Acta neurol. belg., 20 02 , 102, 21-29 Abstract Tropical Spastic Paraparesis / HTLV-I Associated Myelopathy (TSP/HAM) is clinically characterized by chronic insidious spastic paraparesis associated with variable sensory impairment and sphincter symptoms. Neuropatholo gical studies of this condition are based on a few autopsied cases, and on experimental animal mod- els. Howev er , divergen t aspects exist be tween human and experimental animal neuropathology of TSP/HAM, namely, the site of lesions in the s pinal cor d, the in volve- ment of peripheral ner ves and r oots, the nature of histo- logical abnormalit ies, and the cellular reac tions. Moreove r , unanswere d questions as to the prefer ential site of sp inal affection, the tempora l inflammatory pic- tur e, the selec tive dama ge of the corticos pinal trac t, the sparing of lower motor neur ons, the inconsistent af fec- tion of sensory tr acts, and the invo lvement of the brain, ar e outlin ed. A long-t erm, chr onolog ica l, cor related clinical and neuropathological study in HAM experi- mental animals is suggested. Key words : TSP/H AM ; human mye lop ath y ; e xpe ri- mental anima l ; neuropatho logy ; HTL V -I/II. Introduction Tropical Spastic Paraparesis (TSP) is a myelopa- thy described in several countries of tropical and temperate regions, that was originally denominated tropical spastic paraplegia by Mani et al. (1969) in India ( Spilla ne, 1973) . In these pre vious studies, this condition was eti- ologically undefined and of unknown origin, although some considered that different causes such as mal nut riti on, toxins, syp hil is a nd y aws might be implicated. From 1985 on, an association of TSP with the retrovirus HTLV-I was found first- ly by Gessain et al. (1985) and Osame et al. (1986) in around half of their cases, and afterwards by se v- eral other investigato rs (Zanino vic’, 1999). Osame et al. (1986) denominated it as HTLV-I associated myelopathy (HAM). Later on, TSP ass ociated with HTLV-I and HAM was considered to be the same entity (Román & Osame, 1988). The incubation period from HTLV-I infection to clinical manifestation ranges from months to decades and the major modes of transmission includ e blood t ransf usion , parent eral dr ugs, sexu al contact and breast feeding (Edlich et al., 20 00). In the endemic area, besides HTL V-I seroposi- tive TSP patients , seronegativ e TSP cases hav e also been described (De Castro-Costa et al., 1994, 2001 ; León et al., 1997) . They are clin ically simi- lar since they present insidious and progressive paraparesis with sphincter and sensory impairment in some of the cases. Most of them are partially incapa citate d, requi ring some suppo rt for walking such as crutches and other people. A slight trend to more incapacitating states seems occur in the seropositive patients (De Castro-Costa, 1996a). Demographically , the HTL V -I seropositive TSP cases are mainly women, while there is a slight pre- dominance of men in the seronegative ones. Both have a mean age of around 40-45 years. Racially, they are distributed in the C aucasoid, Negroid and Mongoloid populations (De Castro-Costa et al., 1995a ; De Castr o-Costa, 1996a ). Clinically, TSP/H AM is c harac terize d by an insidious (rarely acute) onset of motor dysfunction, which leads to progressive gait disturbance associ- ated with variable sphincter and sensory impair- ment. The patients present symmetrical or asym- metrical spastic paraparesis with hyperreflexia, clonus and Babinski signs in the lower limbs as well as hyperreflexia and Hoffmann signs in the upper limbs. Paresis of the upper limbs is uncom- mon and rare. The TSP/HAM patients become rel- atively stable a few years after onset and most of them die of concurrent interrelated diseases. The laboratorial diagnosis of TSP/HAM in- cludes the presence of anti-HTLV-I/II antibodies (EIA) in serum and CSF and the presence of genomic protein s (GD21 and rgp 46-I, p19 and/o r p24) shown by confirmatory tests such as Western blot and Inno-Lia. Molecular tests such as poly- merase chain reaction (PCR) and real time PCR, may define this infective condition by amplifying Neuropathology of Human and Experimental TSP/HAM : a critical review Carlos Maurício DE CASTRO COSTA 1 , René DOM 2 , Herwig C ARTON 3 , T erezinha DE JESUS TEIXEIRA SANTOS 1 and Maria José ANDRADA-SERPA 4 1 Department of P hysiology and Pharmacology , Federal University of Ceará, Fortaleza-CE, Brazil ; 2 Department of Neurop athology , Katholieke Uni versiteit Leuv en, Leuv en, Belg ium ; 3 Depar tmen t of Neurolog y , Katho lieke Universite it Leuven, Leuven, Belgi um ; 4 Evandro Chagas Hospital Resea rch Center , Oswa ldo Cruz Found ation , Rio de Janeiro- RJ, Brazil ————

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 1/9
Acta neurol. belg., 2002, 102, 21-29
Abstract
Tropical Spastic Paraparesis / HTLV-I Associated Myelopathy (TSP/HAM) is clinically characterized bychronic insidious spastic paraparesis associated withvariable sensory impairment and sphincter symptoms. Neuropathological studies of this condition are based ona few autopsied cases, and on experimental animal mod-els. However, divergent aspects exist between humanand experimental animal neuropathology of TSP/HAM,namely, the site of lesions in the spinal cord, the involve-ment of peripheral nerves and roots, the nature of histo-logical abnormalities, and the cellular reactions. Moreover, unanswered questions as to the preferentialsite of spinal affection, the temporal inflammatory pic-
ture, the selective damage of the corticospinal tract, thesparing of lower motor neurons, the inconsistent affec-tion of sensory tracts, and the involvement of the brain,are outlined. A long-term, chronological, correlated clinical and neuropathological study in HAM experi-mental animals is suggested.
Key words : TSP/HAM ; human myelopathy ; experi-mental animal ; neuropathology ; HTLV-I/II.
