This article was downloaded by: [24.10.222.254] On: 30 September 2014, At: 13:52 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Clinical and Experimental Neuropsychology Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/ncen20 Neuropsychological investigation of motor impairments in autism Tyler C. Duffield a , Haley G. Trontel b , Erin D. Bigler acde , Alyson Froehlich f , Molly B. Prigge fg , Brittany Travers h , Ryan R. Green a , Annahir N. Cariello f , Jason Cooperrider fg , Jared Nielsen fg , Andrew Alexander hij , Jeffrey Anderson k , P. Thomas Fletcher el , Nicholas Lange mn , Brandon Zielinski ho & Janet Lainhart ij a Department of Psychology, Brigham Young University, Provo, UT, USA b Department of Psychology, University of Montana, Missoula, MT, USA c Neuroscience Center, Brigham Young University, Provo, UT, USA d Department of Psychiatry, University of Utah, Salt Lake City, UT, USA e The Brain Institute of Utah, University of Utah, Salt Lake City, UT, USA f Department of Psychiatry, School of Medicine, University of Utah, Salt Lake City, UT, USA g Interdepartmental Neuroscience Program, University of Utah, Salt Lake City, UT, USA h Department of Medical Physics, University of Wisconsin, Madison, WI, USA i Waisman Laboratory for Brain Imaging and Behavior, University of Wisconsin, Madison, WI, USA j Department of Psychiatry, University of Wisconsin, Madison, WI, USA k Department of Radiology, University of Utah, Salt Lake City, UT, USA l School of Computing, University of Utah, Salt Lake City, UT, USA m Departments of Psychiatry and Biostatistics, Harvard University, Boston, MA, USA n Neurostatistics Laboratory, McLean Hospital, Belmont, MA, USA o Department of Pediatrics and Neurology, School of Medicine, University of Utah, Salt Lake City, UT, USA Published online: 28 Aug 2013. To cite this article: Tyler C. Duffield, Haley G. Trontel, Erin D. Bigler, Alyson Froehlich, Molly B. Prigge, Brittany Travers, Ryan R. Green, Annahir N. Cariello, Jason Cooperrider, Jared Nielsen, Andrew Alexander, Jeffrey Anderson, P. Thomas Fletcher, Nicholas Lange, Brandon Zielinski & Janet Lainhart (2013) Neuropsychological investigation of motor impairments in autism, Journal of Clinical and Experimental Neuropsychology, 35:8, 867-881, DOI: 10.1080/13803395.2013.827156 To link to this article: http://dx.doi.org/10.1080/13803395.2013.827156 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

This article was downloaded by: [24.10.222.254]On: 30 September 2014, At: 13:52Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Clinical and ExperimentalNeuropsychologyPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/ncen20
Neuropsychological investigation of motorimpairments in autismTyler C. Duffielda, Haley G. Trontelb, Erin D. Bigleracde, Alyson Froehlichf,Molly B. Priggefg, Brittany Traversh, Ryan R. Greena, Annahir N. Cariellof, JasonCooperriderfg, Jared Nielsenfg, Andrew Alexanderhij, Jeffrey Andersonk, P. ThomasFletcherel, Nicholas Langemn, Brandon Zielinskiho & Janet Lainhartij
a Department of Psychology, Brigham Young University, Provo, UT, USAb Department of Psychology, University of Montana, Missoula, MT, USAc Neuroscience Center, Brigham Young University, Provo, UT, USAd Department of Psychiatry, University of Utah, Salt Lake City, UT, USAe The Brain Institute of Utah, University of Utah, Salt Lake City, UT, USAf Department of Psychiatry, School of Medicine, University of Utah, Salt Lake City,UT, USAg Interdepartmental Neuroscience Program, University of Utah, Salt Lake City, UT,USAh Department of Medical Physics, University of Wisconsin, Madison, WI, USAi Waisman Laboratory for Brain Imaging and Behavior, University of Wisconsin,Madison, WI, USAj Department of Psychiatry, University of Wisconsin, Madison, WI, USAk Department of Radiology, University of Utah, Salt Lake City, UT, USAl School of Computing, University of Utah, Salt Lake City, UT, USAm Departments of Psychiatry and Biostatistics, Harvard University, Boston, MA, USAn Neurostatistics Laboratory, McLean Hospital, Belmont, MA, USAo Department of Pediatrics and Neurology, School of Medicine, University of Utah,Salt Lake City, UT, USAPublished online: 28 Aug 2013.
To cite this article: Tyler C. Duffield, Haley G. Trontel, Erin D. Bigler, Alyson Froehlich, Molly B. Prigge, BrittanyTravers, Ryan R. Green, Annahir N. Cariello, Jason Cooperrider, Jared Nielsen, Andrew Alexander, Jeffrey Anderson,P. Thomas Fletcher, Nicholas Lange, Brandon Zielinski & Janet Lainhart (2013) Neuropsychological investigationof motor impairments in autism, Journal of Clinical and Experimental Neuropsychology, 35:8, 867-881, DOI:10.1080/13803395.2013.827156
To link to this article: http://dx.doi.org/10.1080/13803395.2013.827156
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”)contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors

make no representations or warranties whatsoever as to the accuracy, completeness, or suitabilityfor any purpose of the Content. Any opinions and views expressed in this publication are the opinionsand views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy ofthe Content should not be relied upon and should be independently verified with primary sources ofinformation. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands,costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial orsystematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distributionin any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found athttp://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
Journal of Clinical and Experimental Neuropsychology, 2013
Vol. 35, No. 8, 867–881, http://dx.doi.org/10.1080/13803395.2013.827156
Neuropsychological investigation of motor impairmentsin autism
Tyler C. Duffield1, Haley G. Trontel2, Erin D. Bigler1,3,4,5 , Alyson Froehlich6,Molly B. Prigge6,7, Brittany Travers8, Ryan R. Green1, Annahir N. Cariello6,Jason Cooperrider6,7, Jared Nielsen6,7, Andrew Alexander8,9,10, Jeffrey Anderson11,P. Thomas Fletcher5,12, Nicholas Lange13,14, Brandon Zielinski8,15, and Janet Lainhart9,10
1Department of Psychology, Brigham Young University, Provo, UT, USA2Department of Psychology, University of Montana, Missoula, MT, USA3Neuroscience Center, Brigham Young University, Provo, UT, USA4Department of Psychiatry, University of Utah, Salt Lake City, UT, USA5The Brain Institute of Utah, University of Utah, Salt Lake City, UT, USA6Department of Psychiatry, School of Medicine, University of Utah, Salt Lake City, UT, USA7Interdepartmental Neuroscience Program, University of Utah, Salt Lake City, UT, USA8Department of Medical Physics, University of Wisconsin, Madison, WI, USA9Waisman Laboratory for Brain Imaging and Behavior, University of Wisconsin, Madison, WI, USA10Department of Psychiatry, University of Wisconsin, Madison, WI, USA11Department of Radiology, University of Utah, Salt Lake City, UT, USA12School of Computing, University of Utah, Salt Lake City, UT, USA13Departments of Psychiatry and Biostatistics, Harvard University, Boston, MA, USA14Neurostatistics Laboratory, McLean Hospital, Belmont, MA, USA15Department of Pediatrics and Neurology, School of Medicine, University of Utah, Salt Lake City,UT, USA
(Received 8 March 2013; accepted 9 July 2013)
It is unclear how standardized neuropsychological measures of motor function relate to brain volumes of motorregions in autism spectrum disorder (ASD). An all-male sample composed of 59 ASD and 30 controls (ages5–33 years) completed three measures of motor function: strength of grip (SOG), finger tapping test (FTT), andgrooved pegboard test (GPT). Likewise, all participants underwent magnetic resonance imaging with region ofinterest (ROI) volumes obtained to include the following regions: motor cortex (precentral gyrus), somatosensorycortex (postcentral gyrus), thalamus, basal ganglia, cerebellum, and caudal middle frontal gyrus. These traditionalneuropsychological measures of motor function are assumed to differ in motor complexity, with GPT requiringthe most followed by FTT and SOG. Performance by ASD participants on the GPT and FTT differed significantlyfrom that of controls, with the largest effect size differences observed on the more complex GPT task. Differences
The project described was supported by Grants RO1 MH080826 (J.E.L., E.D.B., A.L.A., N.L.), RO1 MH084795 (J.E.L., P.T.F.,N.L.), and KO8 MH092697 (J.S.A.) from the National Institute of Mental Health; Grants T32 HD07489 (B.T.) and P30 HD003352-45 (Waisman Center Core Grant) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development(NICHD), The Hartwell Foundation (B.T.), and the Primary Children’s Foundation Early Career Development Award (B.Z.). Supportfrom the Poelman Foundation to Brigham Young University for autism research is gratefully acknowledged. The authors report noconflicts of interest. The content is solely the responsibility of the authors and does not necessarily represent the official views of theNational Institute of Mental Health, the National Institute of Child Health and Development, or the National Institutes of Health.We thank former members of the Utah Autism Creative Programs of Excellence in Autism (CPEA) for their assistance during the earlystages of this project. We sincerely thank the children, adolescents, and adults with autism and the individuals with typical developmentwho participated in this study and their families. The assistance of Tracy J. Abildskov with image analysis and Jo Ann Petrie withmanuscript preparation is gratefully acknowledged.
Address correspondence to: Erin D. Bigler, Department of Psychology & Neuroscience Center, 1001 SWKT, Brigham YoungUniversity, Provo, UT 84602, USA (E-mail: [email protected]).
© 2013 Taylor & Francis
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014

868 DUFFIELD ET AL.
on the SOG task between the two groups were nonsignificant. Since more complex motor tasks tap more complexnetworks, poorer GPT performance by those with ASD may reflect less efficient motor networks. There was nogross pathology observed in classic motor areas of the brain in ASD, as ROI volumes did not differ, but FTT wasnegatively related to motor cortex volume in ASD. The results suggest a hierarchical motor disruption in ASD,with difficulties evident only in more complex tasks as well as a potential anomalous size–function relation inmotor cortex in ASD.
Keywords: Autism; Network disruption; Motor impairment; Brain volume differences; Motor cortex volume.
Although Kanner’s (1943) classic paper out-lined the core features of autism that eventu-ally became the triad criteria for the diagnosis ofautism—qualitative impairments in social interac-tion, communication, and repetitive and stereo-typed behaviors—he also noted, “several of thechildren were somewhat clumsy in gait and grossmotor performance . . . ” (p. 248). While mostcontemporary studies of autism spectrum disor-der (ASD) have focused on the core diagnos-tic features of autism (Geschwind, 2009), clini-cally described delays in motor development andimpairments in motor function are commonplacein ASD where meta-analytic findings have sug-gested a more central role (Fournier, Hass, Naik,Lodha, & Cauraugh, 2010), described by some asa motor coordination deficit in ASD (Miyahara,2013). While these reviews have shown motor differ-ences between typically developing (TD) and ASDindividuals, most individuals with ASD do not meetcriteria for a developmental coordination disor-der (Emck, Bosscher, Beek, & Doreleijers, 2009).While individuals with ASD may exhibit motorfindings, as reviewed by Fournier et al. (2010),Miyahara (2013), and Emck et al. (2009), there isconsiderable variability in how motor impairmentshave been assessed in these studies, many of whichhave been based on simple clinical rating scalesand not traditional neuropsychological measuresof motor functioning like strength of grip (SOG),the finger tapping test (FTT), or grooved pegboardtest (GPT; see Lezak, Howieson, Bigler, & Tranel,2012).
