Cytometry 4:174-183 (1983) 0 1983 Alan R. Liss, Inc. Non-Small-Cell Lung Carcinoma: Tumor Characterization on the Basis of Flow Cytometrically Determined Cellular Heterogeneity ‘y2 Laura Teodori, Donatella Tirindelli-Danesi, Francesco Mauro, Raffaele De Vita, Raffaella Uccelli, Claudio Botti, Claudio Modini, Carlo Nervi, and Sergio Stipa2 Laboratorio di Dosimetria e Biofisica, ENEA-Casaccia, Via Anguillarese, 00060 Rome (L.T., R.D.V., F.M., R.U.), IV Patologia Chirurgica, Facolta di Medicina, Universita degli Studi, 00161 Rome (C.B., C.M., S.S., D.T.D.), Istituto Medico e di Ricerca Scientifica, Via S. Stefan0 Rotondo 6,00184 Rome (C.N.),Italy Received for publication January 7, 1983; accepted May 13, 1983. Some 150 tumor specimens from 49 patients with non-small-cell carcinoma of the lung (23 epidermoid, 14 adenocarcinoma, 12 large-cell carcinoma) and three with nonneoplastic lung disease were analysed for cellular DNA con- tent by flow cytometry. Monodispersed cells were stained with ethidium bromide and mithramycin. Normal specimens and samples from patients with nonneoplastic disease con- stantly yielded a single cell population with diploid DNA content. Twenty of 23 epider- moid carcinomas exhibited one or more than one aneuploid subpopulation. Ten of 12 large- cell carcinomas were characterized by one aneuploid clone and 2/12 by two aneuploid clones. Adenocarcinoma exhibited multi- clonal cell subpopulations (one to five aneu- ploid clones). Further information has been obtained on the differential presence of clones in various tumor areas and in infiltrated lymph nodes. These tumors appear character- ized by a remarkable degree of cellular heter- ogeneity. The cytometric ploidy level(s) and the cell population multiclonal structure yield, in comparison with, and in addition to, pathology, indications of possible clinical in- terest. A correlation between the clonal DNA content and a prognostic parameter such as the tumor mass doubling time has been dem- onstrated. Key terms: Non-small-cell carcinoma of the lung, DNA content determination, tumor het- erogeneity, flow cytometry Nowadays, lung cancer is characterized by poor prog- nosis in spite of the recent introduction of combined therapeutic modalities (12). Further advance may de- pend upon an improvement of diagnostic and prognostic procedures, and a better understanding of the biological nature of the disease, in order to define relatively ho- mogeneous groups of patients in whom to evaluate the results of specific protocols or modalities (12). It is already known that growth parameters are im- portant from the point of view of therapeutic manage- ment (4,14). Unfortunately, the reliability of biological and clinical growth parameters is greatly hampered by the high degree of heterogeneity present in the majority of solid tumors (9,16,17,22) and by technical problems and limits (2). The causes of such heterogeneity are not well understood and could be related to the conditions in which tumors arise, develop, and interact with host cell system. The aim of the present work is to apply a cytometric approach to the study of cellular samples from non-small- cell lung carcinoma (NSCLC) patients, carefully classi- fied for disease stage, histological type, immunological status, and tumor doubling time (when available). Flow cytometry is a well-known, potentially powerful tool in cellular pathology (6). The method can be used to obtain information not only on the proliferative characteristics of malignant cell populations but also on their cytoge- netic features of diagnostic andlor prognostic signifi- cance (16). MATERIALS AND METHODS Patients Flow cytometric measurements of cellular DNA con- tent were performed on over 150 specimens from 52 ‘Partially supported by Progetto Finalizzato CNR “Controllo della Crescita Neoplastica,” contract No. 80.01586.06. Presented at the Combined International Conference on Analytical Cytology and Cyto- metry IX and the 6th International Symposium on Flow Cytometry, Schloss Elmau, October 18-23, 1982. ‘Sergio Stipa is a Fellow of the American College of Surgeons. Address reprint requests to Laura Teodori, Laboratorio di Dosirnetria e Biofisica, ENEA-Casaccia,Via Anguillarese, 00060 Roma, Italy.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cytometry 4:174-183 (1983) 0 1983 Alan R. Liss, Inc.
Non-Small-Cell Lung Carcinoma: Tumor Characterization on the Basis of Flow Cytometrically Determined Cellular
Heterogeneity ‘y2
Laura Teodori, Donatella Tirindelli-Danesi, Francesco Mauro, Raffaele De Vita, Raffaella Uccelli, Claudio Botti, Claudio Modini, Carlo Nervi, and Sergio Stipa2
Laboratorio di Dosimetria e Biofisica, ENEA-Casaccia, Via Anguillarese, 00060 Rome (L.T., R.D.V., F.M., R.U.), IV Patologia Chirurgica, Facolta di Medicina, Universita degli Studi, 00161 Rome (C.B., C.M., S.S., D.T.D.), Istituto Medico
e di Ricerca Scientifica, Via S. Stefan0 Rotondo 6,00184 Rome (C.N.), Italy Received for publication January 7, 1983; accepted May 13, 1983.
Some 150 tumor specimens from 49 patients with non-small-cell carcinoma of the lung (23 epidermoid, 14 adenocarcinoma, 12 large-cell carcinoma) and three with nonneoplastic lung disease were analysed for cellular DNA con- tent by flow cytometry. Monodispersed cells were stained with ethidium bromide and mithramycin. Normal specimens and samples from patients with nonneoplastic disease con- stantly yielded a single cell population with diploid DNA content. Twenty of 23 epider- moid carcinomas exhibited one or more than one aneuploid subpopulation. Ten of 12 large- cell carcinomas were characterized by one aneuploid clone and 2/12 by two aneuploid clones. Adenocarcinoma exhibited multi- clonal cell subpopulations (one to five aneu-
ploid clones). Further information has been obtained on the differential presence of clones in various tumor areas and in infiltrated lymph nodes. These tumors appear character- ized by a remarkable degree of cellular heter- ogeneity. The cytometric ploidy level(s) and the cell population multiclonal structure yield, in comparison with, and in addition to, pathology, indications of possible clinical in- terest. A correlation between the clonal DNA content and a prognostic parameter such as the tumor mass doubling time has been dem- onstrated.
Key terms: Non-small-cell carcinoma of the lung, DNA content determination, tumor het- erogeneity, flow cytometry
Nowadays, lung cancer is characterized by poor prog- nosis in spite of the recent introduction of combined therapeutic modalities (12). Further advance may de- pend upon an improvement of diagnostic and prognostic procedures, and a better understanding of the biological nature of the disease, in order to define relatively ho- mogeneous groups of patients in whom to evaluate the results of specific protocols or modalities (12).
It is already known that growth parameters are im- portant from the point of view of therapeutic manage- ment (4,14). Unfortunately, the reliability of biological and clinical growth parameters is greatly hampered by the high degree of heterogeneity present in the majority of solid tumors (9,16,17,22) and by technical problems and limits (2). The causes of such heterogeneity are not well understood and could be related to the conditions in which tumors arise, develop, and interact with host cell system.
