ANESTHESIA FOR SURGERY OF THYMECTOMY TO TREAT MYASTHENIA GRAVIS AT CHORAY HOSPITAL FROM 2004 – 2012. PhD.MD. Dong Pham Van Dr. Thao Trang Nguyen Thi THE ANESTHETIC DEPARTEMENT

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ANESTHESIA FOR SURGERY OF THYMECTOMY TO TREAT MYASTHENIA GRAVIS
AT CHORAY HOSPITAL FROM 2004 – 2012.
PhD.MD. Dong Pham VanDr. Thao Trang Nguyen Thi
THE ANESTHETIC DEPARTEMENT

OVERVIEW

OVERVIEW
An autoimmune disease.An autoimmune disease. Ages, both sexes, female > male.Ages, both sexes, female > male. History of muscle weakness, move is History of muscle weakness, move is
fatigue, rest is gradually improved.fatigue, rest is gradually improved. 10 - 15% for thymomas, 75% for thymic 10 - 15% for thymomas, 75% for thymic
abnormalities.abnormalities. Thymectomy: one of efficacious therapies.Thymectomy: one of efficacious therapies.
OVERVIEW
General anesthesia with double-lumen endotracheal tube, with or without NMBDs.
Some drugs cause weak muscle. Vietnam hasn’t a lot of study topics like
this yet.
Purposes:
To investigate the correlation between 2 groups
patients with and without using NMBDs vs post-op
respiratory failure ratio and recoverable time after
anesthesia.

PHYSIOLOGY OF NEUROMUSCULAR TRANSMISSIONS

MOTOR UNIT

PHYSIOLOGY OF NEUROMUSCULAR TRANSMISSION
Stimulated neuron openning Calci channel Ach from synaptic vesicles in presynapse terminal go out.
Ach – AchR openning channel
Na, Ca flows enter depolarizing motor end plate.
Action potential across on cell membrane surface.
MECHANISM OF NMBDs
Depolarizing NMBDs: linking AChR Depolarize the end plate phase I block prolonged connection of succinylcholin Deforming AchR structure phase II block.
Non-depolarizing NMBDs: linking with 1 unit abnormalities of Ach-AChR no depolarize the end plate.

SITES OF NEUROMUSCULAR SITES OF NEUROMUSCULAR TRANSMISSIBLE DYSFUNCTIONTRANSMISSIBLE DYSFUNCTION

EFFECTS OF NMBDs IN NEUROMUSCULAR DYSFUNCTIONS
Decreasing the number of AChRs Decreasing the number of AChRs because of:because of:
• Changing the function of AChRs .Changing the function of AChRs .• Increasing the degradation of AChRs.Increasing the degradation of AChRs.• Destroying the surface of postsynapse.Destroying the surface of postsynapse.
Resistance with depolarizing NMBDs.Resistance with depolarizing NMBDs.
Sensitivity with non-depolarizing NMBDs.Sensitivity with non-depolarizing NMBDs.

SUBJECTS AND RESEARCH METHODS

SUBJECTS AND RESEARCH METHODS
Research design: retrospection, description with analysis.
Time, place: at Cho Ray hospital from 03/2004 to 06/2012.
Surgical methods:Thymectomy by endoscopic surgery.

SUBJECTS AND RESEARCH METHODS
Research methods:Research methods:Inclusion criteriaInclusion criteria: IIA, IIB (Osserman), 2 : IIA, IIB (Osserman), 2 groups, 1groups, 1stst group: use NMBDs; 2 group: use NMBDs; 2ndnd group: no use group: no use NMBDs.NMBDs.
Exclusion criteriaExclusion criteria: : patients with respiratory patients with respiratory failure, MG crisis, pre-op pyridostigmine failure, MG crisis, pre-op pyridostigmine bromide > 750 mg/d; I, III, IV grade; IIA, IIB with bromide > 750 mg/d; I, III, IV grade; IIA, IIB with cardiac, chronic pulmonary disease, sequela of cardiac, chronic pulmonary disease, sequela of stroke.stroke.
SUBJECTS AND RESEARCH METHODS
Research process:Research process:Preanesthetic examinationPreanesthetic examinationPreanesthetic drugs: Preanesthetic drugs: nonoInductionInduction: Propofol or sevoflurane, : Propofol or sevoflurane, SufentanilSufentanil, , or fentanyl (IV). Use or no use: or fentanyl (IV). Use or no use: suxamethoniume, atracurium, rocuronium. suxamethoniume, atracurium, rocuronium. Intubating double-lumen tube..Intubating double-lumen tube..MaintenanceMaintenance: : Sevoflurane, isoflurane, TIVA Sevoflurane, isoflurane, TIVA or TCI, sufentanil or fentanyl (IV). In end of or TCI, sufentanil or fentanyl (IV). In end of surgery, stop drugs & change endotracheal surgery, stop drugs & change endotracheal tube.tube.Post-op: Post-op: monitoringmonitoring vital signs, ABG, SPOvital signs, ABG, SPO22, , MG crisis…analgesia: tramadol, perfalgan, or MG crisis…analgesia: tramadol, perfalgan, or nisidol.nisidol.

