Newborn care practices in rural Bangladesh: Implications for the adaptation of kangaroo mother care for community-based interventions Erin C. Hunter a , Jennifer A. Callaghan-Koru b, * , Abdullah Al Mahmud c , Rashed Shah a, 1 , Azadeh Farzin d, e , Elizabeth A. Cristofalo f , Sadika Akhter g , Abdullah H. Baqui d a Department of International Health, Johns Hopkins Bloomberg School of Public Health, 615 N. Wolfe Street, Baltimore, MD 21205, USA b Department of International Health, Johns Hopkins Bloomberg School of Public Health, 615 N. Wolfe Street, Suite E8608, Baltimore, MD 21205, USA c Centre for Child and Adolescent Health, International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), GPO Box 128, Dhaka 1000, Bangladesh d International Center for Maternal and Newborn Health, Department of International Health, Johns Hopkins Bloomberg School of Public Health, 615 N. Wolfe Street, Baltimore, MD 21205, USA e Division of Neonatology, Department of Pediatrics, Johns Hopkins University School of Medicine,1800 Orleans Street, Suite 8513-8S, Baltimore, MD 21287, USA f Department of Pediatrics, Johns Hopkins University School of Medicine,1800 Orleans Street, Suite 8513B-8S, Baltimore, MD 21287, USA g Centre for Reproductive Health, International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), GPO Box 128, Dhaka 1000, Bangladesh article info Article history: Received 22 April 2014 Received in revised form 30 September 2014 Accepted 1 October 2014 Available online 2 October 2014 Keywords: Bangladesh Kangaroo mother care Neonatal hypothermia Newborn care practices Neonatal mortality Formative research Low birth weight abstract Bangladesh has one of the world's highest rates of low birth weight along with prevalent traditional care practices that leave newborns highly vulnerable to hypothermia, infection, and early death. We conducted formative research to explore existing newborn care practices in rural Bangladesh with an emphasis on thermal protection, and to identify potential facilitators, barriers, and recommendations for the community level delivery of kangaroo mother care (CKMC). Forty in-depth interviews and 14 focus group discussions were conducted between September and December 2012. Participants included pregnant women and mothers, husbands, maternal and paternal grandmothers, traditional birth attendants, village doctors, traditional healers, pharmacy men, religious leaders, community leaders, and formal healthcare providers. Audio recordings were transcribed and translated into English, and the textual data were analyzed using the Framework Approach. We find that harmful newborn care practices, such as delayed wrapping and early initiation of bathing, are changing as more biomedical advice from formal healthcare providers is reaching the community through word-of-mouth and television campaigns. While the goal of CKMC was relatively easily understood and accepted by many of the participants, logistical and to a lesser extent ideological barriers exist that may keep the practice from being adopted easily. Women feel a sense of inevitable re- sponsibility for household duties despite the desire to provide the best care for their new babies. Our findings showed that participants appreciated CKMC as an appropriate treatment method for ill babies, but were less accepting of it as a protective method of caring for seemingly healthy newborns during the first few days of life. Participants highlighted the necessity of receiving help from family members and wit- nessing other women performing CKMC with positive outcomes if they are to adopt the behavior them- selves. Focusing intervention messages on building a supportive environment for CKMC practice will be critical for the intervention's success. © 2014 Published by Elsevier Ltd. * Corresponding author. E-mail addresses: [email protected] (E.C. Hunter), [email protected], [email protected] (J.A. Callaghan-Koru), [email protected] (A. Al Mahmud), mshah34@jhu. edu, [email protected] (R. Shah), [email protected] (A. Farzin), [email protected] (E.A. Cristofalo), [email protected] (S. Akhter), [email protected] (A.H. Baqui). 1 Primary affiliation address has changed since the time of the study. Current primary affiliation is: Department of Health and Nutrition, Save the Children e USA, Washington DC Office, 2000 L street NW, DC 20036, USA. Contents lists available at ScienceDirect Social Science & Medicine journal homepage: www.elsevier.com/locate/socscimed http://dx.doi.org/10.1016/j.socscimed.2014.10.006 0277-9536/© 2014 Published by Elsevier Ltd. Social Science & Medicine 122 (2014) 21e30

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

lable at ScienceDirect
Social Science & Medicine 122 (2014) 21e30
Contents lists avai
Social Science & Medicine
journal homepage: www.elsevier .com/locate/socscimed
Newborn care practices in rural Bangladesh: Implications for theadaptation of kangaroo mother care for community-basedinterventions
Erin C. Hunter a, Jennifer A. Callaghan-Koru b, *, Abdullah Al Mahmud c, Rashed Shah a, 1,Azadeh Farzin d, e, Elizabeth A. Cristofalo f, Sadika Akhter g, Abdullah H. Baqui d
a Department of International Health, Johns Hopkins Bloomberg School of Public Health, 615 N. Wolfe Street, Baltimore, MD 21205, USAb Department of International Health, Johns Hopkins Bloomberg School of Public Health, 615 N. Wolfe Street, Suite E8608, Baltimore, MD 21205, USAc Centre for Child and Adolescent Health, International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), GPO Box 128, Dhaka 1000,Bangladeshd International Center for Maternal and Newborn Health, Department of International Health, Johns Hopkins Bloomberg School of Public Health, 615 N.Wolfe Street, Baltimore, MD 21205, USAe Division of Neonatology, Department of Pediatrics, Johns Hopkins University School of Medicine, 1800 Orleans Street, Suite 8513-8S, Baltimore,MD 21287, USAf Department of Pediatrics, Johns Hopkins University School of Medicine, 1800 Orleans Street, Suite 8513B-8S, Baltimore, MD 21287, USAg Centre for Reproductive Health, International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), GPO Box 128, Dhaka 1000, Bangladesh
a r t i c l e i n f o
Article history:Received 22 April 2014Received in revised form30 September 2014Accepted 1 October 2014Available online 2 October 2014
Keywords:BangladeshKangaroo mother careNeonatal hypothermiaNewborn care practicesNeonatal mortalityFormative researchLow birth weight
* Corresponding author.E-mail addresses: [email protected] (E.C. Hunter)
edu, [email protected] (R. Shah), afarzin1@jhu1 Primary affiliation address has changed since th
Washington DC Office, 2000 L street NW, DC 20036,
http://dx.doi.org/10.1016/j.socscimed.2014.10.0060277-9536/© 2014 Published by Elsevier Ltd.
a b s t r a c t
Bangladesh has one of the world's highest rates of low birth weight along with prevalent traditional carepractices that leave newborns highly vulnerable to hypothermia, infection, and early death. We conductedformative research to explore existing newborn care practices in rural Bangladesh with an emphasis onthermal protection, and to identify potential facilitators, barriers, and recommendations for the communitylevel delivery of kangaroo mother care (CKMC). Forty in-depth interviews and 14 focus group discussionswere conducted between September and December 2012. Participants included pregnant women andmothers, husbands, maternal and paternal grandmothers, traditional birth attendants, village doctors,traditional healers, pharmacymen, religious leaders, community leaders, and formal healthcare providers.Audio recordingswere transcribed and translated intoEnglish, and the textual datawere analyzedusing theFramework Approach. We find that harmful newborn care practices, such as delayed wrapping and earlyinitiation of bathing, are changing as more biomedical advice from formal healthcare providers is reachingthe community through word-of-mouth and television campaigns. While the goal of CKMC was relativelyeasily understood and accepted by many of the participants, logistical and to a lesser extent ideologicalbarriers exist that may keep the practice from being adopted easily. Women feel a sense of inevitable re-sponsibility for household duties despite the desire to provide the best care for their new babies. Ourfindings showed that participants appreciated CKMC as an appropriate treatmentmethod for ill babies, butwere less accepting of it as a protective method of caring for seemingly healthy newborns during the firstfew days of life. Participants highlighted the necessity of receiving help from family members and wit-nessing other women performing CKMC with positive outcomes if they are to adopt the behavior them-selves. Focusing intervention messages on building a supportive environment for CKMC practice will becritical for the intervention's success.
