Grant and Research Support NATIONAL INSTITUTES OF HEALTH CYSTIC FIBROSIS FOUNDATION CHILDREN’S DISCOVERY INSTITUTE MARCH OF DIMES Speakers’ Bureau MEDPRO COMMUNICATIONS FRANCE FOUNDATION Other Financial or Material Support SCIENTIFIC CO-FOUNDER, COPERNICUS THERAPEUTICS US PATENTS Newborn screening for cystic fibrosis Thomas Ferkol, MD Professor of Pediatrics, Cell Biology and Physiology Washington University School of Medicine St. Louis Children’s Hospital

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Grant and Research SupportNATIONAL INSTITUTES OF HEALTH
CYSTIC FIBROSIS FOUNDATIONCHILDREN’S DISCOVERY INSTITUTE
MARCH OF DIMES
Speakers’ BureauMEDPRO COMMUNICATIONS
FRANCE FOUNDATION
Other Financial or Material SupportSCIENTIFIC CO-FOUNDER, COPERNICUS THERAPEUTICS
US PATENTS
Newborn screening for cystic fibrosis
Thomas Ferkol, MDProfessor of Pediatrics, Cell Biology and Physiology
Washington University School of MedicineSt. Louis Children’s Hospital

What is cystic fibrosis?How is the diagnosis of cystic fibrosis made?Does newborn screening impact on the course of disease?
Cystic fibrosis: objectives of the presentation

What is cystic fibrosis?Cystic fibrosis is a multisystem disease of exocrine gland function.How is the diagnosis of cystic fibrosis made?Does newborn screening impact on the course of disease?
Cystic fibrosis: objectives

Respiratory• recurrent sinopulmonary infections• bronchiolitis/asthma• nasal polyposis• Staphylococcus aureus pneumonia• Pseudomonas aeruginosa endobronchitis
Genitourinary• male infertility
Sweat Gland Dysfunction• hypochloremic, hyponatremic alkalosis
Cystic fibrosis: clinical presentations

Cystic fibrosis: clinical presentations
Gastrointestinal• meconium ileus• meconium plug syndrome• distal intestinal obstruction syndrome• rectal prolapse• neonatal hyperbilirubinemia• failure to thrive• hypoproteinemic edema• hypovitaminosis• recurrent pancreatitis• biliary cirrhosis and portal hypertension

Cystic fibrosis: median survival age, 1940-2006
05
101520
2530
1940 1950 1960 1970 1980 1990 2000
Med
ian
surv
ival
age
(yea
rs)
Year
3536.8
40

What is cystic fibrosis?An autosomal recessive disease, genetic mutations of the cystic fibrosis transmembrane conductance regulator result in abnormalities in chloride and sodium transport across an epithelium.
How is the diagnosis of cystic fibrosis made?Does early diagnosis impact on the course of disease?
Cystic fibrosis: objectives

Cystic fibrosis transmembrane conductance regulator: ion transport
ENaC
CFTR
Cl-a
K+
Na+ Na+ K+
2Cl-
K+
Na+ Na+ K+
2Cl-
Normal Cystic fibrosis
Cl-
Na+ Cl- Cl- Na+ Cl-
H2O

What is cystic fibrosis?How is the diagnosis of cystic fibrosis made?Does early diagnosis impact on the course of disease?
Cystic fibrosis: objectives

Cystic fibrosis: diagnosisRequires:Phenotypic clinical features
• chronic sinopulmonary disease (> 99 %), or• gastrointestinal abnormalities, like pancreatic insufficiency (85 %), recurrent
pancreatitis, meconium ileus, or focal biliary or multilobar cirrhosis• obstructive azospermia in males• history of cystic fibrosis in the immediate family• Positive newborn screen
Laboratory evidence of CFTR dysfunction• elevated sweat chloride measurements (>60 mmol/l)

Cystic fibrosis: pilocarpine iontophoresisDi Sant’Agnese PA, et al. Pediatrics. 12:549;1953.
0 20 40 60 80 100 120 140 160
5
10
15
0
[Cl-] (meq/l)
Num
ber o
f pat
ient
s

Cystic fibrosis: diagnosisRequires:Phenotypic clinical features
• chronic sinopulmonary disease (> 99 %), or• gastrointestinal abnormalities, like pancreatic insufficiency (85 %), recurrent
pancreatitis, meconium ileus, or focal biliary or multilobar cirrhosis• obstructive azospermia in males• history of cystic fibrosis in the immediate family• Positive newborn screen
Laboratory evidence of CFTR dysfunction• elevated sweat chloride measurements (>60 mmol/l)• mutation in CFTR gene on both alleles


