Neuromuscular Neuromuscular Junction Junction Disorders Disorders Abdullah Al-Salti R3 Abdullah Al-Salti R3 AHD 9 march 2011 AHD 9 march 2011

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Neuromuscular Neuromuscular Junction Junction DisordersDisorders
Abdullah Al-Salti R3Abdullah Al-Salti R3
AHD 9 march 2011AHD 9 march 2011
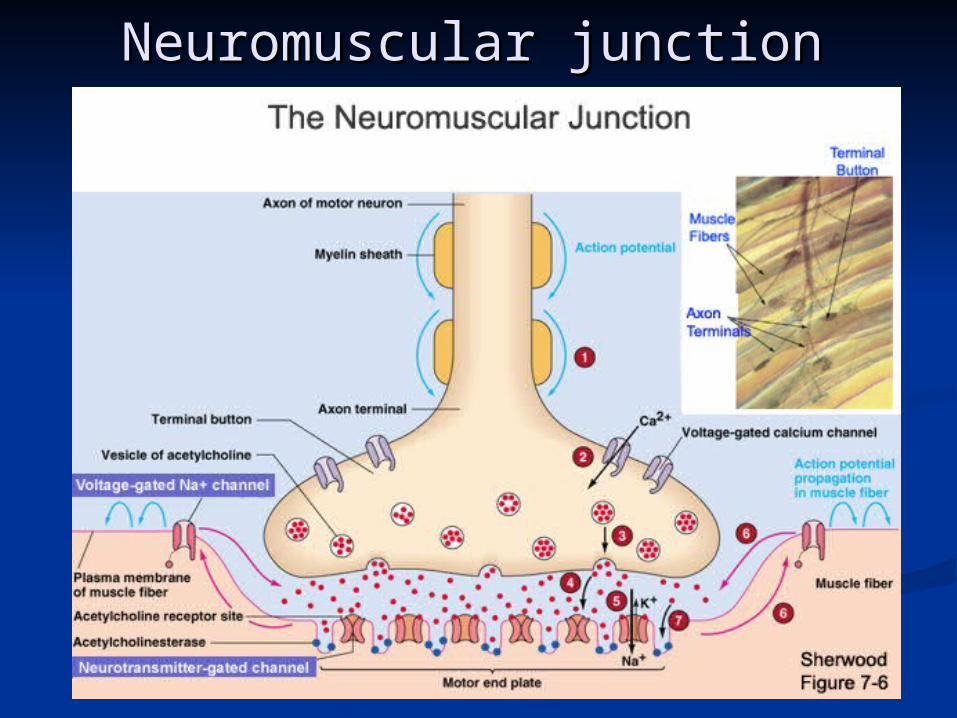
Neuromuscular junctionNeuromuscular junction
Myasthenia GravisMyasthenia Gravis::
a chronic autoimmune neuromuscular disease characterized by a chronic autoimmune neuromuscular disease characterized by varying degrees of weakness of the skeletal (voluntary) muscles varying degrees of weakness of the skeletal (voluntary) muscles of the bodyof the body..
Age and GenderAge and Gender::
Myasthenia gravis presents at any age. Female incidence Myasthenia gravis presents at any age. Female incidence peaks in the third decade of life, whereas male incidence peaks in the third decade of life, whereas male incidence peaks in the sixth or seventh decade.peaks in the sixth or seventh decade.
The female-to-male ratio is said classically to be 6:4, but as The female-to-male ratio is said classically to be 6:4, but as the population has aged, the incidence is now equal in males the population has aged, the incidence is now equal in males and femaleand female
Inheritance:Inheritance: 1st degree relatives have 1000x the rest of general 1st degree relatives have 1000x the rest of general
populationpopulation inc. jitter on SFEMG demonstrated in 33-45% of inc. jitter on SFEMG demonstrated in 33-45% of
asymptomatic 1st degree relativesasymptomatic 1st degree relatives Inc. titres of AChR antibodies in up to 50%Inc. titres of AChR antibodies in up to 50%
Myasthenia GravisMyasthenia Gravis
PathophysiologyPathophysiologyImmunoglobulin G (IgG) directed attack on the NMJ, aimed Immunoglobulin G (IgG) directed attack on the NMJ, aimed specifically at the nicotinic acetylcholine (ACH) receptorspecifically at the nicotinic acetylcholine (ACH) receptor..
Damage to the ACH receptor and Damage to the ACH receptor and postsynaptic postsynaptic membrane membrane involves several stepsinvolves several steps..
First, binding of the antibody to the receptor First, binding of the antibody to the receptor can directly block the binding of ACH. can directly block the binding of ACH.
Second, there is a complement-directed Second, there is a complement-directed attack, with destruction of the ACH receptor attack, with destruction of the ACH receptor and post junctional folds. and post junctional folds.
Third antibody binding can result in an Third antibody binding can result in an increase in the normal removal of ACH increase in the normal removal of ACH receptors from the postsynaptic membrane. receptors from the postsynaptic membrane.
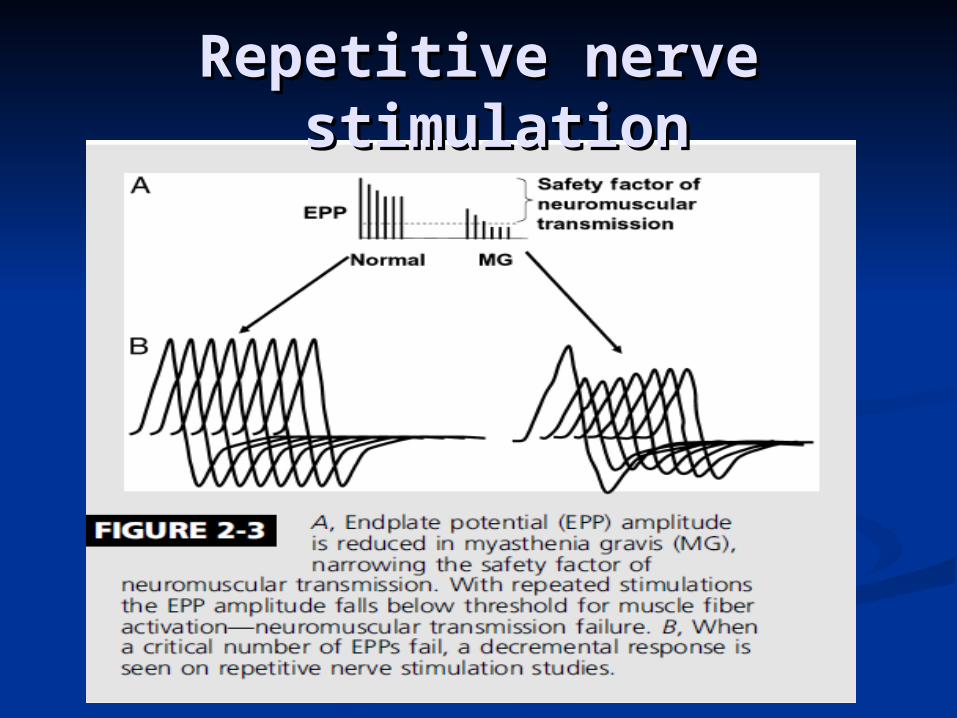
Resulting in a smaller endplate potential and a reduced Resulting in a smaller endplate potential and a reduced safety factor of NMJ transmissionsafety factor of NMJ transmission..
PathophysiologyPathophysiology
The MuSK The MuSK
maintains the maintains the normal functional integrity of the NMJnormal functional integrity of the NMJ anti-MuSK antibodies may anti-MuSK antibodies may alter the normal alter the normal
maintenancemaintenance of a high density of AChRs at the NMJ of a high density of AChRs at the NMJ leading to leading to reduced numbers of functional AChRs.reduced numbers of functional AChRs.
Thymus gland.Thymus gland.greater than 50% of antigreater than 50% of anti–– AChR-positive AChR-positive
patients having thymic hyperplasia and 10% patients having thymic hyperplasia and 10% to 15% having a thymic tumor.to 15% having a thymic tumor.
