10/20/2015 1 From Hygienic Task to Preventive Intervention: Preventing and Managing Incontinence Associated Dermatitis in the Critical Care Unit Presented by: Denise Nix, MS, RN, CWOCN Mikel Gray, PhD, FNP, PNP, CUNP, CCCN, FAANP, FAAN October 21, 2015 1 pm EDT Objectives • Review etiology and epidemiology of IAD in the critical care unit. • Discuss the natural history of IAD in the acute and critical care settings and its relationship to pressure ulcer risk. • Identify strategies to prevent IAD in the critical care unit, and its incorporation into preventive care bundles for hospital acquired pressure ulcers and catheter associated urinary tract infection. • Outline strategies for managing IAD in the critical are unit, including strategies for containing urinary and fecal incontinence. Definition: Incontinence Associated Dermatitis (IAD) • Irritation and inflammation associated with exposure to stool or urine • Often accompanied by erosion of the skin • Sometimes accompanied by secondary cutaneous infection (candidiasis) Gray M, et al. J Wound Ostomy Continence Nurs. 2012;39(1):61-74.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
10/20/2015
1
From Hygienic Task to Preventive Intervention: Preventing and
Managing Incontinence Associated Dermatitis in the Critical Care Unit
Presented by:
Denise Nix, MS, RN, CWOCN
Mikel Gray, PhD, FNP, PNP, CUNP, CCCN, FAANP, FAAN
October 21, 2015
1 pm EDT
Objectives
• Review etiology and epidemiology of IAD in the critical care unit.
• Discuss the natural history of IAD in the acute and critical care settings and its relationship to pressure ulcer risk.
• Identify strategies to prevent IAD in the critical care unit, and its incorporation into preventive care bundles for hospital acquired pressure ulcers and catheter associated urinary tract infection.
• Outline strategies for managing IAD in the critical are unit, including strategies for containing urinary and fecal incontinence.
Definition: Incontinence Associated Dermatitis (IAD)
• Irritation and inflammation associated with
exposure to stool or urine
• Often accompanied by erosion of the skin
• Sometimes accompanied by secondary cutaneous
infection (candidiasis)
Gray M, et al. J Wound Ostomy Continence Nurs. 2012;39(1):61-74.

10/20/2015
2
Etiology
• Two etiologic factors– Fecal incontinence
– Urinary incontinence
• Multiple possible risk
(associated) factors– Nutrition
– Acuity of illness
– Immobility
IAD: Etiologic Factors
• Stool: fecal enzymes– Proteases and lipases are pH sensitive
– Both destroy down principal elements of skin’s
moisture barrier (proteins and fats)1,2
– In vivo evidence shows that exposure to digestive
enzymes in human skin leads to3
• ↑ TEWL
• ↑ pH
– Damage is exacerbated with liquid stool (diarrhea)
1. Atherton DJ. Eur Academy Dermatology Venerology. 2001;15(Supp1):1.
2. Gray M. J Wound Ostomy Continence Nurs. 2004;31(1 Suppl):S2-9.
3. Anderson PH, et al. Contact Dermatitis. 1994;30(3):152.
IAD: Etiologic Factors
• Urine: hyperhydration, pH, mechanical effects– ↓ skin hardness, rendering it more susceptible to
friction, shear and erosion1-3
– Hyperhydration also ↑ pH of skin4
• ↑ permeability to pathogenic species
• ↑ activates/supports activity of lipases and proteases
– Effects exacerbated by saturated occlusive device such
as warp around incontinence brief
1. Berg W, et al. Pediatric Dermatology. 1986;3:102.
2. Leyden JJ, et al. Archives of Dermatology. 1977;113:1678.
3. Gray M. J Wound Ostomy Continence Nurs. 2004;31(1 Suppl):S2-9.
4. Zimmerer RE, et al. Pediatric Dermatology. 1986;3:95.

10/20/2015
3
• Junkin and Selekof: 22%-27% in multisite study of
three acute care facilities1
• National QI database with 3,884 patient
observations involving 424 acute care facilities – 1,716 were incontinent of urine or stool
• 57% had double incontinence (UI and FI)
• 27% had FI alone
• 15% had UI alone
– Prevalence of IAD: 24%
1. Gray M, et al. J Wound Ostomy Continence Nurs. 2012;39(1):61-74.
Epidemiology of IAD: Prevalence in Acute Care (includes critical care units)
Epidemiology of IAD: Prevalence in Acute Care (includes critical care units)
• National QI database (3,884 patient observations;
424 acute care facilities) – 60% of IAD ranked as mild
– 27% of IAD ranked as moderate
– 5% of IAD ranked as severe
• 74.7% of IAD was facility acquired
• Patients with double UI and FI were more likely to
develop UI than patients with FI or UI alone
(p<0.001)
Table from: Gray M, et al. J Wound Ostomy Continence Nurs. 2012;39(1):61-74.
