PARENTERAL NUTRITION IN NEWBORNS Dr. Elsie Constanza Paediatrician/Neonatologist Karl Heusner Memorial Hospital NEONATAL UNIT

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PARENTERAL NUTRITION IN NEWBORNS
Dr. Elsie Constanza
Paediatrician/Neonatologist
Karl Heusner Memorial Hospital
NEONATAL UNIT

Total body water (TBW): the total intracellular andextracellular fluids
Extracellular fluids (ECF): the total Intravascular andInterstitial fluids
Insensible water loss (IWL): the evaporation of waterthrough the skin, respiratory tract and mucousmembranes
Definitions
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014

General Principles
Water accounts for 75%-95% of an infant’s body weight
TBW is inversely proportional to GE.
First week of life: physiologic weight loss due to contraction of ECF.
VLBW infants – 10%-15%Term infants – 10%
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014
ELBW infants at lower GE have the highest Trans-epidermal water loss (TEWL)
*Humidified incubator with Porthole sleeves ready on admission for infants < 32weeks and/or <1,200
grams to decrease TEWL
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014

FACTORS AFFECTING IWL
INCREASE DECREASE
Low maturity High maturity
Low relative humidity Increasing postnatal age
Ambient temperature exceeding neutral thermal environment
High environmental relative humidity
Skin defects (omphalocele, gastroschisis)
High ventilator relative humidity
Phototherapy and use of radientwarmer
Oh W, Fluid and Electrolyte Management of VLBW Infants, Pediatrics and Neonatology 2012
IWL:
Intake – Output (mainly urine) - ∆ in weight
Oh W, Fluid and Electrolyte Management of VLBW Infants, Pediatrics and Neonatology 2012

Urine output: 1-3ml/kg/hr
Urine specific gravity: 1005-1012 is consistent with a balancein TBW
Urine Osmolarity : (specific gravity – 1000) x 30•Premature: 500mosm/l (spec. gravity 1020-1025)•AT: 800 mosm/l (specific gravity 1030)
Serum electrolytes and Cr should be routinely monitored toevaluate Renal Function and Fluid balance.
*Na+ / Cr / BUN
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014

Maintenance Fluid Requirements During the first week of Life
Birth Weight(g)
IWL(ml/kg/d)
Dextrose(g/100ml)
Day 1-2(ml/kg/day)
Day 3-7(ml/kg/Day)
<750 100+ 5-10 100-200 120-200
750-1,000 60-70 10 80-150 100-150
1,001-1,500 30-65 10 60-100 80-150
>1,500 15-30 10 60-80 100-150
Fanaroff and Martin’s Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant. 10th Ed. Elsevier, 2015

ESTIMATED ENERGY REQUIRMENTS FOR GROWING PREMATURE INFANTS
Energy Expenditure Kcal/kg/d
Resting metabolic rate 40-60
Activity 0-5
Thermoregulation 0-5
Synthesis/energy cost of growth 15
Energy stored 20-30
Energy excreted 15
Total energy requirement (estimated)
90-120
Fanaroff and Martin’s Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant. 10th Ed. Elsevier, 2015

RECOMMENDED ENERGY INTAKE
American Academy of Pediatrics:
105-130 kcal/kg/day for preterm infants
ESPGHAN (Committee on Nutrition):
110-135 kcal/kg/day
Fanaroff and Martin’s Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant. 10th Ed. Elsevier, 2015

FORMS OF ADMINISTRATION
PERIPHERAL: max osmolarity 900 mOsm/l Limits increase of energy , Dext 12.5%. Short term nutrition Risk of infiltration, phlebitis, thrombosis
CENTRAL : osmolarity >1000mOsm/l Prolonged Nutrition Dext > 12.5%
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005

COMPONENTS
Macronutrients
Amino acids
Carbohydrates
Lipids
Micronutrients:
Electrolytes: Mg, K, Na
Minerals
Vitamins
Calcium Gluconate
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005