The aim of the present work is to apply a cytometric approach to the study of cellular samples from non-small- cell lung carcinoma (NSCLC) patients, carefully classi-
fied for disease stage, histological type, immunological status, and tumor doubling time (when available). Flow cytometry is a well-known, potentially powerful tool in cellular pathology (6). The method can be used to obtain information not only on the proliferative characteristics of malignant cell populations but also on their cytoge- netic features of diagnostic andlor prognostic signifi- cance (16).
MATERIALS AND METHODS Patients
Flow cytometric measurements of cellular DNA con- tent were performed on over 150 specimens from 52
‘Partially supported by Progetto Finalizzato CNR “Controllo della Crescita Neoplastica,” contract No. 80.01586.06. Presented at the Combined International Conference on Analytical Cytology and Cyto- metry IX and the 6th International Symposium on Flow Cytometry, Schloss Elmau, October 18-23, 1982.
‘Sergio Stipa is a Fellow of the American College of Surgeons. Address reprint requests to Laura Teodori, Laboratorio di Dosirnetria
e Biofisica, ENEA-Casaccia, Via Anguillarese, 00060 Roma, Italy.

NON-SMALL-CELL LUNG CARCINOMA 175
patients affected by histologically confirmed NSCLC or nonmalignant lung disease. Specimens were grouped according to their histopathological type and to the TNM system (1, 13, 15). The histopathological composition of the group (25) (epidermoid, adenocarcinoma, and large- cell carcinoma; non-malignant lung disease) is illus- trated in Table 1 together with other indications of the patients’ state (sex, age, disease stage, and delayed hy- persensitivity reaction to recall antigens such as protein purified derivate, candidine and trichophytine).
Samples and Preparation Cellular specimens were obtained by surgery, fine-
needle biopsy, bronchial washing, and pleural effusion collection from patients suspected to have lung cancer and thereater diagnosed as affected by NSCLC (or non- malignant lung disease). Samples were placed in RPMI 1640 culture medium (Grand Island, NY), supplemented with 5% fetal calf serum at 4°C. Parts of the same specimens were always used for histopathological or cy- tological examinations. Monocellular suspension of bi- opsy material was achieved by mechanical and enzymatic treatment (the mechanical step was omitted in the instance of bronchial washing and pleural effu- sion). Briefly, the tissue was minced with scissors, washed in saline solution, and treated with 0.5% pepsin (Serva, Heidelberg, FRG), for 10 min. Tris-buffer was then added, and samples were centrifuged at 200g for 5 min, and the pellet was resuspended in the same buffer.
Staining and Flow Cytometry Twenty microliters of Nonidet P 40 (Fluka, Buchs,
Switzerland) and 1 ml of 25 pglml ethidium bromide (Serva, Heidelberg, FRG) and 1 ml of 2.5 pg/ml mithra-
Table 1 Composition of the Group of 52 Patients Under Investigation, Classified for Histopathological Type, Disease Stage, Delayed
Hypersensitivity Reaction, and Tumor Doubling Time (When
Patients
Total cases 52 Females, 5; males, 47 Age range 45-77 yr
Epidermoid carcinoma 23 Adenocarcinoma 14
Histology
Large cell carcinoma 12 Nonmalignant lung disease 3 Total cases 52
Stage I (TIN NO Mo, T1 N1 Mo) 14 5
22 8
Total 49
Good 32 Poor 4 Not evaluated 13 Total 49
aTumor doubling time evaluated on 15/49 patients.
Stage
Stage I1 (T2 N1 Mo) Stage I11 (all T N2 Mo, T3 all N Mo) Stage IV (all T N with MI)
Delayed hypersensitivity reaction
mycin (courtesy of Pfizer, Rome, Italy) were added to 0.2 ml of cell suspension (7,161. The samples were then measured with an ICP 22 Phywe-type pulse cytophoto- meter (Ortho, Westwood, MA), equipped with a glass flow chamber kindly supplied by Dr. W. G6hde.
A sample of normal tissue from the same patient was always analyzed before each tumor sample. In the case of surgery, normal lung tissue was collected from an area clinically not suspect but relatively close to the lesion. In the case of biopsy, bronchial washing, and pleural effusion, peripheral blood lymphocytes were used. The position of the GI10 diploid peak was then identified by monitoring a mixture of cells from normal and tumor specimens. The ploidy of each cell subpopu- lation or clone (note that in the Results, the terms “sub- population” and “clone” are used as synonyms) was expressed as DNA index (DI = the ratio between the mode of the aneuploid peak and that of the normal peak). At least a total of 1.5 x lo4 cells was accumulated for each reading.
RESULTS Ploidy and Number of Clones
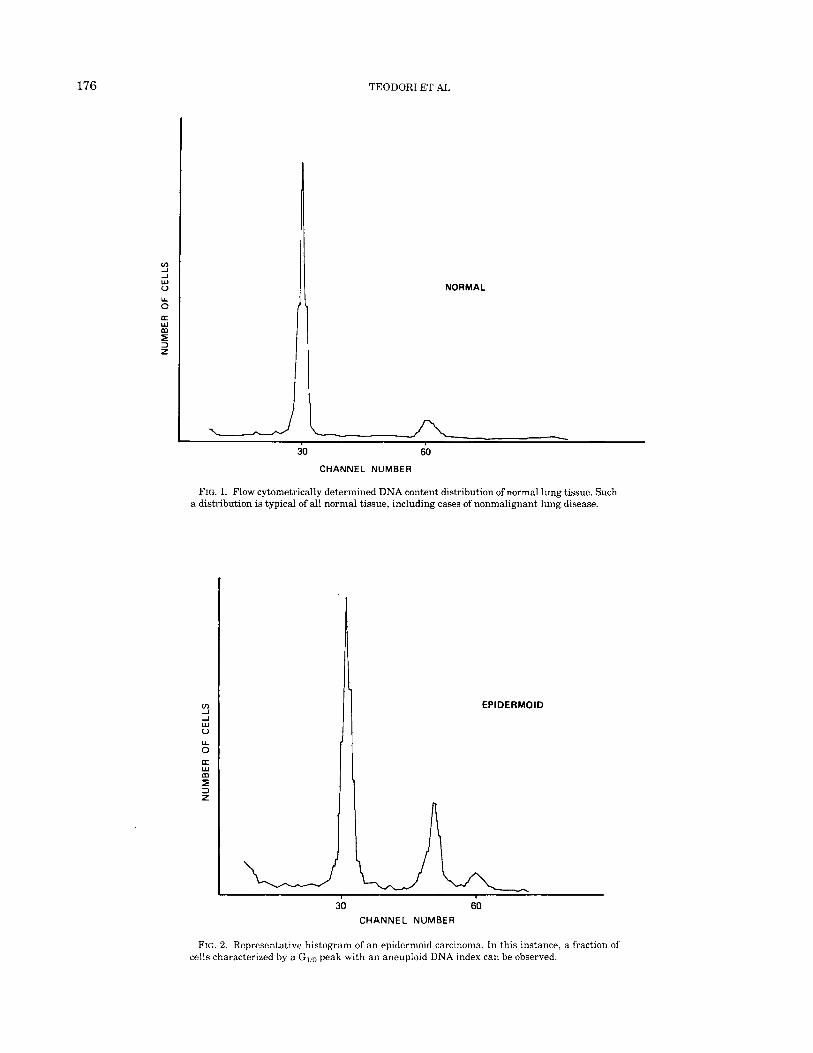
A representative histogram of a cytometrically deter- mined DNA content distribution for a lung normal tis- sue sample shows the usual diploid DNA content pattern of normal tissues (Fig. 1). The nonmalignant cases ex- amined, including Wegener’s syndrome, hyperplastic lymphoadenitis, and chondroma, also showed excusively diploid cell populations.
