Non Invasive & Invasive Blood Pressure Monitoring Presenter- Dr Ranjith R T

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Non Invasive & Invasive Blood Pressure Monitoring
Presenter- Dr Ranjith R T
Introduction
Blood pressure monitoring is the most commonly used method of assessing the cardiovascular system.
The magnitude of BP is directly related to the Cardiac Output and the Systemic vascular resistance.
BP = (HR x TPR) x SVIt can be used for diagnosis and treatment of the patient. This can be achieved by non-invasive or invasive methods, continuously or intermittently depending on the requirements of the patient.

Mean Arterial Pressure
Time-weighted average of arterial pressures during a pulse cycle.
MAP = DBP + (SBP - DBP)/3 or
MAP = [SBP + (DBP x 2)] / 3. or
MAP = CO x TPR
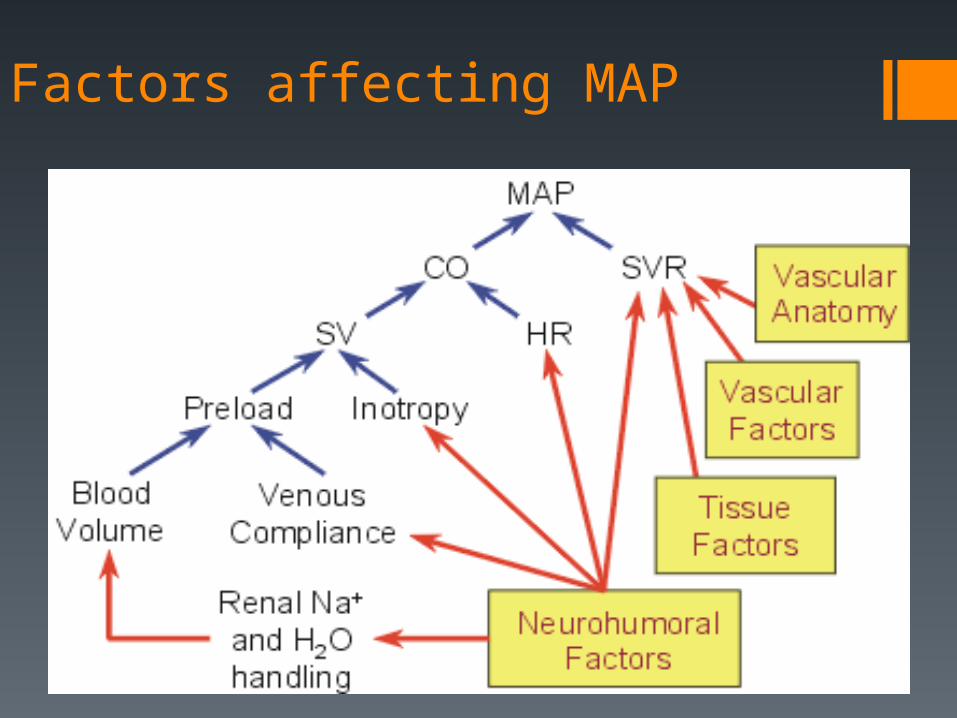
Factors affecting MAP

Types

Non Invasive intermittent BP monitoring INDICATIONS and CONTRAINDICATIONS
Requirements:Three key components:
1. an inflatable cuff for occluding the arterial supply to the distal limb;
2. a method for determining the point of systolic and diastolic blood pressures;
3. a method for measuring pressure.

