Review Article www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefits 269 ABSTRACT Objectives: To assess the pharmacologic and clinical benefits of 3 new oral anticoagulants—the direct thrombin inhibitor dabigatran and 2 Factor Xa inhibitors, rivaroxaban and apixaban—in patients with atrial fibrillation (AF). Study Design: A PubMed literature search was performed using the criteria “atrial fibrillation” and “stroke” with each of the follow- ing: “dabigatran,” “apixaban,” and “rivaroxaban.” Methods: Articles published from January 2009 to October 2011 were analyzed for randomized clinical studies sufficiently powered to identify rates of stroke and non–central nervous system sys- temic embolism. Subgroup analyses were excluded. Articles were analyzed for randomized, controlled studies enrolling more than 500 patients. A search on www.clinicaltrials.gov was performed to identify additional studies. All searches were performed in January 2011 and updated in October 2011. Results: All 3 new oral anticoagulants are at least as effective and safe as warfarin for the prevention of stroke and systemic embolism in patients with AF. Given the differences in the patient populations studied, conclusions about the relative efficacy and safety of these agents cannot be made. Conclusions: The new oral anticoagulants offer potential advan- tages over warfarin, particularly in terms of key safety end points and ease of use, while achieving a comparable level of protection against stroke in patients with AF. These advantages may increase adherence to therapy, improve clinical outcomes, and decrease overall healthcare costs, providing an increased benefit for indi- viduals at greatest risk for AF-induced stroke. (Am J Pharm Benefits. 2012;4(6):269-283) A trial fibrillation (AF) is the most common sustained cardiac arrhythmia, and its prevalence is expected to increase significantly over the next few decades. 1 Currently, it is estimated that between 2.1 and 5.1 million people are affected by AF in the United States. 2,3 As the population ages, this number is expected to increase to ap- proximately 16 million people by 2050. 3 Thromboembolic stroke is the most serious potential con- sequence of AF, and patients with AF face 5-fold higher risk of stroke than those without AF. 3 Identification of discrete risk factors for stroke has enabled the development of risk stratification scoring systems to estimate the composite risk of stroke in patients with AF. The most widely used risk strat- ification system is the CHADS 2 score. This systems assigns points based on various risk factors (ie, Congestive heart failure, Hypertension, Age >75 years, Diabetes mellitus, and prior history of Stroke or transient ischemic attack [TIA]), and uses the composite score to stratify patients into groups at low, moderate, or high risk of stroke. 4 The most recent evidence-based guidelines established by the American Col- lege of Cardiology Foundation/American Heart Association/ European Society of Cardiology (ACCF/AHA/ESC) as well as the guidelines of the American College of Chest Physicians (ACCP) suggest oral anticoagulation therapy rather than no therapy (level of evidence: grade 1B) for patients with AF at moderate risk of stroke (CHADS 2 = 1). 5,6 Because stroke is the leading cause of serious long-term disability and the third-leading cause of death in the United States, effective strategies for stroke prophylaxis in patients with AF have a significant clinical and economic impact. 7 BENEFITS AND LIMITATIONS OF TRADITIONAL ANTICOAGULANTS The current standard of care recommended by ACCF/ AHA/ESC is anticoagulant therapy with warfarin, a vitamin K antagonist (VKA), or antiplatelet therapy when anticoagu- lation is contraindicated or inappropriate. 5 However, many At a Glance Practical Implications p 270 Author Information p 281 Full text and PDF www.ajpblive.com New Oral Anticoagulants for Stroke Prevention in Atrial Fibrillation Daniel E. Hilleman, PharmD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Review
Article
www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts 269
ABSTRACTObjectives: To assess the pharmacologic and clinical benefi ts of 3 new oral anticoagulants—the direct thrombin inhibitor dabigatran and 2 Factor Xa inhibitors, rivaroxaban and apixaban—in patients with atrial fi brillation (AF).
Study Design: A PubMed literature search was performed using the criteria “atrial fi brillation” and “stroke” with each of the follow-ing: “dabigatran,” “apixaban,” and “rivaroxaban.”
Methods: Articles published from January 2009 to October 2011 were analyzed for randomized clinical studies suffi ciently powered to identify rates of stroke and non–central nervous system sys-temic embolism. Subgroup analyses were excluded. Articles were analyzed for randomized, controlled studies enrolling more than 500 patients. A search on www.clinicaltrials.gov was performed to identify additional studies. All searches were performed in January 2011 and updated in October 2011.
Results: All 3 new oral anticoagulants are at least as effective and safe as warfarin for the prevention of stroke and systemic embolism in patients with AF. Given the differences in the patient populations studied, conclusions about the relative effi cacy and safety of these agents cannot be made.
Conclusions: The new oral anticoagulants offer potential advan-tages over warfarin, particularly in terms of key safety end points and ease of use, while achieving a comparable level of protection against stroke in patients with AF. These advantages may increase adherence to therapy, improve clinical outcomes, and decrease overall healthcare costs, providing an increased benefi t for indi-viduals at greatest risk for AF-induced stroke.
(Am J Pharm Benefi ts. 2012;4(6):269-283)
A trial fi brillation (AF) is the most common sustained
cardiac arrhythmia, and its prevalence is expected
to increase signifi cantly over the next few decades.1
Currently, it is estimated that between 2.1 and 5.1 million
people are affected by AF in the United States.2,3 As the
population ages, this number is expected to increase to ap-
proximately 16 million people by 2050.3
Thromboembolic stroke is the most serious potential con-
sequence of AF, and patients with AF face 5-fold higher risk
of stroke than those without AF.3 Identifi cation of discrete
risk factors for stroke has enabled the development of risk
stratifi cation scoring systems to estimate the composite risk
of stroke in patients with AF. The most widely used risk strat-
ifi cation system is the CHADS2 score. This systems assigns
points based on various risk factors (ie, Congestive heart
failure, Hypertension, Age >75 years, Diabetes mellitus, and
prior history of Stroke or transient ischemic attack [TIA]),
and uses the composite score to stratify patients into groups
at low, moderate, or high risk of stroke.4 The most recent
evidence-based guidelines established by the American Col-
lege of Cardiology Foundation/American Heart Association/
European Society of Cardiology (ACCF/AHA/ESC) as well as
the guidelines of the American College of Chest Physicians
(ACCP) suggest oral anticoagulation therapy rather than no
therapy (level of evidence: grade 1B) for patients with AF at
moderate risk of stroke (CHADS2 = 1).5,6
Because stroke is the leading cause of serious long-term
disability and the third-leading cause of death in the United
States, effective strategies for stroke prophylaxis in patients
with AF have a signifi cant clinical and economic impact.7
BENEFITS AND LIMITATIONS OF TRADITIONAL ANTICOAGULANTS
The current standard of care recommended by ACCF/
AHA/ESC is anticoagulant therapy with warfarin, a vitamin
K antagonist (VKA), or antiplatelet therapy when anticoagu-
lation is contraindicated or inappropriate.5 However, many
At a Glance
Practical Implications p 270
Author Information p 281
Full text and PDF www.ajpblive.com
New Oral Anticoagulants for Stroke Prevention in Atrial Fibrillation
Daniel E. Hilleman, PharmD
Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts

270 The American Journal of Pharmacy Benefi ts • November/December 2012 www.ajpblive.com
� Hilleman
P R A C T I C A L I M P L I C A T I O N S
Dabigatran, rivaroxaban, and apixaban are 3 new oral anticoagulants that can be used as alternatives to warfarin in patients with atrial fi brillation.
� The new oral anticoagulants have several clinical advantages over warfarin including lack of necessity for coagulation assay testing and fewer drug and food interactions.
� If the new oral anticoagulants are not used following FDA guidance, they could produce signifi cant adverse clinical outcomes.
� A longer duration of clinical experience with these new oral anticoagu-lants will be required to further defi ne their role in the prevention of stroke in patients with atrial fi brillation.
patients with AF are never prescribed warfarin, and those
who are may use it suboptimally, placing them at high
risk of thromboembolic stroke.8 In addition, warfarin has
several limitations, which makes its use diffi cult outside
the clinical trial setting.9,10
The pharmacodynamic effects of warfarin are infl u-
enced by diet, concomitant medications, comorbid con-
ditions, and genetics, making treatment individualization
and long-term monitoring mandatory. Dosing to maintain
a therapeutic range is adjusted according to a patient’s
international normalized ratio (INR), which is measured
at regular intervals. The potential consequences of exces-
sive anticoagulation (bleeding) or insuffi cient anticoagula-
tion (stroke) can be catastrophic, so frequent monitoring
is recommended during lifelong warfarin treatment.8 The
recently revised ACCP guidelines recommend quarterly
visitations for those with very stable INRs.6
The percentage of time within a therapeutic INR range
(TTR) is directly related to the risk of mortality in patients
with AF, with the lowest risk seen in patients who have
more than 70% of their INR levels within the therapeutic
range.11 Unfortunately, the real-world INR levels seen in
typical outpatient and community care settings are gener-
ally lower than those in patients enrolled in specialized
anticoagulation clinics.12,13 However, results of numerous
studies comparing patient TTRs before and after switch-
ing from a usual care setting to specialized anticoagula-
tion clinics have reported nominal improvements in TTR
levels.14-17 Moreover, the improved TTR levels observed
after switching to an anticoagulation clinic were all be-
low 70% and were associated with improved patient out-
comes, suggesting that the benefi ts associated with a TTR
of more than 70% might be more apparent than real.
