10.1192/bjp.157.5.735 Access the most recent version at doi: 1990 157: 735-739 The British Journal of Psychiatry A Rossi, S De Cataldo, V Di Michele, V Manna, S Ceccoli, P Stratta and M Casacchia Neurological soft signs in schizophrenia References http://bjp.rcpsych.org/cgi/content/abstract/157/5/735#otherarticles Article cited in: permissions Reprints/ [email protected] to To obtain reprints or permission to reproduce material from this paper, please write to this article at You can respond http://bjp.rcpsych.org/cgi/eletter-submit/157/5/735 service Email alerting click here top right corner of the article or Receive free email alerts when new articles cite this article - sign up in the box at the from Downloaded The Royal College of Psychiatrists Published by on July 16, 2011 bjp.rcpsych.org http://bjp.rcpsych.org/subscriptions/ go to: The British Journal of Psychiatry To subscribe to

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
10.1192/bjp.157.5.735Access the most recent version at doi: 1990 157: 735-739 The British Journal of Psychiatry
A Rossi, S De Cataldo, V Di Michele, V Manna, S Ceccoli, P Stratta and M Casacchia
Neurological soft signs in schizophrenia
References
http://bjp.rcpsych.org/cgi/content/abstract/157/5/735#otherarticlesArticle cited in:
permissionsReprints/
[email protected] To obtain reprints or permission to reproduce material from this paper, please write
to this article atYou can respond http://bjp.rcpsych.org/cgi/eletter-submit/157/5/735
serviceEmail alerting
click heretop right corner of the article or Receive free email alerts when new articles cite this article - sign up in the box at the
fromDownloaded
The Royal College of PsychiatristsPublished by on July 16, 2011 bjp.rcpsych.org
http://bjp.rcpsych.org/subscriptions/ go to: The British Journal of PsychiatryTo subscribe to
British Journal of Psychiatry (1990), 157, 735—739
Neurological Soft Signs in Schizophrenia
A. ROSSI,S. DECATALDO, V. Dl MICHELE,V. MANNA, S. CECCOLI,P. STRATTAand M. CASACCHIA
A standardised clinical examination which focused on neurological soft signs (NSS)was usedby a neurologistblind to diagnosisto assessthe presenceof neurologicalsoft signs. Acomparison of NSS score was made among three groups of subjects consisting of 58DSM—lllschizophrenics,31 of theirhealthyfirst-degreerelativesand38 normalcontrols.Theschizophrenicgroup hadsignificantlyhigherNSStotal scoresthan normalcontrols but didnot differ significantlyfrom their first-degreerelatives'group.The relatives'group showedhigherNSStotalscoresthandidnormalcontrolsalthoughto a lesserextentthanschizophrenics.
Inrecentyearspsychiatryhasfocuseditsattentionon neurodysfunctional correlates of schizophreniaand increasingly sophisticated neuroradiological,neurophysical and neuropsychological studies havebeen pursued for this purpose (for a review seeNasrallah & Weinberger, 1986).
Among various abnormalities, neurological signs,either ‘¿�hard'or ‘¿�soft',were reported by some studiesto show a higher incidence in schizophrenics thannormals (for a review see Heinrichs & Buchanan,1988). ‘¿�Hard'signs have predictive localising power,usually referrable to specific lesions of nuclei,tracts, or nerves. ‘¿�Soft'signs represent abnormalperformance on less specific tests, none of whichby themselves indicate a clearly localisable centralnervous system (CNS) lesion. Included under ‘¿�soft'signs are such phenomena as dysdiadochokinesia,astereognosis, mirror phenomena, choreiform movements, primitive reflexes, diminished dexterity,sensory extinction, and cortical sensory loss. In otherstudies, patients with schizophrenia have shown moreneurological soft signs (NSS) than those with affectiveillness (Walker, 1981; Quitkin et al, 1976) but nomore than those with a history of sociopathy(Quitkin et a!, 1976). Affected monozygotic twinsdemonstrated more neurological impairment thantheir discordant siblings for schizophrenia (Moshereta!, 1971; Pollin eta!, 1966). These abnormalitiesalso correlated with lower birthweights and neonatalproblems (Pollin et a!, 1966).
