Thalamus & Related Systems 2 (2003) 103–113 Neuropsychiatric thalamocortical dysrhythmia: surgical implications D. Jeanmonod a,∗ , J. Schulman b , R. Ramirez b , R. Cancro c , M. Lanz d , A. Morel a , M. Magnin a , M. Siegemund a , E. Kronberg b , U. Ribary b , R. Llinas b,1 a Laboratory for Functional Neurosurgery, Neurosurgical Clinic, University Hospital, Zurich, Switzerland b Department of Physiology and Neuroscience, New York University School of Medicine, New York, NY, USA c Department of Psychiatry, New York University School of Medicine, New York, NY, USA d Psychiatry Center Hard, Zurich, Switzerland Accepted 22 November 2002 Abstract Neuropsychiatric surgery has had a long and complex history with examples of less than optimal surgical procedures implemented in wrong settings. Such past errors have raised important philosophical and ethical issues that remain with us for good reasons. However, the existence of enormous suffering due to chronic therapy-resistant disabling neuropsychiatric disorders compels a search for alternative surgical approaches based on a sound understanding of the underlying physiopathological mechanisms. We bring evidence, from single cell physiology and magnetoencephalography, for the existence of a set of neuropsychiatric disorders characterized by localized and pro- tracted low frequency spontaneous recurrent activation of the thalamocortical system. This condition, labeled thalamocortical dysrhythmia, underlies certain chronic psychotic, affective, obsessive compulsive, anxiety and impulse control disorders. Considering the central role of recurrent oscillatory thalamocortical properties in the generation of normal hemispheric functions, we propose a surgical approach that provides a reestablishment of normal thalamocortical oscillations without reduction of cortical tissue and its specific thalamic connectivity. It consists of small strategically placed pallidal and medial thalamic lesions that serve to make subcritical the increased low frequency thalamocortical recurrent network activity. This result is attained via reduction of both thalamic overinhibition and low frequency over- synchronization. Thalamic disinhibition is obtained by a lesion in the anterior medial paralimbic pallidum. The medial thalamic lesion is localized in the posterior part of the central lateral nucleus, where a large majority of cells have been shown to be locked in low frequency production and to have lost their normal activation patterns. We present here our experience with 11 patients, including clinical follow ups and pre- and postsurgical magnetoencephalographic studies. The evidence speaks (1) for a benign and efficient surgical approach, and (2) for the relevance of the patient’s presurgical cognitive and social settings, making them more or less prone to postoperative psychoreactive manifestations upon rekindling of personal goals and social reentry. © 2003 Elsevier Science Ltd. All rights reserved. Keywords: Low threshold calcium spike bursts; Obsessive compulsive disorder; Psychosis; Anterior medial pallidotomy; Central lateral thalamotomy 1. Introduction After the questionable and inordinately wide application of the prefrontal lobotomy (Moniz, 1936; Freeman, 1948) in the first half of the twentieth century, many groups real- ized the necessity of confining surgical interventions to the paralimbic (or mesocortical) domain (Mesulam, 1985). This gave rise to the three main stereotactic operations still in use today in view of their efficiency and limited side effects: (1) ∗ Corresponding author. Sternwartstrasse 6, 8091 Zurich, Switzerland. Tel.: +41-1-2552684; fax: +41-1-2558946. E-mail addresses: [email protected] (D. Jeanmonod), [email protected] (R. Llinas). 1 Co-corresponding author. Present address: 550 First Avenue MSB-442, New York, NY 10016, USA. Tel.: +1-212-263-5415; fax: +1-212-689-9060. the anterior cingulotomy (Ballantine et al., 1977), (2) the subcaudate tractotomy (Knight, 1973) and (3) the anterior capsulotomy (Bingley et al., 1973). These three procedures entail an interruption of the thalamocortical paralimbic frontal network. Such surgical approaches have been effi- cient against major depression and obsessive compulsive dis- order (OCD), but not against psychosis. Very early however, Spiegel and Wycis (1952/1962) had explored the possibili- ties of stereotactic interventions in the mediodorsal nucleus of the thalamus and described positive results in psychotic patients. There are both older and more recent data demonstrating a physiopathological and histological involvement of paralim- bic cortical areas and their corresponding specific thalamic partner, the mediodorsal nucleus, in the generation of the neuropsychiatric disorders. Indeed, electroencephalographic 1472-9288/03/$ – see front matter © 2003 Elsevier Science Ltd. All rights reserved. doi:10.1016/S1472-9288(03)00010-4

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Thalamus & Related Systems 2 (2003) 103–113
Neuropsychiatric thalamocortical dysrhythmia: surgical implications
D. Jeanmonoda,∗, J. Schulmanb, R. Ramirezb, R. Cancroc, M. Lanzd, A. Morela, M. Magnina,M. Siegemunda, E. Kronbergb, U. Ribaryb, R. Llinasb,1
a Laboratory for Functional Neurosurgery, Neurosurgical Clinic, University Hospital, Zurich, Switzerlandb Department of Physiology and Neuroscience, New York University School of Medicine, New York, NY, USA
c Department of Psychiatry, New York University School of Medicine, New York, NY, USAd Psychiatry Center Hard, Zurich, Switzerland
Accepted 22 November 2002
Abstract
Neuropsychiatric surgery has had a long and complex history with examples of less than optimal surgical procedures implemented inwrong settings. Such past errors have raised important philosophical and ethical issues that remain with us for good reasons. However,the existence of enormous suffering due to chronic therapy-resistant disabling neuropsychiatric disorders compels a search for alternativesurgical approaches based on a sound understanding of the underlying physiopathological mechanisms. We bring evidence, from singlecell physiology and magnetoencephalography, for the existence of a set of neuropsychiatric disorders characterized by localized and pro-tracted low frequency spontaneous recurrent activation of the thalamocortical system. This condition, labeled thalamocortical dysrhythmia,underlies certain chronic psychotic, affective, obsessive compulsive, anxiety and impulse control disorders. Considering the central roleof recurrent oscillatory thalamocortical properties in the generation of normal hemispheric functions, we propose a surgical approach thatprovides a reestablishment of normal thalamocortical oscillations without reduction of cortical tissue and its specific thalamic connectivity.It consists of small strategically placed pallidal and medial thalamic lesions that serve to make subcritical the increased low frequencythalamocortical recurrent network activity. This result is attained via reduction of both thalamic overinhibition and low frequency over-synchronization. Thalamic disinhibition is obtained by a lesion in the anterior medial paralimbic pallidum. The medial thalamic lesion islocalized in the posterior part of the central lateral nucleus, where a large majority of cells have been shown to be locked in low frequencyproduction and to have lost their normal activation patterns. We present here our experience with 11 patients, including clinical follow upsand pre- and postsurgical magnetoencephalographic studies. The evidence speaks (1) for a benign and efficient surgical approach, and (2)for the relevance of the patient’s presurgical cognitive and social settings, making them more or less prone to postoperative psychoreactivemanifestations upon rekindling of personal goals and social reentry.© 2003 Elsevier Science Ltd. All rights reserved.
Keywords: Low threshold calcium spike bursts; Obsessive compulsive disorder; Psychosis; Anterior medial pallidotomy; Central lateral thalamotomy
1. Introduction
After the questionable and inordinately wide applicationof the prefrontal lobotomy (Moniz, 1936; Freeman, 1948)in the first half of the twentieth century, many groups real-ized the necessity of confining surgical interventions to theparalimbic (or mesocortical) domain (Mesulam, 1985). Thisgave rise to the three main stereotactic operations still in usetoday in view of their efficiency and limited side effects: (1)
∗ Corresponding author. Sternwartstrasse 6, 8091 Zurich, Switzerland.Tel.: +41-1-2552684; fax:+41-1-2558946.E-mail addresses: [email protected] (D. Jeanmonod),[email protected] (R. Llinas).
1 Co-corresponding author. Present address: 550 First Avenue MSB-442,New York, NY 10016, USA. Tel.:+1-212-263-5415;fax: +1-212-689-9060.
the anterior cingulotomy (Ballantine et al., 1977), (2) thesubcaudate tractotomy (Knight, 1973) and (3) the anteriorcapsulotomy (Bingley et al., 1973). These three proceduresentail an interruption of the thalamocortical paralimbicfrontal network. Such surgical approaches have been effi-cient against major depression and obsessive compulsive dis-order (OCD), but not against psychosis. Very early however,Spiegel and Wycis (1952/1962)had explored the possibili-ties of stereotactic interventions in the mediodorsal nucleusof the thalamus and described positive results in psychoticpatients.