Introduction
Tropical Spastic Paraparesis (TSP) is a myelopa-thy described in several countries of tropical andtemperate regions, that was originally denominatedtropical spastic paraplegia by Mani et al. (1969) inIndia (Spillane, 1973).
In these previous studies, this condition was eti-ologically undefined and of unknown origin,although some considered that different causessuch as malnutrition, toxins, syphilis and yawsmight be implicated. From 1985 on, an associationof TSP with the retrovirus HTLV-I was found first-ly by Gessain et al. (1985) and Osame et al. (1986)in around half of their cases, and afterwards by sev-
eral other investigators (Zaninovic’, 1999). Osameet al. (1986) denominated it as HTLV-I associatedmyelopathy (HAM). Later on, TSP associated withHTLV-I and HAM was considered to be the sameentity (Román & Osame, 1988).
The incubation period from HTLV-I infection to
clinical manifestation ranges from months todecades and the major modes of transmissioninclude blood transfusion, parenteral drugs, sexualcontact and breast feeding (Edlich et al., 2000).
In the endemic area, besides HTLV-I seroposi-tive TSP patients, seronegative TSP cases have alsobeen described (De Castro-Costa et al., 1994,2001 ; León et al., 1997). They are clinically simi-lar since they present insidious and progressiveparaparesis with sphincter and sensory impairmentin some of the cases. Most of them are partiallyincapacitated, requiring some support for walkingsuch as crutches and other people. A slight trend tomore incapacitating states seems occur in theseropositive patients (De Castro-Costa, 1996a).
Demographically, the HTLV-I seropositive TSPcases are mainly women, while there is a slight pre-dominance of men in the seronegative ones. Bothhave a mean age of around 40-45 years. Racially,they are distributed in the Caucasoid, Negroid andMongoloid populations (De Castro-Costa et al.,1995a ; De Castro-Costa, 1996a).
Clinically, TSP/HAM is characterized by aninsidious (rarely acute) onset of motor dysfunction,which leads to progressive gait disturbance associ-
ated with variable sphincter and sensory impair-ment. The patients present symmetrical or asym-metrical spastic paraparesis with hyperreflexia,clonus and Babinski signs in the lower limbs aswell as hyperreflexia and Hoffmann signs in theupper limbs. Paresis of the upper limbs is uncom-mon and rare. The TSP/HAM patients become rel-atively stable a few years after onset and most of them die of concurrent interrelated diseases.
The laboratorial diagnosis of TSP/HAM in-cludes the presence of anti-HTLV-I/II antibodies(EIA) in serum and CSF and the presence of
genomic proteins (GD21 and rgp46-I, p19 and/or p24) shown by confirmatory tests such as Westernblot and Inno-Lia. Molecular tests such as poly-merase chain reaction (PCR) and real time PCR,may define this infective condition by amplifying
Neuropathology of Human and Experimental TSP/HAM : a critical review
Carlos Maurício DE CASTRO COSTA1, René DOM2, Herwig CARTON3, Terezinha DE JESUS TEIXEIRA SANTOS1 andMaria José ANDRADA-SERPA4
1Department of Physiology and Pharmacology, Federal University of Ceará, Fortaleza-CE, Brazil ; 2Department of Neuropathology, KatholiekeUniversiteit Leuven, Leuven, Belgium ; 3Department of Neurology, Katholieke Universiteit Leuven, Leuven, Belgium ; 4Evandro Chagas Hospital
Research Center, Oswaldo Cruz Foundation, Rio de Janeiro-RJ, Brazil
————

8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 2/9
22 C. M. DE CASTRO COSTA ET AL.
the viral nucleic acids (Compton, 1991 ; Wolcott,1992). Besides this specific viral-related diagnosis,CSF studies also show mild lymphocytic pleocyto-sis and milder elevation of proteins. Immunologicalstudies of CSF reveal an inflammatory reactionwith oligoclonal bands, indicative of intrathecal
synthesis of IgG (Puccioni-Sohler et al., 1995).Spinal cord MRI may indicate atrophy of the lower thoracic region and nonspecific changes in thewhite matter, suggestive of possible cerebraldemyelination. Electrophysiological studies mayshow impairment of peripheral nerves and sensoryascending tracts (Moritoyo et al., 1996). Moreover,the impairment of corticospinal tracts in TSP/HAMis shown by studies of motor evoked potentials(Foster et al., 1993).
At present there is no definite treatment for TSP/HAM, although oral prednisone, i.v. methyl-
prednisolone, plasmapheresis, interferon, oral aza-thiaprine and vitamin C have been tried and haveshown transient effects (Edlich et al., 2000).
Experimentally, animal models have been devel-oped to study clinical and histopathological expres-sion of TSP/HAM, with the aim of understandingunderlying pathogenetic mechanisms.
