2005;80:1327-1335 Ann Thorac Surg Hahn, Jesse Marymont and Timothy Sanborn Todd K. Rosengart, Jerry Sweet, Eileen B. Finnin, Penny Wolfe, John Cashy, Elizabeth Intervention Compared With Normal Controls Surgery or Percutaneous Coronary Intervention: Evidence of Impairment Before Neurocognitive Functioning in Patients Undergoing Coronary Artery Bypass Graft http://ats.ctsnetjournals.org/cgi/content/full/80/4/1327 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 9, 2013 ats.ctsnetjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2005;80:1327-1335 Ann Thorac SurgHahn, Jesse Marymont and Timothy Sanborn
Todd K. Rosengart, Jerry Sweet, Eileen B. Finnin, Penny Wolfe, John Cashy, Elizabeth Intervention Compared With Normal Controls
Surgery or Percutaneous Coronary Intervention: Evidence of Impairment Before Neurocognitive Functioning in Patients Undergoing Coronary Artery Bypass Graft
http://ats.ctsnetjournals.org/cgi/content/full/80/4/1327located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 9, 2013 ats.ctsnetjournals.orgDownloaded from
NCPINTJTEI
ocwnl
ktocgab
ww
Cmdaanao
tpcCb
A
PS
AE
©P
CA
RD
IOV
AS
CU
LA
R
eurocognitive Functioning in Patients Undergoingoronary Artery Bypass Graft Surgery orercutaneous Coronary Intervention: Evidence ofmpairment Before Intervention Compared Withormal Controls
odd K. Rosengart, MD, Jerry Sweet, MD, Eileen B. Finnin, RN, Penny Wolfe, PhD,ohn Cashy, PhD, Elizabeth Hahn, MA, Jesse Marymont, MD, andimothy Sanborn, MD
vanston Northwestern Healthcare, Evanston, Illinois, and Feinberg School of Medicine of Northwestern University, Chicago,
llinoisdwc4impms2
bptw
Background. Cognitive deficits have been reported toccur in a significant proportion of patients undergoingoronary artery bypass grafting (CABG), but the extent tohich these deficits were preexistent or related to theatural history of cognitive decline in this patient popu-
ation remains poorly defined.Methods. After excluding patients with conditions
nown to cause brain dysfunction (eg, hepatic dysfunc-ion, stroke), a group of patients referred for percutane-us coronary intervention (PCI) or CABG (n � 82) wasompared with an age- and education-matched controlroup that did not have clinical evidence of coronaryrtery disease (n � 41). These subjects underwent aattery of neurocognitive and emotional testing.Results. Test score means for 5 of 14 different measuresere significantly greater (impaired) in cardiac compared
ith control group subjects. Of cardiac subjects, 20%pcepatd
icttdcocwprr
ddress reprint requests to Dr Rosengart, 2650 Ridge Ave, Burch 100,vanston, IL 60201; e-mail: [email protected].
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
emonstrated clinical impairment (test result > 1 SDorse than mean for normative standards) in 6 of 14 tests,
ompared with 10% of the controls. By clinical standards,6% of cardiac subjects would be considered to bempaired (score 1 SD or more below the control group
ean) on 3 or more neuropsychologic measures, com-ared with 29% of the controls. By this (control groupean) standard, cardiac subjects demonstrated impaired
cores on 3.06 � 2.6 tests compared with impairment in.0 � 2.35 tests for the control group (p � 0.01).
Conclusions. Even excluding patients at high risk forrain dysfunction, cognitive impairment is found inatients with coronary artery disease before interven-
ional therapy. Baseline impairment must be consideredhen evaluating outcomes after intervention.
(Ann Thorac Surg 2005;80:1327–35)
© 2005 by The Society of Thoracic Surgeonsognitive deficits have recently been reported to beanifest in more than 50% of patients at the time of
ischarge after coronary artery bypass grafting (CABG),nd to persist in more than 40% of these patients as longs 5 years later [1]. Aside from its effect on quality of life,eurocognitive decline has been associated with as muchs a 10% increase in hospital mortality, increased lengthsf stay, and prolonged, expensive rehabilitation [2].Use of the heart-lung machine and manipulations of
he aorta associated with the performance of cardio-ulmonary bypass have most frequently been impli-ated as the source of neurocognitive decline afterABG [3, 4].Cerebral microemboli induced by pertur-ation of the atherosclerotic aorta and cerebral hypo-
ccepted for publication June 17, 2005.
resented at the Forty-first Annual Meeting of The Society of Thoracicurgeons, Tampa, FL, Jan 24–26, 2005.
erfusion have, more specifically, been cited as keyontributors to this complication. As a consequence,ither the performance of off-pump CABG (OPCABG)rocedures or percutaneous interventions have beendvocated as alternatives to on-pump CABG to avoidhe potentially devastating sequelae of neurocognitiveecline after this procedure.The great majority of post-CABG neurocognitive stud-
es have consisted of longitudinal evaluations of surgicalohorts without non-CABG controls. As a consequence,he occurrence of neurocognitive decline as a function ofhe typically advanced age of these patients, or in accor-ance with the natural history of systemic (cerebrovas-ular) atherosclerotic disease was not addressed in manyf these reports. Further, because of the lack of “normal”ontrols in these studies, it has been difficult to determinehat percentage of CABG patients are cognitively im-aired at baseline, and are thus potentially at increasedisk for further decline because of impaired cognitive
eserve [1, 5].0003-4975/05/$30.00doi:10.1016/j.athoracsur.2005.06.052
by on June 9, 2013 als.org

wCanoAteawtstc
P
EIFos(sccssgdtoalatsppeg
2ocpSbs
ppsnsarcHpl
IAwg2mctbwcenP
itbwc
TP
RH
R
LSFET
Cs
Ta
ASH
BO
a
i
C
1328 ROSENGART ET AL Ann Thorac SurgNEUROCOGNITIVE FUNCTION IN CABG AND PCI 2005;80:1327–35
CA
RD
IOV
AS
CU
LA
R
As a consequence of these limitations in the literature,e compared a cohort of patients undergoing electiveABG at our institution with a matched population oftherosclerotic patients undergoing percutaneous coro-ary intervention (PCI), and another matched populationf patients with no known history of coronary disease.nalysis of the baseline data in this study demonstrated
hat (CABG and PCI) patients with coronary artery dis-ase demonstrated cognitive impairment compared withnonatherosclerotic control population and as comparedith normative test standards. These findings suggest
hat cognitive deficiencies reported after CABG in priortudies may have, in part, either been present preopera-ively, or may have been precipitated by preexistentognitive disease [1, 5].