Torrey (1980) further reported findings on lateralisation of neurological signs, supporting thehypothesis implicating left hemisphere dysfunctionin schizophrenia. Kennard (1960) suggested thatthese signs were significant and probably related todysfunction in subcortical integrating systems suchas the basal ganglia or the brainstem. Moreover,several attempts were made to clarify a possiblerelationship between neurological signs and outcome(Kolakowska et a!, 1985), intelligence quotient
(Quitkin et a!, 1976), medication, demographicvariables, andlocalisation sites(Heinrichs & Buchanan,1988), but there were no unambiguous conclusions.
Comprehensive studies report abnormalities onintegrative sensory functions (Quitkin et a!, 1976),motor co-ordination, and complex motor acts(Heinnchs & Buchanan, 1988); however it is not clearwhether abnormalities in each of these functionsoccur together in a subgroup of neurologicallyimpaired schizophrenics or whether these subgroupsare characterised by impairment in diffuse systems(Heinrichs & Buchanan, 1988).
Interpretation of these results has been complicatedby several factors. Firstly, the aetiology of theneurological abnormalities remains unclear. Thereis evidence of an association between increasedneurological signs and a history of obstetric complications with schizophrenia (Campion & Tucker,1973; McNeil & Kaij, 1978), but the causal linksremain uncertain. Secondly there is a problem ofspecificity. A number of studies have looked forand found an excess of neurological abnormalitiesin other psychiatric patients, both children withbehavioural disorders (Kennard, 1960; Woods &Eby, 1982)and adults with bipolar affective diseases(Quitkin eta!, 1976;Nasrallah eta!, 1983;Mukherjeeet a!, 1984).
Because of the renewed interest in this field, wedesigned a NSS study to explore the presence ofneurological abnormalities in schizophrenics, theirfirst-degree relatives and normal controls, using astandardised neurological examination.
Method
Fifty-eight schizophrenic patients (SCZ) (37men, 21 women)were selected in an unbiased fashion from consecutiveadmissions to our university ward from the catchment areaserved by the hospital. They were admitted for clinicalrelapseand not for researchpurposes.Selectioncriteriafor
735
Schizophrenics(n=58)
mean (s.d.)Normal
controls(n=38)
mean (s.d.)First-degree
relatives(n=31)
mean(s.d.)Age34.82
(10.74)36.15 (12.38)39.19(11.11)Educationallevel: years8.00 (3.64)8.52 (3.10)6.90(2.85)Current
drug dosage'271.87(215.52)——NSStotal score212.63 (4.79)4.07 (2.53)9.80 (2.42)
736 ROSS! ET AL
patients were: (1) DSM—III(American Psychiatric Association, 1980)diagnosiSofchromcor subchronic schizophrenicdisorder; (2) no history of neurological disorder, drug abuseor alcoholism; (3) no history of electroconvulsive therapy(ECT) and no significant side-effects from neurolepticmedication; (4) no history of institutionalisation, defmedas a stay in hospital for more than six months; (5) abilityto live in the community. Schizophrenic subjects hadbeen ill for an average of 11.14 years (s.d. 8.51). Theirages ranged from 18 to 57 years (mean (s.d.) 34.82(10.74)).
Thirty-one first-degree relatives (FDR) (18 men, 13women) participated in the study: they were siblings (n= 28)and parents (n = 3). Their ages ranged from 18 to 59 years(mean (s.d.) 39.19(11.11)). Only one relative of each patient
was assessed for their psychiatric status. This was done bydirect interview. Relatives with evidence of any DSM—IIIaxis I or II disorders were excluded from the study.However, we did not find any DM5—I!!disorder in the‘¿�index'relative interviewed and none of these subjects werereceiving neuroleptic drugs. In selecting relatives forneurological examination, preference was given first tosiblingsand then to parents. For 27 patients no collaborativerelatives were found.