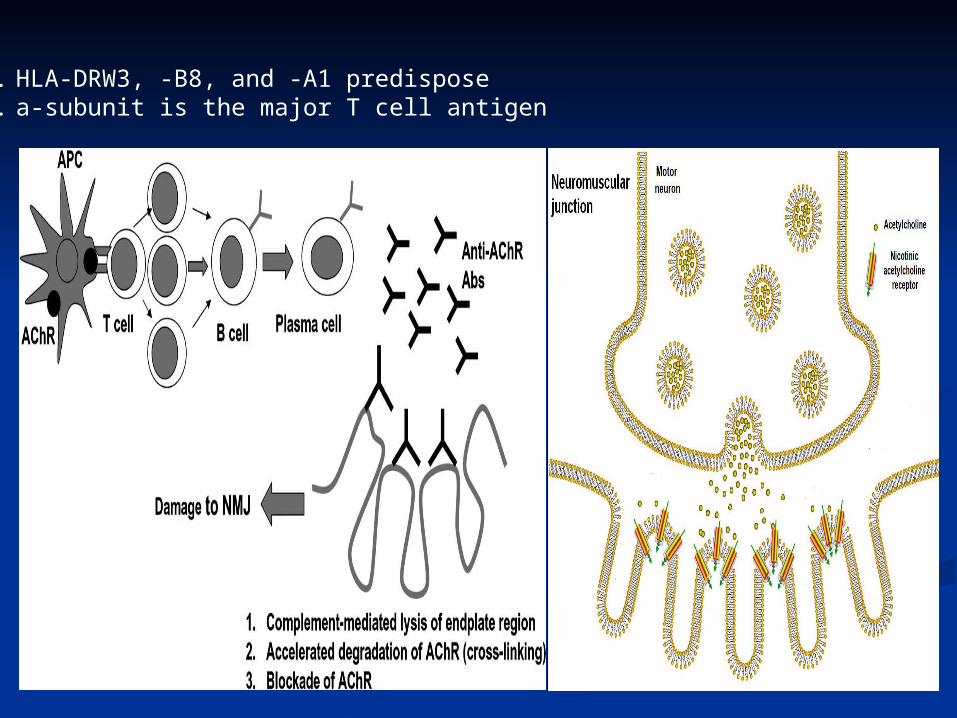
1. HLA-DRW3, -B8, and -A1 predispose2. a-subunit is the major T cell antigen
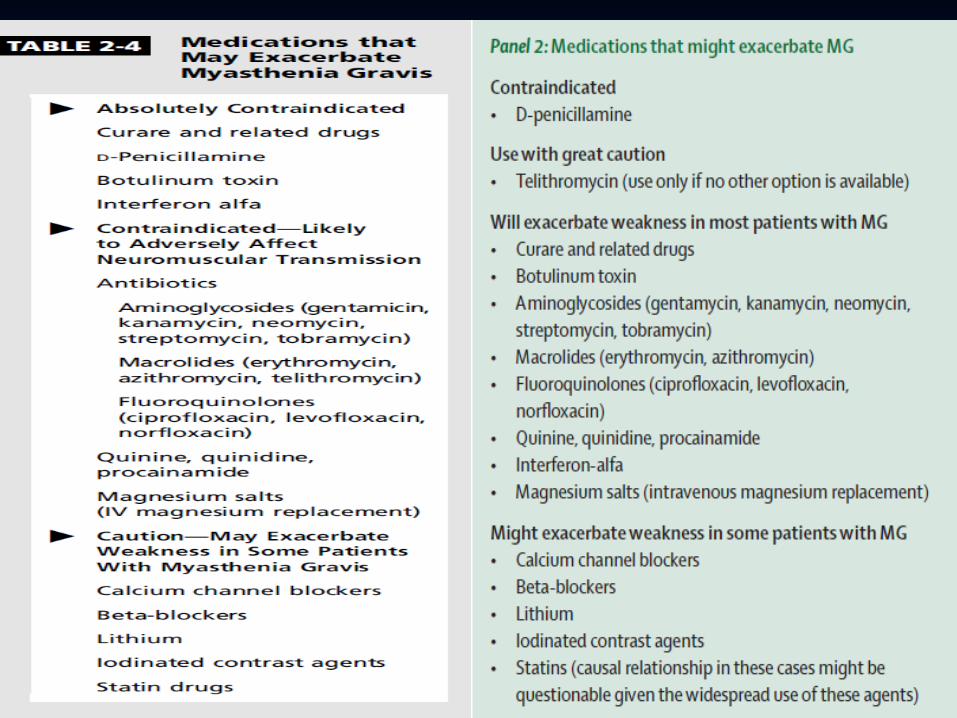
EtiologyEtiology Acquired autoimmune Acquired autoimmune Drug-induced : D-penicillamineDrug-induced : D-penicillamine Transient neonatal (passive transfer Transient neonatal (passive transfer
of maternal anti-AChR antibodies)of maternal anti-AChR antibodies) Congenital myasthenic syndromeCongenital myasthenic syndrome
Clinical presentationClinical presentation most commonly presents with weakness of most commonly presents with weakness of
extraocular muscles ptosis and/or diplopia, +/- extraocular muscles ptosis and/or diplopia, +/- photophobiaphotophobia
can mimic any pattern of ophthalmoplegia can mimic any pattern of ophthalmoplegia including pupil sparing IIIrd nerve palsy, including pupil sparing IIIrd nerve palsy, internuclear ophthalmoplegia (INO) or sixth nerve internuclear ophthalmoplegia (INO) or sixth nerve palsypalsy
Bulbar involvement common eventually dysphagia, Bulbar involvement common eventually dysphagia, dysarthria, dysphonia (hypernasal or hoarse)dysarthria, dysphonia (hypernasal or hoarse)
reduced facial expression, jaw fatiguereduced facial expression, jaw fatigue
generally progresses over time so that within 2 generally progresses over time so that within 2 years of onset of ocular MG, 90% have bulbar and years of onset of ocular MG, 90% have bulbar and proximal symmetric limb weaknessproximal symmetric limb weakness
Early SymptomsEarly Symptoms frequent purchase of new eyeglasses to correct frequent purchase of new eyeglasses to correct
blurred visionblurred vision sleepy or sad facial appearancesleepy or sad facial appearance avoidance of difficult to chew foodsavoidance of difficult to chew foods cessation of activities requiring specific muscles (e.g. cessation of activities requiring specific muscles (e.g.
singing)singing)
Presenting SymptomsPresenting Symptoms ptosis or diplopia (2/3 of patients)ptosis or diplopia (2/3 of patients)
present in almost all within 2 years of onsetpresent in almost all within 2 years of onset difficulty chewing, swallowing, talking (1/6)difficulty chewing, swallowing, talking (1/6) limb weakness (1/10)limb weakness (1/10)
Rarely limited to single muscle groupRarely limited to single muscle group
Diurnal VariationDiurnal VariationExacerbating FactorsExacerbating Factors
Clinical presentationClinical presentation
Natural HistoryNatural History
Restricted to ocular muscles in 10% of patients. Restricted to ocular muscles in 10% of patients. 90% have progressive weakness over two years involving 90% have progressive weakness over two years involving
oropharyngeal and limb muscles.oropharyngeal and limb muscles. 2/3 of patients reach remission within 1 year2/3 of patients reach remission within 1 year Spontaneous remission can occur, usually earlySpontaneous remission can occur, usually early
StagesStages1.1. Active stageActive stage
1.1. brief period of fluctuationbrief period of fluctuation2.2. more severemore severe
2.2. Inactive stageInactive stage1.1. fluctuations attributable to fatigue, intercurrent illnessfluctuations attributable to fatigue, intercurrent illness
3.3. Burnt out stage (15-20 years)Burnt out stage (15-20 years)1.1. fixed weaknessfixed weakness2.2. atrophic musclesatrophic muscles
Clinical presentationClinical presentation

Physical FindingsPhysical FindingsOcular MusclesOcular Muscles
PtosisPtosis assymetricalassymetrical covering ptotic lid may relieve contraction of opposite covering ptotic lid may relieve contraction of opposite
frontalisfrontalis passively lifting ptotic lid may cause opposite lid to fallpassively lifting ptotic lid may cause opposite lid to fall varies during sustained activityvaries during sustained activity may shift from eye to eye - pathognomonicmay shift from eye to eye - pathognomonic edrophonium responseedrophonium response