Studies that have used some of these traditionalneuropsychological measures of motor functionhave found impairments in those with ASD whengroup compared to TD individuals (see T. Muller,Schafer, Kuhn, & Przuntek, 2000; Pedersen, Oberg,Larsson, & Lindval, 1997; Sachdev, Hume, Toohey,& Doutney, 1996); however, other studies havereported either mixed findings or an absence of anymotor difference (Hardan, Kilpatrick, Keshavan, &Minshew, 2003; Jansiewicz et al., 2006; Kern et al.,2011; Minshew, Goldstein, & Siegel, 1997; Rumsey& Hamburger, 1988; Szatmari, Tuff, Finlayson,& Bartolucci, 1990; Weimer, Schatz, Lincoln,
Ballantyne, & Trauner, 2001; Williams, Goldstein,& Minshew, 2006).
The lack of consistent motor findings in ASDacross studies, including the aforementioned stud-ies that did use standardized neuropsychologicalmeasures, likely relates to: design and methodolog-ical differences across studies; the level of motorcomplexity being assessed; the clinical heterogene-ity of autism samples; utilization of a single motortask versus multiple measures; the use of non-standardized versus standardized measures; differ-ences in sample sizes; differences in age ranges(i.e., childhood, adolescence, adulthood, lifespan);and differences in how autism severity is associatedwith cognitive factors (see Carcani-Rathwell, Rabe-Hasketh, & Santosh, 2006) since as Goldman andcolleagues (2009) observed, lower cognitive abil-ity was associated with greater motor impairment.Furthermore, given the heterogeneity of autism andits expression (Rapin, 1991), a universal motorimpairment would not necessarily be expected.
Unfortunately, some of these limitations areinescapable given the nature and constraints ofresearch with this clinical population. Yet, whatis clear from the literature is that motor deficitsin some fashion likely are associated with andrelated to ASD (Bhat, Landa, & Galloway, 2011;Bonnet & Gao, 1996; Downey & Rapport, 2012;Dziuk et al., 2007; Emck, Bosscher, van Wieringen,Doreleijers, & Beek, 2012; Fournier et al., 2010;Gowen & Hamilton, 2012; Jansiewicz et al., 2006;Landa, Gross, Stuart, & Bauman, 2012; Miyahara,2013; Nobile et al., 2011; Travers, Powell, Klinger,& Klinger, 2012). If so, it is important to charac-terize motor performance in ASD using standard-ized neuropsychological measures like SOG, FTT,and GPT.
While these standardized motor tasks representthe behavioral output related to motor function,they also reflect integrity of known motor regionsof the brain such as primary motor cortex and othercortical and subcortical regions that support motorfunction (Lezak et al., 2012). What has not beensystematically investigated in ASD, or even in TDindividuals, is how anatomical indices of knownmotor regions relate to motor control. Using
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
MOTOR IMPAIRMENTS AND STRUCTURAL IMAGING IN AUTISM 869
contemporary neuroimaging methods to calculateregion of interest (ROI) volume of key brain areasinvolved in motor function provides an anatomicalmetric about motor system integrity (see Draganski& Bhatia, 2010; Hervé, Mazoyer, Crivello, Perchey,& Tzourio-Mazoyer, 2005). However, few studieshave been systematic in the application of tradi-tional neuropsychological measures of motor func-tioning in examining motor areas in ASD, let aloneneuroimaging findings (Mostofsky et al., 2009;Qiu, Adler, Crocetti, Miller, & Mostofsky, 2010).Furthermore because of the distributed anomaliesthat may be present in neuroimaging findings asso-ciated with ASD, it is important when ROI anatom-ical studies are performed that multiple regions beexamined rather than one or just a few (Frith,2003; Zielinski et al., 2012). Also, a variety ofissues relate to morphological differences in thedeveloping ASD brain where altered developmentaltrajectories may result in different volumes depend-ing on age (Courchesne, Carper, & Akshoomoff,2003; Courchesne & Pierce, 2005). Disruption ofearly brain development, even if ROI eventuallynormalizes in volume with age, has the potential tosignificantly influence circuitry and resultant func-tion (Polsek, Jagatic, Cepanec, Hof, & Simic, 2011).Regardless of these developmental factors, assess-ing ROI volumes of key brain areas is an establishedquantitative method used as a marker of neuralintegrity (Jara, 2013; Tofts, 2003).
Given the need for characterization of ASDmotor performance in comparison TD individu-als on standardized neuropsychological tests andwhether ROI differences in the volumes of clas-sic motor areas are observed in ASD, the currentinvestigation had three aims: (a) to describe motorfunction based on traditional neuropsychologicalSOG, FTT, and GPT measures in a large sam-ple of individuals with ASD spanning child toadulthood, (b) to compare neuroimaging-derivedvolumes of classic motor ROIs between ASD andtypically developing participants, and (c) to explorewhether same or different relationships betweenneuroimaging identified motor ROIs were observedin ASD participants and TD controls (TDCs).ROI volumes were derived from the automatedFreeSurfer method, to include primary motor andsensory cortices, premotor regions of the frontalcortex, basal ganglia (caudate, globus pallidus, andputamen combined), thalamus, and cerebellum.
The GPT involves motor dexterity, visual pro-cessing, speed, attention, and continuous moni-toring of accuracy, whereas FTT predominatelymeasures simple motor coordination and dexterity,and SOG essentially measures only upper extrem-ity muscle strength (Lezak et al., 2012; Strauss,
Sherman, & Spreen, 2006). Based in part on whatand how these measures assess motor function, ahierarchy of motor control may be inferred. GPTperformance reflects a more cognitively demandingtask that would require a greater level of multi-ple and integrated motor regions than FTT, andFTT requires greater motor complexity than SOGto carry out the task (Haaland & Delaney, 1981).Indeed, evidence for a motor hierarchical modelis provided by factor-analytic findings suggestingthat FTT and pegboard type tasks measure inde-pendent dimensions of manual proficiency (Baser &Ruff, 1987; Stanford & Barratt, 1996). Nonetheless,all of these motor tasks exhibit some degree ofassociation (Schear & Sato, 1989; Strauss et al.,2006), suggesting a common neural substrate likelyinvolving the corticospinal system and associatedmotor pathways (Triggs, Calvanio, Levine, Heaton,& Heilman, 2000).
From this hierarchical perspective of motor con-trol, with increased motor system complexity nec-essary to perform the task, if ASD is associatedwith deficits in neural connectivity (Geschwind,2009) then the greatest likelihood for motor dif-ferences between ASD and TD groups would bewith the GPT and FTT tasks, with the least likeli-hood for differences in SOG. We hypothesized thatparticipants with ASD would exhibit lower motorperformance than TD participants, in particularwith the FTT and GPT measures, and that cor-relates of motor functioning and neuroanatomicalROIs would differ between the two groups.
METHOD
Subjects and assessment
Ascertainment
Participants diagnosed with autism and controlsubjects were a subset from the first wave of datacollection of a longitudinal investigation of braindevelopment. Participant selection from the largersample was based on having complete motor dataand Time Point 1 magnetic resonance imaging(MRI) performed in proximity to motor testing.Details of subject ascertainment are outlined inAlexander et al. (2007). All facets of this investiga-tion were undertaken with the understanding andwritten consent of each subject or legal guardian,with the approval of the University of Utah andBrigham Young University Institutional ReviewBoards, where testing was performed, and in com-pliance with national legislation and the Code ofEthical Principles for Medical Research InvolvingHuman Subjects of the World Medical Association.
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
870 DUFFIELD ET AL.
Subject groups
All subjects were male, ages 5–33 years. Allsubjects had a nonverbal standard IQ scoregreater than 65 on formal psychometric assess-ment using the Differential Ability Scales (Elliot,1990), Wechsler Intelligence Scale for Children–III (Wechsler, 1991), Wechsler Adult Intelli-gence Scale–III (Wechsler, 1997), or WechslerAbbreviated Scales of Intelligence (Wechsler, 1999).Fifty-nine participants formed the ASD group with30 participants in the TDC group. Since this wasa longitudinal project, for subjects with multipletest dates, neuropsychological data were taken onthe date closest to the neuroimaging test date andfirst test administration. Subject demographics arepresented in Table 1.
Autism spectrum disorder (ASD)
All cases of autism were idiopathic with allmeeting ASD criteria as described. Autism was
diagnosed based on the findings of the AutismDiagnostic Interview–Revised (ADI–R), a semi-structured, investigator-based interview with goodreliability and validity (Lord et al., 2000) as wellas directly assessed with the Autism DiagnosticObservation Schedule–Generic (ADOS–G), a semi-structured play and interview session designedto elicit social, communication, and stereotypedrepetitive behaviors characteristic of autism (Lordet al., 2000). ADI–R and ADOS–G descriptiveinformation is presented in Table 2. Where multi-ple administrations of these measures were avail-able, since most of the participants were partof a longitudinal investigation, the administrationon the date closest to the motor test admin-istration was used. Diagnostic classification wasbased on available ADI–R and ADOS–G find-ings along with Diagnostic and Statistical Manualof Mental Disorders–IV (DSM–IV ; AmericanPsychiatric Association, 1994) criteria, with the fol-lowing breakdown: lifetime diagnosis autistic dis-order of 52 and pervasive developmental disorder,
TABLE 1Demographic information
ASD (n = 59) Typically developing (n = 30)
Characteristic Mean SD Range Mean SD Range t p
Age in years 15.61 7.48 5.00–33.17 15.29 6.48 5.17–26.17 0.20 .84Head circumference (cm) 55.54 2.36 50.60–60.20 55.40 2.30 49.20–59.30 0.27 .79Handedness inventory 61.89 52.24 −100.00–100.00 69.90 42.98 −80.00–100.00 −0.72 .47Wechsler FIQ 100.30 17.71 58.00–137.00 120.23 16.72 95.00–153.00 −5.09∗∗ .00Wechsler PIQ 101.38 17.01 64.00–129.00 118.03 19.02 88.00–155.00 −4.15∗∗ .00Wechsler VIQ 98.54 21.34 51.00–138.00 117.57 14.83 94.00–151.00 −4.79∗∗ .00
Notes. Edinburgh Handedness inventory on a scale from –100 (left-handed) to 100 (right-handed). FIQ = Full Scale IQ; PIQ =Performance IQ; VIQ = Verbal IQ.∗∗p < .01.