atients and Methods
nrollmentnstitutional Review Board approval was obtained inebruary 2002, and fully informed written consent wasbtained from patients selected for participation in thistudy. Prospective participants in the two cardiac groupsCABG or PCI) were screened by project personnelubsequent to physician referral based upon standardlinical indications for either CABG or PCI. Exclusionriteria for cardiac patients were as follows: a history oftroke or symptomatic carotid artery disease, dementia,ubstance abuse, renal dysfunction (blood urea nitrogenreater than 50 mg/dL, creatinine greater than 2.5 mg/L), or hepatic dysfunction (serum glutamic-oxaloacetic
ransaminase [SGOT]/aspartate aminotransferase [AST]r serum glutamic-pyruvic transaminase [SGPT]/alanineminotransferase [ALT] more than three times upperimits of normal), language or physical deficiency notllowing test completion, participation in another clinicalrial of an investigational device or drug, or other factorsuggesting the potential inability to successfully com-lete neurocognitive assessments before PCI or isolated,rimary CABG procedure on technical grounds (namely,mergency surgery, prior CABG, concomitant heart sur-
able 1. Reasons for Exclusions Among Potential Studyarticipants
Reason CABG (%) PCI (%) Control (%)
efused 27 (20) 188 (40) 2 (5)istory of neurologicproblems
19 (14) 96 (21) 0
enal failure/emergent/unstable
22 (16) 87 (19) 0
anguage barrier 15 (11) 34 (6) 0ubstance abuse 9 (7) 21 (5) 0ailure on MMSE 1 (1) 1 (0) 0nrolled 41 (31) 41 (9) 41 (95)otal screened 134 (100) 468 (100) 43 (100)
ABG � coronary artery bypass graft surgery; MMSE � mini-mentaltatus examination; PCI � percutaneous coronary intervention.
ery, left ventricular thrombus, ejection fraction less thanaP
ats.ctsnetjournDownloaded from
5%, intra-aortic balloon pump, or extensively calcifiedr atherosclerotic aorta without an appropriate site forannulation). Additionally, upon enrollment, all partici-ants were screened for dementia using the Mini-Mentaltatus Examination (MMSE) [6]. Patients who scoredelow 24 were excluded from further involvement in thetudy.
The reasons and associated frequencies of exclusion ofatients from a total screened population of 645 areresented in Table 1. The cardiac patients enrolled in thetudy represent patients with low risk of preinterventioneurological dysfunction. A second cohort of controlubjects free of cardiac and neurologic disease by historynd demographically similar to the cardiac patients wereecruited from the community. Demographics of theontrols and cardiac patients are presented in Table 2.istory and physical data were obtained relevant toreoperative risk parameters, as determined by existing
iterature, and are presented in Table 3.
ntergroup Conformityge was well matched between groups, and each groupas relatively well educated, with well over half of eachroup having a college degree or advanced degree (Table). There were more men than women in each group, andore women in the control group compared with the
ardiac groups, reflective of the normally occurring dis-ribution of sex in these populations. Patterns of comor-idities in the CABG and PCI subjects were consistentith extent of atherosclerotic disease in these groups as
ompared with relatively limited evidence of such dis-ase in the control group (Table 3). The MMSE scores didot differ significantly across groups: control 28.5 � 1.6;CI 28.4 � 1.7; CABG 28.3 � 1.5.Because general intelligence, as represented in an
ntelligence quotient (IQ), is well known to be correlatedo most neuropsychologic measures, two regression-ased measures of premorbid intellectual functioningere used to determine the need for possible statistical
orrection of any differences between groups in IQ. The
able 2. Demographics and Estimated Intellectual Functiont Time of Enrollment
Variable Control PCI CABG
ge 65 � 10 66 � 9 66 � 11ex (% female) 43 19 18ighest educational level (%)High school or GED 12 13 21Associate/technical degree 23 27 25College degree 36 38 29Advanced degreea 25 22 25
aronab IQ estimate 111 � 6 115 � 5 112 � 6PIE IQ estimate 113 � 7 114 � 7 112 � 7
Advanced degree (MA, MS, MBA, PhD, MD, JD). b Controls signif-cantly lower than PCI on Barona IQ estimate (p � 0.05).
ABG � coronary artery bypass graft surgery; GED � grade equiv-
lency diploma; OPIE � Oklahoma Premorbid Intelligence Estimate;CI � percutaneous coronary intervention.by on June 9, 2013 als.org
fitgswmtlAlwswgstscp
NAmuqmbcosaa
cmwtpAScMmmISBpvitg
SAtNwPdgct
T
S
C
C orona
1329Ann Thorac Surg ROSENGART ET AL2005;80:1327–35 NEUROCOGNITIVE FUNCTION IN CABG AND PCI
CA
RD
IOV
AS
CU
LA
R
rst of these, the Oklahoma Premorbid Intelligence Es-imate (OPIE) [7] includes the Wechsler Adult Intelli-ence Scale-revised vocabulary and picture completionubtests and demographic information as predictors,hereas the second, referred to as the Barona [8] for-ula, relies solely upon demographic information. Both
he OPIE and the Barona indicated above average intel-ectual functioning in the enrolled subjects (Table 2).lthough the controls were only a few mean IQ points
ower on the Barona IQ estimate at baseline comparedith the PCI group, this difference was found to be
ignificant. The Barona IQ estimate for the control groupas not, however, significantly lower than the CABGroup. Also, the OPIE IQ estimate, which includes con-ideration of actual intellectual performances on formalesting in addition to demographic variables, was notignificantly different between groups. Thus, we con-luded that no meaningful intellectual differences wereresent between groups.