Thirty-eight normal controls (NC) (22 men, 16 women)were screened for this study from family-practice clinics,by an experienced psychiatrist. Their ages ranged from18 to 57 years (mean (s.d.) 36.15 (12.38)). All thesesubjects had no history of mental disorder in first-degreerelatives.
Members of the NC group were matched according toage, sex, and educational level with the SCZ samplewhenever possible.
Neurological examination
Based on previous work (Quitkin et al, 1976; Cox &Ludwig, 1979) we selected 26 items, seven of which werebilateral (i.e. left and right) and significantly related to‘¿�softsigns' dysfunction. This allowed us to record theneurological examinations in a standardised format (seeAppendix 1). All participants received this standardneurological examination administered byastaff psychiatrist(SdC) and a senior neurologist (VM) who were blind toresearch diagnoses.
The severityscorewas in all casesthe sum of the scoresof the 26 items assigned by the senior rater (VM); this wasexpressed as a NSS total score. For training purposes thetwo raters examined the subjects simultaneously and ratedindependently.
Reliability
To ensureinter-raterreliability,the tworatershad evaluatedsimultaneously the neurological status of 30 mixed subjectsindependently from this study, and recorded the resultsseparately. Inter-rater reliability was found to be 0.76(Spearman correlation) for the total score. To test thereliability of observing each sign, a kappa analysis(coefficientof agreement)wasdone for those itemsscored0 or 1, measuringthem as a nominal scale. For the otheritems,scoredas an ordinal scale,the Spearmancorrelationcoefficient was used.
Statistical analysis
The NSS total scores were square-root transformed andanalysed with an independentgroup one-wayanalysis ofvariance (ANOVA) and Scheffe's statistic (Nie et al, 1975).A parametric ANOVA instead of a non-parametric one-wayANOVA was used to achieve a better statistical control ofthe a posteriori comparisons. Age and educational levelwere statistically analysed by one-way ANOVA withouttransformation. Pearson's product-moment correlationcoefficient was used where appropriate.
Results
Table I lists the demographicand clinical features of thethree groups. An independent group analysis of variance(ANOVA) showed no significant differences in age andeducational level between the groups.
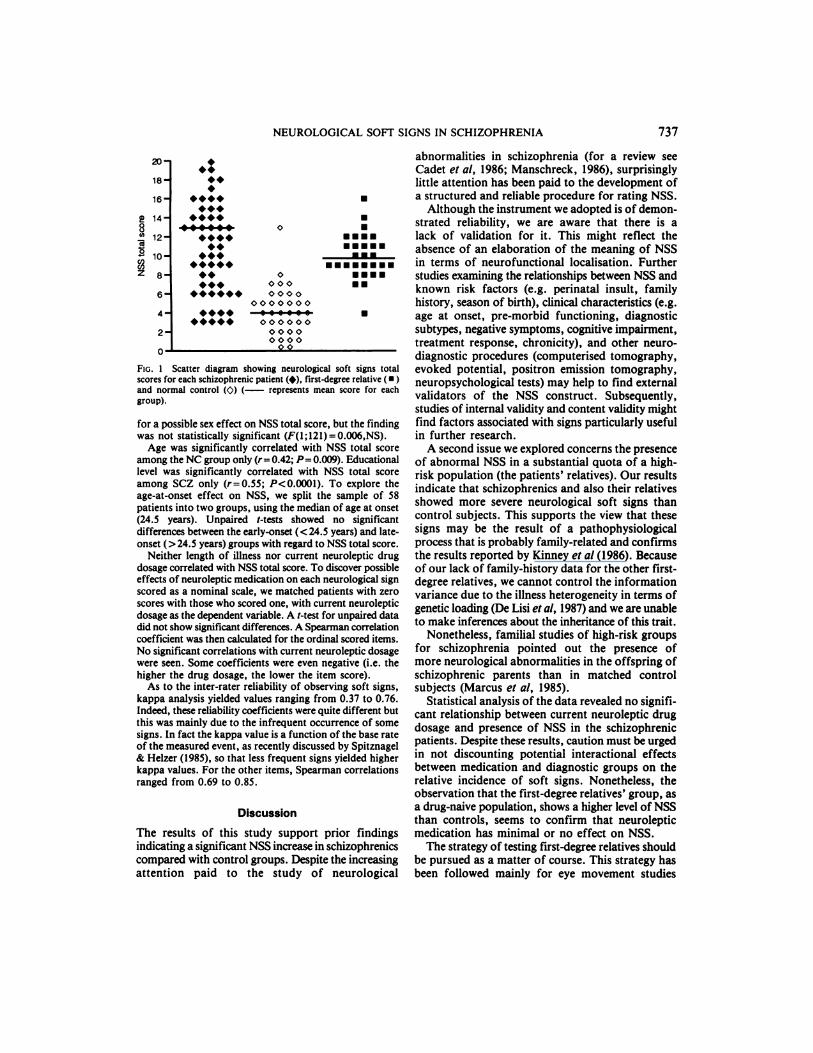