Techniques
PALPATION
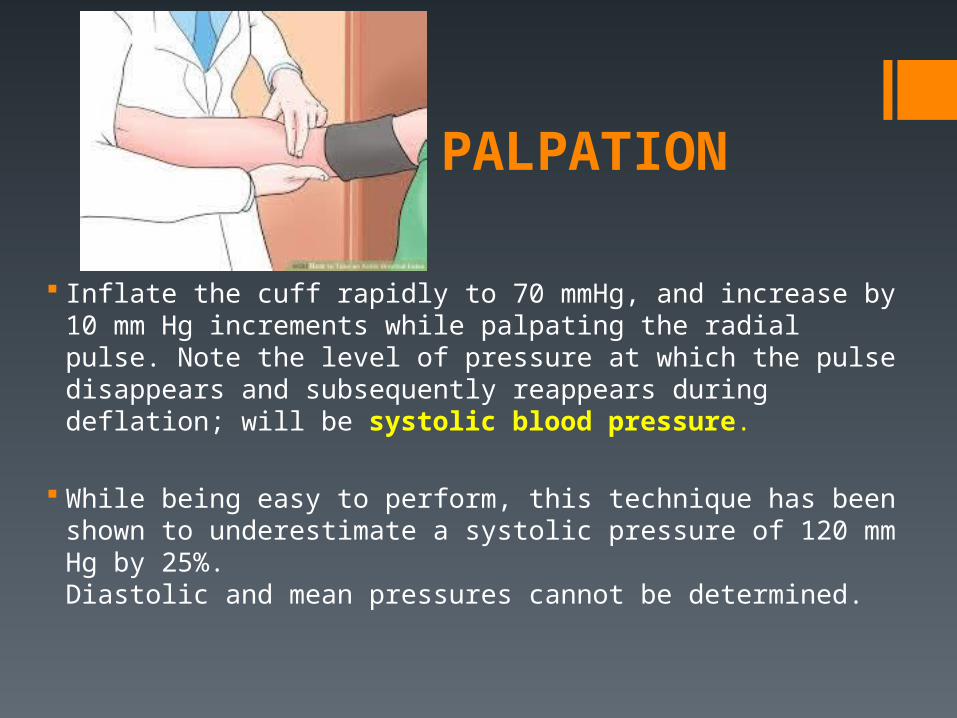
Inflate the cuff rapidly to 70 mmHg, and increase by 10 mm Hg increments while palpating the radial pulse. Note the level of pressure at which the pulse disappears and subsequently reappears during deflation; will be systolic blood pressure.
While being easy to perform, this technique has been shown to underestimate a systolic pressure of 120 mm Hg by 25%.Diastolic and mean pressures cannot be determined.

DO
PPLE
R
Systolic pressure can also be determined using the Doppler principle. Blood flow towards or away from the Doppler probe, reflects sound waves causing a change in frequency that is detected using the same Doppler probe.
As Doppler is so sensitive, this technique is usually reserved for the measurement of low pressures, e.g. vascular insufficiency.

AUSCULTATION
The cuff should be 20% wider than the diameter of the part of the limb being used (or cover two-third its length).

OSCILLOMETRY The Von Recklinghausen Oscillotonometer uses two cuffs and two bellows
connected to a measurement gauge.
The two cuffs overlap, one occludes the artery (occluding cuff) and the other senses the arterial signal (sensing cuff). Pressure from both cuffs is transmitted to the two bellows which is in turn displayed via a single gauge, alternating between the two bellows using a lever.
With the lever in the sensing position, the occlusive cuff is inflated above systolic pressure. The cuff is then deflated using a bleed valve until the needle suddenly starts to move vigorously. The lever is then switched to measure the occluding cuff pressure. This is the systolic blood pressure. With the lever back in the ‘sensing cuff’ position, the occluding cuff is deflated further. The needle will jump further with maximal oscillations occurring at mean arterial pressure (MAP), as measured by moving the lever once more. Diastolic pressure is the point at which these oscillations reduce.

OSCILLOMETRY

PLETHYSMOGRAPHY
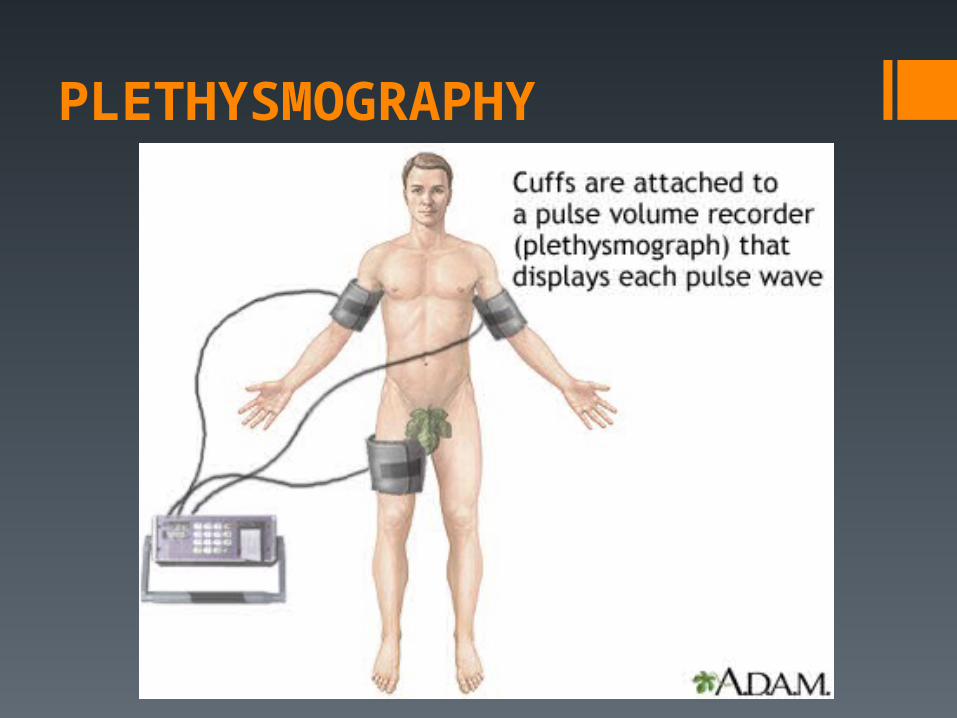
Blood pressure cuffs or other sensors are placed at different locations on the arms, legs, fingers, and/or toes. The sensors record the pulse waves that occur with each heart beat. (This data is translated into a graphic recording for later review.)
In some cases, the test also records changes in pulsation under various conditions, such as exposure to cold or temporary stoppage of blood flow to the limb (which is done by inflating a blood pressure cuff in the upper region of the limb until the blood vessels collapse).
The test usually takes less than 20 to 30 minutes.
PLETHYSMOGRAPHY