eurocognitive Testing Batteryll consenting healthy CABG, PCI, and control patientseeting the inclusion/exclusion criteria described above
nderwent neurocognitive testing and a set of self-reportuestionnaires. The neurocognitive test battery was ad-inistered by experienced psychometricians who had
een trained under the supervision of a board-certifiedlinical neuropsychologist. Each study subject was testedn all occasions by the same psychometrician. Testingessions were held in an environment that was comfort-ble, well lit, and generally free from extraneous visual
able 3. Comorbidities in Subject Populations at Baseline
ystemic comorbiditiesDiabetes mellitusPeripheral vascular diseaseHypertensionObesityHypercholesterolemiaChronic obstructive pulmonary diseasePrior myocardial infarction
ardiovascular variablesAspirin useNew York Heart Association classification
1234
Canadian Cardiovascular Society angina classification1234
ABG � coronary artery bypass graft surgery; PCI � percutaneous c
nd auditory distractions. d
ats.ctsnetjournDownloaded from
The test battery required approximately 1 hour toomplete and can be represented in the following do-ains: immediate attention span: digit span forward;orking memory: digit span backward; fine motor dex-
erity: grooved pegs (dominant and nondominant hands);sychomotor speed: digit symbol from the Wechslerdult Intelligence Scale, third edition, Trail-Making A,troop color-word test (word and color pages); language:ontrolled oral word association and visual naming of the
ultilingual Aphasia Examination; verbal learning andemory: Hopkins Verbal Learning Test; nonverbalemory: digit symbol recall from the Wechsler Adult
ntelligence Scale, third edition; and executive function:troop color-word test (color-word page), Trail-Making. Additionally, all participants completed the Beck De-ression Inventory-II (BDI-II) and the Beck Anxiety In-entory (BAI). Time intervals from baseline testing tonitiation of cardiac intervention were comparable be-ween the patient groups, with medians of 1 day for eachroup.
tatistical Analysisll statistical analyses were conducted by statisticians at
he Center for Research and Education at Evanstonorthwestern Healthcare. Analysis of variance (ANOVA)as used to compare IQ among the three groups (CABG,CI, control). Student’s t test was used to compareifferences in mean scores between cardiac and controlroups. Impairment was defined in comparison withontrol group means (score � 1 SD below [worse than]he control group mean) and to normative standards
Control (%) PCI (%) CABG (%)
9 19 210 10 11
32 61 7118 42 5235 55 713 7 180 42 18
44 63 68
89 29 298 52 253 19 320 0 14
97 37 213 43 320 17 210 3 25
ry intervention.
efined for each neurocognitive test (test result � 1 SD
by on June 9, 2013 als.org
btbcpv
R
Tdacswc75ettt
innct
dtgvopatpTewicc
T
W
W
G
G
M
T
T
S
S
S
M
H
H
H
a
Ht
1330 ROSENGART ET AL Ann Thorac SurgNEUROCOGNITIVE FUNCTION IN CABG AND PCI 2005;80:1327–35
CA
RD
IOV
AS
CU
LA
R
elow normative standards). The Wilcoxon signed rankest was used to compare the number of impairmentsetween groups, and Fisher’s exact test was used toompare the percentage of impaired. All results areresented as mean � SD. Significance was defined as a palue of less than 0.05.
esults
he CABG and PCI subjects were similar in terms ofemographics and baseline intellectual function (Table 2)s well as comorbidities (Table 3) as compared withontrols. Scores for the BAI (anxiety) and BDI-II (depres-ion) assessments were well within the normal range, butere somewhat higher for the CABG and PCI groups
ompared with controls: BAI control 4.4 � 6.1, PCI 7.6 �.8, and CABG 7.1 � 6.8 (p � 0.01); BDI-II control 4.4 �.7, PCI 5.2 � 4.1, and CABG 8.0 � 7.8 (p � 0.047). Toxamine possible relationships of depression and anxietyo neurocognitive outcome measures, relationships be-ween BAI and BDI-II scores and the neurocognitiveesting battery were performed. Of the dozens of result-
able 4. Mean Scores at Baseline, by Groupa
Variable
AIS III, digit symbol (scaled score)
AIS III, digit span (scaled score)
rooved pegboard dominant hand (t score)
rooved pegboard nondominant hand (t score)
AE, controlled oral word association total correct (percentile)
rail-making test, part A (t score)
rail-making test, part B (t score)
troop, Word (t score)
troop, color (t score)
troop, color-word (t score)
AE, visual naming (percentile)
VLT-R total recall (total correct responses for trials 1, 2, and 3
VLT-R delayed recall (trial 4; t score)
VLT-R recognition discrimination index (t score)
For all tests in above Table, higher scores are consistent with better pe
VLT-R � Hopkins Verbal Learning Test-Revised; MAE � Multilingual Ahird edition.
ats.ctsnetjournDownloaded from
ng correlations, only BAI with grooved pegs, nondomi-ant hand, at baseline was statistically significant (dataot shown). These correlations were small in size, ac-ounting for less than 5% of the variance between affec-ive state and fine motor dexterity.
Proportions of patients in the CABG and PCI groupsemonstrating impairment in each of the 14 neurocogni-
ive instruments were also compared using both controlroup means and normative standards criteria for indi-idual tests to define impairment. With the exception ofne instrument (grooved pegboard, dominant hand), theroportions impaired in the CABG and PCI groups werepproximately equal and not statistically significant, andhere was no apparent tendency for the proportion im-aired in CABG to be higher or lower than in PCI.herefore, and also because our initial goal was tovaluate baseline neurocognitive function associatedith clinically meaningful cardiac disease, rather than an
ntention to treat with a particular intervention, the twoardiac disease groups were combined (n � 82) andompared both to the normal control sample (n � 41) and
Group Mean SD Pr � [t]
Control 12.0 2.7 0.01Cardiac 10.7 2.8Control 11.1 3.0 0.5Cardiac 11.5 3.3Control 41.1 14.6 0.3Cardiac 38.7 11.6Control 40.8 12.3 0.8Cardiac 40.2 9.2Control 61.9 26.6 0.003Cardiac 45.4 27.9Control 48.8 13.2 0.7Cardiac 47.8 9.8Control 49.2 10.5 0.3Cardiac 47.0 10.0Control 48.7 10.3 0.4Cardiac 50.5 10.4Control 49.5 10.0 0.6Cardiac 48.4 10.8Control 53.0 10.9 0.4Cardiac 51.2 10.1Control 65.0 23.2 0.3Cardiac 59.5 26.4
ore) Control 47.7 10.7 0.038Cardiac 43.7 9.1Control 47.8 10.5 0.025Cardiac 43.2 10.4Control 47.9 9.9 0.037Cardiac 43.5 11.2
ance.