One-way ANOVA demonstrated a significant differencein NSS total score between the three groups. Comparingthe groups in pairs showed that both the SCZ and their FDRhad higher total scores than the NC group, while nodifferences were found between SCZ and their FDR. Theraw data are shown in Figure 1. A two-way ANOVA withstatus and sex as factors was performed in order to look
TABLE I
Demographic characteristics, clinicalfeatures and neurological soft signs (NSS) total score in the three clinical samples
1. Convertedto clorpromazinemilligramequivalents(CPZmg/eq).2. One-wayANOVA(F(2;124)=44.59,P<O.000l):schizophrenicsvscontrols,P'czO.0001;controlsvsfirst-degreerelatives,P<O.000l;schizophrenics vs first-degree relatives, NS.
abnormalities in schizophrenia (for a review seeCadet et al, 1986; Manschreck, 1986), surprisinglylittle attention has been paid to the development of
U a structured and reliable procedure for rating NSS.
Although the instrument we adopted is of demonstrated reliability, we are aware that there is alack of validation for it. This might reflect theabsence of an elaboration of the meaning of NSSin terms of neurofunctional localisation. Furtherstudies examining the relationships between NSS andknown risk factors (e.g. perinatal insult, familyhistory, season of birth), clinical characteristics (e.g.age at onset, pre-morbid functioning, diagnosticsubtypes, negative symptoms, cognitive impairment,treatment response, chronicity), and other neurodiagnostic procedures (computerised tomography,evoked potential, positron emission tomography,neuropsychological tests) may help to find externalvalidators of the NSS construct. Subsequently,studies of internal validity and content validity mightfind factors associated with signs particularly usefulin further research.
A second issue we explored concerns the presenceof abnormal NSS in a substantial quota of a highrisk population (the patients' relatives). Our resultsindicate that schizophrenics and also their relativesshowed more severe neurological soft signs thancontrol subjects. This supports the view that thesesigns may be the result of a pathophysiologicalprocess that is probably family-related and confirmsthe results reported by Kinney et al (1986). Becauseof our lack of family-history data for the other firstdegree relatives, we cannot control the informationvariance due to the illness heterogeneity in terms ofgenetic loading (De Lisi eta!, 1987) and we are unableto make inferences about the inheritance of this trait.
Nonetheless, familial studies of high-risk groupsfor schizophrenia pointed out the presence ofmore neurological abnormalities in the offspring ofschizophrenic parents than in matched controlsubjects (Marcus et al, 1985).