TABLE 2Characterization of the autism and control sample
ASD Typically developing
Test n Mean (SD) Range n Mean (SD) Range
ADOS S+C: Module 1 1 17.00 (0) 0 0ADOS S+C: Module 2 5 17.20 (4.15) 12–23 1 0 (0) 0ADOS S+C: Module 3 22 14.77 (3.62) 7–21 11 1.55 (1.44) 0–4ADOS S+C: Module 4 31 12.32 (3.90) 1–20 16 0.75 (1.00) 0–3ADI–R Soc 51 20.11 (5.71) 6–30 0ADI–R Com 51 15.65 (4.64) 7–25 0ADI–R RSB 51 7.02 (2.36) 2–12 0
Notes. ADOS S+C = Autism Diagnostic Observation Schedule: Social and Communication Total. The ADOS consists of four modules,and the individual being evaluated is given just one module, depending on expressive language level and chronological age. Each modulehas different cutoff scores, and as such they should not be considered equivalent. Two control participants had incomplete ADOSdata, which is not reported above. ADI–R Soc = Autism Diagnostic Interview, Revised: Reciprocal Social Interactions; ADI–R Com =Autism Diagnostic Interview, Revised: Language/Communication; ADI–R RSB = Autism Diagnostic Interview, Revised: Restricted,Repetitive, and Stereotyped Behaviors and Interests. Four participants in the autism sample were missing ADI–R data, and no ADI–Rdata were available for the control group.
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
MOTOR IMPAIRMENTS AND STRUCTURAL IMAGING IN AUTISM 871
not otherwise specified of 7. History, physical exam,Fragile-X gene testing, and karyotype were per-formed on all subjects to exclude medical causes ofautistic phenotypes.
Control sample
TDC participants had no developmental, neu-rological, or clinical history for major psychiatricdisorders and completed an ADOS–G assessmentto ensure that none met criteria for ASD.
Neuroimaging
Volumetric studies were based on magnetic reso-nance images acquired on a Siemens Trio 3.0 Teslascanner at the University of Utah. A 12-channel,receive-only radio frequency (RF) head coil wasused to obtain 3D T1-weighted image volumes with1-mm isotropic resolution using a magnetizationprepared rapid gradient echo (MPRAGE) sequence(inversion time, TI = 900 ms; time to repetition,TR = 2300 ms; echo time, TE = 2.91 m; flip angle =9 degrees; sagittal, field of view = 25.6 cm; matrix =256 × 256 × 160). Imaging from three ASD sub-jects could not be used and were not part of thequantitative MRI analyses.
Volumetric image analysis
All analyses were performed with FreeSurfer,Version 5.1 (http://surfer.nmr.mgh.harvard.edu/)and followed the methods detailed by Bigler et al.(2010). The following gray matter ROIs were exam-ined: precentral gyrus, postcentral gyrus, caudalmiddle frontal area (i.e., supplementary motorarea), thalamus, cerebellum, and basal ganglia.Whole brain white and gray matter and intracranialvolume were also estimated.
Justification for including these ROIs comesfrom Moritz, Haughton, Cordes, Quigley, andMeyerand (2000), who demonstrated involvementof the precentral and postcentral gyri, supplemen-tary motor area, cerebellum, thalamus, and puta-men during a FTT task using functional MRI(fMRI) techniques. SOG has been shown to beassociated with activation of the postcentral gyriand supplementary motor area as well as cere-bellum (Cramer et al., 2002). All of the abovemotor regions are also the presumed motor con-trol areas involved in the GPT, although GPTperformance has not yet been examined from aneuroimaging perspective. Increased levels of motorskill and precision are required to manipulate thesmall pegs used with the GPT (Lezak et al., 2012),suggesting coordination of primary motor, basal
ganglia, and cerbellar regions along with sensory–perceptual feedback to efficiently perform theGPT task.
IQ
Verbal skills are often diminished in autism(Rapin, 1999) along with considerable variabilityin verbal and performance IQ scores, often result-ing in lower IQ in autism samples (Deutsch &Joseph, 2003). However, in disorders where intellec-tual compromise may be part of the clinical picturefor the dependent variable in question, overcontrol-ling for IQ may, in fact, limit important findings(see Dennis et al., 2009). Likewise, to be inclu-sive of the ASD sample being assessed we utilizeda liberal lower IQ limit (performance IQ, PIQ ≥64) as the minimal level of intellectual functioningto participate in this investigation. Only three ASDparticipants had a PIQ score below 70, and onlyone had a PIQ of 64. To further examine issuesrelated to IQ, because the ASD and control sam-ples were sufficiently large, as part of a secondarycomparison, participants with ASD were matchedto controls to be within five IQ points, to controlfor differences that may be specific to IQ. Since thelowest PIQ score in the control sample was 88, inthis secondary analysis matching on IQ, none ofthe lower functioning participants were included inthose comparisons.
Head circumference and handedness
Standard occipitofrontal head circumference andhandedness based on the Edinburgh HandednessInventory (Oldfield, 1971) were obtained on allsubjects. Demographic findings are reported inTable 1.
Motor tests
Standard FTT and SOG instruments fromthe Halstead–Retain Battery (Reitan Laboratories:www.reitanlabs.com; see also Heaton, Grant, &Matthews, 1991) were used along with the standardGPT (Matthews & Klove, 1964). All participantswere administered the SOG, FTT, and GPT as out-lined by Reitan and Wolfson (1986), Heaton et al.(1991), and Matthews and Klove (1964). The man-ual finger tapping board was used for the majorityof subjects but for younger children the electronicFTT version was used. The number of taps per-formed over 10-second epochs was recorded foreach trial, separately for each hand. To ensure con-sistency of responding, a minimum of five trials wasadministered with the total score required to be
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014

872 DUFFIELD ET AL.
within ±5 points. If this was not achieved, the totalfrom all trials were averaged for each hand and bothhands combined.
For the GPT, the participant was required toinsert pegs in a prescribed order as quickly as pos-sible using the dominant and nondominant handseparately. The number of pegs dropped was alsorecorded. The score was the time required to placepegs into all 25 holes, and the timing was notinterrupted in the event of a dropped peg. Forparticipants over 8 years of age, 25 pegs wereadministered, and for participants aged 5–8 years,only 10 pegs were administered. To compare allsubjects’ motor performance for this test, the stan-dard metric variables of drop rate (number of pegsdropped/total number of peg holes) and unit com-pletion time (number of pegs placed/total comple-tion time) were calculated. The total GPT scorewas computed by combining the nondominanthand completion time and the dominant handcompletion time. SOG was measured by use ofa hand dynamometer. The test requires the per-son to hold the upper part of the dynamome-ter in the palm of the hand and squeeze thestirrup with the fingers as tightly as possible.The average strength in kilograms of the twotrials was recorded for each hand if they werewithin a 5-point range. If the two trials were notwithin ±5 points, a third trial was completed,and the average of those three trials was used.The total SOG score was computed by combin-ing the nondominant hand mean and the dominanthand mean.
Statistical analysis
Group means were calculated and comparedfor autism and control subjects, using analysis ofcovariance (ANCOVA) with age, head circumfer-ence, and PIQ as covariates. FTT mean scoresfor both hands, GPT unit completion time (singlepeg), and peg drop rate for both hands, and theSOG means for both hands were compared betweenASD and control groups. Motor findings were thenexamined in relation to key neuroimaging identi-fied motor areas based on the volumetric data usingpartial correlations. FTT, GPT, and SOG totalswere used for the partial correlations to reducefamilywise error rates, including linear regressionsthat explored possible group by region interac-tions. A testwise false-positive error rate was setat .05, thus controlling for potential experiment-wise errors. Analyses were run using Version 20 ofthe IBM SPSS Statistics package. Clinical impair-ment on standardized neuropsychological measures
is often conservatively defined as falling two stan-dard deviations (z-score = –2.0) below the meanof a normative sample (Lezak et al., 2012; Strausset al., 2006). For each measure, a simple fre-quency count was determined for who performedat this level of impairment based on normative dataderived from the Lafayette Instrument Company(2002), Strauss et al. (2006), Mathiowetz, Wiemer,and Federman (1986), and Nussbaum and Bigler(1997).
RESULTS
Sample characteristics
As previously shown in Table 1, no significant dif-ferences were found for group-matching variables(age, head circumference, handedness index) exceptIQ, as expected.
Motor test performance in autism andcontrols
SOG, FTT, and GPT results, along with effect sizedifferences between the ASD and TDC groups, aresummarized in Table 3. Motor tasks were all pos-itively intercorrelated as shown in Table 4. Thedistributions for SOG and GPT were not normallydistributed; however, after applying log transforma-tions, homogeneity of variance assumptions weremet. Results of SOG, FTT, and GPT performanceby group are detailed in Table 4. As shown inTable 1, because of the IQ differences betweenTDCs and those with ASD, an IQ-matched sample(matching on PIQ) was created from the origi-nal sample (within ± 5 PIQ points) consisting of24 participants in each group, resulting in no sig-nificant difference on PIQ between groups, t(46) =–0.63, p = .54. Even after matching on IQ, there wasno difference in the pattern of motor task findingsbetween the IQ-matched group and the originalsample using PIQ as a covariate; therefore, the find-ings reported below were based on all subjects withPIQ as a covariate.
SOG
Participants with ASD had lower SOG scores,which only approached significance for the non-dominant hand (see Table 3). For the ASD group,7 participants (11.8%) were clinically impaired (i.e.,z-score ≥ –2.0) for either hand with 3 (10.0%) par-ticipants found in the impaired range for the TDCgroup.