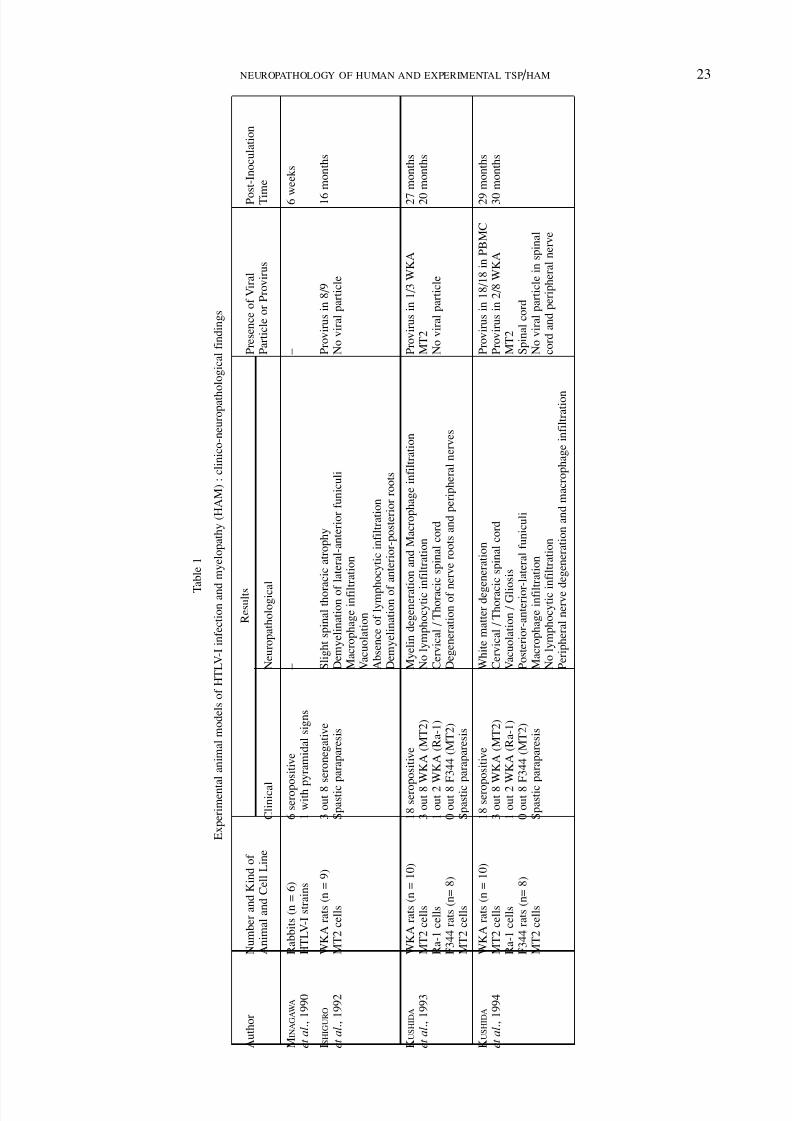
These experimental studies have shown clinical-ly the presence of pyramidal signs in 1 out of 6 rab-bits after six weeks of HTLV-I inoculation(Minagawa et al., 1991), and spastic paraparesis in3 out of 16 seronegative Wistar-King-Aptekman(WKA) rats 16 months after MT2 cell inoculation(Ishiguro et al., 1992), in 1 out of 2 seropositiveWKA rats 27 months after Ra-1 cell inoculationand 1 out of 8 seropositive WKA rats 20 monthsafter MT2 cell inoculation (Kushida et al., 1993),and in 6 out of 8 seropositive WKA rats 29 monthsafter MT2 cell inoculation and 1 out of 2 seroposi-tive WKA rats 30 months after Ra-1 cell inocula-tion (Kushida et al., 1994). No F344 rats showedneurological changes in these studies (Table 1).Beside these results, minor (reduced motor capaci-ty and behavior) and major (paralysis) changeshave been shown in parents and sibling rats inocu-
lated with the whole blood of TSP/HAM patients(De Castro-Costa, 1996b ; De Castro-Costa, 1998 ;De Castro-Costa et al., 1998). Correia et al. (2001)established an experimental model of HTLV-Iinfection in rats (F344) and mice (C3H/Hej andBALB/c), in which they observed that none of theinoculated mice exhibited antibodies whereas91.6% presented provirus in at least one of the ana-lyzed tissues. Eighty percent of the inoculated adultrats exhibited a persistent antibody immuneresponse whereas provirus was found in only 5 outof 15 (33%) rats. The histopathological analysis
showed only minor findings in liver and muscles,whereas the spinal cord and brain were normal. Noanimal, however, showed any motor disability.
Experimental studies with transgenic rats havealso been carried out. However, none of these rats
showed neurological symptoms or lesions, exclud-ing their consideration as HAM models. Never-theless, they are very suited as models for HTLV-Iassociated arthropathy (Grossman & Ratner, 1996).
In brief, most of the animals inoculated withHTLV-I exhibited tardive major neurological signs
(15 to 30 months after inoculation) in seropositiveand seronegative WKA rats. These are in fact oldanimals since rats have an average life span of 24 months (Adams et al., 1997), and this obvious-ly differs from human clinical findings.
This work reviews critically the different neu-ropathological aspects shown in the studies of human and experimental animal TSP/HAM.
Human and Animal Neuropathology of TSP/HAM
HUMAN NEUROPATHOLOGY
To-date there have been around 25 autopsiedcases of TSP/HAM (Akizuki et al., 1987, 1989 ;Furuzono et al., 1989 ; Izumo et al., 1989 ;Kobayashi et al., 1989 ; Picardo et al., 1988 ;Iwasaki, 1990 ; Bhigjee et al., 1991 ; Ogata et al.,1993 ; Wu et al., 1993 ; Yoshioka et al., 1993 ; DeCastro-Costa et al., 1995b ; Cartier et al., 1997 ;Leite et al., 1997).
All cases presented thoracic spinal cord atrophy(Fig. 1) with less prominent cervical or lumbar atrophy. Demyelination of the corticospinal tractswas predominant in all cases, in addition to impair-ment of the posterior and, less frequently, anterior funiculi as shown in one of our cases (De Castro-Costa et al., 1995b) (Fig. 2). Lower motor neuronswere spared and perivascular and parenchymalinflammatory infiltration with lymphocytes andmacrophages was mostly present in the short evo-lutive cases (Yoshioka et al., 1993) and absent(Iwasaki, 1990), or slight, in the long evolutiveones (Figs. 3 and 4) (De Castro-Costa et al.,1995b ; Cartier et al., 1997 ; Wu et al., 1993).Hyaline degeneration of the vessel walls (adventi-
tia and media) (Fig. 4) and astrocytic proliferationwere found in all cases in different stages of thecondition. However, viral particles or viral antigenswere not found in these studies. Moreover, vacuo-lation was not described in most of the cases,except for that of Yoshioka et al. (1993) (Table 2).Brain involvement in TSP/HAM has also been sug-gested (Cartier et al., 1997 ; Aye et al., 2000).However, this inflammatory involvement occursmainly in cases where there is active chronic-inflammation (i.e., with marked perivascular inflammatory infiltration) and in none where there
is inactive-chronic inflammation (i.e., withoutinflammatory change, but with marked fibroticchange of blood vessels), thus suggesting anencephalo-myelitic process in the early stage of this condition.