On the contrary, subpopulations with diploid and aneuploid DNA content were usually observed in tumor samples.
A representative histogram for epidermoid cell carci- noma is shown in Figure 2. In this instance, a subpopu- lation characterized by a Gl/o peak with an aneuploid value can be observed together with the diploid cell subpopulation. In the majority of cases, one or two aneu- ploid (hyperdiploid and/or hypoploid) clones were ob- served. It should be pointed out that the number of subpopulations reported here and below refers to those clones that have been consistently observed in all ali- quots of the same sample or, in the instance of multiple sampling, in all specimens from the same primary or metastasis. All 23 cases of epidermoid cell carcinoma are listed in Table 2, where the DI of all cell clones (Al, A2, etc.) are reported.
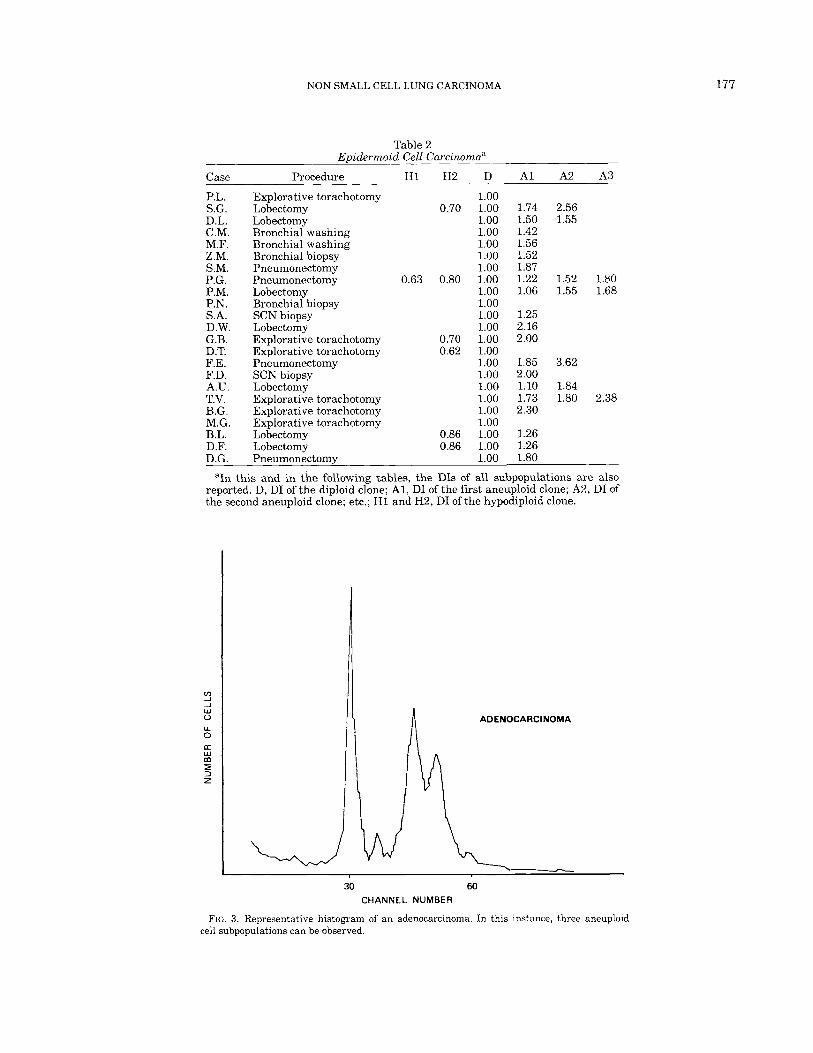
A representative histogram for adenocarcinoma is given in Figure 3. In the case illustrated in this figure, three aneuploid cell clones are present. The maximum number found was five aneuploid (hyperdiploid) clones (Table 3).
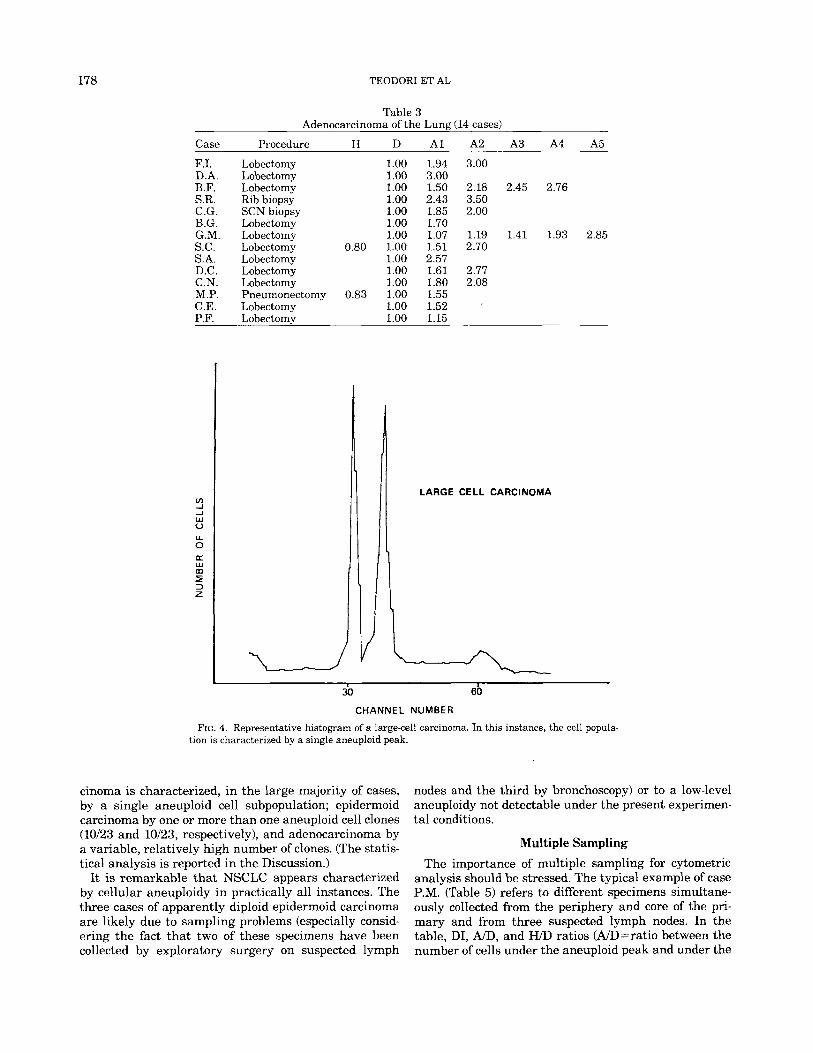
A representative histogram for large-cell carcinoma is shown in Figure 4, and the list of the cases with the DI values are reported in Table 4. In the instance of large- cell carcinoma, 10/12 cases exhibit only one aneuploid clone.