There are both older and more recent data demonstrating aphysiopathological and histological involvement of paralim-bic cortical areas and their corresponding specific thalamicpartner, the mediodorsal nucleus, in the generation of theneuropsychiatric disorders. Indeed, electroencephalographic
1472-9288/03/$ – see front matter © 2003 Elsevier Science Ltd. All rights reserved.doi:10.1016/S1472-9288(03)00010-4
104 D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113
(EEG) (Spiegel and Wycis, 1950; Heath, 1954; Prichep andJohn, 1992; Pascual-Marqui et al., 1999; Sponheim et al.,2000), positron emission tomographic (PET) (Buchsbaumet al., 2002; Hazlett et al., 1999), histological (Bogerts,1984; Shenton et al., 2001) and radiological (Shenton et al.,2001) studies indicate spiking activities, increased lowfrequencies, hypometabolism as well as histopathologicaland magnetic resonance imaging (MRI) changes in thesedomains.
Our surgical approach is based on two premises: (1) thecentral role of the oscillatory thalamocortical propertiesin the generation of normal hemispheric functions (Llinaset al., 1998), and (2) the existence, as a physiopathologi-cal basis to neuropsychiatric disorders, of a thalamocorti-cal dysrhythmia (TCD) evidenced by thalamic single cellrecordings (Jeanmonod et al., 1996, 2001) and magnetoen-cephalography (MEG) (Llinas et al., 1999, 2001; Ribaryet al., 2000; Schulman et al., 2001) and characterized byincreased low frequency generation. In this context, weelected to normalize low frequency production without af-fecting the anatomical integrity of the functional cognitivethalamocortical network.
The goal of this paper is to describe this approachat the surgical, clinical and magnetoencephalographiclevels.
2. Methods
2.1. Patient group
All patients (n = 11) suffered from chronic therapy-resistant neuropsychiatric disorders including at least one,and often several, of the following clinical manifestations:(a) psychotic hallucinatory/delusional disorder (four pa-tients), (b) OCD (eight patients), (c) major (or endogenous)depression (seven patients) or bipolar mood disorder (twopatients), (d) anxiety disorder (seven patients), and (e) im-pulse control disorder (ICD, four patients). The presenceof a high percentage of complex atypical neuropsychiatricsyndromes is due, we think, to the fact that these patientsexhibited particularly resistant disease forms, related towidespread and strong TCD mechanisms, and were thus atthe forefront in terms of surgical indication. Available drugtreatments were used without success in all of them, andelectroconvulsive therapy (ECT) was applied in four pa-tients before being referred to us. In addition, three patientscame to us following prior unsuccessful interventions. Oneof them had a gamma knife capsulotomy, the second agamma knife thalamotomy and the third one a vagal nervestimulator. The patients, seven men and four women, rangedin age between 21 and 59 years (with a mean of 35 years)at the time of the first surgery. The duration of the diseaseprior to the first surgery ranged between 6 and 21 years,with a mean of 15 years. Postoperative relief percentageswere given by the patients themselves.
2.2. Surgical strategy
We have applied the following criteria for surgical in-dication: (a) a protracted evolution of the disease (manyyears), (b) resistance to pharmacological and other conser-vative therapies, and (c) a major impact of the symptoms onthe patient’s quality of life.
Two surgical targets have been developed, the central lat-eral thalamotomy (CLT) and the anterior medial pallidotomy(AMP). The CLT targets the posterior part of the centrallateral nucleus (CL) and its stereotactic coordinates are an-teroposteriorly 2 mm posterior to the posterior commissure,mediolaterally 6 mm lateral to the border of the third ventri-cle and dorsoventrally at the level of the intercommissuralplane. The target is reached using an anteroposterior angleof 60◦ and a mediolateral angle of 5–10◦. The CLT lesionmeasures 4 mm diameter over 12–14 mm length.
The AMP, as its name implies, targets the paralimbic an-terior and medial pallidum and its stereotactic coordinatesare anteroposteriorly 4 mm posterior to the anterior com-missure, mediolaterally 12 mm lateral to the ventricular bor-der and dorsoventrally 2 mm ventral to the intercommissuralplane. It is reached using an anteroposterior angle of 55◦and a mediolateral one of 20◦. The AMP lesion measures4 mm diameter over 6 mm length.
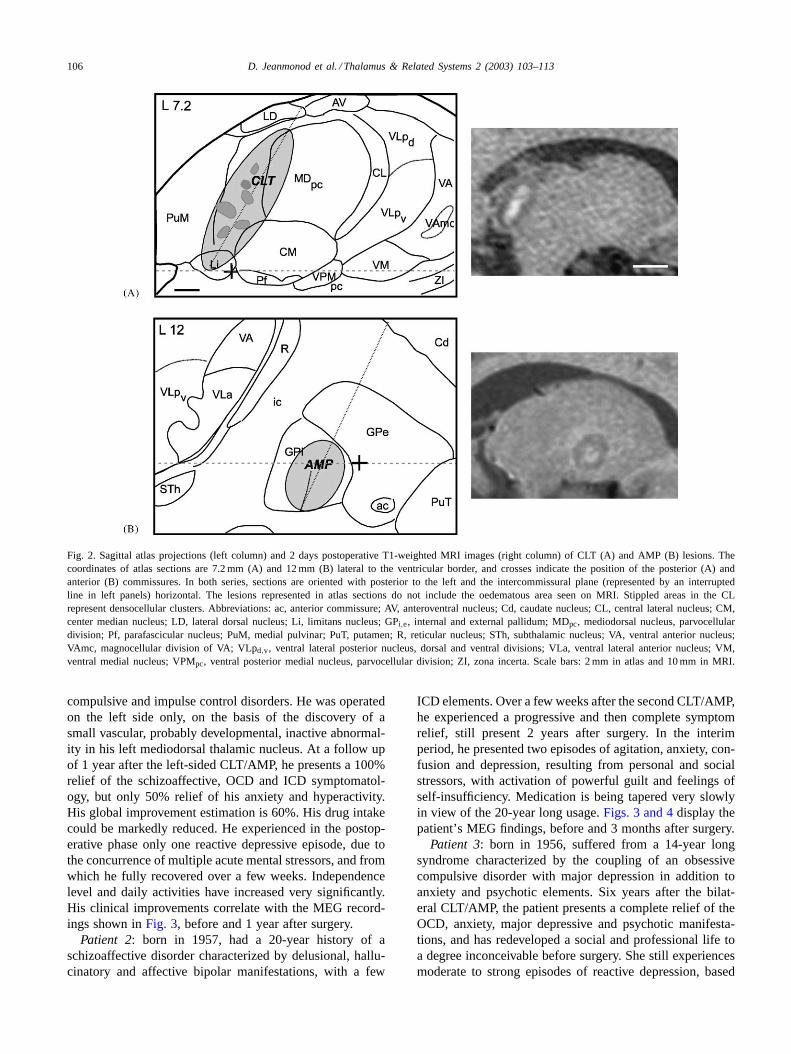
A physiological confirmation of target localizations withingiven geometrical confines is provided by microelectroderecording (Fig. 1) as well as by macrostimulation.Fig. 2displays the CLT and AMP lesions as seen on our stereotacticatlas (Morel et al., 1997) and MRI.
The general surgical goal was a bilateral coupling of CLTand AMP. We report on five patients with such full surgi-cal treatment, two patients operated only on one side on thebasis of the discovery of a unilateral thalamic causal lesion(in this sense and till evidence for the contrary fully oper-ated), two patients partly operated (one with a left CLT/AMPand the other with a bilateral CLT) and two Parkinsonianpatients displaying endogenous neuropsychiatric manifesta-tions (anxiodepressive episodes and ICD plus depression)and treated by a unilateral AMP.
2.3. Magnetoencephalography
Pre- and postoperative MEG recordings were performedon three patients. Analyses included power spectra and co-herence studies (Llinas et al., 1999, 2001) as well as mag-netic source imaging.
