NEUROLOGICAL PRINCIPLES

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
NEUROLOGICAL
PRINCIPLES
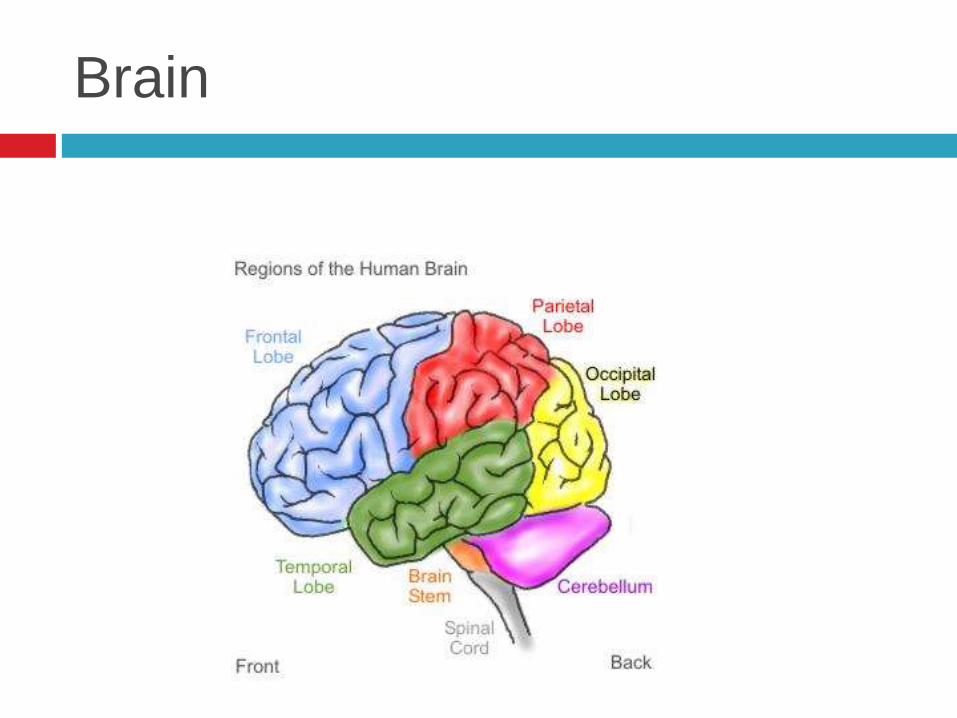
Brain
Localisation
Dominant hemisphere
Almost all right handed have language function in
left hemisphere and prob about 70% left handed
Non-dominant hemisphere
In R hemisphere lesion (in L dominant) causes
abnormalities of perception eg. Losing way,
dressing apraxia or constructional apraxia

Examples of lesions in cortex (L hemisphere dominant)
Either frontal
Intellectual impairment, personality change
L temporoparietal
Acalculia, alexia, agraphia, Wernicke’s aphasia, field defects
R parietal
Dressing apraxia, neglect L limbs
Occipital
Visual field defects, disturbance of visual recognition
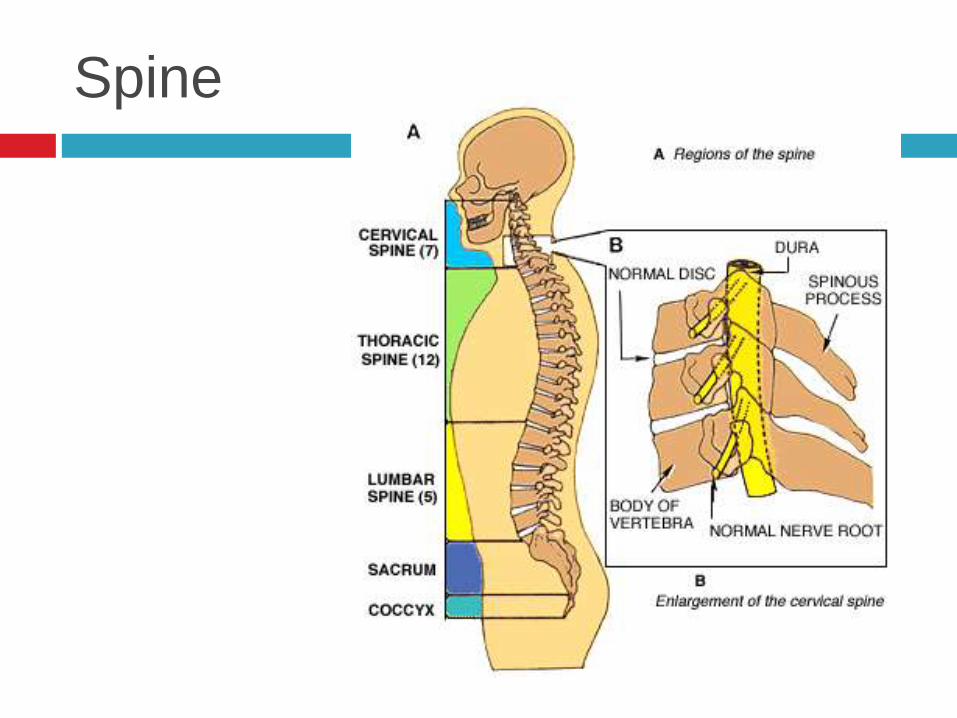
Spine
Neurological diagnosis
Anatomical
Where is the lesion?
Pathological
What disease?
History
History
Crucial
Allow patient to speak
Age
Occupation
Handedness
Timing of symptoms
Discriminant questions
Past medical history
Medication history
Family history
Social history

