NEUROMODULATION IN EPILEPSY Colin Van Hook, M.D., M.P.H. Ochsner Medical Center Department of Neurology International Center for Epilepsy

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

NEUROMODULATION IN EPILEPSY
Colin Van Hook, M.D., M.P.H.
Ochsner Medical Center
Department of Neurology
International Center for Epilepsy
WHAT IS NEUROMODULATION???
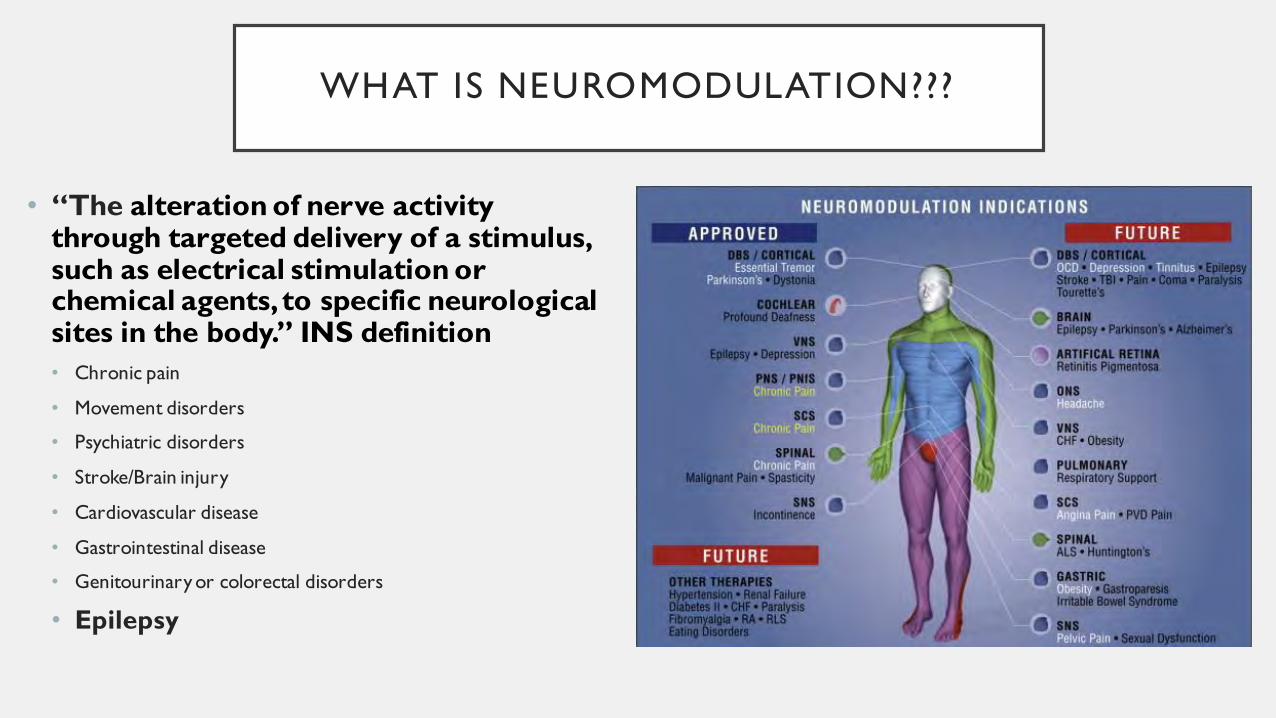
• “The alteration of nerve activity through targeted delivery of a stimulus, such as electrical stimulation or chemical agents, to specific neurological sites in the body.” INS definition
• Chronic pain
• Movement disorders
• Psychiatric disorders
• Stroke/Brain injury
• Cardiovascular disease
• Gastrointestinal disease
• Genitourinary or colorectal disorders
• Epilepsy
NEUROMODULATION IN EPILEPSY: WHEN TO CONSIDER IT
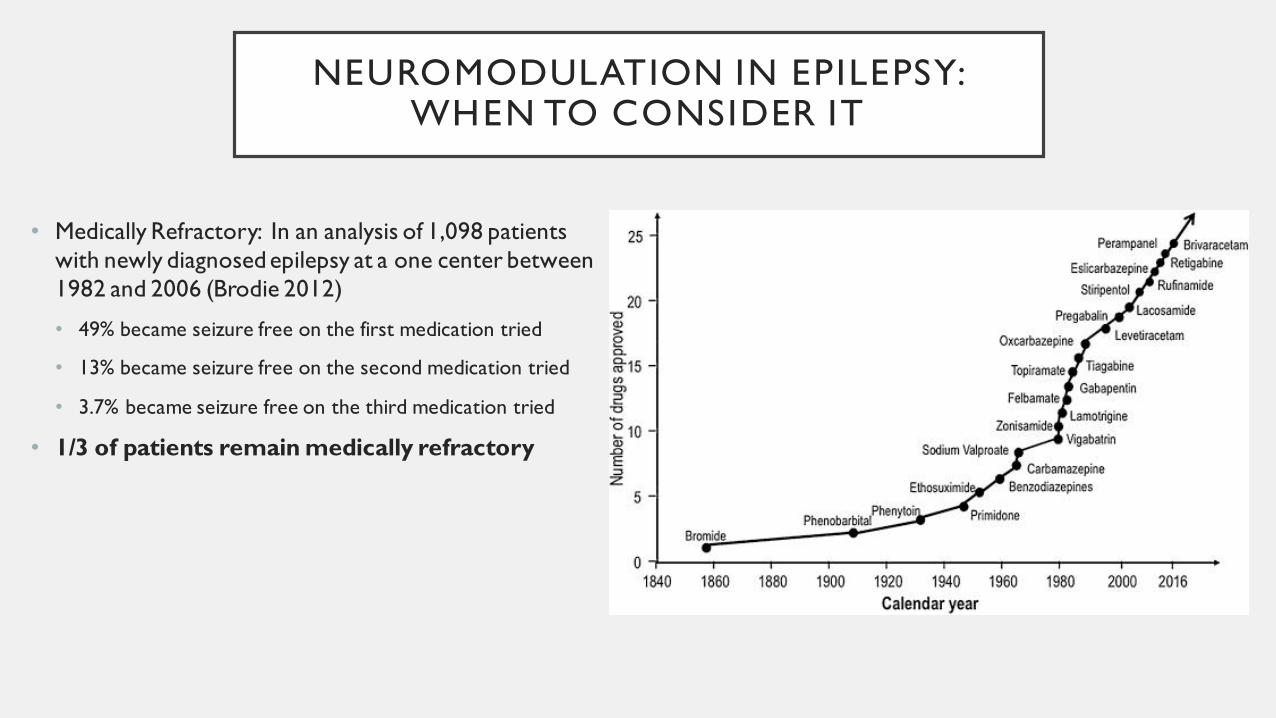
• Medically Refractory: In an analysis of 1,098 patients
with newly diagnosed epilepsy at a one center between
1982 and 2006 (Brodie 2012)
• 49% became seizure free on the first medication tried
• 13% became seizure free on the second medication tried
• 3.7% became seizure free on the third medication tried
• 1/3 of patients remain medically refractory
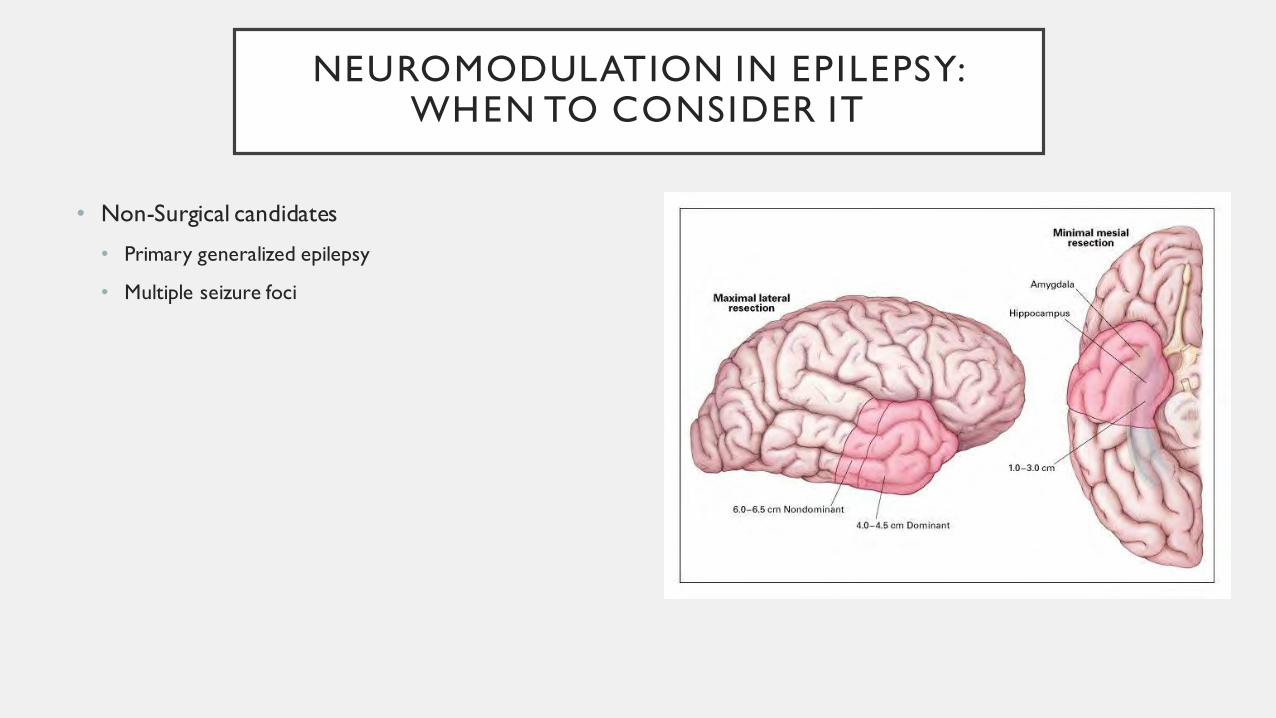
NEUROMODULATION IN EPILEPSY: WHEN TO CONSIDER IT
• Non-Surgical candidates
• Primary generalized epilepsy
• Multiple seizure foci
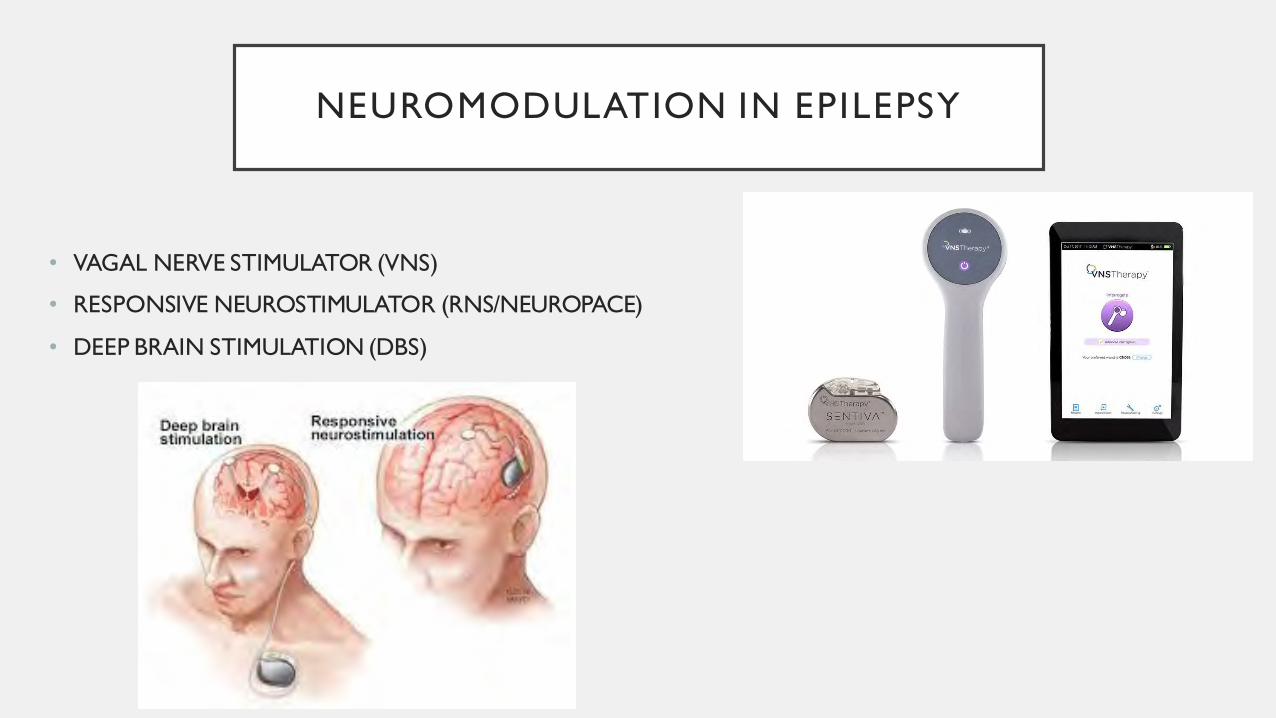
NEUROMODULATION IN EPILEPSY
• VAGAL NERVE STIMULATOR (VNS)
• RESPONSIVE NEUROSTIMULATOR (RNS/NEUROPACE)
• DEEP BRAIN STIMULATION (DBS)

VAGUS NERVE ANATOMY
• CN X (VAGUS NERVE)
• Exits jugular foramen with CN IX and CN XI then travels in the
carotid sheath with the common carotid artery and the internal
jugular vein
• AFFERENT FIBERS = 80%
• Solitary Nucleus and Spinal Trigeminal Nucleus