Even in an ideal anticoagulation setting, factors such as
patient compliance, patient knowledge of and familiar-
ity with correct warfarin use, and drug discontinuation
inevitably play a role in variable and suboptimal INR
control.12,18,19
The limitations of warfarin have prompted exten-
sive research to develop alternative anticoagulants
that are at least as effective, but are safer and easier
to use. Recently approved oral anticoagulants may
provide simpler, more effective, and safer stroke pre-
vention compared with VKAs in patients with AF. Con-
sequently, the use of these agents as an alternative to
VKAs may improve patient adherence, improve out-
comes, and decrease overall healthcare costs. In 2010
and 2011, 2 new oral anticoagulants were approved
by the US Food and Drug Administration (FDA) for
prevention of stroke and systemic embolism in patients
with nonvalvular AF. These new drugs include the direct
thrombin inhibitor (DTI) dabigatran etexilate (approved
October 2010) and the Factor Xa (FXa) inhibitor rivaroxa-
ban (approved October 2011).20,21 In addition, the FXa
inhibitor apixaban is currently being considered for an
AF-indication approval and has already been approved
in the European Union for prophylaxis of deep vein
thrombosis in patients undergoing knee or hip replace-
ment surgery.22 Although dabigatran is currently recom-
mended as an alternative, the majority of patients with
AF continue to be treated with warfarin.23 This review
examines the pharmacologic and clinical benefi ts of the
new anticoagulants in the prevention of stroke and sys-
temic embolism in patients with AF, focusing on major
phase III study results.
STUDY IDENTIFICATIONA literature search was conducted of all PubMed in-
dexed articles from January 2009 to October 2011 to iden-
tify randomized clinical studies suffi ciently powered to
identify rates of stroke and non–central nervous system
systemic embolism. Subgroup analyses were excluded. A
total of 12 publications were identifi ed using the afore-
mentioned search terms and limitations. All studies were
screened for inclusion. Of these, 4 large randomized
studies were identifi ed. A search on www.clinicaltrials
.gov was performed to identify additional studies. Data
inclusion was based on study quality, not publication
date. All searches were performed in January 2011 and
updated in October 2011.
NOVEL ANTICOAGULANTS: COMPARATIVE PHARMACOLOGY
The new oral anticoagulants function by inhibiting the
coagulation pathway via direct inhibition of thrombin
(dabigatran) or selective site-specifi c inhibition of Factor

www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts 271
Stroke Prevention in Atrial Fibrillation
Xa (rivaroxaban and apixaban).10 In contrast, warfarin
modulates the formation of thrombin at multiple points
in the coagulation cascade by inhibiting the recycling of
vitamin K from its oxidized, inactive state to its reduced,
active form. This process is necessary for the biologic
activity of Factors II (prothrombin), VII, IX, and X, as
well as proteins C and S.24 Unlike warfarin, by specifi -
cally targeting a single coagulation factor, DTIs and FXa
inhibitors do not have broad effects on multiple coagu-
lation factors that may predispose to adverse events.25
Table 1 summarizes the pharmacologic profi les of these
agents.26-28
Dabigatran Dabigatran etexilate was the fi rst oral anticoagulant
to be approved in the United States for stroke preven-
tion in AF.21 Dabigatran has an oral bioavailability of
approximately 3% to 7%. It is administered as a prodrug,
dabigatran etexilate, which does not exhibit any phar-
macologic activity. Dabigatran etexilate is a substrate of
the effl ux transporter P-glycoprotein (P-gp). After oral
administration, dabigatran etexilate is rapidly absorbed
and converted to dabigatran by esterase-catalyzed hy-
drolysis in plasma and in the liver. This process occurs
independently of cytochrome P (CYP) 450 isozymes, but
concomitant use of potent P-gp inducers (eg, rifampin)
should be avoided.21 Originally, dose adjustments were
not required when dabigatran was combined with P-gp
inhibitors; however, because of postmarketing experi-
ence reports, dose adjustments (75 mg twice daily)
are recommended when dabigatran is combined with
potent P-gp inhibitors (ketoconazole, dronedarone) in
patients with reduced renal function (creatinine clear-
ance [CrCl] 15-30 mL/min). Dabigatran is also subject
to conjugation, forming pharmacologically active acyl
glucuronides. Four isomers of dabigatran glucuronide
exist, each accounting for less than 10% of total plasma
dabigatran. Dabigatran is not a substrate, inhibitor, or
inducer of CYP450 enzymes. In its active form, dabi-
gatran has a half-life of approximately 12 to 17 hours.
Approximately 80% of dabigatran is excreted via the
kidneys as unchanged drug. The safety of dabigatran in
patients with severe hepatic impairment has not been
established, but after administration to patients with a
Child-Pugh score of B, no consistent changes in expo-
sure or pharmacodynamic were observed.21
Approval of dabigatran in the United States was based
on the results of the phase III RE-LY (Randomized Evalu-
ation of Long-Term Anticoagulation Therapy) study.29 The
ACCP guidelines recommend 150 mg twice daily of dabi-
gatran rather than dose-adjusted VKA therapy for patients
with AF and paroxysmal AF when anticoagulation therapy
is advised (grade 2B).6 The ACCF/AHA Task Force update
on practice guidelines also recommends dabigatran as an
alternative to warfarin in patients with AF (class I, level B),
but indicates that switching patients already on warfarin
with excellent INR control is of little value.23
In the RE-LY study, 2 dosages of dabigatran—110 mg
twice daily and 150 mg twice daily—were compared with
dose-adjusted warfarin (INR 2.0-3.0) in more than 18,000
patients with AF over a median of 2 years.29 The compari-
son between dabigatran doses was double blind, whereas
warfarin was administered in an open-label fashion. The
primary end point was stroke or systemic embolism. The
primary safety outcome was major bleeding events. The
primary analysis was designed to test whether either dose
of dabigatran was noninferior to warfarin in reducing the
primary end point of stroke or systemic embolism. If non-
inferiority was established, the agents were compared for
statistical superiority.29
Table 1. Pharmacologic Profi les of Dabigatran, Rivaroxaban, and Apixaban Characteristic Dabigatran21,26-28 Rivaroxaban20,26 Apixaban22,26
Mechanism of action Direct thrombin inhibitor Factor Xa inhibitor Factor Xa inhibitor
Prodrug Yes (dabigatran etexilate) No No
Frequency of administration Twice daily Once daily Twice daily
Oral bioavailability 6.5% (absolute) 80% to 100% 66% (absolute)
Cmax in volunteers 1.5-3 h 2-4 h 1-3 h
t½ in volunteers 12-14 h 5-9 h 8-15 h
t½ in elderly patients 12-14 h 11-13 h ~12 h
Renal clearance of unchanged drug 80% 36% 25%
Plasma protein binding 35% >90% 87%
CYP450 metabolism No Yes (3A4, 2J2) Yes (3A4)
CYP450 indicates cytochrome P450; Cmax, time to achieve maximal serum concentration; t1/2, half-life.
272 The American Journal of Pharmacy Benefi ts • November/December 2012 www.ajpblive.com
� Hilleman
Patient eligibility for RE-LY included electrocardio-
graphically documented AF with at least 1 additional risk
factor for stroke (eg, previous stroke, TIA, left ventricular
ejection fraction less than 40%, heart failure symptoms of
New York Heart Association class II or higher in the pre-
ceding 6 months, and age >75 years or age 65 to 74 years
with diabetes, hypertension, or coronary artery disease).29
The mean age of all patients was 71 years; 63.6% were
male, and 20% had experienced a previous stroke or TIA.
When stroke risk was stratifi ed by CHADS2 score, 32% of
patients had a score of 0 to 1 (low risk), 36% had a score
of 2 (moderate risk), and 32% had a score of 3 to 6 (high
risk). Half of enrolled patients (50%) had not previously
been treated with warfarin.29
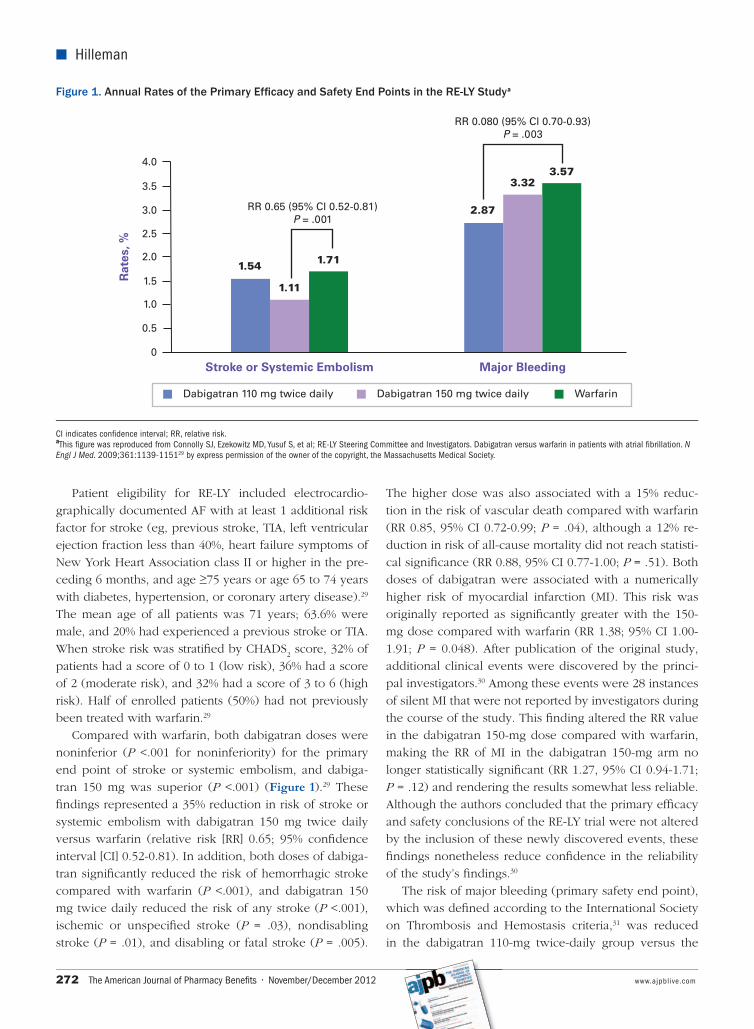
Compared with warfarin, both dabigatran doses were
noninferior (P <.001 for noninferiority) for the primary
end point of stroke or systemic embolism, and dabiga-
tran 150 mg was superior (P <.001) (Figure 1).29 These
fi ndings represented a 35% reduction in risk of stroke or
systemic embolism with dabigatran 150 mg twice daily
versus warfarin (relative risk [RR] 0.65; 95% confi dence
interval [CI] 0.52-0.81). In addition, both doses of dabiga-
tran signifi cantly reduced the risk of hemorrhagic stroke
compared with warfarin (P <.001), and dabigatran 150
mg twice daily reduced the risk of any stroke (P <.001),
ischemic or unspecifi ed stroke (P = .03), nondisabling
stroke (P = .01), and disabling or fatal stroke (P = .005).
