L eg ulceration, often caused by venous stasis, arterial insufficiency, or both, is a common chronic health condition often associated with a prolonged healing trajectory and frequent recurrence. It is estimated that approximately 1.5 to 3.0 per 1,000 adults have active leg ulcers, and the prevalence continues to increase due to an aging population. Management of chronic edema using compression is crucial to promote healing of venous leg ulcers. The principle of compression therapy is simple, involving the use of external pressure in the forms of bandages or wraps to move the fluid from the interstitial space back into the intravascular compartment and prevent reflux. This article synthesizes and appraises the evidence for vari- ous types of compression therapies. It also addresses best practice recommendations for the management of leg ulcers when arterial circulation is considered suboptimal. New Advances in Compression Therapy for Venous Leg Ulcers KEVIN Y. WOO, PHD, RN, FAPWCA ASSISTANT PROFESSOR, SCHOOL OF NURSING QUEEN’S UNIVERSITY KINGSTON, ONTARIO, CANADA - 1 - #483 Woo G - 01 ABSTRACT Wound Healing SURGICAL TECHNOLOGY INTERNATIONAL XXIII AFSANEH ALAVI, MD, FRCPC LECTURER UNIVERSITY OF TORONTO TORONTO, ONTARIO, CANADA ROBYN EVANS, MD, CCFP DIRECTOR, WOUND HEALING CLINIC WOMEN'S COLLEGE HOSPITAL TORONTO, ONTARIO, CANADA MARC DESPATIS, MD, MSC, RVT, FRCSC CHIEF OF V ASCULAR SURGERY AND TRANSPLANTATION CENTRE HOSPITALIER DE SHERBROOKE SHERBROOKE, QUEBEC, CANADA JILL ALLEN, MCISC ,WOCN/ET, RN PROFESSIONAL SERVICES SPECIALIST 3M CANADA COMPANY LONDON, ONTARIO, CANADA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
LLeg ulceration, often caused by venous stasis, arterial insufficiency, or both, is a common chronic health
condition often associated with a prolonged healing trajectory and frequent recurrence. It is estimated
that approximately 1.5 to 3.0 per 1,000 adults have active leg ulcers, and the prevalence continues to
increase due to an aging population. Management of chronic edema using compression is crucial to promote
healing of venous leg ulcers. The principle of compression therapy is simple, involving the use of external
pressure in the forms of bandages or wraps to move the fluid from the interstitial space back into the
intravascular compartment and prevent reflux. This article synthesizes and appraises the evidence for vari-
ous types of compression therapies. It also addresses best practice recommendations for the management of
leg ulcers when arterial circulation is considered suboptimal.
New Advances in Compression Therapy for Venous Leg Ulcers
KEVIN Y. WOO, PHD, RN, FAPWCAASSISTANT PROFESSOR, SCHOOL OF NURSING
QUEEN’S UNIVERSITYKINGSTON, ONTARIO, CANADA
- 1 -
#483 Woo G - 01
ABSTRACT
Wound HealingSURGICAL TECHNOLOGY INTERNATIONAL XXIII
AFSANEH ALAVI, MD, FRCPCLECTURER
UNIVERSITY OF TORONTOTORONTO, ONTARIO, CANADA
ROBYN EVANS, MD, CCFP DIRECTOR, WOUND HEALING CLINIC
WOMEN'S COLLEGE HOSPITALTORONTO, ONTARIO, CANADA
MARC DESPATIS, MD, MSC, RVT, FRCSCCHIEF OF VASCULAR SURGERY AND TRANSPLANTATION
CENTRE HOSPITALIER DE SHERBROOKESHERBROOKE, QUEBEC, CANADA
JILL ALLEN, MCISC ,WOCN/ET, RNPROFESSIONAL SERVICES SPECIALIST
3M CANADA COMPANYLONDON, ONTARIO, CANADA

- 2 -
Leg ulceration is a common chronichealth condition often associated with aprolonged healing trajectory and fre-quent recurrence. It is estimated thatapproximately 1.5 to 3.0 per 1,000adults have active leg ulcers, and theprevalence continues to increase due toan aging population.1,2 In our recentregional survey of 1,331 individualsreceiving home care services, 21%were related to lower leg ulcerations.3
The disease burden of leg ulcers on thehealth care system and individuals issignificant. Many patients living withchronic leg ulcers experience dimin-ished quality of life, pain, psychosocialmaladjustment, limited work capacity,and physical disabil it ies.4,5 Whilechronic leg ulcers involve an array ofpathologies, venous disease is responsi-ble for up to 70% of all cases.6
What Causes Venous Leg Ulcers?In general, blood has to overcome
the force of gravity, especially whenthe person is in a standing position orsitt ing for extended per iods, andreturn to the heart through the venoussystem. To help venous blood flow, anumber of important physiologicalmechanisms have been identif iedincluding the calf muscle pump.7,8 Asthe calf muscle contracts and relaxes,the pressure rises and falls inside theblood vessels propelling the circulationto move upward. One-way valves in
the veins keep blood flowing in onedirection to avoid reflux. However,pooling of venous blood (venous stasis)can occur if the valves are damaged,the lymphatic system is obstructed, orthe calf muscle pump is ineffective dueto muscle wasting, immobility, or lim-ited ankle mobility.9,10 Increased pres-sure and capillary filtration lead toextravasation of blood particles intothe tissues that promote hemosiderin(ferritin and ferric iron from red bloodcells) deposits and hyperpigmentationof the skin. In addition, accumulationof neutrophils and breakdown of fibrintr igger an inflammatory response,increase microthrombus formation,and ultimately compromise local deliv-ery of oxygen (evidence B). Clinically,these changes are responsible forvenous eczema, lipodermatosclerosis(inflammation of the skin and fatty tis-sue causing woody changes of theskin), edema, and difficult to healulcers (Fig. 1).10 Strong evidence indi-cates that compression therapy is oneof the most effective strategies inreducing edema (evidence A).2
Is Leg Swelling Always Related toVenous Stasis?