• EFFERENT FIBERS = 20%
• Originate in Dorsal Motor Nucleus and Nucleus Ambiguus
• Parasympathetic fibers to the viscera
• Right CNX provides significantly more innervation to heart
compared to left (this is why VNS placed usually on left CN X)
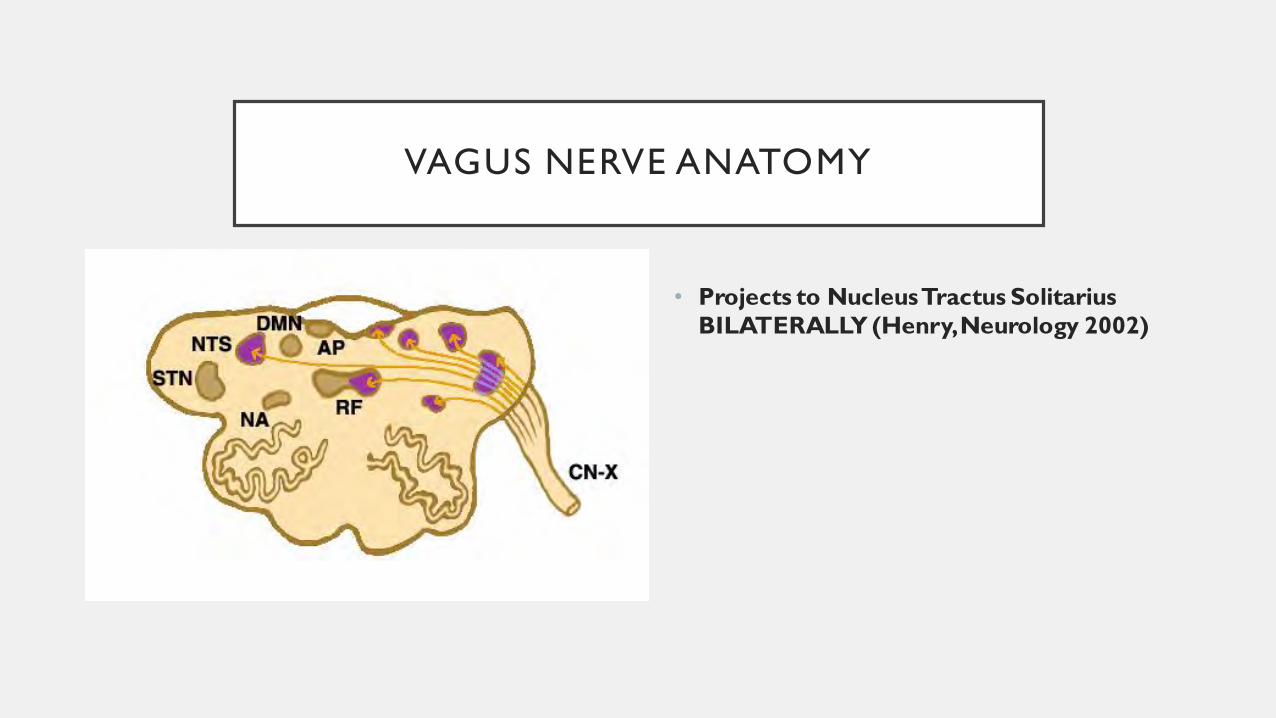
VAGUS NERVE ANATOMY
• Projects to Nucleus Tractus Solitarius
BILATERALLY (Henry, Neurology 2002)

VAGUS NERVE PROJECTIONS
• Vagus nerve works through Nucleus Tractus Solitarus(NTS)
and Pontine Parabrahcial Nucleus (PBN)
• Limbic
• Amygdala: implicated in temporal lobe epilepsy
• Insula: connections to orbitofrontal cortex
• Autonomic
• Connections to hypothalamus and periaqueductal gray (PAG)
• Reticular structures
• Thalamus
Henry 2002.
VAGUS NERVE AND SEIZURES
• 1938 (Bailey and Bremer)
• Stimulation of vagus nerve produced EEG changes in cats
• 1952 (Zanchetti)
• Intermittent vagal nerve stimulation decreased or eliminated chemically induced focal epileptiform discharges
• 1960s
• Repetitive stimulation of vagus nerve led to synchronize or desynchronize cortical electrical activity
• Seizures caused by hypersynchronized cortical activity thus VNS could desynchronize
• 1985 (Zabara)
• Hypothesized that VNS antagonizes hypersynchronous states using animal studies
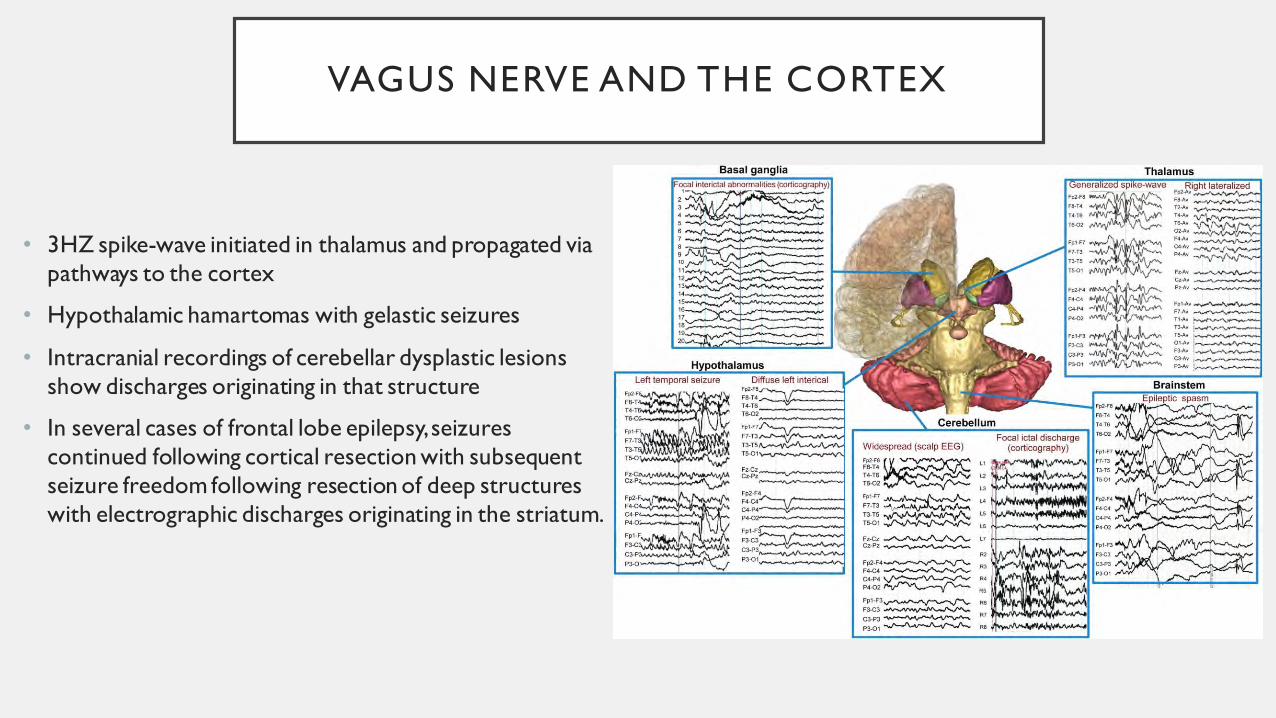
VAGUS NERVE AND THE CORTEX
• 3HZ spike-wave initiated in thalamus and propagated via
pathways to the cortex
• Hypothalamic hamartomas with gelastic seizures
• Intracranial recordings of cerebellar dysplastic lesions
show discharges originating in that structure
• In several cases of frontal lobe epilepsy, seizures
continued following cortical resection with subsequent
seizure freedom following resection of deep structures
with electrographic discharges originating in the striatum.