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
MOTOR IMPAIRMENTS AND STRUCTURAL IMAGING IN AUTISM 873
TABLE 3Motor performance ANCOVAs controlling for age, head circumference, and PIQ
Hand
MeanASD (SD)
N = 56
MeanTD (SD)
N = 30 F p η2p
SOG DH 27.23 (14.94) 31.34 (15.92) 1.57 .21 .019NDH 25.56 (14.16) 29.06 (14.87) 3.47 .07 .040
FTT DH 41.40 (8.46) 44.94 (8.87) 5.90∗ .02 .070NDH 38.95 (8.27) 41.95 (9.55) 9.51∗∗ .003 .110
GPT drop rate DH 0.03 (0.06) 0.02 (0.04) 0.99 .32 .012NDH 0.04 (0.06) 0.01 (0.02) 9.32∗∗ .005 .231
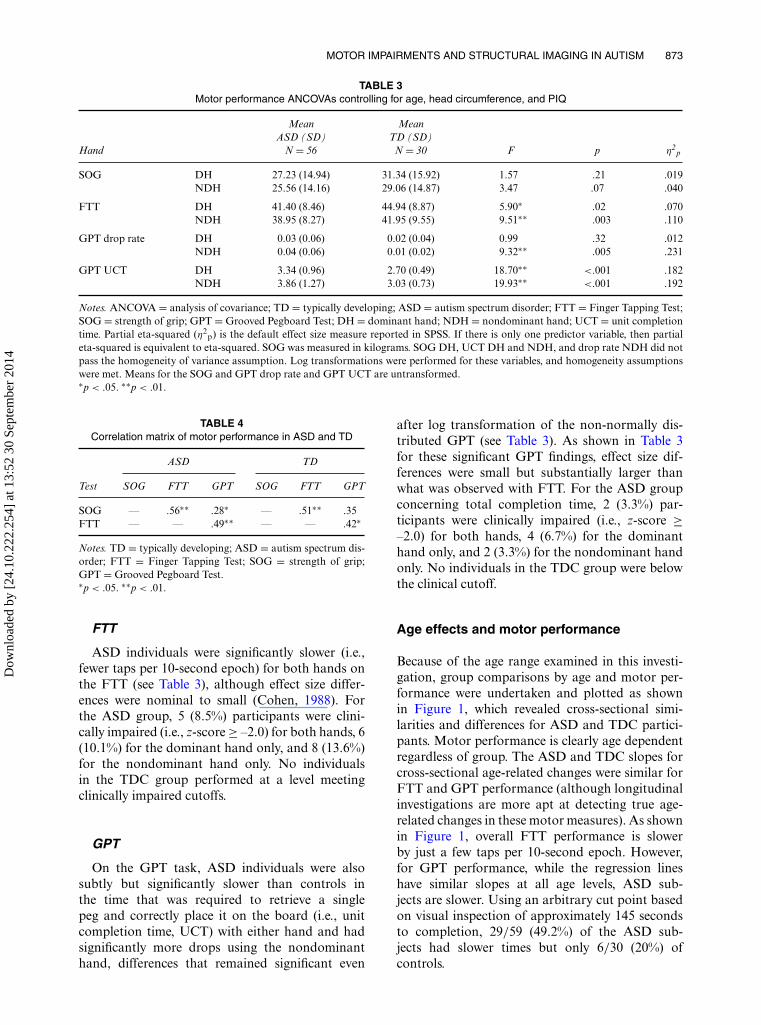
GPT UCT DH 3.34 (0.96) 2.70 (0.49) 18.70∗∗ <.001 .182NDH 3.86 (1.27) 3.03 (0.73) 19.93∗∗ <.001 .192
Notes. ANCOVA = analysis of covariance; TD = typically developing; ASD = autism spectrum disorder; FTT = Finger Tapping Test;SOG = strength of grip; GPT = Grooved Pegboard Test; DH = dominant hand; NDH = nondominant hand; UCT = unit completiontime. Partial eta-squared (η2
p) is the default effect size measure reported in SPSS. If there is only one predictor variable, then partialeta-squared is equivalent to eta-squared. SOG was measured in kilograms. SOG DH, UCT DH and NDH, and drop rate NDH did notpass the homogeneity of variance assumption. Log transformations were performed for these variables, and homogeneity assumptionswere met. Means for the SOG and GPT drop rate and GPT UCT are untransformed.∗p < .05. ∗∗p < .01.
TABLE 4Correlation matrix of motor performance in ASD and TD
ASD TD
Test SOG FTT GPT SOG FTT GPT
SOG — .56∗∗ .28∗ — .51∗∗ .35FTT — — .49∗∗ — — .42∗
Notes. TD = typically developing; ASD = autism spectrum dis-order; FTT = Finger Tapping Test; SOG = strength of grip;GPT = Grooved Pegboard Test.∗p < .05. ∗∗p < .01.
FTT
ASD individuals were significantly slower (i.e.,fewer taps per 10-second epoch) for both hands onthe FTT (see Table 3), although effect size differ-ences were nominal to small (Cohen, 1988). Forthe ASD group, 5 (8.5%) participants were clini-cally impaired (i.e., z-score ≥ –2.0) for both hands, 6(10.1%) for the dominant hand only, and 8 (13.6%)for the nondominant hand only. No individualsin the TDC group performed at a level meetingclinically impaired cutoffs.
GPT
On the GPT task, ASD individuals were alsosubtly but significantly slower than controls inthe time that was required to retrieve a singlepeg and correctly place it on the board (i.e., unitcompletion time, UCT) with either hand and hadsignificantly more drops using the nondominanthand, differences that remained significant even
after log transformation of the non-normally dis-tributed GPT (see Table 3). As shown in Table 3for these significant GPT findings, effect size dif-ferences were small but substantially larger thanwhat was observed with FTT. For the ASD groupconcerning total completion time, 2 (3.3%) par-ticipants were clinically impaired (i.e., z-score ≥–2.0) for both hands, 4 (6.7%) for the dominanthand only, and 2 (3.3%) for the nondominant handonly. No individuals in the TDC group were belowthe clinical cutoff.
Age effects and motor performance
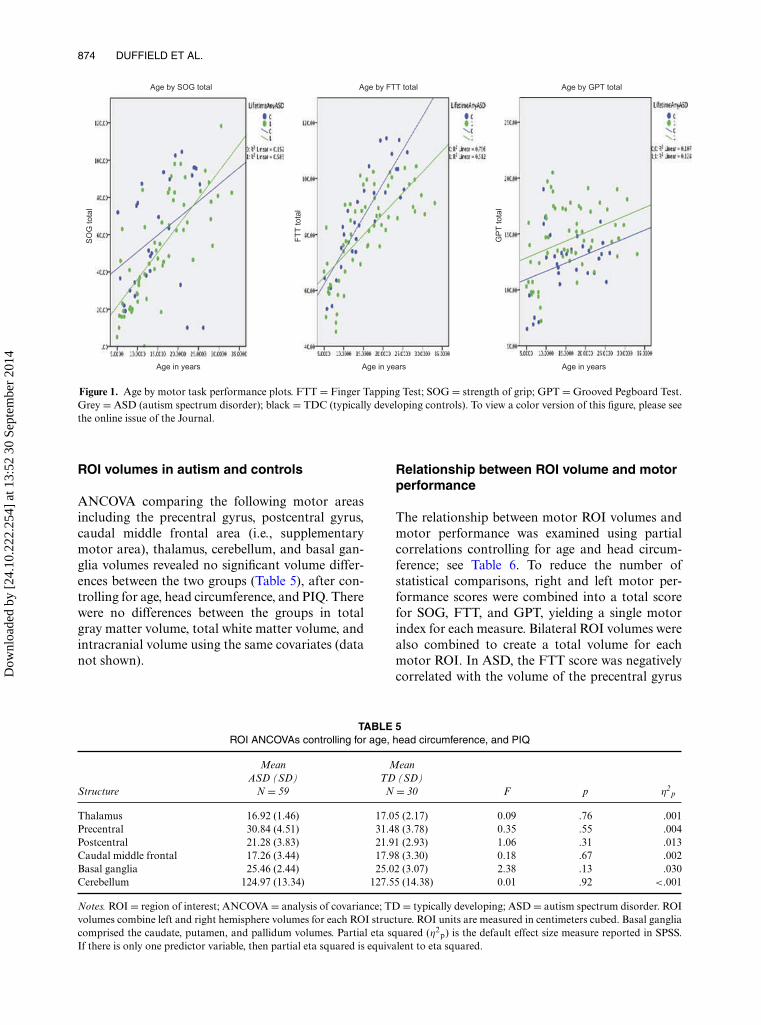
Because of the age range examined in this investi-gation, group comparisons by age and motor per-formance were undertaken and plotted as shownin Figure 1, which revealed cross-sectional simi-larities and differences for ASD and TDC partici-pants. Motor performance is clearly age dependentregardless of group. The ASD and TDC slopes forcross-sectional age-related changes were similar forFTT and GPT performance (although longitudinalinvestigations are more apt at detecting true age-related changes in these motor measures). As shownin Figure 1, overall FTT performance is slowerby just a few taps per 10-second epoch. However,for GPT performance, while the regression lineshave similar slopes at all age levels, ASD sub-jects are slower. Using an arbitrary cut point basedon visual inspection of approximately 145 secondsto completion, 29/59 (49.2%) of the ASD sub-jects had slower times but only 6/30 (20%) ofcontrols.
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
874 DUFFIELD ET AL.
Age by SOG total
Age in years Age in years Age in years
Age by FTT totalS
OG
tota
l
FT
T to
tal
GP
T to
tal
Age by GPT total
Figure 1. Age by motor task performance plots. FTT = Finger Tapping Test; SOG = strength of grip; GPT = Grooved Pegboard Test.Grey = ASD (autism spectrum disorder); black = TDC (typically developing controls). To view a color version of this figure, please seethe online issue of the Journal.
ROI volumes in autism and controls
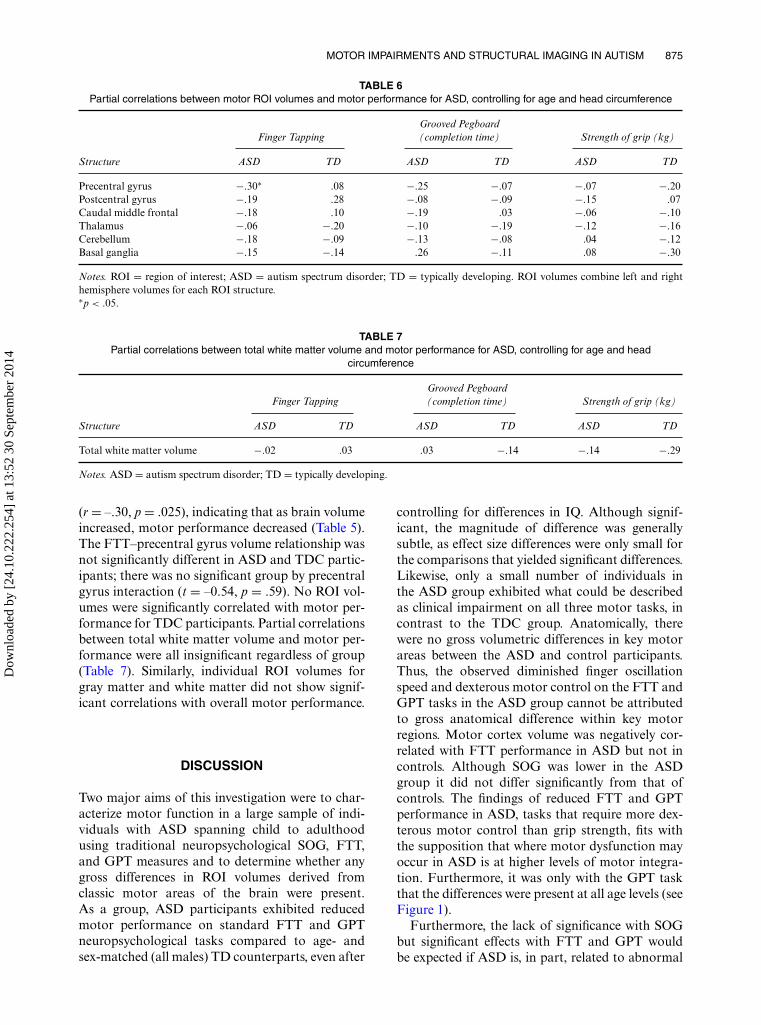
ANCOVA comparing the following motor areasincluding the precentral gyrus, postcentral gyrus,caudal middle frontal area (i.e., supplementarymotor area), thalamus, cerebellum, and basal gan-glia volumes revealed no significant volume differ-ences between the two groups (Table 5), after con-trolling for age, head circumference, and PIQ. Therewere no differences between the groups in totalgray matter volume, total white matter volume, andintracranial volume using the same covariates (datanot shown).