Edema is an excess accumulation offluid in the interstitial compartment asfiltration of fluid out of the capillariesincreases or venous return decreases.Although swelling of the lowerextremities may be related to venousstasis, it is imperative to rule out othercauses of edema such as congestive
heart failure, hypoalbuminemia (indi-cating liver or kidney disease), deepvein thrombosis (DVT), or cellulitisdue to alterations in microvascularpressure, protein concentration, orbarrier permeability.10,11 Lymphedemadue to hyper tension that developswithin the lymphatic may also manifestas chronic edema. Lymphedema is ahigh-protein edema and is classified asprimary or secondary. Primary lym-phedema is caused by congenital dis-ease or intrinsic abnormality of thelymphatic collectors, vessels, or valvu-lar system. Secondary lymphedema iscaused by damage or obstruction of thelymphatic system by extrinsic factorssuch as: radiation, chronic or recurrentinfection, parasites, tumor obstruction,and long-standing venous disease.Edema involving lymphatic damage isusually associated with a positive Stem-mer sign, which is the inability topinch and lift a fold of skin at the baseof the second toe. (evidence B).12
DIFFERENTIAL DIAGNOSIS
More than 75% of leg ulcers areassociated with venous disease, butrecognition of wounds with multipleetiologies and atypical ulcers is pivotal.As the population ages the prevalenceof peripheral arterial disease is increas-ing. In a study by Callam et al. 10% ofpatients with leg ulcers had bothvenous disease and peripheral arterialdisease, and another 10% had onlyperipheral arterial disease.13
The delay in the diagnosis of arterialleg ulcers, may delay the proper refer-ral and management. The majority ofpatients with arterial leg ulcers do notmeet the criteria of chronic critical legischemia.13,14 Leg ulcers in peripheralarterial disease tend to be located atthe lateral or pretibial aspect of the legor on the dorsum of the foot. Theabsence or weakness of foot pulses andcold extremities are seen in mostinstances and wound pain is common.The group with ABPI less than 0.9 hasbeen categorized as mixed arteriove-nous disease while the group with nor-mal ABPI and involvement of oneang iosome are called ar ter ial legulcers.15 The early diagnosis of thesetwo groups is important because man-agement is different, and arterial legulcers with angiosomal involvement