; t sc
rform
phasia Examination; WAIS-III � Wechsler Adult Intelligence Scale,
by on June 9, 2013 als.org

to
ITsc4ImViflE
gf�vr
icmdgttoag
tcttct4m
T
W
W
G
G
M
T
T
S
S
S
M
H
H
H
a
a
H ual At
1331Ann Thorac Surg ROSENGART ET AL2005;80:1327–35 NEUROCOGNITIVE FUNCTION IN CABG AND PCI
CA
RD
IOV
AS
CU
LA
R
o normative standards for each of the tests included inur neurocognitive testing battery.
ntergroup Differences in Neurocognitive Functionest score means for 5 of 14 different measures wereignificantly greater (more impaired) in cardiac subjectsompared with control group subjects at baseline (Table). These five measures included the Wechsler Adultntelligence Scale, third edition, digit symbol (nonverbal
emory deficit), the three components of the Hopkinserbal Learning Test (verbal learning and memory def-
cit), and the controlled oral word association (verbaluency) component of the Multilingual Aphasiaxamination.Examination of individual test scores, as opposed to
roup means, demonstrated that impairment was morerequently identified utilizing control group means (score
1 SD below [worse than] the control group mean)ersus normative standards for individual tests (test
able 5. Percentages of Subjects Considered Neurocognitively
AIS III, digit symbol (scaled score)
AIS III, digit span (scaled score)
rooved pegboard dominant hand (t score)
rooved pegboard nondominant hand (t score)
AE, controlled oral word association total correct (percentile)
rail-making test, part A (t score)
rail-making test, part B (t score)
troop, word (t score)
troop, color (t score)
troop, color-word (t score)
AE, visual naming (percentile)
VLT-R total recall (total correct responses for trials 1, 2, and 3t score)
VLT-R delayed recall (trial 4; t score)
VLT-R recognition discrimination index
Clinical standards refers to the common normative standard suggesbnormality. b Chi-square test statistically significant.
VLT-R � Hopkins Verbal Learning Test-Revised; MAE � Multilinghird edition.
esult � 1 SD below normative standards) to define t
ats.ctsnetjournDownloaded from
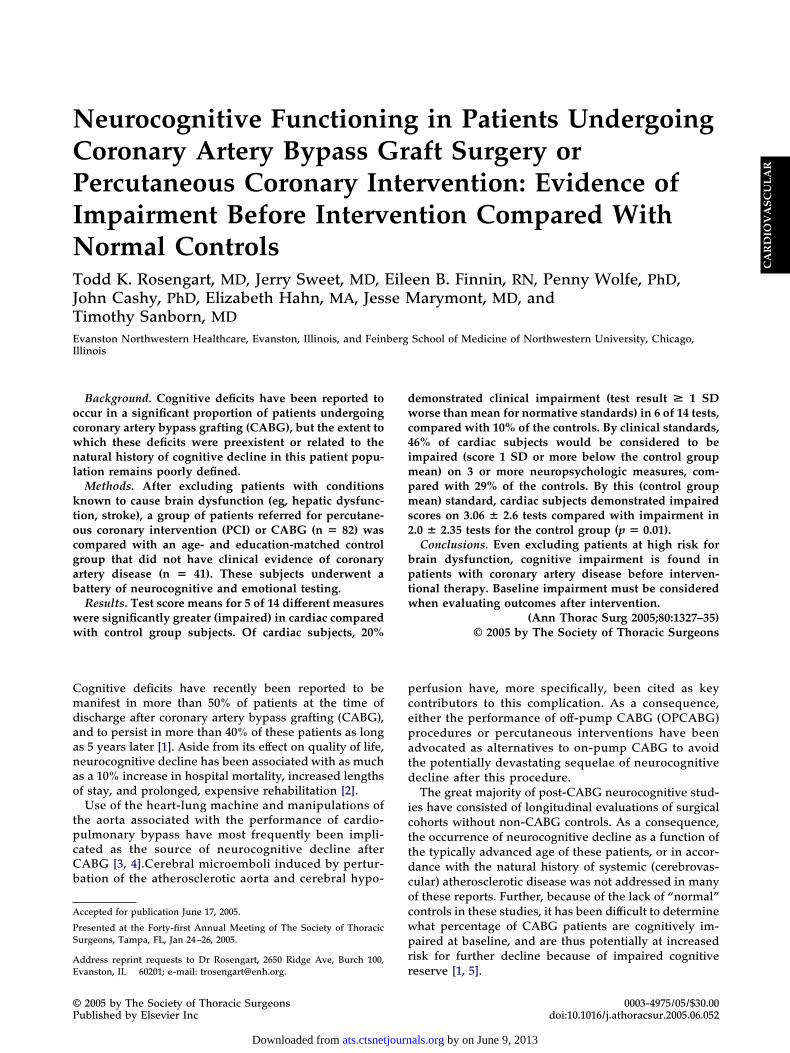
mpairment (Table 5). By this analysis, at least 10% moreardiac versus control subjects demonstrated impair-ent in five tests when using normative standards to
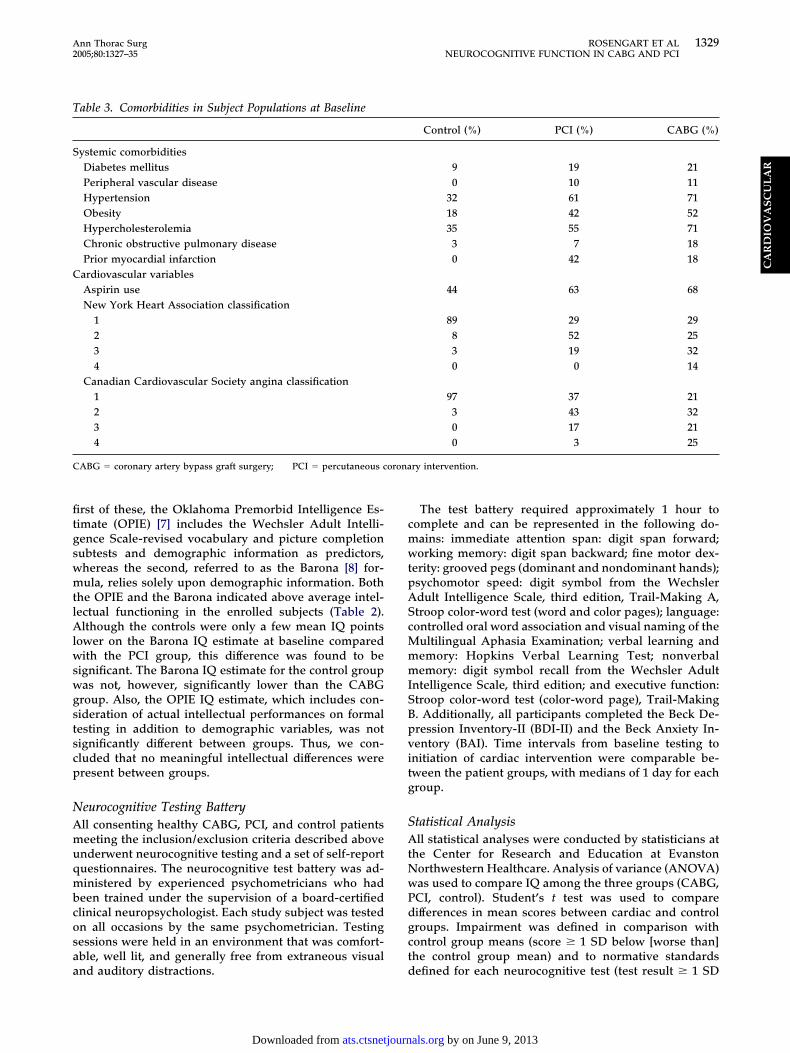
efine impairment (Fig 1), and in six tests when controlroup means was used to define impairment (Fig 2). Inhe most divergent test performances, approximatelyhree times more cardiac than control participants dem-nstrated impaired performance on controlled oral wordssociation and digit symbol when utilizing a controlroup mean definition of impairment.The breadth of impairment in patients was reflected by
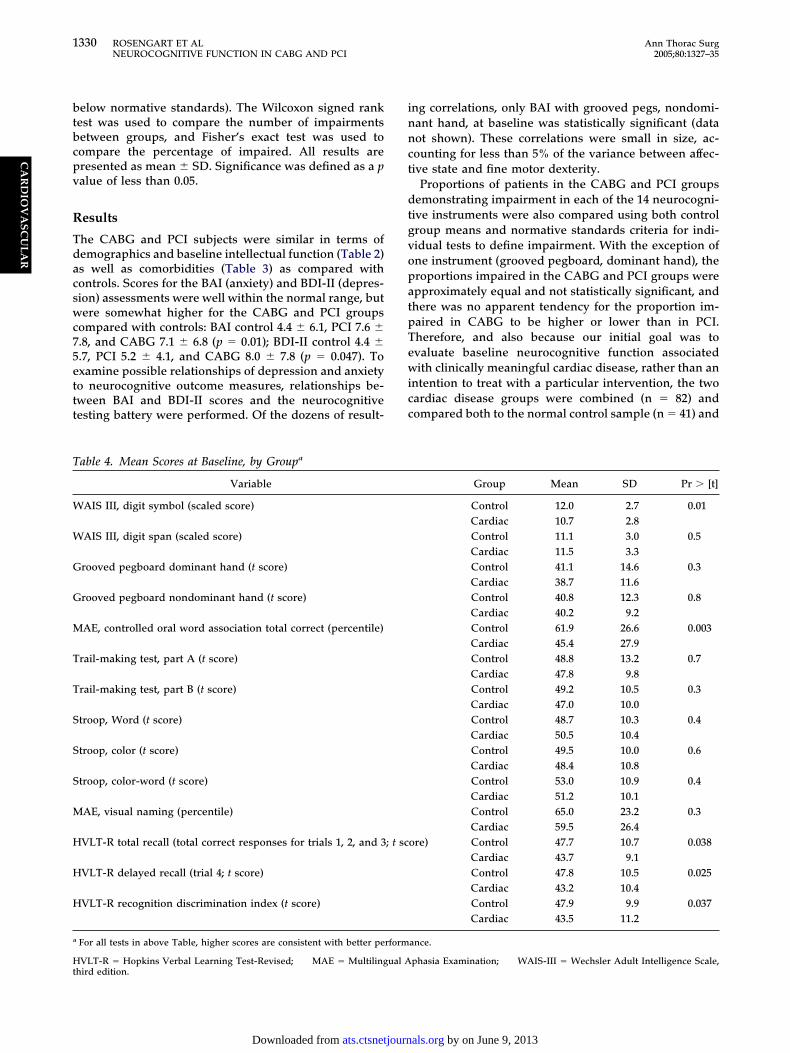
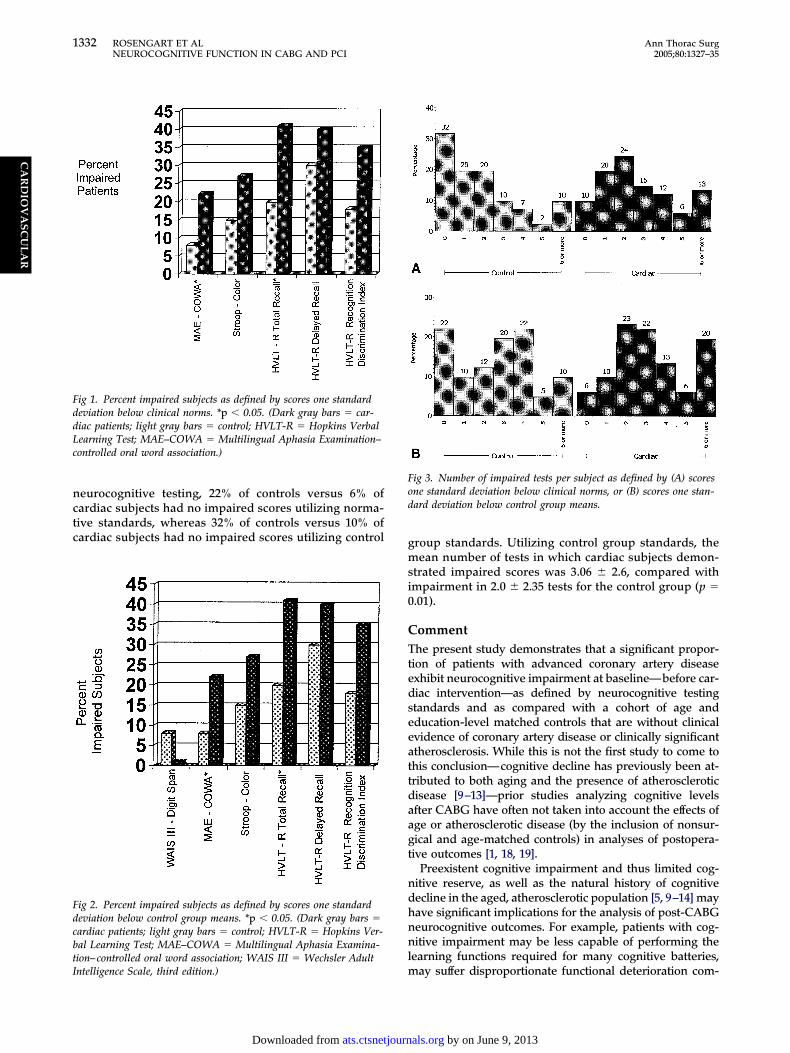
he finding that 20% of cardiac subjects, versus 10% of theontrols, demonstrated clinical impairment in 6 of the 14ests in our neuropsychologic battery utilizing a norma-ive standards definition of impairment (Fig 3A). If dis-repancy from control group means rather than norma-ive standards are used to define cognitive impairment,6% of cardiac subjects demonstrated impairment on 3 orore neuropsychologic measures, compared with 29% of