© 2014 Published by Elsevier Ltd.
, [email protected], [email protected] (J.A. Callaghan-Koru), [email protected] (A. Al Mahmud), [email protected] (A. Farzin), [email protected] (E.A. Cristofalo), [email protected] (S. Akhter), [email protected] (A.H. Baqui).e time of the study. Current primary affiliation is: Department of Health and Nutrition, Save the Children e USA,USA.

E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e3022
1. Introduction
Neonatalmortality is growing in global public health importanceas an increasing proportion of under-five deaths occur during thefirst four weeks of life (Oestergaard et al., 2011). In Bangladesh, 60%of under-five deaths occur during the neonatal period, making it anecessity to specifically address neonatal mortality if the country isto continue to improve child survival rates (National Institute ofPopulation Research and Training, Mitra and Associates, & ICFInternational, 2013). While the top three global causes of neonataldeaths are cited as prematurity, intrapartum-related complications,and infections including sepsis, meningitis, and pneumonia (Liuet al., 2012), low birth weight (LBW) contributes to an estimated60e80% of all neonatal deaths (UNICEF and WHO, 2004). LBW ne-onates (<2.5 kg), both preterm and full term, are more likely thannormal weight neonates to suffer from hypothermia and infections(Lunze and Hamer, 2012; Lunze et al., 2013; Mullany et al., 2010a,b).
In Bangladesh, some studies have estimated that over 30% ofinfants have low birth weight (Arifeen et al., 2012), making it acountry with one of the highest LBW rates in the world. The factthat 71% of deliveries in Bangladesh occur at home (77% in ruralareas) (National Institute of Population Research and Training,Mitra and Associates, & ICF International, 2013), coupled with thecommon practices in some regions of delayed wrapping of babiesafter birth and early immersive bathing, results in a large number ofLBW neonates left vulnerable to hypothermia in Bangladesh(Winch et al., 2005).
Neonatal hypothermia, defined as a body temperature at orbelow 36.0 �C (World Health Organization, 1997), increases mor-tality risk and can occur regardless of setting (Lunze et al., 2013). Asystematic review examining neonatal hypothermia in resource-poor settings globally showed high prevalence of hypothermia ininfants born in hospitals (32%e85%) as well as in homes (11%e92%)(Lunze et al., 2013). One of the included trials, conducted in Nepal,found one-fifth of neonates to be hypothermic even during the hotseason (Mullany et al., 2010a,b). Lunze and Hamer (2012) argue thatwhile addressing neonatal hypothermia globally could substan-tially impact neonatal mortality, so far it has been largely neglected.It is estimated that universal coverage of measures preventingneonatal hypothermia, and quick identification and treatmentwhen it occurs, could eliminate up to 40% of neonatal deaths(Darmstadt et al., 2008). Ensuring thermal protection for newbornsduring the first week of life is particularly important, as up to 75% ofnewborn deaths occur during this period (Baqui et al., 2006; Lawnet al., 2005).
The World Health Organization endorses kangaroo mother care(KMC) for medically stabilized low birth weight or preterm infantsin health facilities in order to prevent hypothermia, especially insettings where incubators or warmers are unavailable (WorldHealth Organization, 2003). The three components of facility-based KMC are: 1) continuous skin-to-skin contact of the neonatebetween the mother's bare breasts; 2) early and frequent breast-feeding; and 3) early discharge from the facility with follow-up(Charpak et al., 2005; World Health Organization, 2003). In addi-tion to thermal regulation, KMC encourages newborn-motherbonding, reduces the occurrence of infections in the neonate,supports infant growth, and facilitates exclusive breastfeeding(Conde-Agudelo et al., 2011; World Health Organization, 2003).Continuation of KMC is recommended until the newborn's gesta-tional age reaches term or weight reaches 2500 g (World HealthOrganization, 2003). Systematic reviews of facility-based KMCstudies report that in low- and middle-income countries, thepractice of facility-based continuous KMC is associated with a sig-nificant reduction in the risk of mortality at the time of discharge or40e41 weeks postmenstrual age when compared to controls
receiving traditional care in infant incubators and warmers (Conde-Agudelo et al., 2011).
The evidence of the effectiveness of KMC in reducing neonatalmortality is thus far limited to facility-based interventions. The onlytrial of community-based KMC (CKMC) encountered difficulties inensuring compliancewith continuousCKMCandhadmethodologicalconcerns, thereby making it difficult to draw conclusions about itsefficacy (Sloanetal., 2008).However, community-basedstrategies arenecessary to reach newborns in settings with low utilization offacility-based care, such as rural Bangladesh. KMC is a promisingintervention to adapt for community-based delivery because it is alow-technologypracticeunder thecontrolof families.Aswith facility-based KMC, mothers providing CKMC are encouraged to clean new-borns with a dry or damp cloth and avoid immersive bathing, sleepwith the baby in the kangaroo position while in a semi-reclined po-sition, provide continuous skin-to-skin contact, breastfeed on de-mand, and seek immediate medical care for babies' danger signs(Quasem et al., 2003; World Health Organization, 2003).
In regard to the recommended length of CKMC provision,Ahmed et al. (2011) recommend �7 h of skin-to-skin contact a day,particularly in the first two days of life, as “an important marker ofadequate training, dose and impact” (p.366). Globally, two-thirds ofneonatal deaths occur within the first week of life, with the first daybeing the riskiest (Lawn et al., 2005). Quasem et al. (2003) thereforesuggest that “prolonged maintenance of skin-to-skin contact maynot be essential to significantly reduce neonatal and infant mor-tality” (p. 650). However promising, rigorous assessment of theeffectiveness of KMC in reducing neonatal mortality when prac-ticed in communities is still urgently needed.
1.1. Changing newborn care practices and the role of formativeresearch
Newborn care practices are “rooted in cultural value systemsembedded in social norms” (Kumar et al., 2008, p. 455), thereforeintervention strategies for behavior change must take into accountsocial, cultural, and economic reasons for current practices (Winchet al., 2005). Furthermore, the locus of control for newborn carepractices is not with one single actor; rather the household as a unitmust be targeted along with other influencers (Kumar et al., 2008).Formative research helps researchers and program planners un-derstand the factors that can facilitate or inhibit the adoption of newhealth behaviors and adapt an intervention to address these factors(Gittelsohn et al., 2006). TheNeonatalMortality Formative ResearchWorkingGroup (2008) has documentedhowformative research canbe particularly useful in exploring the multifactorial influences onnewborn care practices, thus informing community-based inter-vention strategies for improving newborn survival. Peer-reviewedpublication of the results of formative research in intervention tri-als is also important for interpreting the consequent trials' results.
Changing newborn care practices is challenging and requiresincorporating insights gained through formative research withsound behavior change theories (Kumar et al., 2008). Whilecommunity-based kangaroo mother care is technologically simple,it requires an extended active commitment on the part of themother and her family, and is divergent from existing social normsin Bangladesh and many other settings. Indeed, some previous ef-forts to encourage skin-to-skin care in various communities glob-ally have achieved limited success (Sloan et al., 2008; Vesel et al.,2013).
1.2. Conceptual framework
Acknowledging that newborn care practices are products ofone's social and cultural milieu and influenced by multiple actors,

E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e30 23
we used the social ecological model (SEM) (McLeroy et al., 1988) toinform our study's conceptual framework (Fig. 1). To develop thisframework and thus guide our study design, we reviewed existingpublic health and anthropological literature on newborn carepractices in South Asia and identified factors at the individual,household, and cultural/community levels that are likely to influ-ence the uptake of CKMC for prevention of neonatal hypothermiaand reduction of neonatal mortality. At the individual level, con-structs from social cognitive theory (Bandura, 2004) informed ouridentification of influential factors, particularly outcome expecta-tions and mothers' self-efficacy in providing CKMC properly.
