-namics of skin blood flow in humansepsis. Intensive Care Med 21:669–674
68. Sair M, Etherington PJ, Peter WC,Evans TW (2001) Tissue oxygenationand perfusion in patients with systemicsepsis. Crit Care Med 29:1343–1349
69. Hasibeder W, Haisjackl M, Sparr H,Klaunzer S, Horman C, Salak N, Ger-mann R, Stronegger WJ, Hackl JM(1991) Factors influencing transcutane-ous oxygen and carbon dioxide mea-surements in adult intensive care pa-tients. Intensive Care Med 17:272–275
70. Carter B, Hochmann M, Osborne A,Nisbet A, Campbell N (1995) A com-parison of two transcutaneous monitorsfor the measurement of arterial PO2 andPCO2 in neonates. Anaesth IntensiveCare 23:708–714
71. Phan CQ, Tremper KK, Lee SE, BarkerSJ (1987) Noninvasive monitoring ofcarbon dioxide: a comparison of thepartial pressure of transcutaneous andend-tidal carbon dioxide with the partialpressure of arterial carbon dioxide.J Clin Monit 3:149–154
72. Tremper KK, Shoemaker WC (1981)Transcutaneous oxygen monitoring ofcritically ill adults, with and withoutlow flow shock. Crit Care Med 9:706–709
73. Shoemaker WC, Wo CC, Bishop MH,Thangathurai D, Patil RS (1996) Non-invasive hemodynamic monitoring ofcritical patients in the emergency de-partment. Acad Emerg Med 3:675–681
74. Tremper KK, Barker SJ (1987) Trans-cutaneous oxygen measurement: ex-perimental studies and adult applica-tions. Int Anesthesiol Clin 25:67–96
75. Reed RL, Maier RV, Landicho D,Kenny MA, Carrico CJ (1985) Corre-lation of hemodynamic variables withtranscutaneous PO2 measurements incritically ill adult patients. J Trauma25:1045–1053
76. Tremper KK, Shoemaker WC, ShippyCR, Nolan LS (1981) TranscutaneousPCO2 monitoring on adult patients inthe ICU and the operating room. CritCare Med 9:752–755
77. Waxman K, Sadler R, Eisner ME, Ap-plebaum R, Tremper KK, Mason GR(1983) Transcutaneous oxygen moni-toring of emergency department pa-tients. Am J Surg 146:35–38
78. Tatevossian RG, Wo CC, VelmahosGC, Demetriades D, Shoemaker WC(2000) Transcutaneous oxygen andCO2 as early warning of tissue hypoxiaand hemodynamic shock in critically illemergency patients. Crit Care Med28:2248–2253
79. Fiddian-Green RG, Baker S (1987)Predictive value of the stomach wall pHfor complications after cardiac opera-tions: comparison with other monitor-ing. Crit Care Med 15:153–156
80. De Backer D, Creteur J (2003) Regionalhypoxia and partial pressure of carbondioxide gradients: what is the link? In-tensive Care Med 29:2116–2118
81. Nakagawa Y, Weil MH, Tang W, SunS, Yamaguchi H, Jin X, Bisera J (1998)Sublingual capnometry for diagnosisand quantitation of circulatory shock.Am J Respir Crit Care Med 157:1838–1843
82. Povoas HP, Weil MH, Tang W, MoranB, Kamohara T, Bisera J (2000) Com-parisons between sublingual and gastrictonometry during hemorrhagic shock.Chest 118:1127–1132
83. Rackow EC, O’Neil P, Astiz ME, Car-pati CM (2001) Sublingual capnometryand indexes of tissue perfusion in pa-tients with circulatory failure. Chest120:1633–1638
84. Marik PE (2001) Sublingual capnogra-phy: a clinical validation study. Chest120:923–927
85. Marik PE, Bankov A (2003) Sublingualcapnometry versus traditional markersof tissue oxygenation in critically illpatients. Crit Care Med 31:818–822
86. Weil MH, Nakagawa Y, Tang W, SatoY, Ercoli F, Finegan R, Grayman G,Bisera J (1999) Sublingual capnometry:a new noninvasive measurement fordiagnosis and quantitation of severity ofcirculatory shock. Crit Care Med27:1225–1229
87. Pernat A, Weil MH, Tang W, Yam-aguchi H, Pernat AM, Sun S, Bisera J(1999) Effects of hyper- and hypoven-tilation on gastric and sublingual PCO(2). J Appl Physiol 87:933–937
Related Documents