Epidemiology of IAD: Incidence in Critical Care

10/20/2015
4
IAD and Pressure Ulcer Risk
• Association between these conditions is extremely
strong but precise nature of the relationship is not
entirely understood
• IAD vs. Stage II PU especially problematic1
• FI and double incontinence strongly associated
with PU risk, mixed evidence concerning UI alone2-6
1. Bates-Jensen BB. J Wound Ostomy Continence Nurs. 2009;36(3):277-84.
2. Maklebust J, Magnan MA. Advances in Wound Care. 1994;7(6):25.
3. Gunninberg L. Journal of Wound Care. 2004;13(7):286.
4. Fader M, et al. Journal of Clinical Nursing. 2003;12(3):374.
5. Berlowitz DR, et al. Journal of the American Geriatrics Society. 2001;49(7):866-
71.
6. Narayan S, et al. J Wound Ostomy Continence Nurs. 2005;32(3):163.
IAD and PU Risk: Multisite National Database Analysis
• National QI database (3,884 patient observations;
424 acute care facilities) – Relationship of IAD to all sacral pressure ulcers (Stage
II-IV, unstageable), based on modeling using logistic
regression• Incontinence was not associated with PU occurrences
• Persons with IAD were more likely to develop PU than those
without IAD and immobility (OR=4.56; 95% CI 3.68-5.65)
• IAD was associated with greater likelihood of developing any
PU, even when analysis adjusted for immobility (35.4% vs.
12.4%, p<0.001)
IAD and PU Risk: Multisite National Database Analysis
• National QI database (3,884 patient observations;
424 acute care facilities) – Relationship of IAD to full thickness pressure ulcers
(Stage III-IV, unstageable), based on modeling using
logistic regression• Persons with IAD were more likely to develop a full thickness
sacral pressure ulcer (OR=2.65, 95% CI 1.74-4.03)
• Persons with IAD were more likely to develop a full thickness
PU than were persons without IAD, even when controlling for
immobility (6.9% vs. 3.3%, p<0.001)
10/20/2015
5
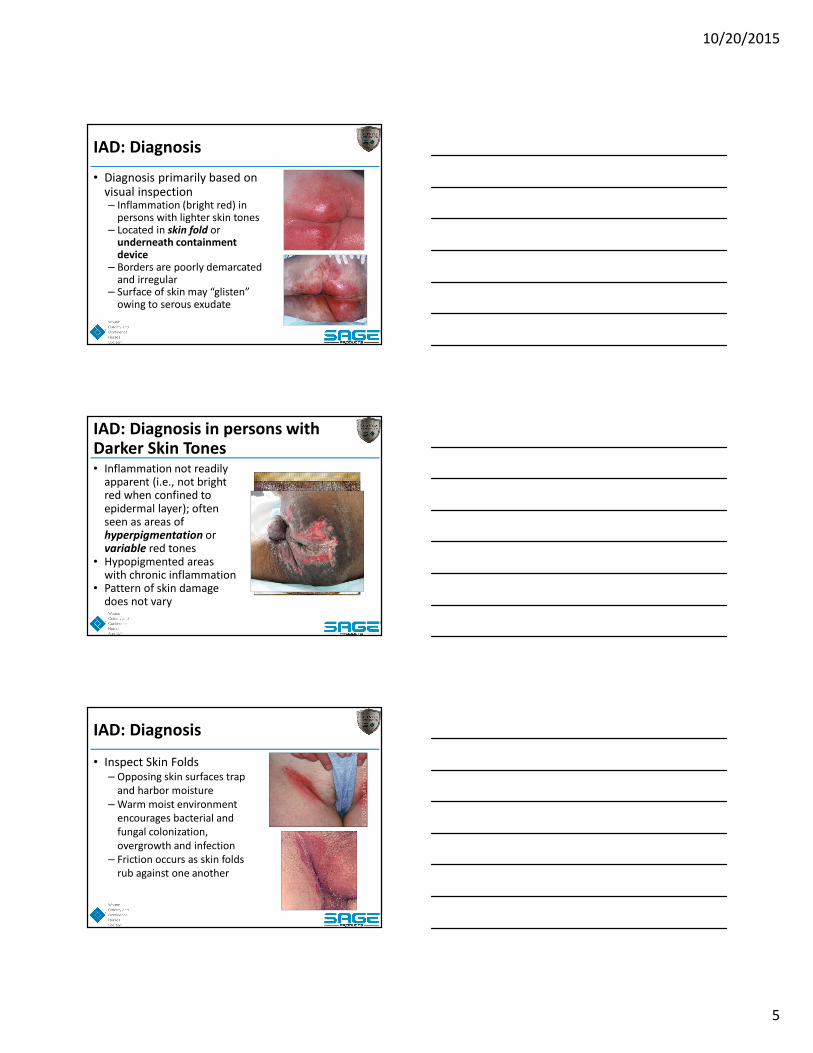
IAD: Diagnosis
• Diagnosis primarily based on visual inspection – Inflammation (bright red) in
persons with lighter skin tones – Located in skin fold or
underneath containment device
– Borders are poorly demarcated and irregular
– Surface of skin may “glisten” owing to serous exudate
IAD: Diagnosis in persons with Darker Skin Tones• Inflammation not readily
apparent (i.e., not bright red when confined to epidermal layer); often seen as areas of hyperpigmentation or variable red tones
• Hypopigmented areas with chronic inflammation
• Pattern of skin damage does not vary
IAD: Diagnosis
• Inspect Skin Folds – Opposing skin surfaces trap
and harbor moisture
– Warm moist environment
encourages bacterial and
fungal colonization,
overgrowth and infection
– Friction occurs as skin folds