PREPARATION
Laminar flow hood

OSMOLARITY DEPENDS MOSTLY ON:
• DEXTROSE 5mOsml/gr• AMINO ACIDS 10mOsml/gr• ELECTROLYTES 1mOsml/mEq
mOsm/L:Total of Osmol x 1000total volume in TPN
PLASMA OSMOLARITY: 280 -290 mosm/L
2x Na + Glucose mg/dl + BUN mg/dl18 2,8
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005

DEXTROSE
Normal Glucose Requirements
Glucose Infusion Rate (GIR):
• Preterm: 6-8mg/kg/min• Term: 3-5mg/kg/min
Normal glucose level: 50-120 mg/dl
1 gram of glucose = 3,4 kcal
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014
Infants who require high infusion ratesor a dextrose concentration (Tenor)
> 12.5% require placement of central venous catheter (UVC, PICC)
Tenor: Total Glucose (g) x100Total fluids in IV
Total grams of glucose= GIR (mg) x Weight (kg) x 1.44
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014
Dextrose solutions and formulas:
D5W D30WD10W D50W
D10W: Glucose (g) - RV0,05
D5W: Remaining volume (RV) – D10W
D30W: Glucose (g) – RV0,2 2
D50W: Glucose (g) x 10 – RV4

AMINO ACIDS
Recommended Protein intake:
3 – 4 g/kg/day in VLBW infants
1g of aa = 4 kcal
This account for obligate protein loss of(1.5 – 2.0 g/kg/day)
This will: limits catabolism improve protein balance preserve endogenous protein stores
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014

Parenteral Amino Acid Solutions
Aminosyn 10%
TrophAmine 10%
Primene 10%
* Presentation also available as 8,5%
Fanaroff and Martin’s Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant. 10th Ed. Elsevier, 2015
LIPIDS
Intravenous lipids: Prevents essential fatty acids deficiency (EFAD)
(linoleic/linolenic acids) Provides a significant source of non-protein energy. Requirments 1-4 g/kg/day
1g of lipid = 9 kcal
EFAD can be avoided with 0.5 – 1.0 g/kg/dayof IV lipids in the first 24 hrs of life.
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014

Intralipids are available as 10% and 20%
20% solutions are preferred due to lower cholesterol and plasma triglyceride levels.
IV lipid solutions have LCT (>12C)
Maintain serum glucose levels
Monitor Triglycerides: <200 mg/dl and < 140mg/dl with hyperbilirubinemia
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014

Care should be taken in:
Infants with unconjugated hyperbilirubinemia to avoid bilirubin toxicity as a result of free fatty acids displacing bilirubin from albumin binding sites.
Infants with BPD due to release of thromboxanesand prostaglandins, and increased pulmonary vascular resistance
Infants with increased sepsis risk
Lipid intake should be limited to 40% - 50% of total calories
R. Bissinger. D. Annibale, GOLDEN HOURS, Care of the VLBWI , Chicago Ill, 2014
ELECTROLYTES: SODIO (NA+):
Initiate:48 hrs
Requirements:
PT: 2 to 5mEq/kg/day
AT: 2 a 4mEq/kg/day.
CLORURO DE SODIO 20%®
Descripción:
Formula
Every 100 ml contains:
Sodium Chloride USP 20,00 g
Inyectable Water c.s.
Each ml has:
3,4 mEq Sodium ion (Na+)
3,4 mEq Cloride ion (Cl-)
Osmolarity: 6.844 mOsm/l
1mOsm/l = 1mEq
(3.4x1000) x 2= 6.800 mOsm/l
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005

Can be adm. As KCLsalt or KH2PO4 salt.
Initiate: 48 hrs
Requirements:
RNPT y RNT:
1-4mEq/kg/day.
CLORURO DE POTASIO
7,5%®
Descripción:
Formula:
Every 100 ml contains:
KCL USP 7,45 g.
Inyectable water c.s.
Every ml has:
1 mEq (K+);
1 mEq (Cl-);
Osmolarity: 2.000 mOsm/l
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005
ELECTROLYTES: Potassium (K+):