TONOMETRYIn order to obtain a stable bp signal, the tonometric sensor must be protected against movement and other mechanical artifacts.The artery wall does not influence the transmission of arterial pressure to a sensor applied to the skin. They have also been used to determine arterial elasticity and pulse wave velocity.
Under favorable conditions, the accuracy of tonometric measurements can be described by standard deviations of 5 mmHg.∼

INVASIVE BP MONITORING
Indications
Major surgical procedures involving large fluid shifts or blood loss
Surgery requiring cardiopulmonary bypass Surgery of the aorta Patients with pulmonary disease requiring frequent arterial
blood gases Patients with recent myocardial infarctions, unstable angina, or
severe coronary artery disease Patients with decreased left ventricular function (congestive
heart failure) or significant valvular heart disease Patients in hypovolemic, cardiogenic, or septic shock or with
multiple organ failure

Indications
Procedures involving the use of deliberate hypotension or deliberate hypothermia
Massive trauma cases Patients with right-sided heart failure, chronic obstructive
pulmonary disease, pulmonary hypertension, or pulmonary embolism
Patients requiring inotropes or intra-aortic balloon counterpulsation
Patients with electrolyte or metabolic disturbances requiring frequent blood samples
Inability to measure BP noninvasively (e.g., morbid obesity)

Arterial BP Monitoring
In short. INDICATIONS:INDICATIONS:
-Anticipated Hypotension-Wide Blood Pressure Deviations-End Organ Damage-Need for multiple ABG measurements

SitesFactors that influence the site of arterial cannulation
Location of surgery, The possible compromise of arterial flow due to patient
positioning or surgical manipulations, and Any history of ischemia of or prior surgery on the limb to be
cannulated. The presence of a proximal arterial cutdown. The proximal
cutdown may cause damped waveforms or falsely low BP readings due to stenosis or vascular thrombosis.

ADVANTAGES DISADVANTAGES
Radial Artery
Superficial location.Easy to identify and
cannulate.Collateral circulation.CC can be assessed.Accessible during major
surgeries.Patient can be mobilized.
Small size artery.Higher rate of catheter
malfunction.Not reliable in
vasoconstriction.Considerable augmentation
of SBP.Overshoot artifact.
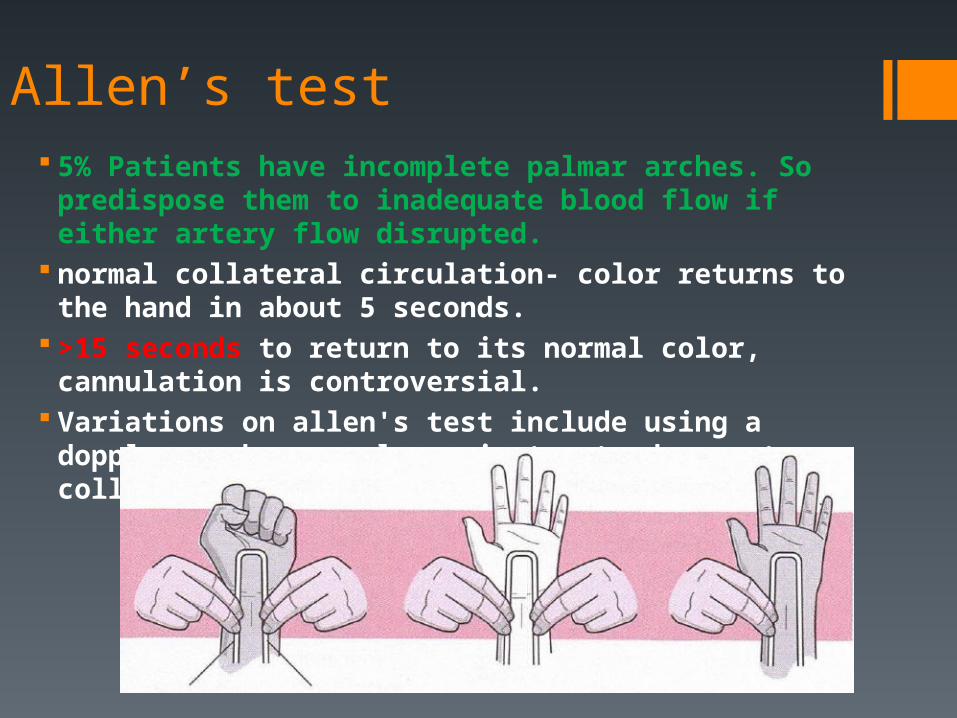
Allen’s test 5% Patients have incomplete palmar arches. So predispose
them to inadequate blood flow if either artery flow disrupted. normal collateral circulation- color returns to the hand in
about 5 seconds. >15 seconds to return to its normal color, cannulation is
controversial. Variations on allen's test include using a doppler probe or
pulse oximeter to document collateral flow