The higher dose was also associated with a 15% reduc-
tion in the risk of vascular death compared with warfarin
(RR 0.85, 95% CI 0.72-0.99; P = .04), although a 12% re-
duction in risk of all-cause mortality did not reach statisti-
cal signifi cance (RR 0.88, 95% CI 0.77-1.00; P = .51). Both
doses of dabigatran were associated with a numerically
higher risk of myocardial infarction (MI). This risk was
originally reported as signifi cantly greater with the 150-
mg dose compared with warfarin (RR 1.38; 95% CI 1.00-
1.91; P = 0.048). After publication of the original study,
additional clinical events were discovered by the princi-
pal investigators.30 Among these events were 28 instances
of silent MI that were not reported by investigators during
the course of the study. This fi nding altered the RR value
in the dabigatran 150-mg dose compared with warfarin,
making the RR of MI in the dabigatran 150-mg arm no
longer statistically signifi cant (RR 1.27, 95% CI 0.94-1.71;
P = .12) and rendering the results somewhat less reliable.
Although the authors concluded that the primary effi cacy
and safety conclusions of the RE-LY trial were not altered
by the inclusion of these newly discovered events, these
fi ndings nonetheless reduce confi dence in the reliability
of the study’s fi ndings.30
The risk of major bleeding (primary safety end point),
which was defi ned according to the International Society
on Thrombosis and Hemostasis criteria,31 was reduced
in the dabigatran 110-mg twice-daily group versus the
Figure 1. Annual Rates of the Primary Effi cacy and Safety End Points in the RE-LY Studya
1.54
1.11
Stroke or Systemic Embolism
Rat
es, %
1.71
2.87
3.32
Major Bleeding
3.57
RR 0.65 (95% Cl 0.52-0.81)P = .001
RR 0.080 (95% Cl 0.70-0.93)P = .003
Dabigatran 110 mg twice daily Dabigatran 150 mg twice daily Warfarin
4.0
3.5
2.5
2.0
1.5
1.0
0.5
0
3.0
CI indicates confi dence interval; RR, relative risk.aThis fi gure was reproduced from Connolly SJ, Ezekowitz MD, Yusuf S, et al; RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fi brillation. N Engl J Med. 2009;361:1139-115129 by express permission of the owner of the copyright, the Massachusetts Medical Society.

www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts 273
Stroke Prevention in Atrial Fibrillation
warfarin group (RR 0.80; 95% CI 0.70-0.93), but was simi-
lar in frequency when the higher dabigatran dose was
compared with warfarin (RR 0.93; 95% CI 0.81-1.07). Ma-
jor bleeding rates per year are shown in Figure 1.29 Dys-
pepsia was the only adverse effect that was signifi cantly
more common in the dabigatran arm, occurring in 348
patients (5.8%) in the warfarin group and in 707 patients
(11.8%) and 688 patients (11.3%) in the dabigatran 110-
mg and 150-mg groups, respectively (P <.001 for both
comparisons). The rate of drug discontinuation for gas-
trointestinal (GI) symptoms was slightly higher than 2%
with either dose of dabigatran and 0.6% with warfarin.29
In a subsequent analysis, the rate of the primary end
point was higher in a subgroup of patients who had
experienced a previous stroke or TIA than in patients
without prior stroke/TIA (2.4% per year vs 1.2% per year;
P <.0001).32 In the subgroup with a prior stroke or TIA,
the reduction in the risk of stroke with dabigatran was
mainly due to a reduction in hemorrhagic stroke, because
both doses of dabigatran were associated with a signifi -
cantly lower rate of intracranial bleeding versus warfarin
in this subgroup. However, there was no signifi cant in-
teraction between previous stroke or TIA and the effects
on the primary outcome with either 110-mg (P = .62) or
150-mg (P = .34) dabigatran. In patients with previous
stroke/TIA, major bleeding occurred in fewer patients on
110-mg twice-daily dabigatran versus warfarin (2.7% vs
4.2% per year) and GI bleeding was more common with
150-mg twice-daily dabigatran versus warfarin (2.3% vs
1.4% per year). Because of the relatively small propor-
tion of patients with prior stroke/TIA (20% of the total
study population), the observed differences in outcomes
between dabigatran and warfarin did not reach statistical
signifi cance, but the direction of effects was consistent
with those seen in the overall study population.32
There was a wide variation in INR values among par-
ticipating centers in the RE-LY trial.33 This variation may
have infl uenced differences observed between warfarin
and dabigatran. The mean warfarin recipient TTR in the
RE-LY study was 64% overall, but ranged from 44% in
Taiwan to 77% in Sweden.29,33 Among warfarin recipients,
there was a signifi cant association between TTR and the
primary end point of stroke or pulmonary embolism (P
= .001), major bleeding (P <.0001), total mortality (P
<.0001), and net clinical benefi t (a composite of stroke,
systemic embolism, pulmonary embolism, death, and
major bleeding; P <.0001).33 Moreover, the difference be-
tween dabigatran 150 mg and warfarin for the second-
ary end points of nonhemorrhagic stroke and mortality
was attenuated at higher quartiles of TTR (ie, better INR
control), such that dabigatran 150 mg twice daily was
not superior to warfarin. Dabigatran was associated with
a lower rate of major bleeding versus warfarin at lower
quartiles of TTR, but with a similar rate of major bleeding
and a higher rate of GI bleeding at higher TTR.33
Patients in the dabigatran arms of RE-LY were given
the option to continue in an ongoing long-term extension
study called RELY-ABLE. The primary end point is ma-
jor bleeding, with secondary end points of stroke, non–
central nervous system systemic embolism, pulmonary
embolism, MI, deep vein thrombosis, all-cause mortality,
and a composite of all of these. This study also includes a
cluster-randomized trial of a knowledge translation inter-
vention, which will assess its impact on patient outcomes.
Caution should be used in administration of dabigatran to
the elderly because conditions such as renal impairment,
reduced body weight, and drug interactions may result in
increased risk of major bleeding and fatality.34,35
In most countries outside of the United States, both
doses of dabigatran used in the RE-LY trial were ap-
proved by the countries’ regulatory agencies. In the Uni-
ted States, the FDA approved the 150-mg twice-daily dose
for patients with a CrCl greater than 30 mL/min. For pa-
tients with a CrCl of 15 to 30 mL/min, the FDA approved
the 75-mg twice-daily dose based on pharmacokinetic
and pharmacodynamic modeling. The FDA published its
rationale for its decision to approve the 150-mg twice-
daily dose and not the 110-mg twice-daily dose.36 A basic
assumption in the FDA’s rationale was that stroke was
a considerably more clinically important outcome than
nonfatal and extracranial bleeding episodes. The FDA
looked at 3 subgroups of patients in whom the benefi ts of
a lower risk of bleeding might be expected to outweigh
the higher risk of stroke associated with the 110-mg dose.
These included patients older than age 75 years, patients
with renal dysfunction, and patients with a higher risk of
bleeding. In the 7238 patients in RE-LY 75 years or older,
the rate of stroke and systemic embolism was 1.4 per 100
patient-years for the 150-mg dose and 1.9 per 100 patient-
years for the 110-mg dose. The rate of major bleeding
was higher with the 150-mg dose compared with the 110-
mg dose (5.1 vs 4.4 per 100 patient-years). These rates
indicate similar risk-benefi t assessments of the 2 doses.
In the 3343 patients in RE-LY with a CrCl of 30 to 50
mL/min, the rate of the primary composite effi cacy out-
come was 1.3 per 100 patient-years for the 150-mg dose
compared with 2.4 per 100 patient-years for the 110-mg
dose. The rate of major bleeding for the 150-mg dose
was no different from the rate for the 110-mg dose (5.3
vs 5.7 per 100 patient-years). Hence, the 150-mg dose

274 The American Journal of Pharmacy Benefi ts • November/December 2012 www.ajpblive.com
� Hilleman
had a superior benefi t-risk profi le
in patients with renal dysfunc-
tion. In RE-LY, 57% of patients
who suffered a major bleeding
event either resumed taking their
study medication or had no inter-
ruption in therapy, continuing to
take the same dose. The percent-
ages of these patients who had
an additional major hemorrhage
were similar: 16%, 14%, and
12% in the 110-mg dabigatran,
150-mg dabigatran, and warfarin
groups, respectively. These data
do not support the strategy of
dose reduction if patients have
a bleeding event while taking a
higher dose. Hence, the FDA’s
decision to approve only the 150-
mg strength was based on its in-
ability to identify any subgroup
in which use of the lower dose
would not represent a substantial
disadvantage.
Dabigatran has also been as-
sessed for effi cacy and safety
in patients with acute coronary
syndrome in the phase II dose-
fi nding study Randomised Dabi-
gatran Etexilate Dose Finding
Study In Patients With Acute
Coronary Syndromes Post Index
Event With Additional Risk Fac-
tors For Cardiovascular Complica-
tions Also Receiving Aspirin And
Clopidogrel (RE-DEEM). A total
of 1861 patients presenting with
ST-segment elevation MI (STEMI)
or non-ST-segment elevation MI
(NSTEMI) and at least 1 cardio-
vascular risk factor were random-
ized to receive dabigatran (50, 75,
110, or 150 mg twice daily) or pla-
cebo in addition to standard dual
antiplatelet therapy.37 Following
6 months of treatment, adjuvant
dabigatran treatment increased
the incidence of the primary end
point (composite of major or
clinically relevant minor bleeding
Figure 2. Cumulative Rates of the Primary End Point (Stroke or Systemic Embolism) in the Per Protocol Population (Panel A) and Intention-to-Treat Population (Panel B) in the ROCKET AF Studya
B. Events in Intention-to-Treat Population
A. Events in Per Protocol Population
Days Since Randomization
Days Since Randomization
Cu
mu
lati
ve E
ven
t R
ate,
%C
um
ula
tive
Eve
nt
Rat
e, %
aThis fi gure was reproduced from Patel MR, Mahaffey KW, Garg J, et al; ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fi brillation. N Engl J Med. 2011;365(10):883-89139 by express permission of the owner of the copyright, the Massachusetts Medical Society.