#483 Woo G - 01
New Advances in Compression Therapy for Venous Leg UlcersWOO/ALAVI/EVANS/DESPATIS/ALLEN
INTRODUCTION
Figure 1. Venous insufficiency
DIFFERENTIAL DIAGNOSIS
afsaneh alavi
afsaneh alavi
More recent studies demonstrates the increase in the rate of lower extremitiy ulcers due to arterial disease up to 30% of lower extremity ulcers. ( ref :Spentzouris G, Labropoulos N)
afsaneh alavi
in 1985
- 3 -
#483 Woo G - 01
Wound HealingSURGICAL TECHNOLOGY INTERNATIONAL XXIII
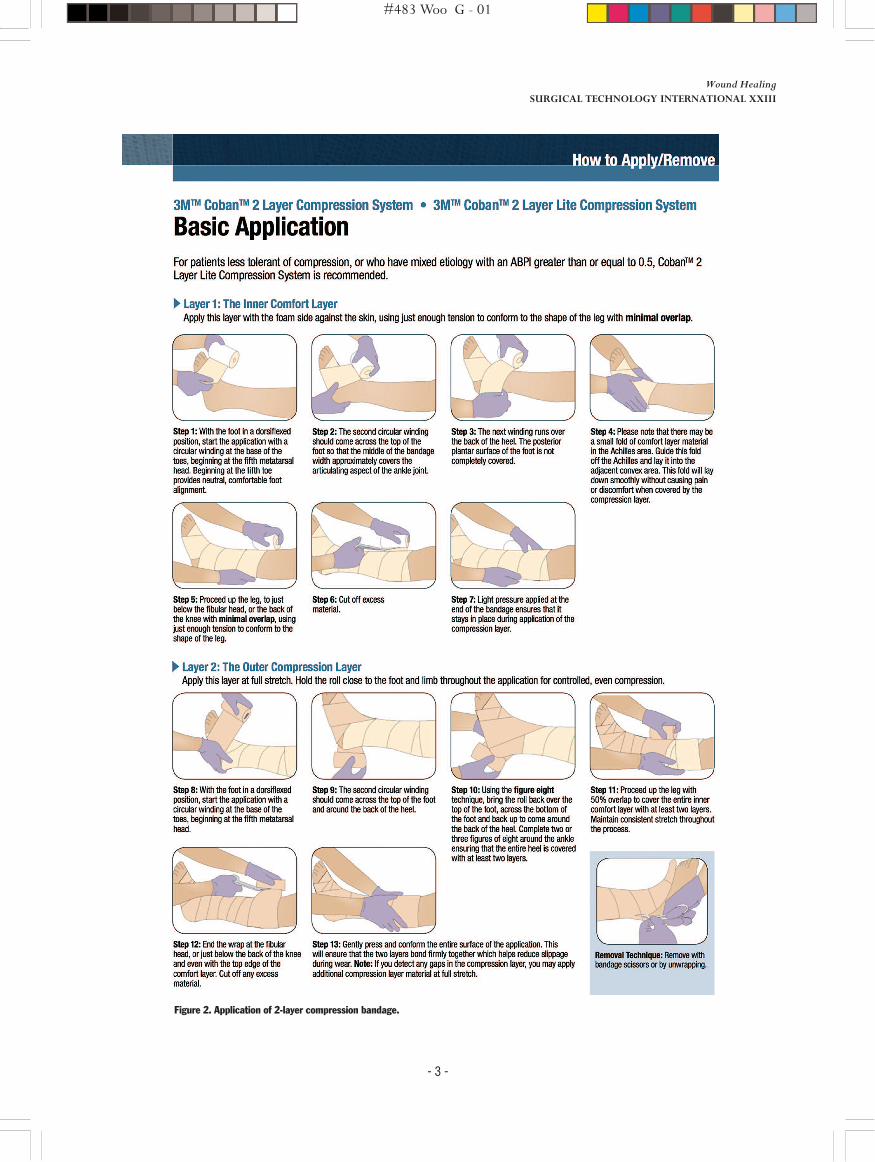
Figure 2. Application of 2-layer compression bandage.

- 4 -
are good candidates for interventionand revascularization.
Martorell ulcer or hypertensiveischemic leg ulcer (HYIL) has beencharacterized as a progressive andpainful ulcer with a violaceous bordercommonly at lateroposterior aspect ofthe leg or over Achilles ulcer. Allpatients have hypertension, and 50%have association with diabetes.16 Adeep punch biopsy demonstrates anarterial occlusion at the subcutaneouslevel.17
Malignant wounds are commonlyunder-diagnosed in the context of legulcers despite the significance of earlydetection in the patients’ outcome.Malignancy and wounds may resultfrom malignant transformation in achronic ulcer (Marjolin ulcer, usuallysquamous cell carcinoma) or may arisede novo or be a presentation of metasta-tic lesions.18 In a prospective study bySenet et al., 16 of 154 non-healing legulcers (10.4%) were associated withskin cancer.18
Ulcers may also present as a parane-oplastic symptom such as pyodermagangrenosum(PG). PG is a rare recur-ring and chronic painful disease withfour distinct clinical variants: ulcera-tive, bullous, pustular, and superficialgranulomatous (or vegetative).Although the cause of PG is unknownup to 45% to 75% of cases are associ-ated with systemic disease includinginflammatory bowel disease, myelo-proliferative disorders, and rheumatoidarthritis.19–22
The pyoderma gangrenosom ulcersusually have a purulent base and theircentrifugally extending borders areirregular, undermined, and overhang-ing, with a gunmetal color. The ulcerseventually heal with an atrophic, crib-riform, pigmented scar. The ulcersassociated with internal disease and theinfectious ulcers are also in the differ-ential diagnosis of leg ulcers as listed inTable I and need relevant work-ups.