Examination
Level of consciousness
Cognitive function
Speech
Cranial nerves
Neck and trunk
Limbs – motor and sensory
Gait
Consciousness
Awareness of self and surroundings
Depends on:
Sensory input into brain
Intrinsic activity of reticular activating system in
brainstem
Intact cerebral hemispheres

Altered level of consciousness
Structural
Trauma, infarction, haemorrhage, tumour, demyelination of brainstem or cerebral hemispheres
Diffuse
Reduced availability of substances required for normal brain metabolism (oxygen, glucose)
Metabolic disorders (renal or liver failure, hypothermia, vitamin deficiencies)
Seizures
Inflammation of brain or meninges
Drugs and toxins (opiates, anti-depressants, hypnotics, alcohol)

Cognitive function
Higher brain function
Distributed functions
Require multiple parts of brain Attention and concentration
Memory
personality
Localised functions
Require part of one cerebral hemisphere language
Cranial nerves
I Olfactory nerve
II Optic nerve
III Oculomotor nerve
IV Trochlear nerve
V Trigeminal nerve
VI Abducens nerve
VII Facial nerve
VIII Vestibulocochlear nerve
IX Glossopharyngeal nerve
X Vagus nerve
XI Accessory nerve
XII Hypoglossal nerve
Motor function
Involves:
Higher centres
Upper motor neurone
Lower motor neurone
Neuromuscular junction
Muscle
Plus input from basal ganglia and cerebellum
Feedback from sensory pathways

Upper and lower motor neurones
Upper motor neurone
Cell body in motor cortex
Axon in corticospinal (pyramidal tracts)
Synapses with anterior horn cell
Lower motor neurone
Axon from anterior horn cell in spinal cord to
voluntary muscle

Upper and lower motor neurones
Examination
Wasting
Most prominent when muscle has been denervated from LMN lesion
Involuntary movements
fasciculations
Tone
Resistance detected on passive movement of patient’s joints
Power
Characteristic patterns of weakness eg. UMN ‘pyramidal distribution’ of weakness
Reflexes
Coordination
Ataxia - cerebellar disease.
Sensory ataxia due to loss of joint position sense
Sensation
Plantars