Our conceptual framework highlights the multifactorial in-fluences on newborn care practices in rural Bangladesh and focuseson how a family's socioeconomic status, religion, householdstructure, and cultural values might affect the care provided to orwithheld from newborns, specifically in regard to thermal protec-tion. Furthermore, we sought to examine underlying power dif-ferentials and decision-making authority within families and howthese dynamics affect newborn care and, potentially, future CKMCprovision. This paper presents our findings with a particular focuson the factors that may facilitate or inhibit the promotion of CKMC,and should therefore be considered in the design of an effectivenesstrial.
2. Methods
2.1. Study setting
The study was conducted in three of the five rural unions ofTungipara Subdistrict, Gopalganj District, Bangladesh. GopalganjDistrict was chosen for this study due to high infant mortality ratescompared with other districts (Bangladesh Bureau of Statistics,(2011)), and an existing relationship between the investigators'research institutions and a local NGO that could coordinate hiringof local community health workers (CHWs) and facilitate partici-pant recruitment. In this district, and across Bangladesh, adult sonscustomarily remain in their natal homes and their wives join theirfamilies' households resulting in joint family structures. The me-dian age at marriage for women is 15.8, and women have onequarter of their children before the age of twenty (National Instituteof Population Research and Training, Mitra and Associates, & ICFInternational, 2013). The predominant religion is Islam (89.37%),while 9.59% of the population identifies as Hindu (BangladeshBureau of Statistics, (2011)).
Women in the study area are not typically involved in incomegenerating activities, while the majority of the men hold farming,fishing, day labor, or transportation-related jobs. With typically justone earning member in each household, inhabitants in the studyarea are poor by international standards, often earning 200e250Bangladesh Taka (BDT) per day (roughly 2.50 USD). Even so, mosthouseholds in the study area have basic access to electricity, canemploy fans during the hot months, and own a television.
2.2. Ethical approval
The study was approved by the Johns Hopkins BloombergSchool of Public Health Institutional Review Board and ICDDR,BEthical Review Committee. All participants gave written informedconsent to participate and were free to withdraw their participa-tion at any time.
2.3. Participant recruitment and sampling
Four CHWs were hired locally and trained to canvass the studyarea household-to-household. Using standard forms, they listed all
individuals who met study eligibility criteria and noted whether ornot they agreed to be contacted by the study team. These includedpregnant women and mothers (delivered within 2 months) andtheir families, traditional healers, village doctors, religious leaders,male and female community leaders, and traditional birth atten-dants. Participants were then purposively sampled from this list toensure inclusion of perspectives from Muslim and Hindu faiths,various ages, nulliparous and multiparous women of both nuclearand joint households, and those of various economic situations.Health workers at health facilities most frequently utilized by thecommunity were also selected for interviews, after gainingapproval from the district's Civil Surgeon. Data collection continueduntil thematic saturation was reached.
2.4. Data collection
We utilized both in-depth interviews (IDIs) and focus groupdiscussions (FGDs) because each method offered distinct advan-tages for addressing our research questions. IDIs were particularlyuseful for gaining a detailed understanding of newborn care prac-tices following childbirth. Focus group research is considered tohave particular advantages for eliciting thoughtful reactions totopics that are abstract, technical, or new to participants (Ritchieand Lewis, 2003). FGDs therefore provided our study participantsa forum to consider a new approach to childcare with the benefit ofhearing the reactions of other participants, allowing them tocompare and contrast their opinions.
Three female qualitative interviewers with health researchexperience and masters degrees in anthropology were hired fromDhaka and underwent weeklong training and field piloting beforecollecting data over a two-month period (SepteOct 2012) and anadditional week in December 2012. Field guides were updated afterpiloting to improve clarity. CHWs contacted study participants viamobile phone or home visit to arrange interview times. IDIs aver-aged 80 min and took place in the participant's home or work placewith strict privacy, while FGDs were held in a private roomwithin anon-governmental free community health clinic and lasted 90 minon average. FGD participants' travel expenses were reimbursed.Interviewers explained the study's purpose and requested written(or thumbprint) informed consent from all participants. Only onewoman refused to participate during the consent process.
During both interviews and focus group discussions, in-terviewers used a field guide to facilitate discussion about localnewborn and infant care practices. Interviewers then briefly pre-sented the concept of CKMC using video, photos (InternationalNetwork of Kangaroo Mother Care, 2012; World HealthOrganization, 2003), and/or a demonstration doll before spendingthe remaining portion of the IDI or FGD eliciting feedback, con-cerns, and suggestions from the participants regarding the practice.Throughout data collection, the study team identified existing carepractices that may facilitate or conflict with CKMC practice, andparticipants were asked to reflect on the role of these factors.Discussions were conducted in Bengali and audio recorded, whileinterviewersmaintained detailed discussion and observation notes.
2.5. Analysis
Thorough debriefing meetings were conducted daily after eachIDI and FGD, during which the study team reviewed field notes,adjusted field guides, identified andmemoed emerging themes andoutlying opinions for member checking through probing in sub-sequent interviews, and assessed the level of data saturation onparticular topics before selecting participants for the following day.Interviewers then transcribed their audio recordings, which werelater translated into English by a translation consultant. Transcripts
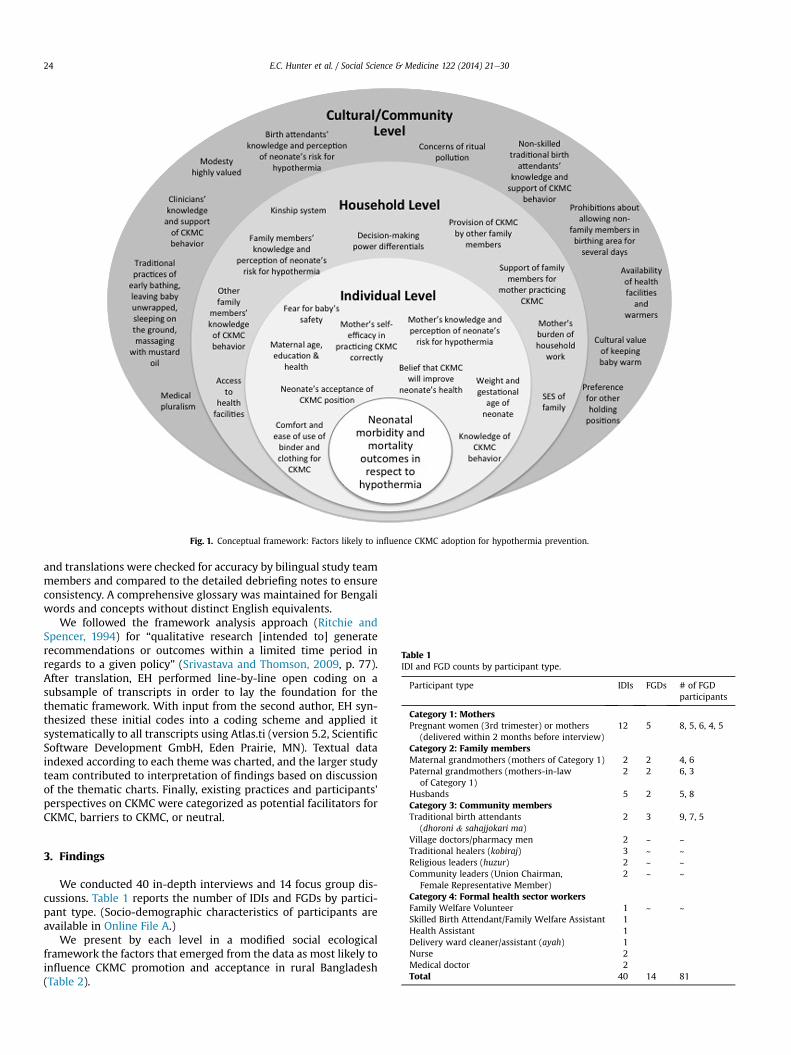
Table 1IDI and FGD counts by participant type.