SUBJECTS AND RESEARCH METHODS
Collected variables:Collected variables:
- Age, sex, MG degree, pulse, BP, SpO- Age, sex, MG degree, pulse, BP, SpO22..
- Surgical time, time of spontaneous - Surgical time, time of spontaneous ventilation via endotracheal tube, recovery ventilation via endotracheal tube, recovery room, in hospital. Ratio of respiratory failure, room, in hospital. Ratio of respiratory failure, post-op mechanism ventilation. post-op mechanism ventilation. - Perioperative drugs: fentanyl, sufentanil; - Perioperative drugs: fentanyl, sufentanil; propofol, isoflurane, sevoflurane; propofol, isoflurane, sevoflurane; suxamethonium, atracurium, rocuronium.suxamethonium, atracurium, rocuronium.- Post-op drugs: tramadol.- Post-op drugs: tramadol.

RESULTS & DISCUSSIONS
RESULTS & DISCUSSIONS
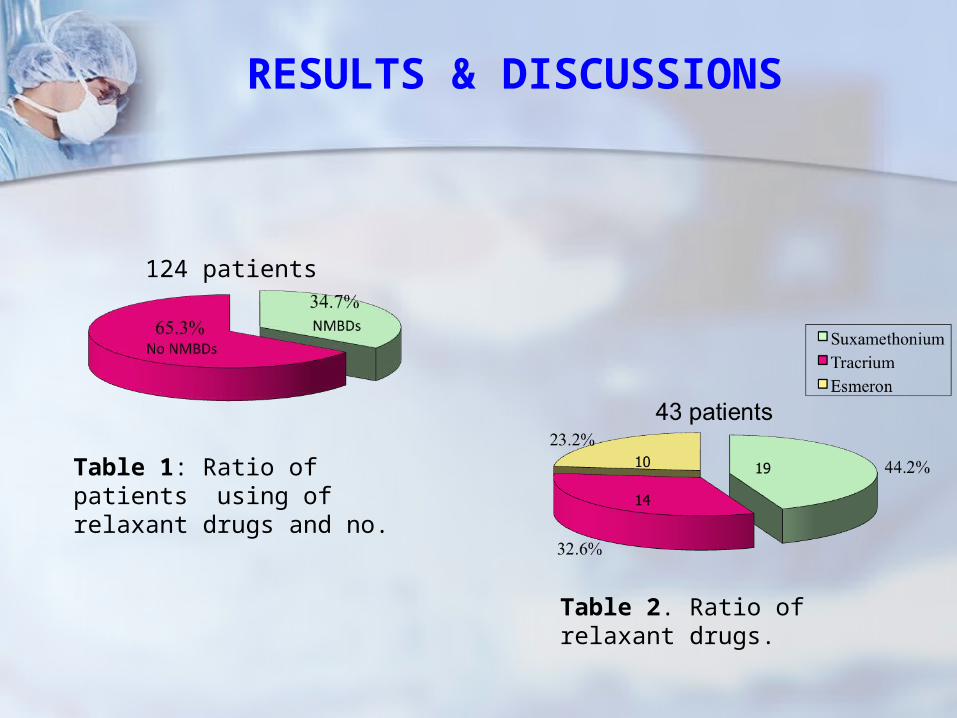
Table 1: Ratio of patients using of relaxant drugs and no.