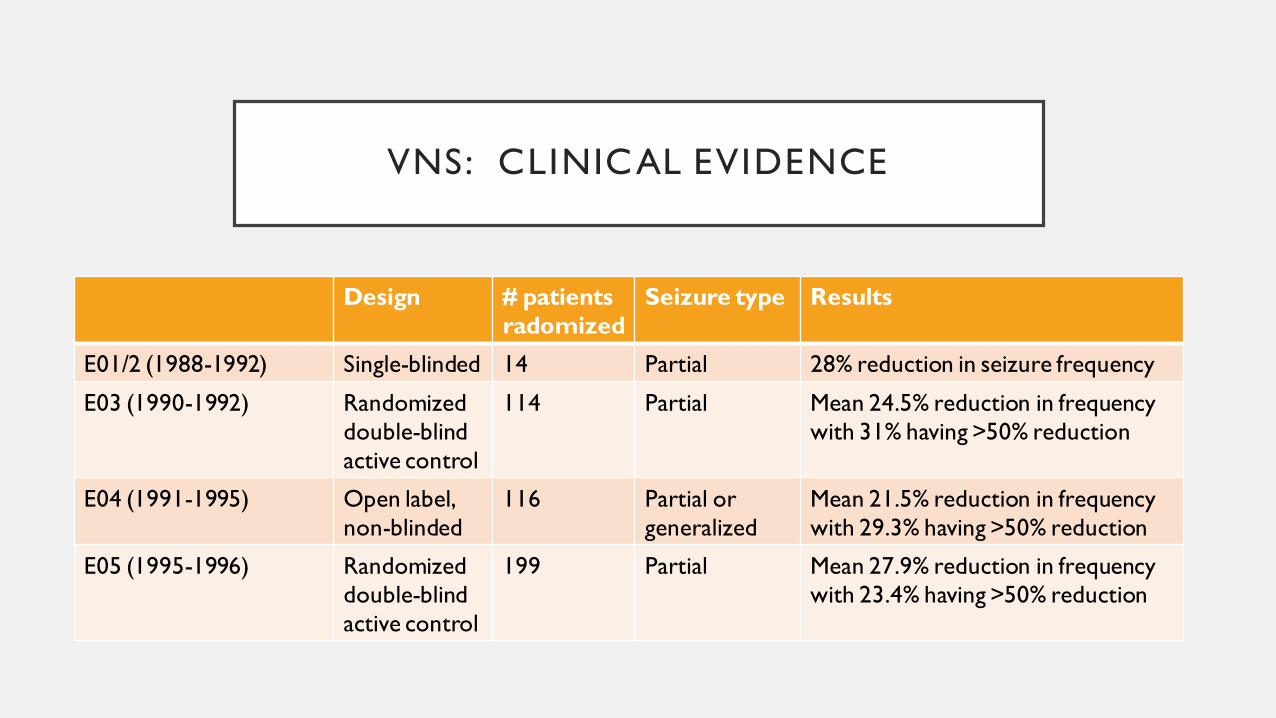
VNS: CLINICAL EVIDENCE
Design # patients
radomized
Seizure type Results
E01/2 (1988-1992) Single-blinded 14 Partial 28% reduction in seizure frequency
E03 (1990-1992) Randomized
double-blind
active control
114 Partial Mean 24.5% reduction in frequency
with 31% having >50% reduction
E04 (1991-1995) Open label,
non-blinded
116 Partial or
generalized
Mean 21.5% reduction in frequency
with 29.3% having >50% reduction
E05 (1995-1996) Randomized
double-blind
active control
199 Partial Mean 27.9% reduction in frequency
with 23.4% having >50% reduction
VNS CLINICAL EVIDENCE
• Reduction of seizure frequency > 50% (Morris and Mueller, Neurology 1999)
• 1 year = 36.8% patients
• 2 years = 43.2% patients
• 3 years = 42.7% patients
• Well tolerated
• 75% patients continued therapy
• There is a persistent VNS‐induced anticonvulsant effect and indicate that its
efficacy is dependent on the cumulative stimulus duration (Takaya, Epilepsia 1996).
VNS APPROVAL
• In 1997, the FDA approved the VNS Therapy System for use as an adjunctive therapy in
reducing the frequency of seizures in adults and adolescents over 12 years of age with
partial onset seizures refractory to antiepileptic medications
• In 2017, device was FDA approved for children as young as 4 due after data from Japan
Post‐Approval Study (PAS) in which followed patients implanted between 2010 and
2012.
• As of 2017, >100,000 patients treated with VNS
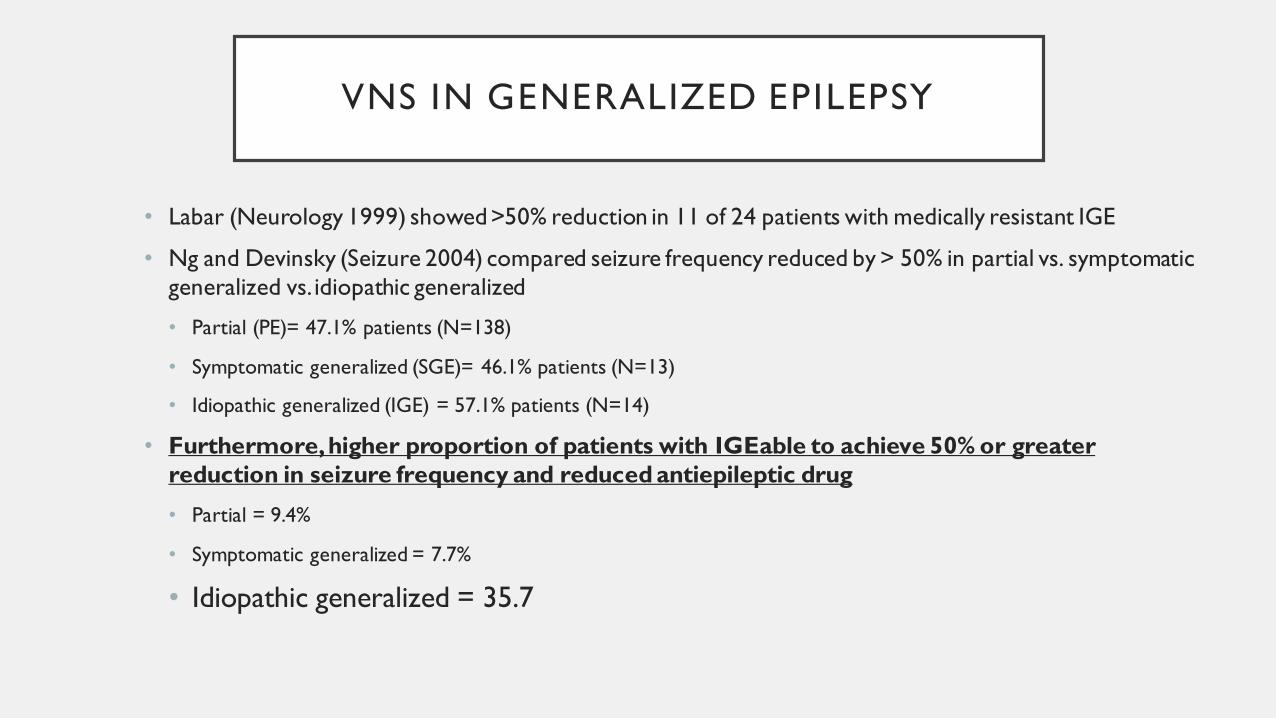
VNS IN GENERALIZED EPILEPSY
• Labar (Neurology 1999) showed >50% reduction in 11 of 24 patients with medically resistant IGE
• Ng and Devinsky (Seizure 2004) compared seizure frequency reduced by > 50% in partial vs. symptomatic
generalized vs. idiopathic generalized
• Partial (PE)= 47.1% patients (N=138)
• Symptomatic generalized (SGE)= 46.1% patients (N=13)
• Idiopathic generalized (IGE) = 57.1% patients (N=14)
• Furthermore, higher proportion of patients with IGEable to achieve 50% or greater
reduction in seizure frequency and reduced antiepileptic drug
• Partial = 9.4%
• Symptomatic generalized = 7.7%
• Idiopathic generalized = 35.7
VNS AND DEPRESSION
• Reduction in depression scores was noted in E03/5 and two subsequent studies (Harden 2000 and
Elger 2000) showed trend to depression reduction was INDEPENDENT of seizure reduction
• One year trial of VNS for patients with depression (n=185) or bipolar I/II (n=20) refractory to at
least 2 medications showed a significant reduction in symptoms on the 24 item Hamilton Rating
Scale for Depression. (Rush 2005)
• Five year open-label, non-randomized trial of patients with treatment resistant depression showed
reduction in Montgomery-Åsberg Depression Rating Scale (MADRS) in patients with VNS (n=494)
versus treatment as usual (n=301). (Aaronson 2017)
• In 2005 FDA approved VNS for adjunct treatment in depression but coverage denied by US