COMPRESSION THERAPY
The mainstay of treatment forvenous leg ulcers is compression toreduce swelling of the legs and correctvenous congestion (evidence A). Theprinciple of compression therapy issimple involving the use of externalpressure, in the form of bandages or
wraps, to move the fluid from theinterstitial space back into the intravas-cular compar tment and preventreflux.11
Elastic or InelasticCompression bandages are classified
as either elastic (long stretch withmaximal extensibil ity >100%) orinelastic (short stretch with maximalextensibility <100%). Elastic bandagescontain elastomeric fibers.10–11 Theystretch allowing a sustained squeeze ofthe tissue as the bandages recoil backto their original length. In contrast,inelastic bandages form a rigid sleevethat resists the lateral expansion of thecalf muscle during active contractions.According to Pascal’s law in fluidmechanics, the compression bandageacts like a closed system wherebyexternal pressure applied to the limb istransmitted equally in all directionswithin the contained area.12 Inelasticbandages have the advantage of gener-ating high-pressure peaks mimickingnormal venous function. Changes inpressure (amplitudes) can also beachieved with turning and reposition-ing for patients in bed as the muscleswork against the r igid sleeve. Thelower resting pressure makes theinelastic bandages more tolerable andless likely to exacerbate pain with arte-r ial compromise than the elastictypes.11,12
Pressure produced by compressionbandages is dependent on the size ofthe limb, activities of the patient, andskill of the person applying the ban-dage system. There are a number oftechniques for applying compressionbandages. It is common practice toapply bandages in a spiral fashionaround the leg with a 50% overlapbetween turns producing a double-layer compression system (66% over-lapping will produce a triple layercompression system). Different appli-cation techniques such as a figure-of-eight bandage increase the number ofoverlapping layers at any one point andtherefore produce higher sub-bandagepressures.10–12
Single Component or MultipleComponents
Compression bandages come with asingle component or a combination ofmultiple components. Multicompo-nent bandages may consist of an initiallayer of orthopaedic wool padding, a
crepe layer, an elastic bandage, and anelastic cohesive bandage as the outerlayer. The interface pressure under thebandages increases with addition ofeach individual layer of compression,suggesting that multiple is superior tosingle-component compression. How-ever, emerging new evidence indicatesthat single component works just aswell in promoting healing of venousleg ulcers as multiple components (evi-dence A).23
Contraindications forCompression Therapy
Appropriate high-compression ther-apy should be initiated and used consis-tently so long as tissue perfusion isdeemed adequate. Pedal pulses can bepalpable in 17% to 20% of patientswith significant arterial disease, sug-gesting that the presence of pedal puls-es alone can be misleading andunreliable for the assessment of vascu-lar supply.24 Arterial brachial pressureindex (ABPI) is a practical alternativeto screen for arterial disease (evidenceB). To calculate ABPI, simply dividethe systolic blood pressure that isobtained at the ankle by the systolicblood pressure reading that is mea-sured at the brachial area. For a