Cystic fibrosis: molecular mechanisms of CFTR dysfunction
ATP
ADP
Golgi
ER
Endosome
ATP ADP
PKAATP
ADP
Nucleus
Class 4: mutants that have altered channel properties, e.g., R117H
Class 1: premature termination of CFTR
mRNA translation, e.g., S489X
Class 3: regulatory mutants that fail to
respond normally to activation signals,
e.g., G551D Class 2: CFTR protein degradation in the endoplasmic reticulum, e.g., ΔF508
Class 5: decreased functional CFTR synthesis or transport, e.g., A455E

Cystic fibrosis: molecular mechanisms of CFTR dysfunction
ATP
ADP
Golgi
ER
Endosome
ATP ADP
PKAATP
ADP
Nucleus
Class 4: mutants that have altered channel properties, e.g., R117H
Class 1: premature termination of CFTR
mRNA translation, e.g., S489X
Class 3: regulatory mutants that fail to
respond normally to activation signals,
e.g., G551D Class 2: CFTR protein degradation in the endoplasmic reticulum, e.g., ΔF508
Class 5: decreased functional CFTR synthesis or transport, e.g., A455E
Proteasome

Cystic fibrosis: molecular mechanisms of CFTR dysfunction
ATP
ADP
Golgi
ER
Endosome
ATP ADP
PKAATP
ADP
Nucleus
Class 4: mutants that have altered channel properties, e.g., R117H
Class 1: premature termination of CFTR
mRNA translation, e.g., S489X
Class 3: regulatory mutants that fail to
respond normally to activation signals,
e.g., G551D Class 2: CFTR protein degradation in the endoplasmic reticulum, e.g., ΔF508
Class 5: decreased functional CFTR synthesis or transport, e.g., A455E

unaffected
Cystic fibrosis: CFTR activity and tissue manifestations
100% (wt, 9T/9T)
50% (wt, 9T, and mutant CFTR)
10% (wt protein, 5T/5T)
5% (wt protein, 5T, and severe mutant)
4% (R117H, 7T, and severe mutant)
1% (R117H, 7T, and severe mutant)
<1% (G551D, ΔF508)
vas deferens
sweat ductairway
pancreas
Tissue affected CFTR activity
Chillon M, et al. New Eng J Med. 332:1475;1995.

The relationship between ΔF508 genotype and pulmonary diseaseKarem E, et al. New Eng J Med. 326:151;1990.
5 45
25
50
75
100
25Age (y)
15 35
125
FEV
1 (%
pre
dict
ed)

Cystic fibrosis: conclusions
• The diagnosis of cystic fibrosis is largely based on clinical presentation, but the clinical spectrum of cystic fibrosis is widening.
• Mutations of the CFTR gene can be associated different clinical phenotypes.• The sweat chloride measurement is still the best diagnostic test for cystic
fibrosis, but genetic analysis of CFTR alleles can be useful in the diagnosis of atypical or mild cases.

What is cystic fibrosis?How is the diagnosis of cystic fibrosis made?Does newborn screening impact on the course of disease?
Cystic fibrosis: objectives

Cystic fibrosis: epidemiology
Population
Caucasian (US)Caucasian (Great Britain)
Hispanic
African American
Native American
Asian (US, England)
Israel
Southern Europe
Epidemiologic
1 in 1,900-3,700
1 in 2,400-3,000
1 in 8,000-9,000
1 in 15,3001 in 40,000
1 in 10,000
1 in 5,000
1 in 2,000-4,000
Newborn screening
1 in 3,400-3,800
1 in 2,200-3,200
--
----
--
--
--

0
20
40
60
80
Age at diagnosis of cystic fibrosis patients
Age
100
Cum
ulative percent
0
1000
2000
3000
4000
5000
Num
ber o
f CF
patie
nts
1-3
m4-
6 m
7-12
m 1 2 3 4 5 6 7 8 9 10 11 12 13 14 1516
-20
21 -
30
31 -
40>
40
Fifty percent of patients are diagnosed by six months of age, and 68 percent by age one(2003 CFF Patient Registry)
birth

Onset of cystic fibrosis disease
• Variable age, depending on genotype and clinical phenotype.
• At birth in 10-15% with meconium ileus (but may have negative screen.
• Malnutrition is often early (by 2 months) Sokol RJ, et al, Am J Clin Nutr. 50:1064;1989.Bronstein MN, et al, J Pediatr. 120; 533;1992.
• Lung disease can also begin early (1-3 months)Abman SH, et al, J Pediatr. 119: 211;1991.Farrell PM et al, Pediatr Pulmonol. 36: 230-240;2003.