Other Sites The brachial artery lies in close proximity to the median nerve.
Its pressure tracings resemble those in the femoral artery, and were found to more accurately reflect central aortic pressures (Kinking problem)
The femoral artery may be cannulated for monitoring purposes but is usually reserved for situations in which other sites are unable to be cannulated or it is specifically indicated (e.g., descending thoracic aortic aneurysm surgery for distal pressure monitoring).
The femoral artery for hemodynamic monitoring purposes was as safe as radial artery cannulation
(Atheroma, Pseuaneurysm, Infections, Thrombosis, Rarely- Aseptic necrosis of head of femur in children)

Other Sites
The Axillary artery Advantages include patient comfort, mobility, and access to a central
arterial pressure waveform. Complications appear to be infrequent and similar in incidence to
radial and femoral artery catheterization If the axillary approach is chosen, the left side is preferred over the
right because the axillary catheter tip will lie distal to the aortic arch and great vessels.
Risk of cerebral embolization is increased whenever more centrally located arterial catheters are used.
Dorsalis pedis, Posterior Tibial


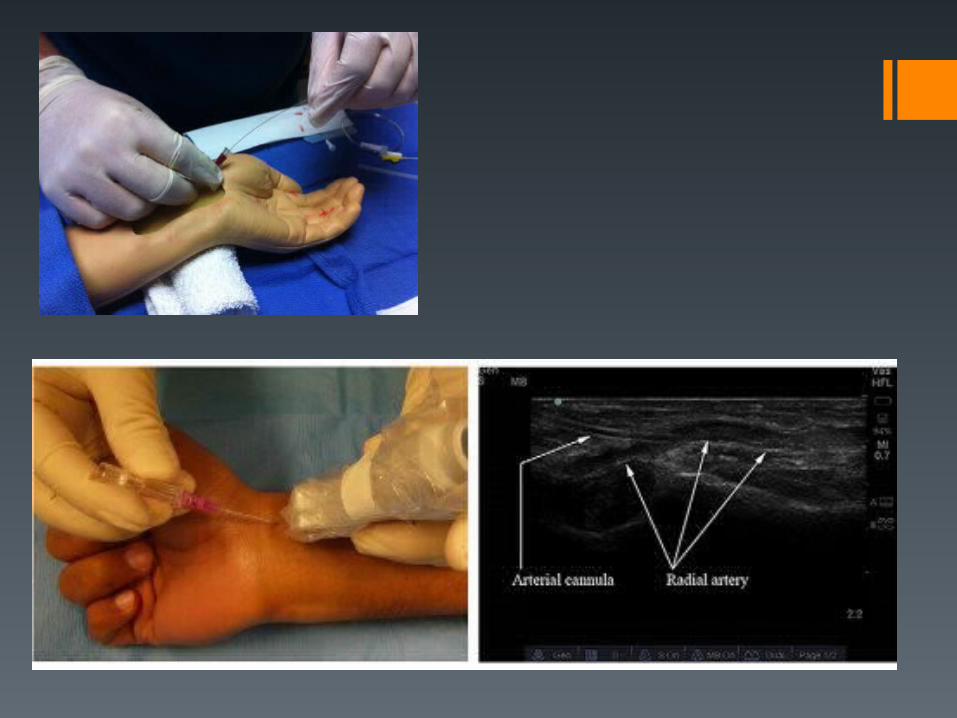
Insertion Techniques
Direct cannulation Transfixation Seldinger technique Doppler assisted technique Two dimentional USG assisted method Surgical cutdown