EOMsEOMs ³³N muscle without pupil involvementN muscle without pupil involvement variable, fluctuating, and fatigablevariable, fluctuating, and fatigable most severe in medial rectusmost severe in medial rectus ““pseudo-INOpseudo-INO”” edrophonium may improve only one of several edrophonium may improve only one of several
weak ocular musclesweak ocular muscles
Physical FindingsPhysical Findings Oropharyngeal MusclesOropharyngeal Muscles
altered facial appearance altered facial appearance –– depressed , snarl/sad depressed , snarl/sad examiner can manually open jaw against resistanceexaminer can manually open jaw against resistance impaired strength of eye closureimpaired strength of eye closure nasal regurgitationnasal regurgitation difficulty swallowingdifficulty swallowing hoarseness (larynx)hoarseness (larynx) nasal voice, especially after prolonged talkingnasal voice, especially after prolonged talking
Limb MusclesLimb Muscles neck flexors > extensorsneck flexors > extensors deltoids, triceps, wrist extensors, finger extensors deltoids, triceps, wrist extensors, finger extensors
especially affectedespecially affected ankle dorsiflexors preferentially affectedankle dorsiflexors preferentially affected fatigabilityfatigability

Diagnostic ProceduresDiagnostic Procedures
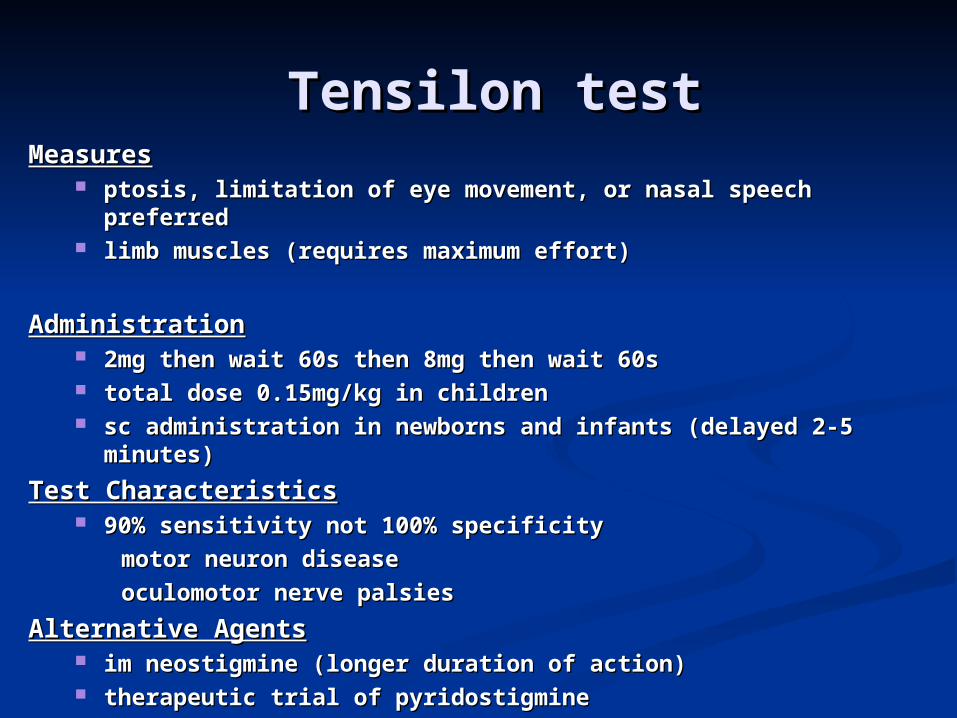
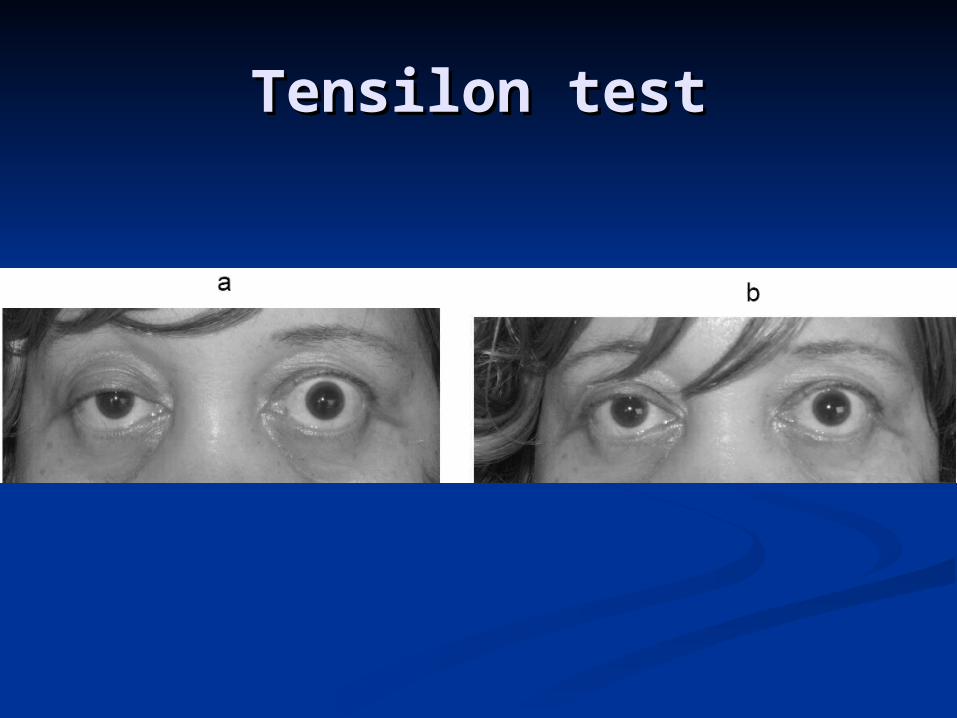
Tensilon testTensilon test MeasuresMeasures
ptosis, limitation of eye movement, or nasal speech ptosis, limitation of eye movement, or nasal speech preferredpreferred
limb muscles (requires maximum effort)limb muscles (requires maximum effort)
AdministrationAdministration 2mg then wait 60s then 8mg then wait 60s 2mg then wait 60s then 8mg then wait 60s total dose 0.15mg/kg in childrentotal dose 0.15mg/kg in children sc administration in newborns and infants (delayed 2-5 sc administration in newborns and infants (delayed 2-5
minutes)minutes)
Test CharacteristicsTest Characteristics 90% sensitivity not 100% specificity90% sensitivity not 100% specificity
motor neuron diseasemotor neuron disease
oculomotor nerve palsiesoculomotor nerve palsies
Alternative AgentsAlternative Agents im neostigmine (longer duration of action)im neostigmine (longer duration of action) therapeutic trial of pyridostigmine therapeutic trial of pyridostigmine
Tensilon testTensilon test
Antibodies Against Antibodies Against Acetylcholine ReceptorsAcetylcholine Receptors
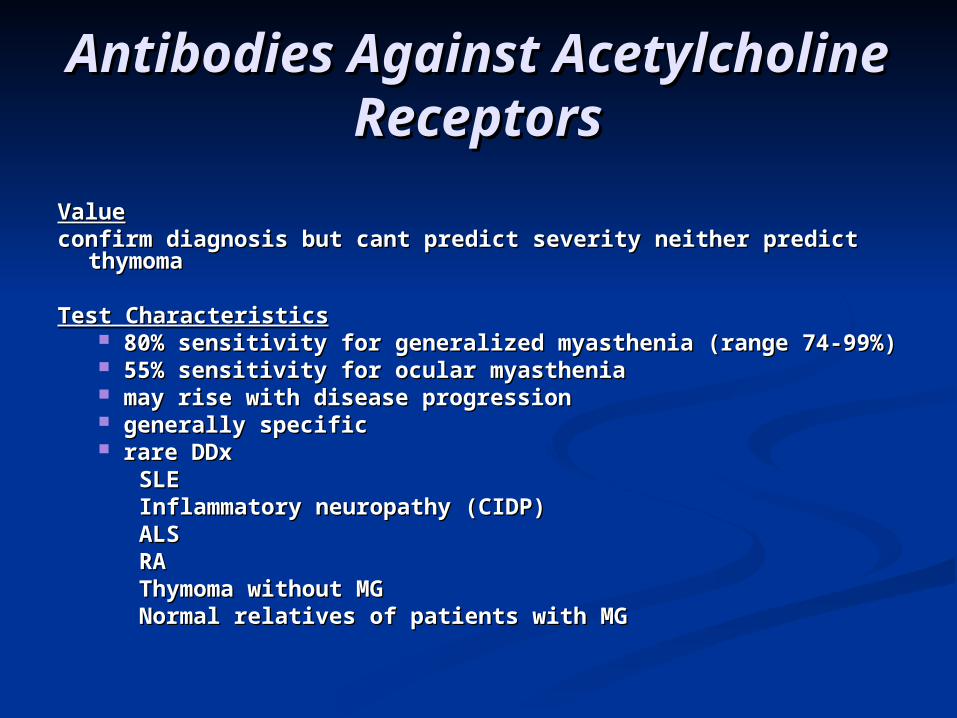
ValueValueconfirm diagnosis but cant predict severity neither predict confirm diagnosis but cant predict severity neither predict
thymomathymoma
Test CharacteristicsTest Characteristics 80% sensitivity for generalized myasthenia (range 74-99%)80% sensitivity for generalized myasthenia (range 74-99%) 55% sensitivity for ocular myasthenia55% sensitivity for ocular myasthenia may rise with disease progressionmay rise with disease progression generally specificgenerally specific rare DDxrare DDx
SLESLEInflammatory neuropathy (CIDP)Inflammatory neuropathy (CIDP)ALSALSRARAThymoma without MGThymoma without MGNormal relatives of patients with MGNormal relatives of patients with MG

Ocular coolingOcular cooling
Specificity??Specificity?? Positive 80%, no positive response in Positive 80%, no positive response in
patients with ptosis not due to myasthenia patients with ptosis not due to myasthenia Alternative to tensilon test Alternative to tensilon test Improvement in lid ptosis after the eye is Improvement in lid ptosis after the eye is
cooled with ice pack 2 minutes cooled with ice pack 2 minutes
Repetitive nerve Repetitive nerve stimulationstimulation
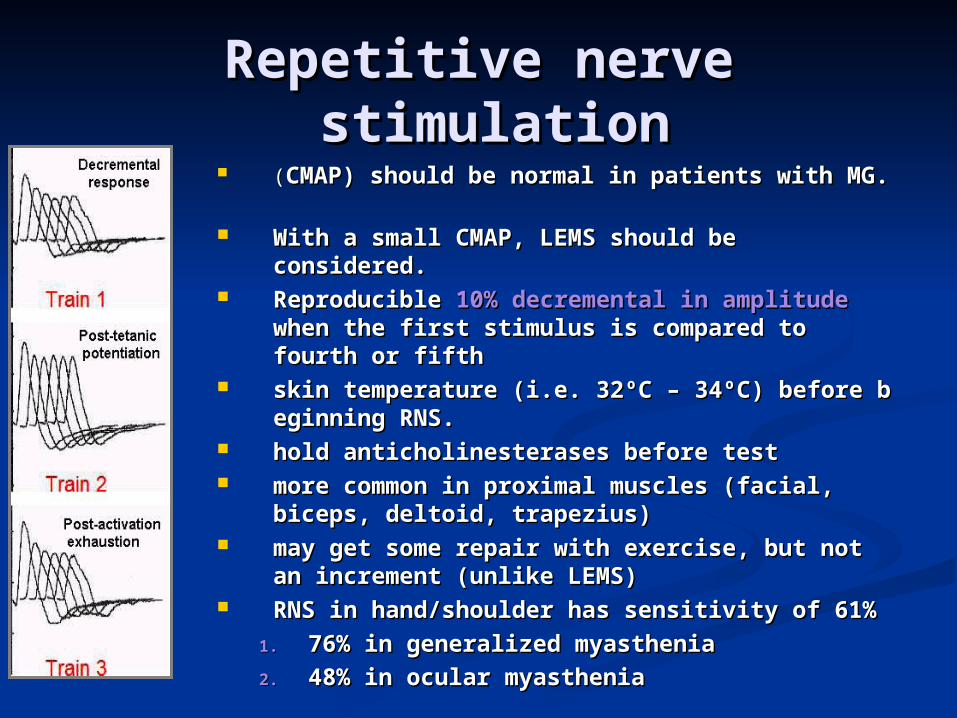
((CMAP) should be normal in patients with CMAP) should be normal in patients with MG. MG.
