NEUROLOGIC COMPLICATIONS

NEUROLOGIC COMPLICATIONS. Delirium, Cognitive Disorder, and Psychosis Seizure Disorders Stroke and Transient Ischemic Attacks.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

NEUROLOGIC COMPLICATIONS

NEUROLOGIC COMPLICATIONS
• Delirium, Cognitive Disorder, and Psychosis• Seizure Disorders• Stroke and Transient Ischemic Attacks

Delirium, Cognitive Disorder, and Psychosis
common complication of surgery.• Most precipitating factors• Postoperative anemia• electrolyte imbalance• Sepsis• Malnutrition• bladder catheterization• extended duration of anesthesia• Infection• respiratory complications• Acute alcoholic withdrawal

Delirium, Cognitive Disorder, and Psychosis
• Presentation• acutely agitated, uncooperative, and confused• altered level of consciousness and changes in
cognition• reduced ability to focus• decreased levels of awareness• and difficulty with attention• Hallucinations• These changes have a tendency to fluctuate during
the course of the day and are worse at night
Delirium, Cognitive Disorder, and Psychosis
Treatment• Recognition of the disorder • Close observation and monitoring • Identification and elimination of the precipitating factor • Treatment of any associated laboratory abnormalities • Selective use of imaging or other studies to rule out an organic
brain lesion • Application of measures to protect the patient and staff • Treatment
– Haloperidol– Benzodiazepines are the drug of choice for acute alcohol withdrawal– β-blockers (to control autonomic manifestations)– clonidine (to control hypertension)
Seizure Disorders
Etiology• Primary causes : intracranial tumor,
hemorrhage, trauma, idiopathic seizure activity
• Secondary causes : metabolic derangement, sepsis, systemic disease processes, and pharmacologic agents
Seizure Disorders
Patients high risk for postoperative seizure• previous history of epilepsy • acutely withdrawing from alcohol or
medications • pharmacologic agents : antidepressants,
hypoglycemic agents, and lidocaine.

Seizure Disorders
Presentation• Convulsions• rhythmic myoclonic activity• loss of consciousness• change in mental status • fecal and urinary incontinence• lack of neurologic responsiveness• postevent amnesia
Seizure DisordersManagement
• IV benzodiazepines is essential to stop the seizure activity and is the standard for immediate care
• maintenance after seizures are carbamazepine (Tegretol) and valproic acid
• diagnostic workup for its cause is initiated– history and physical examination– medication and drug use– white blood cell count to rule out occult infection– electrolyte and metabolic assessment.– CT or MRI – electroencephalogram
Stroke and Transient Ischemic Attacks
• Ischemic strokes most commonly• Cause• perioperative hypotension • overzealous control of hypertension • cardioemboli in patients with atrial
fibrillation,MI, bacterial endocarditis• DVT and traversing a patent foramen ovale

Stroke and Transient Ischemic Attacks
• Presentation• neurologic changes• focal alteration in motor function• alteration in mental status• aphasia
Stroke and Transient Ischemic AttacksManagement
• IV line• echocardiogram to assess the heart for structural disease • Coagulation parameters• CT scan or MRI of the brain for distinguish hemorrhagic and ischemic
stroke • Therapy is dictated by the underling mechanism of the stroke
– control of the hypertensionAntihypertensive– embolic stroke anticoagulation– hemorrhagic stroke coagulopathy with protamine– Mannitol and dexamethasone reduce cerebral swelling.– Surgical intervention indicated in patients with a localized
hematoma or vascular anomaly– low-dose aspirin therapy standard for acute ischemic infarction

RENAL AND URINARY TRACT COMPLICATIONS

RENAL AND URINARY TRACT COMPLICATIONS
• Urinary Retention• Acute Renal Failure

Urinary Retention• a common postoperative complication• Most in perianal operations and hernia repair
Presentation• Most patients should not go more than 6 to 7 hours
without passing some urine• Dull pain, constant discomfort in the hypogastrium• Percussion just above the pubis reveals fullness and
tendernessTreatment
• Foley catheter• initial straight catheterization
Acute Renal Failure
• a sudden reduction in renal output that results in the systemic accumulation of nitrogenous wastes
• Etiology– Any factor that interferes with or disrupts this
mechanism results in ARF• Hypotension• nonsteroidal anti-inflammatory drugs • gram-negative sepsis

Acute Renal Failure
• more prevalent in– major vascular procedures (ruptured aneurysm)– renal transplantation– cardiopulmonary bypass procedures– major abdominal cases associated with septic shock– major urologic operations – cases in which there is major blood loss– life-threatening trauma– major burn injuries– contrast-induced nephropathy