K2PO4 13,6%
1meq/ml
Initiate with aa.
Dosis:20-40mg/kg/day.
FOSFATO MONOBÁSICO DE
POTASIO
13,6%®
Formula:
Every 100 ml contains:
Monobasic K2PO4
USP 13,61 g.
Inyectable water c.s.
Every ml has:
1 mEq (K+)
1 mEq (H2PO4-)
Osmolarity: 2.000 mOsm/l
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005
ELECTROLYTES: PHOSPHUROS
Mostly found in bone tissue
Initiate at birth
Dosis: 1.5 – 4 mEq/kg/day.
Adjustment to increase dose: Asphyxia NB of Diabetic mother PT and SGE
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005
Minerals: Calcium (Ca2+)

GLUCONATO DE CALCIO 10%®
Descripción:
Formula:
Every 100 ml contains:
Calcium Gluconate USP 10,00 g
Inyectable water c.s.
Each ml has:
0,5 mEq (Ca++)
0,5 mEq (Cl2H2O14)
Osmolarity: 1000 mOsm/l
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005

INCOMPATIBILITY Ca-P
RELATION CALCIUM/PHOSPHORUS =Ca mEq/L X (P MMOL X 1.8)
Ca/P Relationship < 300 to be considered safe
Contemporary Nutritional Support Practice: a clinical guide. Saunder 2003
Dosis: 0.25 - 0.5 mEq/kg/day
Serum Mg levels before adm.
Magnesium Sulphate 50% (4meq/ml)
Osmolarity 4057 mOsm/l
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005
Minerals: Magnesium (Mg)

