Neurodegenerative disease April 2008

Neurodegenerative disease April 2008. Pt. 4Major categories of neurologic disease527 30Disturbances of cerebrospinal fluid and its circulation529 31Intracranial.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Neurodegenerative disease
April 2008

QuickTime™ and aTIFF (LZW) decompressor
are needed to see this picture.
Pt. 4 Major categories of neurologic disease 527
30 Disturbances of cerebrospinal fluid and its circulation 52931 Intracranial neoplasms and paraneoplastic disorders 54632 Infections of the nervous system (bacterial, fungal, spirochetal, parasitic) and sarcoidosis 59233 Viral infections of the nervous system, chronic meningitis, and prion diseases 63134 Cerebrovascular diseases 66035 Craniocerebral trauma 74736 Multiple sclerosis and allied demyelinative diseases 77137 The inherited metabolic diseases of the nervous system 79738 Developmental diseases of the nervous system 85039 Degenerative diseases of the nervous system 89540 The acquired metabolic disorders of the nervous system 95941 Diseases of the nervous system due to nutritional deficiency-98342 Alcohol and alcoholism 100443 Disorders of the nervous system due to drugs, toxins, and other chemical agents-1016

Characteristics of neurodegenerative disease
• Insidious in onset
• Progressive course
• Selective death/dysfunction of neurons
Characteristics of neurodegenerative disease
• Insidious in onset
• Progressive course
• Selective death/dysfunction of neurons
• Etiology unclear

Examples of neurodegenerative disease:
• Alzheimer’s disease
• Parkinson’s disease
• Frontotemporal dementia
• Amyotrophic lateral sclerosis (Lou Gehrig’s disease)
• Spinocerebellar ataxia
• Huntington’s disease
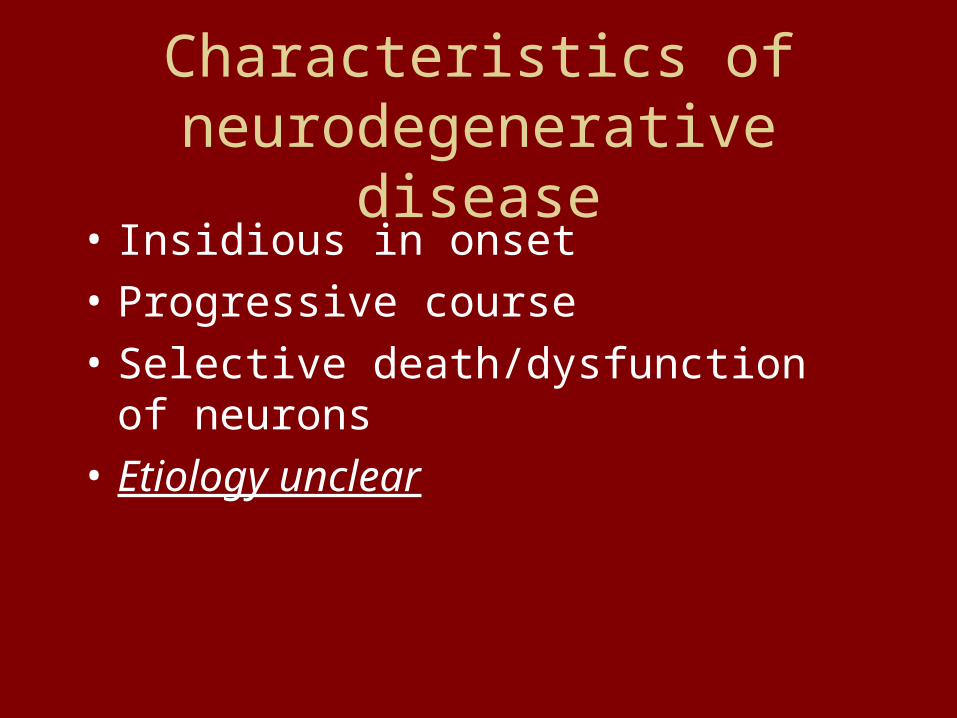
Neurodegenerative disease is common