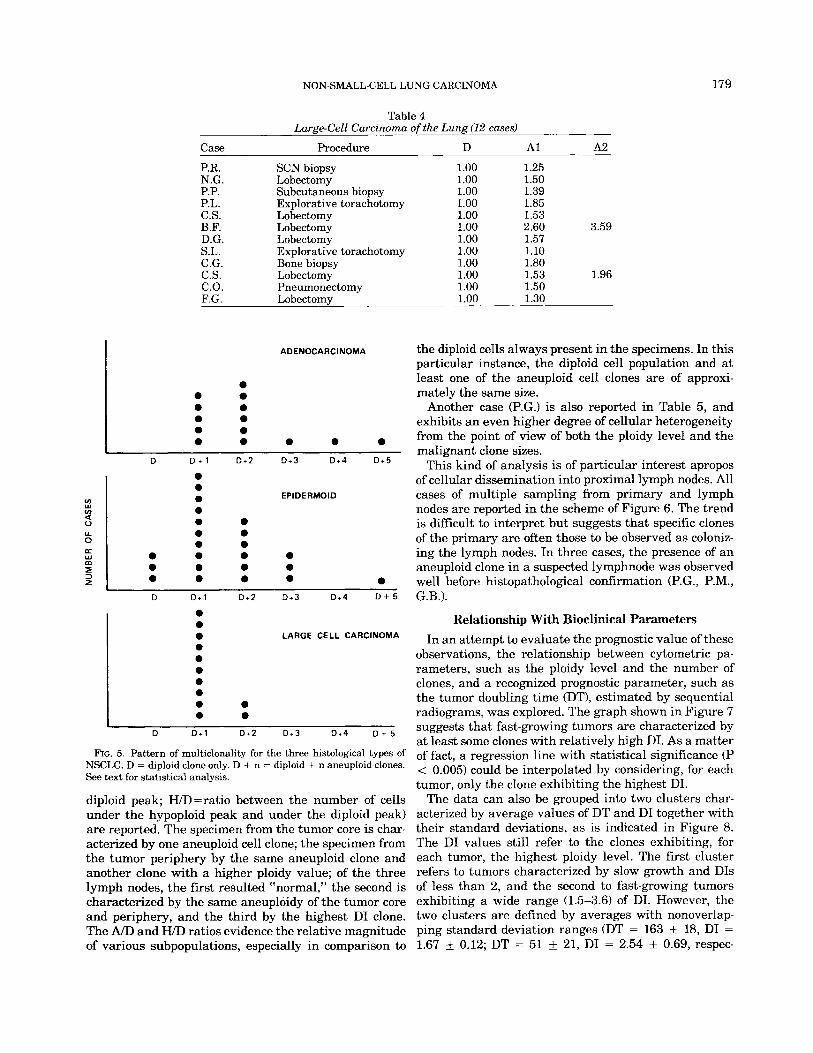
The occurrence of multiclonality, for the three histo- logical types, is summarized in Figure 5. Large-cell car-
176 TEODORI ET AL
m J -I W u Y 0
m 5 2 z
c w
NORMAL
30 60
CHANNEL NUMBER
FIG. 1. Flow cytometrically deterniined DNA content distribution of normal lung tissue. Such a distribution is typical of all normal tissue, including cases of nonmalignant lung disease.
m 1 -I w 0
0 Lc W
Y
m 5 3 z
EPlDERMOlD
30 60 CHANNEL NUMBER
FIG. 2. Representative histogram of an epidermoid carcinoma. In this instance, a fraction of cells characterized by a Glio peak with an aneuploid DNA index can be observed.
NON-SMALL-CELL LUNG CARCINOMA 177
Case
P.L . S.G. D.L. C.M. M.F. Z.M. S.M. P.G. P.M. P.N. S.A. D.W. G.B. D.T. F.E. F.D. A.U. T.V. B.G. M.G. B.L. D.F. D.G.
__
__
Table 2 Epidermoid Cell Carcinoma"
-
fn _I
J W 0 U 0 a m w
5 z
Procedure H1 H2 D A1 A2 A3
-
Explorative torachotomy Lobectomy Lobectomy Bronchial washing Bronchial washing Bronchial biopsy Pneumonectomy Pneumonectomy Lobectomy Bronchial biopsy SCN biopsy Lobectomy Explorative torachotomy Explorative torachotomy Pneumonectomy SCN biopsy Lobectomy Explorative torachotomy Explorative torachotomy Explorative torachotomy Lobectomy Lobectomy Pneumonectomy
1.00 0.70 1.00 1.74 2.56
1.00 1.50 1.55 1.00 1.42 1.00 1.56 1.00 1.52 1.00 1.87
0.63 0.80 1.00 1.22 1.52 1.80 1.00 1.06 1.55 1.68 1.00 1.00 1.25 1.00 2.16
0.70 1.00 2.00 0.62 1.00
1.00 1.85 3.62 1.00 2.00 1.00 1.10 1.84 1.00 1.73 1.80 2.38 1.00 2.30 1.00
0.86 1.00 1.26 0.86 1.00 1.26
1.00 1.80
ADENOCARCINOMA A
178 TEODORI ET AL
Table 3 Adenocarcinoma of the Lung (14 cases)
Case Procedure H D A1 A2 A3 A4 A5
F.I. Lobectomy 1.00 1.94 3.00 D.A. Lobectomy 1.00 3.00 B.F. Lobectomy 1.00 1.50 2.18 2.45 2.76 S.R. Rib biopsy 1.00 2.43 3.50 C.G. SCN biopsy 1.00 1.85 2.00 B.G. Lobectomy 1.00 1.70 G.M. Lobectomy 1.00 1.07 1.19 1.41 1.93 2.85 S.C. Lobectomy 0.80 1.00 1.51 2.70 S.A. Lobectomy 1.00 2.57 D.C. Lobectomy 1.00 1.61 2.77 C.N. Lobectomy 1.00 1.80 2.08 M.P. Pneumonectomy 0.83 1.00 1.55 C.E. Lobectomy 1.00 1.52 P.F. Lobectomv 1.00 1.15
LARGE CELL CARCINOMA
3b 60
CHANNEL NUMBER
FIG. 4. Representative histogram of a large-cell carcinoma. In this instance, the cell popula- tion is characterized by a single aneuploid peak.
cinoma is characterized, in the large majority of cases, by a single aneuploid cell subpopulation; epidermoid carcinoma by one or more than one aneuploid cell clones (10123 and 10123, respectively), and adenocarcinoma by a variable, relatively high number of clones. (The statis- tical analysis is reported in the Discussion.)