Statistical analysis of the data revealed no significant relationship between current neuroleptic drugdosage and presence of NSS in the schizophrenicpatients. Despite these results, caution must be urgedin not discounting potential interactional effectsbetween medication and diagnostic groups on therelative incidence of soft signs. Nonetheless, theobservation that the first-degree relatives' group, asa drug-naive population, shows a higher level of NSSthan controls, seems to confirm that neurolepticmedication has minimal or no effect on NSS.
The strategy of testing first-degree relatives shouldbe pursued as a matter of course. This strategy hasbeen followed mainly for eye movement studies
U
NEUROLOGICAL SOFT SIGNS IN SCHIZOPHRENIA 737
20
18
16@
@ 14-8
@ 12-
...
..
.....
.......
......
........
..
.........
.........
.
U....
•¿�.......U...U.
0
00000000
0000000ooo•oo000000
00000000
Fic. 1 Scatter diagram showing neurological soft signs totalscores for each schizophrenic patient (i), first-degree relative ( •¿�)and normal control (@) (— represents mean score for eachgroup).
for a possible sex effect on NSS total score, but the findingwas not statistically significant (F(l;l21)= 0.006,NS).
Age was significantly correlated with NSS total scoreamong the NC group only (r=0.42; P=0.009). Educationallevel was significantly correlated with NSS total scoreamong SCZ only (r= 0.55; P<0.000l). To explore theage-at-onset effect on NSS, we split the sample of 58patients into two groups, using the median of age at onset(24.5 years). Unpaired t-tests showed no significantdifferences between the early-onset (<24.5 years) and lateonset (>24.5 years) groups with regard to NSS total score.
Neither length of illness nor current neuroleptic drugdosage correlated with NSS total score. To discover possibleeffects of neuroleptic medication on each neurological signscored as a nominal scale, we matched patients with zeroscores with those who scored one, with current neurolepticdosage as the dependent variable. A t-test for unpaired datadid not show significant differences. A Spearman correlationcoefficient was then calculated for the ordinal scored items.No significant correlations with current neuroleptic dosagewere seen. Some coefficients were even negative (i.e. thehigher the drug dosage, the lower the item score).
As to the inter-rater reliability of observing soft signs,kappa analysis yielded values ranging from 0.37 to 0.76.Indeed, these reliability coefficients were quite different butthis was mainly due to the infrequent occurrence of somesigns. In fact the kappa value is a function of the base rateof the measured event, as recently discussed by Spitznagel& Helzer (1985), so that less frequent signs yielded higherkappa values. For the other items, Spearman correlationsranged from 0.69 to 0.85.
Discussion
The results of this study support prior findingsindicating a significant NSS increase in schizophremcscompared with control groups. Despite the increasingattention paid to the study of neurological

738 ROSS! ET AL
(Holzman, 1987) and for psychophysiological studies(Friedman et a!, 1982; Saitoh et a!, 1984) withencouraging results, ruling out the possibility thatthese indices might represent trait-markers in schizophrenia (Erlenmeyer-Kimling & Cornblatt, 1987).
Recent views about thalamic dysfunction in schizophrenia ruled out the possible common role of thesame thalamic regions in both neurological softsigns and smooth pursuit eye movement (SPEM)impairments (Oke & Adams, 1984). In a preliminaryreport Thaker et a! (1988) found an associationbetween NSS and SPEM impairment. Because of thereported SPEM and NSS impairment in first-degreerelatives of schizophrenic patients (Holzman, 1987;Kinney et a!, 1986) these signs appear to be strongcandidates for biological markers of schizophrenia.Taken together, these observations suggest the needto study NSS further in the first-degree relatives ofschizophrenics and in people considered to be at riskof the disorder to establish the potential usefulnessof the NSS as a trait marker for schizophrenia.
Appendix-Condensed neurological examination
Palmomental test The palm is stroked with a key and thechin is observed for the characteristic slight movement. Apositive response is any reflex movement of the chin. Score0—2(0—1left; 0—1right).