aired at Baseline
As Defined byClinical Standardsa
As Defined by OneSD or More Below
Control Group Mean
Control 5% 13%Cardiac 6% 37%b
Control 8% 13%Cardiac 1% 18%Control 56% 15%Cardiac 57% 18%Control 51% 12%Cardiac 52% 10%Control 8% 15%Cardiac 22% 42%b
Control 22% 12%Cardiac 22% 10%Control 20% 15%Cardiac 19% 15%Control 20% 13%Cardiac 19% 15%Control 15% 13%Cardiac 27% 23%Control 13% 18%Cardiac 19% 23%Control 3% 23%Cardiac 10% 27%Control 20% 13%
Cardiac 41%b 23%Control 30% 18%Cardiac 40% 32%Control 18% 18%Cardiac 35% 33%
the manual of test as the beginning point of clinically meaningful
phasia Examination; WAIS-III � Wechsler Adult Intelligence Scale,
Imp
;
ted in
he controls (Fig 3B). At the normal end of the range of
by on June 9, 2013 als.org
nctc g
msi0
CTtedseeattdaagt
ndhnnl
FddLc
FdcbtI
Fod
1332 ROSENGART ET AL Ann Thorac SurgNEUROCOGNITIVE FUNCTION IN CABG AND PCI 2005;80:1327–35
CA
RD
IOV
AS
CU
LA
R
eurocognitive testing, 22% of controls versus 6% ofardiac subjects had no impaired scores utilizing norma-ive standards, whereas 32% of controls versus 10% ofardiac subjects had no impaired scores utilizing control
ig 1. Percent impaired subjects as defined by scores one standardeviation below clinical norms. *p � 0.05. (Dark gray bars � car-iac patients; light gray bars � control; HVLT-R � Hopkins Verbalearning Test; MAE–COWA � Multilingual Aphasia Examination–ontrolled oral word association.)
ig 2. Percent impaired subjects as defined by scores one standardeviation below control group means. *p � 0.05. (Dark gray bars �ardiac patients; light gray bars � control; HVLT-R � Hopkins Ver-al Learning Test; MAE–COWA � Multilingual Aphasia Examina-ion–controlled oral word association; WAIS III � Wechsler Adult
mntelligence Scale, third edition.)
ats.ctsnetjournDownloaded from
roup standards. Utilizing control group standards, theean number of tests in which cardiac subjects demon-
trated impaired scores was 3.06 � 2.6, compared withmpairment in 2.0 � 2.35 tests for the control group (p �.01).
ommenthe present study demonstrates that a significant propor-
ion of patients with advanced coronary artery diseasexhibit neurocognitive impairment at baseline—before car-iac intervention—as defined by neurocognitive testingtandards and as compared with a cohort of age andducation-level matched controls that are without clinicalvidence of coronary artery disease or clinically significanttherosclerosis. While this is not the first study to come tohis conclusion—cognitive decline has previously been at-ributed to both aging and the presence of atheroscleroticisease [9–13]—prior studies analyzing cognitive levelsfter CABG have often not taken into account the effects ofge or atherosclerotic disease (by the inclusion of nonsur-ical and age-matched controls) in analyses of postopera-ive outcomes [1, 18, 19].
Preexistent cognitive impairment and thus limited cog-itive reserve, as well as the natural history of cognitiveecline in the aged, atherosclerotic population [5, 9–14] mayave significant implications for the analysis of post-CABGeurocognitive outcomes. For example, patients with cog-itive impairment may be less capable of performing the