8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 3/9
NEUROPATHOLOGY OF HUMAN AND EXPERIMENTAL TSP / HAM 23
T a b l e 1
E x p e r i m e n t a l a n i m a l m o d e l s o f H T L V - I i n f e c t i o n a n d m y e l o p a t h y ( H A M ) : c l i n i c o - n e u r o p a t h o l o g i c a l f i n d i n g s
A u t h o r
N u m b e r a n d K i n d o f
R e s u l t s
P r e s e n c e o f V i r a l
P o
s t - I n o c u l a t i o n
A n i m a l a n d C e l l L i n e
C l i n i c a l
N e u r o p a t h o l o g i c a
l
P a r t i c l e o r P r o v i r u s
T i m e
M I N A G A W A
R a b b i t s ( n = 6 )
6 s e r o p o s i t i v e
–
–
6 w e e k s
e t a l . ,
1 9 9 0
H T L V - I s t r a i n s
1 w i t h p
y r a m i d a l s i g n s
I S H I G U R O
W K A r a t s ( n = 9 )
3 o u t 8
s e r o n e g a t i v e
S l i g h t s p i n a l t h o r a c i c a t r o p h y
P r o v i r u s i n 8 / 9
1 6
m o n t h s
e t a l . ,
1 9 9 2
M T 2 c e l l s
S p a s t i c
p a r a p a r e s i s
D e m y e l i n a t i o n o f
l a t e r a l - a n t e r i o r f u n i c u l i
N o v i r a l p a r t i c l e
M a c r o p h a g e i n f i l t r a t i o n
V a c u o l a t i o n
A b s e n c e o f l y m p h o c y t i c i n f i l t r a t i o n
D e m y e l i n a t i o n o f
a n t e r i o r - p o s t e r i o r r o o t s
K U S H I D A
W K A r a t s ( n = 1 0 )
1 8 s e r o p o s i t i v e
M y e l i n d e g e n e r a t i o n a n d M a c r o p h a g e i n f i l t r a t i o n
P r o v i r u s i n 1 / 3 W K A
2 7
m o n t h s
e t a l . ,
1 9 9 3
M T 2 c e l l s
3 o u t 8 W K A ( M T 2 )
N o l y m p h o c y t i c i n f i l t r a t i o n
M T 2
2 0
m o n t h s
R a - 1 c e l l s
1 o u t 2 W K A ( R a - 1 )
C e r v i c a l / T h o r a c
i c s p i n a l c o r d
N o v i r a l p a r t i c l e
F 3 4 4 r a t s ( n = 8 )
0 o u t 8
F 3 4 4 ( M T 2 )
D e g e n e r a t i o n o f n e r v e r o o t s a n d p e r i p h e r a l n e r v e s
M T 2 c e l l s
S p a s t i c
p a r a p a r e s i s
K U S H I D A
W K A r a t s ( n = 1 0 )
1 8 s e r o p o s i t i v e
W h i t e m a t t e r d e g e n e r a t i o n
P r o v i r u s i n 1 8 / 1 8 i n P B M C
2 9
m o n t h s
e t a l . ,
1 9 9 4
M T 2 c e l l s
3 o u t 8 W K A ( M T 2 )
C e r v i c a l / T h o r a c
i c s p i n a l c o r d
P r o v i r u s i n 2 / 8 W K A
3 0
m o n t h s
R a - 1 c e l l s
1 o u t 2 W K A ( R a - 1 )
V a c u o l a t i o n / G l i o s i s
M T 2
F 3 4 4 r a t s ( n = 8 )
0 o u t 8
F 3 4 4 ( M T 2 )
P o s t e r i o r - a n t e r i o r
- l a t e r a l f u n i c u l i
S p i n a l c o r d
M T 2 c e l l s
S p a s t i c
p a r a p a r e s i s
M a c r o p h a g e i n f i l t r a t i o n
N o v i r a l p a r t i c l e i n s p i n a l
N o l y m p h o c y t i c i n f i l t r a t i o n
c o r d a n d p e r i p h e r a l n e r v e
P e r i p h e r a l n e r v e d e g e n e r a t i o n a n d m a c r o p h a g e i n f i l t r a t i o n

8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 4/9
24 C. M. DE CASTRO COSTA ET AL.
ANIMAL NEUROPATHOLOGY
Neuropathological studies of the HAM modelhave been carried out by Ishiguro et al. (1992) andKushida et al. (1993, 1994). These studies havebeen reviewed by Iwasaki (1993), Mizusawa et al.(1994) and Yoshiki (1995).
The main findings included demyelination of thelateral and anterior funiculi of the cervical and tho-racic spinal cord, of the nerve roots and peripheralnerves, as well as vacuolation and gliosis of theposterior, anterior and lateral funiculi. In all ratsthere was macrophage infiltration and absence of lymphocytes. This macrophage infiltration wasalso present in peripheral nerves and roots.Mizusawa et al. (1994), however, pointed out sim-ilar but milder lesions in old control WKA normalrats. Despite detecting viral provirus in polymor-phic mononuclear blood cells, and occasionally in
the spinal cord, they did not detect any viral parti-cles in the spinal cord and peripheral nerves of theparetic rats (Yoshiki, 1995) (Table 1). Braininvolvement was only shown in a transgenic modelcarrying the LTR-env-pX gene of HTLV-I, where
infiltration of activated microglia/macrophagesintermingled with many apoptotic cells was evident(Yoshiki, 2001).
Discussion
The Montgomery et al. (1964) anatomopatho-
logical reports on the “Jamaican Neuropathy” (later defined as TSP) were similar to the presentlydescribed cases. However, at that time, an etiologyof these cases had not yet been defined.