Neurodegenerative disease prevalence:
• Alzheimer’s disease: – 1-2% age 65-75; 50% over age 85
• Parkinson’s disease– 13/100,00; 0.5-1% age 60-69; 1-3% over age 80
• Frontotemporal dementia– 1 per 10,000?
• ALS– 1-2 per 100,000 per year
• Spinocerebellar ataxias– 0.3-3 per 100,000
• Huntington’s disease– 1 in 10,000

Organization of presentation:
• Clinical presentation and diagnosis
• Pathology
• Genetic risk factors
• Environmental risk factors
• Pathogenesis (stories we tell)
• Treatments available (ie, the need for better treatments)

Alzheimer’s presentation
• Starts with memory loss--repetitive stories, repetitive questions, forgotten events, progressing to the point that ADLs are affected.
• By the time of diagnosis, a second “cognitive domain” is affected (language, spatial function, executive dysfunction)

Alzheimer’s course:
• Progressive loss of cognitive abilities and ADLs, leading ultimately to a vegetative state, and finally death (infection, malnutrition, MI, CVA)
• Average time from dx to death = 8-10 years• Rate of progression is variable• Behavior changes (psychosis, depression, apathy,
agitation) are especially variable• “If you’ve met one patient with Alzheimer’s……
you’ve met one patient with Alzheimer’s”

Alzheimer’s pathology
• Amyloid plaques
• Neurofibrillary tangles
• Neuronal death and brain atrophy
• Cholinergic projection system withers
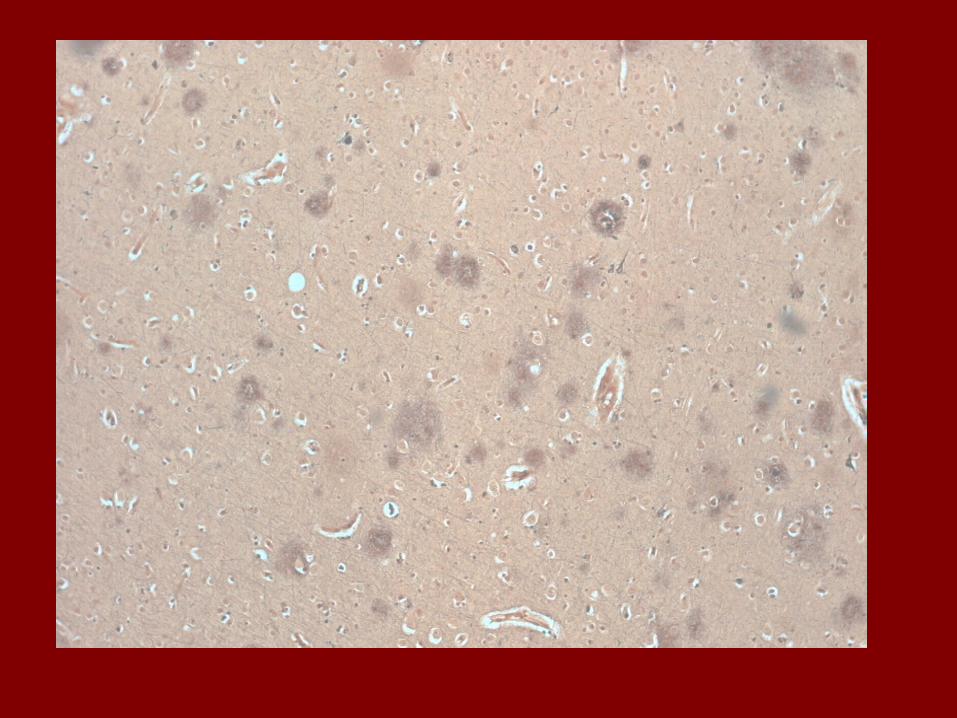