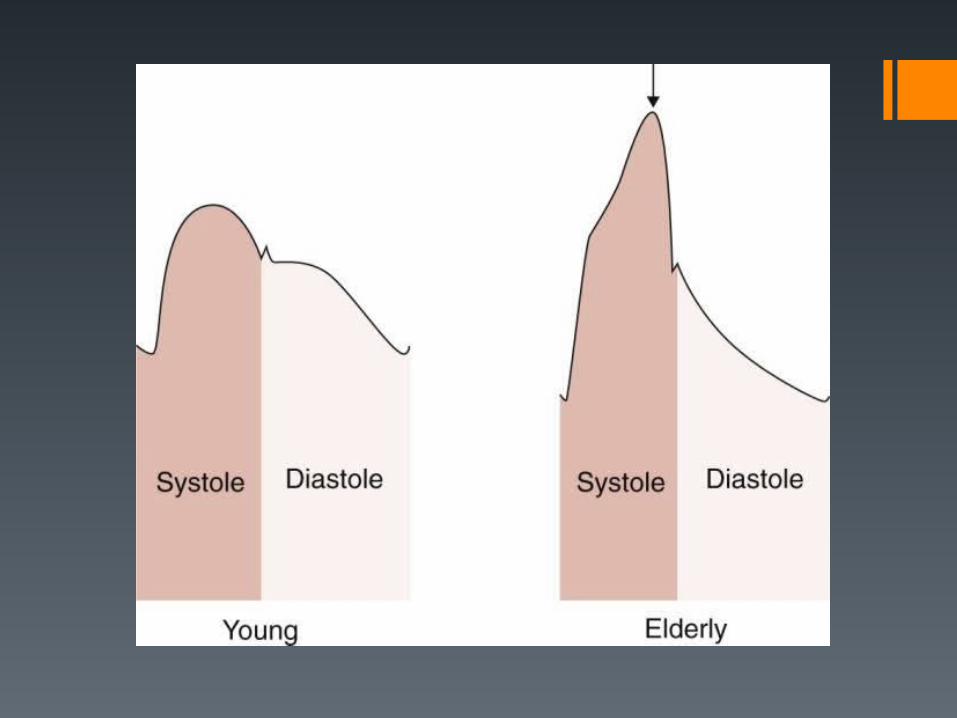
Components of Arterial waveform
Notch- Aortic valve closure as a result of backflow from already existing pressure in aorta.
Sometimes a second notch is seen in waveform. Due to rebound of wave from periphery- Incisure Notch
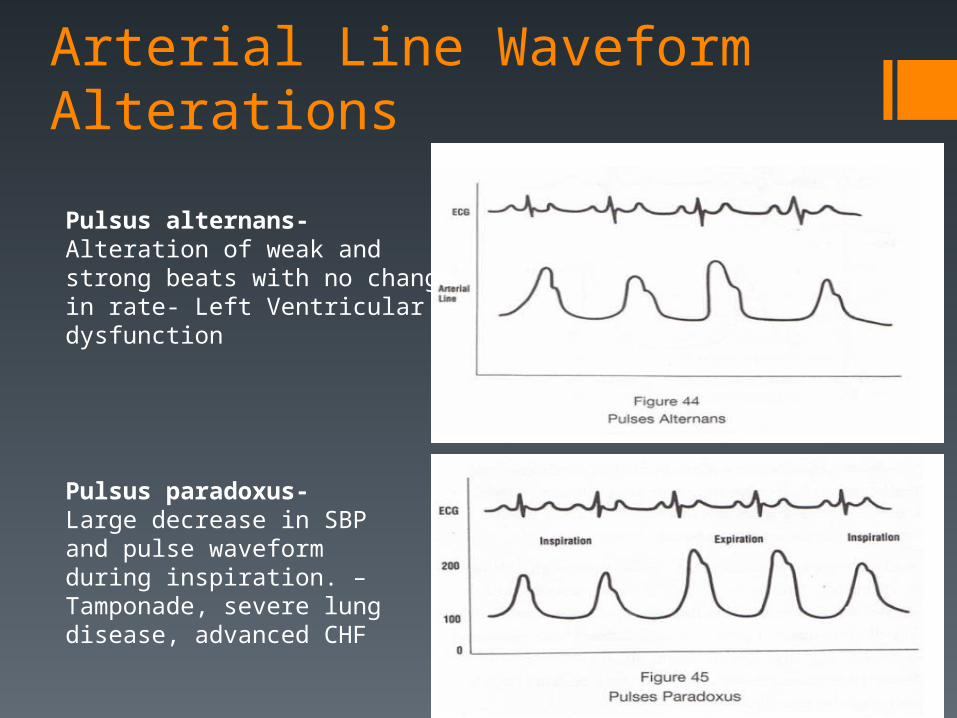
Arterial Line Waveform Alterations
Pulsus alternans- Alteration of weak and strong beats with no change in rate- Left Ventricular dysfunction
Pulsus paradoxus- Large decrease in SBP and pulse waveform during inspiration. – Tamponade, severe lung disease, advanced CHF

Arterial Line Waveform Alterations
Aortic Stenosis- Dicrotic notch not well defined from abnormal closure of leaflet. Narrow pulse pressure
Aortic Insufficiency- Wide pulse pressure. High blood volume. High peak systolic pressure during further systoles.