Snout reflex The upper lip of the patient is percussedwith a percussion hammer and the perioral region isobserved for the characteristic movement. A positiveresponse is any reflex movement of the region. Score 0—1.
Suck reflex This reflex is elicited by the examiner'sfinger which runs from the cheek to the mouth's omolateralcommisure. A positive response is any sucking movementof the mouth. Score0—2(0—1left; 0—1right).
Blink reflex This reflex is elicited by gentle taps of theglabella repeated at one second intervals. An abnormalresponse is a failure to habituate the reflex after five taps.Score 0—1.
Gaze impersistence The patient is asked to gaze at apoint for some seconds. Any gaze impersistence during 30seconds is scored as abnormal. Score 0—1.
Ocular vergence The patient is asked to follow with theeyes a moving target along the visual axis. Any defect ofthe ocular vergence is scored as abnormal. Score 0—1.
Nystagmus The patients' eyes are observed for thepresence of a nystagmus as he gazes at an object that movesaround him describing an angle of 60 degrees respectivelyon the left and on the right-hand side. Score 0—2;(0—1left;0—1right).
Oral apraxia Difficulty in the patient's ability to showhis/her teeth and puff out cheeks is scored as abnormal.Score 0—2;(0—1for each sign).
Motor perseveration inspoken commands test This testattempts to reveal motor perserveration of the patient inspite of the verbal request to perform a simple act. Forexample, the examiner asks the patient to “¿�pointto your
nose with a finger' ‘¿�. Any perseveration of the asked actis scored as abnormal. Score 0—1.
Grasp reflex Each palm is stroked by the examiner withmoderate pressure from the wrists to the fingers. A positiveresponse is any grasping motor movement of the hand andis graded on a scale of 0 to 5. Score 0—10;(0—5left; 0—5right).
Blunt vs sharp discriminationtest The patient is touchedin a random but standardised fashion with the sharp andblunt ends of a pin on the dorsal surface of the left andright hands while the eyes are closed. The patient says“¿�sharp―or “¿�blunt―upon stimulation. Any misperceptionon the left andon the right sideis scoredindependentlyon a scale of 0 to 5. Score 0—10;(0—5left; 0—5right).
Graphestesia The patient is asked to identify a numberthat the examiner traces on the back of the patient's wrist,on the left and the right side alternately. The patient isinformed that the number will be from zero to five. Threestimuli are applied in a random but standardised fashion.Anymisperceptionon the leftand on the rightsideis scoredindependently on a scale of 0 to 3. Score 0—6;(0—3left; 0—3right).
Simultaneous bilateral tactile extinction The patient isseated, with the right hand, dorsal surface exposed, on theright thigh and the left hand, dorsal surface exposed, onthe left thigh,witheyesclosed.The patient is informedthatthe examiner will touch him/her in one or more places, andthat he/she should report exactly where he/she feels this.The followingorder was followed: right hand; right sideof face; right sideof face and right hand; left sideof faceand left hand; both hands; both sides of the face; right sideof face and left hand; and left side of face and right hand.A positive response is an incorrect perception. A scale ofoto6correspondstothenumberofmisperceptions.Score0—6.
Complex motor acts The examiner watches the patienttie a shoe and scores the effort as positive if abnormaldifficulty is exhibited on a scale of 1 to 5. A score of 1corresponds to minimal difficulty and 5 to completeinability to perform the act successfully. No difficulty inperforming the item is scored as 0. Score 0—5.
Imaginary acts The imaginary act of pouring andstirring coffee is observed objectively for omission of theessential parts of the act; holding a coffee pot, then pouringthe coffee in a cup, replacing the coffee pot, taking the teaspoon, and stirring the coffee. Any major omissionconstitutes a positive score. A scale of 0 to 5 is used whichindicates the number of omissions. Score 0—5.
Astereognosis One at a time a coin, key, and pen areplaced into the patient's palm by the examiner. The patientmust identify the object without vision and using only thehand, left or right respectively, in which the object has beenplaced.A positiveresponseisafailuretoidentifyanobject.A scale of 1 to 3 indicates the number of failures for theright and for the left one respectively. Score 0—6(0—3left;0—3right).