Senile plaques
• Extracellular deposits• Plaques described as “diffuse”, “neuritic”, or
“cored”• These may represent different ages of plaque• Neuritic plaques are one of the pathologic criteria
for diagnosis of Alzheimer’s disease• Composed chiefly of beta amyloid

Beta amyloid
• Beta amyloid is a 39-43 amino acid peptide• Derived from 700 amino acid amyloid
precursor protein (APP)• APP may be processed to “amyloidogenic”
or “non-amyloidogenic” pathways

-Amyloid Plaques SIGMA-ALDRICH



Neurofibrillary tangles
• Intracellular inclusion
• Chief component is hyper-phosphorylated tau
• Tau is a normal intracellular protein which stabilizes microtubules



Alzheimer’s pathology
• Amyloid plaques
• Neurofibrillary tangles
• Neuronal death and brain atrophy
• Cholinergic projection system withers
Alzheimer’s disease: genetic risk factors (autosomal dominant)
• Amyloid precursor protein
• Presenilin-1
• Presenilin-2

Alzheimer’s disease: genetic risk factors (sporadic)
• Apolipoprotein E– Alleles: E2, E3, E4– E4 is present in 15% of population– E4 is present in 45-50% of Alzheimer’s

Alzheimer’s disease: environmental risk factors
• Low educational attainment
• Head injury
• Depression
• Vascular risk factors (HTN, DM, hypercholesterolemia)

Alzheimer’s disease: stories re pathogenesis
• Braak staging (“tau hypothesis”?)
• Amyloid hypothesis
• Cholinergic hypothesis

Braak staging
• Based on the predictable spread of tangle pathology– First entorhinal cortex
– Then entorhinal cortex + hippocampus
– Then entorhinal cortex + hippocampus + association cortex

Braak staging of ADBraak 1-2 Braak 3-4 Braak 5-6
Tangle histology
Entorhinal cortex
Entorhinal + hippocampus
Entorhinal + hippocampus + cortex
Atrophy on MRI*
Same as above
Same as above
Same as above
Clinical status
Healthy aging
Isolated memory loss (“MCI”)
AD-type dementia
*(Kaye et al 1997, Silbert et al 2003)

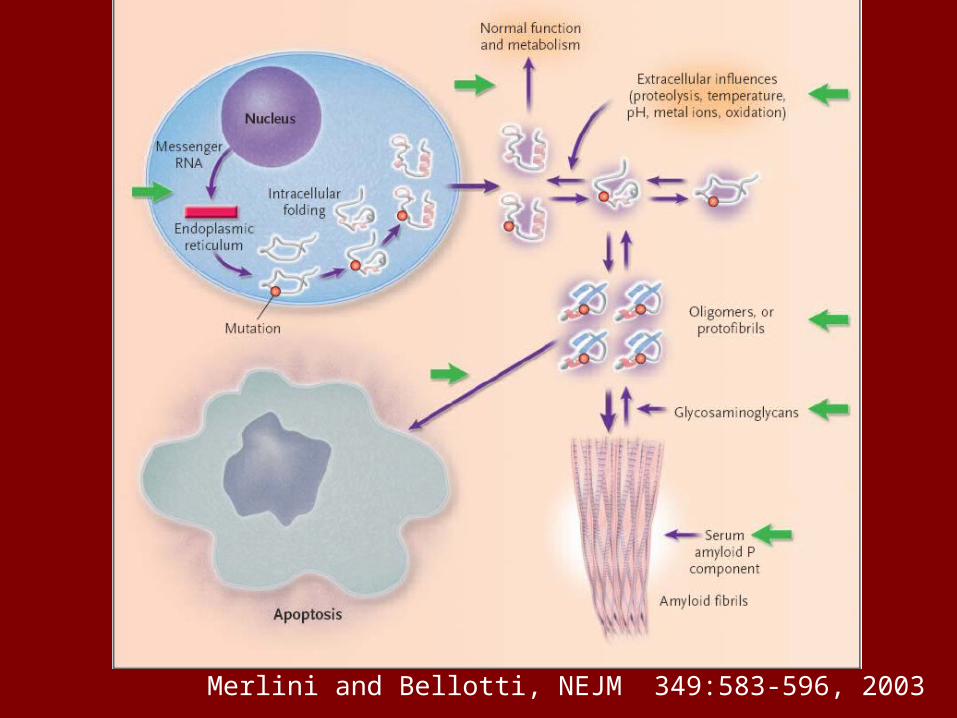
Amyloid hypothesis of AD
• Holds that neurotoxicity of beta amyloid drives the neurodegenerative process
• But: – beta amyloid is produced under physiologic
conditions--how could it be toxic?