124 patients
Table 2. Ratio of relaxant drugs.
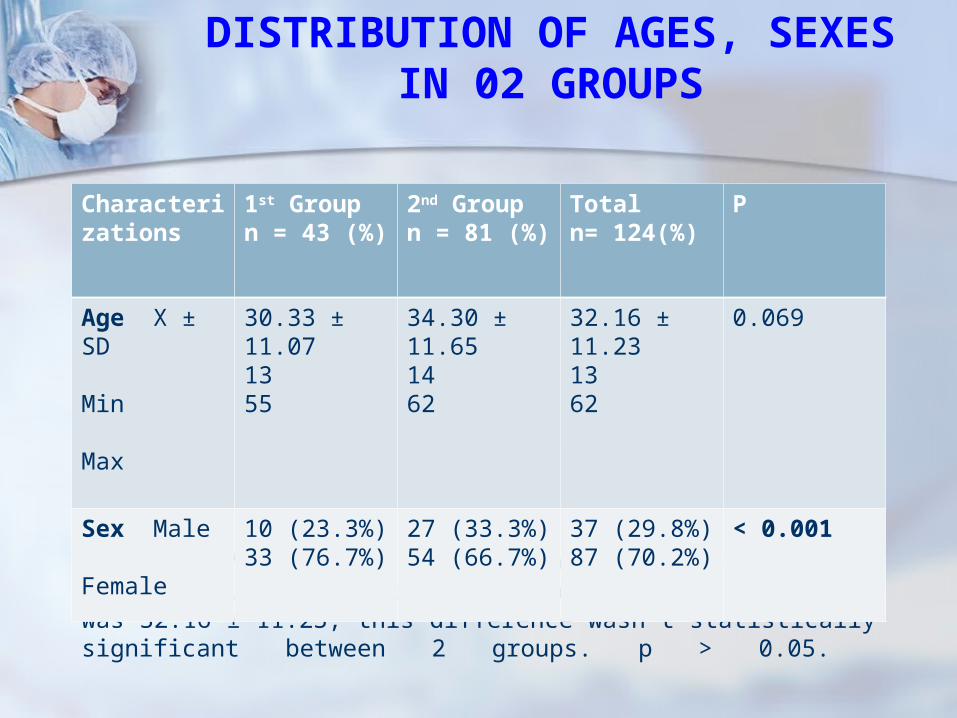
Comments: 70.2% female, 29,8% male, this difference was statistically significant, with p < 0.001. Average age was 32.16 ± 11.23, this difference wasn’t statistically significant between 2 groups. p > 0.05.
DISTRIBUTION OF AGES, SEXES IN 02 GROUPS
Characterizations
1st Groupn = 43 (%)
2nd Groupn = 81 (%)
Totaln= 124(%)
P
Age X ± SD Min Max
30.33 ± 11.071355
34.30 ± 11.651462
32.16 ± 11.231362
0.069
Sex Male Female
10 (23.3%)33 (76.7%)
27 (33.3%)54 (66.7%)
37 (29.8%)87 (70.2%)
< 0.001
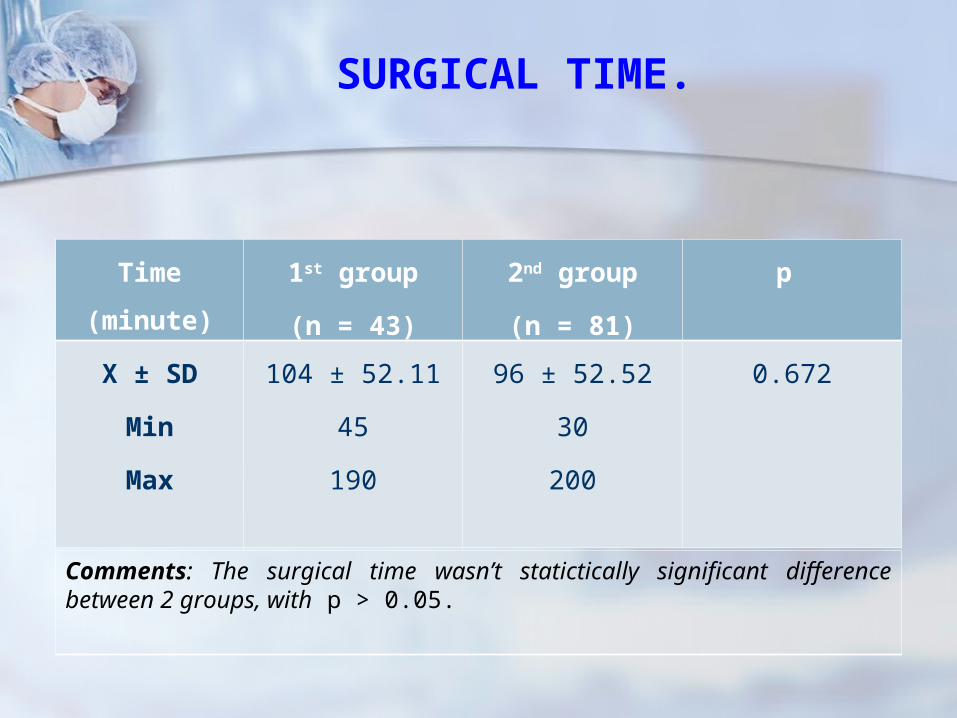
SURGICAL TIME.
Time (minute) 1st group
(n = 43)
2nd group
(n = 81)
p
X ± SD
Min
Max
104 ± 52.11
45
190
96 ± 52.52
30
200
0.672
Comments: The surgical time wasn’t statictically significant difference between 2 groups, with p > 0.05.