The neuropathological lesions described in theTSP/HAM autopsied cases still have many unan-swered questions such as : the preferential affectionof the lower thoracic spinal cord ; the lack of tem-poral correlation of clinical and histopathological(inflammatory) expression ; the sparing of thelower motor neurons ; the inconsistent affection of sensory tracts ; the main and selective damage of
corticospinal tracts and partially of the posterior funiculi (De Castro-Costa et al., 1999). Thedemyelination of the pyramidal tract is predomi-nant, and this is corroborated by electrophysiologi-cal studies with evoked motor potentials (Castillo
FIG. 1. — Spinal cord atrophy
FIG. 2. — Demyelination of the anterior corticospinal tract at
thoracic level (upper right). Normal anterior spinal artery(lower left) (Kluver-Barrera 200).

8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 5/9
NEUROPATHOLOGY OF HUMAN AND EXPERIMENTAL TSP / HAM 25
et al., 1996). However, a correlation between slightto absent cervical demyelination of corticospinaltracts (Iwasaki, 1990) and the presence of hyper-reflexia of the upper limbs with normal force inmost of the patients is still lacking.
When human and animal TSP/HAM cases areneuropathologically compared, striking differencesemerge (De Castro-Costa, 1998 ; De Castro-Costaet al., 1998). The main sites involved in the animals
are the cervico-thoracic-lumbar levels with clinicalexpression limited to the lower limbs. Demye-lination is shown in the lateral and anterior tracts aswell as in the peripheral nerves and roots in a mostexpressive manner. Comparatively, in the humanTSP/HAM cases, peripheral nerve impairment isless frequent. The presence of both lesions in ani-mals makes it difficult to accept the term “spastic”paraparesis since the peripheral impairment shouldlead to flaccid paralysis. Indeed, in addition to thisparalysis, atrophy of the lower limbs of these ani-mals has been described (Kushida et al., 1994).
Vacuolation is a characteristic lesion in AIDSmyelopathy, which does not exist in humanTSP/HAM. It is thus surprising to observe its pres-ence in HAM animals, and possibly this may be theexpression of an age-related phenomenon since
control old rats show similar, but milder, lesions(Mizusawa et al., 1994). The absence of lympho-cytes and presence of macrophage infiltration inanimal models is another of the divergent pointsfrom human TSP/HAM. Possibly different mecha-nisms are involved in these phenomena, and themacrophage infiltration may be correlated with theseverity of myelin loss and vacuolation (Yoshiki,1995) ; it may also represent a scavenger reaction
for myelin debris, and so does not mean an activeimmune process as seen with lymphocytic prolife-ration. Moreover, vacuolation is a non-specificresponse to a variety of stimuli such as nutritionaldeficiencies, cytokine-mediated injuries, metabolicand neurotoxic disorders (Jacobs et al., 1979 ;Lampert et al., 1973 ; Louis et al., 1993). On theother hand, it is remarkable that spinal cord lesionsin seropositive HAM rats were the same as in theseronegative rats, as shown in Table 1 (Yoshiki,1995), and this finding may foretell possiblelesions to be found in human seronegative TSP.
Evidence of apoptosis of myelin-producing cells,oligodendrocytes and Schwann cells, and the par-ticipation of TNF-a (and other cytokines) in theseropositive animals, may represent an importantfinding to clarify the pathogenesis of this HTLV-I
FIG. 3. — Small focus of inflammatory cells in the gray mat-
ter at thoracic level (HE 200).
FIG. 4. — Preservation of some anterior horn cells (*), thick-
ening of vascular walls (↓) and slight lymphocytic perivascular infiltration (HE 200).

8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 6/9
26 C. M. DE CASTRO COSTA ET AL.
T a b l e 2
N e u r o p a t h o l o g i c a l f i n d i n g s i n h u m a n H A M / T S P
A u t h o r
S p i n a l C o r d
D e m y e l i n a t i o n
I n f l a m m a t o r y
V a s c u l a r
A s t r o c y t i c
V i r a l P
a r t i c l e
E v o l u t i o n
V a c u o l a t i o n
N u m b e r
A t r o p h y
I n f i l t r a t i o n
C h a n g e s
R e a c t i o n
o r P r o v i r u s
o f C a s e s
A K I Z U K I
L o w e r
L a t e r a l
L y m p h o c y t e s
P r o l i f e r a t i o n
Y e s
N o n e
2 y e a r s
–
1
e t a l . ,
1 9 8 8
T h o r a c i c
A n t e r i o r
P l a s m o c y t e s
C a p i l l a r y
P o s t e r i o r
M a c r o p h a g e s
H
y a l i n e
P e r i v a s c . / P a r e n c .
T h i c k n e s s
P I C A R D O
N o n e
L a t e r a l
–
C a p i l l a r y
Y e s
?
1 y e a r
N o
2
e t a l . ,
1 9 8 8
P o s t e r i o r
P r o l i f e r a t i o n
5 y e a r s
A n t e r i o r
N e r v e
R o o t
I W A S A K I
M i d d l e
L a t e r a l
L y m p h o c y t e s
H
y a l i n e
Y e s
–
0 - 3 y e a r s
N o
1 0
1 9 9 0
L o w e r
P o s t e r i o r
M o n o n u c l e a r
T h i c k n e s s
4 - 6 y e a r s
T h o r a c i c
N e r v e ( l e s s )
G r a y / W h i t e
9 - 2 8 y e a r s
P e r i v a s c u l a r
( 0 - 3 > 4 - 6 y e a r s )
B H I G J E E
T h o r a c i c
L a t e r a l
L y m p h o c y t e s
–
N R
N o
1 y e a r
N o
1
e t a l . ,
1 9 9 1
P o s t e r i o r
P a r e n c h y m a
P r o v i r a l D N A
P e r i v a s c u l a r
O G A T A
T h o r a c i c
L a t e r a l
N o n e
H
y a l i n e
Y e s
–
3 6 y e a r s
N o
1
e t a l . ,
1 9 9 3
P o s t e r i o r
T h i c k n e s s
A n t e r i o r
Y O S H I O K A
T h o r a c i c
L a t e r a l
L y m p h o c y t e s
–
N R
N o a n t i g e n
9 m o n t h s
Y e s
1
e t a l . ,
1 9 9 3
P o s t e r i o r
P e r i v a s c u l a r
W U
C e r v i c a l
L a t e r a l
L y m p h o c y t e s
A
d v e n t i t i a
Y e s
–
2 5 y e a r s
N o
1
e t a l . ,
1 9 9 3
T h o r a c i c
P o s t e r i o r
P a r e n c h y m a
G
l i o s i s
L u m b a r
P e r i v a s c u l a r
S a c r a l +
B r a i n s t e m
D E C A S T R O - C O
S T A
C e r v i c a l
–
M a c r o p h a g e s
H
y a l i n e
Y e s
–
1 3 - 4 0 y e a r s
–
2
e t a l . ,
1 9 9 5
T h o r a c i c
L y m p h o c y t e s ( T )
T h i c k n e s s
L u m b a r
P e r i v a s c . / M e n i n .