Two-object test The patient is asked to perform fourmanoeuvres of increasing complexity with a pencil and akey, for example, “¿�pointto the pencilwith the tip of thekey―.The score is based on a failure to complete any ofthe manoeuvres. Score 0—4.

NEUROLOGICALSOFT SIGNS IN SCHIZOPHRENIA 739
Tapping-rhythm test The examiner taps out threedifferent rhythms individually and the patient is asked toduplicate each one. A positive response is an erroneousresponse to any rhythm. Score 0—3.
Dysdiadochokinesia The patient's ability to performrapid alternating movements is evaluated. The patient isasked, for example, to slap the palm and then the back ofthe hand rapidly and alternately on his own knee. A positiveresponse is any pattern characterised by irregular rhythm,uneven force and breakdown of the alternating movements.It is graded on a scale of 1 to 2. Score 0—2.
Acknowledgement
This study was supported, in part, by a grant from ConsiglioNazionale dde Richerche (no. 89.00328-75).
ReferencesAMERICAN Psya@raic ASSoCIATION (1980) Diagnostic and Statistical
ManualofMentalDisorders(3rdedn)(DSM-III).Washington,DC: APA.
CADET, J. L., RICKLER, K. C. & WEINBERGER, D. R. (1986) The
clinical neurologic examination in schizophrenia. In TheNeurologyof Schizophrenia (eds H. A. Nasrallah & D. R. Weinberger),pp. 1—47.Amsterdam: Elsevier Science Publishers.
CAMPI0N, E. W. & TUCKER,0. J. (1973) A note on twin studies,schizophrenia, and neurological impairment. Archives of GeneralPsychiatry, 35, 60—65.
Cox, S. M. & LUDWIG,A. M. (1979) Neurological soft signs andpsychopathology. Journal of Nervous and Mental Disease, 167,161—165.
DELISI, L. E., GOLDIN, L. R. & GERSHON, E. S. (1987) Studies of
biological factors associated with the inheritance of schizophrenia:a selective review. Journal of Psychiatric Research, 21, 507-5 13.
E@anYm-KIMuNo, L. & Coai'naAi@r, L. (1987) High-risk research
in schizophrenia: a summary of what has been learned. Journalof Psychiatric Research, 21, 401—411.
FRIEDMAN,D., VAUGHAN,H. 0. & ERLENMEYER-K1MLING,L. (1982)Cognitive brain potentials in children at risk for schizophrenia:preliminary findings. Schizophrenia Bulletin, 8, 514—531.
HEINRICHS, D. S. & BUCHANAN, R. W. (1988) Significance andmeaning of neurological signs in schizophrenia. AmericanJournal of Psychiatry, 145, 11-18.
H0LzMAN,P. 5. (1987) Recent studies of psychophysiology inschizophrenia. Schizophrenia Bulletin, 13, 49—75.
KENNARD,K. (1960) Value of equivocal signs in neurologicaldiagnosis. Neurology, 10, 753—764.
KINNEY, D. K., WOODS, B. T. & YURGELUN-TODD,D. (1986)Neurologic abnormalities in schizophrenic patients and theirfamilies. II: Neurologic and psychiatric findings in relatives.Archives of General Psychiatry, 43, 665—668.
Ko@xowsi@, T., WILLIAMS,A. 0., JAMII0R,K., et a! (1985)Schizophrenia with good and poor outcome. III: Neurological
‘¿�soft'signs, cognitive impairment and their clinical significance.British Journal ofPsychiatry, 146, 348—357.
MANSCHRECK, T. C. (1986) Motor abnormalities in schizophrenia.
In The Neurologyof Schizophrenia(eds H. A. Nasrallah&D. R. Weinberger), pp. 65—96.Amsterdam: Elsevier SciencePublishers.