www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts 275
Stroke Prevention in Atrial Fibrillation
events) in a dose-dependent manner (3.5%, 4.3%, 7.9%,
and 7.8% for increasing dabigatran doses and 2.2% for
placebo; P <.001). There was no clear difference between
the placebo and dabigatran groups for the composite of
cardiovascular death, nonfatal MI, or stroke. It is currently
unknown whether a phase III trial of dabigatran in acute
coronary syndrome will be conducted.37
RivaroxabanRivaroxaban is approved for once-daily administra-
tion in patients with AF.20 The effi cacy of rivaroxaban for
stroke prevention in patients with AF was investigated in
the phase III trial ROCKET AF (Rivaroxaban Once Daily,
Oral, Direct Factor Xa Inhibition Compared with Vitamin
K Antagonism for Prevention of Stroke and Embolism
Trial in Atrial Fibrillation) (Figure 2).38,39 Unlike RE-LY,
ROCKET AF was conducted in a double-blind fashion
through use of a double-dummy double-blind technique
as described by the ROCKET AF Study Investigators.38 In
addition, ROCKET AF enrolled a much higher risk patient
population.38,39 Qualifying criteria included prior stroke,
TIA, or systemic embolism or >2 of the following risk
factors: clinical heart failure or left ventricular ejection
fraction <35%, hypertension, age >75 years, or diabetes
mellitus (ie, a CHADS2 score of >2). The proportion of
patients who had not had a previous ischemic stroke,
TIA, or systemic embolism who had <2 risk factors was
capped at 10% of the cohort for each region; the remain-
der were required to have had either previous throm-
boembolism or >3 risk factors (CHADS2 >3). As a result,
90% of patients in ROCKET-AF had a CHADS2 score of >3
versus ~30% of patients who met the same criteria in RE-
LY.36,39 The primary effi cacy end point was the composite
of stroke (ischemic or hemorrhagic) and systemic embo-
lism. The principal safety end point was a composite of
major and nonmajor clinically relevant bleeding events.31
Briefl y, 14,264 patients with nonvalvular AF and in-
creased risk for stroke were randomly assigned rivaroxa-
ban 20 mg once daily or dose-adjusted warfarin.39 The
results of ROCKET AF demonstrated that in the intention-
to-treat analysis, rivaroxaban was noninferior to warfarin
for the prevention of subsequent stroke or systemic em-
bolism (2.1% vs 2.4% per 100 patient-years; hazard ratio
[HR] 0.88, 95% CI 0.75-1.03; P <.001 for noninferiority;
P = .12 for superiority). In the per protocol population
the primary end point occurred in 188 patients in the
rivaroxaban group (1.7% per 100 patient-years) and 241
in the warfarin group (2.2% per 100 patient-years; HR
0.79, 95% CI 0.66-0.96; P <.001 for noninferiority). Princi-
pal safety end point rates (major and nonmajor clinically
relevant bleeding) were similar between the rivaroxaban
and warfarin treatment arms (14.9% vs 14.5% per 100
patient-years; HR 1.03, 95% CI 0.96-1.11; P = .44) with
signifi cantly reduced incidents of intracranial and fatal
bleeding rates (0.5% vs 0.7% and 0.2% vs 0.5%, respec-
tively, per 100 patient-years) in the rivaroxaban group.
Major bleeding was defi ned according to the Internation-
al Society on Thrombosis and Hemostasis criteria.31 There
was a signifi cant increase in the number of rivaroxaban
patients with a >2 g/dL reduction in hemoglobin and
transfusions, which was predominantly due to a higher
risk of GI bleeding (3.2% vs 2.2%, P <.001).39
One notable caveat was the lower TTR with warfa-
rin (55%) in the ROCKET AF study compared with that
observed with warfarin in the other studies of the new
anticoagulants in AF patients (range 64%-68%).27,38-40
However, the TTR in ROCKET AF was closer to the rates
observed outside of clinical trials or specialty clinics.13
This may have been a primary reason that the differences
observed between warfarin and rivaroxaban were not
statistically signifi cant in the ROCKET AF study. The trials
with higher warfarin TTR rates included fewer higher-risk
patients than the ROCKET AF study. Patients with higher
CHADS2 scores receiving warfarin are typically more dif-
fi cult to maintain in the TTR than patients with lower
CHADS2 scores.
Adverse events that occurred more frequently in pa-
tients receiving rivaroxaban during the ROCKET AF study
included epistaxis and hematuria. Rivaroxaban is a sub-
strate for both the P-gp transport protein and the CYP iso-
zymes 3A4, 3A5, and 2J2; concomitant administration of
rivaroxaban with combined P-gp and strong CYP3A4 in-
hibitors may cause a signifi cant increase in drug exposure
and bleeding risk.20 In addition, pharmacokinetic studies
have demonstrated that patients with renal impairment
may have a heightened drug response, and caution is ad-
vised when coadministering combined P-gp and weak or
moderate CYP3A4 inhibitors such as diltiazem and amio-
darone.20,41,42 Patients in ROCKET AF were allowed use of
combined P-gp and weak or moderate CYP3A4 inhibitors;
however, no increase in bleeding was observed in patients
who had a CrCl of 30 to 50 mL/min.
A similar large, randomized, phase III trial evaluating
the safety of rivaroxaban for prevention of stroke and
systemic embolism was conducted in 1280 Japanese pa-
tients with AF and either prior stroke, TIA, or non–central
nervous system systemic embolism, or >2 risk factors for
stroke (J-ROCKET AF).43 Patients were randomized to ri-
varoxaban 15 mg once daily (10 mg once daily in patients
with CrCl of 30-50 mL/min) or dose-adjusted warfarin. The

276 The American Journal of Pharmacy Benefi ts • November/December 2012 www.ajpblive.com
� Hilleman
15-mg once-daily dose was chosen to address character-
istics of Japanese patients and the lower anticoagulation
targets of Japanese clinical practice. The primary analysis
tested for noninferiority of the principal safety outcome of
adjudicated major and nonmajor clinically relevant bleed-
ing events. Although the study was powered only for the
primary safety outcome, the primary effi cacy end point
was the composite of adjudicated stroke (ischemic and
hemorrhagic) and non–central nervous system systemic
embolism.43
Consistent with the results of ROCKET AF, rivaroxa-
ban was noninferior to warfarin for the primary safety
outcome (18.0 vs 16.4 per 100 patient-years; HR 1.11; P
<.001 for noninferiority) with fewer fatal bleeding events
and intracranial hemorrhages. For the primary effi cacy
end point, there was a strong trend toward a reduction in
stroke/systemic embolism with rivaroxaban (1.3 vs 2.6 per
100 patient-years; HR 0.49, P = .050).43
Rivaroxaban has also been evaluated for safety and ef-
fi cacy in patients with acute coronary syndrome in the re-
cently completed randomized, placebo-controlled, phase
III trial ATLAS ACS2-Thrombolysis in Myocardial Infarc-
tion 51 (Anti-Xa Therapy to Lower Cardiovascular Events
in Addition to Standard in Subjects with Acute Coronary
Syndrome-Thrombolysis in Myocardial Infarction 51).44 The
trial enrolled 15,570 patients who had presented with symp-
toms suggestive of acute coronary syndrome and in whom
STEMI, NSTEMI, or unstable angina had been diagnosed.
In addition to standard medical therapy (low-dose aspirin
and a thienopyridine), patients were randomly assigned to
twice-daily administration of either 2.5 mg or 5.0 mg of riva-
roxaban or placebo. The primary effi cacy end point was the
composite of cardiovascular death, MI, or stroke.44
Results of the study showed that both doses of riva-
roxaban signifi cantly reduced the primary effi cacy end
point compared with placebo (8.9% vs 10.7%; HR 0.84,
P = .008 [combined effi cacy for 2.5- and 5-mg doses]).
However, compared with placebo, rivaroxab an increased
the risk of major bleeding and intracranial hemorrhage,
but not the risk of fatal bleeding.44
Rivaroxaban is a potent and selective Factor Xa inhibi-
tor with a relatively high bioavailability (~80%) and pre-
dictable pharmacokinetic/pharmacodynamic profi le.20 The
mean half-life of rivaroxaban is 5 to 9 hours in healthy
individuals, and 11 to 13 hours in the elderly. Rivaroxaban
is metabolized primarily in the liver via CYP450 and CY-
P3A4 enzymes, and more than 30% of the drug is excreted
in the feces unchanged—a process mediated, at least in
part, by P-gp. Concomitant administration of rivaroxaban
with strong CYP3A4 or P-gp inhibitors (eg, ritonavir, ke-
toconazole) signifi cantly interferes with the metabolism of
rivaroxaban and should be avoided to prevent increased
drug exposure and risk of bleeding events.20,45 Because
rivaroxaban is cleared primarily by the liver and kidneys,
caution should be exercised when prescribing rivaroxa-
ban to patients with moderate to severe renal impairment
(CrCl 15-30 mL/min) or hepatic impairment (Child-Pugh
Class B and C).