With a small CMAP, LEMS should be With a small CMAP, LEMS should be considered.considered.
Reproducible Reproducible 10% decremental in amplitude10% decremental in amplitude when the first stimulus is compared to fourth when the first stimulus is compared to fourth or fifth or fifth
32skin temperature (i.e. 32skin temperature (i.e. ºº C C –– 34 34ºº C) before be C) before be RRRR. RRRR.
hold anticholinesterases before testhold anticholinesterases before test more common in proximal muscles (facial, more common in proximal muscles (facial,
biceps, deltoid, trapezius)biceps, deltoid, trapezius) may get some repair with exercise, but not may get some repair with exercise, but not
an increment (unlike LEMS)an increment (unlike LEMS) RNS in hand/shoulder has sensitivity of 61%RNS in hand/shoulder has sensitivity of 61%
1.1. 76% in generalized myasthenia76% in generalized myasthenia2.2. 48% in ocular myasthenia48% in ocular myasthenia
Repetitive nerve Repetitive nerve stimulationstimulation

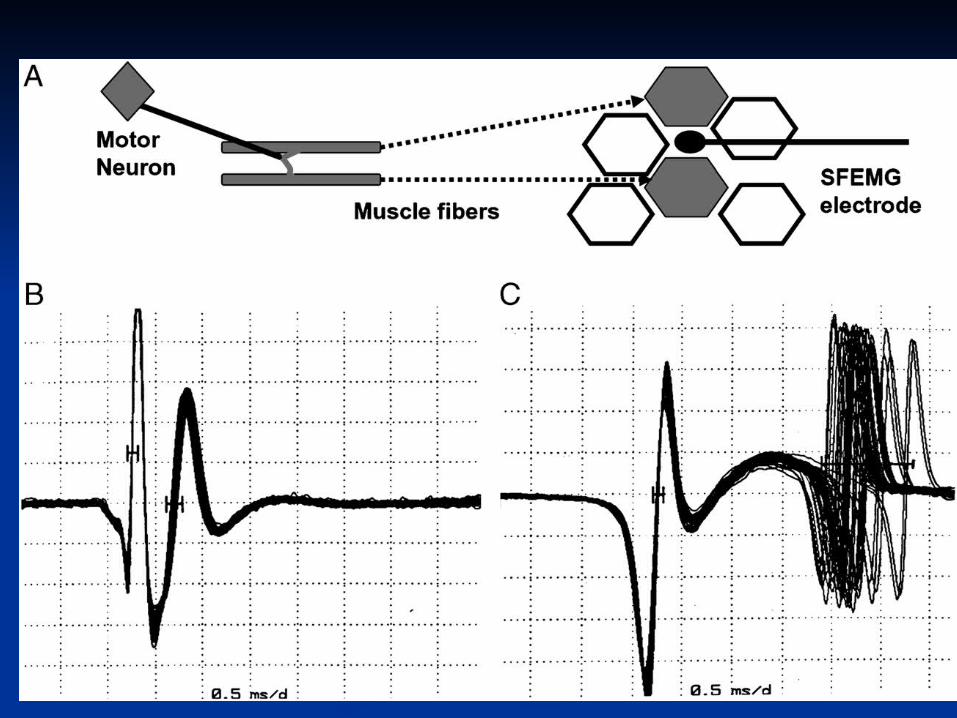
SFEMGSFEMG
(MUAP) abnormalities suggestive of a NMJ disorder,unstable (MUAP) abnormalities suggestive of a NMJ disorder,unstable MUAP, small, short-duration.MUAP, small, short-duration.
At least one symptomatic muscle At least one symptomatic muscle Increased jitter and blockingIncreased jitter and blocking Jitter is greatest in weak musclesJitter is greatest in weak muscles Measure 2 time locked motor unitsMeasure 2 time locked motor units SENSITIVE: 99% sensitive for generalized and 97% SENSITIVE: 99% sensitive for generalized and 97%
sensitive for ocularsensitive for ocular NONSPECIFICNONSPECIFIC
any other motor unit diseaseany other motor unit disease must perform EMG and NCS to exclude neuronopathy, must perform EMG and NCS to exclude neuronopathy,
neuropathy, myopathyneuropathy, myopathy limb limb jitter DOES NOT predict development of generalized jitter DOES NOT predict development of generalized
myastheniamyasthenia should examine 20 pairs in each muscle should examine 20 pairs in each muscle
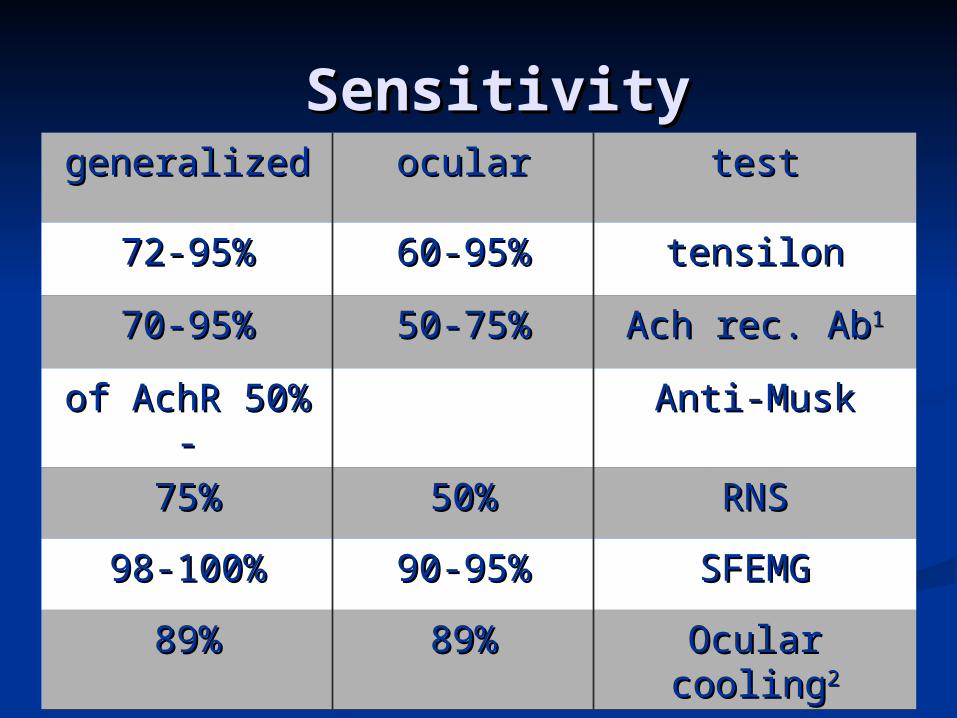
SensitivitySensitivity testtestocularoculargeneralizedgeneralized
tensilontensilon60-95%60-95%72-95%72-95%
Ach rec. AbAch rec. Ab1150-75%50-75%70-95%70-95%
Anti-MuskAnti-Musk50%50% of AchRof AchR- -
RNSRNS50%50%75%75%
SFEMGSFEMG90-95%90-95%98-100%98-100%
Ocular coolingOcular cooling2289%89%89%89%

Comparison of Diagnostic Comparison of Diagnostic TechniquesTechniques
Tensilon test diagnostic if positive in Tensilon test diagnostic if positive in patients with ptosis or ophthalmoparesispatients with ptosis or ophthalmoparesis
AChR Ab specificAChR Ab specific RNS confirms DNMJ transmission but RNS confirms DNMJ transmission but
nonspecific; often normal in mild or nonspecific; often normal in mild or ocular diseaseocular disease
SFEMG sensitive but not specificSFEMG sensitive but not specificOther Diagnostic ProceduresOther Diagnostic Procedures
CT chestCT chest TFTsTFTs TB test prior to immunosupressionTB test prior to immunosupression

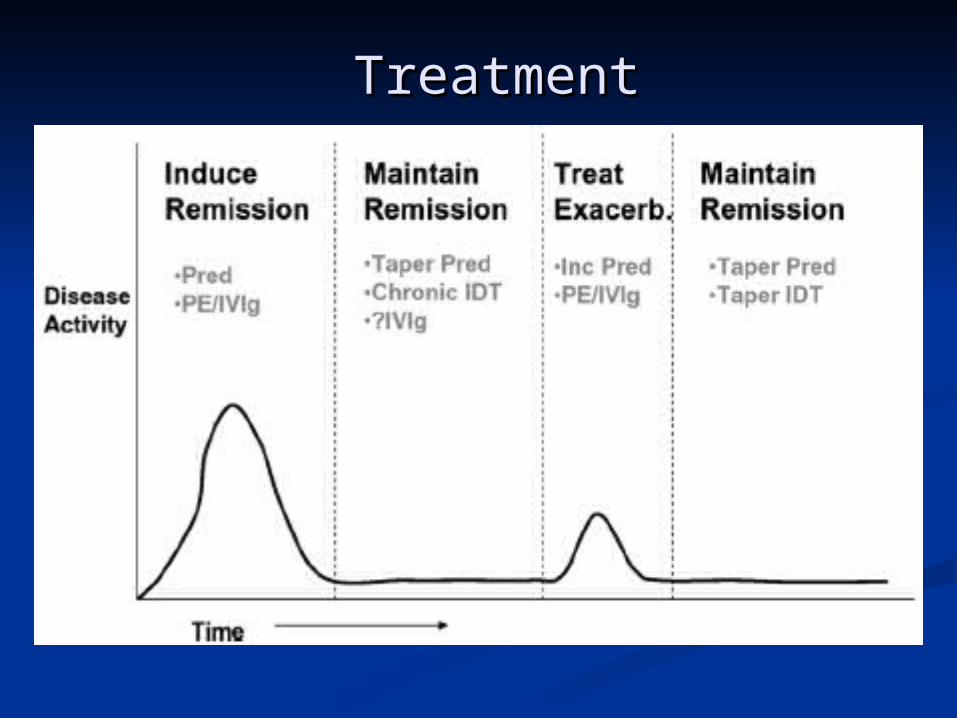
TreatmentTreatment
TreatmentTreatmentCholinesterase InhibitorsCholinesterase Inhibitors
RolesRoles diagnosticdiagnostic early, symptomatic treatmentearly, symptomatic treatment adjunct to immunomodulatory and immunosuppressive adjunct to immunomodulatory and immunosuppressive
therapy.therapy. RARELY can be used as chronic treatmentRARELY can be used as chronic treatment
usually effect diminishes with timeusually effect diminishes with timeDosingDosing
PyridostigminePyridostigmine longer duration of actionlonger duration of action initially 30-60mg q4-8 hoursinitially 30-60mg q4-8 hours 1.0mg/kg in infants and children1.0mg/kg in infants and children available in serum (60mg/5ml)available in serum (60mg/5ml) available as nebulizeravailable as nebulizer RARELY produces normal strength and RARELY RARELY produces normal strength and RARELY
completely corrects diplopiacompletely corrects diplopia
TreatmentTreatmentCholinesterase InhibitorsCholinesterase Inhibitors
NeostigmineNeostigmine initially 7.5-15.0mg q4-8hinitially 7.5-15.0mg q4-8h 0.3mg/kg in infants and children0.3mg/kg in infants and children available as IV and nebulizeravailable as IV and nebulizer
Side EffectsSide EffectsSmooth Muscle (muscarinic)Smooth Muscle (muscarinic) NxVxNxVx crampscramps diarrheadiarrhea Rx with loperamide, propantheline, Rx with loperamide, propantheline,
glycopyrrolate, diphenozylateglycopyrrolate, diphenozylateAutonomic (muscarinic)Autonomic (muscarinic)
bronchial/oral secretions bronchial/oral secretions