C A R T I E R
L u m b a r
L a t e r a l ( L / T )
L y m p h o c y t e s
H
y a l i n e
N R
–
3 - 1 7 y e a r s
–
6
e t a l . ,
1 9 9 7
T h o r a c i c
P o s t e r i o r ( C )
P e r i v a s c u l a r
T h i c k n e s s
S p i n o c e r e b e l l a r
P a r e n c h y m a
N R : n o t r e p o
r t e d
T o t a l : 2 5

8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 7/9
NEUROPATHOLOGY OF HUMAN AND EXPERIMENTAL TSP / HAM 27
associated condition (Yoshiki, 1995). Moreover,chronological examination showed that a highprovirus load and pX expression were evident justbefore the appearance of apoptosis. Additionally,marked suppression of bcl-2 was observed in theisolated oligodendrocytes in vitro. Both elements
may be related to the pathogenesis of HAM rat dis-ease (Yoshiki, 2001).
Only few papers describe long-term observa-tions of human, clinical and neuropathological evo-lution of TSP/HAM (De Castro-Costa, 1996a ;Araújo et al., 1995). However, there is now anincreased interest in detecting minimal neurologi-cal signs in asymptomatic HTLV-I positive blooddonors, and this will allow an accurate follow-up of them, which may be representative of a contribu-tion to pathogenetic and therapeutic purposes(Leite et al., 2001). In this context, it is our inten-
tion to carry out further long-term neuropathologi-cal studies in inoculated rats in order to detect, byhistopathological and molecular methods, the evo-lutive characteristics of the lesions, correlatingeach phase with clinical expression. Moreover, theseronegative TSP patients have not yet been studiedneuropathologically and comparative analysis of both seronegative TSP and TSP/HAM will be of interest and importance for understanding of thepathogenesis of both conditions.
Acknowledgements
We thank Dr. David Neil Criddle for the review of theEnglish style and Sílvio A. Costa for the accurate elec-tronic typewriting of this manuscript.
REFERENCES
ADAMS R. D., VICTOR M., ROPPER A. H. The neurology of aging. In : Principles of Neurology. New York,McGraw-Hill, 1997, 608-620.
AKIZUKI S., NAKAZATO O., HIGUCHI K., TANABE K.,SETOGUCHI M. et al. Necropsy findings in HTLV-Iassociated myelopathy. Lancet , 1987, 1 : 156-157.
AKIZUKI S., YOSHIDA S., SETOGUCHI M., HIGUCHI S.,YAMAMOTO S. et al. The neuropathology of humanT-lymphotropic virus type I associated myelopa-thy. In : HTLV-I and the Nervous System. ROMÁN
G. C., VERNANT J. C., OSAME M. (eds.). New York,Alan R. Liss Inc., 1989, 253-260.
ARAÚJO A. Q. C., LEITE A. C. C. B., DULTRA S. V.,ANDRADA-SERPA M. J. Progression of neurologicaldisability in HTLV-I associated myelopathy / trop-ical spastic paraparesis (HAM/TSP). J . Neurol.Sci., 1995, 129 : 147-151.
AYE M. M., MATSUOKA E., MORITOYO T., UMEHARA F.,SUEHARA M. et al. Histopathological analysis of
four autopsy cases of HTLV-I-associated myelopa-thy / tropical spastic paraparesis : inflammatorychanges occur simultaneously in the entire centralnervous system. Acta Neuropathol., 2000, 100 :245-252.
BHIGJEE A. I., WILEY C. A., WACHMAN W., AMENONIORI T.,PIRIE D. et al. HTLV-I associated myelopathy :clinicopathologic correlation with localization of provirus to spinal cord. Neurology, 1991, 41 :1990-1992.
CARTIER L. M., CEA G., VERGARA C., ARAYA F., BORN P.
Clinical and neuropathological study of sixpatients with spastic paraparesis associated withHTLV-I : an axomyelinic degeneration of the cen-tral nervous system. J . Neuropathol. Exp. Neurol.,1997, 56 (4) : 403-413.
CASTILLO J. L., VERDUGO R. J., CEA J. G. Clinical neuro-physiology of HAM/TSP. In : HTLV – Truths and Questions. ZANINOVIC’ V. (ed.). Cali, Feriva, 1996,187-193.
COMPTON J. Nucleic acid sequence-based amplification. Nature, 1991, 350 : 91-92.
CORREIA T. G., DE PAULA E. F., ANDRADA-SERPA M. J.HTLV-I infection in mice and rats. AIDS Res. Hum. Retroviruses, 2001, 17 (Suppl. 1) : S-45.
DE CASTRO-COSTA C. M. A preliminary analysis of anexperimental long-term study of motor behavior and clinical aspects of Wistar rats inoculated withblood from HTLV-I positive TSP patients fromCeará (Northeastern Brazil). In : HTLV – Truthsand Questions. ZANINOVIC’ V. (ed.). Cali, Feriva,1996b, 89-95.