A whole-head 148-channel MEG system (4D Neuroimag-ing, San Diego, CA) was used for all patients. Spontaneousbrain activity was continuously recorded for 5 min whilethe patient reclined and was asked to stay alert with eyesclosed or eyes open. The bandpass was 0.1–100 Hz and thesample rate 508 Hz. The electrocardiogram was simultane-ously recorded digitally for off-line heartbeat artifact rejec-tion. Spectral analysis of 5 s windows using the multitapertechnique and cross-correlation between spectral amplitudes
D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113 105
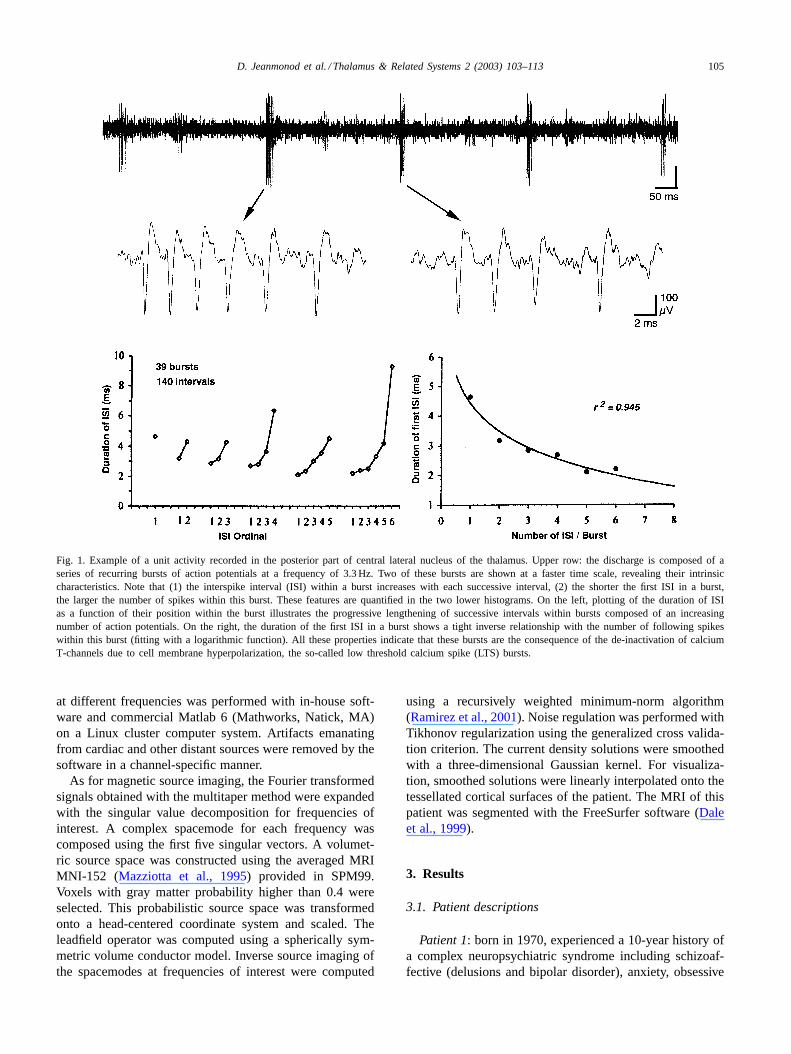
Fig. 1. Example of a unit activity recorded in the posterior part of central lateral nucleus of the thalamus. Upper row: the discharge is composed of aseries of recurring bursts of action potentials at a frequency of 3.3 Hz. Two of these bursts are shown at a faster time scale, revealing their intrinsiccharacteristics. Note that (1) the interspike interval (ISI) within a burst increases with each successive interval, (2) the shorter the first ISI in aburst,the larger the number of spikes within this burst. These features are quantified in the two lower histograms. On the left, plotting of the duration of ISIas a function of their position within the burst illustrates the progressive lengthening of successive intervals within bursts composed of an increasingnumber of action potentials. On the right, the duration of the first ISI in a burst shows a tight inverse relationship with the number of following spikeswithin this burst (fitting with a logarithmic function). All these properties indicate that these bursts are the consequence of the de-inactivation of calciumT-channels due to cell membrane hyperpolarization, the so-called low threshold calcium spike (LTS) bursts.
at different frequencies was performed with in-house soft-ware and commercial Matlab 6 (Mathworks, Natick, MA)on a Linux cluster computer system. Artifacts emanatingfrom cardiac and other distant sources were removed by thesoftware in a channel-specific manner.
As for magnetic source imaging, the Fourier transformedsignals obtained with the multitaper method were expandedwith the singular value decomposition for frequencies ofinterest. A complex spacemode for each frequency wascomposed using the first five singular vectors. A volumet-ric source space was constructed using the averaged MRIMNI-152 (Mazziotta et al., 1995) provided in SPM99.Voxels with gray matter probability higher than 0.4 wereselected. This probabilistic source space was transformedonto a head-centered coordinate system and scaled. Theleadfield operator was computed using a spherically sym-metric volume conductor model. Inverse source imaging ofthe spacemodes at frequencies of interest were computed
using a recursively weighted minimum-norm algorithm(Ramirez et al., 2001). Noise regulation was performed withTikhonov regularization using the generalized cross valida-tion criterion. The current density solutions were smoothedwith a three-dimensional Gaussian kernel. For visualiza-tion, smoothed solutions were linearly interpolated onto thetessellated cortical surfaces of the patient. The MRI of thispatient was segmented with the FreeSurfer software (Daleet al., 1999).
3. Results
3.1. Patient descriptions
Patient 1: born in 1970, experienced a 10-year history ofa complex neuropsychiatric syndrome including schizoaf-fective (delusions and bipolar disorder), anxiety, obsessive
106 D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113
Fig. 2. Sagittal atlas projections (left column) and 2 days postoperative T1-weighted MRI images (right column) of CLT (A) and AMP (B) lesions. Thecoordinates of atlas sections are 7.2 mm (A) and 12 mm (B) lateral to the ventricular border, and crosses indicate the position of the posterior (A) andanterior (B) commissures. In both series, sections are oriented with posterior to the left and the intercommissural plane (represented by an interruptedline in left panels) horizontal. The lesions represented in atlas sections do not include the oedematous area seen on MRI. Stippled areas in the CLrepresent densocellular clusters. Abbreviations: ac, anterior commissure; AV, anteroventral nucleus; Cd, caudate nucleus; CL, central lateral nucleus; CM,center median nucleus; LD, lateral dorsal nucleus; Li, limitans nucleus; GPi,e, internal and external pallidum; MDpc, mediodorsal nucleus, parvocellulardivision; Pf, parafascicular nucleus; PuM, medial pulvinar; PuT, putamen; R, reticular nucleus; STh, subthalamic nucleus; VA, ventral anterior nucleus;VAmc, magnocellular division of VA; VLpd,v, ventral lateral posterior nucleus, dorsal and ventral divisions; VLa, ventral lateral anterior nucleus; VM,ventral medial nucleus; VPMpc, ventral posterior medial nucleus, parvocellular division; ZI, zona incerta. Scale bars: 2 mm in atlas and 10 mm in MRI.
compulsive and impulse control disorders. He was operatedon the left side only, on the basis of the discovery of asmall vascular, probably developmental, inactive abnormal-ity in his left mediodorsal thalamic nucleus. At a follow upof 1 year after the left-sided CLT/AMP, he presents a 100%relief of the schizoaffective, OCD and ICD symptomatol-ogy, but only 50% relief of his anxiety and hyperactivity.His global improvement estimation is 60%. His drug intakecould be markedly reduced. He experienced in the postop-erative phase only one reactive depressive episode, due tothe concurrence of multiple acute mental stressors, and fromwhich he fully recovered over a few weeks. Independencelevel and daily activities have increased very significantly.His clinical improvements correlate with the MEG record-ings shown inFig. 3, before and 1 year after surgery.
Patient 2: born in 1957, had a 20-year history of aschizoaffective disorder characterized by delusional, hallu-cinatory and affective bipolar manifestations, with a few
ICD elements. Over a few weeks after the second CLT/AMP,he experienced a progressive and then complete symptomrelief, still present 2 years after surgery. In the interimperiod, he presented two episodes of agitation, anxiety, con-fusion and depression, resulting from personal and socialstressors, with activation of powerful guilt and feelings ofself-insufficiency. Medication is being tapered very slowlyin view of the 20-year long usage.Figs. 3 and 4display thepatient’s MEG findings, before and 3 months after surgery.