Cause of postoperative acute renal failure
Sabiston Textbook of Surgery, 18th Edition
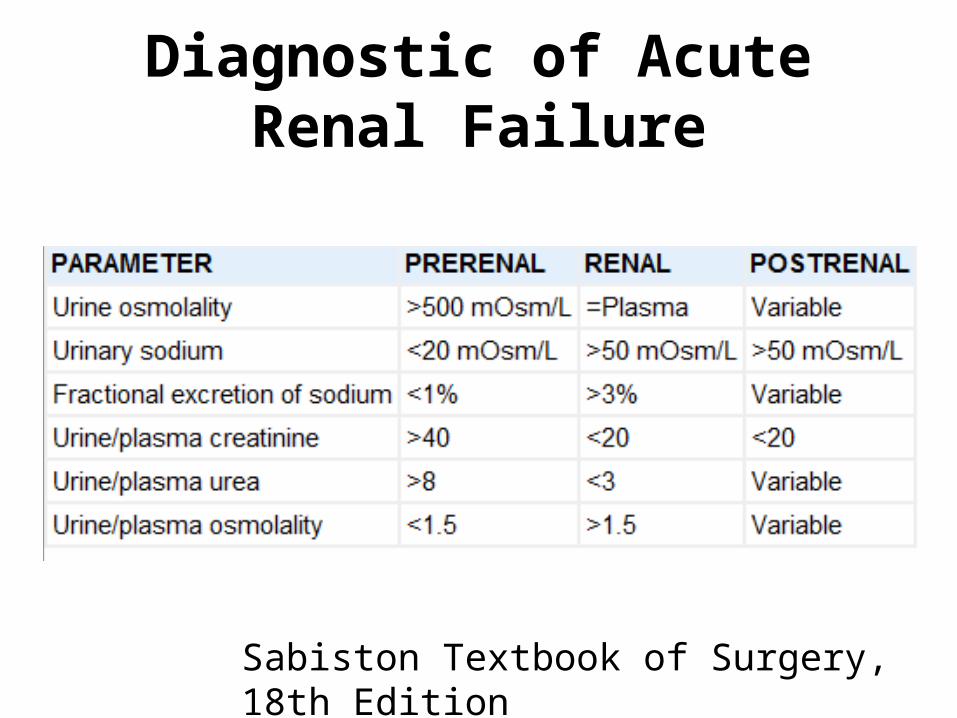
Diagnostic of Acute Renal Failure
Sabiston Textbook of Surgery, 18th Edition
Acute Renal Failure
Treatment• monitoring of fluid administration• avoidance of nephrotoxic agents• provision of adequate nutrition• management electrolyte imbalance• Hyperkalemia– insulin plus glucose– aerosolized b2-adrenergic agonist– calcium gluconate– ion exchange resin (Kayexalate)
• Hemodialysis

Indications for Hemodialysis
Sabiston Textbook of Surgery, 18th Edition
CARDIAC COMPLICATIONS

CARDIAC COMPLICATIONS
• Arterial line complications• Ischemia and Infarction• Cardiogenic Shock

Arterial line complications
Infection; thrombosis, which can lead to finger/hand necrosis; death/hemorrhage from catheter disconnection
Test Allen test or Blood gas
Allen test Measures for adequate collateral blood flowto the hand via the ulnar artery
Ischemia and Infarction
Cardiovascular Risk Leading to Myocardial Infarction
• Major Risk Factors –Unstable coronary syndromes –Decompensated heart failure –Significant arrhythmias –Severe valve disease
•Intermediate Risk Factors –Mild angina pectoris (Canadian class I or II) –Previous myocardial infarction identified by history or pathologic evidence –Q waves –Compensated or previous heart failure –Diabetes mellitus (particularly insulin dependent) –Renal insufficiency

Ischemia and Infarction
Presentation –greatest in the first 48 hours after surgery–chest pain radiating into the jaw and left arm region, is often not present. –shortness of breath–increased heart rate–Hypotension– respiratory failure. –EKG. non–Q wave, non–ST segment

Ischemia and Infarction
Lab Troponin I, cardiac isoenzymes (elevated CK-mb fraction)EKG Change
Treatment Nitrates (paste or drip), as toleratedAspirinOxygenPain control with IV morphineß-blocker, as toleratedHeparin (possibly; thrombolytics are contraindicated in the postoperative patient)ICU monitoring

Cardiogenic Shock• one of the most serious sequelae of acute MI• a highly lethal condition that results in the death
of up to 75% of patients • substantial reduction in cardiac output and
resultant hypoperfusion. • Other serious sequelae from acute MI include
CHF, arrhythmias, and thromboembolic complications.
• Presentation in hypotension and respiratory failure
Cardiogenic Shock
Management• hypotension and respiratory failure• mechanical ventilation with a high FIO2
• Pharmacological Tx.• intra-aortic balloon pumps and ventricular
assist devices • Cardiac transplantation
Related Documents