Committee on Medicare and Medicaid Services

VNS AND QUALITY OF LIFE
• PuLsE (Open Prospective Randomized Long-term Effectiveness) trial showed
significant improvement in Quality of Life in Epilepsy Inventory-89 total score
(QOLIE-89) in 61 patients with VNS versus 61 patient with medical therapy only
(Ryvlin 2017)
• VNS patients with autism showed improved alertness, verbal communication,
memory, and school performance (Levy 2010)
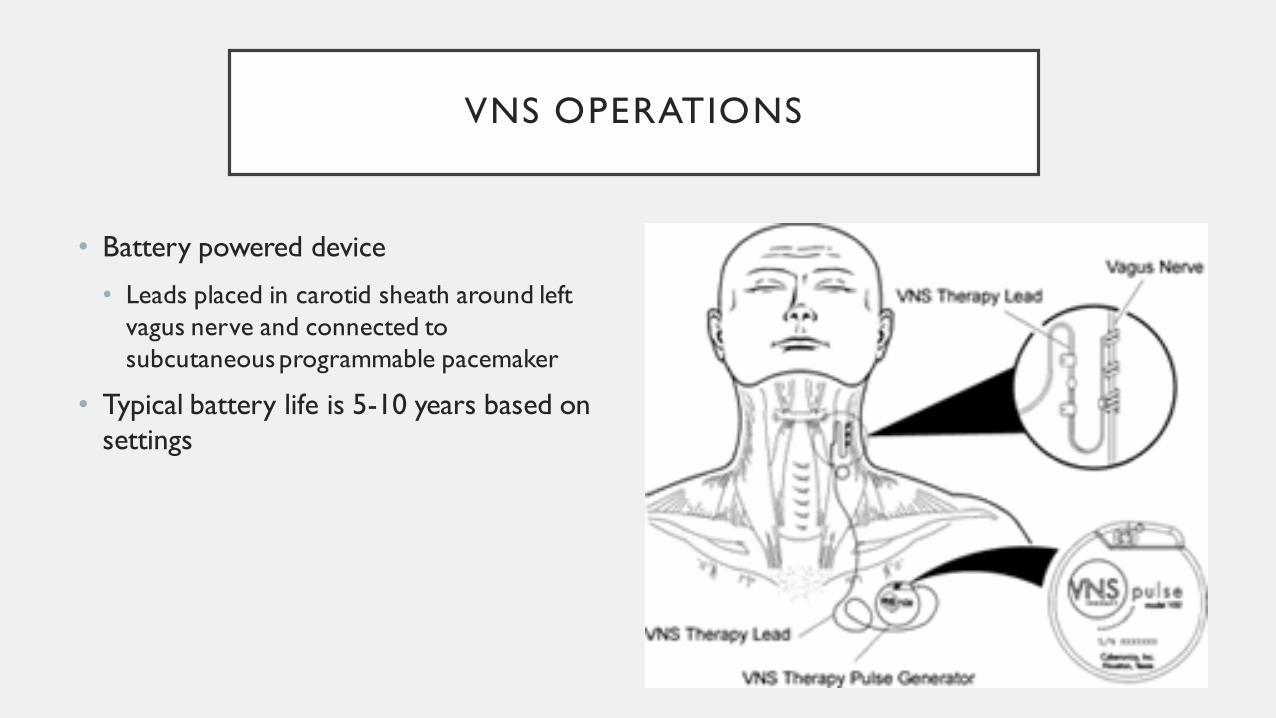
VNS OPERATIONS
• Battery powered device
• Leads placed in carotid sheath around left
vagus nerve and connected to
subcutaneous programmable pacemaker
• Typical battery life is 5-10 years based on
settings
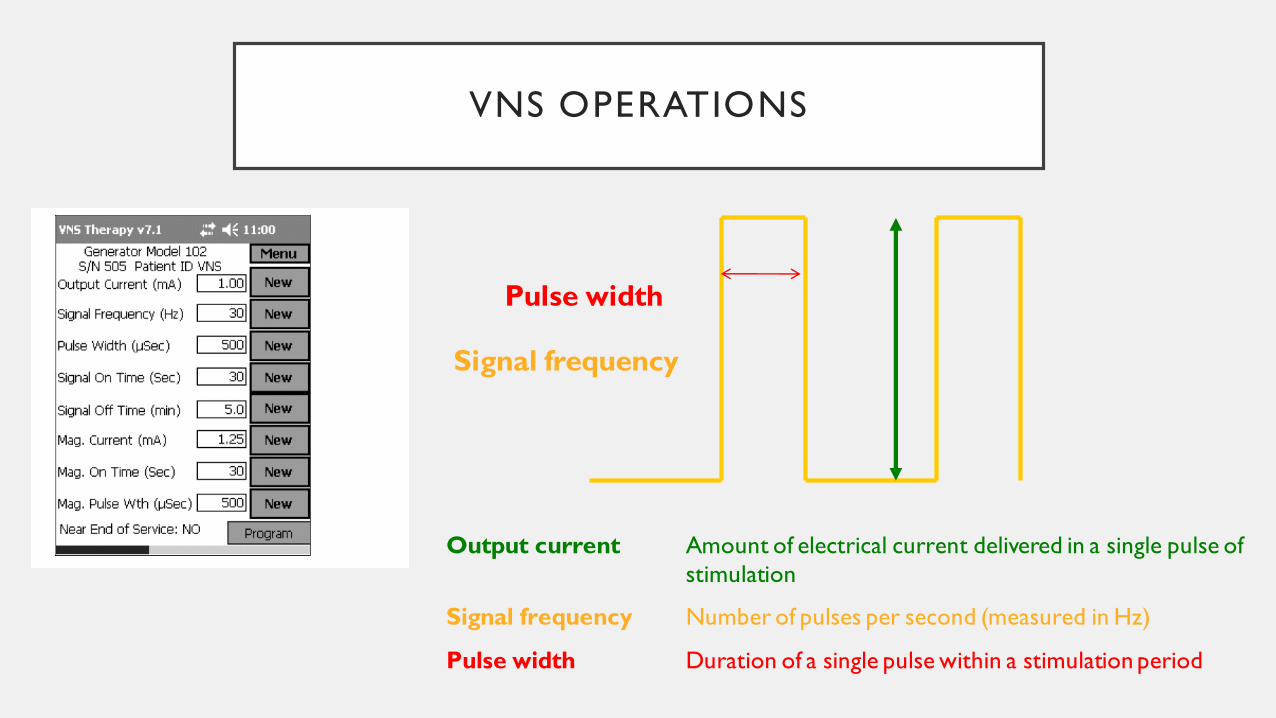
VNS OPERATIONS
Pulse width
Signal frequency
Output current Amount of electrical current delivered in a single pulse of
stimulation
Signal frequency Number of pulses per second (measured in Hz)
Pulse width Duration of a single pulse within a stimulation period
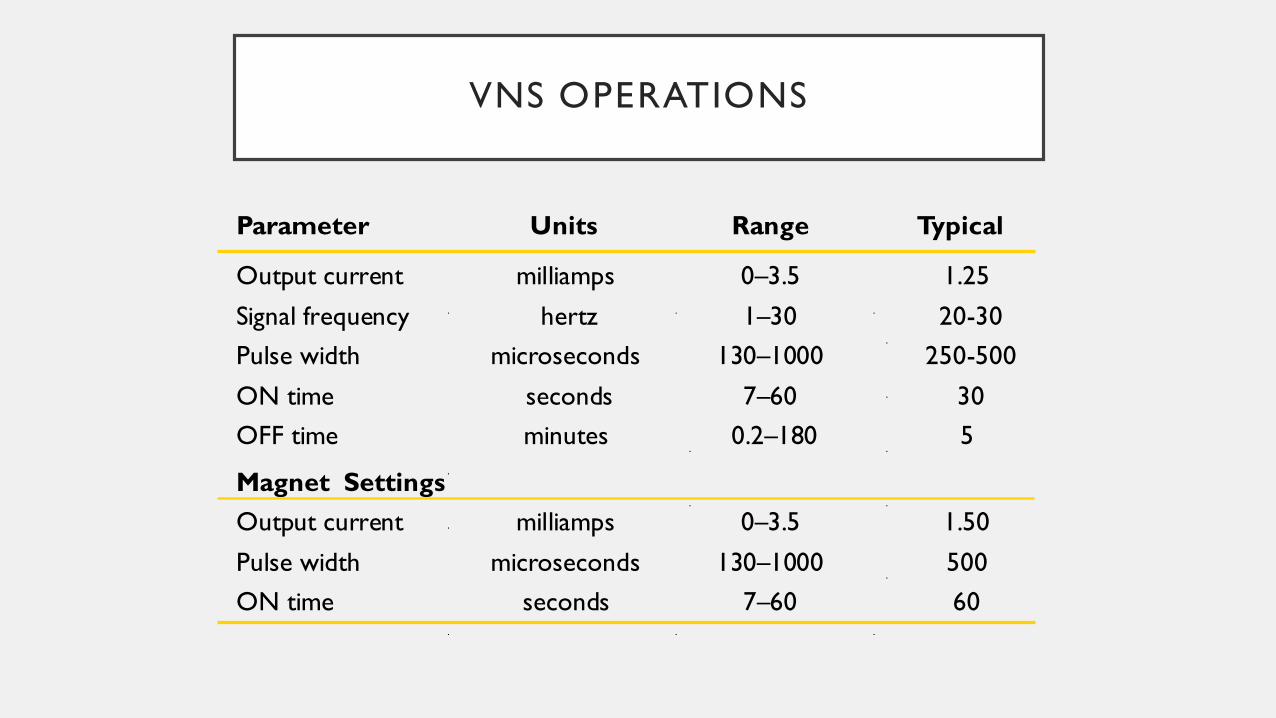
VNS OPERATIONS
Parameter Units Range Typical
Output current milliamps 0–3.5 1.25
Signal frequency hertz 1–30 20-30
Pulse width microseconds 130–1000 250-500
ON time seconds 7–60 30
OFF time minutes 0.2–180 5
Magnet Settings
Output current milliamps 0–3.5 1.50
Pulse width microseconds 130–1000 500
ON time seconds 7–60 60

VNS OPERATIONS: CYCLING AND DUTY CYCLE
• Initial settings typically:
• Output current 0.25mA
• Signal frequency 30Hz
• Pulse Width 250-500 microseconds
• “On” 30 seconds
• “Off” 5 minutes
• Several small studies do not support increased efficacy for “Rapid Cycling” typically connotating 7 seconds “on” and 30 seconds “off”
• Not recommended as this will wear down battery faster
• Duty cycle should be <50%
ON time + 4 seconds
ON time + OFF time

VNS MAGNET
• Patient or other swipes magnet on generator for 1 second
which gives additional current/stimulation to stop or
shorten seizure
• Morris. Epilepsy and Behavior 2003.
• Patients in E03 trial with active magnets were more likely to
report improved seizure control than patients with inactive
magnets
• In the E04 trial, 22% of patients using the magnet reported
seizure termination and 31% reported seizure diminution
• Magnet output current should always be higher (usually
0.25mA higher) than parameter output

VNS SAFETY
• Side Effects
• Data from E0S trials
• Voice alteration/hoarseness 66.3 %
• Cough 45.3%
• Pharyngitis 34.7%
• Dyspnea 24.2%
• Most resolved after 1-2 years of continued treatment
• Mild increase in hypopnea and apnea in patients with OSA, may unmask latent OSA
(Marzed, Edwards, Sagher. Epilepsia 2003)
VNS: MANAGING SIDE EFFECTS
• Reduce pulse width from 500 to 250
• Reduce frequency from 30 to 20
• TAPE MAGNET OVER DEVICE TO AVOID VOICE CHANGE
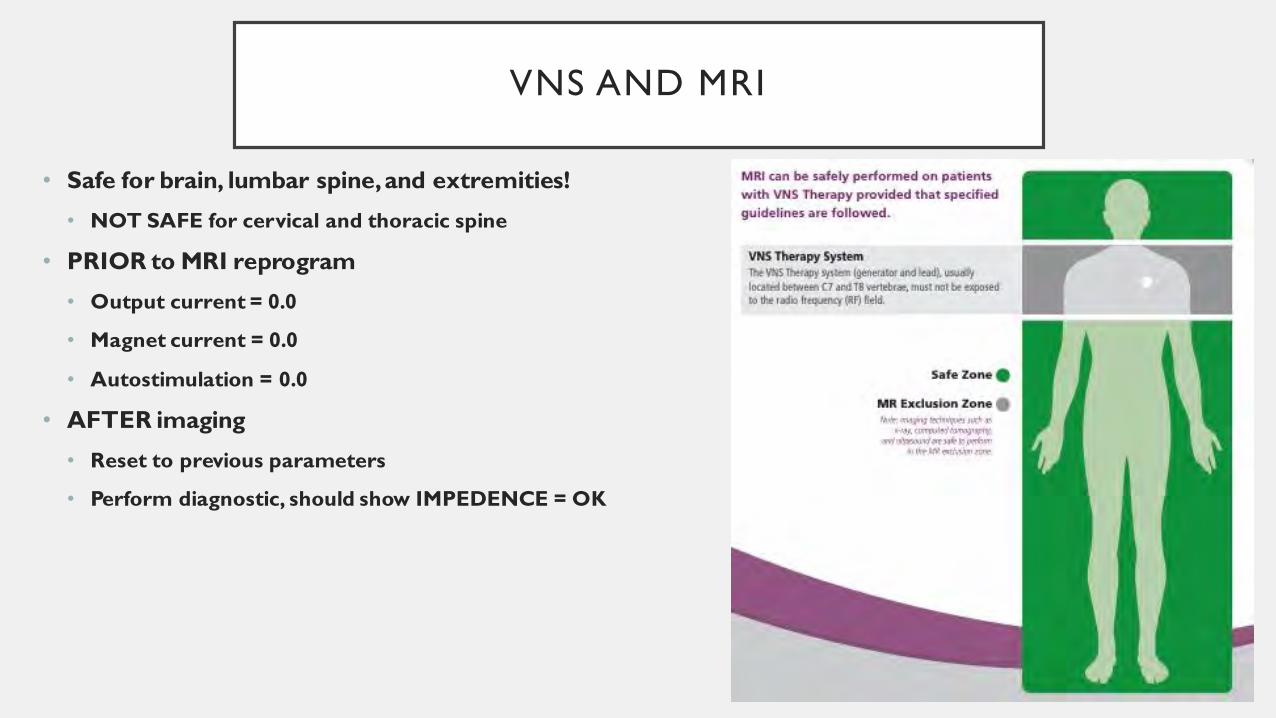
VNS AND MRI
• Safe for brain, lumbar spine, and extremities!