Cystic fibrosis: effect of neonatal screening on growth Farrell PM, et al. J Pediatr. 147:S30:2005.
2 4 6-1.5
-1.0
-0.5
0
+0.5
Age (years)
8 10
Wei
ght f
or a
ge z
-sco
re
12 14
Screened (n = 49)
CFF
Control (n = 32)

Pulmonary function in cystic fibrosis patients by diagnostic categoryAccurso FJ, et al. J Pediatr. 147:S37;2005.
60
70
80
90
6-10 (y)
100FE
V1
(% p
redi
cted
)
NS C MI
11-18 (y)
NS C MI


Cystic fibrosis newborn screening in the United States (2004)
Offered, but not required
Universally offered

Cystic fibrosis newborn screening in the United States (2007)
Planning stages
Offered, but not required
Universally offered

Missouri birth rates and expected numbers of cystic fibrosis patients
Race/ethnicity
Caucasian
African-American
Hispanic
Asian-American
Native American
Missouri birth rate
62,375
11,028
3267
1496
353
Anticipated CF newborns
19-32
0.7
0.4
0.1
0.0
CF frequency
1 in 1,900-3,700
1 in 15,300
1 in 8,000
1 in 10,000
1 in 40,000

no Report as negative screen
yes
IRT > 70 ng/dl percentile*
Sweat testReport as positive screen300 newborns
no Report as negative screen
yes
Perform IRT at 24-48 hours of life
IRT > 100 ng/dl percentile
Repeat IRT at 2-4 weeks of life
75,000 live births
3,000 newborns
Newborn screening for cystic fibrosis (IRT/IRT)
Requires second specimenRecalls more African-American low APGAR babies
Rock MJ, et al. Pediatr Pulmonol. 6:42;1989.

Cystic fibrosis: frequency of common CFTR mutations worldwide
Mutation
ΔF508
G542X
G551D
W1282X
N1303K
R553X
3849 + 10 kB C-to-T
621 +1 G-to-T
1717 +1 G-to-A
1078 del T
% of mutant CFTR alleles
66.0
2.4
1.8
1.5
1.2
0.9
0.6
0.6
0.5
0.5

Cystic fibrosis: ΔF508 frequency in different ethnic groups
Population
Caucasian (worldwide)Caucasian (northern Europe)Caucasian (southern Europe)
Hispanic (US)
Jews (Ashkenazi)
African American
Native American
% of mutant CFTR alleles
66
70-80
50-55
4630
48
<5

Sweat test
Sweat test
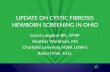
noReport as negative screen
yes
Perform IRT at 24-48 hours of life
2 Report as positive CF
IRT > 96th percentile*
CFTR mutations
Perform CFTR mutation analysis
Report as possible CF
0 1
Report as less likely CF~2900 newborns
100 newborns
18 newborns
Newborn screening for cystic fibrosis (IRT/DNA)
75,000 live births
3,000 newborns
One sampleMore specificUltrahigh IRT levels trigger sweat chloride measurement in some states

Newborn screening for cystic fibrosis: year one results
Missouri (IRT-IRT)Initial newborn screening specimens: 81,100 Total requested repeat screens: 421Total referred to CF Centers: 107Total confirmed CF: 23 (12 from central and southwest Missouri)False Positives: 84False Negatives: 0
Illinois (IRT-DNA)Initial newborn screening specimens: 79,506Positive screens: 320 Total confirmed CF: 22 (11 patients from central and southern Illinois)False Positives: 84False Negatives: 0

Requirements for successful cystic fibrosis newborn screening
• Organize a collaborative program involving cystic fibrosis centers and the state screening lab.
• Establish follow-up mechanisms and communication between center, referring physicians, and the state screening lab.
• High quality sweat testing.
• Multidisciplinary, center-based care.
• Optimize nutritional management using proven methods for both evaluation and treatment.
• Improve respiratory management aimed at early treatment and prevention of chronic infections (especially Pseudomonas aeruginosa acquisition).
Farrell MH and Farrell PM. J Pediatr. 143:707;2003.

Benefits of early diagnosis through cystic fibrosis neonatal screening
• Prevent malnutrition and stunted growth
• Prevent micronutrient deficiencies (fat-soluble vitamins)
• Delay progression of lung disease
• Reduce risk for cognitive dysfunction due to malnutrition
• Enhance quality of care and quality of life
• Reduce costs for diagnosis and possibly treatment
• Improve access and avoid geographic and fiscal barriers
• Avoid disparities related to gender, race and ethnicity
• Provide genetic counseling for parents
Related Documents