Relationship between ROI volume and motorperformance
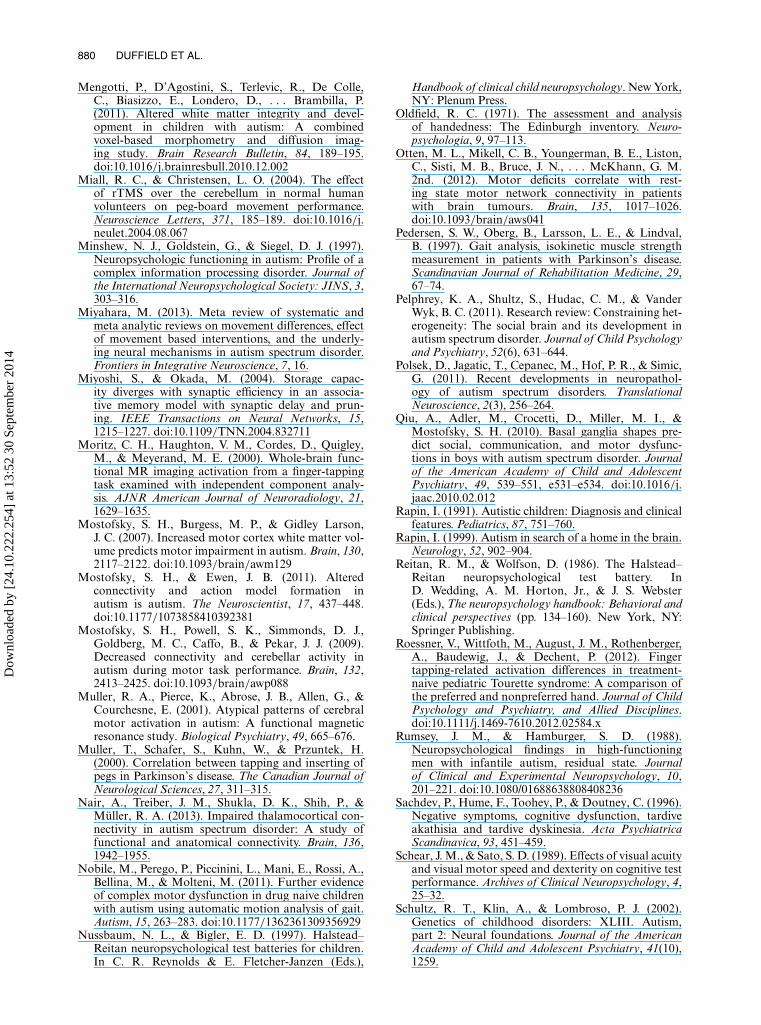
The relationship between motor ROI volumes andmotor performance was examined using partialcorrelations controlling for age and head circum-ference; see Table 6. To reduce the number ofstatistical comparisons, right and left motor per-formance scores were combined into a total scorefor SOG, FTT, and GPT, yielding a single motorindex for each measure. Bilateral ROI volumes werealso combined to create a total volume for eachmotor ROI. In ASD, the FTT score was negativelycorrelated with the volume of the precentral gyrus
TABLE 5ROI ANCOVAs controlling for age, head circumference, and PIQ
Structure
MeanASD (SD)
N = 59
MeanTD (SD)
N = 30 F p η2p
Thalamus 16.92 (1.46) 17.05 (2.17) 0.09 .76 .001Precentral 30.84 (4.51) 31.48 (3.78) 0.35 .55 .004Postcentral 21.28 (3.83) 21.91 (2.93) 1.06 .31 .013Caudal middle frontal 17.26 (3.44) 17.98 (3.30) 0.18 .67 .002Basal ganglia 25.46 (2.44) 25.02 (3.07) 2.38 .13 .030Cerebellum 124.97 (13.34) 127.55 (14.38) 0.01 .92 <.001
Notes. ROI = region of interest; ANCOVA = analysis of covariance; TD = typically developing; ASD = autism spectrum disorder. ROIvolumes combine left and right hemisphere volumes for each ROI structure. ROI units are measured in centimeters cubed. Basal gangliacomprised the caudate, putamen, and pallidum volumes. Partial eta squared (η2
p) is the default effect size measure reported in SPSS.If there is only one predictor variable, then partial eta squared is equivalent to eta squared.
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
MOTOR IMPAIRMENTS AND STRUCTURAL IMAGING IN AUTISM 875
TABLE 6Partial correlations between motor ROI volumes and motor performance for ASD, controlling for age and head circumference
Finger TappingGrooved Pegboard(completion time) Strength of grip (kg)
Structure ASD TD ASD TD ASD TD
Precentral gyrus −.30∗ .08 −.25 −.07 −.07 −.20Postcentral gyrus −.19 .28 −.08 −.09 −.15 .07Caudal middle frontal −.18 .10 −.19 .03 −.06 −.10Thalamus −.06 −.20 −.10 −.19 −.12 −.16Cerebellum −.18 −.09 −.13 −.08 .04 −.12Basal ganglia −.15 −.14 .26 −.11 .08 −.30
Notes. ROI = region of interest; ASD = autism spectrum disorder; TD = typically developing. ROI volumes combine left and righthemisphere volumes for each ROI structure.∗p < .05.
TABLE 7Partial correlations between total white matter volume and motor performance for ASD, controlling for age and head
circumference
Finger TappingGrooved Pegboard(completion time) Strength of grip (kg)
Structure ASD TD ASD TD ASD TD
Total white matter volume −.02 .03 .03 −.14 −.14 −.29
Notes. ASD = autism spectrum disorder; TD = typically developing.
(r = –.30, p = .025), indicating that as brain volumeincreased, motor performance decreased (Table 5).The FTT–precentral gyrus volume relationship wasnot significantly different in ASD and TDC partic-ipants; there was no significant group by precentralgyrus interaction (t = –0.54, p = .59). No ROI vol-umes were significantly correlated with motor per-formance for TDC participants. Partial correlationsbetween total white matter volume and motor per-formance were all insignificant regardless of group(Table 7). Similarly, individual ROI volumes forgray matter and white matter did not show signif-icant correlations with overall motor performance.
DISCUSSION
Two major aims of this investigation were to char-acterize motor function in a large sample of indi-viduals with ASD spanning child to adulthoodusing traditional neuropsychological SOG, FTT,and GPT measures and to determine whether anygross differences in ROI volumes derived fromclassic motor areas of the brain were present.As a group, ASD participants exhibited reducedmotor performance on standard FTT and GPTneuropsychological tasks compared to age- andsex-matched (all males) TD counterparts, even after
controlling for differences in IQ. Although signif-icant, the magnitude of difference was generallysubtle, as effect size differences were only small forthe comparisons that yielded significant differences.Likewise, only a small number of individuals inthe ASD group exhibited what could be describedas clinical impairment on all three motor tasks, incontrast to the TDC group. Anatomically, therewere no gross volumetric differences in key motorareas between the ASD and control participants.Thus, the observed diminished finger oscillationspeed and dexterous motor control on the FTT andGPT tasks in the ASD group cannot be attributedto gross anatomical difference within key motorregions. Motor cortex volume was negatively cor-related with FTT performance in ASD but not incontrols. Although SOG was lower in the ASDgroup it did not differ significantly from that ofcontrols. The findings of reduced FTT and GPTperformance in ASD, tasks that require more dex-terous motor control than grip strength, fits withthe supposition that where motor dysfunction mayoccur in ASD is at higher levels of motor integra-tion. Furthermore, it was only with the GPT taskthat the differences were present at all age levels (seeFigure 1).
Furthermore, the lack of significance with SOGbut significant effects with FTT and GPT wouldbe expected if ASD is, in part, related to abnormal
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014

876 DUFFIELD ET AL.
networks and connectivity, since both FTT andGPT would require larger integrated networks formotor performance than for basic strength. Motordeficits in ASD could also be related to a distur-bance in functional organization of the motor cor-tices (Muller, Pierce, Abrose, Allen, & Courchesne,2001). The one observation of a negative corre-lation between motor cortex and FTT would beconsistent with an overgrowth theory of autism,where overgrowth may be associated with less effi-cient networks (Amaral, Dawson, & Geschwind,2011; Courchesne, Webb, & Schumann, 2011)and, therefore, larger size associated with poorerfunction. Mostofsky, Burgess, and Gidley Larson(2007), relying on clinical motor exam findingsonly, observed that increased white matter volumeof motor cortex in autism was associated withabnormal clinical motor findings. In the currentstudy, volume differences of motor cortex werenot observed, but nonetheless, a larger motor cor-tex was associated with reduced FTT speed inASD participants. It is possible that subtle over-growth and/or lack of pruning within neural sys-tems that control motor function leads to ineffi-ciency (Miyoshi & Okada, 2004) and to the generalnegative relationships of motor cortex volume andFTT in ASD. The normal developmental processof synaptic pruning has been postulated to be com-promised in autism (Frith, 2003; Schultz, Klin,& Lombroso, 2002), disrupting how activity andexperience support the organization of functionalnetworks in typical brain development (Just, Keller,Malave, Kana, & Varma, 2012; Kandel, Schwartz,& Jessell, 2000). Just et al. (2012) have postulatedthat the developing autistic brain may not supportan appropriate balance between maturation andexperience. Errors in pruning may interfere with theemergence of the specialized functions of one ormore of a set of neuroanatomical structures (seePelphrey, Shultz, Hudac, & Vander Wyk, 2011).In TD individuals, normal pruning could help elim-inate faulty connections and optimize coordinatedneural functioning, which compromised pruningmight fail to accomplish. Compromised pruningprocesses possibly result in some degree of aber-ration in typical anatomical size–function relationsthat adversely influences communication amongcortical regions (Just et al., 2012). However, there ismuch to be discovered about development, pruning,white matter connectivity, and cortical maturationin ASD (Cassanova et al., 2006). While the findingsof larger motor cortex being associated with poorermotor function in this ASD sample fit with aberrantdevelopment and potential faulty pruning and/orovergrowth, the precise meaning of these findings isunknown.