rub against one another

10/20/2015
6
IAD: Diagnosis
• Assess for skin erosion– Partial thickness
erosion occurs with IAD
– Necrotic tissue: eschar
or slough, full thickness
damage indicates
pressure ulceration
IAD: Diagnosis
• Look for secondary cutaneous infection, especially candidiasis– Opportunistic infection
with candida albicans
– Thrives in warm, moist environment and damages stratum corneum
– Seen in 18% of one group of 976 acute care inpatients1
1. Junkin J, Selekof J. J Wound Ostomy Continence Nurs. 2007;34(3):260-9.
Black JM, et al. J Wound Ostomy Continence Nurs. 2011;38(4):359-70.
IAD: Diagnosis
• Suspect PU when
wound– Lies over bony
prominence
– Has distinctive borders
– Full thickness
– Necrotic tissue (black
eschar) is present
– Skin is dark to purplish
red

10/20/2015
7
IAD Diagnosis: History is Essential
• Emerging evidence
reminds us that
isolated photographs
do not reflect clinical
reality
• The biggest aid in this
case is a thorough
history
Differential Diagnosis: IAD vs. PU
Black JM, et al. J Wound Ostomy Continence Nurs. 2011;38(4):359-70.
Borchert K, et al. J Wound Ostomy Continence Nurs. 2010;37(5):527.
IAD and its Severity Instrument
• Designed and validated by WOC nurses and their faculty
• Two WOC nurses established initial face validity• Content and criterion validity via 9 WOC nurses in
North Central Region of the WOCN Society• Interrater reliability via 247 WOC nurses attending
2007 National Conference • Descriptive, ranks severity allowing longitudinal
assessment; responsiveness has not yet been tested

10/20/2015
8
IAD and its Severity Instrument
Borchert K, et al. J Wound Ostomy Continence Nurs. 2010;37(5):527.
IAD and its Severity Instrument
Borchert K, et al. J Wound Ostomy Continence Nurs. 2010;37(5):527.
Does Technology Play a Role?
• Three technologies have been proposed to
enhance diagnosis at the bedside
• All attempt to aid clinician to differentiate “bottom
up” damage from “top down” damage such as
exposure to urine/stool– High Resolution Ultrasonography
– Subepidermal moisture detection
– Thermal imaging

10/20/2015
9
1. Quintavalle PR, et al. Advances in Skin & Wound Care. 2006;19(9):498.
High Resolution Ultrasound
• Study using high resolution ultrasound showed
differences in appearance of normal volunteers
and NH residents with Braden scores ≤ 18
Sub-Epidermal Moisture Measurement• Employs small wand that measures
SEM when attached to the skin for several seconds
• Generates a number called DPU (dermal phase unit) ranges from 0-999; no standard unit attached
• Differentiated Stage I PU vs. erythema in 31 residents in 2 NH1
• ↑ SEM associated with 8.5-15 fold increase in Stage I and Stage II PU in 66 subjects with darker skin tone2