It is remarkable that NSCLC appears characterized by cellular aneuploidy in practically all instances. The three cases of apparently diploid epidermoid carcinoma are likely due to sampling problems (especially consid- ering the fact that two of these specimens have been collected by exploratory surgery on suspected lymph
nodes and the third by bronchoscopy) or to a low-level aneuploidy not detectable under the present experimen- tal conditions.
Multiple Sampling The importance of multiple sampling for cytometric
analysis should be stressed. The typical example of case P.M. (Table 5) refers to different specimens simultane- ously collected from the periphery and core of the pri- mary and from three suspected lymph nodes. In the table, DI, A/D, and WD ratios (A/D=ratio between the number of cells under the aneuploid peak and under the
Case
P.R. N.G. P.P. P.L. C.S. B.F. D.G. S.L. C.G. C.S. C.O. F.G.
~
NON-SMALL-CELL LUNG CARCINOMA
Table 4 Large-Cell Carcinoma of the Lung (12 cases)
- Procedure
SCN biopsy Lobectomy Subcutaneous biopsy Explorative torachotomy Lobectomy Lobectomy Lobectomy Explorative torachotomy Bone biopsy Lobectomy Pneumonectomy Lobectomy
ADENOCARCINOMA
0 0 0 0 0 0 0 0 0 0 0 0 0 0
D D + 1 D+2 D + 3 D + 4 D+5
0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0
EPIDERMOID
0 0 0 0 0
D D + 1 D+2 D + 3 D + 4 D + 5
0 0 0 LARGE CELL CARCINOMA 0 0 0 0 0 0 0 0 0
D D + 1 D+2 D+3 D + 4 D + 5
FIG. 5. Pattern of multiclonality for the three histological types of NSCLC. D = diploid clone only. D + n = diploid + n aneuploid clones. See text for statistical analysis.
diploid peak; H/D=ratio between the number of cells under the hypoploid peak and under the diploid peak) are reported. The specimen from the tumor core is char- acterized by one aneuploid cell clone; the specimen from the tumor periphery by the same aneuploid clone and another clone with a higher ploidy value; of the three lymph nodes, the first resulted “normal,” the second is characterized by the same aneuploidy of the tumor core and periphery, and the third by the highest DI clone. The A/D and H/D ratios evidence the relative magnitude of various subpopulations, especially in comparison to
D A1 A2 ~~
1.00 1.25 1.00 1.50 1.00 1.39 1.00 1.85 1.00 1.53 1.00 2.60 3.59 1.00 1.57 1.00 1.10 1.00 1.80 1.00 1.53 1.96 1.00 1.50 1.00 1.30
179
the diploid cells always present in the specimens. In this particular instance, the diploid cell population and at least one of the aneuploid cell clones are of approxi- mately the same size.
Another case (P.G.) is also reported in Table 5, and exhibits an even higher degree of cellular heterogeneity from the point of view of both the ploidy level and the malignant clone sizes.
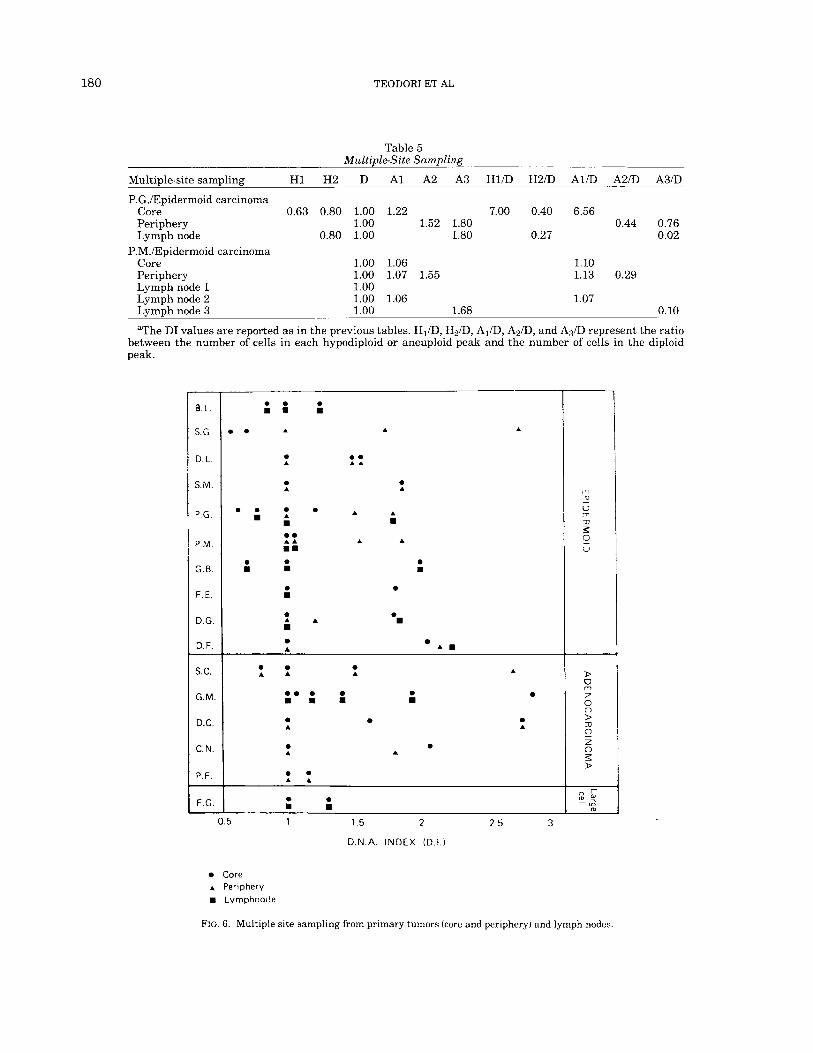
This kind of analysis is of particular interest apropos of cellular dissemination into proximal lymph nodes. All cases of multiple sampling from primary and lymph nodes are reported in the scheme of Figure 6. The trend is difficult to interpret but suggests that specific clones of the primary are often those to be observed as coloniz- ing the lymph nodes. In three cases, the presence of an aneuploid clone in a suspected lymphnode was observed well before histopathological confirmation (P.G., P.M., G.B.).