Neurological gait disorders
Spastic paraparesis scissoring
Spastic hemiparesis Rigid leg, circumducts
Bilateral foot drop steppage
Cerebellar lesion Wide-based gait, staggering, unable to walk heel-toe
Parkinsonism Rigid shuffling gait, ‘festinant’
Proximal myopathy waddling
Sensation
Joint position sense
Vibration sense
Touch and pressure
Pain and temperature
Sensation
Two main pathways
Joint position and vibration sense – posterior columns of spinal cord
Pain and temperature – spinothalamic tracts
Touch and pressure sensation – ascend by a number of routes
Sensory symptoms
Numbness
Inability to detect heat and cold
Paraesthesia – tingling, ‘pins and needles’
Dysaesthesia – distorted sensation from sensory stimuli
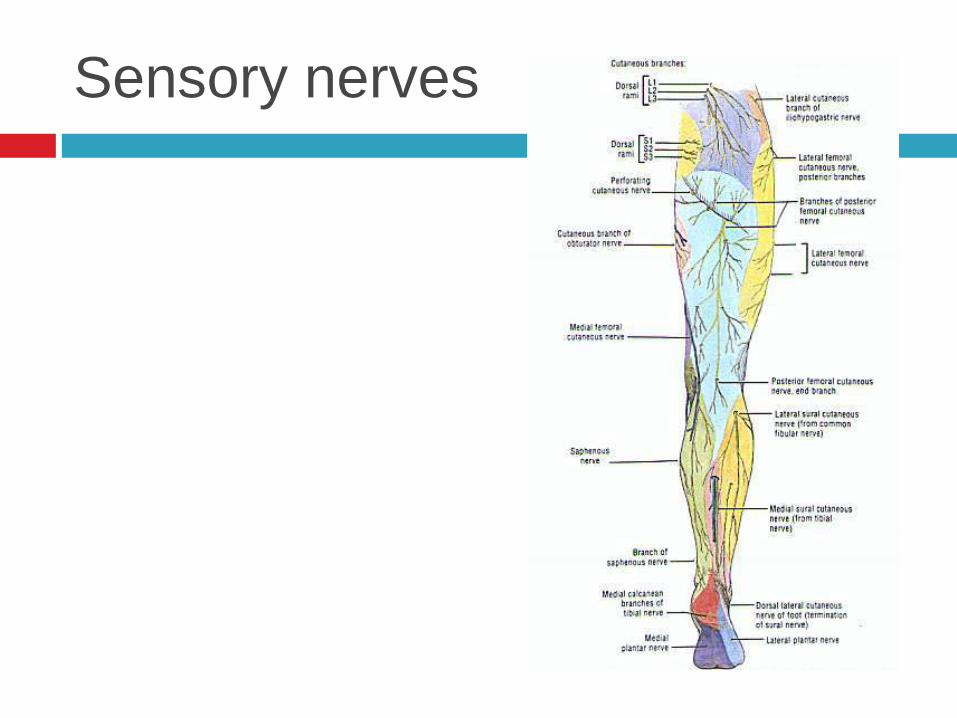
Sensory nerves
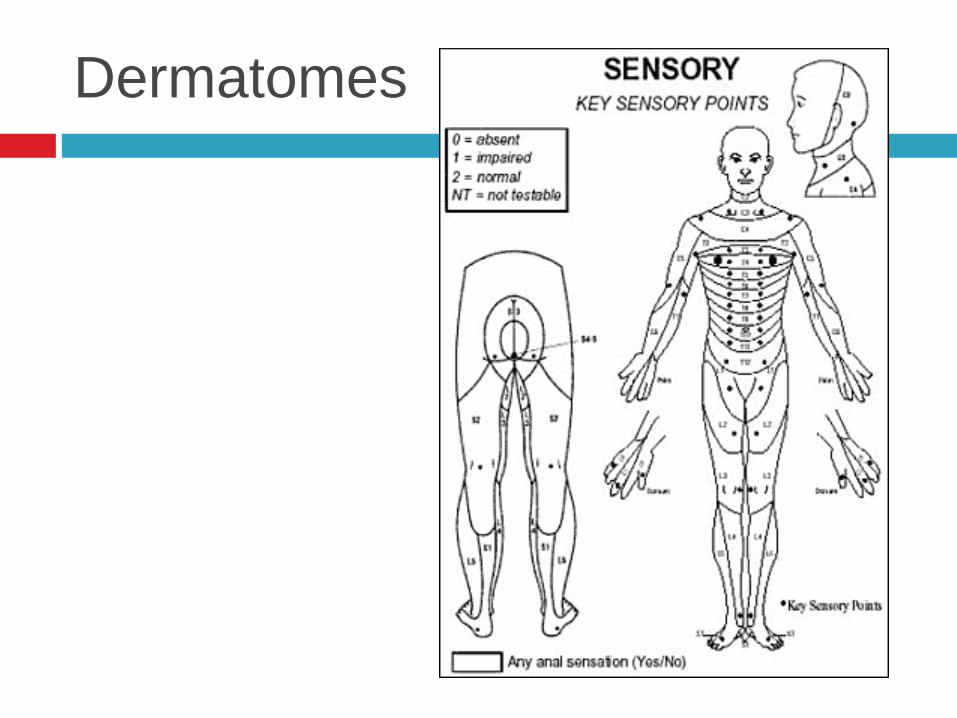
Dermatomes
Autonomic function
Sympathetic and parasympathetic
Involuntary control of viscera and glands
Involved in:
Pupil responses
Blood pressure and heart rate
Bladder, bowel, sexual function
Sweating, lacrimation, salivation
Related Documents