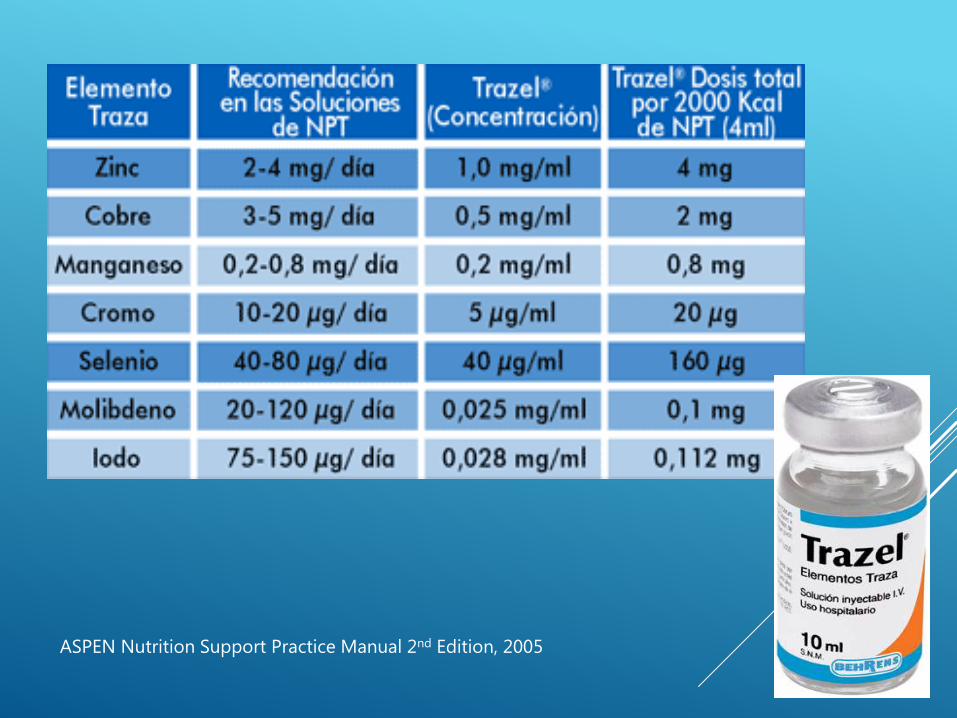
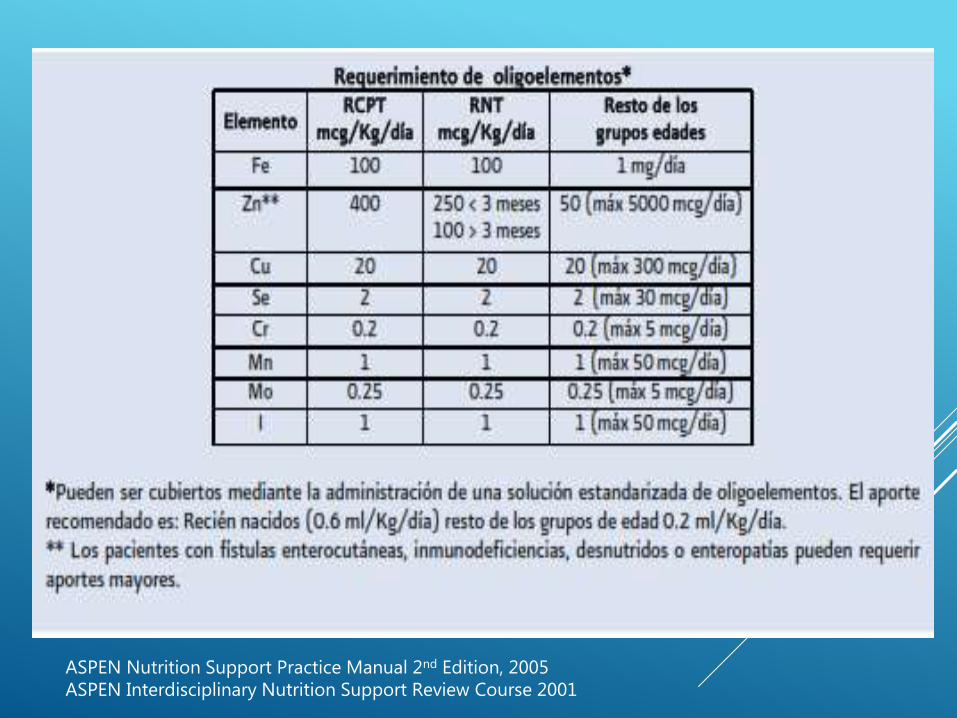
TRACE MINERALS
AT and PT: 0.4 – 0.6 ml/kg/day.
Discontinue:
Copper and manganese in hepaticcholestasis.
Selenium, chromium y molybdenum inAcute Renal Disease.
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005 ASPEN Interdisciplinary Nutrition Support Review Course 2001
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005 ASPEN Interdisciplinary Nutrition Support Review Course 2001

VITAMINS

ASPEN Nutrition Support Practice Manual 2nd Edition, 2005 ASPEN Interdisciplinary Nutrition Support Review Course 2001

WHEN TO DISCONTINUE PN?
Discontinue Parenteral Nutrition when patient has aEnteral Nutrition of 100cc/kg/d
Gradual omission if patient has 75% of total fluids asEnteral Nutrition and compliment with glucose at anadequate GIR.
ASPEN Nutrition Support Practice Manual 2nd Edition, 2005
TO TAKE HOME:
1. Parenteral Nutrition should start as soon as possible2. GIR of 5-6 mg/kg/day; 1g of glucose = 3,4 kcal3. Amino Acids: 2-4g/kg/day; 1g of aa = 4 kcal4. Lipids: 2-4 g/kg/day; 1g of lipid = 9 kcal5. Recommended energy intake: 110 – 135 kcal/kg/day
Take in consideration IWL TBW is inversely proportional to GE Monitor electrolytes and renal function

Related Documents