Relationship With Bioclinical Parameters In an attempt to evaluate the prognostic value of these
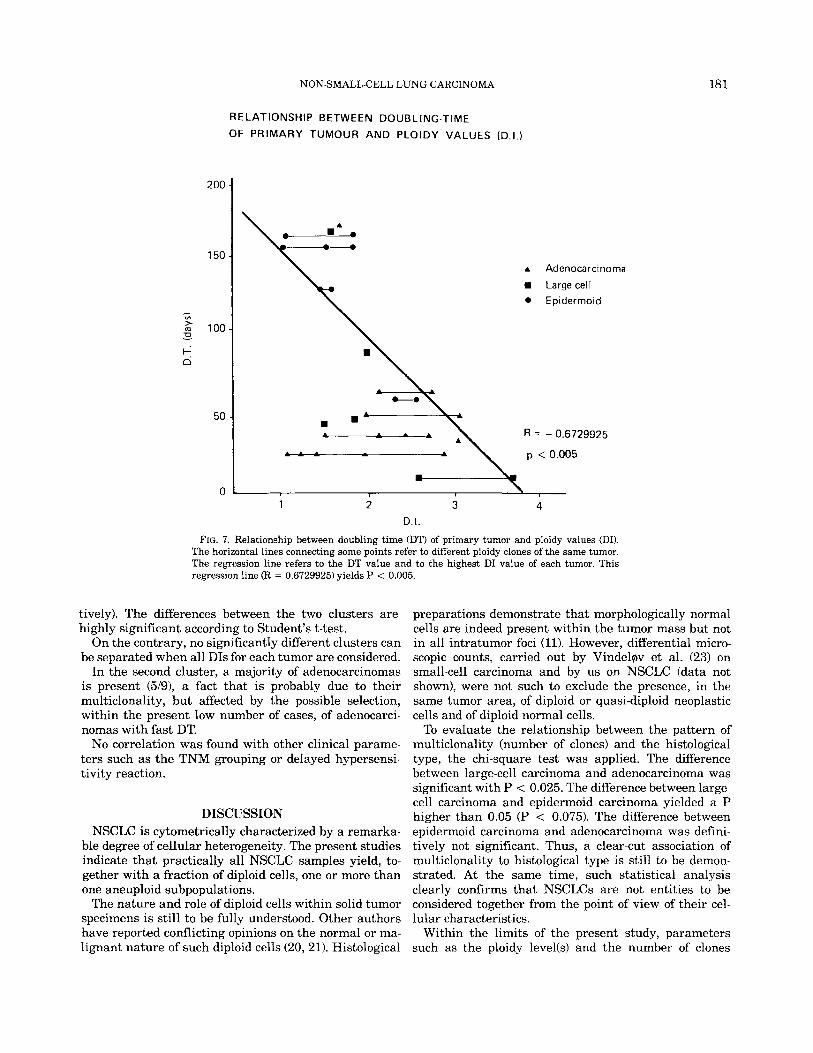
observations, the relationship between cytometric pa- rameters, such as the ploidy level and the number of clones, and a recognized prognostic parameter, such as the tumor doubling time (DT), estimated by sequential radiograms, was explored. The graph shown in Figure 7 suggests that fast-growing tumors are characterized by at least some clones with relatively high DI. As a matter of fact, a regression line with statistical significance (P < 0.005) could be interpolated by considering, for each tumor, only the clone exhibiting the highest DI.
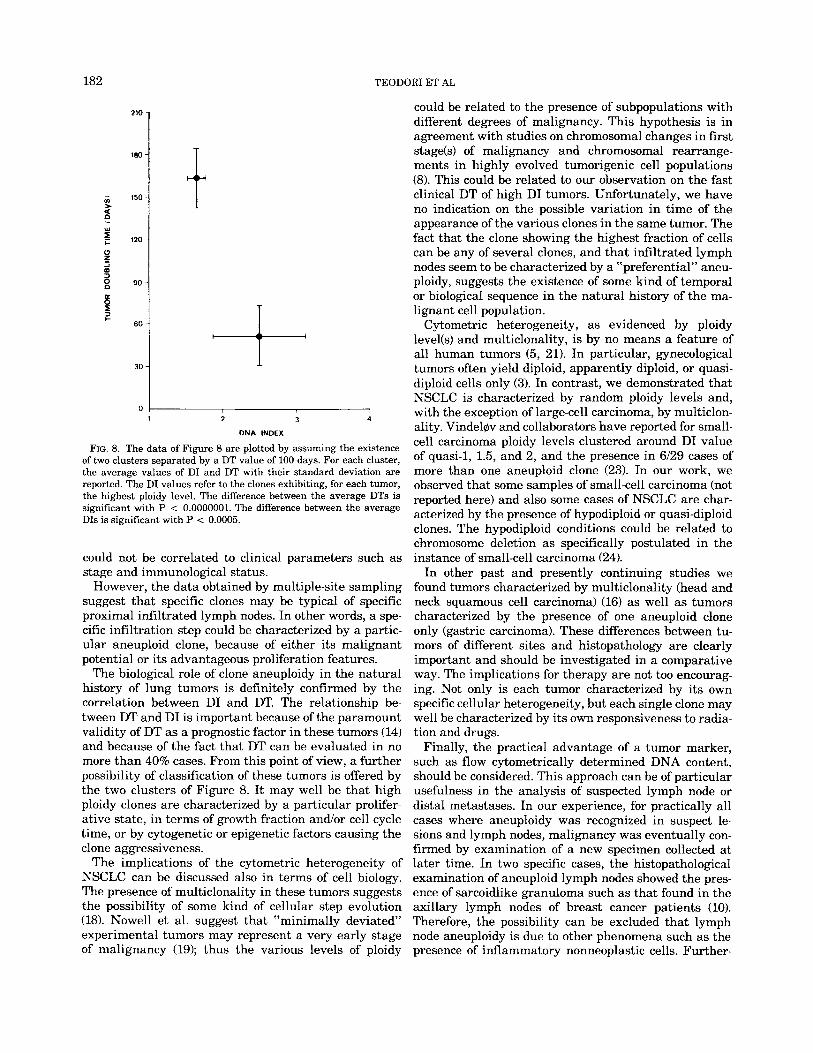
The data can also be grouped into two clusters char- acterized by average values of DT and DI together with their standard deviations, as is indicated in Figure 8. The DI values still refer to the clones exhibiting, for each tumor, the highest ploidy level. The first cluster refers to tumors characterized by slow growth and DIs of less than 2, and the second to fast-growing tumors exhibiting a wide range (1.5-3.6) of DI. However, the two clusters are defined by averages with nonoverlap- ping standard deviation ranges (DT = 163 * 18, DI = 1.67 f 0.12; DT = 51 f 21, DI = 2.54 * 0.69, respec-
180 TEODORI ET AL
Table 5 Multiple-Site Sampling
Multiple-site sampling H1 H2 D A1 A2 A3 H l D H 2 D A1D A2D A3/D
P.G./Epidermoid carcinoma Core 0.63 0.80 1.00 1.22 7.00 0.40 6.56 Periphery 1.00 1.52 1.80 0.44 0.76 Lymph node 0.80 1.00 1.80 0.27 0.02
P.M./Epidermoid carcinoma Core 1.00 1.06 1.10 Periphery 1.00 1.07 1.55 1.13 0.29
Lymph node 2 1.00 1.06 1.07
aThe DI values are reported as in the previous tables. HID, H2D, AID, A&, and A,D represent the ratio between the number of cells in each hypodiploid or aneuploid peak and the number of cells in the diploid peak.