Participant type IDIs FGDs # of FGDparticipants
Category 1: MothersPregnant women (3rd trimester) or mothers
(delivered within 2 months before interview)12 5 8, 5, 6, 4, 5
Category 2: Family membersMaternal grandmothers (mothers of Category 1) 2 2 4, 6Paternal grandmothers (mothers-in-law
of Category 1)2 2 6, 3
Husbands 5 2 5, 8Category 3: Community membersTraditional birth attendants 2 3 9, 7, 5
Fig. 1. Conceptual framework: Factors likely to influence CKMC adoption for hypothermia prevention.
E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e3024
and translations were checked for accuracy by bilingual study teammembers and compared to the detailed debriefing notes to ensureconsistency. A comprehensive glossary was maintained for Bengaliwords and concepts without distinct English equivalents.
We followed the framework analysis approach (Ritchie andSpencer, 1994) for “qualitative research [intended to] generaterecommendations or outcomes within a limited time period inregards to a given policy” (Srivastava and Thomson, 2009, p. 77).After translation, EH performed line-by-line open coding on asubsample of transcripts in order to lay the foundation for thethematic framework. With input from the second author, EH syn-thesized these initial codes into a coding scheme and applied itsystematically to all transcripts using Atlas.ti (version 5.2, ScientificSoftware Development GmbH, Eden Prairie, MN). Textual dataindexed according to each theme was charted, and the larger studyteam contributed to interpretation of findings based on discussionof the thematic charts. Finally, existing practices and participants'perspectives on CKMC were categorized as potential facilitators forCKMC, barriers to CKMC, or neutral.
(dhoroni & sahajjokari ma)Village doctors/pharmacy men 2 ~ ~Traditional healers (kobiraj) 3 ~ ~Religious leaders (huzur) 2 ~ ~Community leaders (Union Chairman,
Female Representative Member)2 ~ ~
Category 4: Formal health sector workersFamily Welfare Volunteer 1 ~ ~Skilled Birth Attendant/Family Welfare Assistant 1Health Assistant 1Delivery ward cleaner/assistant (ayah) 1Nurse 2Medical doctor 2Total 40 14 81
3. Findings
We conducted 40 in-depth interviews and 14 focus group dis-cussions. Table 1 reports the number of IDIs and FGDs by partici-pant type. (Socio-demographic characteristics of participants areavailable in Online File A.)
We present by each level in a modified social ecologicalframework the factors that emerged from the data as most likely toinfluence CKMC promotion and acceptance in rural Bangladesh(Table 2).

E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e30 25
3.1. Cultural and community level
3.1.1. Thermal protection of neonates culturally valuedThe community places value in keeping neonates warm, as
indicated by the customs of regularly bathing newborns and infantswhen the sun is at its warmest, warming bath water, administeringmustard oil massages intended to be warming, refraining fromusing much water whenwiping neonates after defecation, lactatingmothers limiting their exposure to water for fear of “passing cold”through their breast milk to the baby, sitting infants in the sunduring winter months for warmth, and wrapping very small neo-nates in extra blankets. While many practices still exist that leaveneonates vulnerable to hypothermia, study participants werecognizant that cold is risky for neonates and routinely expresseddesire to prevent “cold attaching to babies.” Indeed, participantsreported recent changes in care practices affecting neonates' bodytemperature, including the trend for some families to delay bathingnewborns until 72 h after delivery to prevent cold. Medical rec-ommendations such as these are spreading via word-of-mouth bywomen who deliver in health facilities as well as traditional birthattendants who accompany women during facility deliveries orreceive basic training in safe delivery.
3.1.2. Local understanding of illness etiologiesWhile there is a strong cultural value of keeping neonates pro-
tected from cold, there is also widespread local understanding thatoverheating and excessive sweating causes illness. Holding babiesfor too long against one's body, particularly during the hot season,is thought to be detrimental to their development. Overheating isseen to result in fever and diarrhea, while sweat remaining on one'schest was widely cited by participants as a cause of pneumonia.Participants perceived the kangaroo position as capable of over-heating the neonate and inducing excessive sweating, and there-fore regarded it as potentially dangerous.
In such a [hot] season [KMC is] quite impractical…I always kept mychildren under the fan, so they don't sweat and catch cold fromtheir sweat. (Mother, IDI participant)
Elder people say if you always hold the baby, the baby does not staywell. Getting body heat, the baby won't grow properly. If the babylies down then they grow quickly and stay healthy. (Mother, FGDparticipant)
3.1.3. Existing newborn care practicesKangaroo mother care differs considerably from the care
currently given to neonates in much of rural Bangladesh. Whilesome existing care practices appear to present opportunities forCKMC promotion, our data also revealed a number of challenges.
Table 2Factors most likely to influence CKMC promotion and acceptance.
Community andcultural level
Thermal protection of neonates culturally valuedLocal understanding of illness etiologiesExisting newborn care practicesResistance to an unfamiliar practiceAtur traditionCommunity support
Household level Decision-making dynamicsHeavy household work burdenFamily support for newborn care and household work
Individual level Perceived susceptibility and severityOutcome expectationsObservational learningPhysical discomfort and perceived health risks
A potential challenge to encouraging CKMC is that holding aninfant too often is commonly perceived to habituate him or her tobeing held, thus leading to over-attachment and disruption of thecaregivers' work well into the future. Therefore, there is a strongpreference for leaving a sleeping or contented baby lying on a bedsupported between kol balish (bolster pillows), oftentimes under afan during the summer, while his or her caregiver attends tohousehold work.
Infant feeding practices may also present challenges to CKMCuptake. Breastfeeding is highly valued and universal, but exclusivebreastfeeding is not common. Prelacteal feeds are near universal,and caregivers supplement with infant formula (when affordable)or porridges made of rice, sugar, and water when they feel mothersare insufficiently lactatingda widely expressed concern. As LBW islocally attributed to “malnutrition,” emphasis is placed on feedingsmall neonates more frequently (up to twice an hour), thereforeincreasing the likelihood of supplemental feeds with a bottle. Someparticipants expressed concern that CKMC would disrupt care-givers' ability to provide this bottle-feeding:
If the baby has a nutrition problem [referring to LBW], no one willwant to keep it like this [in KMC position]. They want to give morenutritious food for good growing than KMC. (Mother, IDIparticipant)
With regard to hygiene practices, early and immersive bathing isthe traditional norm in the study area. Most participants said theimmediate bathing of neonates after delivery is necessary becausethey are born dirty and could have a bad odor if left unbathed.Babies are also said to be fussy if not bathed because the feeling ofbeing dirty is unpleasant. However, most participants did not seeimmersive bathing restrictions (a component of CKMC) as a largehindrance to CKMC uptake, because they felt thorough wiping witha damp cloth would be accepted by many as sufficient for a shortperiod of time. A huzur (Muslim religious leader) stated that Islamrequires the immediate bathing of a newborn to rid the innocentchild of the napak (ritually unclean/polluted) blood and fluid frombirth. However, during subsequent FGDs with mothers, their fam-ilies, and dhoroni (traditional birth attendants), most participantsreported being unaware of a specific religious mandate concerningthe bathing of neonates.
Other infant hygiene practices may affect future CKMC provi-sion. Rather than being diapered, neonates are held along with asmall katha (quilt made of old saris), which is replaced every timethe neonate passes waste. Kathasmay be easier to change while theneonate remains in the kangaroo position since the cloth is notfastened to the baby's body, but this practice may result in thecaregiver being soiled more easily by the neonate's excreta.
Theway inwhich neonates andmothers are customarily dressedpresents both opportunities and potential challenges for the intro-duction of CKMC. Kangaroo mother care involves placing a neonateagainst hismother's bare chestwhilewearing only a diaper, hat, andsocks e with the addition of an open-faced sleeveless shirt duringcolder months. In rural Bangladesh, neonates are typically notdressed for the first few days of life, being only wrapped with akatha. After the first few days, the common dress for neonates insummer consists of thin, sleeveless, open-front shirts (neema) andunclothed bottoms. During the winter, babies are dressed in thickerfabrics such as wool or thick cotton. Open-front neema are condu-cive for kangaroo mother care during winter months, but this attiremay be seen as only appropriate for the summer season. Conversely,most participantswere stronglyopposed to the idea of putting socksand hats on neonates during the summer, regardless of their size.