Merlini and Bellotti, NEJM 349:583-596, 2003
Merlini and Bellotti, NEJM 349:583-596, 2003

Evaluating the amyloid hypothesis-pros and cons
• Clinicopathologic correlation
• Genetics of AD
• Cell culture studies
• Animal studies

Pathologic correlates of dementia severity (Terry, 1991)
• Amyloid plaques: poor
• Neurofibrillary tangles: better
• Neuronal loss: same as tangles
• Synaptic density: best
• So…..clin-path studies do not support the amyloid hypothesis

Evaluating the amyloid hypothesis-pros and cons
• Genetics of AD------------------pro– Autosomal dominant AD associated with
mutations in amyloid precursor protein (APP)– Trisomy 21 also associated with over-
expression of APP and AD– “presenilin” initially identified in autosomal
dominant AD, since shown to be a component of gamma secretase-- enzyme which processes APP to beta amyloid

Evaluating the amyloid hypothesis-pros and cons
• Clinicopathologic correlation--con
• Genetics of AD------------------pro
• Cell culture studies--------------pro
• Animal studies-------------------+/-

Cholinergic hypothesis of AD
• Based in part on clin-path observation of correlation between cholinergic markers and dementia severity

Other putative mechanisms:
• Inflammation
• Oxidative damage
• Ubiquitin-proteasome dysfunction
• Mitochondrial dysfunction
• Metal dyshomeostasis (copper, iron)
• Excitotoxicity
• Axonal transport dysfunction

Treatments available for AD
• Clinical trials of multiple cholinergic agents have shown enough efficacy to be FDA-approved, but none is dramatically effective
• Anti-amyloid therapies are in Phase 3 trials• Anti-tau therapies are in earlier trials• Gene therapy with NGF is also under way
targeting the cholinergic system

Parkinson’s disease-clinical
• Cardinal signs:– Tremor– Rigidity– bradykinesia– Gait impairment
Parkinson’s-clinical
• Traditionally considered purely a disorder of movement
• Now appreciated to include autonomic nervous system dysfunction (before motor impairment) and cognitive dysfunction (after motor impairment)

Parkinson’s disease pathology

Parkinson’s pathology:Lewy bodies
• Intraneuronal inclusions comprised of alpha synuclein and other proteins
• Initially thought to be confined to substantia nigra and other projection systems that deteriorate in PD
• Subsequently identified throughout the nervous system, from brainstem to cortex
• Incidental Lewy bodies seen in as many as 7-10% of asymptomatic individuals over age 60



Parkinson’s genetic risk factors
• “familial cases are on record, but the evidence is rather unsubstantial…” Adams and Victor 1985
• “Though there is no evidence to indicate a hereditary factor, a familial evidence is claimed by some.” Merritt’s Textbook of Neurology, 1984

Parkinson’s genetic risk factors

But..despite the number of genes implicated in rare sub-types of PD,Most cases of “garden-variety” PD are not explained by genes (as in AD)

Parkinson’s: environmental risk factors
• Age
• Male gender
• Rural living
• Smoking is protective