earning functions required for many cognitive batteries,
ig 3. Number of impaired tests per subject as defined by (A) scoresne standard deviation below clinical norms, or (B) scores one stan-ard deviation below control group means.
ay suffer disproportionate functional deterioration com-
by on June 9, 2013 als.org

pompplcpctlr
lpndnsac(isstsacp
ofptdpdttrnnanr
pclRmcwtpstls
acifaaCwsopsChi
CTidagepca1gtittbbtfTbft
twmddiolp“porsti
1333Ann Thorac Surg ROSENGART ET AL2005;80:1327–35 NEUROCOGNITIVE FUNCTION IN CABG AND PCI
CA
RD
IOV
AS
CU
LA
R
ared with more intact patients if intraoperative injury doesccur because of their possession of relatively limited re-aining cognitive skills or resources, or may demonstrate
ostoperativedysfunction as a result of predictable naturalatterns of cognitive decline in an aged or impaired popu-
ation [13]. In this regard, it is important to consider that theognitive dysfunction we have demonstrated in cardiacatients at baseline has also been supported by evidence oferebrovascular disease in preoperative CABG patients—he demonstration of multiple, preexisting cerebrovascularesions (moderate to severe infarcts) on brain magneticesonance imaging scan [15].
Moreover, it is important to consider that these base-ine impairments in many cases are not trivial, andotentially reflect a serious compromise not just in cog-itive test taking, but also in day-to-day functioning,espite the fact that these patients appeared to functionormally by casual observation and by preenrollmentcreening parameters specifically designed to detect suchbnormalities in the present study. By example, someardiac subjects demonstrated a fivefold prolongationdeterioration) compared with control means in perform-ng the digit symbol test included in the current study,uch that these subjects took five times as long to copy aeries of symbols over 2 minutes—in some cases, morehan 10 seconds per symbol compared with a norm of 2econds. Such degree of functional impairment, seen inpproximately 20% the cardiac group versus 5% of theontrol group, would likely translate into profound im-airments in normal daily functionality.Given these considerations, it is striking that while a few
f the many prior published studies of neurocognitiveunction in CABG patients have commented on baselinearameters, almost none have provided comparisons be-
ween CABG patients versus nonsurgical coronary arteryisease (CAD) patients and non-CAD patients. For exam-le, Zimpfer and colleagues [16] found no preoperativeifferences in neurocognitive function between CABG pa-
ients and age- and sex-matched nonsurgical controls, buthe CAD status of the control group was not defined in thiseport.16 Similarly, while Selnes and coworkers [17] foundo baseline differences between CABG patients and aonsurgical CAD control group, this study did not includenon-CAD group, and thus does not provide insight into
eurocognitive impairment as a function of CAD in thiselatively aged population.