Hadders-Algra (2008) postulated that the rela-tionship between preterm birth injury, white matterdamage, and motor deficits in children diagnosedwith ASD was a problem of connectivity. Ligamet al. (2009) have shown a greater incidence ofthalamic pathology in periventricular leukomala-cia (PVL) associated with prematurity and spec-ulate about the relation between thalamic dam-age, white matter pathology, and autism (see alsoLimperopoulos et al., 2008). Since PVL has thepotential to disrupt neuronal migration, the poten-tial thalamic damage and disrupted white mat-ter connectivity being related to ASD is intrigu-ing. Furthermore, Nair, Treiber, Shukla, Shih, andMuller (2013) recently reported impaired thalo-mocortical connectivity in ASD. In the currentstudy, prematurity was excluded as a risk factorfor the ASD cohort examined. Thalamic volumein the ASD cohort did not differ from that inthe TDC group, and therefore no gross thalamicpathology was found. Thalamic volume did not sig-nificantly relate to any motor measurement, nor didwhite matter volume. As such, the current findingsare unlikely related to any gross neural insult orabnormality, but these methods do not specificallyaddress issues of connectivity and development.Unfortunately, ROI volumes likely represent poorproxies as indices of brain connectivity, and stud-ies that employ more direct measures of functionalconnectivity should be conducted in relation tomotor performance in ASD (see Miyahara, 2013).
While SOG is primarily a basic measure of theintegrity of the corticospinal tract (Schulz et al.,2012), fMRI studies also indicate that SOG per-formance results in some basal ganglia and cere-bellar activation (Cramer et al., 2002; Keisker,Hepp-Reymond, Blickenstorfer, & Kollias, 2010;van Nuenen, Kuhtz-Buschbeck, Schulz, Bloem, &Siebner, 2012). Nonetheless, this SOG networkis far more simple than the activation patternsobserved during FTT performance as assessedby functional neuroimaging (De Guio, Jacobson,Molteno, Jacobson, & Meintjes, 2012; Lopez-Larson et al., 2012; Witt, Laird, & Meyerand,2008), where coordinated finger movement has beenshown to depend on widespread motor connections(Jin, Lin, & Hallett, 2012; Roessner et al., 2012).
Because of the motion restrictions imposed byfMRI studies of motor function, the SOG and FTTmethods have been readily adapted to the scannerenvironment, but not the GPT task. Neuroimaginglesion studies as well as low-frequency transcranialmagnetic stimulation associated with GPT perfor-mance, have found correlations between GPT pro-ficiency and connectivity between motor, premotor,and supplemental motor cortices, corpus callosum,
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014

MOTOR IMPAIRMENTS AND STRUCTURAL IMAGING IN AUTISM 877
and cerebellum (Franc et al., 2011; Kodl et al., 2008;Miall & Christensen, 2004; Otten et al., 2012) wherereduced parietal white matter integrity on diffusiontensor imaging (DTI) was associated with worseGPT performance. These latter findings may bebest explained by GPT performance requiring notonly motor skill but guided attention as well (Lezaket al., 2012). The preceding considerations sug-gest that the GPT task requires far greater neuralcomplexity than SOG. The significant differencesobserved with FTT and GPT in autism, and thatthese tasks depend on both short- and long-rangeconnectivity, is consistent with the postulated func-tional connectivity problems associated with ASD(Dowell, Mahone, & Mostofsky, 2009; Mostofsky& Ewen, 2011).
ROI volumes and motor function
Previous voxel-based morphometry studies foundenlargements in the right postcentral gyrus, rightmedial frontal gyrus, and right posterior lobe ofcerebellum (Ke et al., 2008) and decreases in theleft precentral gyrus (Cauda et al., 2011) andleft supplementary motor area (Mengotti et al.,2011) in autism when compared with controls. TheMengotti et al. (2011) and Ke et al. (2008) stud-ies differ from the current study in that they havemuch smaller sample sizes and a smaller age range.Cauda et al. (2011) was a meta-analysis of 16 stud-ies with a total of 350 ASD subjects (which includedhigh-functioning autism, Asperger’s syndrome, andunspecified diagnoses), and male and female sub-jects. None of the above studies examined motorfunction with the SOG, FTT, or GPT tasks system-atically as has been done in this investigation.
Size–function relationships may emerge in braindevelopment potentially reflecting optimal size(e.g., volume) of a given structure that maybest relate to cognitive function as measured byneuropsychological variables (Koscik & Tranel,2012). However, ROI volume relationships withneuropsychological functioning are complex, par-ticularly in individuals with neuropsychiatric dis-orders (Crespo-Facorro, Barbadillo, Pelayo-Teran,& Rodriguez-Sanchez, 2007). Because of the com-plexities of brain development and individual dif-ferences in cognitive and neurobehavioral func-tioning, brain volumetry may not correlate withneuropsychological variables in a consistent andsystematic pattern. Given the general lack of ROIvolume relationships, it is likely that such anapproach as used in the current investigation maysimply be insensitive in detecting motor networkabnormalities. Therefore, given prior reports of
white matter pathway abnormalities in autism(Lainhart & Lange, 2011; Mak-Fan et al., 2012;Weinstein et al., 2011), it may be that measuresmore directly assessing white matter connectivity,such as DTI and functional connectivity MRI, mayprovide improved understanding of motor abnor-malities in autism. In fact, those investigations areunderway with this cohort.
LIMITATIONS AND CONCLUSIONS
The autism sample was all male and comprisedhigh-functioning individuals who do not representthose with lower functioning abilities, or femaleswith autism. As already stated, this investigationdid not directly assess connectivity where directmeasures of motor performance using fMRI tech-niques may yield much more specific findingsrelated to motor differences in ASD than in con-trols. Also, this study did not assess presence of clin-ical motor signs and their relationship to objectiveneuropsychological measures of motor functioning.
Despite these limitations, the current findings dofit with a hierarchical model of impaired function-ing in autism where basic motor ability is preserved,but as motor complexity increases, a greater like-lihood of impaired motor function is observedin ASD. As Miyahara (2013) posited, it is moremeaningful and clinically practical to use standardassessments thereby insuring common metrics usedby researchers and clinicians in the study of ASD.Using all three standardized neuropsychologicalmeasures (i.e., SOG, FTT, GPT), as in the cur-rent study, provides a motor profile that hopefullywill be useful to clinicians assessing motor functionin ASD. As shown in Figure 1, regardless of agethere were consistently more individuals with ASDwho exhibited slowed performance times on theGPT than those observed in control participants.The hierarchical model of motor control used inthe current investigation, as well as the findingsreported herein, provides information and heuris-tics to further explore motor findings associatedwith ASD.
REFERENCES
Alexander, A. L., Lee, J. E., Lazar, M., Boudos, R.,DuBray, M. B., Oakes, T. R., . . . Lainhart, J. E.(2007). Diffusion tensor imaging of the corpus callo-sum in autism. NeuroImage, 34, 61–73. doi:10.1016/j.neuroimage.2006.08.032
Amaral, D., Dawson, G., & Geschwind, D. H. (2011).Autism spectrum disorders. Oxford: Oxford UniversityPress.
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014

878 DUFFIELD ET AL.
American Psychiatric Association. (1994). Diagnostic andstatistical manual of mental disorders. Washington,DC: Author.
Athinoula, A. Martinos Center for Biomedical Imaging.Freesurfer. Retrieved from http://surfer.nmr.mgh.harvard.edu
Baser, C. N., & Ruff, R. M. (1987). Construct validityof the San Diego Neuropsychological Test Battery.Archives of Clinical Neuropsychology, 2, 13–32.
Bhat, A. N., Landa, R. J., & Galloway, J. C. (2011).Current perspectives on motor functioning in infants,children, and adults with autism spectrum disor-ders. Physical Therapy, 91, 1116–1129. doi:10.2522/ptj.20100294
Bigler, E. D., Abildskov, T. J., Wilde, E. A., McCauley,S. R., Li, X., Merkley, T. L., . . . Levin, H. S. (2010).Diffuse damage in pediatric traumatic brain injury: Acomparison of automated versus operator-controlledquantification methods. NeuroImage, 50, 1017–1026.doi:10.1016/j.neuroimage.2010.01.003
Bonnet, K. A., & Gao, X. K. (1996). Asperger syndromein neurologic perspective. Journal of Child Neurology,11, 483–489.
Carcani-Rathwell, I., Rabe-Hasketh, S., & Santosh,P. J. (2006). Repetitive and stereotyped behaviours inpervasive developmental disorders. Journal of ChildPsychology and Psychiatry and Allied Disciplines, 47,573–581. doi:10.1111/j.1469-7610.2005.01565.x
Casanova, M. F., van Kooten, I. A., Switala, A. E.,van Engeland, H., Heinsen, H., Steinbusch, H. W.,. . . Schmitz, C. (2006). Minicolumnar abnormalitiesin autism. Acta Neuropathologica, 112(3), 287–303.doi:10.1007/s00401-006-0085-5
Cauda, F., Geda, E., Sacco, K., D’Agata, F., Duca,S., Geminiani, G., & Keller, R. (2011). Grey mat-ter abnormality in autism spectrum disorder: Anactivation likelihood estimation meta-analysis study.Journal of Neurology, Neurosurgery & Psychiatry, 82,1304–1313. doi:10.1136/jnnp.2010.239111
Cohen, J. (1988). Statistical power analysis for the behav-ioral sciences (2nd ed.). Hillsdale, NJ: LawrenceErlbaum Associates.
Courchesne, E., Carper, R., & Akshoomoff, N. (2003).Evidence of brain overgrowth in the first yearof life in autism. JAMA: The Journal of theAmerican Medical Association, 290(3), 337–344.doi:10.1001/jama.290.3.337
Courchesne, E., & Pierce, K. (2005). Brain over-growth in autism during a critical time in devel-opment: Implications for frontal pyramidal neu-ron and interneuron development and connectivity.International Journal of Developmental Neuroscience,23(2–3), 153–170. doi:10.1016/j.ijdevneu.2005.01.003
Courchesne, E., Webb, S. J., & Schumann, C. (2011).From toddlers to adults: The changing landscape ofthe brain in autism. In D. Amaral, G. Dawson, &D. H. Geschwind (Eds.), Autism spectrum disorders(pp. 611–631). Oxford: Oxford University Press.