Patient 3: born in 1956, suffered from a 14-year longsyndrome characterized by the coupling of an obsessivecompulsive disorder with major depression in addition toanxiety and psychotic elements. Six years after the bilat-eral CLT/AMP, the patient presents a complete relief of theOCD, anxiety, major depressive and psychotic manifesta-tions, and has redeveloped a social and professional life toa degree inconceivable before surgery. She still experiencesmoderate to strong episodes of reactive depression, based
D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113 107
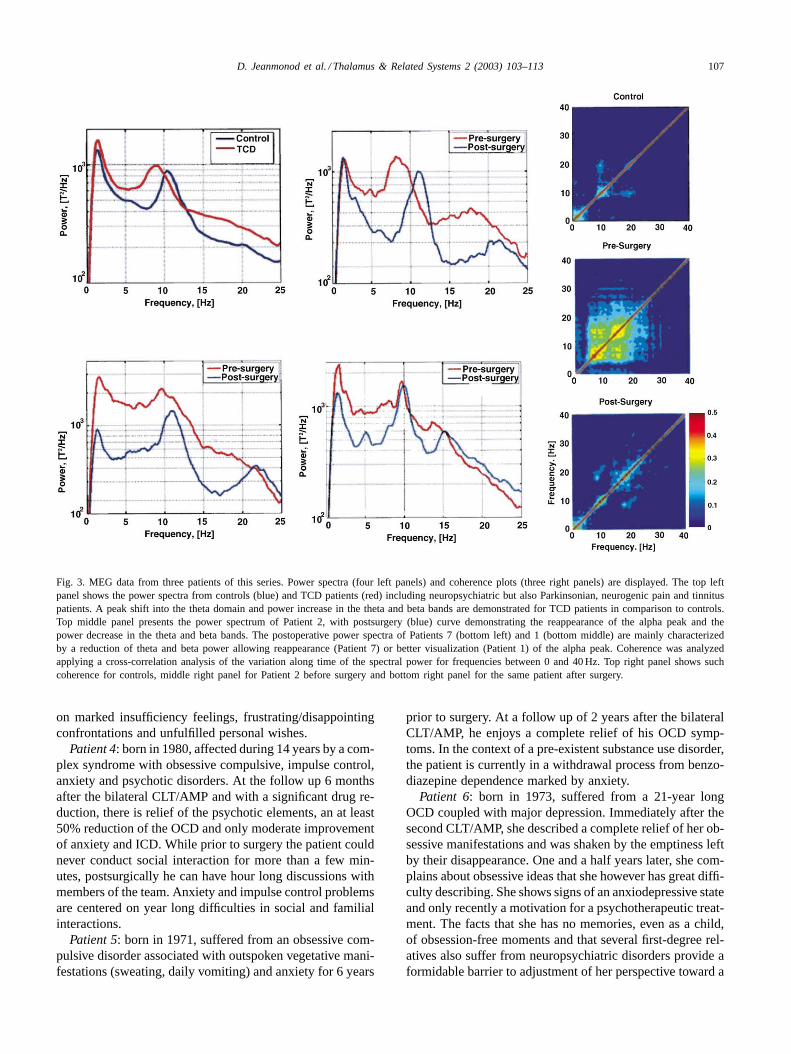
Fig. 3. MEG data from three patients of this series. Power spectra (four left panels) and coherence plots (three right panels) are displayed. The top leftpanel shows the power spectra from controls (blue) and TCD patients (red) including neuropsychiatric but also Parkinsonian, neurogenic pain and tinnituspatients. A peak shift into the theta domain and power increase in the theta and beta bands are demonstrated for TCD patients in comparison to controls.Top middle panel presents the power spectrum of Patient 2, with postsurgery (blue) curve demonstrating the reappearance of the alpha peak and thepower decrease in the theta and beta bands. The postoperative power spectra of Patients 7 (bottom left) and 1 (bottom middle) are mainly characterizedby a reduction of theta and beta power allowing reappearance (Patient 7) or better visualization (Patient 1) of the alpha peak. Coherence was analyzedapplying a cross-correlation analysis of the variation along time of the spectral power for frequencies between 0 and 40 Hz. Top right panel shows suchcoherence for controls, middle right panel for Patient 2 before surgery and bottom right panel for the same patient after surgery.
on marked insufficiency feelings, frustrating/disappointingconfrontations and unfulfilled personal wishes.
Patient 4: born in 1980, affected during 14 years by a com-plex syndrome with obsessive compulsive, impulse control,anxiety and psychotic disorders. At the follow up 6 monthsafter the bilateral CLT/AMP and with a significant drug re-duction, there is relief of the psychotic elements, an at least50% reduction of the OCD and only moderate improvementof anxiety and ICD. While prior to surgery the patient couldnever conduct social interaction for more than a few min-utes, postsurgically he can have hour long discussions withmembers of the team. Anxiety and impulse control problemsare centered on year long difficulties in social and familialinteractions.
Patient 5: born in 1971, suffered from an obsessive com-pulsive disorder associated with outspoken vegetative mani-festations (sweating, daily vomiting) and anxiety for 6 years
prior to surgery. At a follow up of 2 years after the bilateralCLT/AMP, he enjoys a complete relief of his OCD symp-toms. In the context of a pre-existent substance use disorder,the patient is currently in a withdrawal process from benzo-diazepine dependence marked by anxiety.
Patient 6: born in 1973, suffered from a 21-year longOCD coupled with major depression. Immediately after thesecond CLT/AMP, she described a complete relief of her ob-sessive manifestations and was shaken by the emptiness leftby their disappearance. One and a half years later, she com-plains about obsessive ideas that she however has great diffi-culty describing. She shows signs of an anxiodepressive stateand only recently a motivation for a psychotherapeutic treat-ment. The facts that she has no memories, even as a child,of obsession-free moments and that several first-degree rel-atives also suffer from neuropsychiatric disorders provide aformidable barrier to adjustment of her perspective toward a
108 D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113
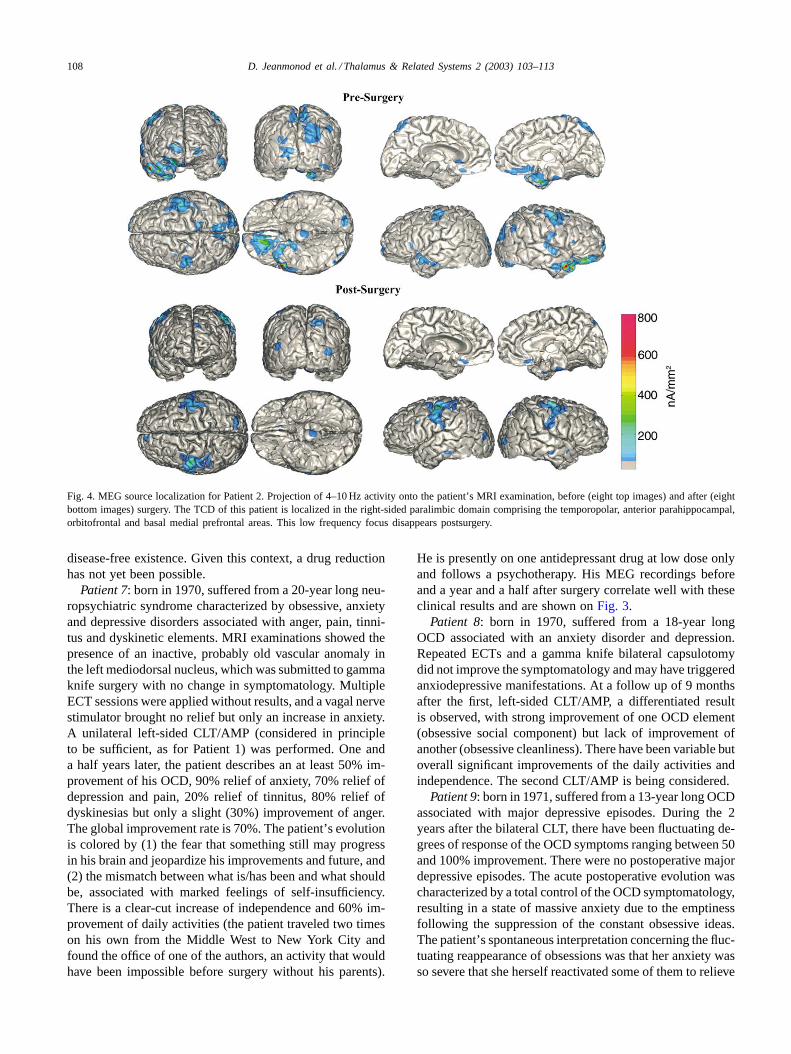
Fig. 4. MEG source localization for Patient 2. Projection of 4–10 Hz activity onto the patient’s MRI examination, before (eight top images) and after (eightbottom images) surgery. The TCD of this patient is localized in the right-sided paralimbic domain comprising the temporopolar, anterior parahippocampal,orbitofrontal and basal medial prefrontal areas. This low frequency focus disappears postsurgery.
disease-free existence. Given this context, a drug reductionhas not yet been possible.