TreatmentTreatment Cholinesterase InhibitorsCholinesterase Inhibitors
Skeletal Muscle (nicotinic)Skeletal Muscle (nicotinic) weaknessweakness
Bromism (from Mestinon)Bromism (from Mestinon) acute psychosisacute psychosis rashrash measure bromine levelmeasure bromine level
Drug InteractionsDrug Interactions succinylcholine metabolized by succinylcholine metabolized by
acetylcholinesterase impaired metabolism acetylcholinesterase impaired metabolism can lead to potential arrythmias can lead to potential arrythmias
CorticosteroidsCorticosteroidsEfficacyEfficacy
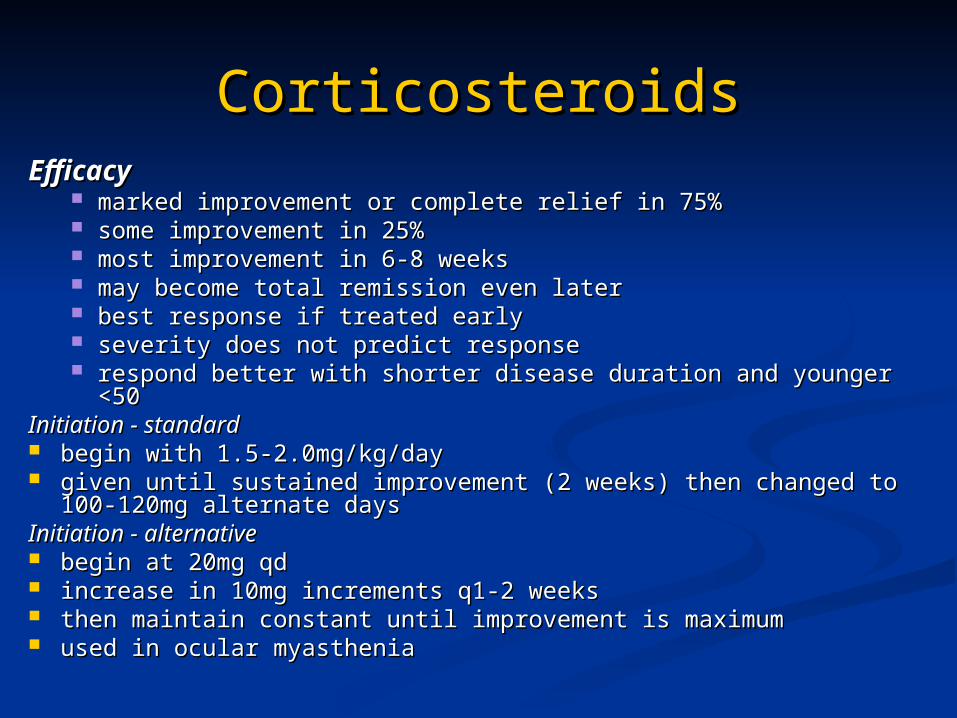
marked improvement or complete relief in 75%marked improvement or complete relief in 75% some improvement in 25%some improvement in 25% most improvement in 6-8 weeksmost improvement in 6-8 weeks may become total remission even latermay become total remission even later best response if treated earlybest response if treated early severity does not predict responseseverity does not predict response respond better with shorter disease duration and younger <50respond better with shorter disease duration and younger <50
Initiation - standardInitiation - standard begin with 1.5-2.0mg/kg/daybegin with 1.5-2.0mg/kg/day given until sustained improvement (2 weeks) then changed to 100-given until sustained improvement (2 weeks) then changed to 100-
120mg alternate days120mg alternate daysInitiation - alternativeInitiation - alternative begin at 20mg qdbegin at 20mg qd increase in 10mg increments q1-2 weeksincrease in 10mg increments q1-2 weeks then maintain constant until improvement is maximumthen maintain constant until improvement is maximum used in ocular myastheniaused in ocular myasthenia
CorticosteroidsCorticosteroids
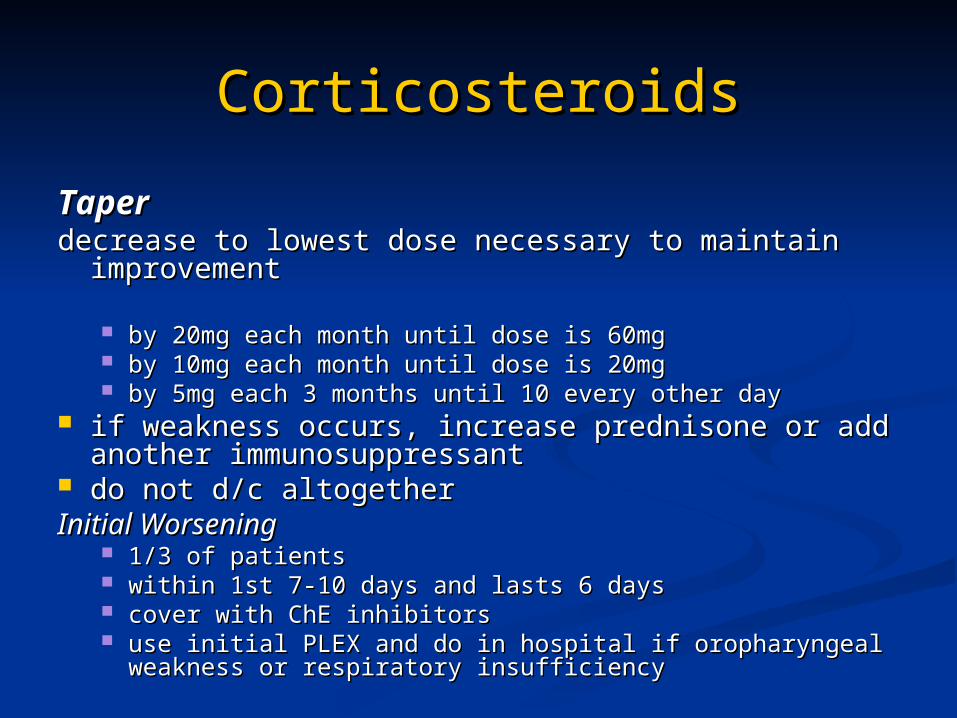
TaperTaperdecrease to lowest dose necessary to maintain decrease to lowest dose necessary to maintain
improvementimprovement
by 20mg each month until dose is 60mgby 20mg each month until dose is 60mg by 10mg each month until dose is 20mgby 10mg each month until dose is 20mg by 5mg each 3 months until 10 every other dayby 5mg each 3 months until 10 every other day
if weakness occurs, increase prednisone or add if weakness occurs, increase prednisone or add another immunosuppressantanother immunosuppressant
do not d/c altogetherdo not d/c altogetherInitial WorseningInitial Worsening
1/3 of patients1/3 of patients within 1st 7-10 days and lasts 6 dayswithin 1st 7-10 days and lasts 6 days cover with ChE inhibitorscover with ChE inhibitors use initial PLEX and do in hospital if oropharyngeal weakness use initial PLEX and do in hospital if oropharyngeal weakness
or respiratory insufficiencyor respiratory insufficiency

ImmunosupressantsImmunosupressants
AzathioprineAzathioprineRegimenRegimen start 50mg/dstart 50mg/d +50mg/d q7d+50mg/d q7d target 150-200mg/dtarget 150-200mg/d
EfficacyEfficacy improvement maintainedimprovement maintained ?synergistic with steroids?synergistic with steroids may start simultaneous with steroids and taper steroids may start simultaneous with steroids and taper steroids
when azathioprine kicks inwhen azathioprine kicks in effect takes 4-8 monthseffect takes 4-8 months maximum improvement within 12 monthsmaximum improvement within 12 months 70-90% response rate 70-90% response rate –– similar to steroids similar to steroids
ImmunosupressantsImmunosupressants
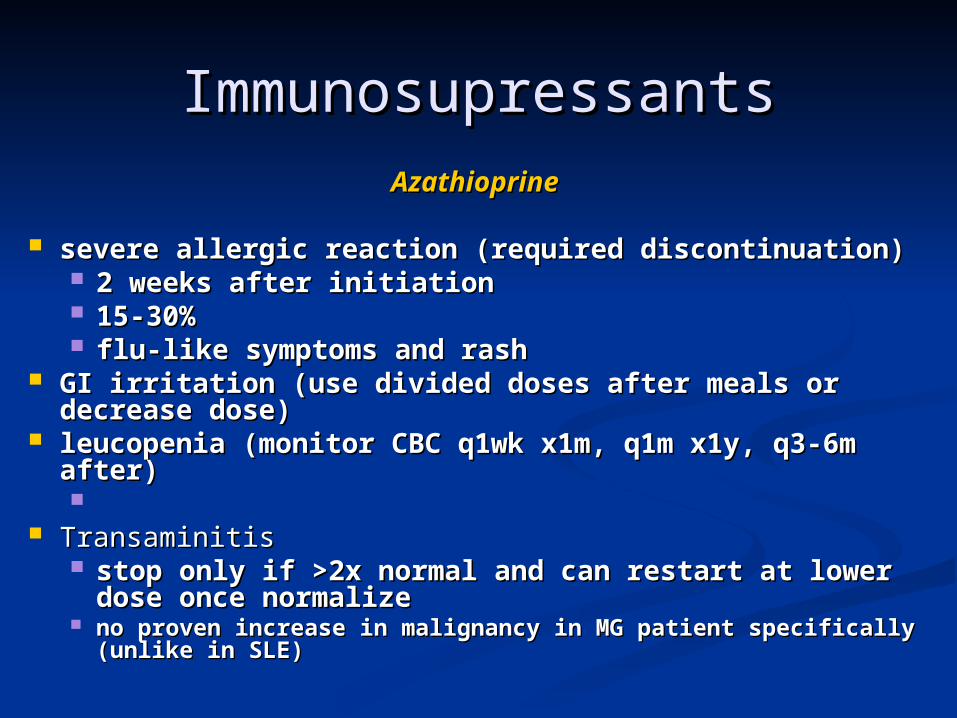
AzathioprineAzathioprine severe allergic reaction (required discontinuation)severe allergic reaction (required discontinuation)
2 weeks after initiation2 weeks after initiation 15-30%15-30% flu-like symptoms and rashflu-like symptoms and rash
GI irritation (use divided doses after meals or GI irritation (use divided doses after meals or decrease dose)decrease dose)
leucopenia (monitor CBC q1wk x1m, q1m x1y, q3-leucopenia (monitor CBC q1wk x1m, q1m x1y, q3-6m after)6m after)
TransaminitisTransaminitis stop only if >2x normal and can restart at lower stop only if >2x normal and can restart at lower
dose once normalizedose once normalize no proven increase in malignancy in MG patient no proven increase in malignancy in MG patient
specifically (unlike in SLE)specifically (unlike in SLE)
ImmunosupressantsImmunosupressants
CyclosporineCyclosporineRegimenRegimen
begin at 5-6mg/kd div q12hbegin at 5-6mg/kd div q12h trough levels after 1 month (allows tissue trough levels after 1 month (allows tissue
saturation) - aim for 75-150ng/mlsaturation) - aim for 75-150ng/mlEfficacyEfficacy
improvement in most patients taking CYAimprovement in most patients taking CYA improve within 1-2 monthsimprove within 1-2 months maximum improvement at >6monthsmaximum improvement at >6months