personwith an ABPI of 0.8 to 1.2 indicatingadequate vascular supply, high com-pression should always be considered.In patients with venous predominantdisease but co-existing arterial com-promise (ABPI between 0.5 and 0.8),compression therapy needs to be mod-ified to reduce the strength of com-pression. Recent studies indicate thatinelastic compression may enhancearterial circulation (increased toe pres-sure and transcutaneous oxygenation)and promote healing in people withmixed venous arterial leg ulcers (evi-dence B).25,26 However, inappropriatecompression bandaging can potentiallybe harmful leading to distal gangreneand limb loss in individuals with arteri-al predominant disease. For patientswith an ABPI of less than 0.5 indicat-ing severe arterial disease, compres-sion is contraindicated until acomprehensive vascular assessment iscompleted (evidence C).11,27
How to Apply Compression1. Venous stasis promotes accumu-
lation of inflammatory cells and theirmediators in the skin. With chronicinflammation, the skin becomes thick-
#483 Woo G - 01
New Advances in Compression Therapy for Venous Leg UlcersWOO/ALAVI/EVANS/DESPATIS/ALLEN
COMPRESSION THERAPY
- 5 -
#483 Woo G - 01
Wound HealingSURGICAL TECHNOLOGY INTERNATIONAL XXIII
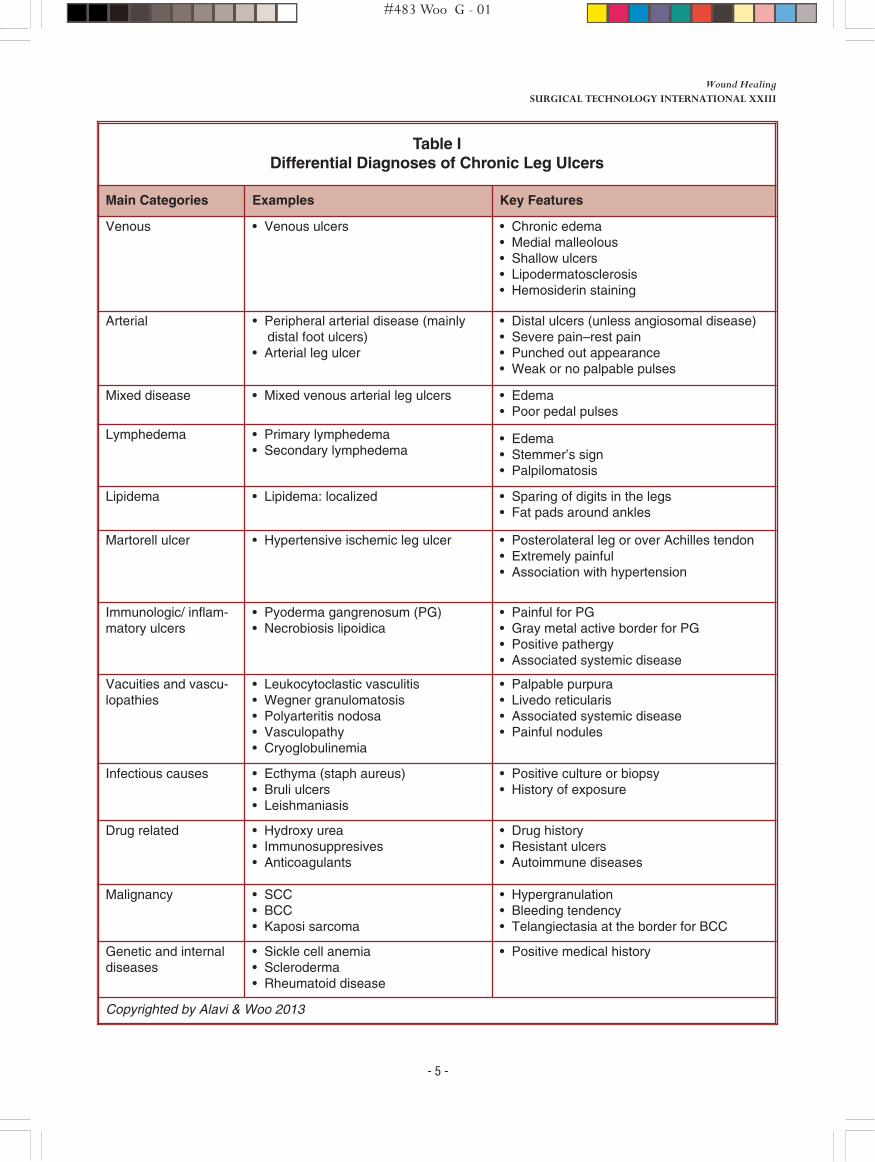
Table IDifferential Diagnoses of Chronic Leg Ulcers
Main Categories Examples Key Features
Venous • Venous ulcers • Chronic edema• Medial malleolous • Shallow ulcers• Lipodermatosclerosis• Hemosiderin staining
Arterial • Peripheral arterial disease (mainlydistal foot ulcers)
• Arterial leg ulcer
• Distal ulcers (unless angiosomal disease)• Severe pain–rest pain• Punched out appearance• Weak or no palpable pulses
Mixed disease • Mixed venous arterial leg ulcers • Edema• Poor pedal pulses
Lymphedema • Primary lymphedema• Secondary lymphedema
• Edema • Stemmer’s sign • Palpilomatosis
Lipidema • Lipidema: localized • Sparing of digits in the legs• Fat pads around ankles
Martorell ulcer • Hypertensive ischemic leg ulcer • Posterolateral leg or over Achilles tendon• Extremely painful• Association with hypertension
Immunologic/ inflam-matory ulcers
• Pyoderma gangrenosum (PG)• Necrobiosis lipoidica
• Painful for PG• Gray metal active border for PG• Positive pathergy• Associated systemic disease
Vacuities and vascu-lopathies
• Leukocytoclastic vasculitis• Wegner granulomatosis• Polyarteritis nodosa• Vasculopathy• Cryoglobulinemia
• Palpable purpura• Livedo reticularis• Associated systemic disease• Painful nodules
Infectious causes • Ecthyma (staph aureus)• Bruli ulcers• Leishmaniasis
• Positive culture or biopsy• History of exposure
Drug related • Hydroxy urea• Immunosuppresives• Anticoagulants
• Drug history• Resistant ulcers• Autoimmune diseases
Malignancy • SCC• BCC• Kaposi sarcoma
• Hypergranulation• Bleeding tendency• Telangiectasia at the border for BCC
Genetic and internaldiseases
• Sickle cell anemia• Scleroderma• Rheumatoid disease
• Positive medical history
Copyrighted by Alavi & Woo 2013

- 6 -
er and scaly, giving the surface of theskin a bumpy, cobblestone appearance.Before application of compression, theleg should be washed with warmwater and a pH-balanced skin cleanser.Moisturizers containing humectantsand skin conditioners should be usedfollowing cleansing to replenish skinmoisture. Products containing sensi-tizers such as fragrance and lanolinshould be avoided.