Patient 7: born in 1970, suffered from a 20-year long neu-ropsychiatric syndrome characterized by obsessive, anxietyand depressive disorders associated with anger, pain, tinni-tus and dyskinetic elements. MRI examinations showed thepresence of an inactive, probably old vascular anomaly inthe left mediodorsal nucleus, which was submitted to gammaknife surgery with no change in symptomatology. MultipleECT sessions were applied without results, and a vagal nervestimulator brought no relief but only an increase in anxiety.A unilateral left-sided CLT/AMP (considered in principleto be sufficient, as for Patient 1) was performed. One anda half years later, the patient describes an at least 50% im-provement of his OCD, 90% relief of anxiety, 70% relief ofdepression and pain, 20% relief of tinnitus, 80% relief ofdyskinesias but only a slight (30%) improvement of anger.The global improvement rate is 70%. The patient’s evolutionis colored by (1) the fear that something still may progressin his brain and jeopardize his improvements and future, and(2) the mismatch between what is/has been and what shouldbe, associated with marked feelings of self-insufficiency.There is a clear-cut increase of independence and 60% im-provement of daily activities (the patient traveled two timeson his own from the Middle West to New York City andfound the office of one of the authors, an activity that wouldhave been impossible before surgery without his parents).
He is presently on one antidepressant drug at low dose onlyand follows a psychotherapy. His MEG recordings beforeand a year and a half after surgery correlate well with theseclinical results and are shown onFig. 3.
Patient 8: born in 1970, suffered from a 18-year longOCD associated with an anxiety disorder and depression.Repeated ECTs and a gamma knife bilateral capsulotomydid not improve the symptomatology and may have triggeredanxiodepressive manifestations. At a follow up of 9 monthsafter the first, left-sided CLT/AMP, a differentiated resultis observed, with strong improvement of one OCD element(obsessive social component) but lack of improvement ofanother (obsessive cleanliness). There have been variable butoverall significant improvements of the daily activities andindependence. The second CLT/AMP is being considered.
Patient 9: born in 1971, suffered from a 13-year long OCDassociated with major depressive episodes. During the 2years after the bilateral CLT, there have been fluctuating de-grees of response of the OCD symptoms ranging between 50and 100% improvement. There were no postoperative majordepressive episodes. The acute postoperative evolution wascharacterized by a total control of the OCD symptomatology,resulting in a state of massive anxiety due to the emptinessfollowing the suppression of the constant obsessive ideas.The patient’s spontaneous interpretation concerning the fluc-tuating reappearance of obsessions was that her anxiety wasso severe that she herself reactivated some of them to relieve
D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113 109
her inner tension. This psychodynamic context was compli-cated by the presence of an excess in self-demands, to com-ply with a very strict and perfectionist picture of herself.At the moment, we await complementary evidence to betterascertain the necessity of the bilateral AMP.
Patient 10: born in 1937, suffered in the context of aParkinsonian disease, from a 16-year long neuropsychiatricdepressive and impulse control disorder. For 5 years after aright-sided AMP coupled to a subthalamotomy to alleviatehis motor syndrome, the patient presented a complete reliefof both motor and neuropsychiatric symptoms. Recently, dis-ease progression at both motor and neuropsychiatric levelsposes the question of a surgical restabilization of the otherhemisphere.
Patient 11: born in 1944, suffered in the context of aParkinsonian disease from a 13-year long major depressivedisorder characterized by unmotivated abrupt anxiodepres-sive episodes. He presented a 80–100% relief of this dis-order during a year and a half after a left-sided CLT/AMPcoupled to a pallidothalamic tractotomy (Jeanmonod et al.,2001). Like for the previous patient, disease progression atboth motor and neuropsychiatric levels raises the possibilityof a right-sided intervention.
Summarizing (seeTable 1), all patients demonstratedsignificant to complete relief from their neuropsychiatricailments. We observed the following postoperative reactivemanifestations: (1) anxiety (one patient), (2) anxiodepr-essive state (three patients), (3) anxiety and non-acceptance/frustration (three patients), and (4) frustration and de-pression (one patient). A conceptual rigidity with lack ofadaptation to the new situation was seen in two patients.
3.2. Magnetoencephalographic data
Preoperative MEG recordings demonstrated a marked in-crease of power in the theta domain (4–8 Hz), with the pres-ence of a variable number of more or less well identified
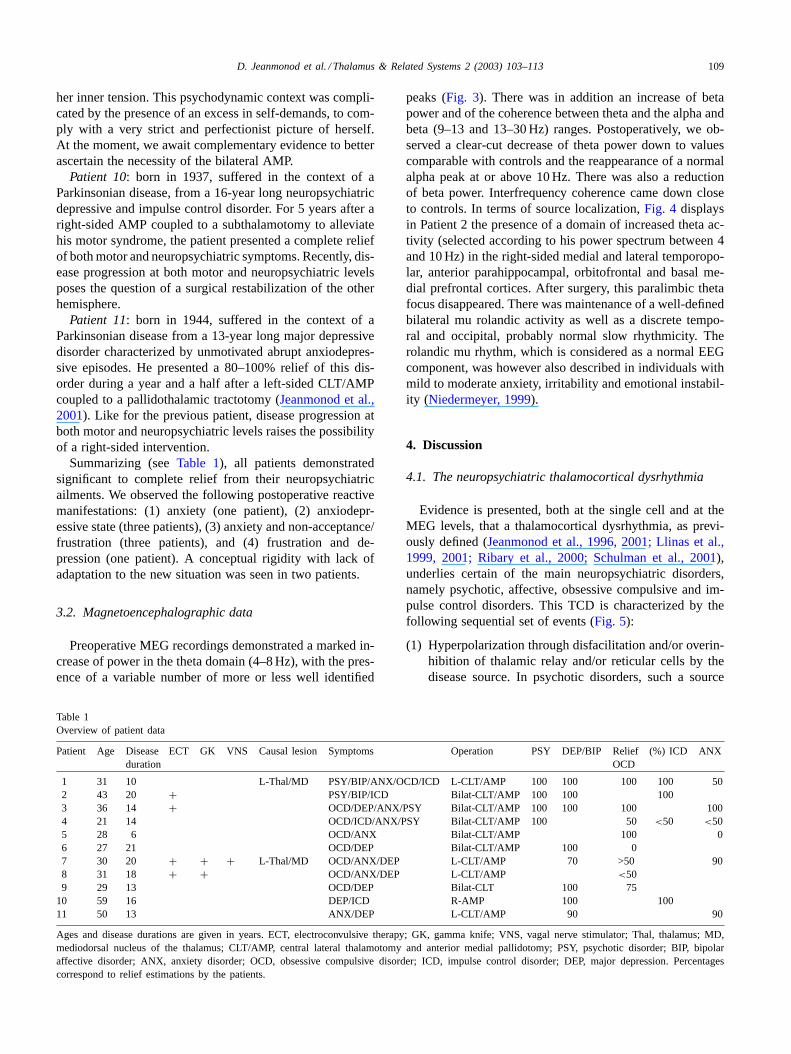
Table 1Overview of patient data
Patient Age Diseaseduration
ECT GK VNS Causal lesion Symptoms Operation PSY DEP/BIP ReliefOCD
(%) ICD ANX
1 31 10 L-Thal/MD PSY/BIP/ANX/OCD/ICD L-CLT/AMP 100 100 100 100 502 43 20 + PSY/BIP/ICD Bilat-CLT/AMP 100 100 1003 36 14 + OCD/DEP/ANX/PSY Bilat-CLT/AMP 100 100 100 1004 21 14 OCD/ICD/ANX/PSY Bilat-CLT/AMP 100 50 <50 <505 28 6 OCD/ANX Bilat-CLT/AMP 100 06 27 21 OCD/DEP Bilat-CLT/AMP 100 07 30 20 + + + L-Thal/MD OCD/ANX/DEP L-CLT/AMP 70 >50 908 31 18 + + OCD/ANX/DEP L-CLT/AMP <509 29 13 OCD/DEP Bilat-CLT 100 75
10 59 16 DEP/ICD R-AMP 100 10011 50 13 ANX/DEP L-CLT/AMP 90 90
Ages and disease durations are given in years. ECT, electroconvulsive therapy; GK, gamma knife; VNS, vagal nerve stimulator; Thal, thalamus; MD,mediodorsal nucleus of the thalamus; CLT/AMP, central lateral thalamotomy and anterior medial pallidotomy; PSY, psychotic disorder; BIP, bipolaraffective disorder; ANX, anxiety disorder; OCD, obsessive compulsive disorder; ICD, impulse control disorder; DEP, major depression. Percentagescorrespond to relief estimations by the patients.
peaks (Fig. 3). There was in addition an increase of betapower and of the coherence between theta and the alpha andbeta (9–13 and 13–30 Hz) ranges. Postoperatively, we ob-served a clear-cut decrease of theta power down to valuescomparable with controls and the reappearance of a normalalpha peak at or above 10 Hz. There was also a reductionof beta power. Interfrequency coherence came down closeto controls. In terms of source localization,Fig. 4 displaysin Patient 2 the presence of a domain of increased theta ac-tivity (selected according to his power spectrum between 4and 10 Hz) in the right-sided medial and lateral temporopo-lar, anterior parahippocampal, orbitofrontal and basal me-dial prefrontal cortices. After surgery, this paralimbic thetafocus disappeared. There was maintenance of a well-definedbilateral mu rolandic activity as well as a discrete tempo-ral and occipital, probably normal slow rhythmicity. Therolandic mu rhythm, which is considered as a normal EEGcomponent, was however also described in individuals withmild to moderate anxiety, irritability and emotional instabil-ity (Niedermeyer, 1999).