Two randomized studies of CABG versus OPCABatients utilizing normative standards to define neuro-ognitive function demonstrated impairments at base-ine, which were consistent with our own findings.ankin and coworkers [18] noted impairment in verbalemory and perceptuo-motor speed, while Van Dijk and
olleagues [19] demonstrated impairment in verbal andorking memory scores and visuo-spatial and informa-
ion processing speeds. These studies did not, however,rovide insight into the extent that these findings repre-ented impairments compared with age-matched con-rols without coronary disease, nor the extent to whichongitudinal changes in their patients were the result of
urgery versus disease state. nats.ctsnetjournDownloaded from
Similar to the present study, Vingerhoets and associ-tes [20] demonstrated that CAD patients were signifi-antly impaired in comparison with non-CAD controls,n 5 of 12 tests encompassing verbal memory, executiveunction, and motor speed.20 Keith and coworkers [21]lso demonstrated learning defects and impairments inuditory memory in the CABG compared with the non-AD control patients.21 The conclusion of these studiesas that the extent of cardiovascular disease was a
ignificant risk factor for neurocognitive decline. The lackf nonsurgical CAD controls in these studies, however,revents specific conclusions in these studies as to thepecific effects of CABG (as opposed to the effects ofAD) on cognitive decline. Although still other studiesave included non-CABG controls, data on baseline
mpairment were not included in these reports [22, 23].
onclusions and Limitationshe present data provide substantial evidence of cognitive
mpairment, even at baseline, in patients undergoing car-iac interventions as compared with normative and age-nd education-matched standards. Although our controlroup was not matched for sex, this would not have beenxpected to artifactually influence the measures within ourarticular neuropsychologic test battery [24]. However, be-ause men and women develop heart disease at differentges, relationships between sex and outcomes of each of the4 neurocognitive tests were examined for each of the threeroups in order to explore the possibility that dispropor-ionate sex between the groups might have artificiallyncreased impairment among the cardiac patients. In 37 ofhe 42 general linear models examined, we found no statis-ically significant difference in neurocognitive performancey sex, and we noticed no tendency for women to performetter or worse on the exams. For the five models in which
here was a statistically significant sex effect, men per-ormed better in three and women performed better in two.hus, there is no evidence to suggest that differencesetween the groups were due to the higher proportion of
emales in the control group, consistent with prior data inhis regard [24].
From a methodologic standpoint, differences withinhe present study between determinations of impairmenthen using normative standards versus control groupeans, or when using group means versus one standard
eviation outliers, highlight the vagaries in properlyefining neurocognitive impairment and the caution that
s needed in making such conclusions. More specifically,ur finding that the use of normative standards at times
ed to underreporting of impairments in the cardiacopulation underscores the importance of includingreal-life” standards in neurocognitive studies. In com-arison, inclusion of “one standard deviation” analysesf single subjects potentially minimizes the “diluted”eporting conveyed by analyses of group means. Wepecifically included each of these analyses in our reporto provide a more comprehensive picture of the extent ofmpairment found in our study subjects.
It is also important to emphasize that a substantial
umber of potential enrollees were excluded because of theby on June 9, 2013 als.org

pTtgtchifim
nbematCeFceacct
TATGt
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
D
DosP
1334 ROSENGART ET AL Ann Thorac SurgNEUROCOGNITIVE FUNCTION IN CABG AND PCI 2005;80:1327–35
CA
RD
IOV
AS
CU
LA
R
resence of risk factors for brain injury, such as prior stroke.he impairment of neurocognitive function in cardiac pa-
ients at baseline in the present study is even more strikingiven the exclusion of these neurocognitive high-risk pa-ients. Failure to take into account and appropriately ex-lude the relatively frequent occurrence of such patientsighlights potentially confounding factors in prior studies
n assessing the effects of CABG on a truly normallyunctioning patient—as opposed to one who may be signif-cantly impaired at baseline—even though these patients
ight not appear to be impaired to the casual observer.Given these findings, then, that a subset even of
ormal CABG patients will demonstrate marginalizedaseline cognitive reserve and may be at risk for postop-rative decline [23], preoperative cognitive screeningay be beneficial, especially if postoperative outcomes
re eventually correlated with preoperative status. Fur-her, it is interesting to speculate whether the presence ofAD might serve as a marker for cognitive dysfunctionven in settings where CABG is not being considered.inally, the present evidence of, in some cases, profoundognitive deficits in CABG or PCI patients at baseline,ven if these patients do not suffer additional intraoper-tive injury, suggests that adherence to medical regimenould be a problem for these patients, and warrantsaution in postoperative teaching and patient adherenceo medical regimens (eg, medication).
his work was supported by a grant from the American Heartssociation. We wish to thank Ronald Curran, Michael Frank,imothy Votapka, Barbara Cushing, Milicia Vukovic, Annealioto, Jenna Duffecy and Lina Nayak for their assistance on
his project.
eferences
1. Newman MF, Kirchner JL, Phillips-Bute B, et al. Longitudi-nal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med 2001;344:395–402.
2. Roach GW, Kanchuger M, Mangano CM, et al. Adversecerebral outcomes after coronary bypass surgery. N EnglJ Med 1996;335:1857–63.
3. Barbut D, Caplan LR. Cerebral emboli detected duringbypass surgery are associated with clamp removal. Stroke1994;25:2398–402.
4. Taylor KM. Brain damage during cardiopulmonary bypass.Ann Thorac Surg 1998;65:20–6.
5. Stern Y. What is cognitive reserve? Theory and researchapplication of the reserve concept. J Intern NeuropsychologSoc 2002;8:448–60.
6. Folstein, Folstein, McHugh, Fanjiang. MMSE: Mini-MentalState Examination user’s guide. Odessa, FL: PsychologicalAssessment Resources, 2004.
7. Scott JG, Krull KR, Williamson JG, Adams RL, Iverson GL.Oklahoma Premorbid Intelligence Estimation (OPIE): utili-
resbyterian as well as out of the group from Holland, and I
tc
y
ats.ctsnetjournDownloaded from
zation in clinical samples. Clin Neuropsychologist1997;11:146–54.
8. Barona A, Reynolds CR, Chastain R. A demographicallycased index of premorbid intelligence for the WAIS-R. JCons Clin Psychol 1984;52: 885–7.
9. Johnson T, Monk T, Rasmussen LS, et al. Postoperativecognitive dysfunction in middle-aged patients. Anesthesiol-ogy 2002;96:1351–7.
0. Saxton J, Ratcliff G, Newman A, et al. Cognitive test perfor-mance and presence of subclinical cardiovascular disease inthe cardiovascular health study. Neuroepidemiology 2000;19:312–9.
1. Fahlander K, Wahlin A, Fastbom J, et. al. The relationshipbetween signs of cardiovascular deficiency and cognitiveperformance in old age: a population-based study. J Geron-tology 2000;55:P259–65.