MARCUS,J., HANS, S. L. LEMOw, E., et al (1985) Neurologicalfindings in high-risk children: assessment and 5 year follow up.Schizophrenia Bulletin, 11, 85—100.
MCNEIL, T. F. & KAIJ, L. (1978) Obstetric factors in the development of schizophrenia: complications in the births of preschizophrenics and in reproduction in schizophrenic parents. InTheNature ofSchizophrenia (eds L. C. Wynne, R. L. Cromwell,S. Matthysse), pp. 401—429.New York: John Wiley & Sons.
MOSHER, L. R., POLLIN, W. & STABENAU,J. (1971) Identical twindiscordant for schizophrenia. Archives of Genera! Psychiatry,24, 422—430.
MUKHERJEE, S., SHUKLA, S. & ROSEN, A. (1984) Neurologicalabnormalities in patients with bipolar disorder. BiologicalPsychiatry, 19, 337—345.
NASRALLAH, H. A., TIPPIN, F. & MCCALLEY-WHII-IERS, M. (1983)Neurological soft signs in manic patients: a comparison withschizophrenic and control group. Journal ofAffective Disorders,5, 45—50.
—¿� & WEINBERGER, D. R. (eds) (1986) The Neurology of
Schizophrenia. Amsterdam: Elsevier Science Publisher.NIE, N. H., HULL, C. H. & JENKINS, 0. J. (1975) SPSS: Statistical
Packagefor the SocialSciences(2nd edn).New York:McGraw-Hill.
OKE, A. F. & ADAMS,R. N. (1984) Elevated thalamic dopamine:possible link to sensory dysfunctions in schizophrenia.Schizophrenia Bulletin, 13, 589—604.
POLLIN, W., STABENAU, J. R. & MOSHER, L. R. (1966) Life historydifferences in identical twins discordant for schizophrenia.American Journal of Orthopsychiatry, 36, 492—509.
QUITKIN,F., RIFKIN,A. & KLEIN,D. F. (1976) Neurologic soft signsin schizophrenia and character disorders. Archives of GeneralPsychiatry, 33, 845—853.
SAn-oH, 0., NIWA, S., HIRAMATSU,K., et a! (1984) Abnormalitiesin late positive components of event-related potentials may reflecta genetic predisposition to schizophrenia. Biological Psychiatry,19, 293—303.
SPITZNAGEL, E. L. & HELZER, J. E. (1985) A proposed solution to
the base rate problem in the Kappa statistic. Archives of GeneralPsychiatry,42,725—728.
THAKER, 0., NGUYEN, J., BUCHANAN, B., et a! (1988) Eye move
ment abnormalities in schizophrenia. In Book of Abstracts,Society of Biological Psychiatry, 43rd annual convention &
scientific meeting, May 4—81988, Montreal, Canada.TORREY,E. F. (1980) Neurological abnormalities in schizophrenic
patients. Biologica! Psychiatry, 15, 381—388.
WALKER, E. (1981) Attentional and neuromotor functions ofschizophrenics, schizoaffectives, and patients with other affectivedisorders. Archives of Genera! Psychiatry, 38, 1355—1358.
Woons,B.T.& EBY,M. D.(1982)Excessivemirrormovementsand aggression. Biological Psychiatry, 17, 23—32.
*Correspondence
*Alessandro Rossi, MD, Psychiatric Clinic, University of L ‘¿�Aquila,Ospedale di S. Maria di Collemaggio, 67100 L ‘¿�Aquila,Italy; Stefano de Cataldo, MD;Vittorio Di Michele, MD;Vincenzo Manna, MD;Simona Ceccoli, MD; Paolo Stratta, MD; Institute of Experimental Medicine, Psychiatric Clinic, Universityof L ‘¿�Aquila;Massimo Casacchia, Professor and Chafrman, Institute of Experimental Medicine, PsychiatricClinic, University of L ‘¿�Aquila
Related Documents