2. In the presence of an activeulcer, an appropriate dressing shouldbe selected to wick away excesswound exudate, but it must be able tokeep the wound base moist for heal-ing.
3. Most bandaging systems consistof a first layer of padding material toprotect bony prominences, t ibialcrest, and the Achilles tendon. It isimportant to remember that extrapadding can alter the sub-bandagepressure that is delivered. The firstlayer of padding is usually appliedfrom the base of the toes to the areajust below the knee in a spiral fashionwith some (or minimal) overlapping.
4. Dependent on the compressionsystem, application of the compressivelayer(s) should follow recommenda-tions from the manufacturer. Bandagesmay be applied in a spiral fashion with50 percent overlapping at each turn orin a f igure-of-eight technique toincrease the amount of compressiondelivered. Compression bandages maybe applied with full stretch or 50%stretch (again dependent on the manu-facturer’s recommendations).
5. Following the application, ensurethe compression system is not imped-ing ankle movement and ambulation.Education should be provided toempower patients to monitor for signsof poor perfusion such as numbness,tingling, discoloration, increased pain,or parathesia (e.g., sensation of tin-gling, pins and needles).28
6. Encourage chronic disease selfmanagement by emphasizing theimportance of “compression for life,”regular exercise that involves the calfmuscle to facilitate venous return, andmaintaining optimal body mass index.
Common Compression SystemsProfore (Smith & Nephew, London,
UK) is one of the most popular 4-layercompression systems that contains awound contact layer, natural paddingbandage, a light comformable ban-
dage; a compression bandage layer,and a cohesive bandage. As per manu-facturer’s instructions, after thewound contact layer is placed on thewound, the padding bandage(orthopaedic wool) is applied from thebase of the toes to the knee using asimple spiral technique and 50% over-lap. The purpose of the padding layeris to provide protection to vulnerableareas such as the Achilles tendon andpretibial crest. The next layer consistsof a light, conformable bandage (crepebandage) that is applied from the baseof the toes to the knee using a simplespiral technique and 50% overlap. Thethird layer is an elastic, extensible ban-dage that is applied from the base ofthe toes to the knee, using a figure-of-eight technique at 50% extension. Thelast layer of flexible cohesive bandageis applied from toe to knee using a spi-ral technique with 50% extension and50% overlap.
3M Coban 2 Layer CompressionSystems (3M, St. Paul, MN) provideshigh compression with 2 layers of ban-dages, and it is designed for patientswith an ABPI of 0.8mmHg and higher.For patients new to compression, lesstolerant of high compression, frail, orwith ABPIs of 0.5mmHg to0.8mmHg, the Coban 2 Layer LiteCompression System (3M St. Paul,MN) should be considered.
The following instructions are pro-vided by the manufacturer:
Layer 1: The inner comfort layer isa laminate of polyurethane foam andlatex-free cohesive material. The firstlayer is applied with the foam sideagainst the skin. It is applied withouttension. This provides a soft, comfort-able layer that mechanically grips theskin, minimizing slippage during wear.
Layer 2: The outer compressionlayer is a latex-free cohesive materialdesigned to provide shor t stretchcompression. It is designed to beapplied at full stretch to ensure consis-tency and take the guesswork out ofthe application process. Whenapplied, Layer 2 adheres to Layer 1,resulting in a comfortable, thin, low-profile compression sleeve that allowspatients to move their ankles and wearmost normal shoes.
Preventing Recurrent UlcersPeople with venous disease require
lifelong maintenance compressiontherapy (evidence C). The key mes-sage that needs to be emphasized is:compression is for life. However, non-adherence with long-term use of com-pression is as high as 37% to 67% for anumber of reasons such as high cost,pain, heat accumulation, and inconve-nience.29 The recurrence rate ofvenous leg ulcers is a serious concernestimated at 26% after one year ofcomplete closure.30 Wound care mod-els based on interprofessional collabo-ration and peer-led support groups toprovide education and psychosocialsupport have demonstrated improvedpatient outcomes.31 There is a need toestablish a coordinated approach toassess, treat, and monitor outcomes oflower extremity leg ulcers.
Medical Management of VenousLeg Ulcers
The mainstay of treatment ofvenous leg ulcers is to reduce thepressure in the venous system throughthe use of compression systems. Thereare 2 medications that have been usedin the treatment of venous leg ulcers:pentoxifylline and micronized purifiedflavonoids.