Lymph node 1 1.00
Lymph node 3 1.00 1.68 0.10
B L
S G
D L
S M
P G
P M
G B
F E
D G
D F
S.C.
G.M.
D.C.
C.N.
P. F. - F.G.
0
D O
0 .
0 m
m
A
0 A
0 A
0 A
0 . A A .B
0
0 B
0 A
0
0
0 . A A
0 A
A
A
A
0 A
A B
A
0
0
A
B
A D
*. 0 0 m m m 0 A
0 A
0 A
0
0 A
A
0 A
0.5 1 1.5 2 2.5 3
D.N A. INDEX (D.I.)
Core A Periphery B Lyrnphnotle
FIG. 6. Multiple-site sampling from primary tumors (core and periphery) and lymph nodes.
NON-SMALL-CELL LUNG CARCINOMA 18 1
RELATIONSHIP BETWEEN DOUBLING-TIME
OF PRIMARY TUMOUR AND PLOIDY VALUES (D.1.)
A Adenocarcinorna
Large cell Epiderrnoid
1 2 3 4 D.I.
FIG. 7. Relationship between doubling time (DT) of primary tumor and ploidy values (DI). The horizontal lines connecting some points refer to different ploidy clones of the same tumor. The regression line refers to the DT value and to the highest DI value of each tumor. This regression line (R = 0.6729925) yields P < 0.005.
tively). The differences between the two clusters are highly significant according to Student’s t-test.
On the contrary, no significantly different clusters can be separated when all DIs for each tumor are considered.
In the second cluster, a majority of adenocarcinomas is present (5/9), a fact that is probably due to their multiclonality, but affected by the possible selection, within the present low number of cases, of adenocarci- nomas with fast DT.
No correlation was found with other clinical parame- ters such as the TNM grouping or delayed hypersensi- tivity reaction.
DISCUSSION NSCLC is cytometrically characterized by a remarka-
ble degree of cellular heterogeneity. The present studies indicate that practically all NSCLC samples yield, to- gether with a fraction of diploid cells, one or more than one aneuploid subpopulations.
The nature and role of diploid cells within solid tumor specimens is still to be fully understood. Other authors have reported conflicting opinions on the normal or ma- lignant nature of such diploid cells (20,211. Histological
preparations demonstrate that morphologically normal cells are indeed present within the tumor mass but not in all intratumor foci (11). However, differential micro- scopic counts, carried out by Vindelqiv et al. (23) on small-cell carcinoma and by us on NSCLC (data not shown), were not such to exclude the presence, in the same tumor area, of diploid or quasi-diploid neoplastic cells and of diploid normal cells.
To evaluate the relationship between the pattern of multiclonality (number of clones) and the histological type, the chi-square test was applied. The difference between large-cell carcinoma and adenocarcinoma was significant with P < 0.025. The difference between large- cell carcinoma and epidermoid carcinoma yielded a P higher than 0.05 (P < 0.075). The difference between epidermoid carcinoma and adenocarcinoma was defini- tively not significant. Thus, a clear-cut association of multiclonality to histological type is still to be demon- strated. At the same time, such statistical analysis clearly confirms that NSCLCs are not entities to be considered together from the point of view of their cel- lular characteristics.
Within the limits of the present study, parameters such as the ploidy level(s) and the number of clones
182 TEODORI ET AL
210
180
150
120
90
60
30
0 1 2 3
DNA INDEX
4
FIG. 8. The data of Figure 8 are plotted by assuming the existence of two clusters separated by a DT value of 100 days. For each cluster, the average values of DI and DT with their standard deviation are reported. The DI values refer to the clones exhibiting, for each tumor, the highest ploidy level. The difference between the average DTs is significant with P < 0.0000001. The difference between the average DIs is significant with P < 0.0005.
could not be correlated to clinical parameters such as stage and immunological status.
However, the data obtained by multiple-site sampling suggest that specific clones may be typical of specific proximal infiltrated lymph nodes. In other words, a spe- cific infiltration step could be characterized by a partic- ular aneuploid clone, because of either its malignant potential or its advantageous proliferation features.
The biological role of clone aneuploidy in the natural history of lung tumors is definitely confirmed by the correlation between DI and DT. The relationship be- tween DT and DI is important because of the paramount validity of DT as a prognostic factor in these tumors (14) and because of the fact that DT can be evaluated in no more than 40% cases. From this point of view, a further possibility of classification of these tumors is offered by the two clusters of Figure 8. It may well be that high ploidy clones are characterized by a particular prolifer- ative state, in terms of growth fraction andor cell cycle time, or by cytogenetic or epigenetic factors causing the clone aggressiveness.
The implications of the cytometric heterogeneity of NSCLC can be discussed also in terms of cell biology. The presence of multiclonality in these tumors suggests the possibility of some kind of cellular step evolution (18). Nowell et al. suggest that “minimally deviated” experimental tumors may represent a very early stage
could be related to the presence of subpopulations with different degrees of malignancy. This hypothesis is in agreement with studies on chromosomal changes in first stage(s) of malignancy and chromosomal rearrange- ments in highly evolved tumorigenic cell populations (8). This could be related to our observation on the fast clinical DT of high DI tumors. Unfortunately, we have no indication on the possible variation in time of the appearance of the various clones in the same tumor. The fact that the clone showing the highest fraction of cells can be any of several clones, and that infiltrated lymph nodes seem to be characterized by a “preferential” aneu- ploidy, suggests the existence of some kind of temporal or biological sequence in the natural history of the ma- lignant cell population.
Cytometric heterogeneity, as evidenced by ploidy level(s) and multiclonality, is by no means a feature of all human tumors (5, 21). In particular, gynecological tumors often yield diploid, apparently diploid, or quasi- diploid cells only (3). In contrast, we demonstrated that NSCLC is characterized by random ploidy levels and, with the exception of large-cell carcinoma, by multiclon- ality. Vindelov and collaborators have reported for small- cell carcinoma ploidy levels clustered around DI value of quasi-1, 1.5, and 2, and the presence in 6/29 cases of more than one aneuploid clone (23). In our work, we observed that some samples of small-cell carcinoma (not reported here) and also some cases of NSCLC are char- acterized by the presence of hypodiploid or quasi-diploid clones. The hypodiploid conditions could be related to chromosome deletion as specifically postulated in the instance of small-cell carcinoma (24).
In other past and presently continuing studies we found tumors characterized by multiclonality (head and neck squamous cell carcinoma) (16) as well as tumors characterized by the presence of one aneuploid clone only (gastric carcinoma). These differences between tu- mors of different sites and histopathology are clearly important and should be investigated in a comparative way. The implications for therapy are not too encourag- ing. Not only is each tumor characterized by its own specific cellular heterogeneity, but each single clone may well be characterized by its own responsiveness to radia- tion and drugs.