2. Baird DL, Murkin JM, Lee DL. Neurologic findings in coro-nary artery bypass patients: perioperative or pre-existing?J Cardiothorac Vasc Anesth 1997;1196:694–8.
3. Millar K, Asbury AJ, Murray GD. Pre-existing cognitiveimpairment as a factor influencing outcome after cardiacsurgery. Br J Anesthes 2001;86:63–7.
4. Knopman D, Boland LL, Mosley T, et al. Cardiovascular riskfactors and cognitive decline in middle-aged adults. Neurol-ogy 2001;56:42–8.
5. Moody DM, Brown WR, Challa VR, Stump DA, ReboussinDM, Legault C. Brain microemboli associated with cardio-pulmonary bypass: a histologic and magnetic resonanceimaging study. Ann Thorac Surg 1995;59:1304–7.
6. Zimpfer D, Czerny M, Vogt F, et al. Neurocognitive deficitfollowing coronary artery bypass grafting: a prospectivestudy of surgical patients and nonsurgical controls. AnnThorac Surg 2004;78:513–8.
7. Selnes OA, Grega MA, Borowicz LM Jr, Royall RM, McK-hann GM, Baumgartner WA. Cognitive changes with coro-nary artery disease: a prospective study of coronary arterybypass graft patients and nonsurgical controls. Ann ThoracSurg 2003;75:1377–84.
8. Rankin KP, Kochamba GS, Boone KB, Petitti DB, BuckwalterJG. Presurgical cognitive deficits in patients receiving coro-nary artery bypass graft surgery. J Int Neuropsychol Soc2003;9: 913–24.
9. Van Dijk D, Jansen EW, Hijman R, et al. Cognitive outcomeafter off-pump and on-pump coronary artery bypass graftsurgery: a randomized trial. JAMA 2002;287:1405–12.
0. Vingerhoets G, Van Nooten G, Jannes C. Neuropsychologi-cal impairment in candidates for cardiac surgery. J IntNeuropsychol Soc 1997;3:480–4.
1. Keith JR, Puente AE, Malcolmson KL, Tartt S, Coleman AE,Marks HF Jr. Assessing postoperative cognitive change aftercardiopulmonary bypass surgery. Neuropsychology 2002;16:411–21.
2. Treasure T, Smith PL, Newman S, et al. Impairment ofcerebral function following cardiac and other major surgery.Eur J Cardiothorac Surg 1989;3:216–21.
3. Murkin JM, Martzke JS, Buchan AM, Bentley C, Wong CJ. Arandomized study of the influence of perfusion techniqueand pH management strategy in 316 patients undergoingcoronary artery bypass surgery. II. Neurologic and cognitiveoutcomes. J Thorac Cardiovasc Surg 1995;110:349–62.
4. Hogue CW, Lillie R, Hershey T, et al. Gender influence on
vognitive function after cardiac operation. Ann Thorac Surg2003;76:1119–25.ISCUSSION
R PAUL KURLANSKY (Miami, FL): I want to congratulate youn a very interesting and very important study. Your baselinetudies corroborate studies that have come out of Columbia
hink it is an extremely important point, which needs to beorroborated, as you have done.
The question I had for you was in your CABG population did
ou make any distinction between patients who had surgeryby on June 9, 2013 als.org

ot
Drsaaae
DVcpttciipc
s
pttw
wkan
Dfipdoyspfaco
1335Ann Thorac Surg ROSENGART ET AL2005;80:1327–35 NEUROCOGNITIVE FUNCTION IN CABG AND PCI
CA
RD
IOV
AS
CU
LA
R
n-pump or off-pump, or were they all done by one technique orhe other? Thank you so much.
R ROSENGART: This study was originally planned as aandomized OPCAB versus CABG trial. We quite frankly wereo pleased about how our CABG patients were doing, overallnd from a neurocognitive standpoint that we were uncomfort-ble from an ethical standpoint with proceeding with OPCABG,nd in we actually completed the study as a straight CABGxamination.
R DIMITRI NOVITZKY (Tampa, FL): I am coinvestigator of aA cooperative study, Outcomes Following Myocardial Revas-
ularization On and Off Cardiopulmonary Bypass. All partici-ating patients undergo preoperative neurocognitive function,
hen after 3 months and at 1 year. In a substudy, neurocognitiveesting is administered to VA patients, who are not subjected tooronary surgery or any other surgical procedures. The objectives to define if there is a decline in cognitive function over 1 yearn nonoperated on patients as well as those operated on off-ump or on-pump. Therefore, having a real control group,omparisons with the surgical arms become more meaningful.
The results of the VA study are not available because the
tudy is still ongoing. The protocol design is to reach 2,400 tats.ctsnetjournDownloaded from
atients on both arms: 1,200 patients on-pump and 1,200 pa-ients off-pump. We expect that within 1 year we will completehe accrual. At the completion of the 1-year follow-up, the studyill be completed.Your study requires further follow-up than a month or 6eeks. I think you need to expand for 1 or 2 years. We don’tnow in a perspective randomized fashion what is the effect ofnesthesia, surgery, or any other interventions on the neurocog-itive function.
R ROSENGART: Thank you. In response to your comments,rst, we are going to continue our follow-up out to 1 yearostoperative. I think the fact that there was relatively littleifference at three weeks is highly encouraging, and we obvi-usly expect the results to become even more equalized at aear. We struggled with the question of our power and sampleize, and certainly a study on the order of that being contem-lated by your consortium is going to be important. We quite
rankly expect, seeing our results with very similar means, thatlthough a larger sample size may alter the statistical signifi-ance, from a pragmatic standpoint we think the similarity inutcomes between our control and CABG group should hold
rue even as the N of the study is increased.by on June 9, 2013 als.org

2005;80:1327-1335 Ann Thorac SurgHahn, Jesse Marymont and Timothy Sanborn
Todd K. Rosengart, Jerry Sweet, Eileen B. Finnin, Penny Wolfe, John Cashy, Elizabeth Intervention Compared With Normal Controls
Surgery or Percutaneous Coronary Intervention: Evidence of Impairment Before Neurocognitive Functioning in Patients Undergoing Coronary Artery Bypass Graft
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/80/4/1327including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/80/4/1327#BIBL
This article cites 22 articles, 8 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/80/4/1327#otherarticleThis article has been cited by 17 HighWire-hosted articles:
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 9, 2013 ats.ctsnetjournals.orgDownloaded from
Related Documents