4. Discussion
4.1. The neuropsychiatric thalamocortical dysrhythmia
Evidence is presented, both at the single cell and at theMEG levels, that a thalamocortical dysrhythmia, as previ-ously defined (Jeanmonod et al., 1996, 2001; Llinas et al.,1999, 2001; Ribary et al., 2000; Schulman et al., 2001),underlies certain of the main neuropsychiatric disorders,namely psychotic, affective, obsessive compulsive and im-pulse control disorders. This TCD is characterized by thefollowing sequential set of events (Fig. 5):
(1) Hyperpolarization through disfacilitation and/or overin-hibition of thalamic relay and/or reticular cells by thedisease source. In psychotic disorders, such a source
110 D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113
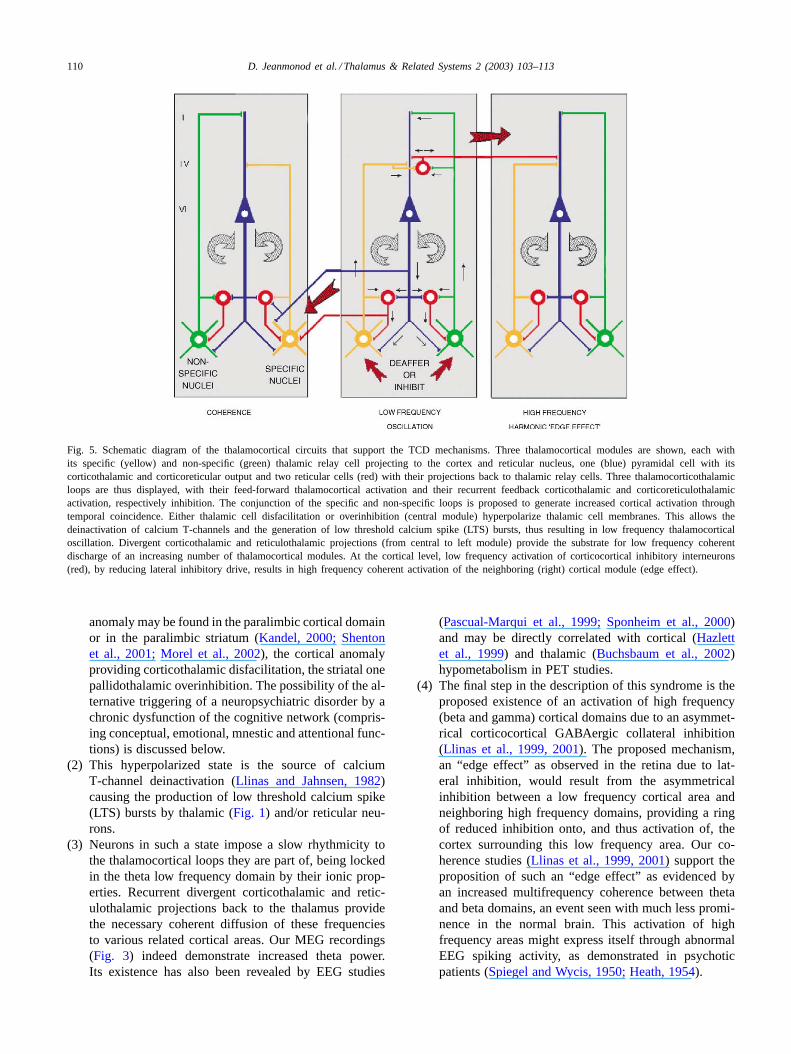
Fig. 5. Schematic diagram of the thalamocortical circuits that support the TCD mechanisms. Three thalamocortical modules are shown, each withits specific (yellow) and non-specific (green) thalamic relay cell projecting to the cortex and reticular nucleus, one (blue) pyramidal cell with itscorticothalamic and corticoreticular output and two reticular cells (red) with their projections back to thalamic relay cells. Three thalamocorticothalamicloops are thus displayed, with their feed-forward thalamocortical activation and their recurrent feedback corticothalamic and corticoreticulothalamicactivation, respectively inhibition. The conjunction of the specific and non-specific loops is proposed to generate increased cortical activation throughtemporal coincidence. Either thalamic cell disfacilitation or overinhibition (central module) hyperpolarize thalamic cell membranes. This allows thedeinactivation of calcium T-channels and the generation of low threshold calcium spike (LTS) bursts, thus resulting in low frequency thalamocorticaloscillation. Divergent corticothalamic and reticulothalamic projections (from central to left module) provide the substrate for low frequency coherentdischarge of an increasing number of thalamocortical modules. At the cortical level, low frequency activation of corticocortical inhibitory interneurons(red), by reducing lateral inhibitory drive, results in high frequency coherent activation of the neighboring (right) cortical module (edge effect).
anomaly may be found in the paralimbic cortical domainor in the paralimbic striatum (Kandel, 2000; Shentonet al., 2001; Morel et al., 2002), the cortical anomalyproviding corticothalamic disfacilitation, the striatal onepallidothalamic overinhibition. The possibility of the al-ternative triggering of a neuropsychiatric disorder by achronic dysfunction of the cognitive network (compris-ing conceptual, emotional, mnestic and attentional func-tions) is discussed below.
(2) This hyperpolarized state is the source of calciumT-channel deinactivation (Llinas and Jahnsen, 1982)causing the production of low threshold calcium spike(LTS) bursts by thalamic (Fig. 1) and/or reticular neu-rons.
(3) Neurons in such a state impose a slow rhythmicity tothe thalamocortical loops they are part of, being lockedin the theta low frequency domain by their ionic prop-erties. Recurrent divergent corticothalamic and retic-ulothalamic projections back to the thalamus providethe necessary coherent diffusion of these frequenciesto various related cortical areas. Our MEG recordings(Fig. 3) indeed demonstrate increased theta power.Its existence has also been revealed by EEG studies
(Pascual-Marqui et al., 1999; Sponheim et al., 2000)and may be directly correlated with cortical (Hazlettet al., 1999) and thalamic (Buchsbaum et al., 2002)hypometabolism in PET studies.
(4) The final step in the description of this syndrome is theproposed existence of an activation of high frequency(beta and gamma) cortical domains due to an asymmet-rical corticocortical GABAergic collateral inhibition(Llinas et al., 1999, 2001). The proposed mechanism,an “edge effect” as observed in the retina due to lat-eral inhibition, would result from the asymmetricalinhibition between a low frequency cortical area andneighboring high frequency domains, providing a ringof reduced inhibition onto, and thus activation of, thecortex surrounding this low frequency area. Our co-herence studies (Llinas et al., 1999, 2001) support theproposition of such an “edge effect” as evidenced byan increased multifrequency coherence between thetaand beta domains, an event seen with much less promi-nence in the normal brain. This activation of highfrequency areas might express itself through abnormalEEG spiking activity, as demonstrated in psychoticpatients (Spiegel and Wycis, 1950; Heath, 1954).

D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113 111
4.2. Surgical control of the thalamocortical dysrhythmia
Considering the central role of resonant oscillatory tha-lamocortical properties in the generation of normal hemi-spheric functions, we propose a surgical approach thatdoes not imply a reduction of functional thalamocorticalloops and is based on a regulation toward normality ofdysrhythmic thalamocortical oscillations, as documentedby our MEG data. For this purpose, we use small pallidaland medial thalamic lesions, the goal of which is to makesubcritical the increased low frequency thalamocortical gen-eration, in other words to move the dynamic properties ofthe system away from the increased low frequency coherentactivity. The CLT has as a goal a reduction of low frequencyoveramplification and oversynchronization, which can beaccomplished by a carefully placed and restricted lesion inthe medial thalamus. A similar if less well defined procedurewas known as medial thalamotomy since the dawn of stereo-tactic neurosurgery (Hécaen et al., 1949). The rationaleand general results of this operation are in full accordancewith long standing electrophysiological studies (Morisonand Dempsey, 1942) demonstrating a cortical recruitingresponse during low frequency stimulation of the medialthalamus. In addition, the thalamic non-specific system hasbeen shown to serve as a temporal coincidence activatorwhen summed with the thalamic specific input to the samecortical site (Llinas et al., 2002). We have taken advantageof physiopathological data in order to focus our medial tha-lamotomy target on the posterior part of the CL, where morethan 95% of the cells produced spontaneous LTS bursts(Fig. 1) and/or were unresponsive to stimuli (Jeanmonodet al., 1996). By doing so we restrict the lesion to the af-fected site and spare the other medial thalamic subnuclei,which, over time, seem to have taken over the function orig-inally fulfilled by CL. This is a very reasonable conjecturegiven the fact that patients experience no obvious reductionin sensory, motor or cognitive abilities following CLT. Thesecond target, the AMP, addresses the issue of reducingthalamic excess inhibition. In the case of neuropsychiatricdisorders, this reduction in inhibition (or disinhibition) is at-tained by targeting the paralimbic anterior internal pallidum(Morel et al., 2002).