The customary dress of recently delivered women is veryconducive to CKMC provision, in that sari blouses with front closure

E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e3026
and three-piece suits (salawar kameez) or maxi gowns with frontzippers all provide easy access to the mother's bare chest. Addi-tionally, the ubiquitous orna (scarf) women wear to cover theirchests was suggested as appropriate for using to secure neonates inthe kangaroo position. Concerns that practicing CKMC wouldcompromise women's modesty were not issued by participants,since the women would provide this care only within their home.
3.1.4. Resistance to an unfamiliar practiceHaving never before witnessed a neonate being cared for with
CKMC, many participants were hesitant about the method despitehearing of its potential benefits. Participants reported that elders,who are influential in the community, as well as those in thecommunity who are less educatedmay be less accepting of the newmethod because they hold on to old day thinking. That is to say,they may see no reason to change traditional care practices thatseem harmless.
Even those who view CKMC as potentially beneficial may beunwilling to be early adopters of the practice or may do so onlywhen others cannot see, due to fears of being criticized by thecommunity for their unusual behavior.
Participant: If my husband permits it, then I may keep the baby likethis (in KMC position). But since I haven't seen anyone keeping thebaby like this, I am a little skeptical.
Interviewer: If you think it has benefit then why don't you want tokeep the baby like this?
Participant: Because if I do it for the first time then people maymake fun of me and call me names. So if I see someone do it then Ican also do it. (Mother, IDI participant)
Interestingly, the community seems to have recently been opento changes in other newborn care practices, such as feedingcolostrum rather than disposing of the first milk. Numerous par-ticipants reported this recent shift and attributed it to the effects ofhealth messages aired on television. However, there is a tremen-dous difference in the time and effort required to feed neonatescolostrum versus the commitment needed for the provision ofcontinuous CKMC.
3.1.5. Atur traditionAnother cultural/community level factor with implications for
CKMC promotion is the traditional practice of rest and confinementduring aturda special period of time following delivery. Whileparticipants said aturmay last up to 45 days, the first six days (chotoatur) are the most important for maintaining rituals, and arecharacterized by the recently delivered woman remaining with herneonate alone in bed inside the room where the delivery occurred(atur ghor). Traditionally, only relatives or elder women enter theatur ghor, and before doing so, must follow rituals intended toprevent bringing evil into the room. Restrictions lessen after thesixth day and more so after the 21st day of atur.
Some participants said that the tradition of seclusion in the aturghor is observed because a recently delivered woman's bleeding isnapak and lojja (shameful) and so she is therefore kept away fromothers to avoid polluting them, exposing them to the smell, andembarrassing the recently delivered woman. Others explained thata woman is weak and tired following delivery and she and her newbaby should rest and remain protected from germs, evil eye, andbad winds during this especially vulnerable period. While manyindividual and household level factors such as the location of de-livery and the support available from family affect how strictly arecently delivered woman observes atur traditions, the observance
of such could potentially facilitate CKMC provision in some in-stances. Choto atur coincides with the most vital period for theprovision of continuous kangaroo mother care. Mothers able toobserve at least choto atur might find CKMC more feasible becausethey are not required to move around or perform household workduring this time.
3.1.6. Community supportWith the majority of births occurring at home, dhoroni play a
significant role in the care and support of laboring and recentlydelivered women. Study participants expressed how having sup-port from dhoroni and other neighbors during the first few daysfollowing delivery could likely facilitate CKMC. Some dhoroniexpressed their willingness to take on recently delivered women'shousehold workloads or to hold neonates in the kangaroo positionfor short periods if it was determined to be necessary for a neo-nate's survival. However, dhoroni have their own families to care forand are thus limited in the amount of time they can spend assistingmothers with CKMC.
3.2. Household level
3.2.1. Decision-making dynamicsHousehold factors emerged as highly influential in determining
whether or not caregivers would consider providing CKMC.Younger mothers lack autonomy and decision-making powerwithin the household, having to acquiesce decisions to mothers-in-law and husbands often even regarding infant care.
Participant 2: No one might object openly but some people havesisters-in-law or mothers-in-law who may not approve of thismethod.
Participant 4: Yes. There are some in-laws who do not care whathappens to the baby. They just want the household work to getdone. (Mothers, FGD participants)
Participants indicated that convincing senior family memberswith decision making power of the benefits of CKMC, and gainingtheir support, would be critical for CKMC adoption. They suggestedthis be done through promotional messages on television and byformal health care providers and CHWs.
3.2.2. Heavy household work burdenThe most salient perceived barrier to practicing CKMC in the
home is that of the need for women to continue their householdwork responsibilities after childbirth. Women are responsible forcooking, cleaning, collecting water, washing clothes, taking care oflivestock, and rearing children. In the cases of women living innuclear families or with unsympathetic mothers-in-law, the aturperiod may not be traditionally observed, and neglecting workresponsibilities to care for a neonate could result in the family goingwithout prepared meals, physical abuse of a recently deliveredwoman, strife between her and her in-laws, and even abandon-ment by her husband.
You see, we are poor people and have to work hard to make ourends meet. So doing such a method [CKMC] is almost a luxury forus, leaving aside all the work and stuff. (Husband of a recentlydelivered woman, IDI participant)
Participants believed holding a neonate in the kangaroo positionwhile working would be unacceptable due to the dangers it couldpose to the baby, such as exposure to extreme heat or jumping hotoil and embers from cooking over clay stoves. The only instance

E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e30 27
where a participant felt it would be safe was in the case of fisher-men's wives who could safely sit and knit fishing nets.
3.2.3. Family support for newborn care and household workWomen in the study area prefer to return to their natal homes to
give birth with the support of their own mothers, when feasibleand allowable by their husbands. A woman who spends the aturperiod in her natal home with her own able-bodied mother is mostlikely to be allowed a period of rest during which she has little to nohousehold responsibilities and can focus on providing CKMC.However, if she is required to spend the atur period in her hus-band's household, she must have a caring and supportive mother-in-law and ideally sisters-in-law willing to take on her householdresponsibilities during the time of CKMC provision.
If the mother is at her maternal home, then it is possible. Themother does not have to do anything. But when you are back atyour in-laws and your husband then you have to look after yourhusband and other children. You cannot stick with the baby all thetime. (Mother, FGD participant)
Participants noted that motivated husbands, sisters-in-law,mothers, mothers-in-laws and older children of recently deliv-ered women could, in some cases, step in to help hold the neonateskin-to-skin or take on extra household work, which would facili-tate CKMC provision. Participants suggested that willing in-dividuals should be identified and a plan for assistance fixed beforethe delivery occurs.
3.3. Individual level
3.3.1. Perceived susceptibility and severityNeonates born at home are not weighed, and are deemed
“normal size” or “small” by comparing them to a couple's previouschildren or other neonates seen in the community. Babies consid-ered small are typically fed more frequently and are sometimescovered with more blankets than babies judged to be normal
Table 3Summary of CKMC intervention design considerations.
Primary design considerations Associat
Promoting CKMC before delivery� During pregnancy period, CHWs educate household on CKMC� Identification of decision-makers in the home and potential helpers� Communication on local TV channels (restricted to the viewership
of a particular village area)� Messages from doctors and nurses� Engagement of community elders, dhoroni, kobiraj, village doctors� Early adopters of CKMC serve as examples to others
� Build� Educa
extrem� Prom� Babie
Addressing initial concerns� Discomfort� Sweating� Cord care� Feeding� Sleeping
� Acknoand e
� Babie� Preter� Moth� KMC� KMC� Ackno
result
Supporting families of LBW neonates� Early identification of LBW neonates for referral and continued
KMC beyond the first week of life� Frequent visits by CHWs
� Proble� Impor
conce
Potential tools to promote CKMC� KMC pouch� Adapting katha to be secured like a diaper� Support pillows for sleeping
� KMCin kan
� Provid
weight, but they are not often taken for postnatal care due to theirsize alonedrather only in the case of having other recognizableillnesses. Discussions with study participants across participantcategories indicate that caregivers would be more likely to viewCKMC as necessary and beneficial if a neonate is noticeably ill andmuch less likely to adopt a new caretaking practice for neonatesperceived to be otherwise “well,” even if they are of low birthweight. Additionally, participants were much more receptive to theidea of practicing CKMC during winter, and indeed a few partici-pants reported already keeping their neonates close to their chestfor warmth during the colder months, although not going so far asto provide direct and continuous skin-to-skin contact.