Arterial Line Waveform Alterations
Atrial Fibrillation- Irregular. Shorter diastolic filling time. Decreasing systolic peak amplitude during premature ventricular complexes.
Technical Aspects
The SBP, DBP and MAP are all displayed. But it is the MAP that tends to guide practice. Provides overall indication of peripheral tissue perfusion. In critically ill patients, MAP is maintained >70 mm Hg in order to maintain adequate renal and cerebral perfusion.
Usefulness of information depends on accuracy. Accuracy depends on responsibility to maintain that accuracy.
Responsibilities:Patency, Levelling, Zeroing, Square wave testing
Patency Soft Tubing to bag of NaCl containing 500mL flush solution placed in
pressure bag and inflated to 300 mm Hg. Why 300 mm Hg?
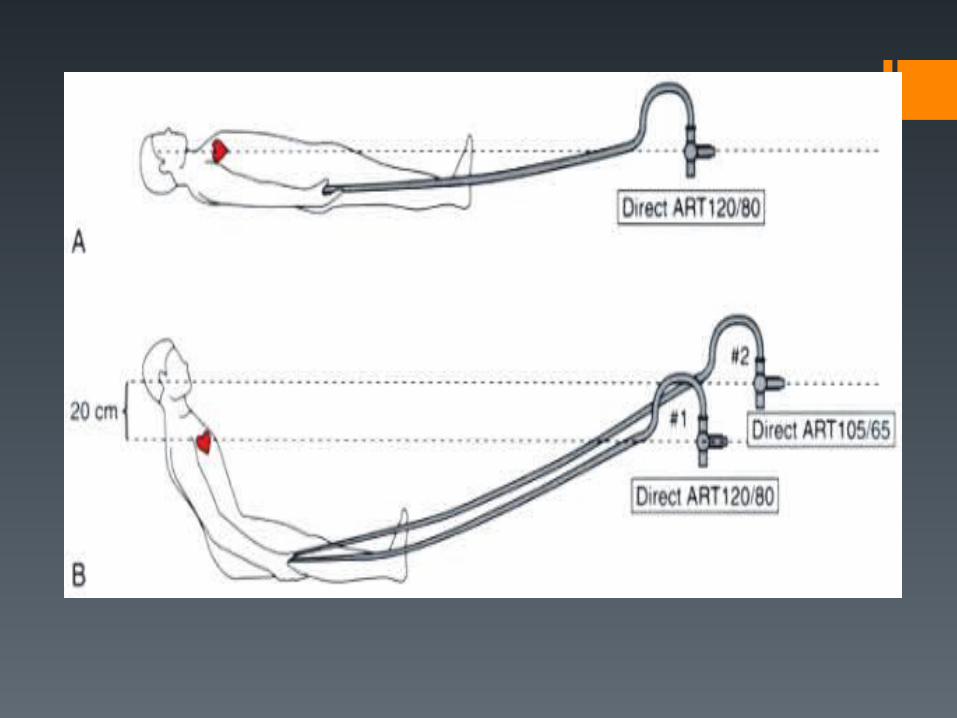
Leveling Minimises effect of hydrostatic pressure on the transducer.
Too High- lower pressure. Abnormally low pressure, Too Low- greater pressure. Abnormally high pressure.
Zeroing Negates influence of external pressures on monitoring system.