Pentoxifylline is a xanthine deriva-tive that reduces blood viscosity andincreases the flexibility of the erythro-cytes.32 It also has been shown to be aninhibitor of prostaglandin E andreduce levels of elastase.33 Pentoxi-fylline has been validated to be effec-t ive when used together withcompression to improve the healing ofvenous leg ulcer s.34 A Cochranereview evaluated 11 clinical trials toconclude that pentoxifylline resultedin a 21% overall increase in healing.The most common side effect withpentoxifylline is gastrointestional dis-turbance.34
Flavanoids are a large family ofcompounds synthesized by plants thatappear in certain foods such as cocoa,chocolate, teas, and red wines. Theyhave been used in the form ofmicronized purified protein fractionto promote healing in venous legulcers. A recent Cochrane reviewindicates there is some evidence tosuggest flavonoids may have some ben-ef it; however, it was not strongenough to suggest use in clinical prac-tice.35
As par t of the assessment of avenous ulcer it is important to exam-
#483 Woo G - 01
New Advances in Compression Therapy for Venous Leg UlcersWOO/ALAVI/EVANS/DESPATIS/ALLEN

- 7 -
ine for infection and inflammation.Diagnosis of infection in a chronicwound can be challenging. Infectionshould be classified as either critical col-onization (sometimes referred to asbioburden) or deep infection. It is theamount of tissue destruction and hostresponse that differentiates the two.Critical colonization can be treated withdressings with antimicrobial propertieswhile deeper infection would requireoral or intravenous antibiotics.
An ulcer stuck in the inflammatoryphase is unlikely to heal. It is believedthat it is the imbalance in the metalmet-alloproteases (MMP) and elastase andthe inhibitors of the MMP that result infailure of the ulcer to progress towardhealing. Elevation of the MMPs result inuncontrolled proteolysis with thedestruction of many of the growth fac-tors necessary for healthy wound heal-ing.36 There are dressings that can trapthe MMPs in the form of oxidizedregenerated collagen and cellulose.
To optimize healing of a venous legulcer requires the careful assessment ofthe patient’s underlying medical condi-tions and person-centered issues. Opti-mal management of venous leg ulcerwould involve debridement to removedevitalized tissue, treatment of infec-tion/inflammation, and the possibleuse of medication such as pentoxy-fylline together with compression.
CONCLUSION
Leg ulcers are common involving anumber of causative factors. Managingchronic edema using compression iscrucial to promote healing of venous legulcers. The principle of compressiontherapy is simple, involving the use ofexternal pressure in the forms of ban-dages or wraps to move the fluid fromthe interstitial space back into theintravascular compartment and preventreflux. Clinicians must also considerpotential medical therapies to promotewound healing and to prevent recur-rence.
AUTHORS’ DISCLOSURES
Dr. Woo received a project grantfrom 3M Canada. Ms. Allen isemployed by 3M Canada. The other
authors have no financial relationshipsto report.
REFERENCES
1. Takahashi PY, Chandra A, Cha SS, et al.A predictive model for venous ulceration inolder adults: results of a retrospectivecohort study. Ostomy Wound Manage2010; 56(4):60–6.2. O’Meara S, Cullum NA, Nelson EA.Compression for venous leg ulcers.Cochrane Database Syst Rev 2009;1(2):50.3. Woo KY, Sibbald RG. Prevalence ofchronic wounds in a regional community-based survey. Poster presentation at Canadi-an Association of Wound Care Conference,Calgary, 2008.4. Abbade LP, Lastória S, Rollo Hde A.Venous ulcer: clinical characteristics and riskfactors. Int J Dermatol 2011;50(4):405–11.5. Neglen P. Writing Group II of the PacificVascular Symposium 6, Eklöf B, Kulwicki A,Davies A, et al. Prevention and treatment ofvenous ulcers in primary chronic venousinsufficiency. J Vasc Surg 2010;52(5 Suppl):15S–20S.6. Labropoulos N, Wang ED, Lanier ST, etal. Factors associated with poor healing andrecurrence of venous ulceration. PlastReconstr Surg 2012;129(1):179–86.7. Kolluri R. Compression therapy fortreatment of venous disease and l imbswelling. Curr Treat Options CardiovascMed 2011; 13(2):169–78.8. van den Boezem PB, Klem TM, le Cocqd’Armandville E, et al. The management ofsuperficial venous incompetence. BMJ2011;343(7818):308–11.9. Gaweesh AS. Impeded venous drainage:novel view of chronic venous disease patho-physiology. Med Hypotheses 2009;73(4):548–52.10.Mosti G. Compression and venoussurgery for venous leg ulcers. Clin PlastSurg 2012;39(3):269–80.11.Mosti G, Mattaliano V, Polignano R, etal. Compression therapy in the treatment ofleg ulcers. Acta Vulnologica 2009;7(3):1–20.12.Glover D. Compression therapy: a posi-tion document on compression bandaging.The International Lymphoedema Frameworkin association with the World Alliance forWound and Lymphoedema Care.Imprimerie Reboul, Saint-Etienne France2012.13. Callam MJ, Harper DR, Dale JJ , et al.Arterial disease in chronic leg ulceration: anunderestimated hazard? Lothian and ForthValley leg ulcer study. Br Med J (Clin ResEd) 1987;294(6577):929–31. 14. Second European Consensus Documenton chronic critical leg ischemia. Circulation1991;8494(Suppl):IV1–26.