• NOT SAFE for cervical and thoracic spine
• PRIOR to MRI reprogram
• Output current = 0.0
• Magnet current = 0.0
• Autostimulation = 0.0
• AFTER imaging
• Reset to previous parameters
• Perform diagnostic, should show IMPEDENCE = OK
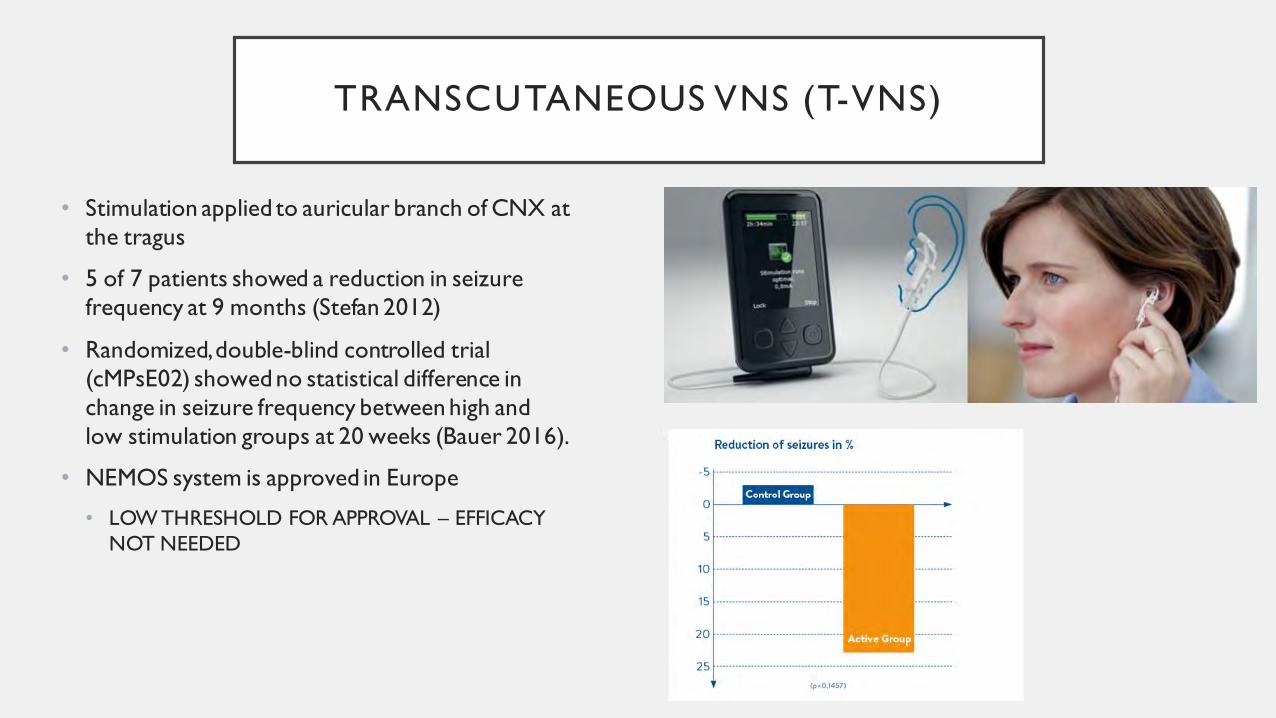
TRANSCUTANEOUS VNS (T-VNS)
• Stimulation applied to auricular branch of CNX at
the tragus
• 5 of 7 patients showed a reduction in seizure
frequency at 9 months (Stefan 2012)
• Randomized, double-blind controlled trial
(cMPsE02) showed no statistical difference in
change in seizure frequency between high and
low stimulation groups at 20 weeks (Bauer 2016).
• NEMOS system is approved in Europe
• LOW THRESHOLD FOR APPROVAL – EFFICACY
NOT NEEDED
PRO
• Option for anyone who is not a candidate for resection
• No cognitive side effects
• Compliance is not an issue
• Improved quality of life
• More alertness
• Less daytime sleepiness
• Improved memory
• Improved mood
• Provides patient/family with sense of control
• Safe in pregnancy
• Surgery required
• Battery replacement 5-10 years
• Still need AEDs
• Rarely seizure-freedom (5%)
• What are best settings?
CON
VNS: WHO TO CONSIDER?
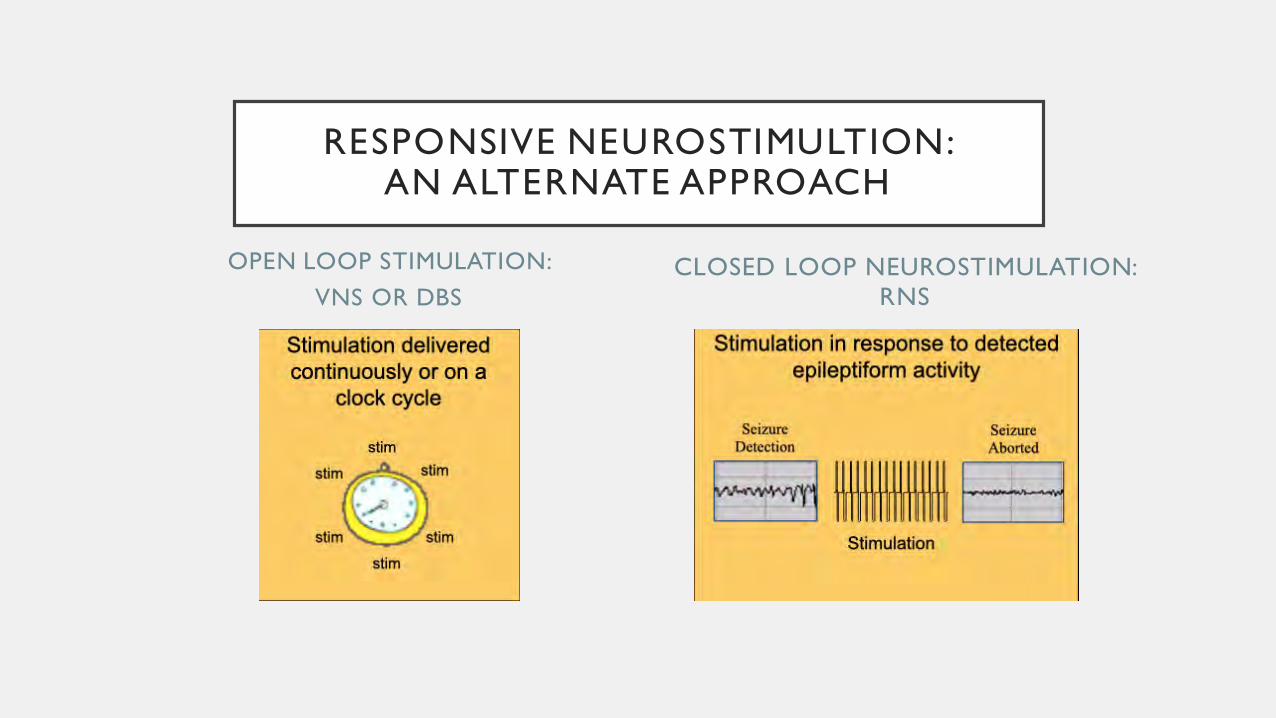
OPEN LOOP STIMULATION:
VNS OR DBS
CLOSED LOOP NEUROSTIMULATION:
RNS
RESPONSIVE NEUROSTIMULTION: AN ALTERNATE APPROACH

CORTICAL STIMULATION
• In the 1950’s Penfield and Jasper noted that cortical
stimulation could disrupt epileptiform activity and lead to
suppression of both normal and epileptiform activity at
distant sites.
• Cooper (1978) noted that closed loop stimulation of the
cerebellum could reduce seizures
• Kinoshita et al (2004, 2005) noted reduction in interictal
spikes in high versus low open-loop stimulation in
patients undergoing intracranial monitoring and
functional mapping.