Square wave testing Helps identify if arterial line is over or under damped.
Method:-Activating the fast flush-Observe arterial waveform square off at the top and then drop to zero as the flush is released.
Normal- Immediate downstroke with just 1 or 2 oscillations within 0.12 seconds and rapid return to baseline.
Overdamped- slurred upstroke or downstroke with no oscillations above or below the baseline. Underestimates SBP and falsely high DBP. CORRECTION- check for air bubbles, clots, kinking.
Underdamped- Numerous oscillations above or below the baseline. Over estimates SBP. Under estimates DBP. CORRECTION- excessive tubing, multiple stopcocks. (Tachycardia, High CO)
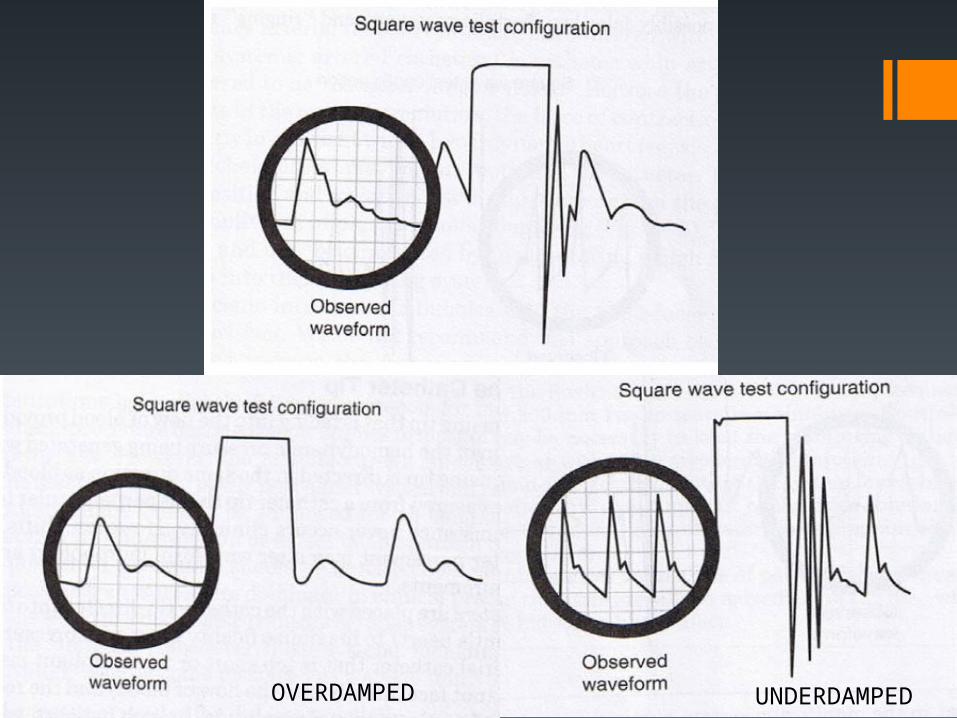
OVERDAMPED UNDERDAMPED
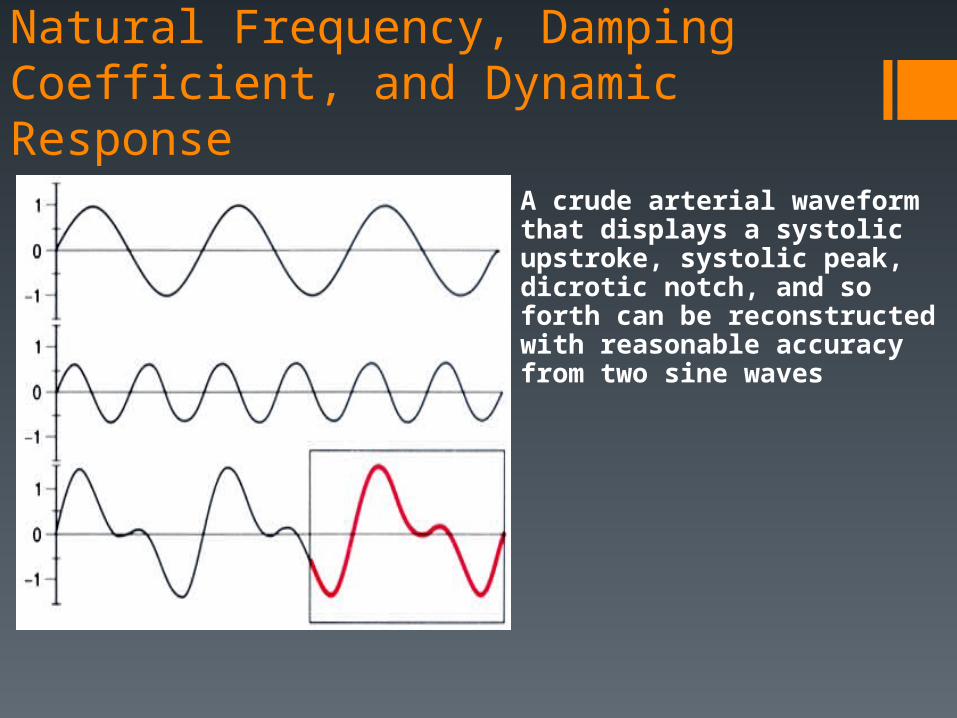
Natural Frequency, Damping Coefficient, and Dynamic Response
A crude arterial waveform that displays a systolic upstroke, systolic peak, dicrotic notch, and so forth can be reconstructed with reasonable accuracy from two sine waves