SFXSFX Renal toxicity . Renal toxicity . HTN (monitor q1month until steady state)HTN (monitor q1month until steady state) ++drug interactions ++drug interactions
ImmunosupressantsImmunosupressants
CyclophosphamideCyclophosphamideUseUse
severe, refractory MGsevere, refractory MGRegimenRegimen
200mg/m2 q1month200mg/m2 q1month titrate to changes in strength and side effectstitrate to changes in strength and side effects 150-200mg/d po to total of 5-10g to relieve Sx150-200mg/d po to total of 5-10g to relieve Sx
SFXSFX alopeciaalopecia cystitiscystitis leucopenialeucopenia NxVx anorexiaNxVx anorexia

ImmunosupressantsImmunosupressants Mycophenolate MofetilMycophenolate Mofetil
MechanismMechanism Selectively inhibits proliferation of B- and T- lymphocyte clones Selectively inhibits proliferation of B- and T- lymphocyte clones
responding to antigenic stimulationresponding to antigenic stimulation Suppresses formation of antibodiesSuppresses formation of antibodies
EvidenceEvidence Open label pilot study demonstrated role as adjunctive therapy Open label pilot study demonstrated role as adjunctive therapy
in refractory MGin refractory MGDosingDosing
2g/d div bid2g/d div bidEfficacyEfficacy
Improvement as early as 2 weeks and usually seen within 2 Improvement as early as 2 weeks and usually seen within 2 monthsmonths
RoleRole Refractory MGRefractory MG Steroid sparing agent when imuran intolerable or ineffectiveSteroid sparing agent when imuran intolerable or ineffective
Side EffectsSide Effects DiarrheaDiarrhea leukopenia leukopenia
Plasma ExchangePlasma Exchange RolesRoles sudden worsening of myasthenic symptoms for any reasonsudden worsening of myasthenic symptoms for any reason rapidly improve strength before surgeryrapidly improve strength before surgery concomitantly with high dose steroidsconcomitantly with high dose steroids chronic intermittent Rx in refractory MGchronic intermittent Rx in refractory MGProtocolProtocol2-3L of plasma 3x per week until improvement plateaus (usually 2-3L of plasma 3x per week until improvement plateaus (usually
after 5-6 exchanges)after 5-6 exchanges)
Adverse EffectsAdverse Effects cardiac arrhythmiascardiac arrhythmias LightheadednessLightheadedness ChillsChills Obscured visionObscured vision Pedal edemaPedal edema Hemorrhage (removal of coagulation factors)Hemorrhage (removal of coagulation factors) Hypercoagulation (removal of antithrombin III)Hypercoagulation (removal of antithrombin III) Coagulation defects corrected within24hCoagulation defects corrected within24h
IVIGIVIG IndicationsIndications Similar to PLEXSimilar to PLEX
MechanismsMechanisms blocks Fc receptors on macrophagesm blocks Fc receptors on macrophagesm anti-idiotype Ab against AChR antibodiesanti-idiotype Ab against AChR antibodies
ProtocolProtocol2g/kg over 2-5 days2g/kg over 2-5 days
SFXSFXHeadache , fever and chills, alopecia, aseptic meningitis, Headache , fever and chills, alopecia, aseptic meningitis,
leucopenialeucopeniaretinal necrosis, renal failure. retinal necrosis, renal failure.
TreatmentTreatment
Other Types Of Other Types Of Myasthenia GraviesMyasthenia Gravies
Transitory Neonatal Transitory Neonatal MyastheniaMyasthenia
clinical featuresclinical features
hypotonichypotonic onset within hours of birth but can be onset within hours of birth but can be
delayed up to 3 daysdelayed up to 3 days feed poorly in 1st 3 daysfeed poorly in 1st 3 days can get weak cry and lack of facial can get weak cry and lack of facial
expression in 50%expression in 50% 15% have limited EOM and ptosis15% have limited EOM and ptosis respiratory insufficiency rarerespiratory insufficiency rare worsens for first few days then improvesworsens for first few days then improves last 2-12 weeks (usually 2 weeks)last 2-12 weeks (usually 2 weeks)
neonatal antibodies have half life of 2-3 neonatal antibodies have half life of 2-3 weeks and not detected after 5 monthsweeks and not detected after 5 months
recovery is completerecovery is complete
Transitory Neonatal Transitory Neonatal MyastheniaMyasthenia
diagnosisdiagnosis tensilon test OR RNStensilon test OR RNS high AChR in neonate bloodhigh AChR in neonate blood
treatmenttreatment ChE for swallowing or breathing - just ChE for swallowing or breathing - just
before feedingbefore feeding neostigmine im before feedingneostigmine im before feeding can also give via NG tube at 10 times can also give via NG tube at 10 times
parenteral levelparenteral level PLEX if respiratory weakness (rare).PLEX if respiratory weakness (rare).