1. Bates-Jensen BM, et al. Wound Repair & Regeneration. 2008;16:189.
2. Bates-Jensen BM. J Wound Ostomy Continence Nurs. 2009;36(3):277-84.
1. Andersen ES, Karlsmark T. Skin Research & Technology. 2008;14(3):270-6.
Thermography
• Thermography evaluates local tissue circulation by visualizing temperature of targeted tissue1
• Sparse evidence suggests it does not characterize severity but may differentiate PU from MASD, and may be useful for prediction of SDIT progression
• Imaging system recently approved for use by United States FDA (early 2015); device weighs about 2 pounds; attached to laptop computer
10/20/2015
10
IAD Prevention and Management
• Identify/treat reversible causes of
incontinence
• Structured skin care regimen– Cleanse and protect
– Restore (moisturize) as indicated
– Contain as indicated
• Education and collaboration– Overlapping bundles:
– CAUTI (C), HAPU (P), and Falls (F)
Address Reversible Causes of Incontinence!
• Restricted mobility or dexterity (F, P, C)
• Psychological conditions/delirium (F, P, C)
• Stool impaction or constipation (F, P, C)
• Urinary retention (C, P)
• Pharmaceuticals (F, P, C)
• Infection (F, P, C)
Willson M, et al. Executive summary: a quick reference guide for managing FI. J
Wound Ostomy Continence Nurs. 2014;41(1): 61-9.
• Scheduled assistance with urinal, bedpan, or
commode
• As normal of a position as possible– Commode preferable to bedpan
– Toilet preferable to commode
– Male and female urinals
Restricted Mobility/Dexterity
10/20/2015
11
Diarrhea in Critical Care
• Incidence 14-15%1,2
• Linked to– increased LOS1
– significant mortality and morbidity1,2
• Several Types/causes– osmotic– secretory– exudative– motility disorders– infections
1. Marcon A, et al. Nosocomial diarrhea in the intensive care unit. Braz J Infect
Dis. 2006;10(6)6:384-389.
2. Thibault R, et al. Diarrhoea in the intensive care unit: respective contribution
of feeding and antibiotics. Crit Care. 2013;17(4):153.
Infection Induced Diarrhea
• C. difficile = most common HA diarrhea1,2
• 20-40% of hospitalized patients1
• 5-30% suffer relapse1
• Early identification/culture1,2
• Prevent transmission!1,2
1. Willson M, et al. Executive summary: a quick reference guide for managing FI.
J Wound Ostomy Continence Nurs. 2014;41(1):61-9
2. http://www.msnbc.msn.com/id/27633551/ns/health-health_care/t/nasty-
intestinal-bug-spikes-us-hospitals/
Antibiotics
Medication Induced Diarrhea
Willson M, et al. Executive summary: a quick reference guide for managing FI. J
Wound Ostomy Continence Nurs. 2014;41(1):61-9.
10/20/2015
12
• Incidence of constipation in ICU up to 70-83%1,2
• Linked to failure to wean, increased LOS, and
delayed enteral feeding1,2
• Evaluate history and symptoms� Continuous leaking of stool � Continuous urge to defecate� Restlessness and agitation � Hydration� Medications (opioids, diuretics, CA channel blocker,
CNS depressants)� Rectal exam
Stool Impaction/Constipation
1. Nassar AP, et al. Constipation in intensive care unit: incidence and risk
factors. J Crit Care. 2009 Dec;24(4):630
2. Mostafa SM, et al. Constipation and its implications in the critically ill patient.
Br J Anaesth. 2003;91(6):815–819.
ICU Bowel Management Protocols
• Ferris & East (2007) 13% � diarrhea, 8% � ICU
days1
• McPeake, et al. (2011) 20.7% �constipation,
15.2%� diarrhea2
• Knowles, et al. (2014) no change in practice
despite education sessions, printed facts sheets
and reminders3
1. Ferris S, East V. Managing diarrhoea in intensive care. Aust Crit Care.
2007;20(1):7-13.
2. McPeake J, et al. The implementation of a bowel management protocol in an
adult intensive care unit. Nurs Crit Care. 2011;16(5):235-42.
3. Knowles S, et al. Evaluation of the implementation of a bowel management
protocol in intensive care: effect on clinician practices and patient outcomes. J
Clin Nurs. 2014;23(5-6):716-30.
ICU Bowel Management Protocol
Pittman J, Beeson T, Carter B, Terry C. Implementation of a bowel management
program in critical care. J Wound Ostomy Continence Nurs. 2015;42(4):389-394.