Cramer, S. C., Weisskoff, R. M., Schaechter, J. D., Nelles,G., Foley, M., Finklestein, S. P., & Rosen, B. R.(2002). Motor cortex activation is related to forceof squeezing. Human Brain Mapping, 16, 197–205.doi:10.1002/hbm.10040
Crespo-Facorro, B., Barbadillo, L., Pelayo-Teran,J. M., & Rodriguez-Sanchez, J. M. (2007).Neuropsychological functioning and brain structure
in schizophrenia. International Review of Psychiatry,19, 325–336. doi:10.1080/09540260701486647
De Guio, F., Jacobson, S. W., Molteno, C. D., Jacobson,J. L., & Meintjes, E. M. (2012). Functional magneticresonance imaging study comparing rhythmic fingertapping in children and adults. Pediatric Neurology,46, 94–100. doi:10.1016/j.pediatrneurol.2011.11.019
Dennis, M., Francis, D. J., Cirino, P. T., Schachar, R.,Barnes, M. A., & Fletcher, J. M. (2009). Why IQis not a covariate in cognitive studies of neurode-velopmental disorders. Journal of the InternationalNeuropsychological Society, 15, 331–343. doi:10.1017/S1355617709090481
Deutsch, C. K., & Joseph, R. M. (2003). Brief report:Cognitive correlates of enlarged head circumferencein children with autism. Journal of Autism andDevelopmental Disorders, 33, 209–215.
Dowell, L. R., Mahone, E. M., & Mostofsky, S. H.(2009). Associations of postural knowledge and basicmotor skill with dyspraxia in autism: Implicationfor abnormalities in distributed connectivity andmotor learning. Neuropsychology, 23, 563–570.doi:10.1037/a0015640
Downey, R., & Rapport, M. J. (2012). Motor activ-ity in children with autism: A review of cur-rent literature. Pediatric Physical Therapy, 24, 2–20.doi:10.1097/PEP.0b013e31823db95f
Draganski, B., & Bhatia, K. P. (2010). Brain struc-ture in movement disorders: A neuroimaging per-spective. Current Opinion in Neurology, 23, 413–419.doi:10.1097/WCO.0b013e32833bc59c
Dziuk, M. A., Gidley Larson, J. C., Apostu, A., Mahone,E. M., Denckla, M. B., & Mostofsky, S. H. (2007).Dyspraxia in autism: Association with motor, social,and communicative deficits. Developmental Medicineand Child Neurology, 49, 734–739. doi:10.1111/j.1469-8749.2007.00734.x
Elliot, C. D. (1990). Differential ability scales. SanAntonio, TX: The Pyschological Corporation.
Emck, C., Bosscher, R., Beek, P., & Doreleijers, T. (2009).Gross motor performance and self-perceived motorcompetence in children with emotional, behavioural,and pervasive developmental disorders: A review.Developmental Medicine & Child Neurology, 51(7),501–517.
Emck, C., Bosscher, R. J., van Wieringen, P. C.,Doreleijers, T., & Beek, P. J. (2012). Psychiatric symp-toms in children with gross motor problems. AdaptedPhysical Activity Quarterly: APAQ, 29, 161–178.
Fournier, K. A., Hass, C. J., Naik, S. K., Lodha, N., &Cauraugh, J. H. (2010). Motor coordination in autismspectrum disorders: A synthesis and meta-analysis.Journal of Autism and Developmental Disorders, 40,1227–1240. doi:10.1007/s10803-010-0981-3
Franc, D. T., Kodl, C. T., Mueller, B. A., Muetzel, R. L.,Lim, K. O., & Seaquist, E. R. (2011). High connectiv-ity between reduced cortical thickness and disruptedwhite matter tracts in long-standing type 1 diabetes.Diabetes, 60, 315–319. doi:10.2337/db10-0598
Frith, C. (2003). What do imaging studies tell us aboutthe neural basis of autism? In G. Boch & J. Goode(Eds.), Autism: Neural basis and treatment possibilities(pp. 149–176). London: Wiley.
Geschwind, D. H. (2009). Advances in autism. AnnualReview of Medicine, 60, 367–380. doi:10.1146/annurev.med.60.053107.121225
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014

MOTOR IMPAIRMENTS AND STRUCTURAL IMAGING IN AUTISM 879
Goldman, S., Wang, C., Salgado, M. W., Greene, P. E.,Kim, M., & Rapin, I. (2009). Motor stereotypies inchildren with autism and other developmental disor-ders. Developmental Medicine and Child Neurology,51, 30–38. doi:10.1111/j.1469-8749.2008.03178.x
Gowen, E., & Hamilton, A. (2012). Motor abilitiesin autism: A review using a computational con-text. Journal of Autism and Developmental Disorders.Advance online publication. doi:10.1007/s10803-012-1574-0
Haaland, K. Y., & Delaney, H. D. (1981). Motor deficitsafter left or right hemisphere damage due to stroke ortumor. Neuropsychologia, 19, 17–27.
Hadders-Algra, M. (2008). Reduced variability in motorbehaviour: An indicator of impaired cerebral con-nectivity? Early Human Development, 84, 787–789.doi:10.1016/j.earlhumdev.2008.09.002
Hardan, A. Y., Kilpatrick, M., Keshavan, M. S., &Minshew, N. J. (2003). Motor performance andanatomic magnetic resonance imaging (MRI) of thebasal ganglia in autism. Journal of Child Neurology,18, 317–324.
Heaton, R. K., Grant, I., & Matthews, C. G. (1991).Comprehensive norms for an expanded Halstead–Reitan Battery: Demographic corrections, researchfindings, and clinical applications. Odessa, FL:Psychological Assessment Resources.
Hervé, P. Y., Mazoyer, B., Crivello, F., Perchey, G., &Tzourio-Mazoyer, N. (2005). Finger tapping, handed-ness and grey matter amount in the Rolando’s genuarea. NeuroImage, 25, 1133–1145.
Jansiewicz, E. M., Goldberg, M. C., Newschaffer,C. J., Denckla, M. B., Landa, R., & Mostofsky,S. H. (2006). Motor signs distinguish children withhigh functioning autism and Asperger’s syndromefrom controls. Journal of Autism and DevelopmentalDisorders, 36, 613–621. doi:10.1007/s10803-006-0109-y
Jara, H. (2013). Theory of quantitative magnetic resonanceimaging. Hackensack, NJ: World Scientific.
Jin, S. H., Lin, P., & Hallett, M. (2012). Reorganizationof brain functional small-world networks during fin-ger movements. Human Brain Mapping, 33, 861–872.doi:10.1002/hbm.21253
Just, M. A., Keller, T. A., Malave, V. L., Kana, R. K.,& Varma, S. (2012). Autism as a neural systemsdisorder: A theory of frontal-posterior underconnec-tivity. Neuroscience & Biobehavioral Reviews, 36(4),1292–1313.
Kandel, E. R., Schwartz, J. H., & Jessell, T. M. (Eds.).(2000). Principles of neural science (4th ed.). NewYork, NY: McGraw-Hill.
Kanner, L. (1943). Autistic disturbances of affective con-tact. Nervous Child, 2, 217–250.
Ke, X., Hong, S., Tang, T., Zou, B., Li, H., Hang,Y., . . . Liu, Y. (2008). Voxel-based morphom-etry study on brain structure in children withhigh-functioning autism. Neuroreport, 19, 921–925.doi:10.1097/WNR.0b013e328300edf3
Keisker, B., Hepp-Reymond, M. C., Blickenstorfer, A.,& Kollias, S. S. (2010). Differential representationof dynamic and static power grip force in the sen-sorimotor network. The European Journal of Neuro-science, 31, 1483–1491. doi:10.1111/j.1460-9568.2010.07172.x
Kern, J. K., Geier, D. A., Adams, J. B., Troutman, M. R.,Davis, G., King, P. G., . . . Geier, M. R. (2011). Autism
severity and muscle strength: A correlation analysis.Research in Autism Spectrum Disorders, 5, 1011–1015.
Kodl, C. T., Franc, D. T., Rao, J. P., Anderson, F. S.,Thomas, W., Mueller, B. A., . . . Seaquist, E. R.(2008). Diffusion tensor imaging identifies deficitsin white matter microstructure in subjects with type1 diabetes that correlate with reduced neurocognitivefunction. Diabetes, 57, 3083–3089. doi:10.2337/db08-0724
Koscik, T. R., & Tranel, D. (2012). Brain evolutionand human neuropsychology: The inferential brainhypothesis. Journal of the International Neuropsycho-logical Society: JINS, 18, 394–401. doi:10.1017/s1355617712000264
Lafayette Instrument Company. (2002). Grooved pegboardtest user instructions. Retrieved from http://www.si-instruments.com.au/industry/download/lafayette-current-version-grooved-pegboard-test-32025-lafayette-32025-grooved-pegboard-test-manual-pdf.html
Lainhart, J. E., & Lange, N. (2011). Increased neuronnumber and head size in autism. JAMA: The Journalof the American Medical Association, 306, 2031–2032.doi:10.1001/jama.2011.1633
Landa, R. J., Gross, A. L., Stuart, E. A., & Bauman,M. (2012). Latent class analysis of early develop-mental trajectory in baby siblings of children withautism. Journal of Child Psychology and Psychiatry,53, 986–996. doi:10. 1111/j.1469-7610.2012.02558.x
Lezak, M. D., Howieson, D. B., Bigler, E. D., & Tranel,D. (2012). Neuropsychological assessment (5th ed.).New York, NY: Oxford University Press.
Ligam, P., Haynes, R. L., Folkerth, R. D., Liu, L., Yang,M., Volpe, J. J., & Kinney, H. C. (2009). Thalamicdamage in periventricular leukomalacia: Novel patho-logic observations relevant to cognitive deficits in sur-vivors of prematurity. Pediatric Research, 65, 524–529.
Limperopoulos, C., Bassan, H., Sullivan, N. R., Soul,J. S., Robertson, R. L., Moore, M., . . . du Plessis, A. J.(2008). Positive screening for autism in ex-preterminfants: Prevalence and risk factors. Pediatrics, 121(4),758–765.
Lopez-Larson, M. P., Rogowska, J., Bogorodzki, P.,Bueler, C. E., McGlade, E. C., & Yurgelun-Todd,D. A. (2012). Cortico-cerebellar abnormalities inadolescents with heavy marijuana use. PsychiatryResearch, 202, 224–232. doi:10.1016/j.pscychresns.2011.11.005
Lord, C., Risi, S., Lambrecht, L., Cook, E. H.,Jr., Leventhal, B. L., DiLavore, P. C., . . . Rutter,M. (2000). The Autism Diagnostic ObservationSchedule–Generic: A standard measure of social andcommunication deficits associated with the spec-trum of autism. Journal of Autism and DevelopmentalDisorders, 30, 205–223.
Mak-Fan, K. M., Morris, D., Vidal, J., Anagnostou, E.,Roberts, W., & Taylor, M. J. (2012). White matterand development in children with an autism spec-trum disorder. Autism. Advance online publication.doi:10.1177/1362361312442596
Mathiowetz, V., Wiemer, D. M., & Federman, S. M.(1986). Grip and pinch strength: Norms for 6-to19-year-olds. The American Journal of OccupationalTherapy, 40(10), 705–711.
Matthews, C., & Klove, H. (1964). Instruction manualfor the Adult Neuropsychology Test Battery. Madison:University of Wisconsin Medical School.