Anti-Musk MyastheniaAnti-Musk MyastheniaEpidemiologyEpidemiology
25% of all MG patients are seronegative25% of all MG patients are seronegative 40% of seronegative MG patients are MuSK positive (about 10% 40% of seronegative MG patients are MuSK positive (about 10%
overall)overall) M=FM=F Same age of onset as usual myastheniaSame age of onset as usual myasthenia
Normal Function of MuSKNormal Function of MuSK Tyrosine kinaseTyrosine kinase Regulates and maintains AChR at NMJRegulates and maintains AChR at NMJ
Clinical Features Clinical Features –– Differences from Typical Myasthenia Differences from Typical Myasthenia More involvement of neck, shoulder, respiratoryMore involvement of neck, shoulder, respiratory Less limbLess limb More bulbarMore bulbar Increased risk of myasthenic crisis in 1st 2 yearsIncreased risk of myasthenic crisis in 1st 2 years Greater proportion in more severe categoryGreater proportion in more severe category Outcome similar, but require more steroidsOutcome similar, but require more steroids
TreatmentTreatment Treatment generally the sameTreatment generally the same Can respond to thymectomyCan respond to thymectomy Less likely to have thymic hyperplasiaLess likely to have thymic hyperplasia
Genetic Myasthenic Genetic Myasthenic SyndromesSyndromes
Congenital MyastheniaCongenital MyastheniaGeneticsGeneticsseveral genetic defectsseveral genetic defects
EpidemiologyEpidemiology2:1 male predominance2:1 male predominance
CausesCauses Deficiency of muscle acetylcholine receptors at the end Deficiency of muscle acetylcholine receptors at the end
plateplate Some have AChR mutationsSome have AChR mutations Some have deficiency of rapsyn (receptor-associated Some have deficiency of rapsyn (receptor-associated
protein at the synapse)protein at the synapse) Abnormalities of acetylcholine resynthesis or Abnormalities of acetylcholine resynthesis or
immoblilizationimmoblilization Reduced end plate acetylcholinesteraseReduced end plate acetylcholinesterase Impaired AChR functionImpaired AChR function
Genetic Myasthenic Genetic Myasthenic SyndromesSyndromes
Congenital MyastheniaCongenital Myasthenia Clinical FeaturesClinical Features ophthalmoparesis and ptosis developing in infancyophthalmoparesis and ptosis developing in infancy
incomplete at onsetincomplete at onset progresses to complete paralysis during infancy or progresses to complete paralysis during infancy or
childhoodchildhood mild facial paresismild facial paresis limb weakness mild compared to opthalmoplegialimb weakness mild compared to opthalmoplegia respiratory distress unusualrespiratory distress unusual symptoms may not fluctuate muchsymptoms may not fluctuate much
Genetic Myasthenic Genetic Myasthenic SyndromesSyndromes
Congenital MyastheniaCongenital Myasthenia
DiagnosisDiagnosis subcutaneous injection of edrophonium subcutaneous injection of edrophonium
transitory improvement in ocular motilitytransitory improvement in ocular motility RNSRNS
Decrement found in some limb musclesDecrement found in some limb muscles May be necessary to test proximal or facial muscles if May be necessary to test proximal or facial muscles if
limbs normallimbs normal
SFEMGSFEMGTreatmentTreatment
ChE inhibitors improve limb weakness in many formsChE inhibitors improve limb weakness in many forms Ocular muscle weakness less responsiveOcular muscle weakness less responsive
Some children respond to DAPSome children respond to DAP
Congenital Myasthenic Congenital Myasthenic Syndrome with Episodic Apnea Syndrome with Episodic Apnea (Familial Infantile Myasthenia)(Familial Infantile Myasthenia)
Clinical FeaturesClinical Features
Similar problems in other siblings Similar problems in other siblings generalized hypotonic at birth +/- arthrogryposisgeneralized hypotonic at birth +/- arthrogryposis respiratory insufficiency and feeding difficulty at birthrespiratory insufficiency and feeding difficulty at birth repeated episodes of life-threatening apnea and repeated episodes of life-threatening apnea and
feeding difficulty neonatallyfeeding difficulty neonatally may require ventilationmay require ventilation usually improves within weeks of birth, allowing usually improves within weeks of birth, allowing
weaning from ventilationweaning from ventilation episodes may persist throughout infancy and even episodes may persist throughout infancy and even
into adulthoodinto adulthood sudden bouts of respiratory distress with sudden bouts of respiratory distress with
intercurrent illnessintercurrent illness ocular function usually normalocular function usually normal
Congenital Myasthenic Congenital Myasthenic Syndrome with Episodic Apnea Syndrome with Episodic Apnea (Familial Infantile Myasthenia)(Familial Infantile Myasthenia) DiagnosisDiagnosis edrophonium test - 0.15mg/kgedrophonium test - 0.15mg/kg decremental RNSdecremental RNS
TreatmentTreatment ChE inhibitors improve strength in most children ChE inhibitors improve strength in most children
- long term to prevent episodes of apnea at time - long term to prevent episodes of apnea at time of intercurrent illnessof intercurrent illness
DAP + pyridostigmine works for children from DAP + pyridostigmine works for children from several familiesseveral families
many require mechanical ventilationmany require mechanical ventilation
Slow-Channel Congenital Slow-Channel Congenital Myasthenic SyndromeMyasthenic Syndrome
EpidemiologyEpidemiologyRARERARE
Genetics and Molecular BiologyGenetics and Molecular Biology ADAD Prolonged open time of Ach channelProlonged open time of Ach channel
Clinical FeaturesClinical Features Normal at birthNormal at birth Onset always after infancyOnset always after infancy
onset may be delayed until adult lifeonset may be delayed until adult life can present in 20can present in 20’’ss
begins with weakness of cervical and scapular musclesbegins with weakness of cervical and scapular muscles slowly progressive weakness of arm leg neck facial musclesslowly progressive weakness of arm leg neck facial muscles exercise intoleranceexercise intolerance ophthalmoparesisophthalmoparesis Rare to have ptosis, bulbar dysfunction, leg weaknessRare to have ptosis, bulbar dysfunction, leg weakness atrophy of affected musclesatrophy of affected muscles
Slow-Channel Congenital Slow-Channel Congenital Myasthenic SyndromeMyasthenic Syndrome
CourseCourse
progresses slowlyprogresses slowly many patients do not present until after age 10many patients do not present until after age 10
DiagnosisDiagnosis decremental RNSdecremental RNS repetitive discharges after nerve repetitive discharges after nerve
stimulation (like ChE inhibitor toxicity)stimulation (like ChE inhibitor toxicity) muscle Bx muscle Bx –– type I predominance, group type I predominance, group
atrophy, tubular aggregates, abrnomal atrophy, tubular aggregates, abrnomal end-plate configurationsend-plate configurations
Slow-Channel Congenital Slow-Channel Congenital Myasthenic SyndromeMyasthenic Syndrome
TreatmentTreatment not effectivenot effective
ChE inhibitorsChE inhibitors ThymectomyThymectomy ImmunosuppressionImmunosuppression
May be effectiveMay be effective Quinidine sulfate improves strengthQuinidine sulfate improves strength
Fluoxetine equally effective Fluoxetine equally effective
Fast Channel Myasthenic Fast Channel Myasthenic SyndromesSyndromes
PathophysiologyPathophysiology Ach receptor/channel complex does not Ach receptor/channel complex does not
let in sufficient sodiumlet in sufficient sodium MechanismsMechanisms
Channel open for too short a timeChannel open for too short a time Channel takes long time to open upChannel takes long time to open up Ach does not bind sufficiently long to receptorAch does not bind sufficiently long to receptor Channel requires too much energy to switch Channel requires too much energy to switch
from inactive to active statefrom inactive to active stateTreatmentTreatment Responds well to 3,4 DAP and Responds well to 3,4 DAP and
anticholinesterases.anticholinesterases. Ephedrine may help Ephedrine may help
LEMSLEMS EpidemiologyEpidemiology
usually after 40usually after 40’’ss has been reported in childrenhas been reported in children M=FM=F 50% have underlying malignancy (80% of these SCLC)50% have underlying malignancy (80% of these SCLC)
ImmunopathologyImmunopathology antibodies to VGCCsantibodies to VGCCs disorganization of motor nerve terminal active zone disorganization of motor nerve terminal active zone
particlesparticles SCLC cells contained high concentrations of VGCCs and SCLC cells contained high concentrations of VGCCs and
SCLC VGCC are inhibited by LEMS seraSCLC VGCC are inhibited by LEMS seraClinical FeaturesClinical FeaturesWeaknessWeakness proximal muscles, especially legsproximal muscles, especially legs oropharyngeal and ocular relatively spared (although can be oropharyngeal and ocular relatively spared (although can be
affected)affected) objective weakness mild compared to severity of symptomsobjective weakness mild compared to severity of symptoms weakness improves briefly after exercise, then returns with weakness improves briefly after exercise, then returns with
sustained activitysustained activity absent DTR which are enhanced by repeated muscle contraction absent DTR which are enhanced by repeated muscle contraction
or repeated tapping of tendonor repeated tapping of tendon can present as prolonged paralysis following use of can present as prolonged paralysis following use of
neuromuscular blocking agents in surgeryneuromuscular blocking agents in surgery
Clinical FeaturesClinical FeaturesAutonomic FeaturesAutonomic Features
dry mouth commondry mouth common impotenceimpotence postural hypotensionpostural hypotension
Temperature DependenceTemperature Dependence worse in heatworse in heat avoid hot showers or bathsavoid hot showers or baths
DiagnosisDiagnosis edrophonium not as effective as seen in MGedrophonium not as effective as seen in MG EMG/NCs EMG/NCs –– most sensitive in distal muscles most sensitive in distal muscles Neoplastic WorkupNeoplastic Workup bronchoscopybronchoscopy PET scanPET scan
LEMSLEMS
NCSNCSCMAP amplitudes lowCMAP amplitudes low
Repetitive Nerve Stimulation and Exercise TestingRepetitive Nerve Stimulation and Exercise Testing
>10% decrement in CMAP amplitude on slow repetitive >10% decrement in CMAP amplitude on slow repetitive nerve stimulation (3Hz) between 1st and 4th potentialnerve stimulation (3Hz) between 1st and 4th potential
>40% (often >100%) increase in distal CMAP amplitude >40% (often >100%) increase in distal CMAP amplitude after 10 seconds of maximal voluntary exercise. after 10 seconds of maximal voluntary exercise.