Rivaroxaban is currently approved for stroke preven-
tion in AF at a dose of 20 mg once daily with the evening
meal, and in patients with CrCl of 15 to 50 mL/min at a
dose of 15 mg once daily with the evening meal; rivar-
oxaban is not recommended for use in patients with a
CrCl of <15 mL/min or severe hepatic impairment (Child-
Pugh C) (Table 2).20 Results of clinical studies have shown
that discontinuation of rivaroxaban places patients with
AF at increased risk for thrombotic events. If anticoagula-
tion with rivaroxaban must be discontinued for a reason
other than pathologic bleeding, alternative anticoagula-
tion measures should be considered.20
ApixabanAlthough apixaban is not yet approved in the United
States, its use for stroke prevention in patients with AF
Table 2. Dose Adjustment Requirements of Oral Anticoagulants According to Degree of Renal Impairmenta
Degree of Renal Impairment (GFR CrCl)b Warfarin Dabigatran Rivaroxaban Apixabanc
Mild (50-89 mL/min/1.73 m2) Not required Not required Not required Not required
Moderate (30-49 mL/min/1.73 m2) Not required Not required Dose reduction to15 mg/d
2.5 mg twice dailyd if 2 or more of the following:
• Age >80 y
• Weight <60 kg
• SCr >1.5 mg/dL
Severe (15-29 mL/min/1.73 m2) Not required Dose reduction to 75 mg/d
Dose reduction to15 mg/d
Renal failure (<15 mL/min/1.73 m2) Not required Contraindicated Contraindicated
CrCl indicates creatinine clearance; GFR, glomerular fi ltration rate; SCr, serum creatinine.aAdapted from Harder S. Renal profi les of anticoagulants. J Clin Pharmacol. 2012;52(7):964-975.46 Copyright © 2012 SAGE Publications. Reprinted by permission of SAGE Publications.bCrCl based on Cockroft-Gault equation. cApixaban is not approved, so labeled dose recommendations are not available. dBased on dosing used in the ARISTOTLE trial.
www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts 277
Stroke Prevention in Atrial Fibrillation
has been evaluated in 2 large-scale phase III clinical tri-
als: ARISTOTLE (Apixaban for Reduction In Stroke and
Other Thromboembolic Events) and AVERROES (Apixa-
ban Versus Acetylsalicylic Acid to Reduce the Risk Of
Stroke) (Table 3). Apixaban is currently approved in the
European Union for thromboprophylaxis following total
hip and knee replacement surgeries in adults.21
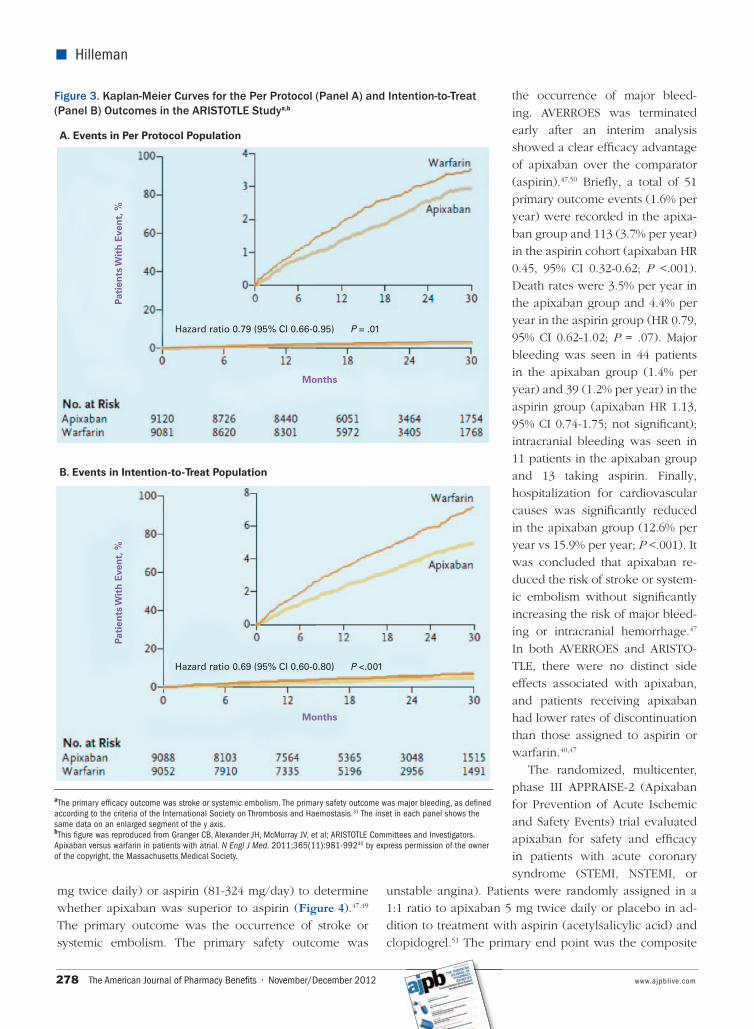
In the ARISTOTLE study, 18,201 patients with AF and >1 additional risk factor for stroke were randomized to
receive either apixaban 5 mg twice daily or dose-adjusted
warfarin (Figure 3).40,48 Patient inclusion criteria were simi-
lar to those in RE-LY; eligible stroke risk factors in ARIS-
TOTLE included age >75 years, prior stroke/TIA/systemic
embolism, symptomatic congestive heart failure or left
ventricular ejection fraction <40%, diabetes, and hyper-
tension requiring treatment.40,48 The key objective of ARIS-
TOTLE was to demonstrate noninferiority to warfarin for
the primary outcome of ischemic or hemorrhagic stroke or
systemic embolism. Secondary objectives included testing
for superiority with respect to the primary outcome, rates
of major bleeding events, and death from any cause.
Apixaban met the primary effi cacy objective of non-
inferiority to warfarin in the ARISTOTLE trial on the
combined outcome of stroke (ischemic, hemorrhagic, or
unspecifi ed type) and systemic embolism. The rate of the
primary outcome was 1.27% per year in the apixaban
group versus 1.60% per year in the warfarin group (HR
with apixaban of 0.79; 95% CI 0.66-0.95; P <.001 for non-
inferiority, P = .01 for superiority).40 In addition, apixaban
met the key secondary end points of superiority to warfa-
rin with respect to the primary outcome and to the rates
of major bleeding (defi ned according to the International
Society on Thrombosis and Hemostasis criteria31) and
death from any cause (2.13% per year in the apixaban
group vs 3.09% per year in the warfarin group; HR 0.69,
95% CI 0.60-0.80; P <.001).40
In the apixaban group, the rate of hemorrhagic stroke
was 0.24% per year versus 0.47% per year in the warfarin
group (HR 0.51, 95% CI 0.35-0.75; P <.001). Moreover, the
rate of ischemic or uncertain-type stroke was 0.97% per
year in the apixaban group versus 1.05% per year in the
warfarin group (HR 0.92, 95% CI 0.74-1.13; P = .42).40 Pa-
tients in the warfarin group were within the therapeutic
range for a mean of 62.2% of the time after the exclusion
of INR values during the fi rst 7 days after randomization.
The investigators concluded that apixaban was superior
to warfarin in patients with AF for prevention of stroke or
systemic embolism, decreased bleeding risk, and reduced
mortality.40
In the AVERROES trial, 5599 patients with AF (mean
age 70 years) who were deemed clinically unsuitable for
VKA treatment were randomized to receive apixaban (5
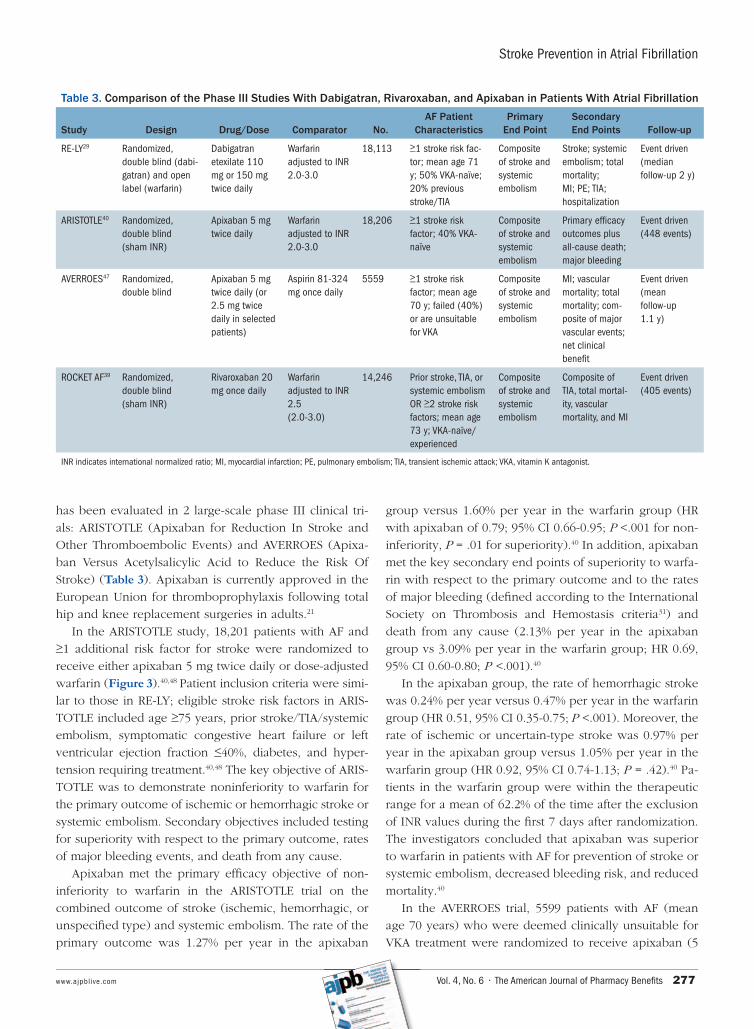
Table 3. Comparison of the Phase III Studies With Dabigatran, Rivaroxaban, and Apixaban in Patients With Atrial Fibrillation
Study Design Drug/Dose Comparator No.AF Patient
CharacteristicsPrimary
End PointSecondary End Points Follow-up
RE-LY29 Randomized, double blind (dabi-gatran) and open label (warfarin)
Dabigatran etexilate 110 mg or 150 mg twice daily
Warfarin adjusted to INR 2.0-3.0
18,113 >1 stroke risk fac-tor; mean age 71 y; 50% VKA-naïve; 20% previous stroke/TIA
Composite of stroke and systemic embolism
Stroke; systemic embolism; total mortality;MI; PE; TIA; hospitalization
Event driven (median follow-up 2 y)
ARISTOTLE40 Randomized, double blind (sham INR)
Apixaban 5 mg twice daily
Warfarin adjusted to INR 2.0-3.0
18,206 >1 stroke risk factor; 40% VKA- naïve
Composite of stroke and systemic embolism
Primary effi cacy outcomes plus all-cause death; major bleeding
Event driven (448 events)
AVERROES47 Randomized, double blind
Apixaban 5 mg twice daily (or 2.5 mg twice daily in selected patients)
Aspirin 81-324 mg once daily
5559 >1 stroke risk factor; mean age 70 y; failed (40%) or are unsuitable for VKA
Composite of stroke and systemic embolism
MI; vascular mortality; total mortality; com-posite of major vascular events; net clinical benefi t
Event driven (mean follow-up 1.1 y)
ROCKET AF39 Randomized, double blind (sham INR)
Rivaroxaban 20 mg once daily
Warfarin adjusted to INR 2.5 (2.0-3.0)
14,246 Prior stroke, TIA, or systemic embolism OR >2 stroke risk factors; mean age 73 y; VKA-naïve/experienced
Composite of stroke and systemic embolism
Composite of TIA, total mortal-ity, vascular mortality, and MI
Event driven (405 events)
INR indicates international normalized ratio; MI, myocardial infarction; PE, pulmonary embolism; TIA, transient ischemic attack; VKA, vitamin K antagonist.