DE CASTRO-COSTA C. M. A review of tropical spasticparaparesis in Ceará (Northeastern Brazil). In : HTLV – Truths and Questions. ZANINOVIC’ V. (ed.).Cali, Feriva, 1996a, pp. 105-130.
DE CASTRO-COSTA C. M. Análisis comparativo entre laParaparesia Espástica Tropical humana y la exper-
imental. In : La PET/HAM – La Paraparesia Espástica Tropical o Mielopatía Asociada con el HTLV-I . ZANINOVIC’ V., DE CASTRO-COSTA C. M.(eds.). Cali, Colciencias-Feriva, 1998, 124-130.
DE CASTRO-COSTA C. M., CARTON H., GOUBAU P., DE
FIGUEIREDO E. G., GIFFONI S. D. A. ParaparesiaEspástica Tropical nos Trópicos e Brasil : AnáliseHistórica. Arq. Neuropsiquiatr., 1994, 52 (1) : 106-109.
DE CASTRO-COSTA C. M., CARTON H., SANTOS T. J. T.HTLV-I Negative Tropical Spastic Paraparesis : AScientific Challenge. Arq. Neuropsiquiatr., 2001,59 (2-A) : 289-294 ;
DE CASTRO-COSTA C. M., DOM R.,CARTON H.,GOUBAU P.,
FERREIRA M. V. P., NETO F. U. S. A pathologicalanalysis of two first Brazilian autopsied cases of HAM/TSP (abstract). J . Acquir . Immune Defic.Syndr . Hum. Retrovirol., 1995b, 10 : 229.
DE CASTRO-COSTA C. M., FIGUEIREDO E. G., SANTOS T. J.T., FROTA C. H., LOBO C. C. G. et al. ExperimentalHTLV-I infection and associated myelopathy. Arq. Neuropsiquiatr ., 1998, 56 (3-A) : 44-497.
DE CASTRO-COSTA C. M., GOUBAU P., LIU H. F.,VANDAMME A. M., DA CUNHA F. M. B. et al. HTLV-Negative and HTLV Type I-Positive TropicalSpastic Paraparesis in Northeastern Brazil. AIDS Res. Hum. Retroviruses, 1995a, 11 (2) : 315-318.
DE CASTRO-COSTA C. M., SCIOT R., CARTON H. Are spe-cific HTLV-I antibodies involved in the selectivedegeneration of the lateral columns of the thoracicspinal cord in HAM/TSP ? Acta Neurol. Colomb.,1999, 15 (Suppl. 2) : 9-10.

8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 8/9
28 C. M. DE CASTRO COSTA ET AL.
EDLICH R. F., ARNETTE J. A., WILLIAMS F. M. Globalepidemic of human T-cell lymphotropic virustype-I (HTLV-I). J. Emerg. Med ., 2000, 18 (1) :109-119.
FOSTER A., MORGAN O., YOUNG R., MCKECHNIE R.,RODGERS-JOHNSON P. Central motor conduction
time in tropical spastic paraparesis – a magneticstimulation study. Electroencephal. Clin. Neurophysiol., 1993, 86 : 10P.
FURUZONO H., NAKAZATO O., GOTO K., AKIZUKI S.,OKAJIMA T. An autopsy case of HTLV-I associatedmyelopathy (HAM). Clin. Neurol. (Japan), 1989,29 : 349-354.
GESSAIN A., BARIN F., VERNANT J. C., GOUT O., MAURS L.et al. Antibodies to human T-lymphotropic virustype I in patients with tropical spastic paraparesis. Lancet , 1985, 2 : 407-409.
GROSSMAN W. J., RATNER L. Transgenic mouse modelsfor HTLV-I infection. J. Acquir. Immune Defic.Syndr. Hum. Retrovirol., 1996, 13 (suppl. 1) :
S162-S169.ISHIGURO H., ABE M., SETO K., SAKURAI H., IKEDA H. et
al. A rat model of human T-lymphocyte virus typeI (HTLV-I) infection. 1. Humoral antibodyresponse, provirus integration, and HTLV-I associ-ated myelopathy / tropical spastic paraparesis-likemyelopathy in seronegative HTLV-I carrier rats. J . Exp. Med ., 1992, 176 : 981-989.
IWASAKI Y. Pathology of chronic myelopathy associatedwith HTLV-I infection (HAM/TSP). J . Neurol.Sci., 1990, 96 : 103-123.
IZUMO S., USUKU K., OSAME M., MACHIGASHIRA K.,JOHNOSONO J., NAKAGAWA M. The neuropathology
of HTLV-I associated myelopathy in Japan : reportof an autopsy case and review of the literature. In : HTLV-I and the Nervous System. ROMÁN G. C.,VERNANT J. C., OSAME M. (eds.). New York, AlanR. Liss Inc., 1989, 261-267.
JACOBS J. M., MILLER R. H., WHITTLE A., CAVANAH J. B.Studies on the early changes in acute isoniazidneuropathy in the rat. Acta Neuropathol. (Berl.),1979, 47 : 85-92.
KOBAYASHI I., OTA K., YAMAMOTO K., MURAKAMI H.,MARUYAMA S. An autopsy case of HTLV-I asso-ciated myelopathy. Neurol. Med ., 1989, 30 : 409-412.
KUSHIDA S., MATSUMURA M., TANAKA H.,AMI Y., HORI M.et al. HTLV-I associated myelopathy / tropicalspastic paraparesis-like rats by intravenous infec-tion of HTLV-I producing rabbit or human T-cellline into adult WKA rats. Jpn. J . Cancer Res.(Gann), 1993, 84 : 831-833.
KUSHIDA S., MIZUSAWA H., MATSUMURA M., TANAKA H.,AMI Y. et al. High incidence of HAM/TSP-likesymptoms in WKA rats after administration of human T-cell leukemia virus type I producingcells. J . Virol., 1994, 68 (11) : 7221-7226.