The results presented here for 11 patients unequivocallydemonstrate that this surgical approach has significant ther-apeutic value against symptoms pertaining to psychotic,obsessive compulsive, major depressive, bipolar and im-pulse control disorders. There is however a clear-cut limitconcerning reactive, as opposed to endogenous, symp-toms in the domains of anxiety, depression and frustration(see later). Postoperative reactive decompensations are un-derstandable by the fact that the disinhibitory approachpresented here may result, in the acute postoperative pe-riod, in a momentary hyperactive phase. This conditionserves to emphasize the fundamental difference betweenthe procedure described here and the other available surgi-cal approaches, such as capsulotomies, cingulotomies and
subcaudate tractotomies, in which the goal is a reduction ofcortical activity through thalamocortical disconnection.
As expected given the nature of the lesions, we did not ob-serve permanent classical postoperative prefrontal deficits.Patient 6 presented neuropsychological impairments in theexecutive and memory domains, which were fully com-patible with her anxiodepressive postoperative reactiveprofile (Cummings, 1985), and happened in the context ofa maintained general cognitive performance and improvedgeneral IQ. Patient 3 presented clear-cut neuropsychologi-cal improvements in a large number of domains includingprefrontal and perceptual functions. The neuropsychologi-cal sparing quality of CLT has been documented in a largegroup of patients suffering from other TCDs (in prepara-tion). A future systematic study will address this issue con-cerning the coupling of CLT and AMP lesions. However,the observed patient histories already dispel the possibilityof adverse postoperative prefrontal abulic manifestationsor personality changes, and neither patients nor familiescomplained about a personality reduction or alteration.
4.3. Thalamocortical slow burn
Evidence of progressive cortical (Corvit et al., 2001) andthalamic (Shenton et al., 2001) atrophy has been documentedin patients suffering from neuropsychiatric disorders. Thisphenomenon leads to a thalamocortical self-destruction. Onelikely mechanism for such morbidity is a persistent increaseof calcium entry into the thalamic cells generating LTSbursts, which may cause long-term deleterious effects, e.g.via calcium-triggered apoptosis. Furthermore, the continu-ous high frequency cortical activation due to the edge effectprovides a framework for the development of excitotoxic-ity of cortical cells. Under these conditions, the system mayfall into a self-reduction mode, a sort of “slow burn” withloss of neuronal substrate. This process however serves toreinforce the TCD, as the level of thalamocortical and corti-cothalamic activation decreases and exposes thalamic cellsto more disfacilitation and, consequently, to more LTS burstgeneration and more low frequency production. If this isconfirmed, the surgical treatment of a TCD would not onlyprovide symptom relief and disease control but additionallyacquire a protective role.
4.4. The cognitive factor
By cognitive we mean conceptual, emotional, mnesticand attentional functions, which are supported by the acti-vation of the widespread paralimbic (or mesocortical) andassociation networks (Mesulam, 1985), located in dorsolat-eral and medial prefrontal, orbitofrontal, cingulate, posteriorparietal, insular and medial temporal areas. Accumulat-ing evidence from EEG and MEG studies underscores thefact that conceptual and mnestic (Klimesch, 1999; Prichepand John, 1992; Sasaki et al., 1994; von Stein and Sarnthein,2000) as well as emotional (Machleidt et al., 1989)

112 D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113
activation in humans increases low frequency theta activity.A low frequency increase may thus arise either on the basisof a disease-related, or endogenous abnormal input to thethalamus (due to a micro- or macroscopic brain anomaly), orvia a “top–down” mechanism, driven by mental activity andgenerating low frequencies on a reactive basis. This findingprovides a substratum for (1) the appearance of reactivephenomena in the postoperative period, (2) the genesis ofchronic reactive psychiatric disorders, with at their source along term unsolved mental conflict, and (3) the grouping ofmany if not all neuropsychiatric disorders into a dynamicrealm of thalamocortical dysfunction. Indeed, whether theirtriggering mechanism is endogenous or reactive, they maybe regarded as mirroring an uninterrupted continuum of un-controllable and thus disturbing low frequency distortionsof the cognitive network. In this sense, the loss of con-trol which may occur in any healthy human brain duringstrong stimulus-bound transitory emotional reactions maybe viewed as a short-lived and in this sense not unhealthy(although sometimes quite undesirable!) TCD phenomenon.
Our clinical observations show that surgery can providemarked reduction or even suppression of the disease-relatedTCD, but does however not address the cognitive reactivemanifestations of the patient to her/his new postoperative sit-uation. Fear, expectations, despair and frustration may evenincrease for a time following surgery, representing a pow-erful cognitive source for increased low frequency activitynecessitating intensive psychotherapeutic support. Our ex-perience has however shown that this situation provides anew chance to approach and solve long standing resistantemotional conflicts by psychotherapy.
Such postoperative reactive manifestations are repre-sented by anxious or anxiodepressive states, or are alsocharacterized by non-acceptance/frustration postures pos-sibly leading to depression or by lack of adaptation to thenew situation. Distinctive characteristics indicating a reac-tive basis to these observations are: (1) symptomatologynot present before surgery, in relation to the new postop-erative situation (e.g. Patient 9), (2) large variations acrosstime and according to situations (e.g. Patients 4, 6, 7), (3)difficulties to describe the symptoms (e.g. Patient 6), and(4) symptoms fitting well with the personal internal andsituational profile (e.g. Patients 1, 2, 3, 4, 6, 7).
Psychotic and affective (bipolar and major depressive)disorders described are viewed here as having an endoge-nous origin and are well controlled by the CLT/AMP. OCDand ICD manifestations receded also postoperatively, but theissue of the endogenous or reactive origin of these diseaseentities remains as yet unresolved. As for the postoperativeanxiodepressive and frustration-related manifestations, thequestion may be raised as to their origin and their resistanceto surgery, in view of the fact that on the other side anxiousand depressive symptoms may respond to surgery. Onepossibility is that these manifestations may be responsiveto surgery in the measure in which they are endogenous.Another way of viewing this is that, while all anxiodepres-
sive and frustration-related disorders are of reactive origin,some of them may be self-entertained, thus presenting theobserved resistance to surgery. Along this line, postopera-tive anxiety reactions may be initially strong, but amenableto external and internal relieving factors and thus subsiderelatively quickly and easily (Patients 1, 2). To the con-trary, frustration/anger and conceptual rigidity do not causedirect suffering, and frustration is even self-entertained.Non-acceptance of a given situation recedes only whenthe person has decided that it should indeed recede. Thismental profile may thus represent a stronger challenge forthe relevant network and correlate with more difficult andprotracted postoperative evolutions (Patients 3, 4, 6, 7).
5. Conclusion
Clearly, more clinical experience must be amassed to de-fine in details the possibilities of this surgical approach indisabling neuropsychiatric disorders. We feel however thatthe evidence for a benign and efficient surgical interventionagainst the neuropsychiatric TCD syndrome is already com-pelling. The potential appearance of strong postoperative re-active manifestations requires the close association betweensurgery and psychotherapy, the latter providing support forthe integration of the new situation as well as the resolutionof old unresolved issues.
Acknowledgements
This work was supported by the University of Zürich,the University Hospital of Zürich, the Swiss National Sci-ence Foundation (Grants 31-36330.92, 31-47238.96 and31-54179.98), the NIH/NINDS 1 F31 NS42973-01, theCharles A. Dana Foundation and the NYU Medical CenterGeneral Clinical Research Center (NYU GCRC NIH NCRRM01RR00096). We thank V. Streit for histological work, C.Lebzelter for psychotherapeutic support to the patients, J.Dodd for instrumentation and V. Bügler for secretarial help.