3.3.2. Outcome expectationsParticipants who showed the most interest in CKMC readily
accepted the potentially lifesaving benefits of the practice andstated that they would do anything in their power to ensure theirnewborn's wellbeing. As several participants put it, “for the sake ofthe baby, everything is possible.” Participants responsive to CKMCperceived it to be likely capable of calming upset neonates leadingto less crying, keeping them “warm and cozy,” protecting them from“dust, germs, and wind,” and therefore likely to keep the baby “welland good.” Participants also valued the ease with which a neonatein the kangaroo position could breastfeed, granted the mother islactating sufficiently.
3.3.3. Observational learningParticipants reported that they would have more trust in the
practice of CKMC and its benefits if they were to directly observeothers caring for their neonates in this waywith positive outcomes.As early adopters in the community begin to care for their neonateswith CKMC, the practice's acceptability and perceived efficacy willlikely increase within the community.
There are people who might get convinced in using the methodonce they see that my baby is doing fine. (Husband, FGDparticipant)
ed focus points
on the existing local knowledge of the importance of keeping neonates warmtion of and buy-in from husbands, mothers, and mothers-in-law isely important
ote observational learnings can suffer from hypothermia even during hot seasons
wledge existing holding preferences, but highlight that KMC is not permanent,vidence shows it impacts mother-newborn bonding positivelys gain weight and grow quicker when cared for with KMCm and LBW babies may not sweat for the first couple weeks of lifeers' breasts thermoregulate to keep neonate from overheatingshould not inhibit cord healingpromotes lactationwledge there may be a normal increase in frequency of neonate's defecationing from more exclusive breastfeeding
m solving related to household work responsibilitiestance of CHWs providing reinforcement, encouragement, and addressingrns as they arise
pouch can be made inexpensively and locally, and may increase sense of securitygaroo position, but is NOT compulsory for CKMCe prototypes of KMC pouch to local tailors

E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e3028
3.3.4. Physical discomfort and perceived health risksParticipants of all types mentioned the likelihood that CKMC
could cause bodily discomfort to recently delivered women andtheir neonates, and may even lead to problems with breathing andinfection of the cord stump from the prolonged close contact. Sinceparticipants were resistant to the notion of working or movingabout while providing CKMC, they were also concerned about thepains they would feel from remaining in one position for anextended period of time.
Concerns over discomfort were especially heightened in thecase of adolescent mothers who were said to suffer from intensepain and weakness (hanglar betha) in the days following delivery:
Actually young mothers cannot keep the baby like this. Thegrandmothers can do. Young mothers are very weak after delivery[…] They suffer a lot with the first baby but with the next babies thisproblem is reduced. A young mother would need to sleep and restand during this time they may drop the baby in this method.(Mother, IDI participant)
Indeed, study participants mentioned that many women,particularly adolescents and primiparas do not hold their ownneonates to breastfeed for a period following delivery, rather theyrely on female relatives to hold the neonates to their breasts.Holding one's own neonate to the breast was perceived to increasehanglar betha.
Across participant types, therewaswidespread concern over thediscomfort and safety risk of providing CKMC during the nightwhile the mother sleeps. Only a few participants suggested solu-tions to making sleeping in the kangaroo position safer, while mostwere categorically opposed to the idea.
If the mother turns in her sleep then the baby may get under themother and get hurt, so that would be a problem. In fact the babymay suffocate and die too. That is why the baby has to be kept wellwrapped up at night. But the method that you have shown seems tobe effective. If the mother keeps a few pillows then the risk isminimized a lot. (Husband, IDI participant)
4. Discussion
4.1. Principal findings
We find that this study population values thermal protection ofneonates and has shown openness to changing certain traditionalnewborn care practices for the health of babies. At the same time,local understandings of illness etiologies lead to fear that CKMCcould cause pneumonia and other illnesses by overheating neo-nates and inducing excessive sweating. Concerns over discomfort,particularly for young mothers, and the risk of private and publicridicule for practicing a method contrary to traditional care prac-tices were prevalent, however the most salient identified barrierwas that of women's heavy burdens of household work. Opportu-nities exist to promote universal CKMC practice during the post-natal confinement period, and adoption is more likely if householddecision makers, including husbands and the mothers andmothers-in-law of pregnant and recently delivered women areconvinced of the benefits of CKMC.
While we acknowledge the existence of influential structuraland super-structural level factors such as widespread poverty,gender inequality, and poor financing for social services, we focusin this paper on the factors that span the cultural/community,household, and individual levels since these are often the mostamenable to change through community-level interventions. We
found the social ecological model incorporated with constructsfrom social cognitive theory to be useful in structuring our study,informing the development of our field guides, and focusing ourdata analysis. This conceptual framework enabled the study teamto remain cognizant that a multifactorial web of influences de-termines newborn care practices, and this guided the interviewersin their probes.
4.2. Trial recommendations
A previous randomized controlled cluster trial in 42 unions ofDhaka and Sylhet Divisions, Bangladesh sought to determinewhether or not CKMC would have an effect on neonatal mortality(Sloan et al., 2008). However, there was only a 24% CKMC adoptionrate and short duration of CKMC practice in the intervention armand no effect on mortality was seen (Ahmed et al., 2011). The au-thors acknowledge limitations in their trial and stress that futuretrials should ensure baseline comparability of mortality betweenintervention and control arms, ensure adequate CKMC imple-mentation and behavior uptake through better training of pro-moters, and include birth weight assessments (Sloan et al., 2008).Beyond these recommendations, our formative research suggestsadditional strategies for designing a locally acceptable interventionpackage to test strategies for promoting continuous CKMC througha methodologically rigorous trial.
A CKMC trial should begin with the implementation of facility-based KMC in the study region and Trials of Improved Practices(TIPs) (Dickin et al., 1997) to elicit locally devised solutions for thebarriers to CKMC presented in this paperdsuch as concerns overdiscomfort, sweating, cord care, feeding, and sleeping in the kan-garoo position. TIPs will also be useful in determining the best useof “tools” for CKMC, such as a fabric pouch to better secure new-borns in the kangaroo position and the use of support pillows forsleeping, and the adaptation of the katha to be secured like a diaperduring CKMC provision.
Following the establishment of facility KMC and TIPs, werecommend that CKMC be promoted broadly in the community byCHWs and formal healthcare providers, but especially to pregnantwomen and their families as a practice to be performed universallyduring the choto atur period. CKMC promotion activities shouldengage community members such as elders, dhoroni, kobiraj, andvillage doctors who are influential in determining newborn care,and promotional messages on local television channels should beconsidered where available. CHWs should identify decision-makersin the home and include them in counseling and education aboutCKMC. Additionally, CHWs should assist pregnant women indeveloping a plan for conducting CKMC and recruiting familymembers or other helpers willing to assist new mothers withhousehold chores during the choto atur period. Following de-liveries, CHWs should assist in identifying LBW babies as early aspossible, make necessary referrals to facilities, and provide supportand counseling to those families whose newborns would particu-larly benefit from CKMC beyond just the choto atur period. Toencourage observational learning, early-adopter families thatpractice and benefit from CKMC should be encouraged to activelyparticipate in CKMC promotion within the community. Table 3outlines these design considerations along with associated focuspoints.