278 The American Journal of Pharmacy Benefi ts • November/December 2012 www.ajpblive.com
� Hilleman
mg twice daily) or aspirin (81-324 mg/day) to determine
whether apixaban was superior to aspirin (Figure 4).47,49
The primary outcome was the occurrence of stroke or
systemic embolism. The primary safety outcome was
the occurrence of major bleed-
ing. AVERROES was terminated
early after an interim analysis
showed a clear effi cacy advantage
of apixaban over the comparator
(aspirin).47,50 Briefl y, a total of 51
primary outcome events (1.6% per
year) were recorded in the apixa-
ban group and 113 (3.7% per year)
in the aspirin cohort (apixaban HR
0.45, 95% CI 0.32-0.62; P <.001).
Death rates were 3.5% per year in
the apixaban group and 4.4% per
year in the aspirin group (HR 0.79,
95% CI 0.62-1.02; P = .07). Major
bleeding was seen in 44 patients
in the apixaban group (1.4% per
year) and 39 (1.2% per year) in the
aspirin group (apixaban HR 1.13,
95% CI 0.74-1.75; not signifi cant);
intracranial bleeding was seen in
11 patients in the apixaban group
and 13 taking aspirin. Finally,
hospitalization for cardiovascular
causes was signifi cantly reduced
in the apixaban group (12.6% per
year vs 15.9% per year; P <.001). It
was concluded that apixaban re-
duced the risk of stroke or system-
ic embolism without signifi cantly
increasing the risk of major bleed-
ing or intracranial hemorrhage.47
In both AVERROES and ARISTO-
TLE, there were no distinct side
effects associated with apixaban,
and patients receiving apixaban
had lower rates of discontinuation
than those assigned to aspirin or
warfarin.40,47
The randomized, multicenter,
phase III APPRAISE-2 (Apixaban
for Prevention of Acute Ischemic
and Safety Events) trial evaluated
apixaban for safety and effi cacy
in patients with acute coronary
syndrome (STEMI, NSTEMI, or
unstable angina). Patients were randomly assigned in a
1:1 ratio to apixaban 5 mg twice daily or placebo in ad-
dition to treatment with aspirin (acetylsalicylic acid) and
clopidogrel.51 The primary end point was the composite
Figure 3. Kaplan-Meier Curves for the Per Protocol (Panel A) and Intention-to-Treat (Panel B) Outcomes in the ARISTOTLE Studya,b
Hazard ratio 0.69 (95% Cl 0.60-0.80) P <.001
Hazard ratio 0.79 (95% Cl 0.66-0.95) P = .01
A. Events in Per Protocol Population
Months
Months
Pati
ents
Wit
h E
ven
t, %
Pa
tien
ts W
ith
Eve
nt,
%
B. Events in Intention-to-Treat Population
aThe primary effi cacy outcome was stroke or systemic embolism. The primary safety outcome was major bleeding, as defi ned according to the criteria of the International Society on Thrombosis and Haemostasis.31 The inset in each panel shows the same data on an enlarged segment of the y axis.bThis fi gure was reproduced from Granger CB, Alexander JH, McMurray JV, et al; ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial. N Engl J Med. 2011;365(11):981-99240 by express permission of the owner of the copyright, the Massachusetts Medical Society.

www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts 279
Stroke Prevention in Atrial Fibrillation
of cardiovascular death, MI, or
ischemic stroke, and the primary
safety end point was major bleed-
ing according to the Thrombolysis
in Myocardial Infarction defi ni-
tion.52 However, in November
2010, the trial was discontinued
prematurely by the Data and Safe-
ty Monitoring Board because of an
increase in major bleeding events
with apixaban in the absence of a
signifi cant reduction in recurrent
ischemic events.51,53
Apixaban is a small-molecule
inhibitor that selectively and re-
versibly targets Factor Xa in both
its free and bound states.22 The bio-
availability of apixaban is approxi-
mately 50%, with peak plasma
levels reached in approximately
3 hours, resulting in a half-life of
12 hours. Similar to the other new
anticoagulants, apixaban has mini-
mal drug interactions. Concomi-
tant use of CYP3A4 inhibitors and
P-gp should be avoided because
they increase the risk of bleeding
events signifi cantly. In addition,
combined inducers of CYP3A4 and
P-gp (eg, rifampin, phenytoin, St.
John’s wort) can signifi cantly re-
duce antithrombotic effi cacy.22
EXPERT OPINIONThe new generation of oral an-
ticoagulants for stroke prophylaxis
in AF includes a DTI (dabigatran)
and 2 FXa inhibitors (rivaroxaban
and apixaban). The pharmaco-
logic profi les of these agents—in-
cluding their specifi c targeting of
single coagulation factors, a wider
therapeutic window, once-daily or
twice-daily fi xed dosing, obviation
of the need for therapeutic drug
monitoring, and lower propensity
for harmful drug or dietary interactions—are likely to re-
sult in signifi cant clinical advantages over warfarin. Based
on the data available from the published trials comparing
the new anticoagulants with warfarin, it is not possible to
reach conclusions about the relative effi cacy of one agent
against another. Differences in the characteristics of the
study populations, the study designs of the trials, and def-
initions of some key study end points make cross-study
Figure 4. Cumulative Hazard Rates for the Primary Effi cacy (Panel A) and Safety (Panel B) Outcomes According to Treatment Group in the AVERROES Studya,b
Months
Months
Cu
mu
lati
ve H
azar
dC
um
ula
tive
Haz
ard
Hazard ratio with apixaban, 0.45(95% Cl 0.32-0.62)
Hazard ratio with apixaban, 1.13(95% Cl 0.74-1.75)
A. Stroke or Systemic Embolism
B. Major Bleeding
P <.001
P = .57
aThe primary effi cacy outcome was stroke or systemic embolism. The primary safety outcome was major bleeding. Patients received either apixaban or aspirin.bThis fi gure was reproduced from Connolly SJ, Eikelboom J, Joyner C, et al; AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fi brillation. N Engl J Med. 2011;364:806-81747 by express permission of the owner of the copyright, the Massachusetts Medical Society.

280 The American Journal of Pharmacy Benefi ts • November/December 2012 www.ajpblive.com
� Hilleman
comparisons impossible. In addition to different mecha-
nisms of action, the new oral anticoagulants have dif-
ferent pharmacokinetic properties (Table 1), potential
drug interactions, and dose-adjustment requirements in
patients with renal impairment (Table 2),20-22,42,46,54 further
hampering the possibility of any meaningful comparative
analyses. Ultimately, the drug product selection and deci-
sion process will be dictated by the level of postmarket-
ing experience, as well as the number and various types
of FDA-approved indications.
Data from phase III studies and recent FDA approvals
indicate that these drugs may provide promising alterna-
tives to warfarin in the prevention of stroke in patients
with AF. Dabigatran and apixaban demonstrated superior
effi cacy compared with warfarin in reducing stroke and
systemic embolism29,40; rivaroxaban demonstrated nonin-
feriority to warfarin with regard to this end point.39 Dabi-
gatran 150 mg twice daily and rivaroxaban had similar
rates of major hemorrhage, while dabigatran 110 mg and
apixaban were shown to have lower rates of major bleed-
ing events compared with warfarin. All of the new agents
were associated with signifi cantly lower rates of critical/
fatal and intracranial bleeding compared with warfa-
rin.29,39,40,47 However, dabigatran and rivaroxaban increased
the risk of GI bleeding compared with warfarin, whereas
apixaban did not.29,39 Furthermore, in January 2012, the
Institute for Safe Medication Practices reported FDA data
from the fi rst quarter of 2011 indicating a 19.5% increase
in reports of serious, disabling, or fatal injuries associated
with dabigatran therapy compared with reports from the
fi rst quarter of 2010.55 These fi ndings were corroborated
in a multicenter observational study of periprocedural
dabigatran compared with warfarin treatment in patients
undergoing AF ablation.56 Results of the study showed that
periprocedural dabigatran (150 mg twice daily) use for AF
ablation was associated with an increased risk of bleeding
and thromboembolic complications compared with war-
farin (6% vs 1%; P = .019).56
Findings from reports and studies such as the afore-
mentioned have increased physician concerns regarding
the potential risks associated with dabigatran and empha-
size the need for ongoing postmarketing surveillance and
adverse-event reporting to detect specifi c risk factors in
patients that may not be apparent in a clinical trial setting.
In addition, because bleeding is potentially compounded
by poor renal function and low body weight, careful
evaluation of the risks and benefi ts of dabigatran must be
exercised in all patients prior to treatment.
As demonstrated in the AVERROES trial, apixaban of-
fers clear benefi ts over aspirin in warfarin-intolerant or
warfarin-unsuitable patients.47 In terms of study design,
ARISTOTLE and ROCKET-AF used a more rigorous ap-
proach to minimizing bias through the double-dummy
and sham INR methodology.40,48 However, many ques-
tions remain unanswered with regard to these agents.
First, the reduced 75-mg dose of dabigatran approved
by the FDA was never tested in RE-LY and was based
solely on pharmacokinetic data modeling.54 In addition,
according to the recently updated ACCP guidelines, this
dose is contraindicated in patients with severe renal
impairment6; thus, it remains unclear whether this dose
will be as effi cacious as warfarin in stroke prevention.