Parkinson’s pathogenesis: Braak staging suggests a progressive
“synuclein-opathy”:• Lewy bodies spread caudal-->rostral
• Stage 1-2: Lewy bodies in medulla and olfactory bulb (asymptomatic)
• Stage 3-4: Lewy bodies in substantia nigra, locus coeruleus, cholinergic basal forebrain (parkinson’s symptoms appear when >80% of nigral neurons gone))
• Stage 5-6: Lewy bodies in forebrain (dementia)

Parkinson’s pathogenesis: other models:
• MPTP model– Gives rise to selective neuronal death and
parkinsonism, but no Lewy bodies
• Rotenone model (Greenamyre)– Chronic intravenous infusion of mitochondrial
complex I inhibitor in rats– Produces selective neuronal death,
parkinsonism, and Lewy bodies

Parkinson’s treatments:
• Dopaminergic therapy has dramatic symptomatic effects
• Surgical therapies--both ablative and deep brain stimulator therapies have symptomatic effects
• Gene therapy with trophic factors is under investigation
• No proven neuroprotectant therapy to date
Frontotemporal dementia-clinical
• Presents as personality change and disinhibition, in the absence of significant memory loss
• Also may present as a primary disorder of language
• Progresses to a more generalized dementia over time
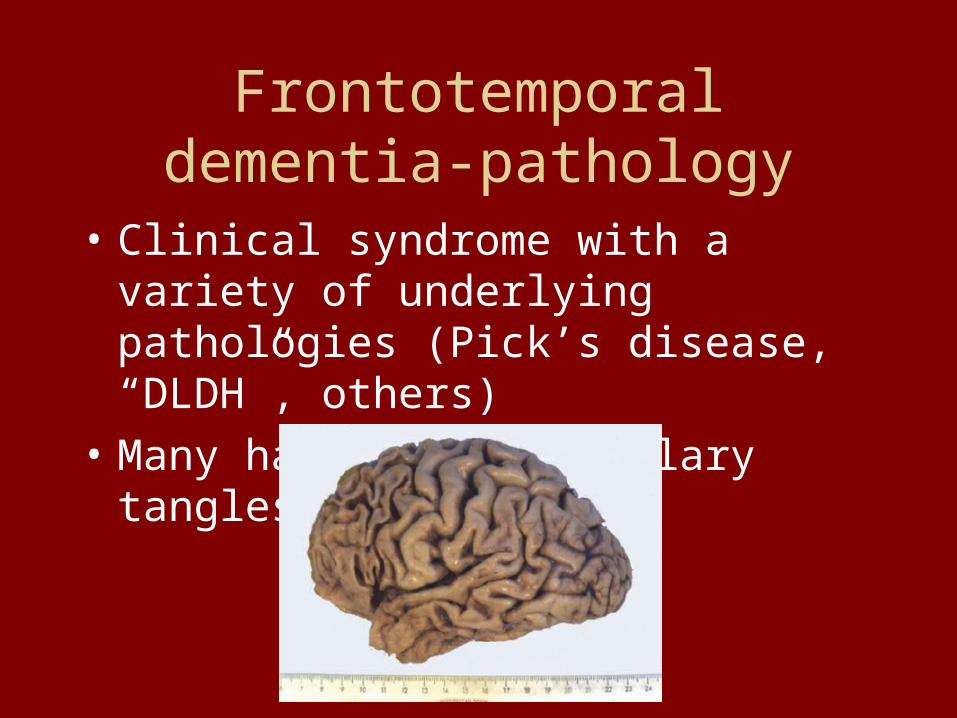
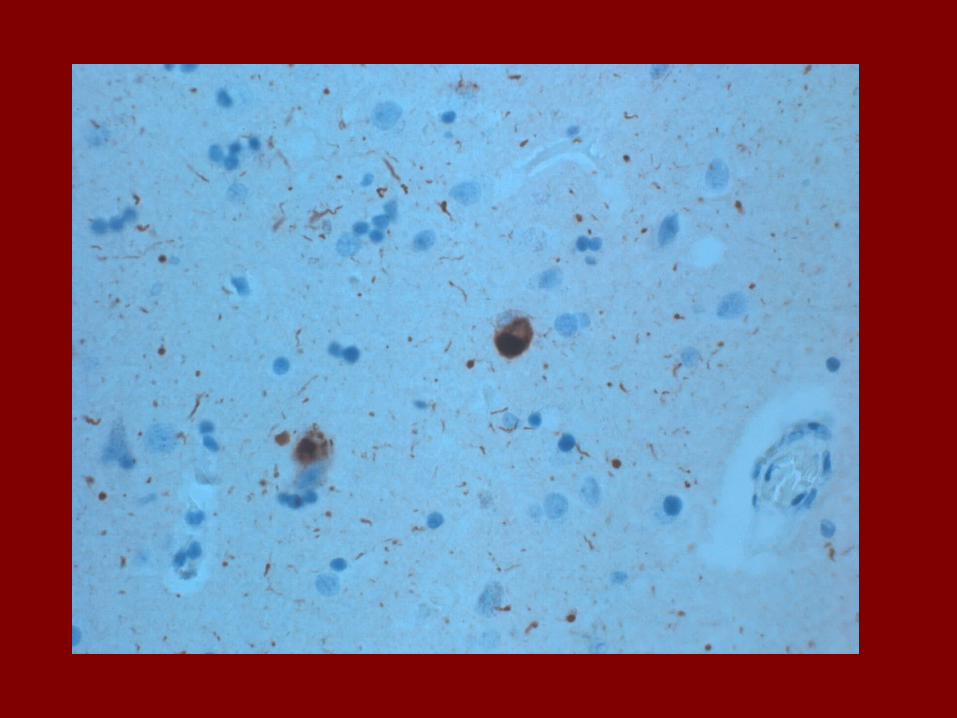
Frontotemporal dementia-pathology
• Clinical syndrome with a variety of underlying pathologies (Pick’s disease, “DLDH”, others)
• Many have neurofibrillary tangles