4.3. Comparison with other findings
As we found the threat of cold to be a salient concern in ourstudy population, so too have researchers in the Sylhet region ofBangladesh (Winch et al., 2005). Winch et al. (2005) depart fromthe often-cited notion that “a sense of fatalism and cultural

E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e30 29
acceptance of high mortality” (Lawn et al., 2004, p. 399) in familiesof neonates is a reason for persistent high rates of neonatal mor-tality in low-income countries. He asserts that anthropologicalstudies across the world have shown that families of neonates areoften far from fatalistic:
[Instead they] plan and undertake a series of measures based oncore principles, such as: children are very vulnerable and atincreased risk for serious health problems during the first weeks oflife; […] and coldness is dangerous and efforts are required to keepthe baby warm at all times (Winch et al., 2005, p. 483).
Indeed, our findings reveal how cognizant families are of therisk that cold presents to newborns and the many practices theyadhere to in order to minimize the risk.
Confinement and seclusion following delivery is rather strictlypracticed in the conservative district of Sylhet, which has beennoted as a potential barrier to neonatal health programs (Winchet al., 2005). Dissimilarly, a study in an urban slum in Dhakafound that this tradition was difficult to adhere to since poor urbanfamilies often live together in one room (Choudhury et al., 2009). Inour study area, the confinement period is observed less strictly thanin Sylhet, and indeed many participants reported receiving supportand care during this time or exhibited willingness to seek medicalassistance outside the home if deemed necessary, accessible, andaffordable. Mothers and their families in our study population oftenmake pragmatic decisions, keeping the best interest of their baby'shealth in mind while working within the constraints of their eco-nomic means.
Our participants' statements suggest that mothers may bereceptive to practicing CKMC provided that they recognize theirnewborn to be sick or requiring extra care, and they have observedCKMC successfully modeled in the community. Convincingmothersof healthy, full-term babies to universally practice CKMC immedi-ately after birth until the newborn can be assessed by a healthworkerda consideration that is likely necessary for CKMC to beeffective at reducing neonatal mortality in settings with limitedpostnatal caredis expected to be more challenging.
Previous exploratory studies have examined CKMC's accept-ability in other contexts. A CKMC pilot study in Sylhet foundresistance from mothers to sleeping in the KMC position. Theirparticipants reported little familial resistance to the practice ofCKMC, however those women who did report resistance felt itmost from mothers-in-law and sisters-in-law (Quasem et al.,2003). Similarly, efforts in Nepal to evaluate the feasibility ofusing female community health workers to identify LBW babiesin the community and to provide them with home-based careand support, including skin-to-skin care counseling, found thatwomen were adverse to sleeping with their neonates in thekangaroo position due to discomfort and fears of smothering(Saving Newborn Lives, ACCESS, and USAID, 2008). They werealso uncomfortable providing skin-to-skin care during hotweather (mainly due to sweating), were sometimes too shy toprovide such care, feared being soiled with the neonate'sexcreta, and found that some babies' cords became infected(Saving Newborn Lives, ACCESS, and USAID, 2008). A study inGhana found skin-to-skin care to be disruptive to women'sroutines, as they were not comfortable working with their ne-onates in the kangaroo position, and expressed concern over therisk of cord infection (Vesel et al., 2013). Fears about cord stumpinfection were also reported as a barrier in a study promotingskin-to-skin care in India, as were weakness and pain of thepostpartum mother and discomfort during the summer months(Darmstadt et al., 2006). Our similar findings reinforce recom-mendations to address these specific factors in a future CKMC
intervention and trial to test the efficacy of CKMC in reducingneonatal mortality.
4.4. Study limitations
Our interviewers were university educated in Dhaka and thismay have influenced participants to provide socially desirable re-sponses concerning practices they know modern medical scienceconsiders harmful. For example, one interviewee denied givingliquids other than breast milk to her baby, yet the interviewer notedthe presence of a baby bottle full of water next to a jar of honey inthe home. (Water and honey are common prelacteal feeds inBangladesh.) In effort to prevent these occurrences, interviewerswere trained to take an informal approach to the interviews andclearly explain that discussions were not health education visits.The lead author refrained in most cases from accompanying in-terviewers during IDIs, since she is noticeably foreign and assumedto be university educated.
5. Conclusion
The importance the study population places on keeping neo-nates warm bodes well for the introduction of a low cost, lowtechnology intervention to achieve this objective in the communitysetting. However, given the existence of several barrierseparticu-larly the heavy burden of household work placed on mother-seestablishing a supportive home and community environmentwill be critical for successful CKMC adoption. The recommendationthat CKMC be universally encouraged for all neonates regardless oftheir gestational age and birth weight (Saving Newborn Lives,ACCESS, and USAID, 2008) will be especially difficult to achieve.Our findings clearly showed that participants appreciated CKMC asan appropriate treatment method for ill babies, but were lessaccepting of it as a protective method of caring for seeminglyhealthy newborns during their first few days of life. Moving for-ward, further emphasis should be placed on ensuring adequatecommunity-level birth weight assessments so families are awarewhen their babies' birth weights are too low and special newborncare is needed.
Acknowledgments
The study was funded by a grant from the Johns Hopkins Uni-versity Center for Global Health. We acknowledge the administra-tive and logistical support from the Centre for SustainableDevelopment and Research (CSDR) staff; the generosity of theProjahnmo Clinic staff in Tungipara, Bangladesh; our hardworkinginterviewers Maksuda Akter, Sufia Khatun, and Anifron Nessa Jany;and Johns Hopkins School of Public Health student intern ZaynahChowdhury. Most importantly, we thank our study participantswho graciously welcomed us into their homes, work places, andhealth facilities or traveled to participate in focus group discussionsdespite sometimes difficult transportation conditions.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.socscimed.2014.10.006.
References
Ahmed, S., Mitra, S.N., Chowdhury, A.M.R., Camacho, L.L., Winikoff, B., Sloan, N.L.,2011. Community kangaroo mother care: implementation and potential forneonatal survival and health in very low-income settings. J. Perinatol. 31 (5),361e367. http://dx.doi.org/10.1038/jp.2010.131.
E.C. Hunter et al. / Social Science & Medicine 122 (2014) 21e3030
Arifeen, S.E., Mullany, L.C., Shah, R., Mannan, I., Rahman, S.M., Talukder, M.R.,Baqui, A.H., 2012. The effect of cord cleansing with chlorhexidine on neonatalmortality in rural Bangladesh: a community-based, cluster-randomised trial.Lancet 379 (9820), 1022e1028. http://dx.doi.org/10.1016/S0140-6736(11)61848-5.
Bandura, A., 2004. Health promotion by social cognitive means. Health Educ. Behav.: Off. Publ. Soc. Public Health Educ. 31 (2), 143e164. http://dx.doi.org/10.1177/1090198104263660.
Bangladesh Bureau of Statistics, 2011. Report on the Sample Vital RegistrationSystem-2010.
Baqui, A.H., Darmstadt, G.L., Williams, E.K., Kumar, V., Kiran, T.U., Panwar, D.,Santosham, M., 2006. Rates, timing and causes of neonatal deaths in rural india:implications for neonatal health programmes. Bull. World Health Organ. 84 (9),706e713.
Charpak, N., Ruiz, J.G., Zupan, J., Cattaneo, A., Figueroa, Z., Tessier, R., Worku, B.,2005. Kangaroo mother care: 25 years after. Acta Paediatr. (Oslo, Norway 1992)94 (5), 514e522. http://dx.doi.org/10.1080/08035250510027381.
Choudhury, N., Neeloy, A., Rashid, S., Moran, A., Sharmin, T., 2009. Maternal,Newborn, and Child Healthcare Practices: an Exploratory Study of Korail Slumin Dhaka. ICDDR,B; BRAC, Dhaka (Manoshi-WP03).
Conde-Agudelo, A., Belizan, J.M., Diaz-Rossello, J., 2011. Kangaroomother care to reducemorbidity and mortality in low birthweight infants. Cochrane Database Syst. Rev.(Online) 3, CD002771. http://dx.doi.org/10.1002/14651858.CD002771.pub2 doi(3),CD002771.