>40% (often>100%) increase in distal CMAP amplitude >40% (often>100%) increase in distal CMAP amplitude after high frequency (30-50Hz) repetitive nerve after high frequency (30-50Hz) repetitive nerve stimulationstimulation
EMGEMG generally normalgenerally normal motor unit action potentials may be unstable; motor unit action potentials may be unstable;
may be short, small, or polyphasic (i.e. may be short, small, or polyphasic (i.e. myopathic); may have normal or early myopathic); may have normal or early recruitmentrecruitment
SFEMGSFEMG increased jitter and blockingincreased jitter and blocking
LEMSLEMS
TreatmentTreatment
ChE InhibitorsChE Inhibitors may work in occasional patientsmay work in occasional patients pyridostigmine 30-60mg q6h x several dayspyridostigmine 30-60mg q6h x several days major benefit is relief of dry mouthmajor benefit is relief of dry mouth
Guanidine HydrochlorideGuanidine Hydrochloride increases release of Achincreases release of Ach add on agent to mestinonadd on agent to mestinon temporary improvement in strength in many patients with temporary improvement in strength in many patients with
LEMSLEMS start 5-10mg/kg/d div 4-6h apartstart 5-10mg/kg/d div 4-6h apart increase to maximum of 30mg/kg/d q3d increase to maximum of 30mg/kg/d q3d
SFXSFXBM suppression ,RTA ,Chronic interstitial nephritis ,Cardiac BM suppression ,RTA ,Chronic interstitial nephritis ,Cardiac
arrhythmia ,Hepatic toxicity ,Pancreatic arrhythmia ,Hepatic toxicity ,Pancreatic dysfunction ,Paresthesiae ,Ataxia .Confusion ,Mood changesdysfunction ,Paresthesiae ,Ataxia .Confusion ,Mood changes
LEMSLEMS
TreatmentTreatmentDAPDAP 5-25mg tid-qid5-25mg tid-qid facilitates release of Ach from motor nerve terminalsfacilitates release of Ach from motor nerve terminals synergistic with pyridostigminesynergistic with pyridostigmine
PLEX and IVIGPLEX and IVIG can provide transitory improvementcan provide transitory improvement((Immunosupression ,prednisone,azathioprine ,cyclosporine)Immunosupression ,prednisone,azathioprine ,cyclosporine) not as good as in MGnot as good as in MG
Severe WeaknessSevere Weakness PLEX/IVIG 1stPLEX/IVIG 1st Prednisone and imuran added after improvement beginsPrednisone and imuran added after improvement begins
Prognosis Prognosis variablevariable
LEMSLEMS

BotulismBotulism
PathophysiologyPathophysiology botulinum toxin block release of Ach from motor botulinum toxin block release of Ach from motor
nerve terminalnerve terminal 8 types of toxin8 types of toxin
types A and B cause most occurrences of botulism types A and B cause most occurrences of botulism in USin US
type E transmitted in seafoodtype E transmitted in seafood
Clinical FeaturesClinical Features CourseCourse
NxVx 1st Sx of food-borne botulismNxVx 1st Sx of food-borne botulism Neuromuscular Sx begin 12-36h after exposureNeuromuscular Sx begin 12-36h after exposure
Ocular : blurred vision and impaired pupillary Ocular : blurred vision and impaired pupillary reflexesreflexes
Motor : weakness and decreased DTRsMotor : weakness and decreased DTRs Autonomic : dry mouth ,constipation ,urinaryAutonomic : dry mouth ,constipation ,urinary
retentionretention
BotulismBotulism DiagnosisDiagnosis
Tensilon TestTensilon Test positive in 1/3 of patientspositive in 1/3 of patients do not distinguish botulism from other causesdo not distinguish botulism from other causes
MicrobiologicalMicrobiological Botulinium toxin in stoolBotulinium toxin in stool C. Botulinium culture from stoolC. Botulinium culture from stool Wound cultures and serum for Botulinium toxinWound cultures and serum for Botulinium toxin
EMG/NCSEMG/NCS1.1. reduced CMAP in at least 2 musclesreduced CMAP in at least 2 muscles2.2. at least 20% facilitation of CMAP amplitude during titanic at least 20% facilitation of CMAP amplitude during titanic
stimulationstimulation3.3. persistence of facilitation at least 2 minutes after activationpersistence of facilitation at least 2 minutes after activation4.4. no postactivation exhaustionno postactivation exhaustion
SFEMGSFEMG Jitter and blockingJitter and blocking Sensitivity 100% ,Poor specificitySensitivity 100% ,Poor specificity
BotulismBotulism
TreatmentTreatment bivalent (type A, B) or trivalent (A, B, E) antitoxinbivalent (type A, B) or trivalent (A, B, E) antitoxin antibiotics NOT effectiveantibiotics NOT effective supportive therapysupportive therapy ChE inhibitors NOT beneficialChE inhibitors NOT beneficial DAP improves strength but not respiratory DAP improves strength but not respiratory
functionfunction
PrognosisPrognosis Most patients make complete recovery within 2-3 Most patients make complete recovery within 2-3
monthsmonths If sever einvolvement, may not return to normal for a If sever einvolvement, may not return to normal for a
yearyear
VenomsVenomsClinical FeaturesClinical Features progressive, symmetrical muscle weaknessprogressive, symmetrical muscle weakness
oculomotor/eyelids most oftenoculomotor/eyelids most often neck flexion, and pelvic and pectoral girdles nextneck flexion, and pelvic and pectoral girdles next bulbar or respiratory if severebulbar or respiratory if severe
cognition and sensation preservedcognition and sensation preserved DTR preserved, or minimally diminishedDTR preserved, or minimally diminished
MechanismsMechanisms initial augmentation of Ach release with subsequent depletioninitial augmentation of Ach release with subsequent depletion facilitation of Ach release without subsequent depletion of facilitation of Ach release without subsequent depletion of
neurotransmitterneurotransmitter depletion of Ach releasedepletion of Ach release blockade of post junctional Ach receptorblockade of post junctional Ach receptor
Specific VenomsSpecific VenomsFunnel Web and Black Widow Spiders (latrodectism)Funnel Web and Black Widow Spiders (latrodectism)facilitation of neurotransmitter release by depolarization of facilitation of neurotransmitter release by depolarization of
presynaptic terminalpresynaptic terminal
VenomsVenomsTick ParalysisTick Paralysis
MicrobiologyMicrobiology dermacentor andersoni ,dermacentor variabilisdermacentor andersoni ,dermacentor variabilis
Clincial FeaturesClincial Features usually children <5yousually children <5yo similar to GBSsimilar to GBS ocular motor palsies and papillary abnormalities ocular motor palsies and papillary abnormalities <<GBSGBS
MechanismMechanismpostsynaptic blockade of neurotoxinpostsynaptic blockade of neurotoxin
DiagnosisDiagnosis CSF protein normalCSF protein normal NCS normal or mild slowing of NCVNCS normal or mild slowing of NCV decreased CMAPdecreased CMAP high frequency RNS may be normal or abnormal incremental high frequency RNS may be normal or abnormal incremental
responseresponse
TreatmentTreatment remove tick usually lead to rapid recoveryremove tick usually lead to rapid recovery Australian variant may have continued worsening for another 1-2 daysAustralian variant may have continued worsening for another 1-2 days
Other Neurotoxins Other Neurotoxins Affecting The NMJAffecting The NMJ
Marine neurotoxinsMarine neurotoxins are rare and come primarily from poisonous fish (stonustoxin), a are rare and come primarily from poisonous fish (stonustoxin), a
few mollusks (conotoxins), and dinoflagellates. few mollusks (conotoxins), and dinoflagellates.
Heavy metal intoxicationHeavy metal intoxication is a rare cause of neuromuscular toxicity. is a rare cause of neuromuscular toxicity. Ingestion of contaminated grain used for flour in bread. Ingestion of contaminated grain used for flour in bread.
produced weakness with characteristic decremental responses produced weakness with characteristic decremental responses partial reversal with ChE inhibitors.partial reversal with ChE inhibitors.
OrganophosphatesOrganophosphates impair neuromuscular transmission by irreversibly impair neuromuscular transmission by irreversibly
inhibiting acetylcholinesterase.inhibiting acetylcholinesterase. producing a depolarizing neuromuscular block.producing a depolarizing neuromuscular block.
Neuromuscular Neuromuscular Junction Junction DisordersDisorders
Related Documents