TIME OF SPONTANEOUS VENTILATION VIA ENDOTRACHEAL TUBE IN
RECOVERY ROOM
Comments: 1st group 21.61 ± 11.40 was longer 2nd group 5.69 ± 5.13, the difference was statictically significant, with p < 0.001.
1st Group 2nd Group
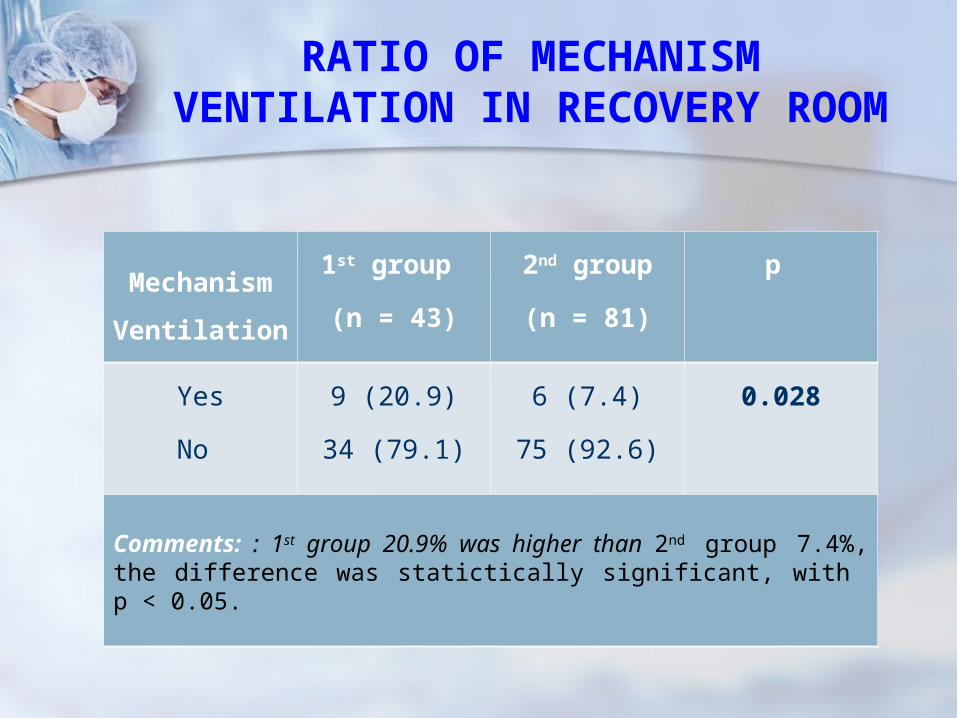
RATIO OF MECHANISM VENTILATION IN RECOVERY ROOM
Mechanism
Ventilation
1st group
(n = 43)
2nd group
(n = 81)
p
Yes
No
9 (20.9)
34 (79.1)
6 (7.4)
75 (92.6)
0.028
Comments: : 1st group 20.9% was higher than 2nd group 7.4%, the difference was statictically significant, with p < 0.05.

TIME OF POST-OP MECHANISM TIME OF POST-OP MECHANISM VENTILATION BETWEEN 02 VENTILATION BETWEEN 02
GROUPSGROUPS
Comments : 1st group 56.06 ± 57.98 was longer than 2nd group 3.50 ± 1.33, the difference was statictically significant, with p < 0.05.
56.06 ± 57.98
1st Group 2nd Group

POST-OP RESPIRATORY FAILURE RATIO BETWEEN 02 GROUPS.
Comments: : 1st group 60.5% was higher than 2nd group 7.4%, the difference was statictically significant, with p < 0.001.
1st Group 2nd Group Total

TIME IN RECOVERY ROOM OF 02 GROUPS.
Comments: : 1st group 30.94 ± 34.81 was longer than 2nd group 9.77 ± 9.38, the difference was statictically significant, with p < 0.001.
1st Group 2nd Group

CONCLUSIONCONCLUSION
MG patients have the same status, general anesthesia, surgical time, using the same anesthetic and analgesic drugs during and post-op the patients, who use NMBDs were the time of post-op spontaneous ventilation via endotrachea, of mechanism ventilation, of staying recovery room longer and ratio of post-op mechanism ventilation, respiratory faillure higher than the ones no use NMBDs.

Related Documents

![[123doc.vn] bg-giai-tich-iii-nguyen-xuan-thao-2014](https://static.cupdf.com/doc/110x72/55cc1040bb61ebe9598b46a2/123docvn-bg-giai-tich-iii-nguyen-xuan-thao-2014.jpg)