Natural Frequency, Damping Coefficient, and Dynamic Response
As a general rule, 6 to 10 harmonics are required to provide distortion-free reproduction of most arterial pressure waveforms

Damping
Most catheter-tubing transducer systems are underdamped but have an acceptable natural frequency that exceeds 12 Hz.
If the system's natural frequency is lower than 7.5 Hz, the pressure waveform is often distorted, and no amount of damping adjustment can restore the monitored waveform to adequately resemble the original waveform
If the natural frequency can be increased sufficiently (e.g., 24 Hz), damping will have minimal effect on the monitored waveform


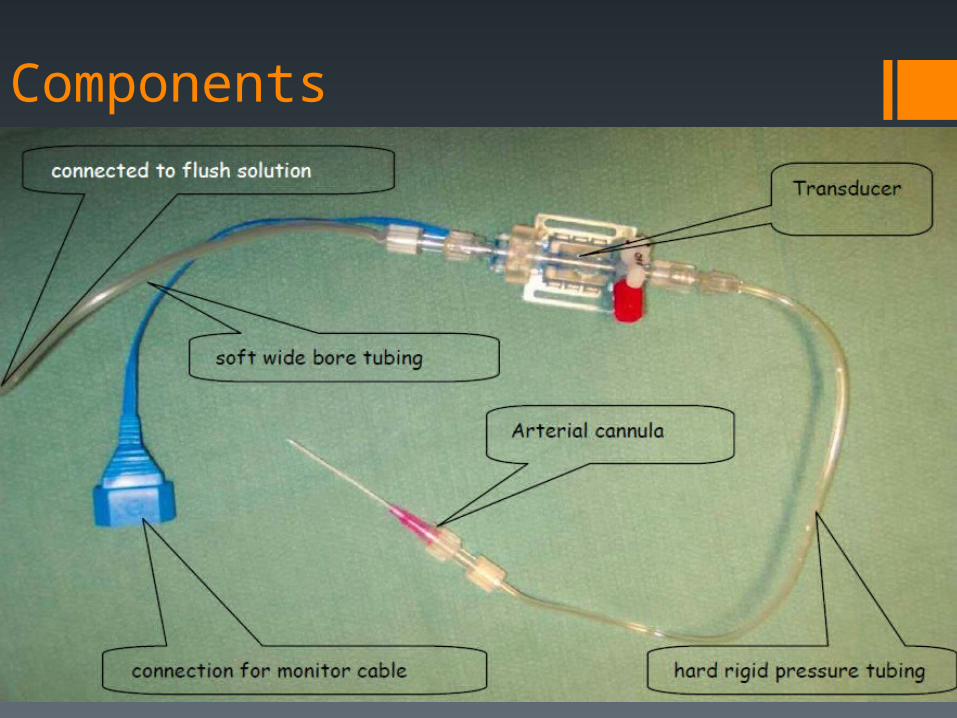
Components

Components
The intra-arterial catheter, extension tubing, stopcocks, in-line blood sampling set, pressure transducer, continuous-flush device, and electronic cable connecting the bedside monitor and waveform display screen.
The flush device provides a continuous, slow (1 to 3 mL/hr) infusion of saline to purge the monitoring system
Transducers Most transducers are resistance types that are based on the strain
gauge principle: stretching a wire or silicone crystal changes its electrical resistance.
The sensing elements are arranged as a Wheatstone bridge circuit so that the voltage output is proportionate to the pressure applied to the diaphragm




Arterial BP Gradient
Various pathophysiologic disturbances may produce generalized arterial pressure gradients in the body. Large differences in peripheral and central arterial pressure may be seen in patients in shock. Other vasoactive drugs, anesthetics (particularly neuraxial blockade), and changes in patient temperature produce pressure gradients. During hypothermia, thermoregulatory vasoconstriction causes radial artery systolic pressure to exceed femoral artery systolic pressure, whereas during rewarming, vasodilation reverses this gradient and causes radial artery pressure to underestimate femoral artery pressure.

Pulse Pressure Variation
Inspiration Expiration
Complications Hematoma/blood loss (Diagnostic also) Thrombosis/Embolisation: Fibrin/Particulate/Air Distal ischemia Retrograde emboli to brain
Vascular insufficiency: Large catheter small vessel Radial>Femoral Peripheral vascular disease DM Extended duration
Ischaemic necrosis of overlying skin Arterial injury Infection Accidental intraarterial injection of drugs Pseudoaneurysm HIT Bowel perforation AVF

52
Care
Aseptic precautions Daily inspection & dressing Pressure bag Transducer to be changed every 72 hours Arterial line to be changed/removed after 1 week Joint near the cannulation site: neutral position Prompt removal if signs of ischaemia

Thank you
Related Documents