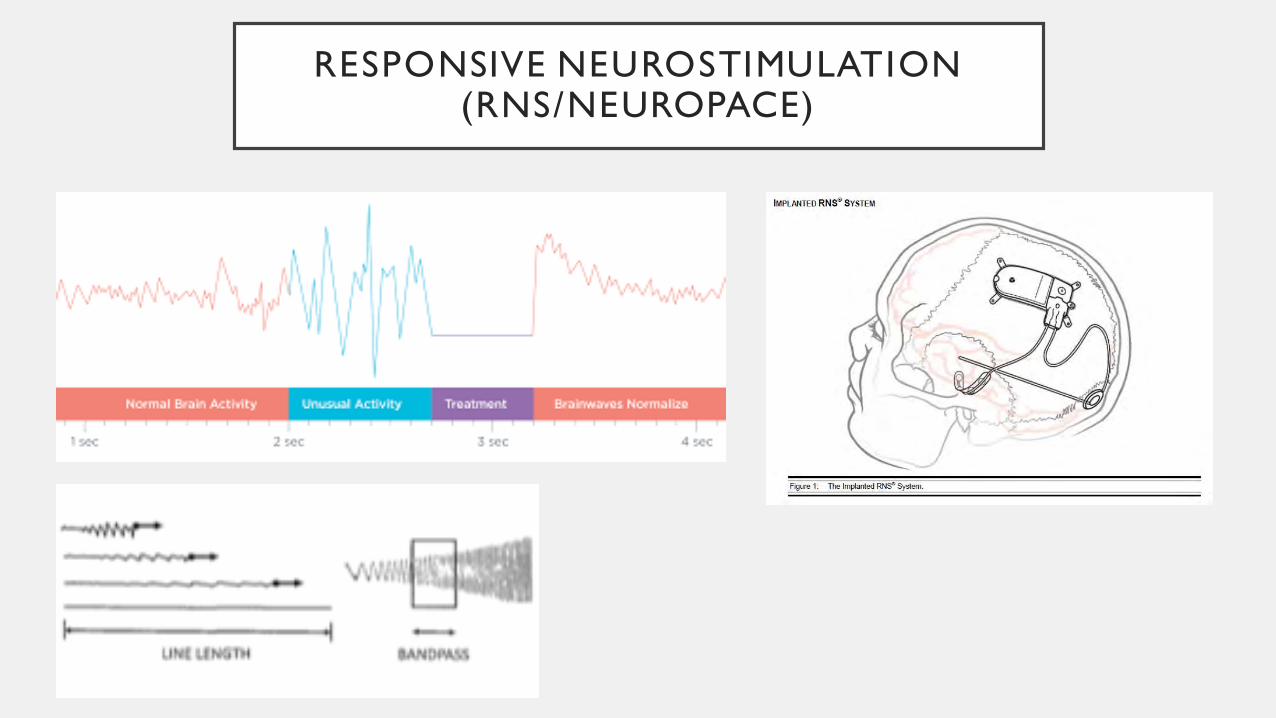
RESPONSIVE NEUROSTIMULATION (RNS/NEUROPACE)

RESPONSIVE NEUROSTIMULATION (RNS/NEUROPACE)
• Allows for significant amounts of electorcortography (ECoG) recording based
on several triggers
• Scheduled storage (up to 4)
• Magnet swipes by the patient
• Long episode: specified duration of time meeting detection parameters
• Saturation: when ECoG amplitude exceeds a designated threshold
RESPONSIVE NEUROSTIMULATION (RNS/NEUROPACE)
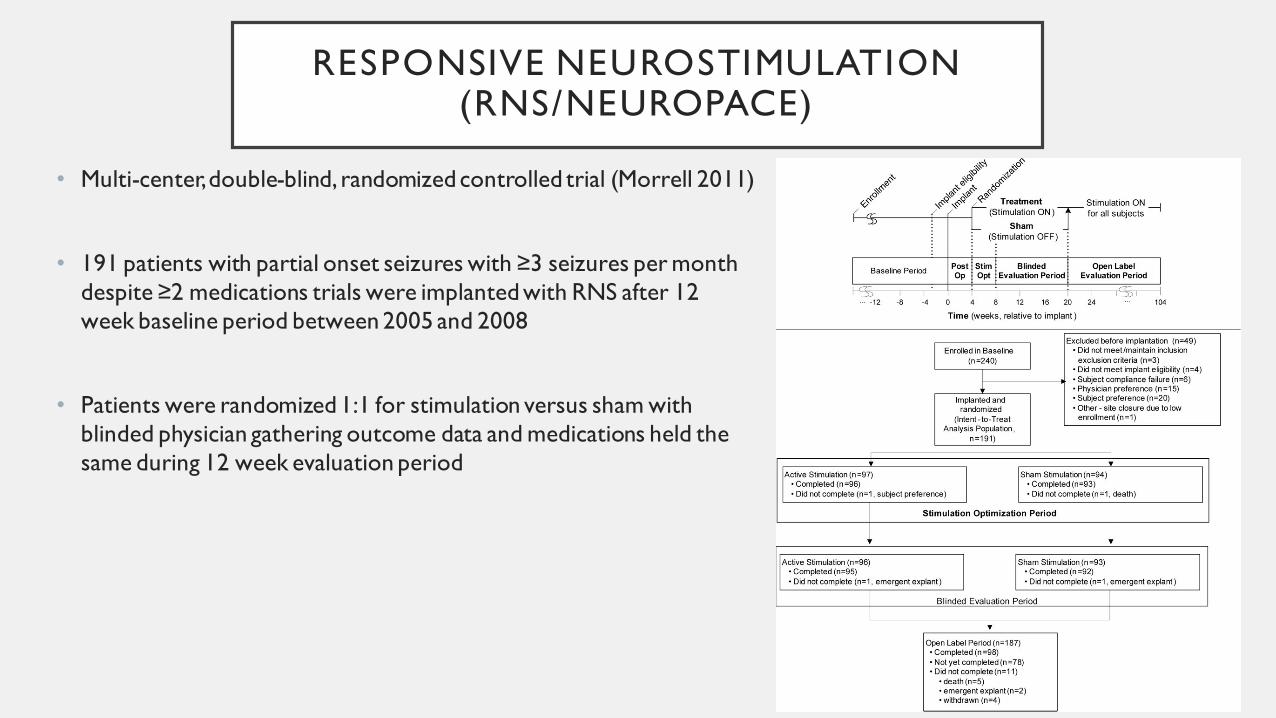
• Multi-center, double-blind, randomized controlled trial (Morrell 2011)
• 191 patients with partial onset seizures with ≥3 seizures per month
despite ≥2 medications trials were implanted with RNS after 12
week baseline period between 2005 and 2008
• Patients were randomized 1:1 for stimulation versus sham with
blinded physician gathering outcome data and medications held the
same during 12 week evaluation period
RESPONSIVE NEUROSTIMULATION (RNS/NEUROPACE)
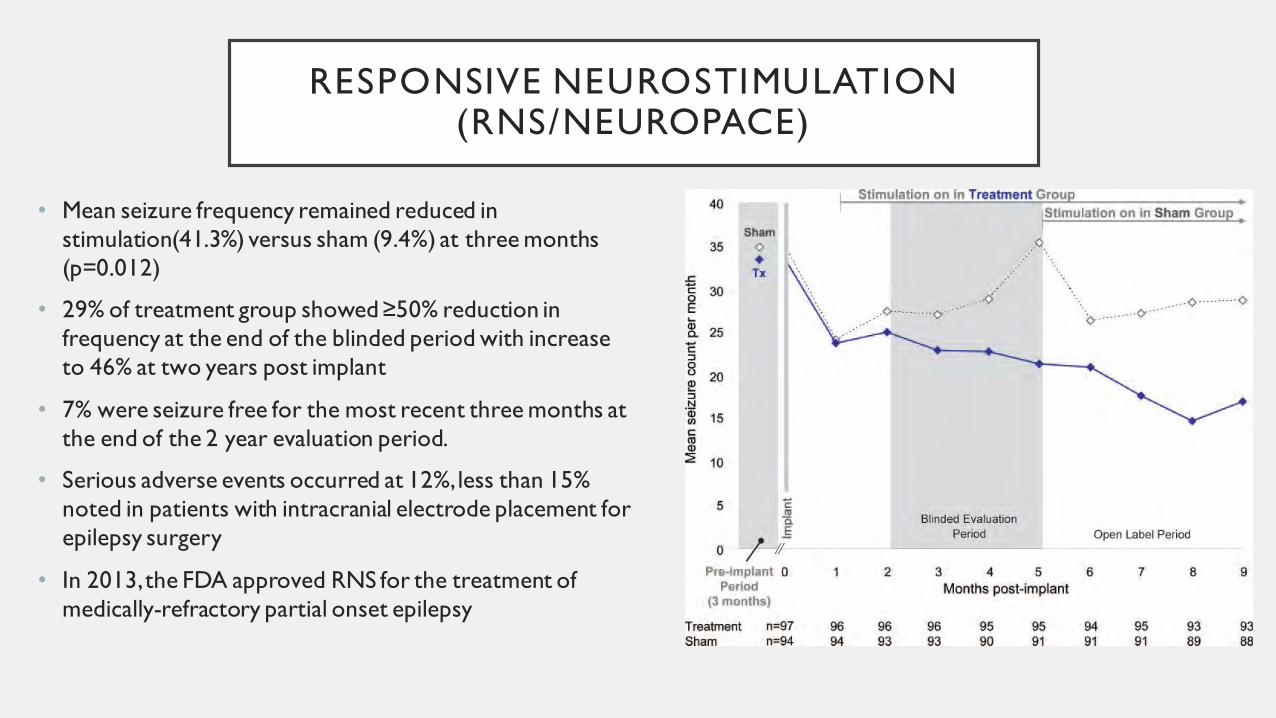
• Mean seizure frequency remained reduced in
stimulation(41.3%) versus sham (9.4%) at three months
(p=0.012)
• 29% of treatment group showed ≥50% reduction in
frequency at the end of the blinded period with increase
to 46% at two years post implant
• 7% were seizure free for the most recent three months at
the end of the 2 year evaluation period.
• Serious adverse events occurred at 12%, less than 15%
noted in patients with intracranial electrode placement for
epilepsy surgery
• In 2013, the FDA approved RNS for the treatment of
medically-refractory partial onset epilepsy
RESPONSIVE NEUROSTIMULATION (RNS/NEUROPACE)
• In an open-label follow, 191 patients were followed for an average of 5.4 years and showed a sustained response rate (≥50% reduction) of >60% at six years post-implant
• Serious adverse events were rare following immediate implantation period.
• Improvement in QUOLIE scores was sustained through year 4 on follow up (p=0.001)
IMPLICATIONS OF LONG TERM RECORDING IN RNS
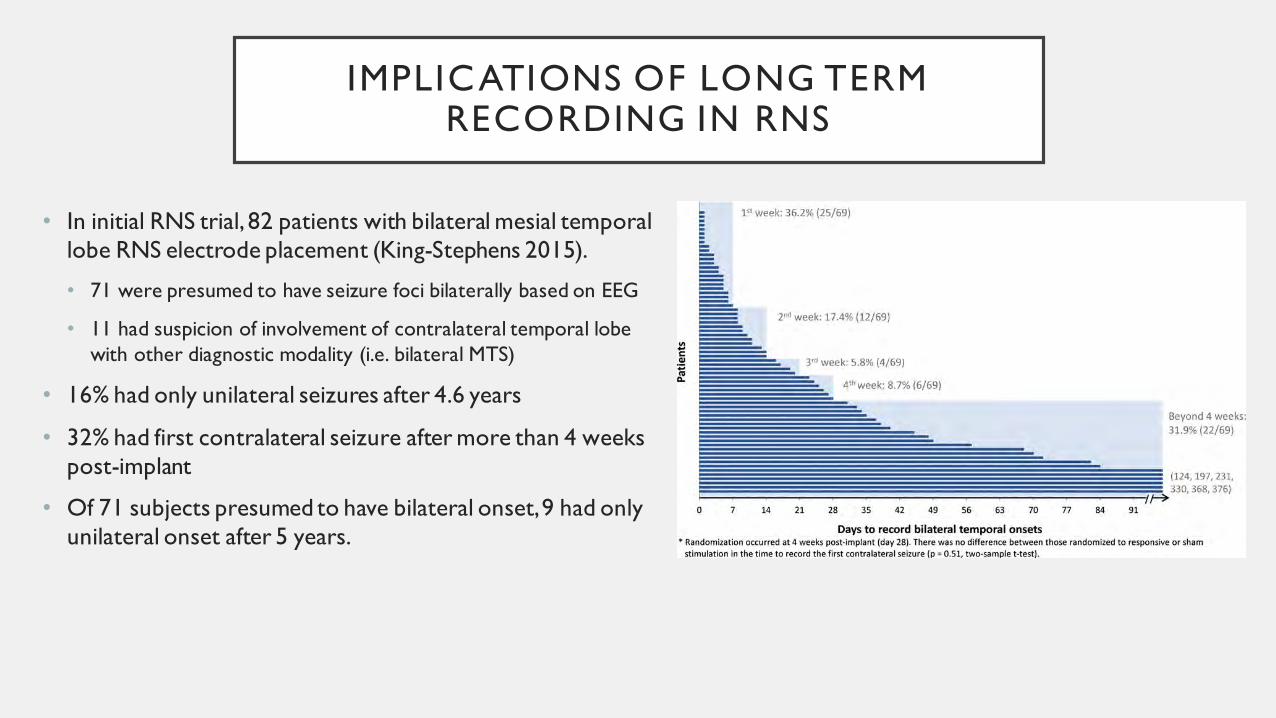
• In initial RNS trial, 82 patients with bilateral mesial temporal
lobe RNS electrode placement (King-Stephens 2015).