15.Hafner J, Schaad I, Schneider E, et al.Leg ulcers in peripheral arterial disease(arterial leg ulcers): impaired wound healingabove the threshold of chronic critical limbischemia. J Am Acad Dermatol 2000;43(6):1001–8.16. Hafner J, Nobbe S, Partsch H, et al.Martorell hypertensive ischemic leg ulcer: amodel of ischemic subcutaneous arteri-olosclerosis. Arch Dermatol 2010;146(9):961–8.17.Alavi A, Mayer D, Hafner J, et al. Mar-torell hypertensive ischemic leg ulcer: Anunderdiagnosed entity(c). Adv Skin WoundCare 2012;25(12):563–72.18. Senet P, Combemale P, Debure C, et al.Angio-Dermatology Group of the FrenchSociety of Dermatology. Malignancy andchronic leg ulcers: the value of systematicwound biopsies: a prospective, multicenter,cross-sectional study. Arch Dermatol2012;148(6):704–8.19. Setterfield JF, Shirlaw PJ, ChallacombeSJ, et al. Pyoderma gangrenosum associatedwith severe oropharyngeal involvement andIgA paraproteinaemia. Br J Dermatol2001;144(2):393–6.20. Ahronowitz I, Harp J, Shinkai K. Etiolo-gy and management of pyoderma gangreno-sum: a comprehensive review. Am J ClinDermatol 2012;13(3):191–211.21. Marzano AV, Ishak RS, Saibeni S, et al.Autoinflammatory skin disorders in inflam-matory bowel diseases, pyoderma gangreno-sum and sweet’s syndrome: a comprehensivereview and disease classification criteria.Clin Rev Allergy Immunol 2013.22.Davatchi F, Shahram F, Chams-DavatchiC, et al. Behcet’s disease in Iran: analysis of6500 cases. Int J Rheum Dis 2010;13(4):367–73.23.Harrison MB, Vandenkerkh EG, HopmanWM, et al. The Canadian Bandaging TrialGroup. The Canadian Bandaging Trial: Evi-dence-informed leg ulcer care and the effec-tiveness of two compression technologies.BMC Nurs 2011;10(1):20.24.Sibbald RG, Goodman L, Woo KY, et al.Special considerations in wound bed prepa-ration 2011: an update. Adv Skin WoundCare 2011;24(9):415–3.25.Top S, Arveschoug AK, Fogh K. Doshort-stretch bandages affect distal bloodpressure in patients with mixed etiology legulcers? J Wound Care 2009;18(10):439–42. 26.Mosti, G, Iabichella ML, Partsch H.Compression therapy in mixed ulcersincreases venous output and arterial perfu-sion. J Vasc Surg 2012;55:122–8.27.Stout N, Partsch H, Szolnoky G, et al.Chronic edema of the lower extremities:international consensus recommendationsfor compression therapy clinical research tri-als. Int Angiol 2012;31(4):316–29.28.Hopkins A. How to apply effective mul-tilayer compression bandaging. WoundEssentials 2006:38–42.29.Labropoulos N, Wang ED, Lanier ST, et
#483 Woo G - 01
Wound HealingSURGICAL TECHNOLOGY INTERNATIONAL XXIII
CONCLUSION
REFERENCES
AUTHORS’ DISCLOSURES
STI

- 8 -
al. Factors associated with poor healing andrecurrence of venous ulceration. PlastReconstr Surg 2012;129(1):179–86.30.Reich-Schupke S, Murmann F, AltmeyerP, et al. Quality of life and patients’ view ofcompression therapy. Int Angiol 2009;28(5):385–93.31.Nelson EA, Bell-Syer SE. Compressionfor preventing recurrence of venous ulcers.Cochrane Database Syst Rev 2012;(8).
32. Jull A, Waters J, Arroll B. Pentoxi-fylline for treatment of venous leg ulcers. Asystematic review. Lancet 2002;359:1550–54.33. Liu Y, Margolis DJ, Isseroff R. Doesinflammation have a role in the pathogenesisof venous ulcers? A critical review of theevidence. J Investigative Dermatology 2011;131:818–27.34. Jull AB, Arroll B, Walters J. Pentoxi-
fyl l ine for treating venous leg ulcers.Cochrane Database of Systemic Reviews2011;(1).35. Scallon C, Bell-Seyer SEM, Aziz Z.Flavonoids for treating venous leg ulcers.Cochrane Database of Systemic Reviews2013;(5).36. Raffetto J, Marston WA. Venous ulcer:What is new? Plast Reconstr Surg 2011;127:279S–288S.
#483 Woo G - 01
New Advances in Compression Therapy for Venous Leg UlcersWOO/ALAVI/EVANS/DESPATIS/ALLEN
Related Documents