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
880 DUFFIELD ET AL.
Mengotti, P., D’Agostini, S., Terlevic, R., De Colle,C., Biasizzo, E., Londero, D., . . . Brambilla, P.(2011). Altered white matter integrity and devel-opment in children with autism: A combinedvoxel-based morphometry and diffusion imag-ing study. Brain Research Bulletin, 84, 189–195.doi:10.1016/j.brainresbull.2010.12.002
Miall, R. C., & Christensen, L. O. (2004). The effectof rTMS over the cerebellum in normal humanvolunteers on peg-board movement performance.Neuroscience Letters, 371, 185–189. doi:10.1016/j.neulet.2004.08.067
Minshew, N. J., Goldstein, G., & Siegel, D. J. (1997).Neuropsychologic functioning in autism: Profile of acomplex information processing disorder. Journal ofthe International Neuropsychological Society: JINS, 3,303–316.
Miyahara, M. (2013). Meta review of systematic andmeta analytic reviews on movement differences, effectof movement based interventions, and the underly-ing neural mechanisms in autism spectrum disorder.Frontiers in Integrative Neuroscience, 7, 16.
Miyoshi, S., & Okada, M. (2004). Storage capac-ity diverges with synaptic efficiency in an associa-tive memory model with synaptic delay and prun-ing. IEEE Transactions on Neural Networks, 15,1215–1227. doi:10.1109/TNN.2004.832711
Moritz, C. H., Haughton, V. M., Cordes, D., Quigley,M., & Meyerand, M. E. (2000). Whole-brain func-tional MR imaging activation from a finger-tappingtask examined with independent component analy-sis. AJNR American Journal of Neuroradiology, 21,1629–1635.
Mostofsky, S. H., Burgess, M. P., & Gidley Larson,J. C. (2007). Increased motor cortex white matter vol-ume predicts motor impairment in autism. Brain, 130,2117–2122. doi:10.1093/brain/awm129
Mostofsky, S. H., & Ewen, J. B. (2011). Alteredconnectivity and action model formation inautism is autism. The Neuroscientist, 17, 437–448.doi:10.1177/1073858410392381
Mostofsky, S. H., Powell, S. K., Simmonds, D. J.,Goldberg, M. C., Caffo, B., & Pekar, J. J. (2009).Decreased connectivity and cerebellar activity inautism during motor task performance. Brain, 132,2413–2425. doi:10.1093/brain/awp088
Muller, R. A., Pierce, K., Abrose, J. B., Allen, G., &Courchesne, E. (2001). Atypical patterns of cerebralmotor activation in autism: A functional magneticresonance study. Biological Psychiatry, 49, 665–676.
Muller, T., Schafer, S., Kuhn, W., & Przuntek, H.(2000). Correlation between tapping and inserting ofpegs in Parkinson’s disease. The Canadian Journal ofNeurological Sciences, 27, 311–315.
Nair, A., Treiber, J. M., Shukla, D. K., Shih, P., &Müller, R. A. (2013). Impaired thalamocortical con-nectivity in autism spectrum disorder: A study offunctional and anatomical connectivity. Brain, 136,1942–1955.
Nobile, M., Perego, P., Piccinini, L., Mani, E., Rossi, A.,Bellina, M., & Molteni, M. (2011). Further evidenceof complex motor dysfunction in drug naive childrenwith autism using automatic motion analysis of gait.Autism, 15, 263–283. doi:10.1177/1362361309356929
Nussbaum, N. L., & Bigler, E. D. (1997). Halstead–Reitan neuropsychological test batteries for children.In C. R. Reynolds & E. Fletcher-Janzen (Eds.),
Handbook of clinical child neuropsychology. New York,NY: Plenum Press.
Oldfield, R. C. (1971). The assessment and analysisof handedness: The Edinburgh inventory. Neuro-psychologia, 9, 97–113.
Otten, M. L., Mikell, C. B., Youngerman, B. E., Liston,C., Sisti, M. B., Bruce, J. N., . . . McKhann, G. M.2nd. (2012). Motor deficits correlate with rest-ing state motor network connectivity in patientswith brain tumours. Brain, 135, 1017–1026.doi:10.1093/brain/aws041
Pedersen, S. W., Oberg, B., Larsson, L. E., & Lindval,B. (1997). Gait analysis, isokinetic muscle strengthmeasurement in patients with Parkinson’s disease.Scandinavian Journal of Rehabilitation Medicine, 29,67–74.
Pelphrey, K. A., Shultz, S., Hudac, C. M., & VanderWyk, B. C. (2011). Research review: Constraining het-erogeneity: The social brain and its development inautism spectrum disorder. Journal of Child Psychologyand Psychiatry, 52(6), 631–644.
Polsek, D., Jagatic, T., Cepanec, M., Hof, P. R., & Simic,G. (2011). Recent developments in neuropathol-ogy of autism spectrum disorders. TranslationalNeuroscience, 2(3), 256–264.
Qiu, A., Adler, M., Crocetti, D., Miller, M. I., &Mostofsky, S. H. (2010). Basal ganglia shapes pre-dict social, communication, and motor dysfunc-tions in boys with autism spectrum disorder. Journalof the American Academy of Child and AdolescentPsychiatry, 49, 539–551, e531–e534. doi:10.1016/j.jaac.2010.02.012
Rapin, I. (1991). Autistic children: Diagnosis and clinicalfeatures. Pediatrics, 87, 751–760.
Rapin, I. (1999). Autism in search of a home in the brain.Neurology, 52, 902–904.
Reitan, R. M., & Wolfson, D. (1986). The Halstead–Reitan neuropsychological test battery. InD. Wedding, A. M. Horton, Jr., & J. S. Webster(Eds.), The neuropsychology handbook: Behavioral andclinical perspectives (pp. 134–160). New York, NY:Springer Publishing.
Roessner, V., Wittfoth, M., August, J. M., Rothenberger,A., Baudewig, J., & Dechent, P. (2012). Fingertapping-related activation differences in treatment-naive pediatric Tourette syndrome: A comparison ofthe preferred and nonpreferred hand. Journal of ChildPsychology and Psychiatry, and Allied Disciplines.doi:10.1111/j.1469-7610.2012.02584.x
Rumsey, J. M., & Hamburger, S. D. (1988).Neuropsychological findings in high-functioningmen with infantile autism, residual state. Journalof Clinical and Experimental Neuropsychology, 10,201–221. doi:10.1080/01688638808408236
Sachdev, P., Hume, F., Toohey, P., & Doutney, C. (1996).Negative symptoms, cognitive dysfunction, tardiveakathisia and tardive dyskinesia. Acta PsychiatricaScandinavica, 93, 451–459.
Schear, J. M., & Sato, S. D. (1989). Effects of visual acuityand visual motor speed and dexterity on cognitive testperformance. Archives of Clinical Neuropsychology, 4,25–32.
Schultz, R. T., Klin, A., & Lombroso, P. J. (2002).Genetics of childhood disorders: XLIII. Autism,part 2: Neural foundations. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 41(10),1259.
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
MOTOR IMPAIRMENTS AND STRUCTURAL IMAGING IN AUTISM 881
Schulz, R., Park, C. H., Boudrias, M. H., Gerloff, C.,Hummel, F. C., & Ward, N. S. (2012). Assessingthe integrity of corticospinal pathways from pri-mary and secondary cortical motor areas after stroke.Stroke, 43, 2248–2251. doi:10.1161/STROKEAHA.112.662619
Stanford, M. S., & Barratt, E. S. (1996). Verbal skills,finger tapping, and cognitive tempo define a second-order factor of temporal information processing.Brain and Cognition, 31, 35–45.
Strauss, E., Sherman, E. S., & Spreen, O. (2006). A com-pendium of neuropsychological tests: Administration,norms, and commentary (3rd ed.). New York, NY:Oxford University Press.
Szatmari, P., Tuff, L., Finlayson, M. A., & Bartolucci,G. (1990). Asperger’s syndrome and autism:Neurocognitive aspects. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 29,130–136.
Tofts, P. (2003). Quantitative MRI of the brain: Measuringchanges caused by disease (P. Tofts, Ed.). Chichester:Wiley.
Travers, B. G., Powell, P. S., Klinger, L. G., & Klinger,M. R. (2012). Motor difficulties in autism spectrumdisorder: Linking symptom severity and postural sta-bility. Journal of Autism and Developmental Disorders.Advance online publication. doi:10.1007/s10803-012-1702-x
Triggs, W. J., Calvanio, R., Levine, M., Heaton, R. K.,& Heilman, K. M. (2000). Predicting hand prefer-ence with performance on motor tasks. Cortex, 36,679–689.
van Nuenen, B. F., Kuhtz-Buschbeck, J., Schulz, C.,Bloem, B. R., & Siebner, H. R. (2012). Weight-specificanticipatory coding of grip force in human dorsal
premotor cortex. The Journal of Neuroscience, 32,5272–5283. doi:10.1523/JNEUROSCI.5673-11.2012
Wechsler, D. (1991). Wechsler Intelligence Scale ForChildren–III (WISC–III). San Antonio, TX: ThePsychological Corporation.
Wechsler, D. (1997). Wechsler Adult Intelligence Scale–III (WAIS–III). San Antonio, TX: The PsychologicalCorporation.
Wechsler, D. (1999). Wechsler Abbreviated Scaleof Intelligence (WASI). San Antonio, TX: ThePsychological Corporation.
Weimer, A. K., Schatz, A. M., Lincoln, A., Ballantyne,A. O., & Trauner, D. A. (2001). “Motor” impairmentin Asperger syndrome: Evidence for a deficit in pro-prioception. Journal of Developmental and BehavioralPediatrics, 22, 92–101.
Weinstein, M., Ben-Sira, L., Levy, Y., Zachor, D. A.,Ben Itzhak, E., Artzi, M., . . . Ben Bashat, D. (2011).Abnormal white matter integrity in young childrenwith autism. Human Brain Mapping, 32, 534–543.doi:10.1002/hbm.21042
Williams, D. L., Goldstein, G., & Minshew, N. J.(2006). Neuropsychologic functioning in children withautism: Further evidence for disordered complexinformation-processing. Child Neuropsychology, 12,279–298. doi:10.1080/09297040600681190
Witt, S. T., Laird, A. R., & Meyerand, M. E. (2008).Functional neuroimaging correlates of finger-tappingtask variations: An ALE meta-analysis. NeuroImage,42, 343–356. doi:10.1016/j.neuroimage.2008.04.025
Zielinski, B. A., Anderson, J. S., Froehlich, A. L., Prigge,M. B., Nielsen, J. A., Cooperrider, J. R., . . . Lainhart,J. E. (2012). scMRI reveals large-scale brain networkabnormalities in autism. PLoS ONE, 7(11), e49172.doi:10.1371/journal.pone.0049172
Dow
nloa
ded
by [
24.1
0.22
2.25
4] a
t 13:
52 3
0 Se
ptem
ber
2014
Related Documents