• 71 were presumed to have seizure foci bilaterally based on EEG
• 11 had suspicion of involvement of contralateral temporal lobe
with other diagnostic modality (i.e. bilateral MTS)
• 16% had only unilateral seizures after 4.6 years
• 32% had first contralateral seizure after more than 4 weeks
post-implant
• Of 71 subjects presumed to have bilateral onset, 9 had only
unilateral onset after 5 years.
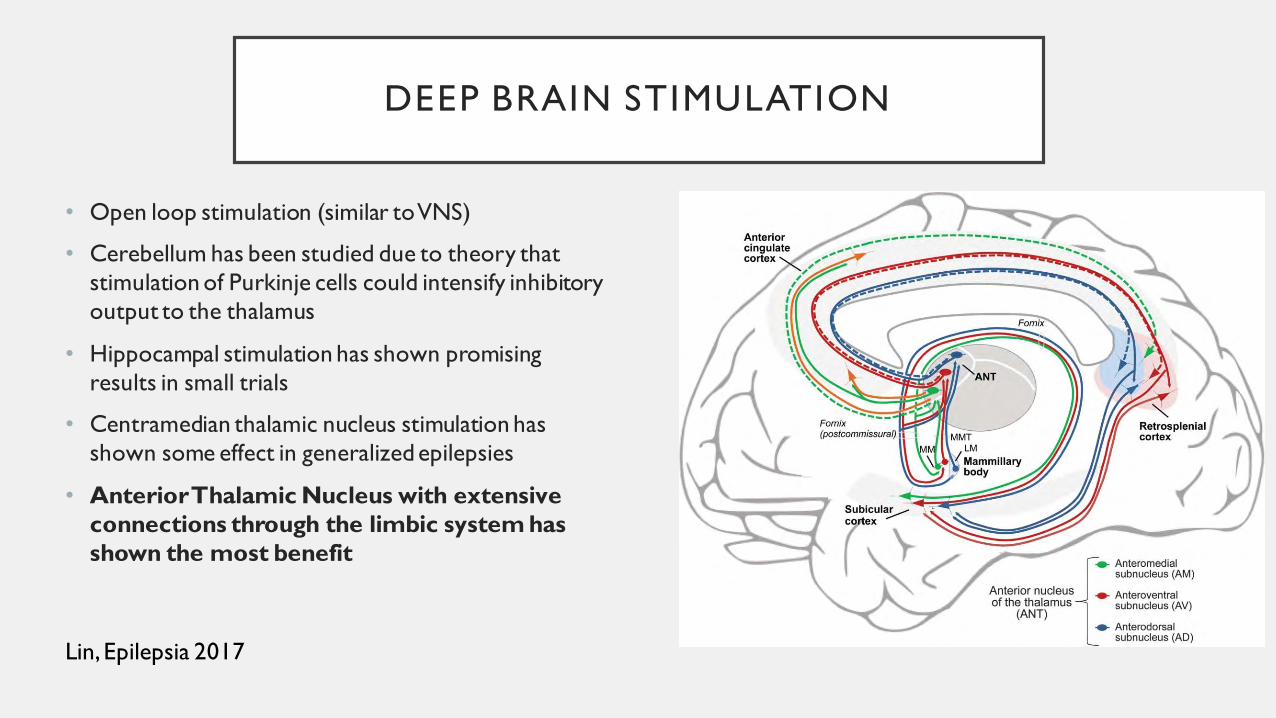
DEEP BRAIN STIMULATION
• Open loop stimulation (similar to VNS)
• Cerebellum has been studied due to theory that
stimulation of Purkinje cells could intensify inhibitory
output to the thalamus
• Hippocampal stimulation has shown promising
results in small trials
• Centramedian thalamic nucleus stimulation has
shown some effect in generalized epilepsies
• Anterior Thalamic Nucleus with extensive
connections through the limbic system has
shown the most benefit
Lin, Epilepsia 2017
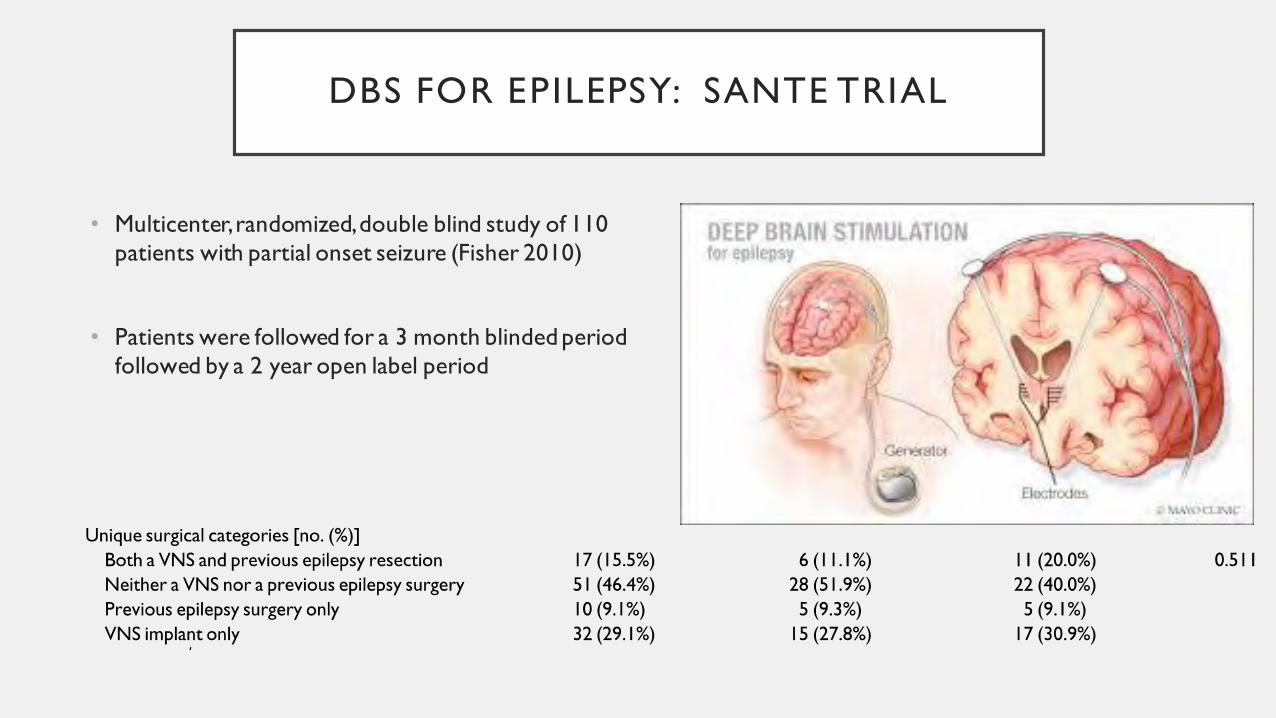
DBS FOR EPILEPSY: SANTE TRIAL
• Multicenter, randomized, double blind study of 110
patients with partial onset seizure (Fisher 2010)
• Patients were followed for a 3 month blinded period
followed by a 2 year open label period
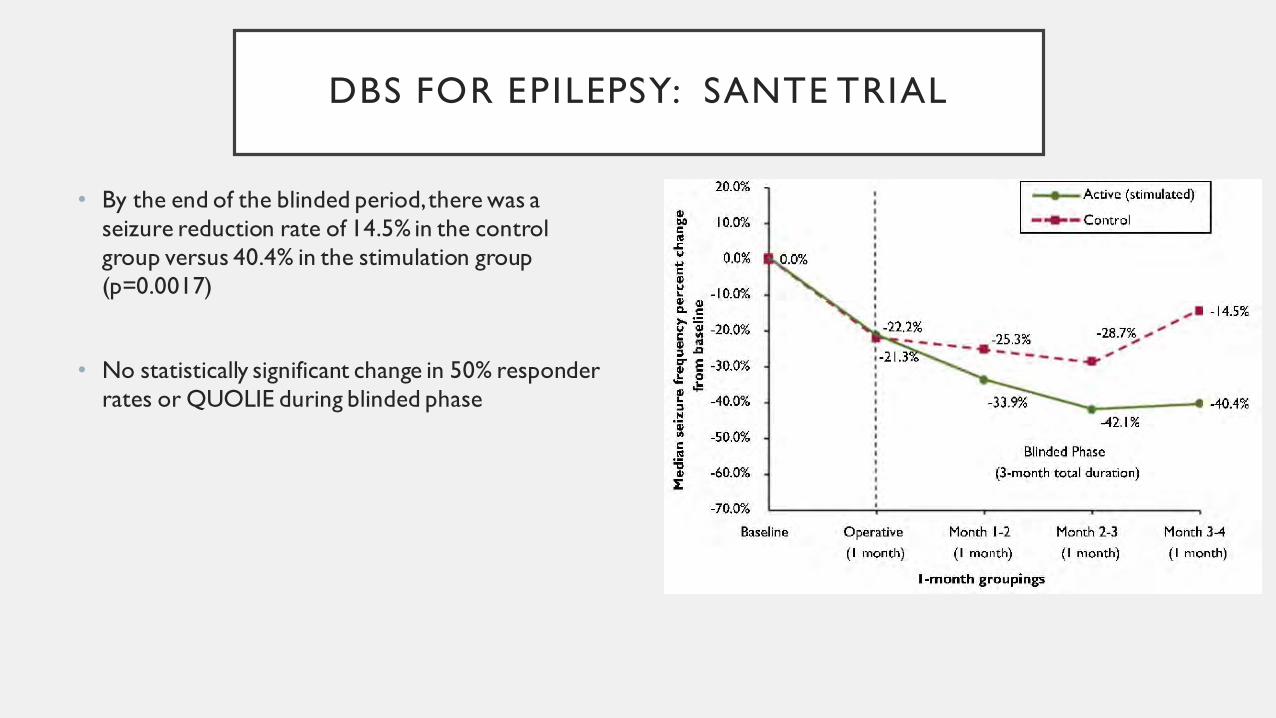
DBS FOR EPILEPSY: SANTE TRIAL
• By the end of the blinded period, there was a
seizure reduction rate of 14.5% in the control
group versus 40.4% in the stimulation group
(p=0.0017)
• No statistically significant change in 50% responder
rates or QUOLIE during blinded phase

DBS FOR EPILEPSY: SANTE TRIAL
• In patients followed long term, median reduction in
seizure frequency was
• 41% at 13 months (n=99),
• 56% at 25 months (n=81),
• 67% at 37 months (n=42).