Second, the variable INR control of patients in the RE-
LY and ROCKET AF study had an important impact on
the difference between dabigatran 150 mg twice daily
and rivaroxaban and warfarin.30 This type of subanalysis
based on the results of the ARISTOTLE trial has not been
published to date. Finally, the true comparative effi cacy
of dabigatran, apixaban, and rivaroxaban can only be
determined in head-to-head clinical trials, and it is highly
unlikely that such trials will be conducted.
From a formulary perspective, the cost-effectiveness
of these agents is also unclear. Warfarin is inexpensive,
and its cost-effectiveness has been proved in a number
of clinical trials, with substantial savings arising from pre-
vention of strokes.7,57,58 However, the cost-effectiveness
of warfarin is highly dependent on INR control, and the
need for frequent monitoring is a substantial economic
burden.7,57 Indirect costs associated with transportation
to anticoagulation clinics, lost time from work, appoint-
ments, and blood tests are seldom considered in cost-ef-
fectiveness studies, which tend to focus on direct medical
costs, but these may be important factors to patients.59
Unlike warfarin, none of the new anticoagulants require
monitoring—an important advantage in terms of both
convenience and cost. However, the absence of neces-
sary monitoring may not be suffi cient to designate the
novel agents more cost-effective than warfarin.
Recent cost-comparison analyses have indicated that
dabigatran 150 mg twice daily is cost-effective compared
with warfarin in AF patient populations at high risk of
hemorrhage or high risk of stroke. Using a decision anal-
ysis model, Shah and Gage demonstrated that dabigatran
was cost-effective versus warfarin in a hypothetical co-
hort of 70-year-old AF patients, based on patient crite-
ria derived from the RE-LY study.60 Their model showed
that dabigatran was cost-effective in patients with a
high stroke risk (CHADS2 >3) and in lower-risk patients
(CHADS2 of 2) with high risk of major hemorrhage. Ka-
mel and colleagues used a similar model to show the

www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts 281
Stroke Prevention in Atrial Fibrillation
cost-effectiveness of dabigatran 150 mg twice daily in AF
patients with prior stroke or TIA.61 However, in both stud-
ies, the cost-effectiveness of dabigatran was associated
with the adequacy of warfarin INR management.
Another potential economic advantage of the new an-
ticoagulants is improved patient compliance. Data indi-
cate that discontinuation of warfarin is common among
patients, particularly after a bleeding event and as a result
of safety concerns and the economic burden of INR test-
ing and dose adjustments. Discontinuation of treatment
has been demonstrated to signifi cantly increase healthcare
costs by placing patients at high risk for stroke.57
Despite the clinical and potential economic advan-
tages of the new anticoagulants, complications such as
bleeding remain at the forefront of physician and patient
concerns due to the limited strategies available for re-
versal of their anticoagulant effects. Regardless of the
relatively short half-lives of these agents, immediate an-
ticoagulation reversal may be required in cases of major
bleeding or emergency surgery. Prothrombin complex
concentrate has been considered for use as a potential
antidote due to its high concentration of clotting fac-
tors and ability to enhance thrombin generation. Eeren-
berg and colleagues were the fi rst to evaluate the use
of prothrombin complex concentrate for anticoagulation
reversal of dabigatran and rivaroxaban in humans.62 The
results of the clinical trial showed that the anticoagulant
effect of rivaroxaban was completely reversed immedi-
ately after infusion of prothrombin complex concentrate
in all subjects, whereas the anticoagulant effect of dabi-
gatran remained unaffected. While this study may have
important clinical implications, it is important to note
that all tests were performed in healthy volunteers; the
effect of prothrombin complex concentrate has yet to
be confi rmed in patients with bleeding events who are
treated with these anticoagulants.62
Unlike traditional anticoagulants, a defi ning disadvan-
tage of the new agents is the absence of an antidote.
Furthermore, because there are currently no defi nitive
methods by which to monitor the anticoagulant activ-
ity and intensity of the these agents, it is important that
physicians take into consideration various patient charac-
teristics (eg, age, weight, CrCl, CHADS2 score) and align
therapy choice with clinical outcomes seen in similar pa-
tient populations.
SUMMARYPharmacists have an important role to play in the
pharmacologic management of patients on warfarin. The
identifi cation of potential food and drug interactions,
patient counseling and guidance, and frequent INR test-
ing are all factors that must be carefully monitored during
anticoagulation therapy. The new oral anticoagulants of-
fer potential advantages over warfarin, particularly related
to major hemorrhage, ease of use, and ability to maintain
similar levels of protection against stroke in AF patients.
However, a number of questions remain unanswered, such
as the comparative effi cacy and safety of these agents rela-
tive to one another, the impact of administration sched-
ules on compliance, and the cost-effectiveness of these
agents relative to warfarin. Additional research is needed
to answer these questions, and future head-to-head stud-
ies examining the effi cacy of these new anticoagulants
are unlikely. Ultimately, the drug product selection and
decision process, as well as the number and various types
of FDA-approved indications, will be important in further
defi ning the relative effi cacy and safety of these agents
when used in real-world settings.
Acknowledgment
The author would like to acknowledge Lisa Grauer, MSc, who pro-vided editorial support with funding from Janssen Scientifi c Affairs, LLC.
Author Affi liation: From Department of Pharmacy Practice, Creigh-ton University School of Pharmacy and Health Professions, Omaha, NE.
Funding Source: None.
Author Disclosures: Dr Hilleman reports that he has received grants from Baxter, sanofi -aventis, and Gilead, as well as lecture fees from Janssen, Abbot, sanofi -aventis, Baxter, and AstraZenca.
Authorship Information: Concept and design; acquisition of data; drafting of the manuscript; critical revision of the manuscript for impor-tant intellectual content; and supervision.
Address correspondence to: Daniel E. Hilleman, PharmD, Depart-ment of Pharmacy Practice, Creighton University School of Pharmacy and Health Professions, 2500 California Plaza, Omaha, NE 68178. E-mail: [email protected].
REFERENCES1. Fuster V, Rydén LE, Cannom DS, et al; Task Force on Practice Guidelines, American College of Cardiology/American Heart Association; Committee for Practice Guidelines, European Society of Cardiology; European Heart Rhythm Association; Heart Rhythm Society. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fi brillation-executive summary: a report of the American College of Cardiology/American Heart Association Task Force on prac-tice guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation) [published correction appears in Eur Heart J. 2007;28(16):2046]. Eur Heart J. 2006;27(16):1979-2030.2. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fi brillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence [published correction appears in Circulation. 2006;114(11):e498]. Circulation. 2006;114(2):119-125.
3. Stroke Risk in Atrial Fibrillation Working Group. Independent predictors of stroke in patients with atrial fi brillation: a systematic review. Neurology. 2007;69(6):546-554.
4. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classifi cation schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285(22):2864-2870.
5. Wann LS, Curtis AB, January CT, et al; ACCF/AHA/HRS. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fi brillation (updating the 2006 guideline): a report of the American College of Cardiology Foundation/

282 The American Journal of Pharmacy Benefi ts • November/December 2012 www.ajpblive.com
� Hilleman
American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;57(2):223-242.
6. You JJ, Singer DE, Howard PA, et al; American College of Chest Physicians. Antithrombotic therapy for atrial fi brillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2)(suppl):e531S-e575S.
7. Mercaldi CJ, Ciarametaro M, Hahn B, et al. Cost effi ciency of anticoagulation with warfarin to prevent stroke in medicare benefi ciaries with nonvalvular atrial fi brillation. Stroke. 2011;42(1):112-118.
8. Gladstone DJ, Bui E, Fang J, et al. Potentially preventable strokes in high-risk patients with atrial fi brillation who are not adequately anticoagulated. Stroke. 2009;40(1):235-240.
9. Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G; American College of Chest Physicians. Pharmacology and management of the vitamin K an-tagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6)(suppl):160S-198S.
10. Schirmer SH, Baumhäkel M, Neuberger HR, et al. Novel anticoagulants for stroke prevention in atrial fi brillation: current clinical evidence and future develop-ments. J Am Coll Cardiol. 2010;56(25):2067-2076.
11. Morgan CL, McEwan P, Tukiendorf A, Robinson PA, Clemens A, Plumb JM. Warfarin treatment in patients with atrial fi brillation: observing outcomes associ-ated with varying levels of INR control. Thromb Res. 2009;124(1):37-41.
12. Rose AJ, Ozonoff A, Berlowitz DR, Henault LE, Hylek EM. Warfarin dose man-agement affects INR control. J Thromb Haemost. 2009;7(1):94-101.
13. Baker WL, Cios DA, Sander SD, Coleman CI. Meta-analysis to assess the quality of warfarin control in atrial fi brillation patients in the United States. J Manag Care Pharm. 2009;15(3):244-252.
14. Cortelazzo S, Finazzi G, Viero P, et al. Thrombotic and hemorrhagic complica-tions in patients with mechanical heart valve prosthesis attending an anticoagula-tion clinic. Thromb Haemost. 1993;69(4):316-320.
15. Chiquette E, Amato MG, Bussey HI. Comparison of an anticoagulation clinic with usual medical care: anticoagulation control, patient outcomes, and health care costs. Arch Intern Med. 1998;158(15):1641-1647.
16. Wilson SJ, Wells PS, Kovacs MJ, et al. Comparing the quality of oral anticoag-ulant management by anticoagulation clinics and by family physicians: a random-ized controlled trial [published correction appears in CMAJ. 2004;170(4):451]. CMAJ. 2003;169(4):293-298.
17. Witt DM, Sadler MA, Shanahan RL, Mazzoli G, Tillman DJ. Effect of a central-ized clinical pharmacy anticoagulation service on the outcomes of anticoagulation therapy. Chest. 2005;127(5):1515-1522.
18. Nieuwlaat R, Barker L, Kim YK, et al. Underuse of evidence-based warfarin dosing methods for atrial fi brillation patients. Thromb Res. 2010;125(4):e128-e131.