Frontotemporal dementia-genetics
• Most cases of FTD are sporadic• A mutation in the tau protein is a cause of FTD in
a minority of cases (FTDP=17).• Tau is a normal intracellular protein which
stabilizes microtubules.

FTD-treatment
• Nothing available

Amyotrophic lateral sclerosis-clinical
• Also known as “motor neuron disease” or “Lou Gehrig’s disease”
• Presents as slowly progressive weakness and muscle wasting.
• Death within 2-5 years in most patients due to respiratory failure
• Concomitant FTD in a sub-population of patients (subclinical neuropsych changes may be more common)

ALS-pathology

ALS-genetics
• About 10% of cases are familial
• About 2-3% are caused by mutations in Cu/Zn SOD

ALS-treatment
• Riluzole, a glutamate antagonist, prolongs survival by a few months
• Treatment trials with trophic factors have failed
• No other symptomatic or neuroprotectant therapy
• No SOD-directed therapy

Spinocerebellar ataxia-clinical
• Slowly progressive gait disorder, slurred speech, and clumsiness
• Age of onset widely variable--from early childhood to late life
• Patients look like they are intoxicated with alcohol

Spinocerebellar ataxia-pathology

Spinocerebellar ataxia-genetics(autosomal dominant)
How and why does a polyglutamine repeat in several differentproteins--give rise to a single phenotype? (there are other phenotypesassociated with other polyglutamine repeats)

Neurodegeneration-summarysigns region histology protein
AD dementia HC, ctx Plq, NFT AB, tau
PD motor S. nigra Lewy b. alphasyn
FTD dementia ctx NFT tau
ALS weakness Motor n. MN loss SOD
SCA ataxia Cb, SC Cerebel’r atrophy
many
HD Chorea, dementia
Caudate,
ctx
inclusion Hunting-tin
Unanswered questions
• How does the identification of the deranged protein in each disease explain the selective vulnerability of neurons?
• Are the mutated proteins themselves neurotoxic? Or what?
• What can we learn from transgenic mouse models? (examples: APP, tau mutants)

Questions?
Related Documents