• 50% responder rate was 54% at 2 years
• QUOLIE score improved significantly at 13 and 25
months (p<0.001)
• No clinical hemorrhages associated with with device
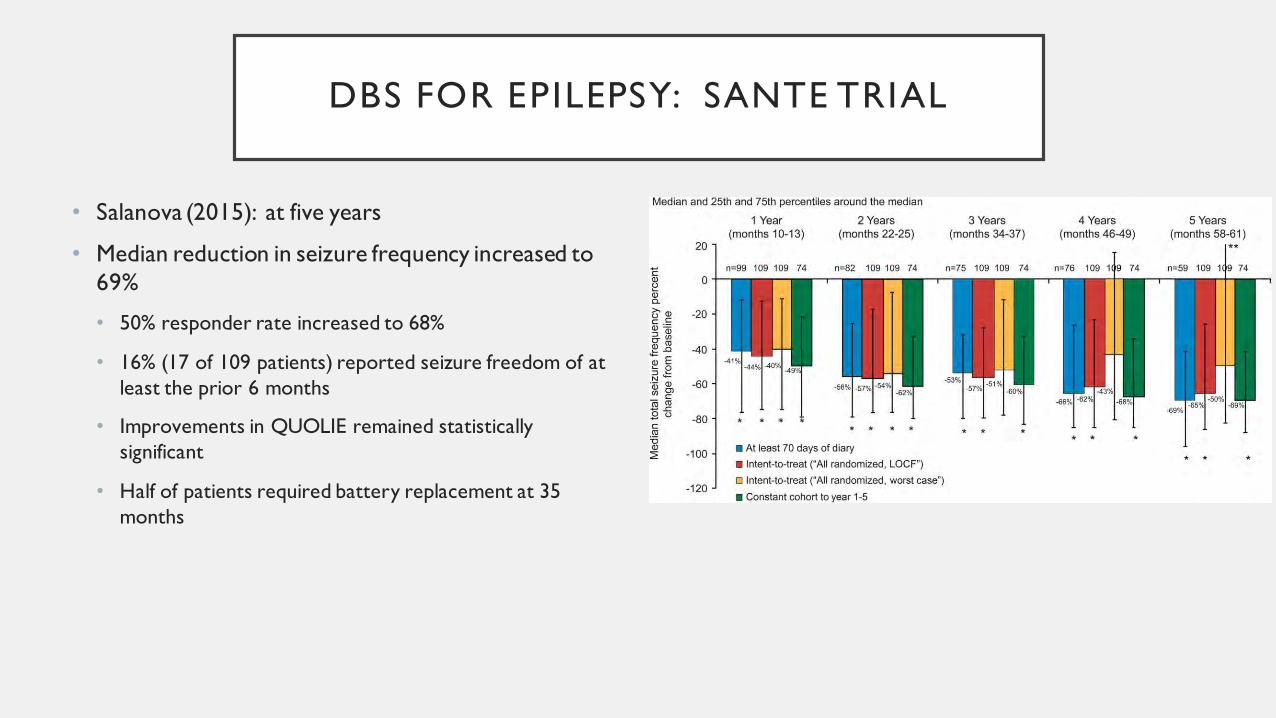
DBS FOR EPILEPSY: SANTE TRIAL
• Salanova (2015): at five years
• Median reduction in seizure frequency increased to
69%
• 50% responder rate increased to 68%
• 16% (17 of 109 patients) reported seizure freedom of at
least the prior 6 months
• Improvements in QUOLIE remained statistically
significant
• Half of patients required battery replacement at 35
months

DBS FOR EPILEPSY
• In 2010, CE (Conformité Européenne) Mark approved DBS of the anterior
thalamic nucleus for treatment of medically refractory partial onset seizures in
Europe.
• In April 2018 the FDA approved DBS of the anterior thalamic nucleus for
treatment of medically refractory partial onset seizures in the United States
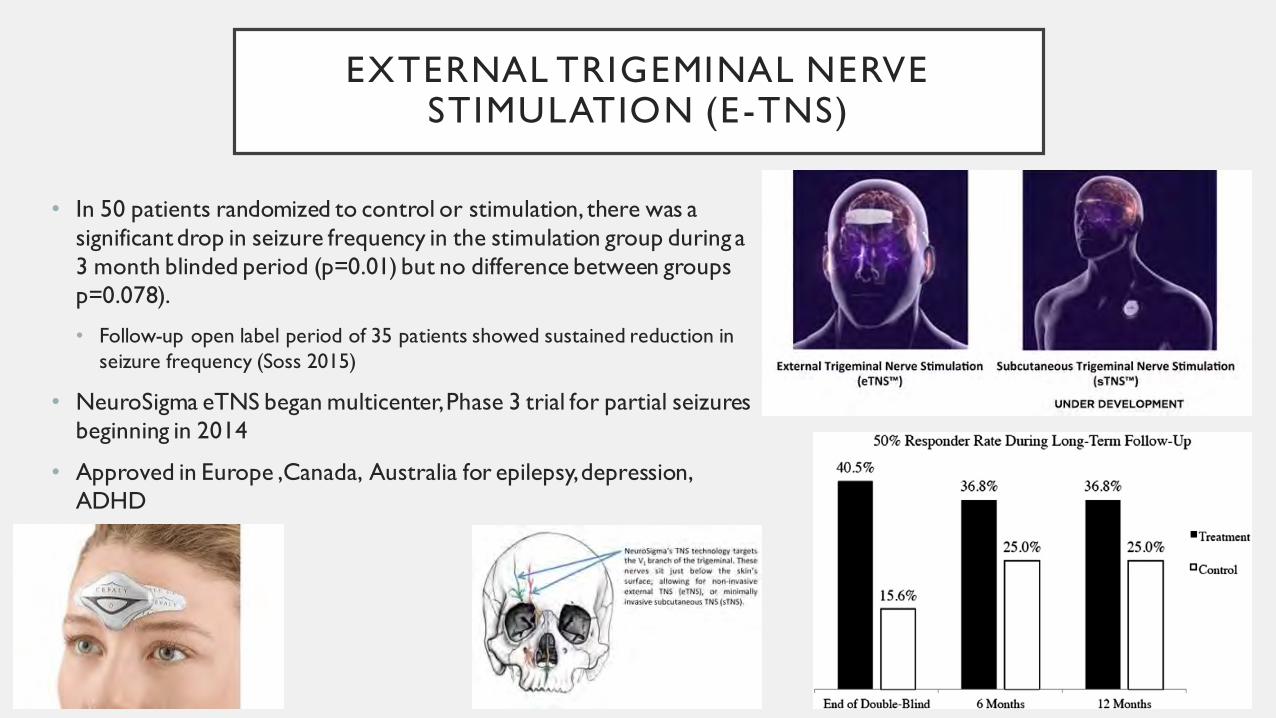
EXTERNAL TRIGEMINAL NERVE STIMULATION (E-TNS)
• In 50 patients randomized to control or stimulation, there was a
significant drop in seizure frequency in the stimulation group during a
3 month blinded period (p=0.01) but no difference between groups
p=0.078).
• Follow-up open label period of 35 patients showed sustained reduction in
seizure frequency (Soss 2015)
• NeuroSigma eTNS began multicenter, Phase 3 trial for partial seizures
beginning in 2014
• Approved in Europe ,Canada, Australia for epilepsy, depression,
ADHD
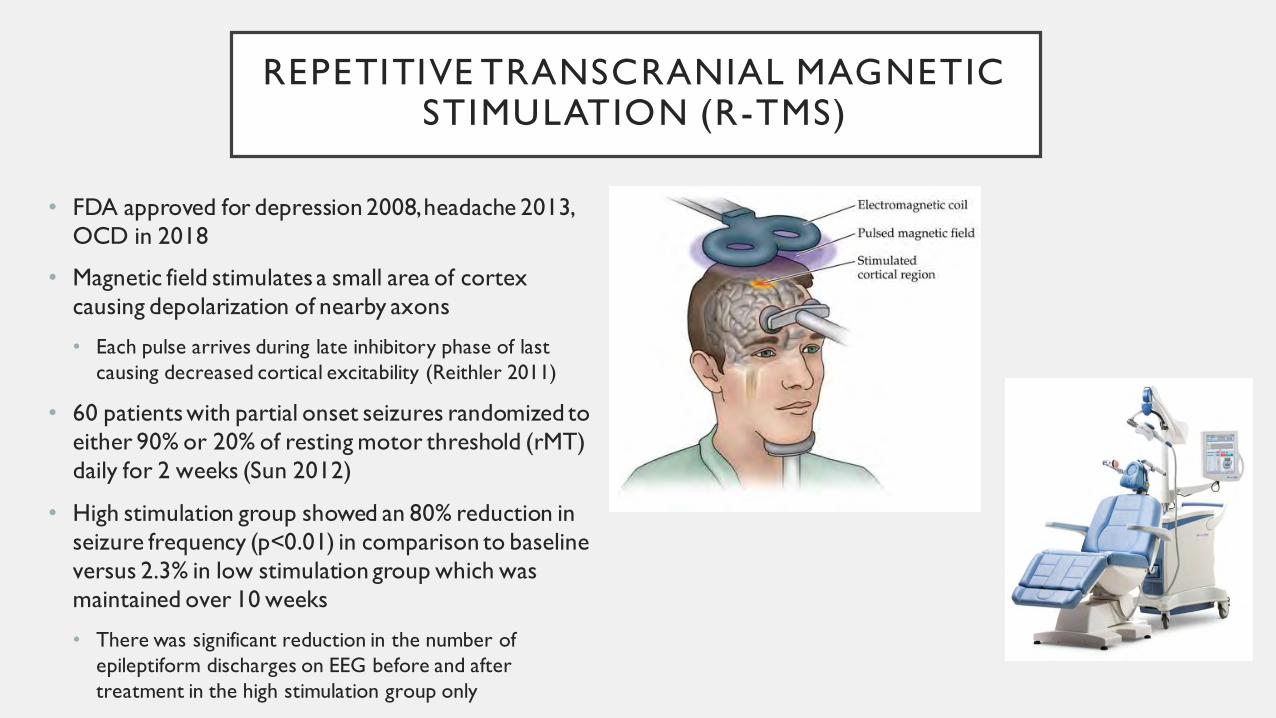
REPETITIVE TRANSCRANIAL MAGNETIC STIMULATION (R-TMS)
• FDA approved for depression 2008, headache 2013,
OCD in 2018
• Magnetic field stimulates a small area of cortex
causing depolarization of nearby axons
• Each pulse arrives during late inhibitory phase of last
causing decreased cortical excitability (Reithler 2011)
• 60 patients with partial onset seizures randomized to
either 90% or 20% of resting motor threshold (rMT)
daily for 2 weeks (Sun 2012)
• High stimulation group showed an 80% reduction in
seizure frequency (p<0.01) in comparison to baseline
versus 2.3% in low stimulation group which was
maintained over 10 weeks
• There was significant reduction in the number of
epileptiform discharges on EEG before and after
treatment in the high stimulation group only
TRANSCRANIAL DIRECT CURRENT STIMULATION (T-DCS)
• tDCS hypothesized to change resting membrane potential by influencing
ion concentrations, transmembrane proteins, and synaptic function to
altering cortical excitability
• 28 patients with mesial temporal lobe epilepsy randomized to placebo
stimulation or to 2mA tDCS for either 3 days, or 5 days with TCD 1ch
Stimulator (San-Juan 2017)
• There was a significant reduction in mean in seizure frequency between both
treatment groups and placebo stimulation at 2 months post-treatment (p=0.0001)
• 5 min showed 54.6% reduction
• 3 min showed 43.4% reduction
• Placebo showed 62.5% reduction
THE END!!!
Related Documents