Darmstadt, G.L., Kumar, V., Yadav, R., Singh, V., Singh, P., Mohanty, S., Santosham, M.,2006. Introduction of community-based skin-to-skin care in rural Uttar pra-desh, india. J. Perinatol. Off. J. Calif. Perinat. Assoc. 26 (10), 597e604. http://dx.doi.org/10.1038/sj.jp.7211569.
Darmstadt, G.L., Walker, N., Lawn, J.E., Bhutta, Z.A., Haws, R.A., Cousens, S., 2008.Saving newborn lives in Asia and Africa: cost and impact of phased scale-up ofinterventions within the continuum of care. Health Policy Plan. 23 (2), 101e117.http://dx.doi.org/10.1093/heapol/czn001.
Dickin, K., Griffiths, M., Piwoz, E., 1997. DESIGNING BY DIALOGUE: A ProgramPlanners' Guide to Consultative Research for Improving Young ChildFeeding.
Gittelsohn, J., Steckler, A., Johnson, C.C., Pratt, C., Grieser, M., Pickrel, J., Staten, L.K.,2006. Formative research in school and community-based health programs andstudies: “State of the art” and the TAAG approach. Health Educ. Behav. Off. Publ.Soc. Public Health Educ. 33 (1), 25e39. http://dx.doi.org/10.1177/1090198105282412.
International Network of Kangaroo Mother Care, 2012. In: IX International Con-ference on Kangaroo Mother Care. Photos available at: http://www.kmcindia2012.org/ (accessed 28.06.12.).
Kumar, V., Mohanty, S., Kumar, A., Misra, R.P., Santosham, M., Awasthi, S., SakshamStudy Group, 2008. Effect of community-based behaviour change managementon neonatal mortality in Shivgarh, Uttar pradesh, India: a cluster-randomisedcontrolled trial. Lancet 372 (9644), 1151e1162. http://dx.doi.org/10.1016/S0140-6736(08)61483-X.
Lawn, J.E., Cousens, S., Bhutta, Z.A., Darmstadt, G.L., Martines, J., Paul, V., Horton, R.,2004. Why are 4 million newborn babies dying each year? Lancet 364 (9432),399e401. http://dx.doi.org/10.1016/S0140-6736(04)16783-4.
Lawn, J.E., Cousens, S., Zupan, J., Lancet Neonatal Survival Steering Team, 2005. 4million neonatal deaths: when? where? why? Lancet 365 (9462), 891e900.http://dx.doi.org/10.1016/S0140-6736(05)71048-5.
Liu, L., Johnson, H.L., Cousens, S., Perin, J., Scott, S., Lawn, J.E., Child Health Epide-miology Reference Group of WHO and UNICEF, 2012. Global, regional, andnational causes of child mortality: an updated systematic analysis for 2010 withtime trends since 2000. Lancet 379 (9832), 2151e2161. http://dx.doi.org/10.1016/S0140-6736(12)60560-1.
Lunze, K., Bloom, D.E., Jamison, D.T., Hamer, D.H., 2013. The global burden ofneonatal hypothermia: systematic review of a major challenge for newbornsurvival. BMC Med. 11 (1), 24. http://dx.doi.org/10.1186/1741-7015-11-24.
Lunze, K., Hamer, D.H., 2012. Thermal protection of the newborn in resource-limited environments. J. Perinatol. Off. J. Calif. Perinat. Assoc. 32 (5), 317e324.http://dx.doi.org/10.1038/jp.2012.11.
McLeroy, K.R., Bibeau, D., Steckler, A., Glanz, K., 1988. An ecological perspective onhealth promotion programs. Health Educ. Q. 15 (4), 351e377.
Mullany, L.C., Katz, J., Khatry, S.K., Leclerq, S.C., Darmstadt, G.L., Tielsch, J.M., 2010a.Incidence and seasonality of hypothermia among newborns in southern Nepal.Arch. Pediatr. Adolesc. Med. 164 (1), 71e77. http://dx.doi.org/10.1001/archpediatrics.2009.239.
Mullany, L.C., Katz, J., Khatry, S.K., LeClerq, S.C., Darmstadt, G.L., Tielsch, J.M., 2010b.Neonatal hypothermia and associated risk factors among newborns of southernNepal. BMC Med. 8 http://dx.doi.org/10.1186/1741-7015-8-43, 43-7015-8-43.
National Institute of Population Research and Training, Mitra and Associates, & ICFInternational, 2013. Bangladesh demographic and Health Survey 2011.
Neonatal Mortality Formative Research Working Group, 2008. Developingcommunity-based intervention strategies to save newborn lives: lessonslearned from formative research in five countries. J. Perinatol. Off. J. Calif. Per-inat. Assoc. 28 (Suppl. 2), S2eS8. http://dx.doi.org/10.1038/jp.2008.166.
Oestergaard, M.Z., Inoue, M., Yoshida, S., Mahanani, W.R., Gore, F.M., Cousens, S.,United Nations Inter-Agency Group for Child Mortality Estimation and the ChildHealth Epidemiology Reference Group, 2011. Neonatal mortality levels for 193countries in 2009 with trends since 1990: a systematic analysis of progress,projections, and priorities. PLoS Med. 8 (8), e1001080. http://dx.doi.org/10.1371/journal.pmed.1001080.
Quasem, I., Sloan, N.L., Chowdhury, A., Ahmed, S., Winikoff, B., Chowdhury, A.M.,2003. Adaptation of kangaroo mother care for community-based application.J. Perinatol. Off. J. Calif. Perinat. Assoc. 23 (8), 646e651. http://dx.doi.org/10.1038/sj.jp.7210999.
Ritchie, J., Lewis, J., 2003. Qualitative Research Practice: a Guide for Social ScienceStudents and Researchers. Sage Publications, London.
Ritchie, J., Spencer, L., 1994. Qualitative data analysis for applied policy research. In:Bryman, A., Burgess, R.G. (Eds.), Analyzing Qualitative Data. Routledge, London.
Saving Newborn Lives, ACCESS, USAID, 2008. Community-based Care for Low BirthWeight Newborns: the Role of Community Skin-to-skin Care [meeting sum-mary]. Washington, DC: Available at: http://www.savethechildren.org/atf/cf/%7B9def2ebe-10ae-432c-9bd0-df91d2eba74a%7D/KMC-MEETING-REPORT.PDF.
Sloan, N.L., Ahmed, S., Mitra, S.N., Choudhury, N., Chowdhury, M., Rob, U.,Winikoff, B., 2008. Community-based kangaroo mother care to preventneonatal and infant mortality: a randomized, controlled cluster trial. Pediatrics121 (5), e1047e59. http://dx.doi.org/10.1542/peds.2007-0076.
Srivastava, A., Thomson, B., 2009. Framework analysis: a qualitative methodologyfor applied policy research. JOAAG 4 (2), 72.
UNICEF and WHO, 2004. Low Birthweight: Country, Regional, and Global Estimates.Vesel, L., ten Asbroek, A.H., Manu, A., Soremekun, S., Tawiah Agyemang, C., Okyere, E.,
Kirkwood, B.R., 2013. Promoting skin-to-skin care for low birthweight babies:findings from the ghana newhints cluster-randomised trial. Trop. Med. Int.Health TM & IH 18 (8), 952e961. http://dx.doi.org/10.1111/tmi.12134.
Winch, P.J., Alam, M.A., Akther, A., Afroz, D., Ali, N.A., Ellis, A.A., Bangladesh PRO-JAHNMO Study Group, 2005. Local understandings of vulnerability and pro-tection during the neonatal period in sylhet district, bangladesh: a qualitativestudy. Lancet 366 (9484), 478e485. http://dx.doi.org/10.1016/S0140-6736(05)66836-5.
World Health Organization, 1997. Thermal protection of the Newborn: a PracticalGuide. World Health Organization, Geneva.
World Health Organization, 2003. Kangaroo Mother Care: a Practical Guide. WorldHealth Organization, Geneva.
Related Documents