• Effectiveness of education
• 6 critical care units and 230 nurses – web-based module
– unit based skills session/competency
– Self efficacy scores
• Significant (P<.001) improvement in knowledge
and self efficacy scores
• Enhanced collaboration with the WOC nurses/CNS
10/20/2015
13
Skin Care
• Cleanse
• Restore (if indicated)
• Treat infection (if indicated)
• Protect
• Contain (if indicated)
Safe and Gentle Cleansing (P, C)
• Specifically indicated for continence care
• Low dermatitis potential (hypoallergenic)
• pH alkaline similar to normal skin
• No-rinse skin cleanser; liquid or wipe
• Minimal friction, rubbing
• Soft, disposable non-woven cloth
• Dry skin if needed after cleansing
Beekman D, et al. Wounds International. 2015. www.woundsinternational.com
Doughty D, et al. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.
Avoid
• Bar Soap– Bacteria, pH
• Basins– Bacteria
• Fragrance– Sensitivities
• Regular Washcloths – Friction
• Antibacterials– Normal flora, pH, sensitivities
Beekman D, et al. Wounds International. 2015. www.woundsinternational.com
Doughty D, et al. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.

10/20/2015
14
Antibacterials and CAUTI
• CDC and CAUTI1
– Use routine hygiene while catheter in place– Routine antimicrobial prophylaxis NOT
recommended– Cleaning periurethral area with antiseptics NOT
recommended
• Dedicated meatal cleansing? – One option to prevent cross contamination– Choose products that are pH balanced and without
antiseptics
1. http://www.cdc.gov/hicpac/cauti/001_cauti.html
Moisturize/Restore as Needed
• Prevents TEWL and dryness
• Not indicated for overhydrated or maceration skin
• No need for another product IF cleanser or barrier
contains moisturizer ingredient– Emollients smooth and soften skin (e.g., oils and
synthetics)
– Humectants draw and hold water in the stratum
corneum (e.g., urea and glycerine)
– Lipids (e.g., ceramides)
Beekman D, et al. Wounds International. 2015. www.woundsinternational.com
Doughty D, et al. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.
Skin Protectants/Moisture Barriers
• Knowing about a protectant ingredient is useful (e.g., Petrolatum, Dimethicone, Zinc Oxide)
• Total formulation MORE important– Creams/ointments (oils/lipid + water)
– Pastes (ointment + absorbent powder adheres to wet,
weepy skin)
– Films (liquid + polymer dissolved in a solvent applied
with wand or spray)
Beekman D, et al. Wounds International. 2015. www.woundsinternational.com
Doughty D, et al. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.
10/20/2015
15
Protectant Ingredients
• Petrolatum– Occlusive, transparent, increases skin hydration, may impair fluid
uptake of absorbent pads/briefs, often found in combination with
Zinc or Dimethicone
• Dimethicone silicone (siloxane)– Non-occlusive, transparent
• Zinc oxide– Opaque/white, requires remove for skin inspection
• Acrylate terpolymer film– Liquid transparent film, dissolved in solvent for delivery then
dries, does not moisturize, fewer applications if compatible skin
cleanser used
Beekman D, et al. Wounds International. 2015. www.woundsinternational.com
Doughty D, et al. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.
Protectant Ingredients
• Hoggarth, et al. 2005
• Dimethecone hydrates > petrolatum
• Petrolatum macerates > dimethecone
• Zinc associated with more irritation than others
• Interpret with caution!– Applied under occlusive tape
– On healthy forearms
Hoggarth A, et al. A controlled, three-part trial to investigate the barrier function
and skin hydration properties of six skin protectants. Ostomy Wound Manage.
2005;51(12):30-42.
Ideal* Skin Protectant/Moisture Barrier
� Waterproof to protect repel moisture/irritants� Stays in place on the skin� Long lasting, durable� Breathable to prevent maceration� Easy to apply/remove or no removal required � Comfortable, no sting� Able to observe skin through the barrier
* If not ideal, how will you compensate?
Beekman D, et al. Wounds International. 2015. www.woundsinternational.com
Doughty D, et al. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.

10/20/2015
16
Treat Candidiasis When Present
• Do not treat prophylactically
• Clotrimizole/Miconizole common choices in
absence of lab test (broad spectrum and low cost)
• Available in powders, sprays, ointments, creams or
antifungals/moisture barriers combined
• If not combined; apply antifungal followed by
moisture barrier
• Occasional need for systemic antifungals
Nix D, Haugen V. Prevention and management of incontinence-associated
dermatitis. Drugs Aging. 2010;27(6):491-96.