References
Ballantine, H.T., Levy, B.S., Dagi, T.F., Giriunas, I.B., 1977. Cingulotomyfor psychiatric illness: report of 13 years’ experience. In: Sweet, W.H.,Obrador, S., Martin-Rodriguez, J.G. (Eds.), Neurosurgical Treatmentin Psychiatry, Pain and Epilepsy. University Park Press, Baltimore, pp.333–353.
Bingley, T., Leksell, L., Meyerson, B.A., Rylander, G., 1973. Stereotacticanterior capsulotomy in anxiety and obsessive-compulsive states.In: Laitinen, L.V., Livingston, K.E. (Eds.), Surgical Approaches inPsychiatry. Medical and Technical Publishing, Lancaster, pp. 159–164.
Bogerts, B., 1984. Neuropathology of schizophrenias. Fortschr. Neurol.Psychiatr. 52, 428–437.
Buchsbaum, M.S., Nenadic, I., Hazlett, E.A., Spiegel-Cohen, J.,Fleischman, M.B., Akhavan, A., et al., 2002. Differential metabolicrates in prefrontal and temporal Brodmann areas in schizophrenia andschizotypal personality disorder. Schizophrenia Res. 54, 141–150.
D. Jeanmonod et al. / Thalamus & Related Systems 2 (2003) 103–113 113
Corvit, A., Wolf, O.T., de Leone, M.J., Patalinjug, M., Kandil, E., Caraos,C., et al., 2001. Volumetric analysis of the prefrontal regions: findingsin aging and schizophrenia. Psychiatr. Res. 107, 61–73.
Cummings, J.L., 1985. Clinical Neuropsychiatry. Grune and Stratton, NewYork.
Dale, A.M., Fischl, B., Sereno, M.I., 1999. Cortical surface-based analysisI: segmentation and surface reconstruction. NeuroImage 9, 179–194.
Freeman, W., 1948. Transorbital leucotomy. Lancet 2, 371–373.Hazlett, E.A., Buchsbaum, M.S., Byne, W., Wie, T.C., Spiegel-Cohen, J.,
Geneve, C., et al., 1999. Three-dimensional analysis with MRI and PETof the size, shape, and function of the thalamus in the schizophreniaspectrum. Am. J. Psychiatr. 156, 1190–1199.
Heath, R.G., 1954. Studies in Schizophrenia. Harvard University Press,Cambridge.
Hécaen, H., Talairach, T., David, M., Dell, M.B., 1949. Coagulationslimitées du thalamus dans les algies du syndrome thalamique. Rev.Neurol. 81, 917–931.
Jeanmonod, D., Magnin, M., Morel, A., 1996. Low-threshold calciumspike bursts in the human thalamus: common physiopathology forsensory, motor and limbic positive symptoms. Brain 119, 363–375.
Jeanmonod, D., Magnin, M., Morel, A., Siegemund, M., Cancro, R., Lanz,M., et al., 2001. Thalamocortical dysrhythmia II. Clinical and surgicalaspects. Thalamus 1, 245–254.
Kandel, E.R., 2000. Disorders of thought and volition: schizophrenia. In:Kandel, E.R., Schwartz, J.H., Jessel, T.M. (Eds.), Principles of NeuralScience, fourth ed. McGraw-Hill, New York, pp. 1188–1208.
Klimesch, W., 1999. EEG alpha and theta oscillations reflect cognitiveand memory performance: a review and analysis. Brain Res. Rev. 29,169–195.
Knight, G., 1973. Further observations from am experience of 660 casesof stereotactic tractotomy. Postgrad. Med. J. 49, 845–854.
Llinas, R., Jahnsen, H., 1982. Electrophysiology of mammalian thalamicneurons in vitro. Nature 297, 406–408.
Llinas, R., Ribary, U., Contreras, D., Pedroarena, C., 1998. The neuronalbasis for consciousness. Philos. Trans. R. Soc. Lond. B Biol. 353,1841–1849.
Llinas, R., Ribary, U., Jeanmonod, D., Kronberg, E., Mitra, P.P., 1999.Thalamocortical dysrhythmia: a neurological and neuropsychiatricsyndrome characterized by magneto-encephalography. Proc. Natl.Acad. Sci. U.S.A. 96, 15222–15227.
Llinas, R., Ribary, U., Jeanmonod, D., Cancro, R., Kronberg, E.,Schulman, J., et al., 2001. Thalamocortical dysrhythmia I. Functionaland imaging aspects. Thalamus 1, 237–244.
Llinas, R., Leznik, E., Urbano, F., 2002. Temporal binding via corticalcoincidence detection of specific and non-specific thalamocorticalinputs: a voltage dependent dye imaging study in mouse brain slices.Proc. Natl. Acad. Sci. U.S.A. 99, 449–452.
Machleidt, W., Gutjahr, L., Mügge, A., 1989. Grundgefühle: Phänomeno-logie, Psychodynamik, EEG-Spektralanalytik. Springer-Verlag, Berlin.
Mazziotta, J.C., Toga, A.W., Evans, A.C., Fox, P., Lancaster, J., 1995.A probabilistic atlas of the human brain: theory and rationale for itsdevelopment. NeuroImage 2, 89–101.
Mesulam, M.M., 1985. Principles of Behavioral Neurology. FA DavisCompany, Philadelphia.
Moniz, E., 1936. Les premières tentatives opératoires dans le traitementde certaines psychoses. Encéphale 31, 1–29.
Morel, A., Magnin, M., Jeanmonod, D., 1997. Multiarchitectonic andstereotactic atlas of the human thalamus. J. Comp. Neurol. 387, 588–630.
Morel, A., Loup, F., Magnin, M., Jeanmonod, D., 2002. Neurochemicalorganization of the human basal ganglia: anatomofunctional territoriesdefined by the distributions of calcium-binding proteins and SMI-32.J. Comp. Neurol. 443, 86–103.
Morison, R., Dempsey, E., 1942. A study of thalamocortical relations.Am. J. Physiol 135, 281–292.
Niedermeyer, E., 1999. The normal EEG of the waking adult. In:Niedermeyer, E., Lopes Da Silva, F. (Eds.), Electroencephalography.Basic Principles, Clinical Applications and Related Fields, fourth ed.Williams & Wilkins, Baltimore, pp. 149–173.
Pascual-Marqui, R.D., Lehmann, D., Koenig, T., Kochi, K., Merlo,M.C.G., Hell, D., et al., 1999. Low resolution brain electromagnetictomography (LORETA) functional imaging in acute, neuroleptic-naive,first-episode, productive schizophrenia. Psychiat. Res. Neuroimag. Sect.90, 169–179.
Prichep, L.S., John, E.R., 1992. QEEG profiles of psychiatric disorders.Brain Topogr. 4, 249–257.
Ramirez, R., Horenstein, C., Kronberg, E., Ribary, U., Llinas, R., 2001.Anatomically constrained iterative algorithm for MEG-based mappingof electrical activity in the time and frequency domains. NeuroImage13 (Suppl.), 227.
Ribary, U., Jeanmonod, D., Kronberg, E., Schulman, J., Sauve, K.,Ramirez, R., et al., 2000. Thalamo-cortical spatio-temporal dynamicsand its alterations in human brain pathology. NeuroImage 11,168.
Sasaki, K., Tsujimoto, T., Nambu, A., Matsuzaki, R., Kyuhou, S., 1994.Dynamic activities of the frontal association cortex in calculating andthinking. Neurosci. Res. 19, 229–233.
Schulman, J., Horenstein, C., Ribary, U., Kronberg, E., Cancro, R.,Jeanmonod, D., et al., 2001. Thalamocortical dysrhythmia in depressionand obsessive-compulsive disorder. NeuroImage 13, 1004.
Shenton, M.E., Dickey, C.C., Frumin, M., McCarley, R.W., 2001. Areview of MRI findings in schizophrenia. Schizophrenia Res. 49, 1–52.
Spiegel, E.A., Wycis, H.T., 1950. Thalamic recordings in man withspecial reference to seizure discharges. Electroencephalogr. Clin.Neurophysiol. 2, 23–27.
Spiegel, E.A., Wycis, H.T., 1952/1962. Stereoencephalotomy, parts I/II.Grune and Stratton, New York.
Sponheim, S.R., Clementz, B.A., Iacono, W.G., Beiser, M., 2000. Clinicaland biological concomitants of resting state EEG power abnormalitiesin schizophrenia. Biol. Psychiatr. 48, 1088–1097.
von Stein, A., Sarnthein, J., 2000. Different frequencies for different scalesof cortical integration: from local gamma to long range alpha/thetasynchronization. Int. J. Psychophysiol. 38, 301–313.
Related Documents