LAMPERT P., O’BRIEN J., GARRET R. Hexachloropheneencephalopathy. Acta Neuropathol. (Berl.), 1973,23 : 326-333.
LEITE A. C., ALAMY A. H., OLIVEIRA A. L. A.,VEZZANI R.,GUIMARÃES P. A. P. et al. Other neurological abnor-malities associated to HTLV-1. AIDS Res. Hum. Retroviruses, 2001, 17 (Suppl. 1) : S-19.
LEITE A. C., SERAPIÃO M. J., NEVES E. S., LENZI M. E. R.,NASCIMENTO D. J., ARAÚJO A. Q. C. Autopsy find-
ings in two cases of HTLV-I myelopathy(HAM/TSP). In : VIII th International Conferenceon Human Retrovirology : HTLV . Rio de Janeiro,Brazil, Jun., 1997, CS 15.
LEÓN-S F. E., DE CASTRO-COSTA C. M., GAFFGA M.Discrepancy, coincidence or evidence in chronic
idiopathic spastic paraparesis throughout theworld : a meta-analysis of 2811 patients. Arq. Neuropsiquiatr ., 1997, 55 (3-B) : 530-535.
LOUIS J. C., MAGAL E., TAKAYAMA S., VARON S. CNTFprotection of oligodendrocytes against natural andtumor necrosis factor-induced death. Science,1993, 259 : 689-692.
MANI K. S., MANI A. J., MONTGOMERY R. D. A spasticparaplegic syndrome in South India. J . Neurol.Sci., 1969, 9 : 179-199.
MINAGAWA H., MORA C. A., ASHER D. M., STONE G. A.,LIBERSKI P. P., GIBBS C. J. Transmission of humanT-cell leukemia virus type I from a patient withHTLV-I associated myelopathy / tropical spastic
paraparesis and a asymptomatic carrier to rabbits. Arch. Virol., 1991, 118 : 235-245.
MIZUSAWA H., KUSHIDA S., MATSUMURA M., TANAKA H.,AMI Y. et al. A neuropathological study of para-paretic rats infected with HTLV-I producing T-cells. J . Neurol. Sci., 1994, 126 : 101-108.
MONTGOMERY R. D., CRUICKSHANK E. K., ROBERTSON W.E., MACMENEMEY W. H. Clinical and pathologicalobservation on Jamaican neuropathy : a report of 206 cases. Brain, 1964, 87 : 425-462.
MORITOYO H., ARIMURA K., ARIMURA Y., TOKIMURA Y.,ROSALES R., OSAME M. Study of lower limbsomatosensory evoked potentials in 96 cases of
HTLV-I associated myelopathy / tropical spasticparaparesis. J. Neurol. Sci., 1996, 138 : 78-81.OGATA A., NAGASHIMA K., TASHIRO K., MIYAKAWA A.,
MIKUNI C. H. MRI-pathological correlate of brainlesions in a necropsy case of HTLV-I associatedmyelopathy. J . Neurol. Neurosurg. Psychiatry,1993, 56 : 194-196.
OSAME M., USUKU K., IZUMO S., IJICHI N., AMITANI H. et al. HTLV-I associated myelopathy : a new clinicalentity. Lancet , 1985, 1 : 1031-1032.
PICARDO P., CERONI M., RODGERS-JOHNSON P., MORA C.,ASHER D. M. et al. Pathological and immunologi-cal observations on tropical spastic paraparesis inpatients from Jamaica. Ann. Neurol., 1988, 23
(Suppl.) : S156-S160.PUCCIONI-SOHLER M., KITZE B., FELGENHAUER K. HTLV-I
associated myelopathy in patients from Brazil andIran : neurological manifestations and cere-brospinal fluid findings. Arq. Neuropsiquiatr .,1995, 53 : 213-217.
ROMÁN G. C., OSAME M. Identity of HTLV-I associatedtropical spastic paraparesis and HTLV-I associatedmyelopathy (Letter). Lancet , 1988, 1 : 651.
SPILLANE J. D. Tropical neurology. Oxford Univ. Press.,1973.
WOLCOTT M. J. Advances in nucleic acid-based detectionmethods. Clin. Microbiol. Rev., 1992, 5 (4) : 370-
386.WU E., DICKSON D. W., JACOBSON S., RAINE C. S.Neuroaxonal dystrophy in HTLV-I associatedmyelopathy / tropical spastic paraparesis : neuro-pathologic and neuroimmunologic correlations. Acta Neuropathol., 1993, 86 : 224-235.

8/10/2019 Neuropathology of Human and Experimental TSP-HAM a Critical Review
http://slidepdf.com/reader/full/neuropathology-of-human-and-experimental-tsp-ham-a-critical-review 9/9
NEUROPATHOLOGY OF HUMAN AND EXPERIMENTAL TSP / HAM 29
YOSHIKI T. Chronic progressive myeloneuropathy inWKA rats induced by HTLV-I infection as an ani-mal model for HAM/TSP in humans. Inter-virology, 1995, 38 : 229-237.
YOSHIKI T. Rat models for HTLV-I infection. AIDS Res. Hum. Retroviruses, 2001, 17 (Suppl.) : S14.
YOSHIOKA A.,HIROSE G.,VEDA Y., NISHIMURA Y., SAKAI K.Neuropathological studies of the spinal cord inearly stage HTLV-I associated myelopathy(HAM). J . Neurol. Neurosurg. Psychiatry, 1993,56 : 1004-1007.
ZANINOVIC’ V. On the etiology of tropical spastic para-paresis and human T-cell lymphotropic virus-I-associated myelopathy. Intern. J. Infect. Dis.,1999, 3 (3) : 168-177.
C. M. DE CASTRO COSTA,Lab. de Neurologia
Experimental e Neurofisiologia,Depto. de Fisiologia e Farmacologia,
Universidade Federal do Ceará,Rua Cel. Nunes de Melo, 1127,
Rodolfo Teófilo, Fortaleza-CE – 60.430-270.E-mail : [email protected]
Related Documents