19. Smith MB, Christensen N, Wang S, et al. Warfarin knowledge in patients with atrial fi brillation: implications for safety, effi cacy, and education strategies. Cardiol-ogy. 2010;116(1):61-69.
20. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals Inc; 2011.
21. Pradaxa [package insert]. Ridgefi eld, CT: Boehringer Ingelheim Pharmaceuti-cals Inc; 2011.
22. Eliquis [summary of product characteristics]. Middlesex, UK: Bristol-Myers Squibb/Pfi zer; 2011.
23. Wann LS, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fi brillation (update on dabigatran): a report of the American College of Cardiology Foundation/Ameri-can Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2011;57(11):1330-1337.
24. Hirsh J, Dalen J, Anderson DR, et al. Oral anticoagulants: mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest. 2001;119(1)(suppl):8S-21S.
25. Ansell J, Hollowell J, Pengo V, Martinez-Brotons F, Caro J, Drouet L. Descrip-tive analysis of the process and quality of oral anticoagulation management in real-life practice in patients with chronic non-valvular atrial fi brillation: the International Study of Anticoagulation Management (ISAM). J Thromb Thromboly-sis. 2007;23(2):83-91.
26. Eriksson BI, Quinlan DJ, Weitz JI. Comparative pharmacodynamics and phar-macokinetics of oral direct thrombin and factor xa inhibitors in development. Clin Pharmacokinet. 2009;48(1):1-22.
27. Stangier J, Clemens A. Pharmacology, pharmacokinetics, and pharmacody-namics of dabigatran etexilate, an oral direct thrombin inhibitor. Clin Appl Thromb Hemost. 2009;15(suppl 1):9S-16S.
28. Stangier J, Stähle H, Rathgen K, Fuhr R. Pharmacokinetics and pharmacody-namics of the direct oral thrombin inhibitor dabigatran in healthy elderly subjects. Clin Pharmacokinet. 2008;47(1):47-59.
29. Connolly SJ, Ezekowitz MD, Yusuf S, et al; RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fi brillation [pub-lished correction appears in N Engl J Med. 2010;363(19):1877]. N Engl J Med. 2009;361(12):1139-1151.
30. Connolly SJ, Ezekowitz MD, Yusuf S, Reilly PA, Wallentin L; Randomized Evalu-ation of Long-Term Anticoagulation Therapy Investigators. Newly identifi ed events in the RE-LY trial. N Engl J Med. 2010;363(19):1875-1876.
31. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientifi c and Standardization Committee of the International Society on Throm-bosis and Haemostasis. Defi nition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost. 2005;3(4):692-694.
32. Diener HC, Connolly SJ, Ezekowitz MD, et al; RE-LY study group. Dabigatran compared with warfarin in patients with atrial fi brillation and previous transient ischaemic attack or stroke: a subgroup analysis of the RE-LY trial [published cor-rection appears in Lancet Neurol. 2011;10(1):27]. Lancet Neurol. 2010;9(12):1157-1163.
33. Wallentin L, Yusuf S, Ezekowitz MD, et al; RE-LY investigators. Effi cacy and safety of dabigatran compared with warfarin at different levels of international normalised ratio control for stroke prevention in atrial fi brillation: an analysis of the RE-LY trial. Lancet. 2010;376(9745):975-983.
34. Jacobs JM, Stessman J. New anticoagulant drugs among elderly patients is caution necessary?: comment on “the use of dabigatran in elderly patients.” Arch Intern Med. 2011;171(14):1287-1288.
35. Legrand M, Mateo J, Aribaud A, et al. The use of dabigatran in elderly patients. Arch Intern Med. 2011;171(14):1285-1286.
36. Beasley BN, Unger EF, Temple R. Anticoagulant options—why the FDA ap-proved a higher but not a lower dose of dabigatran. N Engl J Med. 2011;364(19):1788-1790.
37. Oldgren J, Budaj A, Granger CB, et al; RE-DEEM Investigators. Dabigatran vs. placebo in patients with acute coronary syndromes on dual antiplatelet therapy: a randomized, double-blind, phase II trial. Eur Heart J. 2011;32(22):2781-2789.
38. ROCKET AF Study Investigators. Rivaroxaban-once daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation: rationale and design of the ROCKET AF study. Am Heart J. 2010;159(3):340-347.
39. Patel MR, Mahaffey KW, Garg J, et al; ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fi brillation. N Engl J Med. 2011;365(10):883-891.
40. Granger CB, Alexander JH, McMurray JJ, et al; ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial fi brillation. N Engl J Med. 2011;365(11):981-992.
41. Fleming TR, Emerson SS. Evaluating rivaroxaban for nonvalvular atrial fi brilla-tion—regulatory considerations. N Engl J Med. 2011;365(17):1557-1559.
42. Kubitza D, Becka M, Mueck W, et al. Effects of renal impairment on the phar-macokinetics, pharmacodynamics and safety of rivaroxaban, an oral, direct Factor Xa inhibitor. Br J Clin Pharmacol. 2010;70(5):703-712.
43. Hori M, Matsumoto M, Tanahashi N, et al. J-ROCKET AF: the safety and effi cacy of rivaroxaban for the prevention of stroke in Japanese patients with non-valvular atrial fi brillation. Presented at: XXII Congress of the International Society on Thrombosis and Haemostasis; July 23, 2011; Kyoto Japan. Abstract O-MO-032.
44. Mega JL, Braunwald E, Wiviott SD, et al; ATLAS ACS 2–TIMI 51 Investigators. Rivaroxaban in patients with a recent acute coronary syndrome. N Engl J Med. 2012;366(1):9-19.
45. Kubitza D, Becka M, Wensing G, Voith B, Zuehlsdorf M. Safety, pharmaco-dynamics, and pharmacokinetics of BAY 59-7939—an oral, direct Factor Xa inhibitor—after multiple dosing in healthy male subjects. Eur J Clin Pharmacol. 2005;61(12):873-880.
46. Harder S. Renal profi les of anticoagulants. J Clin Pharmacol. 2012;52(7):964-975.

www.ajpblive.com Vol. 4, No. 6 • The American Journal of Pharmacy Benefi ts 283
Stroke Prevention in Atrial Fibrillation
47. Connolly SJ, Eikelboom J, Joyner C, et al; AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fi brillation. N Engl J Med. 2011;364(9):806-817.48. Lopes RD, Alexander JH, Al Khatib SM, et al; ARISTOTLE Investigators. Apixa-ban for reduction in stroke and other ThromboemboLic events in atrial fi brillation (ARISTOTLE) trial: design and rationale [published correction appears in Am Heart J. 2010;159(6):1162]. Am Heart J. 2010;159(3):331-339. 49. Connoelly SJ, Eikenbloom J, Joyner C, et al. for the AVERROES Steering Com-mittee and Investigators. Abixaban in patients with atrial fi brillation. N Engl J Med. 2011;364:806-817. 50. Connolly S. AVERROES trial terminated early: apixaban associated with “important” relative risk reduction for stroke and systemic embolism in AF [press release]. http://www.escardio.org/about/press/press-releases/esc10-stockholm/Pages/AVERROES-trial.aspx. Published August 31, 2010. Accessed February 18, 2012.51. Alexander JH, Lopes RD, James S, et al; APPRAISE-2 Investigators. Apixaban with antiplatelet therapy after acute coronary syndrome. N Engl J Med. 2011;365(8):699-708.52. Chesebro JH, Knatterud G, Roberts R, et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, phase I: a comparison between intravenous tissue plas-minogen activator and intravenous streptokinase: clinical fi ndings through hospital discharge. Circulation. 1987;76(1):142-154.53. Husten L. APPRAISE-2 dashes hope of adding anticoagulant to antiplatelet therapy in ACS [press release]. http://cardiobrief.org/2011/07/24/appraise-2-dashes-hope-of-adding-anticoagulant-to-antiplatelet-therapy-in-acs/. Published July 24, 2011. Accessed February 29, 2012.54. Lehr T, Haertter S, Liesenfeld KH, et al. Dabigatran etexilate in atrial fi brillation patients with severe renal impairment: dose identifi cation using pharmacokinetic modeling and simulation. J Clin Pharmacol. 2012;52(9):1373-1378.
55. Institute for Safe Medication Practices. QuarterWatch™ (First Quarter 2011) Signals for dabigatran and metoclopramide. http://www.ismp.org/newsletters/acutecare/showarticle.asp?id=12. Published January 12, 2012. Accessed Febru-ary 29, 2012.
56. Lakkireddy D, Reddy YM, Di Biase L, et al. Feasibility and safety of dabigatran versus warfarin for periprocedural anticoagulation in patients undergoing radiofrequency ablation for atrial fi brillation: results from a multicenter prospective registry. J Am Coll Cardiol. 2012;59(13):1168-1174.
57. Sorensen SV, Dewilde S, Singer DE, Goldhaber SZ, Monz BU, Plumb JM. Cost-effectiveness of warfarin: trial versus “real-world” stroke prevention in atrial fi bril-lation. Am Heart J. 2009;157(6):1064-1073.
58. Solomon MD, Ullal AJ, Hoang DD, Freeman JV, Heidenreich P, Turakhia MP. Cost-effectiveness of pharmacologic and invasive therapies for stroke prophylaxis in atrial fi brillation. J Cardiovasc Med (Hagerstown). 2012;13(2):86-96.
59. Hwang JM, Clemente J, Sharma KP, Taylor TN, Garwood CL. Transportation cost of anticoagulation clinic visits in an urban setting. J Manag Care Pharm. 2011;17(8):635-640.
60. Shah SV, Gage BF. Cost-effectiveness of dabigatran for stroke prophylaxis in atrial fi brillation. Circulation. 2011;123(22):2562-2570.
61. Kamel H, Johnston SC, Easton JD, Kim AS. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in patients with atrial fi brillation and prior stroke or transient ischemic attack. Stroke. 2012;43(3):881-883.
62. Eerenberg ES, Kamphuisen PW, Sijpkens MK, Meijers JC, Buller HR, Levi M. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation. 2011;124(14):1573-1579.
Related Documents