Finally, the practical advantage of a tumor marker, such as flow cytometrically determined DNA content, should be considered. This approach can be of particular usefulness in the analysis of suspected lymph node or distal metastases. In our experience, for practically all cases where aneuploidy was recognized in suspect le- sions and lymph nodes, malignancy was eventually con- firmed by examination of a new specimen collected at later time. In two specific cases, the histopathological examination of aneuploid lymph nodes showed the pres- ence of sarcoidlike granuloma such as that found in the axillary lymph nodes of breast cancer patients (10). Therefore, the possibility can be excluded that lymph node aneuploidy is due to other phenomena such as the
of malignancy (19); thus the various levels of ploidy presence of inflammatory nonneoplastic cells. Further-

NON-SMALL-CELL I
more, we were also able to perform flow cytometric mea- surements on fluid samples such as bronchial washing, pleural effusion, and expectorate.
In conclusion, flow cytometry appears to be a powerful tool for the study and the characterization of human solid tumors. Follow-up studies are presently under way in the attempt to establish the diagnostic and prognostic value of the flow cytometric approach.
LITERATURE CITED 1. American Joint Committe for Cancer Staging and End Results
Reporting: Manual for Staging of Cancer 1978, Library of Con- gress Catalogue No. 78-67059, 1978.
2. Arcangeli G, Mauro F, Nervi C, Starace G A critical appraisal of the usefulness of some biological parameters in predicting tumor radiation response of human head and neck cancer. Br J Cancer 41(Suppl IVk39-44, 1980.
3. Atkin NB, Kay R Prognostic significance of modal DNA value and other factors in malignant tumors, based on 1465 cases. Br J Cancer 40:210-221, 1979.
4. Barlogie B, Drewinko B, Dosik G, Freireich E J Cell kinetics and the management of malignant disease. In: Flow Cytometry IV, Laerum OD, Lindmo T, Thorud E (eds). Universitetsforlaget, Ber- gen, 1980, pp 385-391.
5. Barlogie B, Drewinko B, Raber M, Schwartzendruber DE: Cell kinetics in clinical oncology. In: Cell Growth, Nicolini C (ed), vol 2. Plenum Press, New York, 1982, pp 773-798.
6. Barlogie B, Drewinko B, Schumann J, Gdhde W, Dosik G, Latreille J, Johnston DA, Freirich E J Cellular DNA content as a marker of neoplasia in man. Am J Med 69:195-203,1980,
7. Barlogie B, Spitzer G, Hart JS, Johnston DA, Buchner T, Schu- mann J, Drewinko B DNA histogram analysis of human hemo- poietic cells. Blood 48:245-258, 1976.
8. Deaven LL, Scott-Cram L, Wells RS, Kraemer PM: Relationships between chromosome complement and cellular DNA content in tumorigenic cell populations. In: Genes Chromosomes and Neopla- sia, Arrighi FE, Rao PN, Stubblefield E (eds). Raven Press, New York, 1981, pp 419449.
9. Dethlefsen LA, Bauer KD, Riley R M Analytical cytometric ap- proaches to heterogeneous populations in tumors; A review. Cyto- metry 1:89-97,1980.
10. Fisher ER, Palekar AS, Gregorio RM, Redmond C, Fisher B: Path- ological findings from the National Surgical Adjuvant Breast Proj- ect. Significance of tumor necrosis. Hum Pathol9:523-530,1978.
11. Gazdar AF, Zweig MH, Carney DN, Van Steirteghen AC, Baylin SB, Minna JD: Levels of creatine kinease and its BB isoenzyme in lung cancer specimens and cultures. Cancer Res 41:2773-2777,
AJNG CARCINOMA 183
1981. 12. Ishikawa S, Hayata Y, Suemasu K: Lung cancer 1982. Exerpta
Medica International Congress Series 569, 1982. 13. Modini C, Passariello R, Loscone C, Cicconetti F, Simonetti G,
Zerilli M, Tirindelli-Danesi D, Stipa S: TNM staging in lung can- cer: Role of computered tomography. J Thorac Cardiovasc Surg 84569-574,1982.
14. Modini C, Pasquali-Lasagni R, Albertucci R, Botti C, Nadi F, Stipa S Role of the doubling time in the evaluation of lung cancer patients. 3rd World Conference on Lung Cancer, p 208,1982.
15. Modini C, Zerilli M, Tirindelli-Danesi D, Cicconetti F, Cristini R, Pasquali-Lasagni R, Albertucci M, Stipa S La classificazione dei carcinomi broncopolmonari in funzione della prognosi. Atti VII Corm di Aggiornamento in Chirurgia Generale, Pozzi L (ed), Roma, 1980, pp 97-105.
16. Nervi C, Badaracco G, Maisto A, Mauro F, Tirindelli-Danesi D, Starace G Cytometric evidence of cytogenetic and proliferative heterogeneity of human solid tumors. Cytometry 2:303-308, 1982.
17. Nervi C, Tirindelli-Danesi D, Modini C, Botti C, Teodori L, De Vita R, Mauro F, Starace G, Stipa S Non-smallcell carcinoma of the lung: Diagnostic value of cytometrically determined heteroge- neity. 3rd World Conference on Lung Cancer, p 69, 1982.
18. Nowell PC: The clonal evolution of tumor cell populations. Science 194:23-28; 1976.
19. Nowell PC, Morris HP, Potter VR: Chromosomes of “minimal deviation” hepatomas and some other transplantable rat tumors. Cancer Res 27:1565-1579, 1967.
20. Perez DJ, Taylor IW, Milthorpe BK, Govern VJ, Tattersall MHN: Identification and quantitation of tumour cells in cell suspensions: A comparison of cytology and flow cytometry. Br J Cancer 43526- 531,1981.
21. Temple WG, Sugarbaker EV, Thornthwartee ST, Hensley GT, Ket- cham A S Correlation of cell cycle analysis with Duke’s staging in colon cancer patients. J Surg Res 28:314-318, 1980.
22. Teodori L, De Vita R, Cordelli E, Tirindelli-Danesi D, Modini C, Nervi C, Stipa S, Mauro F Non-smallcellcarcinoma of the lung: Diagnostic and prognostic value of cytometrically determined cel- lular heterogeneity. 6th International Symposium on Flow Cytom- etry, p 210,1982.
23. Vindelev LL, Hansen HH, Christensen IJ, Spang-Thomsen M, Hirsch FR, Hansen M, Nissen NI: Clonal heterogeneity of small- cell anaplastic carcinoma of the lung demonstrated by flow cyto- metric DNA analysis. Cancer Res 40:4295-4300, 1980.
24. Whang-Peng JW, Kao-Shan CS, Lee EC, Bunn Pa, Carney DN, Gazdar AF, Minna JD: Specific chromosome defect associated with human smallcell-lung cancer: Delection 3P (14-23). Science 215:181-182, 1982.
25. World Health Organization. Histological typing of lung tumours. Tumori 6253-272, 1981.
Related Documents