IAD Skin Care
Intact no redness
Prevention with _________
(e.g., 3 and 1 product)
Moderate to severe nonintact
weepy, denuded _________
(e.g., Paste, Spray Film,
Containment device)
Candidiasis erythema satellite
lesions _________
(e.g., antifungal followed by
skin protectant)
Intact mild red OR anticipated
diarrhea- add additional
protection _________
(e.g., ointment)
Reassessment
• Expect improvement in 2-3 days
• If no improvement:– Ensure plan of care is in place
• If compliance is an issue, don’t ask what’s wrong with the
patient or staff before asking “what’s wrong with the plan?”
– Re-evaluate differential diagnosis
– Adjust plan of care
– Keep it simple, save time
Beekman D, et al. Wounds International. 2015. www.woundsinternational.com
Doughty D, et al. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.

10/20/2015
17
Save Time, Improve Compliance
• No rinse cleansers• Moisturizing cleanser and skin protectant
incorporated into a spray• Cleanser, moisturizers, and skin protectant
incorporated into a disposable cloth• Antifungal and skin protectant combined into an
ointment or cream• Products that require fewer applications• Containment devices (external pouches and FDA
approved indwelling devices)
Beekman D, et al. Wounds International. 2015. www.woundsinternational.com
Doughty D, et al. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.
External Pouches
• Pouches with attached adherent solid skin barrier
• Clamp or attach to drainage
• Skin under adhesive must be moisture and and an
and emollient free
• As needed – cut larger opening, dust denuded
weepy areas with ostomy powder and add ostomy
paste for better seal and/or add barrier film to
protect exposed skin, LET IT DRY)
Beitz JM. Fecal incontinence in acutely and critically ill patients: options in
management. Ostomy Wound Manage. 2006;52(12):56-8, 60, 62-6.
FDA Approved Indwelling Fecal Devices• Inserts into rectum
• Closed system diverts stool away from skin
• Saves time, skin, and spread of C-diff
• Use with moisture barrier in case of leakage
• Critical to know indications and
contraindications for safety
• Complications include mucosal injury, lower GI
bleeding, temporary anal sphincter atony
• Complication rate correlates with length of
time used
Beitz JM. Fecal incontinence in acutely and critically ill patients: options in
management. Ostomy Wound Manage. 2006;52(12):56-8, 60, 62-6.
10/20/2015
18
Absorptive Pads/Briefs: Complaints
• Traps moisture
• Increases perspiration
• Increases pH
• May impair pressure redistribution capacity of
some products
• Product clogged/less effective due to moisture
barrier ointments
• Look alike pads not intended for incontinence use
Langemo D, et al. Adv Skin Wound Care. 2011;24(3):126-40.
Gray M, et al. J Wound Ostomy Continence Nurs. 2012;39(1):61-74.
Zimmerer, et al. Pediatric Dermatol. 1986; 3:95-101.
Fader M, et al. Cochrane DataBase Syst Rev. 2008.
• High absorbent polymers “wick”
moisture off skin1
• Maintain acidity of skin pH2
• More sizes for better fit and less leakage2
• Breathable/air permeable materials1,2
• Microclimate Disposable Body Pad
Absorptive Pads/Briefs: Improving
1. Palese A, Carniel G. The effects of a multi-intervention incontinence care program on
clinical, economic, and environmental outcomes. J Wound Ostomy Continence Nurs.
2011;8(2):177-83.
2. Beguin AM, et al. Improving diaper design to address incontinence associated
dermatitis. BMC Geriatrics. 2010;10:86.
Special Populations
• Bariatric– Assist to lift panniculus/pannus for urinal
placement
– Commode with size and weight specifications
for safety
– Elbow length gloves
• Neonatal– Sensitivities
– Transcutaneous absorption
Gallagher S. Skin Care Needs of the Obese, Nix, et al. Skin Care Needs of the
Neonatal and Pediatric patient, Bryant R, Nix D. Coeditors: Acute and Chronic
Wounds: Current Management Concepts, 5th Edition. St. Louis, Mosby, 2015 In
Print.
10/20/2015
19
Education (F, P, C)
• Leaders, KOL, and IT for overlapping bundles– Infection control, Falls committee, CAUTI Champions
• Materials Management– Quality and accessibility of products
• Patients and Family
• Clinical Staff AND Administrators
• Build your case!
THANK YOU!
Related Documents











